Label: APTIVUS- tipranavir capsule, liquid filled

- NDC Code(s): 0597-0003-02
- Packager: Boehringer Ingelheim Pharmaceuticals, Inc.
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: New Drug Application
Drug Label Information
Updated May 17, 2024
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use APTIVUS safely and effectively. See full prescribing information for APTIVUS.
APTIVUS® (tipranavir) capsules, for oral use
Initial U.S. Approval: 2005WARNING: HEPATOTOXICITY and INTRACRANIAL HEMORRHAGE
See full prescribing information for complete boxed warning.
RECENT MAJOR CHANGES
INDICATIONS AND USAGE
APTIVUS, a protease inhibitor, co-administered with ritonavir, is indicated for combination antiretroviral treatment of HIV-1 infected adult and pediatric patients weighing 36 kg or higher who are treatment-experienced and infected with HIV-1 strains resistant to more than one protease inhibitor (1)
- Do not use APTIVUS/ritonavir in treatment-naïve patients (1)
DOSAGE AND ADMINISTRATION
- Adults: 500 mg APTIVUS, co-administered with 200 mg ritonavir, twice daily (2.2)
- Pediatric patients (weighing 36 kg or higher): 500 mg APTIVUS, co-administered with 200 mg ritonavir twice daily. (2.2)
- APTIVUS taken with ritonavir tablets must be taken with meals (2.1)
- APTIVUS capsules must be swallowed whole and must not be opened or chewed (2.1)
- Children should be assessed for their ability to swallow capsules before prescribing APTIVUS capsules. (2.1)
- Store unopened bottles of APTIVUS capsules in the refrigerator. (16)
DOSAGE FORMS AND STRENGTHS
- Capsules: 250 mg (3)
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
- Co-administration with Ritonavir: APTIVUS must be co-administered with ritonavir and food to achieve the desired antiviral effect. Failure to administer APTIVUS with ritonavir and food may result in a loss of efficacy of tipranavir. (5.1)
- Hepatic Impairment: Discontinue for signs and symptoms of clinical hepatitis or asymptomatic increases in ALT/AST >10 times ULN or asymptomatic increases in ALT/AST 5-10 times ULN with concomitant increases in total bilirubin. Monitor liver function tests prior to therapy and frequently thereafter. (5.2)
- Intracranial Hemorrhage/Platelet Aggregation and Coagulation: Use with caution in patients at risk for increased bleeding or who are receiving medications that increase the risk of bleeding. (5.3, 5.5)
- The concomitant use of APTIVUS/ritonavir and certain other drugs may result in known or potentially significant drug interactions. Consult the full prescribing information prior to and during treatment for potential drug interactions. (5.4, 7.2)
- Rash: Discontinue and initiate appropriate treatment if severe skin reaction occurs or is suspected. (5.6) Use with caution in patients with a known sulfonamide allergy. (5.7)
- Patients may develop new onset or exacerbations of diabetes mellitus, hyperglycemia (5.8), immune reconstitution syndrome (5.9), redistribution/accumulation of body fat (5.10), and elevated lipids. (5.11) Monitor cholesterol and triglycerides prior to therapy and periodically thereafter.
- Hemophilia: Spontaneous bleeding may occur, and additional factor VIII may be required. (5.12)
ADVERSE REACTIONS
- In adults the most frequent adverse reactions (incidence >4%) were diarrhea, nausea, pyrexia, vomiting, fatigue, headache, and abdominal pain. (6.1)
- In pediatric subjects the most frequent adverse reactions were generally similar to those seen in adults. However, rash was more frequent in pediatric subjects than in adults. (6.2)
To report SUSPECTED ADVERSE REACTIONS, contact Boehringer Ingelheim Pharmaceuticals, Inc. at 1-800-542-6257 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 4/2024
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: HEPATOTOXICITY and INTRACRANIAL HEMORRHAGE
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Dosage and Administration Overview
2.2 Recommended Dosage in Adults and Pediatric Patients Weighing 36 kg or Higher
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Importance of Co-administration with Ritonavir
5.2 Hepatic Impairment and Toxicity
5.3 Intracranial Hemorrhage
5.4 Risk of Serious Adverse Reactions Due to Drug Interactions
5.5 Effects on Platelet Aggregation and Coagulation
5.6 Rash
5.7 Sulfa Allergy
5.8 Diabetes Mellitus/Hyperglycemia
5.9 Immune Reconstitution Syndrome
5.10 Fat Redistribution
5.11 Elevated Lipids
5.12 Patients with Hemophilia
5.13 Resistance/Cross Resistance
6 ADVERSE REACTIONS
6.1 Clinical Trials in Adults
6.2 Clinical Trials in Pediatrics
7 DRUG INTERACTIONS
7.1 Potential for APTIVUS/ritonavir to Affect Other Drugs
7.2 Potential for Other Drugs to Affect Tipranavir
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Hepatic Impairment
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
12.4 Microbiology
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
14.1 Clinical Trials in Adults
14.2 Clinical Trials in Pediatrics
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
BOXED WARNING
(What is this?)
WARNING: HEPATOTOXICITY and INTRACRANIAL HEMORRHAGE
Hepatotoxicity:
Clinical hepatitis and hepatic decompensation, including some fatalities, have been reported. Extra vigilance is warranted in patients with chronic hepatitis B or hepatitis C co-infection, as these patients have an increased risk of hepatotoxicity [see Warnings and Precautions (5.2)].
Intracranial Hemorrhage:
Both fatal and non-fatal intracranial hemorrhage have been reported [see Warnings and Precautions (5.3)].
-
1 INDICATIONS AND USAGE
APTIVUS, co-administered with ritonavir, is indicated for combination antiretroviral treatment of HIV-1 infected adults and pediatric patients weighing 36 kg or higher who are treatment-experienced and infected with HIV-1 strains resistant to more than one protease inhibitor (PI) [see Use in Specific Populations (8.4)].
This indication is based on analyses of plasma HIV-1 RNA levels in two controlled studies of APTIVUS/ritonavir of 48 weeks duration in treatment-experienced adults and one open-label 48-week study in pediatric patients. The adult studies were conducted in clinically advanced, 3-class antiretroviral (NRTI, NNRTI, PI) treatment-experienced adults with evidence of HIV-1 replication despite ongoing antiretroviral therapy.
The following points should be considered when initiating therapy with APTIVUS/ritonavir:
- The use of APTIVUS/ritonavir in treatment-naïve patients is not recommended [see Warnings and Precautions (5.2)].
- The use of other active agents with APTIVUS/ritonavir is associated with a greater likelihood of treatment response [see Microbiology (12.4) and Clinical Studies (14)].
- Genotypic or phenotypic testing and/or treatment history should guide the use of APTIVUS/ritonavir [see Microbiology (12.4)]. The number of baseline primary protease inhibitor mutations affects the virologic response to APTIVUS/ritonavir [see Microbiology (12.4)].
- Use caution when prescribing APTIVUS/ritonavir to patients with elevated transaminases, hepatitis B or C co-infection or patients with mild hepatic impairment [see Warnings and Precautions (5.2)].
- Liver function tests should be performed at initiation of therapy with APTIVUS/ritonavir and monitored frequently throughout the duration of treatment [see Warnings and Precautions (5.2)].
- The drug-drug interaction potential of APTIVUS/ritonavir when co-administered with other drugs must be considered prior to and during APTIVUS/ritonavir use [see Contraindications (4) and Drug Interactions (7)].
- Use caution when prescribing APTIVUS/ritonavir in patients who may be at risk for increased bleeding or who are receiving medications known to increase the risk of bleeding [see Warnings and Precautions (5.5)].
There are no study results demonstrating the effect of APTIVUS/ritonavir on clinical progression of HIV-1.
-
2 DOSAGE AND ADMINISTRATION
2.1 Dosage and Administration Overview
APTIVUS must be co-administered with ritonavir to exert its therapeutic effect. Failure to correctly co-administer APTIVUS with ritonavir will result in plasma levels of tipranavir that will be insufficient to achieve the desired antiviral effect and will alter some drug interactions [see Warnings and Precautions (5.1)].
- Children should be assessed for their ability to swallow capsules before prescribing APTIVUS capsules [see Use in Specific Populations (8.4)].
- APTIVUS co-administered with ritonavir tablets must only be taken with meals [see Clinical Pharmacology (12.3)].
- APTIVUS is supplied as capsules. APTIVUS capsules must be swallowed whole and must not be opened or chewed.
- Due to the need for co-administration of APTIVUS with ritonavir, please refer to the ritonavir prescribing information.
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
- APTIVUS is contraindicated in patients with moderate or severe (Child-Pugh Class B or C, respectively) hepatic impairment [see Warnings and Precautions (5.2)].
- APTIVUS/ritonavir is contraindicated when co-administered with drugs that are highly dependent on CYP3A for clearance or are potent CYP3A inducers (see Table 1) [see Drug Interactions (7.2)].
Table 1 Drugs that are Contraindicated with APTIVUS Co-Administered with Ritonavir Drug Class Drugs within Class that are Contraindicated with APTIVUS Co-administered with Ritonavir Clinical Comments: Alpha 1-adrenoreceptor antagonist Alfuzosin Potentially increased alfuzosin concentrations can result in hypotension. Antiarrhythmics Amiodarone, bepridil, flecainide, propafenone, quinidine Potential for serious and/or life-threatening reactions such as cardiac arrhythmias secondary to increases in plasma concentrations of antiarrhythmics. Antimycobacterials Rifampin May lead to loss of virologic response and possible resistance to APTIVUS or to the class of protease inhibitors or other co-administered antiretroviral agents. Ergot derivatives Dihydroergotamine, ergonovine, ergotamine, methylergonovine Potential for acute ergot toxicity characterized by peripheral vasospasm and ischemia of the extremities and other tissues. GI motility agent Cisapride Potential for cardiac arrhythmias. Herbal products St. John's wort (hypericum perforatum) May lead to loss of virologic response and possible resistance to APTIVUS or to the class of protease inhibitors. HMG CoA reductase inhibitors Lovastatin, simvastatin Potential for myopathy including rhabdomyolysis. Antipsychotics Pimozide Potential for cardiac arrhythmias. Lurasidone Potential for serious and/or life-threatening reactions. PDE-5 inhibitors Sildenafil (Revatio) [for treatment of pulmonary arterial hypertension] A safe and effective dose has not been established when used with APTIVUS/ritonavir. There is increased potential for sildenafil-associated adverse events (which include visual disturbances, hypotension, prolonged erection, and syncope). Sedatives/hypnotics Oral midazolam, triazolam Prolonged or increased sedation or respiratory depression. Due to the need for co-administration of APTIVUS with ritonavir, please refer to the ritonavir prescribing information for a description of ritonavir contraindications.
-
5 WARNINGS AND PRECAUTIONS
5.1 Importance of Co-administration with Ritonavir
APTIVUS must be co-administered with ritonavir and food to achieve the desired antiviral effect. Failure to administer APTIVUS with ritonavir and food may result in a loss of efficacy of tipranavir. Please refer to the ritonavir prescribing information for additional information on precautionary measures.
5.2 Hepatic Impairment and Toxicity
Clinical hepatitis and hepatic decompensation, including some fatalities, were reported with APTIVUS co-administered with 200 mg of ritonavir. These have generally occurred in subjects with advanced HIV-1 disease taking multiple concomitant medications. A causal relationship to APTIVUS/ritonavir could not be established. Physicians and patients should be vigilant for the appearance of signs or symptoms of hepatitis, such as fatigue, malaise, anorexia, nausea, jaundice, bilirubinuria, acholic stools, liver tenderness or hepatomegaly. Patients with signs or symptoms of clinical hepatitis should discontinue APTIVUS/ritonavir treatment and seek medical evaluation.
All patients should be followed closely with clinical and laboratory monitoring, especially those with chronic hepatitis B or C co-infection, as these patients have an increased risk of hepatotoxicity. Liver function tests should be performed prior to initiating therapy with APTIVUS/ritonavir, and frequently throughout the duration of treatment.
If asymptomatic elevations in AST or ALT greater than 10 times the upper limit of normal occur, APTIVUS/ritonavir therapy should be discontinued. If asymptomatic elevations in AST or ALT between 5 – 10 times the upper limit of normal and increases in total bilirubin greater than 2.5 times the upper limit of normal occur, APTIVUS/ritonavir therapy should be discontinued.
Treatment-experienced patients with chronic hepatitis B or hepatitis C co-infection or elevated transaminases are at approximately 2-fold risk for developing Grade 3 or 4 transaminase elevations or hepatic decompensation. In two large, randomized, open-label, controlled clinical trials with an active comparator (1182.12 and 1182.48) of treatment-experienced subjects, Grade 3 and 4 increases in hepatic transaminases were observed in 10.3% (10.9/100 PEY) receiving APTIVUS/ritonavir through week 48. In a study of treatment-naïve subjects, 20.3% (21/100 PEY) experienced Grade 3 or 4 hepatic transaminase elevations while receiving APTIVUS/ritonavir 500 mg/200 mg through week 48.
Tipranavir is principally metabolized by the liver. Caution should be exercised when administering APTIVUS/ritonavir to patients with mild hepatic impairment (Child-Pugh Class A) because tipranavir concentrations may be increased [see Clinical Pharmacology (12.3)].
5.3 Intracranial Hemorrhage
APTIVUS, co-administered with 200 mg of ritonavir, has been associated with reports of both fatal and non-fatal intracranial hemorrhage (ICH). Many of these subjects had other medical conditions or were receiving concomitant medications that may have caused or contributed to these events. No pattern of abnormal coagulation parameters has been observed in subjects in general, or preceding the development of ICH. Therefore, routine measurement of coagulation parameters is not currently indicated in the management of patients on APTIVUS.
5.4 Risk of Serious Adverse Reactions Due to Drug Interactions
Initiation of APTIVUS/ritonavir, a CYP3A inhibitor, in patients receiving medications metabolized by CYP3A or initiation of medications metabolized by CYP3A in patients already receiving APTIVUS/ritonavir, may increase plasma concentrations of medications metabolized by CYP3A. Initiation of medications that inhibit or induce CYP3A may increase or decrease concentrations of APTIVUS/ritonavir, respectively. These interactions may lead to:
- Clinically significant adverse reactions, potentially leading to severe, life-threatening, or fatal events from greater exposures of concomitant medications.
- Clinically significant adverse reactions from greater exposures of APTIVUS/ritonavir.
- Loss of therapeutic effect of APTIVUS/ritonavir and possible development of resistance.
