Label: MILNACIPRAN HCL tablet




-
NDC Code(s):
65162-091-06,
65162-092-06,
65162-093-06,
65162-093-50, view more65162-094-06, 65162-094-50
- Packager: Amneal Pharmaceuticals LLC
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: Abbreviated New Drug Application
Drug Label Information
Updated March 15, 2024
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Medication Guide: HTML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use MILNACIPRAN HYDROCHLORIDE TABLETS safely and effectively. See full prescribing information for MILNACIPRAN HYDROCHLORIDE TABLETS.
MILNACIPRAN HYDROCHLORIDE tablets, for oral use
Initial U.S. Approval: 2009WARNING: SUICIDALITY AND ANTIDEPRESSANT DRUGS
See full prescribing information for complete boxed warning.
- Increased risk of suicidal ideation, thinking, and behavior in children, adolescents, and young adults taking antidepressants for major depressive disorder (MDD) and other psychiatric disorders. (5.1)
INDICATIONS AND USAGE
DOSAGE AND ADMINISTRATION
- Administer milnacipran hydrochloride tablets in two divided doses per day. (2.1)
- Based on efficacy and tolerability, dosing may be titrated according to the following schedule (2.1):
Day 1: 12.5 mg once
Days 2 to 3: 25 mg/day (12.5 mg twice daily)
Days 4 to 7: 50 mg/day (25 mg twice daily)
After Day 7: 100 mg/day (50 mg twice daily)DOSAGE FORMS AND STRENGTHS
- Tablets: 12.5 mg, 25 mg, 50 mg, 100 mg (3)
CONTRAINDICATIONS
- Serotonin Syndrome and MAOIs: Do not use MAOIs intended to treat psychiatric disorders with milnacipran hydrochloride or within 5 days of stopping treatment with milnacipran hydrochloride. Do not use milnacipran hydrochloride within 14 days of stopping an MAOI intended to treat psychiatric disorders. In addition, do not start milnacipran hydrochloride in a patient who is being treated with linezolid or intravenous methylene blue. (4.1, 5.2)
WARNINGS AND PRECAUTIONS
- Suicidality: Monitor for worsening of depressive symptoms and suicide risk. (5.1)
- Serotonin Syndrome: Increased risk when co-administered with other serotonergic agents, but also when taken alone. If it occurs, discontinue Milnacipran hydrochloride and any other serotonergic agents and initiate supportive treatment. (5.2)
- Elevated Blood Pressure and Heart Rate: Milnacipran hydrochloride may increase blood pressure and heart rate. Measure blood pressure and heart rate prior to initiating treatment with milnacipran hydrochloride and monitor periodically throughout treatment. (5.3, 5.4)
- Seizures: Cases have been reported with milnacipran hydrochloride therapy. Prescribe milnacipran hydrochloride with care in patients with a history of seizure disorder. (5.5)
- Hepatotoxicity: Milnacipran hydrochloride may cause elevations of ALT and AST. Avoid concomitant use of milnacipran hydrochloride in patients with substantial alcohol use or chronic liver disease. (5.6)
- Discontinuation: Withdrawal symptoms have been reported in patients when discontinuing treatment with milnacipran hydrochloride. A gradual dose reduction is recommended. (5.7)
- Increased Risk of Bleeding: Milnacipran hydrochloride may increase the risk of bleeding events. Caution patients about the risk of bleeding associated with the concomitant use of milnacipran hydrochloride and NSAIDs, aspirin, or other drugs that affect coagulation. (5.9)
- History of Dysuria: Male patients with a history of obstructive uropathies may experience higher rates of genitourinary adverse events. (5.11)
- Sexual Dysfunction: Milnacipran hydrochloride use may cause symptoms of sexual dysfunction. (5.12)
ADVERSE REACTIONS
The most frequently occurring adverse reactions (≥ 5% and greater than placebo) were nausea, headache, constipation, dizziness, insomnia, hot flush, hyperhidrosis, vomiting, palpitations, heart rate increased, dry mouth, and hypertension. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Amneal Pharmaceuticals, at 1-877-835-5472 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