See Table 4 for steps to prevent or manage these possible and known significant drug interactions, including dosing recommendations [see Drug Interactions (7)]. Consider the potential for drug interactions prior to and during APTIVUS/ritonavir therapy; review concomitant medications during APTIVUS/ritonavir therapy; and monitor for the adverse reactions associated with the concomitant medications [see Contraindications (4) and Drug Interactions (7)].
5.5 Effects on Platelet Aggregation and Coagulation
APTIVUS/ritonavir should be used with caution in patients who may be at risk of increased bleeding from trauma, surgery or other medical conditions, or who are receiving medications known to increase the risk of bleeding such as antiplatelet agents and anticoagulants, or who are taking supplemental high doses of vitamin E.
In rats, tipranavir treatment alone induced dose-dependent changes in coagulation parameters, bleeding events and death. Co-administration with vitamin E significantly increased these effects [see Nonclinical Toxicology (13.2)]. However, analyses of stored plasma from adult and pediatric subjects treated with APTIVUS capsules plus low-dose ritonavir showed no effect of APTIVUS/ritonavir on vitamin K-dependent coagulation factors (Factor II and Factor VII), Factor V, or on prothrombin or activated partial thromboplastin times.
In in vitro experiments, tipranavir was observed to inhibit human platelet aggregation at levels consistent with exposures observed in subjects receiving APTIVUS/ritonavir.
5.6 Rash
Rash, including urticarial rash, maculopapular rash, and possible photosensitivity, has been reported in subjects receiving APTIVUS/ritonavir. In some cases rash was accompanied by joint pain or stiffness, throat tightness, or generalized pruritus. In controlled adult clinical trials, rash (all grades, all causality) was observed in 10% of females and in 8% of males receiving APTIVUS/ritonavir through 48 weeks of treatment. The median time to onset of rash was 53 days and the median duration of rash was 22 days. The discontinuation rate for rash in clinical trials was 0.5%. In an uncontrolled compassionate use program (n=3920), cases of rash, some of which were severe, accompanied by myalgia, fever, erythema, desquamation, and mucosal erosions were reported. In the pediatric clinical trial, the frequency of rash (all grades, all causality) through 48 weeks of treatment was 21%. Overall, most of the pediatric subjects had mild rash and 5 (5%) had moderate rash. Overall 3% of pediatric subjects interrupted APTIVUS treatment due to rash and the discontinuation rate for rash in pediatric subjects was 0.9%. Discontinue and initiate appropriate treatment if severe skin rash develops.
5.7 Sulfa Allergy
APTIVUS should be used with caution in patients with a known sulfonamide allergy. Tipranavir contains a sulfonamide moiety. The potential for cross-sensitivity between drugs in the sulfonamide class and APTIVUS is unknown.
5.8 Diabetes Mellitus/Hyperglycemia
New onset diabetes mellitus, exacerbation of pre-existing diabetes mellitus and hyperglycemia have been reported during post-marketing surveillance in HIV-1 infected patients receiving protease inhibitor therapy. Some patients required either initiation or dose adjustments of insulin or oral hypoglycemic agents for treatment of these events. In some cases, diabetic ketoacidosis has occurred. In those patients who discontinued protease inhibitor therapy, hyperglycemia persisted in some cases. Because these events have been reported voluntarily during clinical practice, estimates of frequency cannot be made and a causal relationship between protease inhibitor therapy and these events has not been established.
5.9 Immune Reconstitution Syndrome
Immune reconstitution syndrome has been reported in patients treated with combination antiretroviral therapy, including APTIVUS. During the initial phase of combination antiretroviral treatment, patients whose immune system responds may develop an inflammatory response to indolent or residual opportunistic infections (such as Mycobacterium avium infection, cytomegalovirus, Pneumocystis jiroveci pneumonia, tuberculosis, or reactivation of herpes simplex and herpes zoster), which may necessitate further evaluation and treatment.
Autoimmune disorders (such as Graves' disease, polymyositis, and Guillain-Barré syndrome) have also been reported to occur in the setting of immune reconstitution, however, the time to onset is more variable, and can occur many months after initiation of treatment.
5.10 Fat Redistribution
Redistribution/accumulation of body fat including central obesity, dorsocervical fat enlargement (buffalo hump), peripheral wasting, facial wasting, breast enlargement, and "cushingoid appearance" have been observed in patients receiving antiretroviral therapy. The mechanism and long-term consequences of these events are currently unknown. A causal relationship has not been established.
5.11 Elevated Lipids
Treatment with APTIVUS co-administered with 200 mg of ritonavir has resulted in large increases in the concentration of total cholesterol and triglycerides [see Adverse Reactions (6)]. Triglyceride and cholesterol testing should be performed prior to initiating APTIVUS/ritonavir therapy and at periodic intervals during therapy. Lipid disorders should be managed as clinically appropriate; taking into account any potential drug-drug interactions [see Drug Interactions (7.2)].
5.12 Patients with Hemophilia
There have been reports of increased bleeding, including spontaneous skin hematomas and hemarthrosis in patients with hemophilia type A and B treated with protease inhibitors. In some patients additional Factor VIII was given. In more than half of the reported cases, treatment with protease inhibitors was continued or reintroduced if treatment had been discontinued. A causal relationship between protease inhibitors and these events has not been established.
-
6 ADVERSE REACTIONS
The following adverse reactions are described, in greater detail, in other sections:
- Hepatic Impairment and Toxicity [see Warnings and Precautions (5.2)]
- Intracranial Hemorrhage [see Warnings and Precautions (5.3)]
- Rash [see Warnings and Precautions (5.6)]
Due to the need for co-administration of APTIVUS with ritonavir, please refer to ritonavir prescribing information for ritonavir-associated adverse reactions.
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
6.1 Clinical Trials in Adults
APTIVUS, co-administered with ritonavir, has been studied in a total of 6308 HIV-1 positive adults as combination therapy in clinical studies. Of these, 1299 treatment-experienced subjects received the dose of 500 mg/200 mg BID. Nine hundred nine (909) adults, including 541 in the 1182.12 and 1182.48 controlled clinical trials, have been treated for at least 48 weeks [see Clinical Studies (14)].
In 1182.12 and 1182.48 in the APTIVUS/ritonavir arm, the most frequent adverse reactions were diarrhea, nausea, pyrexia, vomiting, fatigue, headache, and abdominal pain. The 48-Week Kaplan-Meier rates of adverse reactions leading to discontinuation were 13.3% for APTIVUS/ritonavir-treated subjects and 10.8% for the comparator arm subjects.
Adverse reactions reported in the controlled clinical trials 1182.12 and 1182.48, based on treatment-emergent clinical adverse reactions of moderate to severe intensity (Grades 2 - 4) in at least 2% of treatment-experienced subjects in either treatment group are summarized in Table 2 below.
Table 2 Adverse Reactions Reported in Randomized, Controlled Clinical Trials (1182.12 and 1182.48) Based on Treatment-Emergent Clinical Adverse Reactions of Moderate to Severe Intensity (Grades 2 - 4) in at least 2% of Treatment-Experienced Subjects in either Treatment Groupa (48-week Analyses) Percentage of patients (rate per 100 patient-exposure years) APTIVUS/ritonavir (500/200 mg BID) + OBRc
(n=749; 757.4 patient-exposure years)Comparator PI/ritonavirb + OBR
(n=737; 503.9 patient-exposure years)aExcludes laboratory abnormalities that were Adverse Events bComparator PI/ritonavir: lopinavir/ritonavir 400/100 mg BID, indinavir/ritonavir 800/100 mg BID, saquinavir/ritonavir 1000/100 mg BID, amprenavir/ritonavir 600/100 mg BID cOptimized Background Regimen Blood and Lymphatic Disorders Anemia 3.3% (3.4) 2.3% (3.4) Neutropenia 2.0% (2.0) 1.0% (1.4) Gastrointestinal Disorders Diarrhea 15.0% (16.5) 13.4% (21.6) Nausea 8.5% (9.0) 6.4% (9.7) Vomiting 5.9% (6.0) 4.1% (6.1) Abdominal pain 4.4% (4.5) 3.4% (5.1) Abdominal pain upper 1.5% (1.5) 2.3% (3.4) General Disorders Pyrexia 7.5% (7.7) 5.4% (8.2) Fatigue 5.7% (5.9) 5.6% (8.4) Investigations Weight decreased 3.1% (3.1) 2.2% (3.2) ALT increased 2.0% (2.0) 0.5% (0.8) GGT increased 2.0% (2.0) 0.4% (0.6) Metabolism and Nutrition Disorders Hypertriglyceridemia 3.9% (4.0) 2.0% (3.0) Hyperlipidemia 2.5% (2.6) 0.8% (1.2) Dehydration 2.1% (2.1) 1.1% (1.6) Musculoskeletal and Connective Tissue Disorders Myalgia 2.3% (2.3) 1.8% (2.6) Nervous System Disorders Headache 5.2% (5.3) 4.2% (6.3) Peripheral neuropathy 1.5% (1.5) 2.0% (3.0) Psychiatric Disorders Insomnia 1.7% (1.7) 3.7% (5.5) Respiratory, Thoracic and Mediastinal Disorders Dyspnea 2.1% (2.1) 1.0% (1.4) Skin and Subcutaneous Tissue Disorders Rash 3.1% (3.1) 3.8% (5.7) Less Common Adverse Reactions
Other adverse reactions reported in <2% of adult subjects (n=1474) treated with APTIVUS/ritonavir 500 mg/200 mg in Phase 2 and 3 clinical trials are listed below by body system:
Blood and Lymphatic System Disorders: thrombocytopenia
Gastrointestinal Disorders: abdominal distension, dyspepsia, flatulence, gastroesophageal reflux disease, pancreatitis
General Disorders: influenza-like illness, malaise
Hepatobiliary Disorders: hepatitis, hepatic failure, hyperbilirubinemia, cytolytic hepatitis, toxic hepatitis, hepatic steatosis
Immune System Disorders: hypersensitivity
Investigations: hepatic enzymes increased, liver function test abnormal, lipase increased
Metabolism and Nutrition Disorders: anorexia, decreased appetite, diabetes mellitus, facial wasting, hyperamylasemia, hypercholesterolemia, hyperglycemia, mitochondrial toxicity
Musculoskeletal and Connective Tissue Disorders: muscle cramp
Nervous System Disorders: dizziness, intracranial hemorrhage, somnolence
Psychiatric Disorders: sleep disorder
Renal and Urinary Disorders: renal insufficiency
Skin and Subcutaneous System Disorders: exanthem, lipoatrophy, lipodystrophy acquired, lipohypertrophy, pruritus
Laboratory Abnormalities
Treatment-emergent laboratory abnormalities reported at 48 weeks in the controlled clinical trials 1182.12 and 1182.48 in adults are summarized in Table 3 below.
Table 3 Treatment-Emergent Laboratory Abnormalities Reported in ≥2% of Adult Patients (48-week Analyses) Randomized, Controlled Clinical Trials 1182.12 and 1182.48 Percentage of Patients (rate per 100 patient-exposure years) Limit APTIVUS/ritonavir (500/200 mg BID) + OBR
(n=738)Comparator PI/ritonavir + OBR*
(n=724)*Comparator PI/ritonavir: lopinavir/ritonavir 400/100 mg BID, indinavir/ritonavir 800/100 mg BID, saquinavir/ritonavir 1000/100 mg BID, amprenavir/ritonavir 600/100 mg BID Hematology WBC count decrease Grade 3 <2.0 × 103/µL 5.4% (5.6) 4.8% (7.7) Grade 4 <1.0 × 103/µL 0.3% (0.3) 1.1% (1.7) Chemistry Amylase Grade 3 >2.5 × ULN 5.7% (5.9) 6.4% (10.4) Grade 4 >5 × ULN 0.3% (0.3) 0.7% (1.1) ALT Grade 2 >2.5-5 × ULN 14.9% (16.5) 7.5% (12.4) Grade 3 >5-10 × ULN 5.6% (5.7) 1.7% (2.6) Grade 4 >10 × ULN 4.1% (4.1) 0.4% (0.7) AST Grade 2 >2.5-5 × ULN 9.9% (10.5) 8.0% (13.3) Grade 3 >5-10 × ULN 4.5% (4.6) 1.4% (2.2) Grade 4 >10 × ULN 1.6% (1.6) 0.4% (0.6) ALT and/or AST Grade 2-4 >2.5 × ULN 26.0% (31.5) 13.7% (23.8) Cholesterol Grade 2 >300 – 400 mg/dL 15.6% (17.7) 6.4% (10.5) Grade 3 >400 – 500 mg/dL 3.3% (3.3) 0.3% (0.4) Grade 4 >500 mg/dL 0.9% (1.0) 0.1% (0.2) Triglycerides Grade 2 400 – 750 mg/dL 35.9% (49.9) 26.8% (51.0) Grade 3 >750 – 1200 mg/dL 16.9% (19.4) 8.7% (14.6) Grade 4 >1200 mg/dL 8.0% (8.4) 4.3% (7.0) In controlled clinical trials 1182.12 and 1182.48 extending up to 96 weeks, the proportion of subjects who developed Grade 2-4 ALT and/or AST elevations increased from 26% at week 48 to 32.1% at week 96 with APTIVUS/ritonavir. The risk of developing transaminase elevations is greater during the first year of therapy.
6.2 Clinical Trials in Pediatrics
APTIVUS, co-administered with ritonavir, has been studied in a total of 135 HIV-1 infected pediatric subjects as combination therapy. Study 1182.14 enrolled HIV-1 infected, treatment-experienced pediatric subjects (with the exception of 3 treatment-naïve subjects), with baseline HIV-1 RNA of at least 1500 copies/mL. One hundred and ten (110) subjects were enrolled in a randomized, open-label 48-week clinical trial (Study 1182.14) and 25 subjects were enrolled in other clinical studies including Expanded Access and Emergency Use Programs.
The adverse reactions profile seen in Study 1182.14 was similar to adults. However, rash (5.5%), was reported more frequently in pediatric subjects than in adults.
The most common Grade 3-4 laboratory abnormalities were increases in CPK (11%), ALT (6.5%), and amylase (7.5%).
-
7 DRUG INTERACTIONS
7.1 Potential for APTIVUS/ritonavir to Affect Other Drugs
APTIVUS co-administered with ritonavir at the recommended dose is a net inhibitor of CYP3A and may increase plasma concentrations of agents that are primarily metabolized by CYP3A. Thus, co-administration of APTIVUS/ritonavir with drugs highly dependent on CYP3A for clearance and for which elevated plasma concentrations are associated with serious and/or life-threatening events is contraindicated [see Contraindications (4)]. Co-administration with other CYP3A substrates may require a dose adjustment or additional monitoring [see Drug Interactions (7)].
Clinically significant drug-drug interactions of APTIVUS co-administered with ritonavir are summarized in Table 4 below.
A phenotypic cocktail study was conducted with 16 healthy volunteers to quantify the influence of 10 days of APTIVUS/ritonavir capsule administration on the activity of hepatic CYP1A2 (caffeine), 2C9 (warfarin), 2C19 (omeprazole), 2D6 (dextromethorphan) and the activity of intestinal and hepatic CYP3A4/5 (midazolam) and P-glycoprotein (P-gp) (digoxin). This study determined the first-dose and steady-state effects of 500 mg of APTIVUS co-administered with 200 mg of ritonavir twice daily in capsule form.
There was no net effect on CYP2C9 or hepatic P-gp at first dose or steady state. There was no net effect after first dose on CYP1A2, but there was moderate induction at steady state. There was modest inhibition of CYP2C19 at the first dose, but there was marked induction at steady state. Potent inhibition of CYP2D6 and both hepatic and intestinal CYP3A4/5 activities were observed after first dose and steady state.
Intestinal and hepatic P-gp activity was assessed by administering oral and intravenous digoxin, respectively. The digoxin results indicate P-gp was inhibited after the first dose of APTIVUS/ritonavir followed by induction of P-gp over time. Thus, it is difficult to predict the net effect of APTIVUS administered with ritonavir on oral bioavailability and plasma concentrations of drugs that are dual substrates of CYP3A and P-gp. The net effect will vary depending on the relative affinity of the co-administered drugs for CYP3A and P-gp, and the extent of intestinal first-pass metabolism/efflux. An in vitro induction study in human hepatocytes showed an increase in UGT1A1 by tipranavir similar to that evoked by rifampin. The clinical consequences of this finding have not been established.
7.2 Potential for Other Drugs to Affect Tipranavir
Tipranavir is a CYP3A substrate and a P-gp substrate. Co-administration of APTIVUS/ritonavir and drugs that induce CYP3A and/or P-gp may decrease tipranavir plasma concentrations. Co-administration of APTIVUS/ritonavir and drugs that inhibit P-gp may increase tipranavir plasma concentrations. Co-administration of APTIVUS/ritonavir with drugs that inhibit CYP3A may not further increase tipranavir plasma concentrations, because the level of metabolites is low following steady-state administration of APTIVUS/ritonavir 500 mg/200 mg twice daily.
Clinically significant drug-drug interactions of APTIVUS co-administered with ritonavir are summarized in Table 4 below [see Contraindications (4), Warnings and Precautions (5.4), and Clinical Pharmacology (12.3)].
Table 4 Established and Other Potentially Significant Drug Interactions: Alterations in Dose or Regimen May be Recommended Based on Drug Interaction Studies or Predicted Interaction Concomitant Drug Class:
Drug nameEffect on Concentration of Tipranavir or Concomitant Drug Clinical Comment ↑ increase, ↓ decrease, ↔ no change, ↕ unable to predict HIV-1 Antiviral Agents Fusion Inhibitors: Enfuvirtide ↑ Tipranavir At steady state, tipranavir trough concentrations were approximately 45% higher in patients co-administered enfuvirtide in the Phase 3 trials. The mechanism for this increase is not known. Dose adjustments are not recommended. Non-Nucleoside Reverse Transcriptase Inhibitors: Etravirine ↓ Etravirine APTIVUS/ritonavir when coadministered with etravirine may cause a significant decrease in the plasma concentrations of etravirine and loss of therapeutic effect of etravirine. Etravirine and APTIVUS/ritonavir should not be coadministered. Rilpivirine The use of rilpivirine co-administered with APTIVUS/ritonavir has not been studied. Concomitant use of rilpivirine with Aptivus/ritonavir may cause an increase in the plasma concentrations of rilpivirine (inhibition of CYP3A enzymes). Rilpivirine is not expected to affect the plasma concentrations of Aptivus/ritonavir. Nucleoside Reverse Transcriptase Inhibitors: Abacavir ↓ Abacavir AUC by approximately 40% Clinical relevance of reduction in abacavir levels not established. Dose adjustment of abacavir cannot be recommended at this time. Didanosine (EC) ↓ Didanosine Clinical relevance of reduction in didanosine levels not established. For optimal absorption, didanosine should be separated from APTIVUS/ritonavir dosing by at least 2 hours. Zidovudine ↓ Zidovudine AUC by approximately 35%. ZDV glucuronide concentrations were unaltered. Clinical relevance of reduction in zidovudine levels not established. Dose adjustment of zidovudine cannot be recommended at this time. Protease Inhibitors (co-administered with 200 mg of ritonavir): Fosamprenavir ↓ Amprenavir Combining a protease inhibitor with APTIVUS/ritonavir is not recommended. Lopinavir ↓ Lopinavir Saquinavir ↓ Saquinavir Protease Inhibitors (co-administered with 100 mg of ritonavir): Atazanavir ↓ Atazanavir ↑ Tipranavir Virus Integrase Strand Transfer Inhibitors (INSTI): Raltegravir ↓ Raltegravir No dose adjustment is needed for 400 mg twice daily dosing regimen of raltegravir. For all other dosing regimens of raltegravir, refer to current prescribing information for raltegravir. Dolutegravir ↓ Dolutegravir For dosage recommendations, refer to dolutegravir prescribing information. Agents for Opportunistic Infections Antifungals: Fluconazole
Itraconazole
Ketoconazole↑ Tipranavir, ↔ Fluconazole Fluconazole increases tipranavir concentrations but dose adjustments are not needed. Fluconazole doses >200 mg/day are not recommended. Voriconazole ↑ Itraconazole (not studied) ↑ Ketoconazole (not studied) Based on theoretical considerations itraconazole and ketoconazole should be used with caution. High doses (>200 mg/day) are not recommended. ↕ Voriconazole (not studied) Due to multiple enzymes involved with voriconazole metabolism, it is difficult to predict the interaction. Antimycobacterials: Clarithromycin ↑ Tipranavir, ↑ Clarithromycin,
↓ 14-hydroxy-clarithromycin metaboliteNo dose adjustment of APTIVUS or clarithromycin for patients with normal renal function is necessary. For patients with renal impairment the following dosage adjustments should be considered: - For patients with CLCR 30 to 60 mL/min the dose of clarithromycin should be reduced by 50%.
- For patients with CLCR <30 mL/min the dose of clarithromycin should be decreased by 75%.
Rifabutin Tipranavir not changed, ↑Rifabutin
↑ Desacetyl-rifabutinSingle dose study. Dosage reductions of rifabutin by 75% are recommended (e.g., 150 mg every other day). Increased monitoring for adverse events in patients receiving the combination is warranted. Further dosage reduction may be necessary. Other Agents Commonly Used Anticonvulsants: Carbamazepine
Phenobarbital
Phenytoin↓ Tipranavir Caution should be used when prescribing carbamazepine, phenobarbital and/or phenytoin. APTIVUS may be less effective due to decreased tipranavir plasma concentration in patients taking these agents concomitantly. Valproic Acid ↓ Valproic Acid Caution should be used when prescribing valproic acid. Valproic acid may be less effective due to decreased valproic acid plasma concentration in patients taking APTIVUS concomitantly. Antidepressants: Trazodone ↑ Trazodone Concomitant use of trazodone and APTIVUS/ritonavir may increase plasma concentrations of trazodone. Adverse events of nausea, dizziness, hypotension, and syncope have been observed following co-administration of trazodone and ritonavir. If trazodone is used with a CYP3A4 inhibitor such as APTIVUS/ritonavir, the combination should be used with caution and a lower dose of trazodone should be considered. Desipramine Combination with APTIVUS/ritonavir not studied
↑ DesipramineDosage reduction and concentration monitoring of desipramine is recommended. Selective Serotonin-Reuptake Inhibitors: Combination with APTIVUS/ritonavir not studied Antidepressants have a wide therapeutic index, but doses may need to be adjusted upon initiation of APTIVUS/ritonavir therapy. Fluoxetine
Paroxetine
Sertraline↑ Fluoxetine
↑ Paroxetine
↑ SertralineAnti-gout Colchicine ↑ Colchicine In patients with renal or hepatic impairment, co-administration of colchicine in patients on APTIVUS/ritonavir is contraindicated. In combination with APTIVUS/ritonavir, the following dosage adjustments are recommended in patients with normal renal and hepatic function: Treatment of gout flares: Co-administration of colchicine in patients on APTIVUS/ritonavir: - 0.6 mg (1 tablet) × 1 dose, followed by 0.3 mg (half tablet) 1 hour later. Dose to be repeated no earlier than 3 days.
Prophylaxis of gout flares: Co-administration of colchicine in patients on APTIVUS/ritonavir: - If the original colchicine regimen was 0.6 mg twice a day, the regimen should be adjusted to 0.3 mg once a day.
- If the original colchicine regimen was 0.6 mg once a day, the regimen should be adjusted to 0.3 mg once every other day.
Treatment of familial Mediterranean fever (FMF): Co-administration of colchicine in patients on APTIVUS/ritonavir: - Maximum daily dose of 0.6 mg (may be given as 0.3 mg twice a day).
Antipsychotics: Quetiapine ↑ Quetiapine Initiation of APTIVUS with ritonavir in patients taking quetiapine: Consider alternative antiretroviral therapy to avoid increases in quetiapine exposures. If co-administration is necessary, reduce the quetiapine dose to 1/6 of the current dose and monitor for quetiapine-associated adverse reactions. Refer to the quetiapine prescribing information for recommendations on adverse reaction monitoring. Initiation of quetiapine in patients taking APTIVUS with ritonavir: Refer to the quetiapine prescribing information for initial dosing and titration of quetiapine. Benzodiazepines: Parenterally administered midazolam ↑ Midazolam Midazolam is extensively metabolized by CYP3A4. Increases in the concentration of midazolam are expected to be significantly higher with oral than parenteral administration. Therefore, APTIVUS should not be given with orally administered midazolam [see Contraindications (4)]. If APTIVUS is co-administered with parenteral midazolam, close clinical monitoring for respiratory depression and/or prolonged sedation should be exercised and dosage adjustments should be considered. Buprenorphine/naloxone ↔ Buprenorphine
↓ TipranavirAPTIVUS/ritonavir did not result in changes in the clinical efficacy of buprenorphine/naloxone. Compared to historical controls tipranavir Cmin was decreased approximately 40% with this combination. Dose adjustments cannot be recommended. Calcium Channel Blockers: Combination with APTIVUS/ritonavir not studied. Cannot predict effect of TPV/ritonavir on calcium channel blockers that are dual substrates of CYP3A and P-gp due to conflicting effect of TPV/ritonavir on CYP3A and P-gp. Caution is warranted and clinical monitoring of patients is recommended. Diltiazem
Felodipine
Nicardipine
Nisoldipine
Verapamil↕ Diltiazem
↑ Felodipine (CYP3A substrate but not P-gp substrate)
↕ Nicardipine
↕ Nisoldipine (CYP3A substrate but not clear whether it is a P-gp substrate)
↕ VerapamilDisulfiram/Metronidazole Combination with TPV/ritonavir not studied APTIVUS capsules contain alcohol that can produce disulfiram-like reactions when co-administered with disulfiram or other drugs which produce this reaction (e.g., metronidazole). Endothelin receptor antagonists Co-administration of bosentan in patients on APTIVUS/ritonavir: Bosentan ↑ Bosentan In patients who have been receiving APTIVUS/ritonavir for at least 10 days, start bosentan at 62.5 mg once daily or every other day based upon individual tolerability. Co-administration of APTIVUS/ritonavir in patients on bosentan: Discontinue use of bosentan at least 36 hours prior to initiation of APTIVUS/ritonavir. After at least 10 days following the initiation of APTIVUS/ritonavir, resume bosentan at 62.5 mg once daily or every other day based upon individual tolerability. HMG-CoA Reductase Inhibitors: Atorvastatin
Rosuvastatin↑ Atorvastatin
↓ Hydroxy-atorvastatin metabolites
↑ RosuvastatinAvoid co-administration with atorvastatin. Hypoglycemics: Combination with APTIVUS/ritonavir not studied Careful glucose monitoring is warranted. Glimepiride
Glipizide
Glyburide
Pioglitazone
Repaglinide
Tolbutamide↔ Glimepiride (CYP2C9)
↔ Glipizide (CYP2C9)
↔ Glyburide (CYP2C9)
↕ Pioglitazone (CYP2C8 and CYP3A4)
↕ Repaglinide (CYP2C8 and CYP3A4)
↔ Tolbutamide (CYP2C9)The effect of TPV/ritonavir on CYP2C8 substrate is not known. Immunosuppressants: Combination with APTIVUS/ritonavir not studied. Cannot predict effect of TPV/ritonavir on immunosuppressants due to conflicting effect of TPV/ritonavir on CYP3A and P-gp. Increased frequency of monitoring of plasma levels of immunosuppressant drugs is recommended. Cyclosporine
Sirolimus
Tacrolimus↕ Cyclosporine
↕ Sirolimus
↕ TacrolimusInhaled beta agonist: Concurrent administration of APTIVUS/ritonavir is not recommended. The combination may result in increased risk of cardiovascular adverse events associated with salmeterol, including QT prolongation, palpitations, and sinus tachycardia. Salmeterol ↑ Salmeterol Inhaled/Nasal Steroids: Fluticasone ↑ Fluticasone Concomitant use of fluticasone propionate and APTIVUS/ritonavir may increase plasma concentrations of fluticasone propionate, resulting in significantly reduced serum cortisol concentrations. Co-administration of fluticasone propionate and APTIVUS/ritonavir is not recommended unless the potential benefit to the patient outweighs the risk of systemic corticosteroid side effects. Narcotic Analgesics: Combinations with APTIVUS/ritonavir not studied Dosage increase and long-term use of meperidine are not recommended due to increased concentrations of the metabolite normeperidine which has both analgesic activity and CNS stimulant activity (e.g., seizures). Meperidine ↓ Meperidine, ↑ Normeperidine Methadone ↓ Methadone Dosage of methadone may need to be increased when co-administered with APTIVUS and 200 mg of ritonavir. ↓ S-Methadone, ↓ R-Methadone Oral Contraceptives/Estrogens: Ethinyl estradiol ↓ Ethinyl estradiol concentrations by 50% Alternative methods of nonhormonal contraception should be used when estrogen based oral contraceptives are co-administered with APTIVUS and 200 mg of ritonavir. Patients using estrogens as hormone replacement therapy should be clinically monitored for signs of estrogen deficiency. Women using estrogens may have an increased risk of non-serious rash. Proton Pump Inhibitors: Omeprazole ↓ Omeprazole, ↔ Tipranavir Dosage of omeprazole may need to be increased when co-administered with APTIVUS and ritonavir. PDE-5 Inhibitors: Only the combination of tadalafil with APTIVUS/ritonavir has been studied (at doses used for treatment of erectile dysfunction). Co-administration with APTIVUS/ritonavir may result in an increase in PDE-5 inhibitor-associated adverse events, including hypotension, syncope, visual disturbances, and priapism. Sildenafil
Tadalafil
Vardenafil
↑ Sildenafil (not studied)
↑ Tadalafil with first dose APTIVUS/ritonavir
↔ Tadalafil at APTIVUS/ritonavir steady-state
↑ Vardenafil (not studied)Use of PDE-5 inhibitors for pulmonary arterial hypertension (PAH): - Use of sildenafil (Revatio) is contraindicated when used for the treatment of pulmonary arterial hypertension (PAH) [see Contraindications (4)].