- Pregnancy: Third trimester use may increase risk for symptoms of poor adaptation (respiratory distress, temperature instability, feeding difficulty, hypotonia, tremor, irritability) in the neonate. (8.1)
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 3/2024
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: SUICIDALITY AND ANTIDEPRESSANT DRUGS
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosing
2.2 Patients with Renal Insufficiency
2.3 Patients with Hepatic Insufficiency
2.4 Discontinuing Milnacipran Hydrochloride Tablets
2.5 Switching a Patient to or from a Monoamine Oxidase Inhibitor (MAOI) Intended to Treat Psychiatric Disorders
2.6 Use of Milnacipran Hydrochloride Tablets with other MAOIs such as Linezolid or Methylene Blue
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
4.1 Monoamine Oxidase Inhibitors (MAOIs)
5 WARNINGS AND PRECAUTIONS
5.1 Suicide Risk
5.2 Serotonin Syndrome
5.3 Elevated Blood Pressure
5.4 Elevated Heart Rate
5.5 Seizures
5.6 Hepatotoxicity
5.7 Discontinuation of Treatment with Milnacipran Hydrochloride
5.8 Hyponatremia
5.9 Increased Risk of Bleeding
5.10 Activation of Mania
5.11 Patients with a History of Dysuria
5.12 Sexual Dysfunction
5.13 Angle Closure Glaucoma
5.14 Concomitant Use with Alcohol
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Post-marketing Experience
7 DRUG INTERACTIONS
7.1 Monoamine Oxidase Inhibitors (MAOIs)
7.2 Serotonergic Drugs
7.3 Triptans
7.4 Catecholamines
7.5 CNS-active drugs
7.6 Clinically Important Interactions with Select Cardiovascular Agents
7.7 Drugs that Interfere with Hemostasis
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
9 DRUG ABUSE AND DEPENDENCE
9.1 Controlled Substance
9.2 Abuse
9.3 Dependence
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
BOXED WARNING
(What is this?)
WARNING: SUICIDALITY AND ANTIDEPRESSANT DRUGS
Milnacipran hydrochloride is a selective serotonin and norepinephrine reuptake inhibitor (SNRI), similar to some drugs used for the treatment of depression and other psychiatric disorders. Antidepressants increased the risk compared to placebo of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults in short-term studies of major depressive disorder (MDD) and other psychiatric disorders. Anyone considering the use of such drugs in a child, adolescent, or young adult must balance this risk with the clinical need. Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24; there was a reduction in risk with antidepressants compared to placebo in adults aged 65 and older. Depression and certain other psychiatric disorders are themselves associated with increases in the risk of suicide. Patients of all ages who are started on milnacipran hydrochloride should be monitored appropriately and observed closely for clinical worsening, suicidality, or unusual changes in behavior. Families and caregivers should be advised of the need for close observation and communication with the prescriber. Milnacipran hydrochloride is not approved for use in the treatment of major depressive disorder. Milnacipran hydrochloride is not approved for use in pediatric patients [see Indications and Usage (1), Warnings and Precautions (5.1), Use in Specific Populations (8.4)].
-
1 INDICATIONS
AND USAGE
Milnacipran hydrochloride tablets are indicated for the management of fibromyalgia.
Milnacipran hydrochloride tablets are not approved for use in pediatric patients [see Use in Specific Populations (8.4)].
-
2 DOSAGE AND ADMINISTRATION
Milnacipran hydrochloride tablets are given orally with or without food.
Taking milnacipran hydrochloride tablets with food may improve the tolerability of the drug.
2.1 Recommended Dosing
The recommended dose of milnacipran hydrochloride tablets is 100 mg/day (50 mg twice daily).
Based on efficacy and tolerability dosing may be titrated according to the following schedule:
Day 1: 12.5 mg once
Days 2 to 3: 25 mg/day (12.5 mg twice daily)
Days 4 to 7: 50 mg/day (25 mg twice daily)
After Day 7: 100 mg/day (50 mg twice daily)Based on individual patient response, the dose may be increased to 200 mg/day (100 mg twice daily).