- The following dose adjustments are recommended for use of tadalafil (Adcirca) with APTIVUS/ritonavir:
Co-administration of tadalafil (Adcirca) in patients on APTIVUS/ritonavir: In patients receiving APTIVUS/ritonavir for at least one week, start Adcirca at 20 mg once daily. Increase to 40 mg once daily based upon individual tolerability. Co-administration of APTIVUS/ritonavir in patients on tadalafil (Adcirca): Avoid use of tadalafil (Adcirca) during the initiation of APTIVUS/ritonavir. Stop Adcirca at least 24 hours prior to starting APTIVUS/ritonavir. After at least one week following the initiation of APTIVUS/ritonavir, resume Adcirca at 20 mg once daily. Increase to 40 mg once daily based upon individual tolerability. Use of PDE-5 inhibitors for erectile dysfunction: Concomitant use of PDE-5 inhibitors with APTIVUS/ritonavir should be used with caution and in no case should the starting dose of: - sildenafil exceed 25 mg within 48 hours
- tadalafil exceed 10 mg every 72 hours
- vardenafil exceed 2.5 mg every 72 hours
Use with increased monitoring for adverse events. Oral Anticoagulants: Warfarin ↔ S-Warfarin Frequent INR (international normalized ratio) monitoring upon initiation of APTIVUS/ritonavir therapy. -
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to APTIVUS during pregnancy. Healthcare providers are encouraged to register patients by calling the Antiretroviral Pregnancy Registry (APR) at 1-800-258-4263.
Risk Summary
Prospective pregnancy data from the APR and an Expanded Access program are not sufficient to adequately assess the risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. Tipranavir use during pregnancy has been evaluated in a limited number of women as reported by the APR and an Expanded Access program, and available data show no birth defects in 13 first trimester exposures (see Data) compared with the background rate for major birth defects of 2.7% in the US reference population of the Metropolitan Atlanta Congenital Defects Program (MACDP). The rate of miscarriage is not reported in the APR. The estimated background rate of miscarriage in clinically recognized pregnancies in the U.S. general population is 15-20%. The background risk of birth defects and miscarriage for the indicated population is unknown. Methodological limitations of the APR include the use of MACDP as the external comparator group. The MACDP population is not disease-specific, evaluates women and infants from a limited geographic area, and does not include outcomes for births that occurred at <20 weeks gestation.
In animal reproduction studies, fetal toxicities were observed with tipranavir at maternally toxic doses with systemic exposures (AUC) less than those in humans at the recommended human dose (RHD) (see Data).
Data
Human Data
Based on prospective reports to the APR and an Expanded Access program for approximately 17 live births following exposure to tipranavir-containing regimens (including 13 live births exposed in the first trimester and 4 live births exposed in the second/third trimester), there were no birth defects reported in live-born infants.
Tipranavir has been shown to cross the placenta.
Animal Data
Tipranavir was administered orally to pregnant rats (at 0, 40, 400, or 1000 mg/kg/day from gestation day 6 to 17) and rabbits (at 0, 75, 150, or 375 mg/kg/day from gestation day 6 to 20). In rats, fetal toxicities including decreased body weight and sternebrae ossification occurred at maternally toxic doses (≥400 mg/kg/day) (approximately 0.8 times human exposure at the RHD). In rabbits, fetal toxicities including decreased fetal body weights, wavy ribs, and bent femurs occurred at a maternally toxic dose (375 mg/kg/day) (approximately 0.05 times human exposure at the RHD). Maternal toxicity included an increased incidence of abortions at doses ≥150 mg/kg/day (approximately 0.05 times human exposure at the RHD).
In the pre/post-natal development study, tipranavir was administered orally to rats at 0, 40, 400, 1000 mg/kg/day from gestation day 6 to lactation day 21. The only significant effect observed was growth inhibition of the offspring at maternally toxic doses (≥400 mg/kg/day) (approximately 0.8 times human exposure at the RHD).
8.2 Lactation
Risk Summary
There is no information regarding the presence of tipranavir in human milk, the effects on the breastfed infant, or the effects on milk production. Tipranavir is present in rat milk (see Data). Potential risks of breastfeeding include: (1) HIV-1 transmission (in HIV-1 negative infants), (2) developing viral resistance (in HIV-1-positive patients), and (3) adverse reactions in a breastfed infant similar to those seen in adults.
Data
In a lactation study, tipranavir was excreted into the milk of lactating rats following a single oral dose of tipranavir (10 mg/kg) on lactation/postpartum day 14, with a maximal milk concentration achieved 2 hours post-administration (milk concentration 0.13 times that of maternal plasma concentration).
8.3 Females and Males of Reproductive Potential
Contraception
Use of APTIVUS may reduce the efficacy of estrogen-based oral contraceptives. Advise patients to use alternative methods of nonhormonal contraception [see Drug Interactions (7.2)].
8.4 Pediatric Use
The safety and effectiveness of APTIVUS, co-administered with ritonavir have been established in pediatric patients for combination antiretroviral treatment of HIV-1 infected pediatric patients weighing 36 kg or higher who are treatment-experienced and infected with HIV-1 strains resistant to more than one protease inhibitor (PI) [see Indications and Usage (1) and Dosage and Administration (2.2)].
The safety, pharmacokinetic profile, and virologic and immunologic responses of APTIVUS in those weighing 36 kg or higher were similar to those observed in adults. However, rash was reported more frequently in pediatric subjects than in adults [see Warnings and Precautions (5.6), Adverse Reactions (6.2), Clinical Pharmacology (12.3), and Clinical Studies (14.2)].
The safety and effectiveness of APTIVUS, co-administered with ritonavir have been established in pediatric patients greater than 2 years of age or weighing less than 36 kg, but not recommended due to lack of a suitable pediatric formulation.
8.5 Geriatric Use
Clinical studies of APTIVUS/ritonavir did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently than younger subjects. In general, caution should be exercised in the administration and monitoring of APTIVUS in elderly patients reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
8.6 Hepatic Impairment
Tipranavir is principally metabolized by the liver. Caution should be exercised when administering APTIVUS/ritonavir to patients with mild (Child-Pugh Class A) hepatic impairment because tipranavir concentrations may be increased [see Clinical Pharmacology (12.3)]. APTIVUS/ritonavir is contraindicated in patients with moderate or severe (Child-Pugh Class B or Child-Pugh Class C) hepatic impairment [see Contraindications (4)].
-
10 OVERDOSAGE
There is no known antidote for APTIVUS overdose. Treatment of overdose should consist of general supportive measures, including monitoring of vital signs and observation of the patient's clinical status. If indicated, elimination of unabsorbed tipranavir should be achieved by emesis or gastric lavage. Administration of activated charcoal may also be used to aid in removal of unabsorbed drug. Since tipranavir is highly protein bound, dialysis is unlikely to provide significant removal of the drug.
-
11 DESCRIPTION
APTIVUS is a protease inhibitor of HIV-1 belonging to the class of 4-hydroxy-5,6-dihydro-2-pyrone sulfonamides.
The chemical name of tipranavir is 2-Pyridinesulfonamide, N-[3-[(1R)-1-[(6R)-5,6-dihydro-4-hydroxy-2-oxo-6-(2-phenylethyl)-6-propyl-2H-pyran-3-yl]propyl]phenyl]-5-(trifluoromethyl). It has a molecular formula of C31H33F3N2O5S and a molecular weight of 602.7. Tipranavir has the following structural formula and is a single stereoisomer with the 1R, 6R configuration.
Tipranavir is a white to off-white to slightly yellow solid. It is freely soluble in dehydrated alcohol and propylene glycol, and insoluble in aqueous buffer at pH 7.5.
APTIVUS soft gelatin capsules are for oral administration. Each capsule contains 250 mg tipranavir. The major inactive ingredients in the capsule are dehydrated alcohol (7% w/w or 0.1 g per capsule), polyoxyl 35 castor oil, propylene glycol, mono/diglycerides of caprylic/capric acid and gelatin.
-
12 CLINICAL PHARMACOLOGY
12.2 Pharmacodynamics
ECG Evaluation
The effect of APTIVUS/ritonavir on the QTcF interval was measured in a study in which 81 healthy subjects received the following treatments twice daily for 2.5 days: APTIVUS/ritonavir (500 mg/200 mg), APTIVUS/ritonavir at a supra-therapeutic dose (750 mg/200 mg), and placebo/ritonavir (-/200 mg). After baseline and placebo adjustment, the maximum mean QTcF change was 3.2 ms (1-sided 95% Upper CI: 5.6 ms) for the 500 mg/200 mg dose and 8.3 ms (1-sided 95% Upper CI: 10.9 ms) for the supra-therapeutic 750 mg/200 mg dose.
Antiviral Activity in vivo
The median Inhibitory Quotient (IQ) determined from 264 treatment-experienced adult subjects was about 80 (inter-quartile range: 31-226), from the controlled clinical trials 1182.12 and 1182.48. The IQ is defined as the tipranavir trough concentration divided by the viral EC50 value, corrected for protein binding. There was a relationship between the proportion of subjects with a ≥1 log10 reduction of viral load from baseline at week 48 and their IQ value. Among the 198 subjects receiving APTIVUS/ritonavir with no new enfuvirtide use (e.g., new enfuvirtide, defined as initiation of enfuvirtide for the first time), the response rate was 23% in those with an IQ value <80 and 59% in those with an IQ value ≥80. Among the 66 subjects receiving APTIVUS/ritonavir with new enfuvirtide, the response rates in subjects with an IQ value <80 versus those with an IQ value ≥80 were 55% and 71%, respectively. These IQ groups are derived from a select population and are not meant to represent clinical breakpoints.
12.3 Pharmacokinetics
In order to achieve effective tipranavir plasma concentrations and a twice-daily dosing regimen, co-administration of APTIVUS with ritonavir is essential [see Dosage and Administration (2)]. Ritonavir inhibits hepatic cytochrome P450 3A (CYP3A), the intestinal P-gp efflux pump and possibly intestinal CYP3A. In a dose-ranging evaluation in 113 HIV-1 negative male and female volunteers, there was a 29-fold increase in the geometric mean morning steady-state trough plasma concentrations of tipranavir following APTIVUS co-administered with low-dose ritonavir (500 mg/200 mg twice daily) compared to APTIVUS 500 mg twice daily without ritonavir. In adults the mean systemic ritonavir concentration when 200 mg of ritonavir was given with 500 mg of APTIVUS was similar to the concentrations observed when 100 mg was given with the other protease inhibitors.
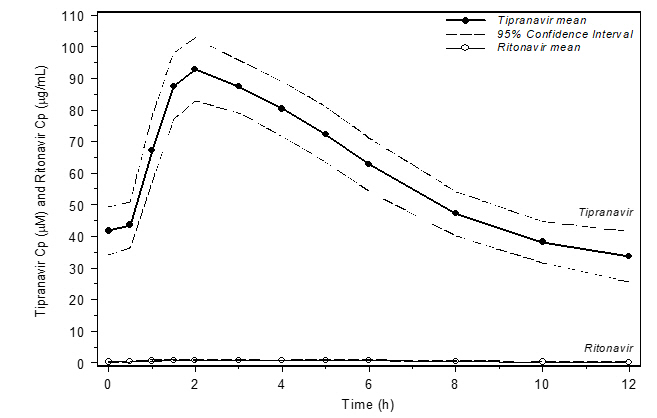
Figure 1 displays mean plasma concentrations of tipranavir and ritonavir at steady state for 30 HIV-1 infected adult subjects dosed with 500 mg/200 mg tipranavir/ritonavir for 14 days.
Figure 1 Mean Steady State Tipranavir Plasma Concentrations (95% CI) with Ritonavir Co-administration (tipranavir/ritonavir 500 mg/200 mg BID)
Absorption and Bioavailability
Absorption of tipranavir in humans is limited, although no absolute quantification of absorption is available. Tipranavir is a P-gp substrate, a weak P-gp inhibitor, and appears to be a potent P-gp inducer as well. In vivo data suggest that tipranavir/ritonavir, at the dose of 500 mg/200 mg, is a P-gp inhibitor after the first dose and induction of P-gp occurs over time. Tipranavir trough concentrations at steady-state are about 70% lower than those on Day 1, presumably due to intestinal P-gp induction. Steady state is attained in most subjects after 7-10 days of dosing.
Dosing APTIVUS 500 mg with 200 mg ritonavir capsules twice daily for greater than 2 weeks and without meal restriction produced the pharmacokinetic parameters for male and female HIV-1 positive subjects presented in Table 5.
Table 5 Pharmacokinetic Parametersa of tipranavir/ritonavir 500 mg/200 mg for HIV-1 Positive Subjects by Gender Parameter Females
(n=14)Males
(n=106)aPopulation pharmacokinetic parameters reported as mean ± standard deviation Cptrough (µM) 41.6 ± 24.3 35.6 ± 16.7 Cmax (µM) 94.8 ± 22.8 77.6 ± 16.6 Tmax (h) 2.9 3.0 AUC0-12h (µM∙h) 851 ± 309 710 ± 207 CL (L/h) 1.15 1.27 V (L) 7.7 10.2 t1/2 (h) 5.5 6.0 Effects of Food on Oral Absorption
For APTIVUS capsules co-administered with ritonavir capsules at steady-state, no clinically significant changes in tipranavir Cmax, Cp12h, and AUC were observed under fed conditions (500-682 Kcal, 23-25% calories from fat) compared to fasted conditions [see Dosage and Administration (2)]. The effect of food on tipranavir exposure when APTIVUS capsules is co-administered with ritonavir tablets has not been evaluated [see Dosage and Administration (2)]. For information on the effect of food on the bioavailability of ritonavir tablets, please refer to the ritonavir tablet prescribing information.