Doses above 200 mg/day have not been studied.
Taper milnacipran hydrochloride tablets and do not abruptly discontinue after extended use [see Dosage and Administration (2.4) and Warnings and Precautions (5.7)].
2.2 Patients with Renal Insufficiency
No dosage adjustment is necessary in patients with mild renal impairment.
Use milnacipran hydrochloride tablets with caution in patients with moderate renal impairment.
For patients with severe renal impairment (indicated by an estimated creatinine clearance of 5 to 29 mL/min), reduce the maintenance dose by 50% to 50 mg/day (25 mg twice daily).
Based on individual patient response, the dose may be increased to 100 mg/day (50 mg twice daily).
Milnacipran hydrochloride tablets are not recommended for patients with end-stage renal disease.
2.3 Patients with Hepatic Insufficiency
No dosage adjustment is necessary for patients with hepatic impairment.
As with any drug, exercise caution in patients with severe hepatic impairment.
2.4 Discontinuing Milnacipran Hydrochloride Tablets
Withdrawal symptoms have been observed in clinical trials following discontinuation of milnacipran, as with other serotonin and norepinephrine re-uptake inhibitors (SNRIs) and selective serotonin re-uptake inhibitors (SSRIs). Monitor patients for these symptoms when discontinuing treatment. Taper milnacipran hydrochloride tablets and do not abruptly discontinue after extended use [see Warnings and Precautions (5.7)].
2.5 Switching a Patient to or from a Monoamine Oxidase Inhibitor (MAOI) Intended to Treat Psychiatric Disorders
At least 14 days should elapse between discontinuation of a MAOI intended to treat psychiatric disorders and initiation of therapy with milnacipran hydrochloride tablets. Conversely, allow at least 5 days after stopping milnacipran hydrochloride tablets before starting a MAOI intended to treat psychiatric disorders [see Contraindications (4.1)].
2.6 Use of Milnacipran Hydrochloride Tablets with other MAOIs such as Linezolid or Methylene Blue
Do not start milnacipran hydrochloride tablets in a patient being treated with linezolid or intravenous methylene blue because there is increased risk of serotonin syndrome. In a patient who requires more urgent treatment of a psychiatric condition, consider other interventions, including hospitalization [see Contraindications (4.1)].
In some cases, a patient already receiving milnacipran hydrochloride tablets therapy may require urgent treatment with linezolid or intravenous methylene blue. If acceptable alternatives to linezolid or intravenous methylene blue treatment are not available and the potential benefits of linezolid or intravenous methylene blue treatment are judged to outweigh the risks of serotonin syndrome in a particular patient, discontinue milnacipran hydrochloride tablets promptly, and consider administering linezolid or intravenous methylene blue. Monitor the patient for symptoms of serotonin syndrome for 5 days or until 24 hours after the last dose of linezolid or intravenous methylene blue, whichever comes first. Therapy with milnacipran hydrochloride tablets may be resumed 24 hours after the last dose of linezolid or intravenous methylene blue [see Warnings and Precautions (5.2)].
The risk of administering methylene blue by non-intravenous routes (such as oral tablets or by local injection) or in intravenous doses much lower than 1 mg/kg with milnacipran hydrochloride tablets are unclear. The clinician should nevertheless be aware of the possibility of emergent symptoms of serotonin syndrome with such use [see Warnings and Precautions (5.2)].
-
3 DOSAGE FORMS AND STRENGTHS
Film-coated, immediate-release tablets available in four strengths: 12.5 mg, 25 mg, 50 mg, and 100 mg of milnacipran hydrochloride.
Milnacipran hydrochloride tablets, 12.5 mg are blue color, round shaped, biconvex, film-coated tablets, debossed with "AN" on one side and "091" on the other side.
Milnacipran hydrochloride tablets, 25 mg are white to off-white, round shaped, biconvex, film-coated tablets, debossed with "AN" on one side and "092" on the other side.
Milnacipran hydrochloride tablets, 50 mg are white to off-white, oval shaped, biconvex, film-coated tablets, debossed with "AN" on one side and "093" on the other side.
Milnacipran hydrochloride tablets, 100 mg are pink color, oval shaped, biconvex, film-coated tablets, debossed with "AN" on one side and "094" on the other side.
-
4 CONTRAINDICATIONS
4.1 Monoamine Oxidase Inhibitors (MAOIs)
The use of MAOIs intended to treat psychiatric disorders with milnacipran hydrochloride or within 5 days of stopping treatment with milnacipran hydrochloride is contraindicated because of an increased risk of serotonin syndrome. The use of milnacipran hydrochloride within 14 days of stopping an MAOI intended to treat psychiatric disorders is also contraindicated [see Dosage and Administration (2.5), Warnings and Precautions (5.2)].
Starting milnacipran hydrochloride in a patient who is being treated with MAOIs such as linezolid or intravenous methylene blue is also contraindicated because of an increased risk of serotonin syndrome [see Dosage and Administration (2.6), Warnings and Precautions (5.2)].
-
5 WARNINGS AND PRECAUTIONS
5.1 Suicide Risk
Milnacipran hydrochloride is a selective serotonin and norepinephrine re-uptake inhibitor (SNRI), similar to some drugs used for the treatment of depression and other psychiatric disorders.
Patients, both adult and pediatric, with depression or other psychiatric disorders may experience worsening of their depression and/or the emergence of suicidal ideation and behavior (suicidality) or unusual changes in behavior, whether or not they are taking these medications, and this risk may persist until significant remission occurs. Suicide is a known risk of depression and certain other psychiatric disorders, and these disorders themselves are the strongest predictors of suicide. There has been a long-standing concern, however, that antidepressants, including drugs that inhibit the reuptake of norepinephrine and/or serotonin, may have a role in inducing worsening of depression and the emergence of suicidality in certain patients during the early phases of treatment.
In the placebo-controlled clinical trials of adults with fibromyalgia, among the patients who had a history of depression at treatment initiation, the incidence of suicidal ideation was 0.5% in patients treated with placebo, 0% in patients treated with milnacipran hydrochloride 100 mg/day, and 1.3% in patients treated with milnacipran hydrochloride 200 mg/day. No suicides occurred in the short-term or longer-term (up to 1 year) fibromyalgia trials.
Pooled analyses of short-term placebo-controlled trials of drugs used to treat depression (SSRIs and others) showed that these drugs increase the risk of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults (ages 18 to 24) with major depressive disorder (MDD) and other psychiatric disorders. Short-term studies did not show an increase in the risk of suicidality with these drugs compared to placebo in adults beyond age 24; there was a reduction in suicidality risk with antidepressants compared to placebo in adults age 65 and older.
The pooled analyses of placebo-controlled trials in children and adolescents with MDD, obsessive compulsive disorder (OCD), or other psychiatric disorders included a total of 24 short-term trials of 9 drugs used to treat depression in over 4,400 patients. The pooled analyses of placebo-controlled trials in adults with MDD or other psychiatric disorders included a total of 295 short-term trials (median duration of 2 months) of 11 antidepressant drugs in over 77,000 patients.
There was considerable variation in risk of suicidality among drugs, but a tendency toward an increase in the younger patients for almost all drugs studied. There were differences in absolute risk of suicidality across the different indications, with the highest incidence in MDD. The risk of differences (drug versus placebo), however, were relatively stable within age strata and across indications. These risk differences (drug-placebo difference in the number of cases of suicidality per 1,000 patients treated) are provided in Table 1.
Table 1: Risk Differences (Drug – Placebo) in the number of Cases of Suicidality, per 1,000 patients treated
Age Range
Drug-Placebo Difference in Number of Cases of Suicidality per 1,000 Patients Treated
< 18
14 additional cases
18 to 24
5 additional cases
Decreases Compared to Placebo
25 to 64
1 fewer case
≥ 65
6 fewer cases
No suicides occurred in any of the pediatric trials. There were suicides in the adult trials, but the number was not sufficient to reach any conclusion about drug effect on suicide.
It is unknown whether the suicidality risk extends to longer-term use, i.e. beyond several months.