Distribution
Tipranavir is extensively bound to plasma proteins (>99.9%). It binds to both human serum albumin and α-1-acid glycoprotein. The mean fraction of tipranavir (dosed without ritonavir) unbound in plasma was similar in clinical samples from healthy volunteers and HIV-1 positive subjects. Total plasma tipranavir concentrations for these samples ranged from 9 to 82 µM. The unbound fraction of tipranavir appeared to be independent of total drug concentration over this concentration range.
No studies have been conducted to determine the distribution of tipranavir into human cerebrospinal fluid or semen.
Metabolism
In vitro metabolism studies with human liver microsomes indicated that CYP3A4 is the predominant CYP enzyme involved in tipranavir metabolism.
The oral clearance of tipranavir decreased after the addition of ritonavir, which may represent diminished first-pass clearance of the drug at the gastrointestinal tract as well as the liver.
The metabolism of tipranavir in the presence of 200 mg ritonavir is minimal. Administration of 14C-tipranavir to subjects that received APTIVUS/ritonavir 500 mg/200 mg dosed to steady-state demonstrated that unchanged tipranavir accounted for 98.4% or greater of the total plasma radioactivity circulating at 3, 8, or 12 hours after dosing. Only a few metabolites were found in plasma, and all were at trace levels (0.2% or less of the plasma radioactivity). In feces, unchanged tipranavir represented the majority of fecal radioactivity (79.9% of fecal radioactivity). The most abundant fecal metabolite, at 4.9% of fecal radioactivity (3.2% of dose), was a hydroxyl metabolite of tipranavir. In urine, unchanged tipranavir was found in trace amounts (0.5% of urine radioactivity). The most abundant urinary metabolite, at 11.0% of urine radioactivity (0.5% of dose) was a glucuronide conjugate of tipranavir.
Elimination
Administration of 14C-tipranavir to subjects (n=8) that received APTIVUS/ritonavir 500 mg/200 mg dosed to steady-state demonstrated that most radioactivity (median 82.3%) was excreted in feces, while only a median of 4.4% of the radioactive dose administered was recovered in urine. In addition, most radioactivity (56%) was excreted between 24 and 96 hours after dosing. The effective mean elimination half-life of tipranavir/ritonavir in healthy volunteers (n=67) and HIV-1 infected adult subjects (n=120) was approximately 4.8 and 6.0 hours, respectively, at steady state following a dose of 500 mg/200 mg twice daily with a light meal.
Special Populations
Renal Impairment
APTIVUS pharmacokinetics has not been studied in patients with renal dysfunction. However, since the renal clearance of tipranavir is negligible, a decrease in total body clearance is not expected in patients with renal insufficiency.
Hepatic Impairment
In a study comparing 9 HIV-1 negative subjects with mild (Child-Pugh Class A) hepatic impairment to 9 HIV-1 negative controls, the single and multiple dose plasma concentrations of tipranavir and ritonavir were increased in subjects with hepatic impairment, but were within the range observed in clinical trials. No dosing adjustment is required in patients with mild hepatic impairment.
The influence of moderate hepatic impairment (Child-Pugh Class B) or severe hepatic impairment (Child-Pugh Class C) on the multiple-dose pharmacokinetics of tipranavir administered with ritonavir has not been evaluated [see Dosage and Administration (2), Contraindications (4), and Warnings and Precautions (5.2)].
Gender
Evaluation of steady-state plasma tipranavir trough concentrations at 10-14 h after dosing from the controlled clinical trials 1182.12 and 1182.48 demonstrated that females generally had higher tipranavir concentrations than males. After 4 weeks of APTIVUS/ritonavir 500 mg/200 mg BID, the median plasma trough concentration of tipranavir was 43.9 µM for females and 31.1 µM for males. The difference in concentrations does not warrant a dose adjustment.
Race
Evaluation of steady-state plasma tipranavir trough concentrations at 10-14 h after dosing from the controlled clinical trials 1182.12 and 1182.48 demonstrated that white males generally had more variability in tipranavir concentrations than black males, but the median concentration and the range making up the majority of the data are comparable between the races.
Geriatric Patients
Evaluation of steady-state plasma tipranavir trough concentrations at 10-14 h after dosing from the controlled clinical trials 1182.12 and 1182.48 demonstrated that there was no change in median trough tipranavir concentrations as age increased for either gender through 65 years of age. There were an insufficient number of women greater than age 65 years in the two trials to evaluate the elderly.
Pediatric Patients
Among pediatric subjects in clinical trial 1182.14, steady-state plasma tipranavir trough concentrations were obtained 10 to 14 hours following study drug administration. The exposure differences between pediatric subjects and adults are not considered to be clinically significant based on the activity and safety data.
Drug Interactions
Drug interaction studies were performed with APTIVUS capsules co-administered with ritonavir, and other drugs likely to be co-administered and some drugs commonly used as probes for pharmacokinetic interactions. The effects of co-administration of APTIVUS with 200 mg ritonavir on the AUC, Cmax, and Cmin of tipranavir or the co-administered drug, are summarized in Tables 6 and 7, respectively. For information regarding clinical recommendations see Drug Interactions (7.2).
Table 6 Drug Interactions: Pharmacokinetic Parameters for Tipranavir in the Presence of Co-administered Drugs Co-administered Drug Co-administered Drug Dose (Schedule) tipranavir/ ritonavir Drug Dose (Schedule) n PK Ratio (90% Confidence Interval) of Tipranavir Pharmacokinetic Parameters with/without Co-administered Drug;
No Effect = 1.00Cmax AUC Cmin *steady state comparison to historical data (n) ↑ increase, ↓ decrease, ↔ no change, ↕ unable to predict Antacids (Maalox®) 20 mL
(1 dose)500 mg/200 mg
(1 dose)23 ↓ 0.75 (0.63, 0.88) 0.73 (0.64, 0.84) - Atazanavir/ritonavir 300 mg/100 mg QD
(9 doses)500 mg/100 mg BID
(34 doses)13 ↑ 1.08 (0.98, 1.20) 1.20 (1.09, 1.32) 1.75 (1.39, 2.20) Atorvastatin 10 mg
(1 dose)500 mg/200 mg BID
(14 doses)22 ↔ 0.96 (0.86, 1.07) 1.08 (1.00, 1.15) 1.04 (0.89, 1.22) Clarithromycin 500 mg BID
(25 doses)500 mg/200 mg BID* 24 (68) ↑ 1.40 (1.24, 1.47) 1.66 (1.43, 1.73) 2.00 (1.58, 2.47) Didanosine 400 mg
(1 dose)500 mg/100 mg BID
(27 doses)5 ↓ 1.32 (1.09, 1.60) 1.08 (0.82, 1.42) 0.66 (0.31, 1.43) Efavirenz 600 mg QD
(8 doses)500 mg/100 mg BID* 21 (89) ↓ 0.79 (0.69, 0.89) 0.69 (0.57, 0.83) 0.58 (0.36, 0.86) 750 mg/200 mg BID* 25 (100) ↔ 0.97 (0.85, 1.09) 1.01 (0.85, 1.18) 0.97 (0.69, 1.28) Ethinyl estradiol /Norethindrone 0.035 mg/1.0 mg
(1 dose)500 mg/100 mg BID
(21 doses)21 ↓ 1.10 (0.98, 1.24) 0.98 (0.88, 1.11) 0.73 (0.59, 0.90) 750 mg/200 mg BID
(21 doses)13 ↔ 1.01 (0.96, 1.06) 0.98 (0.90, 1.07) 0.91 (0.69, 1.20) Fluconazole 100 mg QD
(12 doses)500 mg/200 mg BID* 20 (68) ↑ 1.32 (1.18, 1.47) 1.50 (1.29, 1.73) 1.69 (1.33, 2.09) Loperamide 16 mg
(1 dose)750 mg/200 mg BID
(21 doses)24 ↓ 1.03 (0.92, 1.17) 0.98 (0.86, 1.12) 0.74 (0.62, 0.88) Rifabutin 150 mg
(1 dose)500 mg/200 mg BID
(15 doses)21 ↔ 0.99 (0.93, 1.07) 1.00 (0.96, 1.04) 1.16 (1.07, 1.27) Rosuvastatin 10 mg
(1 dose)500 mg/200 mg BID
(24 doses)16 ↔ 1.08 (1.00, 1.17) 1.06 (0.97, 1.15) 0.99 (0.88, 1.11) Tadalafil 10 mg
(1 dose)500 mg/200 mg BID
(17 doses)17 ↔ 0.90 (0.80, 1.01) 0.85 (0.74, 0.97) 0.81 (0.70, 0.94) Tenofovir 300 mg
(1 dose)500 mg/100 mg BID 22 ↓ 0.83 (0.74, 0.94) 0.82 (0.75, 0.91) 0.79 (0.70, 0.90) 750 mg/200 mg BID
(23 doses)20 ↔ 0.89 (0.84, 0.96) 0.91 (0.85, 0.97) 0.88 (0.78, 1.00) Valacyclovir 500 mg
(1 dose)500 mg/200 mg BID
(23 doses)26 ↔ 1.02 (0.95, 1.10) 1.01 (0.96, 1.06) 0.98 (0.93, 1.04) Zidovudine 300 mg
(1 dose)500 mg/100 mg BID 29 ↓ 0.87 (0.80, 0.94) 0.82 (0.76, 0.89) 0.77 (0.68, 0.87) 750 mg/200 mg BID
(23 doses)25 ↔ 1.02 (0.94, 1.10) 1.02 (0.92, 1.13) 1.07 (0.86, 1.34) Table 7 Drug Interactions: Pharmacokinetic Parameters for Co-administered Drug in the Presence of APTIVUS/ritonavir Co-administered Drug Co-administered Drug Dose (Schedule) tipranavir/ ritonavir Drug Dose (Schedule) n PK Ratio (90% Confidence Interval) of Co-administered Drug Pharmacokinetic Parameters with/without tipranavir/ritonavir;
No Effect = 1.00Cmax AUC Cmin a HIV-1 positive subjects b Buprenorphine/Naloxone maintenance subjects c HIV-1 positive subjects (tipranavir/ritonavir 250 mg/200 mg, 750 mg/200 mg and 1250 mg/100 mg) and healthy volunteers (tipranavir/ritonavir 500 mg/100 mg and 750 mg/200 mg) d Normalized sum of parent drug (rifabutin) and active metabolite (25-O-desacetyl-rifabutin) e Intensive PK analysis f Drug levels obtained at 8-16 hrs post-dose g n = 14 for Cmin hAdministered as Valacyclovir ↑ increase, ↓ decrease, ↔ no change, ↕ unable to predict Abacavira 300 mg BID
(43 doses)250 mg/200 mg BID
750 mg/100 mg BID
1250 mg/100 mg BID
(42 doses)28
14
11↓
↓
↓0.56 (0.48, 0.66)
0.54 (0.47, 0.63)
0.48 (0.42, 0.53)0.56 (0.49, 0.63)
0.64 (0.55, 0.74)
0.65 (0.55, 0.76)-
-
-Acyclovirh 500 mg
(1 dose)500 mg/200 mg BID
(23 doses)26 ↔ 0.95 (0.88, 1.02) 1.07 (1.04, 1.09) - Amprenavir/ritonavira 600 mg/100 mg BID
(27 doses)500 mg/200 mg BID
(28 doses)16
74↓
↓0.61 (0.51, 0.73)e 0.56 (0.49, 0.64)e
-0.45 (0.38, 0.53)e
0.44 (0.39, 0.49)fAtazanavir/ritonavir 300 mg/100 mg QD
(9 doses)500 mg/100 mg BID
(34 doses)13 ↓ 0.43 (0.38, 0.50) 0.32 (0.29, 0.36) 0.19 (0.15, 0.24) Atorvastatin 10 mg
(1 dose)500 mg/200 mg BID
(17 doses)22 ↑ 8.61 (7.25, 10.21) 9.36 (8.02, 10.94) 5.19 (4.21, 6.40) Orthohydroxy-atorvastatin
Parahydroxy-atorvastatin21, 12, 17 ↓ 0.02 (0.02, 0.03) 0.11 (0.08, 0.17) 0.07 (0.06, 0.08) 13, 22, 1 ↓ 1.04 (0.87, 1.25) 0.18 (0.14, 0.24) 0.33 (NA) Buprenorphine/Naloxoneb 16 mg/4 mg
24 mg/6 mg
(daily)500 mg/200 mg BID
(16 doses)Buprenorphine 10 ↔ 0.86 (0.68, 1.10) 0.99 (0.80, 1.23) 0.94 (0.74, 1.19) Carbamazepine 100 mg BID
(29 doses)500 mg/200 mg
(1 dose)7 ↔ 1.04 (1.00, 1.07) 1.05 (1.02, 1.09) 1.17 (1.11, 1.24) (43 doses) (15 doses) 7 ↔ 1.10 (0.85, 1.42) 1.08 (0.91, 1.27) 1.07 (0.90, 1.27) 200 mg BID
(29 doses)500 mg/200 mg
(1 dose)17 ↔ 1.00 (0.96, 1.04) 1.04 (1.00, 1.08) 1.16 (1.11, 1.22) (43 doses) (15 doses) 17 ↑ 1.22 (1.11, 1.34) 1.26 (1.15, 1.38) 1.35 (1.22, 1.50) Clarithromycin 500 mg BID
(25 doses)500 mg/200 mg BID
(15 doses)21 ↑ 0.95 (0.83, 1.09) 1.19 (1.04, 1.37) 1.68 (1.42, 1.98) 14-OH-clarithromycin 21 ↓ 0.03 (0.02, 0.04) 0.03 (0.02, 0.04) 0.05 (0.04, 0.07) Didanosinec 200 mg BID, ≥60 kg
125 mg BID, <60 kg
(43 doses)250 mg/200 mg BID
750 mg/100 mg BID
1250 mg/100 mg BID
(42 doses)10
8
9↓
↔
↔0.57 (0.42, 0.79)
0.76 (0.49, 1.17)
0.77 (0.47, 1.26)0.67 (0.51, 0.88)
0.97 (0.64, 1.47)
0.87 (0.47, 1.65)-
-
-400 mg
(1 dose)500 mg/100 mg BID
(27 doses)5 ↔ 0.80 (0.63, 1.02) 0.90 (0.72, 1.11) 1.17 (0.62, 2.20) Dolutegravir 50 mg QD 500 mg/200 mg BID 14 ↓ 0.54 (0.50-0.57) 0.41 (0.38-0.44) 0.24 (0.21-0.27) Efavirenzc 600 mg QD
(15 doses)500 mg/100 mg BID
750 mg/200 mg BID
(15 doses)24
22↔
↔1.09 (0.99, 1.19)
1.12 (0.98, 1.28)1.04 (0.97, 1.12)
1.00 (0.93, 1.09)1.02 (0.92, 1.12)
0.94 (0.84, 1.04)Ethinyl estradiol 0.035 mg
(1 dose)500 mg/100 mg BID
750 mg/200 mg BID
(21 doses)21
13↓
↓0.52 (0.47, 0.57)
0.48 (0.42, 0.57)0.52 (0.48, 0.56)
0.57 (0.54, 0.60)-
-Fluconazole 200 mg (Day 1) then 100 mg QD
(6 or 12 doses)500 mg/200 mg BID
(2 or 14 doses)19
19↔
↔0.97 (0.94, 1.01)
0.94 (0.91, 0.98)0.99 (0.97, 1.02)
0.92 (0.88, 0.95)0.98 (0.94, 1.02)
0.89 (0.85, 0.92)Lopinavir/ritonavira 400 mg/100 mg BID
(27 doses)500 mg/200 mg BID
(28 doses)21
69↓
↓0.53 (0.40, 0.69)e
-0.45 (0.32, 0.63)e - 0.30 (0.17, 0.51)e
0.48 (0.40, 0.58)fLoperamide 16 mg
(1 dose)750 mg/200 mg BID
(21 doses)24 ↓ 0.39 (0.31, 0.48) 0.49 (0.40, 0.61) - N-Demethyl-Loperamide 24 ↓ 0.21 (0.17, 0.25) 0.23 (0.19, 0.27) - Lamivudinea 150 mg BID
(43 doses)250 mg/200 mg BID
750 mg/100 mg BID
1250 mg/100 mg BID
(42 doses)64
46
35↔
↔
↔0.96 (0.89, 1.03)
0.86 (0.78, 0.94)
0.71 (0.62, 0.81)0.95 (0.89, 1.02)
0.96 (0.90, 1.03)
0.82 (0.66, 1.00)-
-
-Methadone 5 mg
(1 dose)500 mg/200 mg BID
(16 doses)14 ↓ 0.45 (0.41, 0.49) 0.47 (0.44, 0.51) 0.50 (0.46, 0.54) R-methadone 0.54 (0.50, 0.58) 0.52 (0.49, 0.56) - S-methadone 0.38 (0.35, 0.43) 0.37 (0.34, 0.41) - Nevirapinea 200 mg BID
(43 doses)250 mg/200 mg BID
750 mg/100 mg BID
1250 mg/100 mg BID
(42 doses)26
22
17↔
↔
↔0.97 (0.90, 1.04)
0.86 (0.76, 0.97)
0.71 (0.62, 0.82)0.97 (0.91, 1.04)
0.89 (0.78, 1.01)
0.76 (0.63, 0.91)0.96 (0.87, 1.05)
0.93 (0.80, 1.08)
0.77 (0.64, 0.92)Norethindrone 1.0 mg
(1 dose)500 mg/100 mg BID
750 mg/200 mg BID
(21 doses)21
13↔
↔1.03 (0.94, 1.13)
1.08 (0.97, 1.20)1.14 (1.06, 1.22)
1.27 (1.13, 1.43)-
-Raltegravir 400 mg BID 500 mg/200 mg BID 15 ↓ 0.82 (0.46, 1.46) 0.76 (0.49, 1.19) 0.45 (0.31, 0.66)g Rifabutin 150 mg
(1 dose)500 mg/200 mg BID
(15 doses)20 ↑ 1.70 (1.49, 1.94) 2.90 (2.59, 3.26) 2.14 (1.90, 2.41) 25-O-desacetyl-rifabutin 20 ↑ 3.20 (2.78, 3.68) 20.71 (17.66, 24.28) 7.83 (6.70, 9.14) Rifabutin + 25-O-desacetyl-rifabutind 20 ↑ 1.86 (1.63, 2.12) 4.33 (3.86, 4.86) 2.76 (2.44, 3.12) Rosuvastatin 10 mg
(1 dose)500 mg/200 mg BID
(24 doses)16 ↑ 2.23 (1.83, 2.72) 1.26 (1.08, 1.46) 1.06 (0.93, 1.20) Saquinavir/ritonavira 600 mg/100 mg BID
(27 doses)500 mg/200 mg BID
(28 doses)20
68↓
↓0.30 (0.23, 0.40)e
-0.24 (0.19, 0.32)e - 0.18 (0.13, 0.26)e
0.20 (0.16, 0.25)fStavudinea 40 mg BID ≥60 kg
30 mg BID <60 kg
(43 doses)250 mg/200 mg BID
750 mg/100 mg BID
1250 mg/100 mg BID
(42 doses)26
22
19↔
↔
↔0.90 (0.81, 1.02)
0.76 (0.66, 0.89)
0.74 (0.69, 0.80)1.00 (0.91, 1.11)
0.84 (0.74, 0.96)
0.93 (0.83, 1.05)-
-
-Tadalafil 10 mg
(1 dose)500 mg/200 mg
(1 dose)17 ↑ 0.78 (0.72, 0.84) 2.33 (2.02, 2.69) - 10 mg
(1 dose)500 mg/200 mg BID
(17 doses)17 ↔ 0.70 (0.63, 0.78) 1.01 (0.83, 1.21) - Tenofovir 300 mg
(1 dose)500 mg/100 mg BID
750 mg/200 mg BID
(23 doses)22
20↓
↓0.77 (0.68, 0.87)
0.62 (0.54, 0.71)0.98 (0.91, 1.05)
1.02 (0.94, 1.10)1.07 (0.98, 1.17)
1.14 (1.01, 1.27)Zidovudinec 300 mg BID 250 mg/200 mg BID 48 ↓ 0.54 (0.47, 0.62) 0.58 (0.51, 0.66) - 300 mg BID 750 mg/100 mg BID 31 ↓ 0.51 (0.44, 0.60) 0.64 (0.55, 0.75) - 300 mg BID (43 doses) 1250 mg/100 mg BID (42 doses) 23 ↓ 0.49 (0.40, 0.59) 0.69 (0.49, 0.97) - 300 mg
(1 dose)500 mg/100 mg BID
750 mg/200 mg BID
(23 doses)29
25↓
↔0.39 (0.33, 0.45)
0.44 (0.36, 0.54)0.57 (0.52, 0.63)
0.67 (0.62, 0.73)0.89 (0.81, 0.99)
1.25 (1.08, 1.44)Zidovudine glucuronide 500 mg/100 mg BID
750 mg/200 mg BID
(23 doses)29
25↑
↑0.82 (0.74, 0.90)
0.82 (0.73, 0.92)1.02 (0.97, 1.06)
1.09 (1.05, 1.14)1.52 (1.34, 1.71)
1.94 (1.62, 2.31)12.4 Microbiology
Mechanism of Action
Tipranavir (TPV) is an HIV-1 protease inhibitor that inhibits the virus-specific processing of the viral Gag and Gag-Pol polyproteins in HIV-1 infected cells, thus preventing formation of mature virions.
Antiviral Activity
Tipranavir inhibits the replication of laboratory strains of HIV-1 and clinical isolates in acute models of T-cell infection, with 50% effective concentrations (EC50) ranging from 0.03 to 0.07 µM (18-42 ng/mL). Tipranavir demonstrates antiviral activity in cell culture against a broad panel of HIV-1 group M non-clade B isolates (A, C, D, F, G, H, CRF01 AE, CRF02 AG, CRF12 BF). Group O and HIV-2 isolates have reduced susceptibility in cell culture to tipranavir with EC50 values ranging from 0.164 -1 µM and 0.233-0.522 µM, respectively. The cell culture antiviral activity of tipranavir in combination with the HIV-1 protease inhibitors amprenavir, atazanavir, lopinavir and saquinavir, and with the HIV-1 NRTI lamivudine was additive to antagonistic. No antagonism was seen when combined with the HIV-1 protease inhibitors indinavir, nelfinavir, or ritonavir, with the NNRTIs delavirdine, efavirenz, and nevirapine, with the NRTIs abacavir, didanosine, emtricitabine, stavudine, tenofovir, and zidovudine, or with the gp41 fusion inhibitor enfuvirtide in cell culture. There was no antagonism of the cell culture combinations of tipranavir with either adefovir or ribavirin, used in the treatment of viral hepatitis.
Resistance
In cell culture:
HIV-1 isolates with a decreased susceptibility to tipranavir have been selected in cell culture and obtained from subjects treated with APTIVUS/ritonavir (TPV/ritonavir). After 9 months of culture in TPV-containing medium, HIV-1 isolates with 87-fold reduced susceptibility to tipranavir were selected in cell culture; these contained 10 protease substitutions that developed in the following order: L33F, I84V, K45I, I13V, V32I, V82L, M36I, A71V, L10F, and I54V/T. Changes in the Gag polyprotein CA/P2 cleavage site were also observed following drug selection. Experiments with site-directed mutants of HIV-1 showed that the presence of 6 substitutions in the protease coding sequence (I13V, V32I, L33F, K45I, V82L, I84V) conferred >10-fold reduced susceptibility to tipranavir.
Clinical Trials of Treatment-Experienced Subjects:
In controlled clinical trials 1182.12 and 1182.48, multiple protease inhibitor-resistant HIV-1 isolates from 59 treatment-experienced adult subjects who received APTIVUS/ritonavir and experienced virologic rebound developed amino acid substitutions that were associated with resistance to tipranavir. The most common amino acid substitutions that developed on 500 mg/200 mg APTIVUS/ritonavir in greater than 20% of APTIVUS/ritonavir virologic failure isolates were L33V/I/F, V82T, and I84V. Other substitutions that developed in 10 to 20% of APTIVUS/ritonavir virologic failure isolates included L10V/I/S, I13V, E35D/G/N, I47V, I54A/M/V, K55R, V82L, and L89V/M. Evolution at protease gag polyprotein cleavage sites was also observed. Among 28 pediatric subjects in clinical trial 1182.14 who experienced virologic failure or non-response, the emergent protease amino acid codon substitutions were similar to those observed in adult virologic failure isolates.
In clinical trials 1182.12 and 1182.48 tipranavir resistance was detected at virologic rebound after an average of 38 weeks of APTIVUS/ritonavir treatment with a median 14-fold decrease in tipranavir susceptibility. Similarly, reduced tipranavir susceptibility was associated with emergent substitutions in pediatric subject isolates.
Cross-resistance
Cross-resistance among protease inhibitors has been observed. Tipranavir had <4-fold decreased susceptibility against 90% (94/105) of HIV-1 clinical isolates resistant to amprenavir, atazanavir, indinavir, lopinavir, nelfinavir, ritonavir, or saquinavir. Tipranavir-resistant viruses which emerged in cell culture from wild-type HIV-1 had decreased susceptibility to the protease inhibitors amprenavir, atazanavir, indinavir, lopinavir, nelfinavir and ritonavir but remained sensitive to saquinavir.
Baseline Genotype and Virologic Outcome Analyses
Genotypic and/or phenotypic analysis of baseline virus may aid in determining tipranavir susceptibility before initiation of APTIVUS/ritonavir therapy. Several analyses were conducted to evaluate the impact of specific substitutions and combination of substitutions on virologic outcome. Both the type and number of baseline protease inhibitor substitutions as well as use of additional active agents (e.g., enfuvirtide) affected APTIVUS/ritonavir response rates in controlled clinical trials 1182.12 and 1182.48 through Week 48 of treatment.
Regression analyses of baseline and/or on-treatment HIV-1 genotypes from 860 treatment-experienced subjects in Phase 2 and 3 trials demonstrated that amino acid substitutions at 16 codons in the HIV-1 protease coding sequence were associated with reduced virologic responses and/or reduced tipranavir susceptibility: L10V, I13V, K20M/R/V, L33F, E35G, M36I, K43T, M46L, I47V, I54A/M/V, Q58E, H69K, T74P, V82L/T, N83D or I84V.
As-treated analyses were also conducted to assess virologic outcome by the number of primary protease inhibitor substitutions present at baseline. Response rates were reduced if five or more protease inhibitor-associated substitutions were present at baseline and subjects did not receive concomitant new enfuvirtide with APTIVUS/ritonavir. See Table 8.
Table 8 Controlled Clinical Trials 1182.12 and 1182.48: Proportion of Responders (confirmed ≥1 log10 decrease at Week 48) by Number of Baseline Primary Protease Inhibitor (PI) Resistance-Associated Substitutions Number of Baseline Primary PI Substitutionsa APTIVUS/ritonavir
N=578Comparator PI/ritonavir
N=610No New Enfuvirtideb + New Enfuvirtidec No New Enfuvirtideb + New Enfuvirtidec aPrimary PI substitutions include any amino acid substitution at positions 30, 32, 36, 46, 47, 48, 50, 53, 54, 82, 84, 88 and 90 bNo new enfuvirtide is defined as recycled or continued use of enfuvirtide or no use of enfuvirtide cNew enfuvirtide is defined as initiation of enfuvirtide for the first time Overall 38%
(180/470)69%
(75/108)18%
(92/524)26%
(22/86)1 – 2 62%
(24/39)60%
(3/5)33%
(14/43)0%
(0/1)3 – 4 48%
(96/202)71%
(27/38)23%
(45/193)38%
(13/34)5+ 26%
(60/229)69%
(45/65)11%
(33/288)18%
(9/51)The median change from baseline in plasma HIV-1 RNA at weeks 2, 4, 8, 16, 24 and 48 was evaluated by the number of baseline primary protease inhibitor resistance- associated substitutions (1-4 or ≥5) in subjects who received APTIVUS/ritonavir with or without new enfuvirtide. The following observations were made:
- Approximately 1.5 log10 decrease in HIV-1 RNA at early time points (Week 2) regardless of the number of baseline primary protease inhibitor resistance- associated substitutions (1-4 or 5+).