However, there is substantial evidence from placebo-controlled maintenance trials in adults with depression that the use of antidepressants can delay the recurrence of depression.
All patients being treated with drugs inhibiting the reuptake of norepinephrine and/or serotonin for any indication should be monitored appropriately and observed closely for clinical worsening, suicidality, and unusual changes in behavior, especially during the initial few months of a course of drug therapy, or at times of dose changes, either increases or decreases.
The following symptoms, anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania, mania, have been reported in adult and pediatric patients being treated with drugs inhibiting the reuptake of norepinephrine and/or serotonin for major depressive disorder as well as for other indications, both psychiatric and non-psychiatric. Although a causal link between the emergence of such symptoms and either the worsening of depression and/or the emergence of suicidal impulses has not been established, there is concern that such symptoms may represent precursors to emerging suicidality.
Consideration should be given to changing the therapeutic regimen, including possibly discontinuing the medication, in patients who may experience worsening depressive symptoms, or who are experiencing emergent suicidality or symptoms that might be precursors to worsening depression or suicidality, especially if these symptoms are severe or abrupt in onset, or were not part of the patient’s presenting symptoms.
If the decision has been made to discontinue treatment due to worsening depressive symptoms or emergent suicidality, medication should be tapered, as rapidly as is feasible, but with recognition that abrupt discontinuation can produce withdrawal symptoms [see Dosage and Administration (2.1, 2.4) and Warnings and Precautions (5.7)].
Families and caregivers of patients being treated with drugs inhibiting the reuptake of norepinephrine and/or serotonin for major depressive disorder or other indications, both psychiatric and nonpsychiatric, should be alerted about the need to monitor patients for the emergence of agitation, irritability, unusual changes in behavior, and the other symptoms described above, as well as the emergence of suicidality, and to report such symptoms immediately to health care providers. Such monitoring should include daily observation by families and caregivers. Prescriptions for milnacipran hydrochloride should be written for the smallest quantity of tablets consistent with good patient management, in order to reduce the risk of overdose.
5.2 Serotonin Syndrome
Selective-serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs), including milnacipran hydrochloride, can precipitate serotonin syndrome, a potentially life-threatening condition. The risk is increased with concomitant use of other serotonergic drugs (including triptans, tricyclic antidepressants, fentanyl, tramadol, meperidine, methadone, lithium, tryptophan, buspirone, amphetamines, and St. John’s Wort) and with drugs that impair metabolism of serotonin i.e. MAOIs [see Contraindications (4), Drug Interactions (7)]. Serotonin syndrome can also occur when these drugs are used alone.
Serotonin syndrome symptoms may include mental status changes (e.g., agitation, hallucinations, delirium, and coma), autonomic instability (e.g., tachycardia, labile blood pressure, dizziness, diaphoresis, flushing, hyperthermia), neuromuscular symptoms (e.g., tremor, rigidity, myoclonus, hyperreflexia, incoordination), seizures, and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea).
The concomitant use of milnacipran hydrochloride with MAOIs is contraindicated. In addition, do not initiate milnacipran hydrochloride in a patient who is being treated with MAOIs such as linezolid or intravenous methylene blue. No reports involved the administration of methylene blue by other routes (such as oral tablets or local tissue injection). If it is necessary to initiate treatment with a MAOI such as linezolid or intravenous methylene blue in a patient taking milnacipran hydrochloride, discontinue milnacipran hydrochloride before initiating treatment with the MAOI [see Contraindications (4.1), Dosage and Administration (2.5, 2.6), Drug Interactions (7.1)].
Monitor all patients taking milnacipran hydrochloride for the emergence of serotonin syndrome. Discontinue treatment with milnacipran hydrochloride and any concomitant serotonergic agents immediately if the above events occur and initiate supportive symptomatic treatment. If concomitant use of milnacipran hydrochloride with other serotonergic drugs is clinically warranted, inform patients of the increased risk for serotonin syndrome and monitor for symptoms.