- Subjects with 5 or more primary protease inhibitor resistance-associated substitutions in their HIV-1 at baseline who received APTIVUS/ritonavir without new enfuvirtide (n=303) began to lose their antiviral response after Week 4.
- Early HIV-1 RNA decreases (1.5-2 log10) were sustained through Week 48 in subjects with 5 or more primary protease inhibitor resistance-associated substitutions at baseline who received new enfuvirtide with APTIVUS/ritonavir (n=74).
Baseline Phenotype and Virologic Outcome Analyses
APTIVUS/ritonavir response rates were also assessed by baseline tipranavir phenotype. Relationships between baseline phenotypic susceptibility to tipranavir, substitutions at protease amino acid codons 33, 82, 84 and 90, tipranavir resistance-associated substitutions, and response to APTIVUS/ritonavir therapy at Week-48 are summarized in Tables 9 and 10. These baseline phenotype groups are not meant to represent clinical susceptibility breakpoints for APTIVUS/ritonavir because the data are based on the select 1182.12 and 1182.48 subject population. The data are provided to give clinicians information on the likelihood of virologic success based on pre-treatment susceptibility to APTIVUS/ritonavir in protease inhibitor-experienced subjects.
Table 9 Response by Baseline Tipranavir Phenotype at 48 weeks in the Controlled Clinical Trials 1182.12 and 1182.48 Baseline Tipranavir Phenotype
(Fold Change)aProportion of Respondersb with No New Enfuvirtidec Use
N=211Proportion of Respondersb with New Enfuvirtided Use
N=68Tipranavir Susceptibility aChange in tipranavir EC50 value from wild-type reference bConfirmed ≥1 log10 decrease at Week 48 cNo new enfuvirtide is defined as recycled or continued use of enfuvirtide or no use of enfuvirtide dNew enfuvirtide is defined as initiation of enfuvirtide for the first time 0-3 48% (73/153) 70% (33/47) Susceptible >3-10 21% (10/48) 53% (8/15) Decreased Susceptibility >10 10% (1/10) 50% (3/6) Resistant Table 10 Correlation of Baseline Tipranavir Phenotype to Genotype using HIV-1 isolates from Phase 2 and Phase 3 Clinical Trials Baseline Tipranavir Phenotype (Fold Change)a # of Baseline Protease Substitutions at 33, 82, 84, 90 # of Baseline Tipranavir Resistance-Associated Substitutionsb Tipranavir Susceptibilityc aChange in tipranavir EC50 value from wild-type reference bNumber of amino acid substitutions in HIV-1 protease among L10V, I13V, K20M/R/V, L33F, E35G, M36I, K43T, M46L, I47V, I54A/M/V, Q58E, H69K, T74P, V82L/T, N83D or I84V cDefined by Week 48 response 0-3 0-2 0-4 Susceptible >3-10 3 5-7 Decreased Susceptibility >10 4 8+ Resistant Analyses of pediatric clinical trial 1182.14 also demonstrated that response to therapy was influenced by the number of baseline protease inhibitor substitutions present.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term carcinogenicity studies in mice and rats have been conducted with tipranavir. Mice were administered 30, 150 or 300 mg/kg/day tipranavir, 150/40 mg/kg/day tipranavir/ritonavir in combination, or 40 mg/kg/day ritonavir. The incidences of benign hepatocellular adenomas and combined adenomas/carcinomas were increased in females of all groups except the low dose of tipranavir. These tumors were also increased in male mice at the high-dose of tipranavir and the tipranavir/ritonavir combination group. Hepatocellular carcinoma incidence was increased in female mice given the high dose of tipranavir and both sexes receiving tipranavir/ritonavir. The combination of tipranavir and ritonavir caused an exposure-related increase in this same tumor type in both sexes. The clinical relevance of the carcinogenic findings in mice is unknown. Systemic exposures in mice (based on AUC or Cmax) at all dose levels tested were below those in humans receiving the recommended dose level. Rats were administered 30, 100 or 300 mg/kg/day tipranavir, 100/26.7 mg/kg/day tipranavir/ritonavir in combination, or 10 mg/kg/day ritonavir. No drug-related findings in male rats were observed. At the highest dose of tipranavir, an increased incidence of benign follicular cell adenomas of the thyroid gland was observed in female rats. Based on AUC measurements, exposure to tipranavir at this dose level in rats is approximately equivalent to exposure in humans at the recommended therapeutic dose. This finding is probably not relevant to humans, because thyroid follicular cell adenomas are considered a rodent-specific effect secondary to enzyme induction.
Tipranavir showed no evidence of mutagenicity or clastogenicity in a battery of five in vitro and in vivo tests including the Ames bacterial reverse mutation assay using S. typhimurium and E. coli, unscheduled DNA synthesis in rat hepatocytes, induction of gene mutation in Chinese hamster ovary cells, a chromosome aberration assay in human peripheral lymphocytes, and a micronucleus assay in mice.
Tipranavir had no effect on fertility or early embryonic development in rats at dose levels up to 1000 mg/kg/day, equivalent to a Cmax of 258 µM in females. Based on Cmax levels in these rats, as well as an exposure (AUC) of 1670 µM∙h in pregnant rats from another study, this exposure was approximately equivalent to the anticipated exposure in humans at the recommended dose level of 500 mg/200 mg APTIVUS/ritonavir BID.
13.2 Animal Toxicology and/or Pharmacology
In preclinical studies in rats, tipranavir treatment induced dose-dependent changes in coagulation parameters (increased prothrombin time, increased activated partial thromboplastin time, and a decrease in some vitamin K dependent factors). In some rats, these changes led to bleeding in multiple organs and death. The co-administration of vitamin E in the form of TPGS (d-alpha-tocopherol polyethylene glycol 1000 succinate) with tipranavir resulted in a significant increase in effects on coagulation parameters, bleeding events, and death.
In preclinical studies of tipranavir in dogs, an effect on coagulation parameters was not seen. Co-administration of tipranavir and vitamin E has not been studied in dogs. Clinical evaluation of coagulation effects on HIV-1-infected subjects demonstrated no tipranavir plus ritonavir effect on coagulation parameters [see Warnings and Precautions (5.5)].
-
14 CLINICAL STUDIES
14.1 Clinical Trials in Adults
The following clinical data is derived from analyses of 48-week data from studies measuring effects on plasma HIV-1 RNA levels and CD4+ cell counts. At present there are no results from controlled studies evaluating the effect of APTIVUS/ritonavir on clinical progression of HIV-1.
APTIVUS/ritonavir 500 mg/200 mg BID + optimized background regimen (OBR) vs. Comparator Protease Inhibitor/ritonavir BID + OBR
The two clinical trials 1182.12 and 1182.48 (RESIST 1 and RESIST 2) are ongoing, randomized, controlled, open-label, multicenter studies in HIV-1 positive, triple antiretroviral class experienced subjects. All subjects were required to have previously received at least two protease inhibitor-based antiretroviral regimens and were failing a protease inhibitor-based regimen at the time of study entry with baseline HIV-1 RNA at least 1000 copies/mL and any CD4+ cell count. At least one primary protease gene mutation from among 30N, 46I, 46L, 48V, 50V, 82A, 82F, 82L, 82T, 84V or 90M had to be present at baseline, with not more than two mutations at codons 33, 82, 84 or 90.
These studies evaluated treatment response at 48 weeks in a total of 1483 subjects receiving either APTIVUS co-administered with 200 mg of ritonavir plus OBR versus a control group receiving a ritonavir-boosted protease inhibitor (lopinavir, amprenavir, saquinavir or indinavir) plus OBR. Prior to randomization, OBR was individually defined for each subject based on genotypic resistance testing and subject history. The investigator had to declare OBR, comparator protease inhibitor, and use of new enfuvirtide prior to randomization. Randomization was stratified by choice of comparator protease inhibitor and use of new enfuvirtide.
After Week 8, subjects in the control group who met the protocol defined criteria of initial lack of virologic response or confirmed virologic failure had the option of discontinuing treatment and switching to APTIVUS/ritonavir in a separate roll-over study.
Demographics and baseline characteristics were balanced between the APTIVUS/ritonavir arm and control arm. In both studies combined, the 1483 subjects had a median age of 43 years (range 17-80), and were 86.3% male, 75.6% white, 12.9% black, and 0.9% Asian. The median baseline plasma HIV-1 RNA for both treatment groups was 4.8 (range 2.0 to 6.8) log10 copies/mL and median baseline CD4+ cell count was 162 (range 1 to 1894) cells/mm3. Overall, 38.4% of subjects had a baseline HIV-1 RNA of >100,000 copies/mL, 58.6% had a baseline CD4+ cell count ≤200 cells/mm3, and 57.8% had experienced an AIDS defining Class C event at baseline.
Subjects had prior exposure to a median of 6 NRTIs, 1 NNRTI, and 4 PIs. A total of 10.1% of subjects had previously used enfuvirtide. In baseline subject samples (n=454), 97% of the HIV-1 isolates were resistant to at least one protease inhibitor, 95% of the isolates were resistant to at least one NRTI, and >75% of the isolates were resistant to at least one NNRTI.
The individually pre-selected protease inhibitor based on genotypic testing and the subject's medical history was lopinavir in 48.7%, amprenavir in 26.4%, saquinavir in 21.8% and indinavir in 3.1% of subjects. A total of 85.1% were possibly resistant or resistant to the pre-selected comparator protease inhibitors. Approximately 21% of subjects used enfuvirtide during the study of which 16.6% in the APTIVUS/ritonavir arm and 13.2% in the comparator/ritonavir arm represented first time use of enfuvirtide (new enfuvirtide).
Treatment response and efficacy outcomes of randomized treatment through Week 48 of studies 1182.12 and 1182.48 are shown in Table 11.
Table 11 Outcomes of Randomized Treatment Through Week 48 (Pooled Studies 1182.12 and 1182.48) Outcome APTIVUS/ritonavir (500/200 mg BID) + OBR
(N=746)Comparator Protease Inhibitor*/ritonavir + OBR
(N=737)*Comparator protease inhibitors were lopinavir, amprenavir, saquinavir or indinavir and 85.1% of subjects were possibly resistant or resistant to the chosen protease inhibitors. aSubjects achieved and maintained a confirmed ≥1 log10 HIV-1 RNA drop from baseline through Week 48 without prior evidence of treatment failure. bSubjects did not achieve a 0.5 log10 HIV-1 RNA drop from baseline and did not have viral load <100,000 copies/mL by Week 8. cDeath only counted if it was the reason for treatment failure. dIncludes subjects who were lost to-follow-up, withdrawn consent, non-adherent, protocol violations, added/changed background antiretroviral drugs for reasons other than tolerability or toxicity, or discontinued while suppressed. Virologic Respondersa (confirmed at least 1 log10 HIV-1 RNA below baseline) 33.8% 14.9% Virologic failures 55.1% 77.3% Initial lack of virologic response by Week 8b 33.0% 57.9% Rebound 18.9% 16.4% Never suppressed 3.2% 3.0% Deathc or discontinued due to adverse events 5.9% 1.9% Death 0.5% 0.3% Discontinued due to adverse events 5.4% 1.6% Discontinued due to other reasonsd 5.2% 5.8% Through 48 weeks of treatment, the proportion of subjects in the APTIVUS/ritonavir arm compared to the comparator PI/ritonavir arm with HIV-1 RNA <400 copies/mL was 30.3% and 13.6% respectively, and with HIV-1 RNA <50 copies/mL was 22.7% and 10.2% respectively. Among all randomized and treated subjects, the median change from baseline in HIV-1 RNA at the last measurement up to Week 48 was -0.64 log10 copies/mL in subjects receiving APTIVUS/ritonavir versus -0.22 log10 copies/mL in the comparator PI/ritonavir arm.
Among all randomized and treated subjects, the median change from baseline in CD4+ cell count at the last measurement up to Week 48 was +23 cells/mm3 in subjects receiving APTIVUS/ritonavir (N=740) versus +4 cells/mm3 in the comparator PI/ritonavir (N=727) arm.
Subjects in the APTIVUS/ritonavir arm achieved a significantly better virologic outcome when APTIVUS/ritonavir was combined with enfuvirtide. Among subjects with new enfuvirtide use, the proportion of subjects in the APTIVUS/ritonavir arm compared to the comparator PI/ritonavir arm with HIV-1 RNA <400 copies/mL was 52.4% and 19.6% respectively, and with HIV-1 RNA <50 copies/mL was 37.3% and 14.4% respectively [see Clinical Pharmacology (12.2) and Microbiology (12.4)]. The median change from baseline in CD4+ cell count at the last measurement up to Week 48 was +89 cells/mm3 in subjects receiving APTIVUS/ritonavir in combination with newly introduced enfuvirtide (N=124) and +18 cells/mm3 in the comparator PI/ritonavir (N=96) arm.
14.2 Clinical Trials in Pediatrics
The pharmacokinetic profile, safety and activity of APTIVUS/ritonavir was evaluated in a randomized, open-label, multicenter study. This study enrolled a total of 52 HIV-1 infected, treatment-experienced pediatric subjects 12 to 18 years of age with baseline HIV-1 RNA of at least 1500 copies/mL.
The 52 randomized pediatric subjects had a median age of 15 years (range 12 to 18), and were 53.8% male, 67.3% white, 32.7% black, and 0% Asian. The median baseline plasma HIV-1 RNA was 4.7 (range 2.98 to 6.78) log10 copies/mL and median baseline CD4+ cell count was 318 (range 2 to 650) cells/mm3. Overall, 63.5% had a baseline CD4+ cell count ≤200 cells/mm3 and 29.6% had experienced a prior AIDS defining Class C event at baseline. Subjects had prior exposure to a median of 5 NRTIs, 1 NNRTI, and 4 PIs.
At 48 weeks, the overall proportion of subjects 12 to 18 years of age with HIV-1 RNA <400 copies/mL and <50 copies/mL were 33% and 25%, respectively and were similar to adults.
-
16 HOW SUPPLIED/STORAGE AND HANDLING
APTIVUS capsules 250 mg are pink, oblong soft gelatin capsules imprinted in black with "TPV 250". They are packaged in HDPE unit-of-use bottles with a child resistant closure and 120 capsules. (NDC 0597-0003-02).
Storage
- APTIVUS capsules should be stored in a refrigerator 2°C-8°C (36°F-46°F) prior to opening the bottle. After opening the bottle, the capsules may be stored at 20°C-25°C (68°F-77°F); excursions permitted to 15°C-30°C (59°F-86°F) [see USP Controlled Room Temperature] and must be used within 60 days after first opening of the bottle.
Store in a safe place out of the reach of children.
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information).
- Hepatic Impairment and Toxicity
Inform patients that APTIVUS co-administered with 200 mg of ritonavir, has been associated with severe liver disease, including some deaths. Patients with signs or symptoms of clinical hepatitis should discontinue APTIVUS/ritonavir treatment and seek medical evaluation. Symptoms of hepatitis include fatigue, malaise, anorexia, nausea, jaundice, bilirubinuria, acholic stools, liver tenderness or hepatomegaly. Extra vigilance is needed for patients with chronic hepatitis B or C co-infection, as these patients have an increased risk of developing hepatotoxicity.
Liver function tests should be performed prior to initiating therapy with APTIVUS and 200 mg of ritonavir, and frequently throughout the duration of treatment. Patients with chronic hepatitis B or C co-infection or elevations in liver enzymes prior to treatment are at increased risk (approximately 2-fold) for developing further liver enzyme elevations or severe liver disease. Caution should be exercised when administering APTIVUS/ritonavir to patients with liver enzyme abnormalities or history of chronic liver disease. Increased liver function testing is warranted in these patients. APTIVUS should not be given to patients with moderate to severe hepatic impairment.
- Intracranial Hemorrhage
Inform patients that APTIVUS co-administered with 200 mg of ritonavir has been associated with reports of both fatal and non-fatal intracranial hemorrhage. Patients should report any unusual or unexplained bleeding to their physician.
- Drug Interactions
APTIVUS may interact with some drugs; therefore, advise patients to report to their healthcare provider the use of any other prescription or non-prescription medications or herbal products, particularly St. John's wort.
- Rash
Rash, including flat or raised rashes or sensitivity to the sun, have been reported in approximately 10% of subjects receiving APTIVUS. Some patients who developed rash also had one or more of the following symptoms: joint pain or stiffness, throat tightness, generalized itching, muscle aches, fever, redness, blisters, or peeling of the skin. Women taking birth control pills may get a skin rash. Tell patients to discontinue use of APTIVUS and call their physician right away if any of these symptoms develop.
- Contraceptives
Instruct women receiving estrogen-based hormonal contraceptives that additional or alternative contraceptive measures should be used during therapy with APTIVUS. There may be an increased risk of rash when APTIVUS is given with hormonal contraceptives [see Use in Specific Populations (8.3)].
- Fat Redistribution
Inform patients that redistribution or accumulation of body fat may occur in patients receiving antiretroviral therapy and that the cause and long-term health effects of these conditions are not known at this time.
- Administration
Inform patients that APTIVUS must be co-administered with ritonavir to ensure its therapeutic effect. Failure to correctly co-administer APTIVUS with ritonavir will result in reduced plasma levels of tipranavir that may be insufficient to achieve the desired antiviral effect.
- APTIVUS co-administered with ritonavir tablets must only be taken with meals
Instruct patients to swallow APTIVUS capsules whole. They must not be opened or chewed.
Tell patients that sustained decreases in plasma HIV-1 RNA have been associated with a reduced risk of progression to AIDS and death. Patients should remain under the care of a physician while using APTIVUS. Advise patients to take APTIVUS and other concomitant antiretroviral therapy every day as prescribed. APTIVUS, co-administered with ritonavir, must be given in combination with other antiretroviral drugs. Patients should not alter the dose or discontinue therapy without consulting with their healthcare professional. If a dose of APTIVUS is missed, patients should take the dose as soon as possible and then return to their normal schedule. However, if a dose is skipped the patient should not double the next dose.
- Pregnancy Registry
Advise patients that there is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to APTIVUS during pregnancy [see Use in Specific Populations (8.1)].
- Lactation
Inform individuals with HIV-1 infection that the potential risks of breastfeeding include: (1) HIV 1 transmission (in HIV-1–negative infants), (2) developing viral resistance (in HIV-1–positive infants), and (3) adverse reactions in a breastfed infant similar to those seen in adults [see Use in Specific Populations (8.2)].
-
SPL UNCLASSIFIED SECTION
Distributed by:
Boehringer Ingelheim Pharmaceuticals, Inc.
Ridgefield, CT 06877 USALicensed from:
Boehringer Ingelheim International GmbHAddress medical inquiries to: 1-800-542-6257.
APTIVUS is a registered trademark of and used under license from Boehringer Ingelheim International GmbH.
The other brands listed are trademarks of their respective owners and are not trademarks of Boehringer Ingelheim Pharmaceuticals, Inc.
Copyright © 2024 Boehringer Ingelheim International GmbH
ALL RIGHTS RESERVED
COL9294CD042024
SPL9296E -
PATIENT PACKAGE INSERT
This Patient Information has been approved by the U.S. Food and Drug Administration. Revised: 04/2024 PATIENT INFORMATION
APTIVUS® (AP-tih-vus)
(tipranavir) capsulesWhat is the most important information I should know about APTIVUS?
APTIVUS can cause serious side effects, including:- Liver problems. People who take APTIVUS with ritonavir may develop severe liver disease that can cause death. If you have chronic hepatitis B or C infection, you are at increased risk for liver problems. Your healthcare provider should do blood tests before you start taking APTIVUS with ritonavir and regularly during treatment. If you get any of the following symptoms of liver problems, you should stop taking APTIVUS and ritonavir and tell your healthcare provider right away:
- tiredness
- not feeling well
- loss of appetite
- nausea
- yellowing of your skin or whites of your eyes
- dark (tea-colored) urine
- pale stools (bowel movements)
- pain, ache, or sensitivity on your right side below your ribs
- Bleeding in your brain (intracranial hemorrhage, or ICH). People taking APTIVUS with ritonavir may develop bleeding in the brain that can cause death. Tell your healthcare provider about any unusual or unexplained bleeding during treatment with APTIVUS with ritonavir.
What is APTIVUS?
APTIVUS is a prescription medicine used with ritonavir and other HIV-1 medicines to treat Human Immunodeficiency Virus-1 (HIV-1) infection in adults and children weighing 79 pounds (36 kg) or higher who:- have taken HIV-1 medicines in the past, and
- whose healthcare provider determines that they meet certain requirements
Do not take APTIVUS if you: - have moderate to severe liver problems
- take any of the following medicines:
- alfuzosin
- amiodarone
- atorvastatin or a product that contains atorvastatin
- bepridil
- cisapride
- ergot-containing medicines:
- dihydroergotamine
- ergonovine
- ergotamine
- methylergonovine
- flecainide
- lovastatin or a product that contains lovastatin
- lurasidone
- midazolam, when taken by mouth
- pimozide
- propafenone
- quinidine
- rifampin
- sildenafil, when used for the treatment of pulmonary arterial hypertension (PAH)
- simvastatin or a product that contains simvastatin
- St. John's wort, or a product that contains St. John's wort
- triazolam
Before taking APTIVUS, tell your healthcare provider about all of your medical conditions, including if you: - have hemophilia
- have a medical condition that increases your risk of bleeding, including trauma or surgery, or take medicines that increase your risk of bleeding, or take a high dose of vitamin E.
- have liver problems, including hepatitis B or hepatitis C
- have high cholesterol or high triglycerides
- are allergic to sulfa (sulfonamide)
- have diabetes
- are pregnant or plan to become pregnant. It is not known if APTIVUS can harm your unborn baby. Tell your healthcare provider if you become pregnant during treatment with APTIVUS.
- APTIVUS may reduce how well hormonal birth control (contraceptives) pills work. Women who may become pregnant should use a different form of birth control or an additional barrier method of birth control during treatment with APTIVUS. In addition, there may be an increased risk of rash when APTIVUS is taken with birth control pills.
- are breastfeeding or plan to breastfeed. It is not known if APTIVUS can pass into your breast milk. Talk to your healthcare provider about the following risks of breastfeeding during treatment with APTIVUS:
- The HIV-1 virus may pass to your baby if your baby does not have the HIV-1 infection
- The HIV-1 virus may become harder to treat if your baby has HIV-1 infection.
- Your baby may get side effects from APTIVUS.
- You can ask your healthcare provider or pharmacist for a list of medicines that interact with APTIVUS.
- Do not start taking a new medicine without telling your healthcare provider. Your healthcare provider can tell you if it is safe to take APTIVUS with other medicines.
How should I take APTIVUS? - Take APTIVUS exactly as your healthcare provider tells you.
- You must take APTIVUS at the same time you take ritonavir.
- APTIVUS taken with ritonavir tablets must only be taken with meals.
- Take 2 APTIVUS capsules with your prescribed dose of ritonavir twice a day.
- Swallow APTIVUS capsules whole. Do not open or chew the capsules.
- APTIVUS taken with ritonavir must be used together with other HIV-1 medicines.
- Do not change your dose or stop taking APTIVUS without talking to your healthcare provider.
- Stay under the care of your healthcare provider during treatment with APTIVUS.
- If you forget to take APTIVUS, take the next dose of APTIVUS together with ritonavir as soon as you remember. Take your next dose of APTIVUS at your normal time. Do not take a double dose to make up for a missed dose.
- When your APTIVUS supply starts to run low, get more from your healthcare provider or pharmacy. This is very important because the amount of virus in your blood may increase if the medicine is stopped for even a short time. The virus may develop resistance to APTIVUS and become harder to treat.
- If you take too much APTIVUS, call your healthcare provider or go to the nearest hospital emergency room right away.
What are the possible side effects of APTIVUS?
APTIVUS may cause serious side effects, including:- See "What is the most important information I should know about APTIVUS?"
- Rash. Some people who take APTIVUS can get a rash including flat or raised rashes or sensitivity to the sun. Women taking hormonal therapy (birth control pills or hormonal replacement therapy) may be at an increased risk of getting a skin rash. If you get any of the following symptoms, stop taking APTIVUS and call your healthcare provider right away:
- joint pain or stiffness
- throat tightness
- itching
- muscle aches
- fever
- redness
- blisters
- peeling of the skin
- Diabetes and high blood sugar (hyperglycemia). Some people who take protease inhibitors including APTIVUS can get high blood sugar, develop diabetes, or your diabetes can get worse. Tell your healthcare provider if you notice an increase in thirst or if you start urinating more often during treatment with APTIVUS.
- Changes in your immune system (Immune Reconstitution Syndrome) can happen when you start taking HIV-1 medicines. Your immune system may get stronger and begin to fight infections that have been hidden in your body for a long time. Tell your healthcare provider right away if you start having new symptoms after starting your HIV-1 medicine.
- Changes in body fat can happen in people who take HIV-1 medicines. The changes may include an increased amount of fat in the upper back and neck ("buffalo hump"), breast, and around the middle of your body (trunk). Loss of fat from the legs, arms, and face may also happen. The exact cause and long-term health effects of these conditions are not known.
- Increased blood fat (lipid) levels. Some people who take APTIVUS with ritonavir have increases in blood fat levels (cholesterol and triglycerides). Your healthcare provider will do blood tests to monitor your blood fat levels before you start taking and during treatment of APTIVUS with ritonavir.
- Increased bleeding in people with hemophilia. Some people with hemophilia have increased bleeding with protease inhibitors including APTIVUS.
- diarrhea
- nausea
- fever
- vomiting
- tiredness
- headache
- stomach pain
The most common side effects of APTIVUS in children were the same as those seen in adults. Rash was seen more frequently in children than in adults.
These are not all of the possible side effects of APTIVUS.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.How should I store APTIVUS? - Store unopened bottles of APTIVUS capsules in a refrigerator at 36°F to 46°F (2°C to 8°C).
- After opening the bottle of APTIVUS, the capsules may be stored at room temperature between 68°F to 77°F (20°C to 25°C) and must be used within 60 days after first opening of the bottle.
- APTIVUS capsules come in a bottle with a child resistant closure.
General information about the safe and effective use of APTIVUS.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use APTIVUS for a condition for which it was not prescribed. Do not give APTIVUS to other people, even if they have the same condition you have. It may harm them. You can ask your pharmacist or healthcare professional for information about APTIVUS that is written for health professionals.What are the ingredients in APTIVUS?
Active Ingredient: tipranavir
Major Inactive Ingredients: dehydrated alcohol, polyoxyl 35 castor oil, propylene glycol, mono/diglycerides of caprylic/capric acid, and gelatin.
Distributed by: Boehringer Ingelheim Pharmaceuticals, Inc. Ridgefield, CT 06877 USA
Licensed from: Boehringer Ingelheim International GmbH
APTIVUS is a registered trademark of and used under license from Boehringer Ingelheim International GmbH.
The other brands listed are trademarks of their respective owners and are not trademarks of Boehringer Ingelheim Pharmaceuticals, Inc.
Copyright © 2024 Boehringer Ingelheim International GmbH
ALL RIGHTS RESERVED
COL9294CD042024
For current prescribing information, scan the code or for additional information, you may also call Boehringer Ingelheim Pharmaceuticals, Inc. at 1-800-542-6257.
-
PRINCIPAL DISPLAY PANEL - 250 mg Capsule Bottle Label
NDC 0597-0003-02
Aptivus®
(tipranavir)
Capsules 250 mg120 capsules
Unit of Use ContainerEach capsule contains 250 mg tipranavir and
7% w/w dehydrated alcohol (0.1 g per capsule).ALERT
Find out about medicines that should
not be taken with AptivusNote to Pharmacist: Do not cover
ALERT box with Pharmacy labelBoehringer
IngelheimRx only
-
INGREDIENTS AND APPEARANCE
APTIVUS
tipranavir capsule, liquid filledProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:0597-0003 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength TIPRANAVIR (UNII: ZZT404XD09) (TIPRANAVIR - UNII:ZZT404XD09) TIPRANAVIR 250 mg Product Characteristics Color PINK Score no score Shape CAPSULE (oval) Size 22mm Flavor Imprint Code TPV;250 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:0597-0003-02 120 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2005 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA021814 07/01/2005 Labeler - Boehringer Ingelheim Pharmaceuticals, Inc. (603175944) Registrant - Boehringer Ingelheim Pharmaceuticals, Inc. (603175944) Establishment Name Address ID/FEI Business Operations West-Ward Columbus Inc. 058839929 PACK(0597-0003) , LABEL(0597-0003) Establishment Name Address ID/FEI Business Operations Catalent Pharma Solutions 051762268 MANUFACTURE(0597-0003) Establishment Name Address ID/FEI Business Operations Boehringer Ingelheim Pharma GmbH and Co. KG 551147440 API MANUFACTURE(0597-0003)