5.3 Elevated Blood Pressure
A double-blind, placebo-controlled ambulatory blood pressure monitoring (ABPM) study was conducted to evaluate the effects of milnacipran (up to 200 mg/day) on blood pressure in 321 fibromyalgia patients. Among fibromyalgia patients who were normotensive at baseline, an analysis of the blood pressure findings demonstrated a substantially higher proportion of milnacipran hydrochloride-treated patients had a hypertensive blood pressure measurement at the Week 4, 50 mg BID steady-state visit (17.7% [n=21/119]) and the Week 7, 100 mg BID steady-state visit (14.3% [n=15/105]) as compared to placebo-treated patients (3.7% [n=2/54] and 0% [0/49] at the Week 4 and Week 7 visits, respectively). Hypertension was defined as mean systolic blood pressure (SBP) ≥ 140 mmHg and change from baseline in mean SBP ≥ 10 mmHg or mean diastolic blood pressure (DBP) ≥ 90 mmHg and change from baseline in mean DBP ≥ 5 mmHg for the 12-hour period post AM study drug measurement at that visit. Furthermore, 1.9% (4/210) of milnacipran hydrochloride-treated and 0.9% (1/111) of placebo patients discontinued treatment for increases in blood pressure.
The increased risk of blood pressure measurements in the hypertensive range in milnacipran hydrochloride-treated patients is supported by substantial increases in mean SBP and DBP measurements observed in the ABPM study. Table 2 shows that, following treatment with milnacipran hydrochloride 50 mg BID for three weeks in patients who were normotensive at baseline, the mean increase from baseline was 5 mmHg in systolic blood pressure (SBP) and diastolic blood pressure (DBP). After further treatment with milnacipran hydrochloride 100 mg BID for two weeks, the mean increase from baseline in SBP and DBP was 6 mmHg. Similar elevations occurred in milnacipran hydrochloride-treated patients who were hypertensive at baseline.
Table 2: Mean (Standard Error) Change from Baseline in Mean 24-hour Systolic and Diastolic Blood Pressure (mmHg) of Milnacipran or Placebo following 4 Weeks of Treatment (50mg BID) and a Subsequent 2 Weeks of Treatment (100mg BID)
Normotensive
Hypertensive
n
Systolic
Diastolic
n
Systolic
Diastolic
Placebo
39
0(2)
-1(1)
50
0(2)
0(2)
50 mg BID*
92
5(1)
5(1)
84
5(2)
4(1)
Placebo
37
0(2)
-1(1)
47
-1(2)
0(1)
100 mg BID^
82
6(1)
6(1)
80
5(2)
4(1)
*Blood pressure measurements made after 3 weeks of milnacipran 50mg BID
^Blood pressure measurements made after 2 weeks of milnacipran 100mg BID
Similar patterns of treatment-emergent blood pressure elevations were observed in Phase 3 and clinical pharmacology studies as manifested by an increased risk of new onset hypertension or substantial increases in end of study blood pressure measurements in patients with hypertension at baseline (Table 3).
Table 3: Blood pressure changes in Phase 3 randomized controlled trials
Milnacipran
50 mg BIDMilnacipran
100 mg BIDPlacebo
FM patients normotensive at baseline
who became hypertensive (defined as
SBP ≥ 140 mmHg or DBP ≥ 90 mmHg
on three consecutive post-baseline visits)20%
17%
7%
FM patients with sustained increases in
SBP (increase of ≥ 15 mmHg on three
consecutive post-baseline visits)9%
6%
2%
FM patients with sustained increases in
DBP (increase of ≥ 10 mmHg on three
consecutive post-baseline visits)13%
10 %
4%
FM patients hypertensive at baseline
who had increases in SBP ≥ 15 mmHg at
end of study10%
7%
4%
FM patients hypertensive at baseline
who had increases in DBP ≥ 10 mmHg at
end of study8%
6%
3%
Sustained increases in blood pressure may have adverse consequences. Cases of elevated blood pressure requiring immediate treatment have been reported.
Concomitant use of milnacipran hydrochloride with drugs that increase blood pressure and heart rate has not been evaluated and such combinations should be used with caution [see Drug Interactions (7)].
Effects of milnacipran hydrochloride on blood pressure in patients with significant hypertension or cardiac disease have not been systematically evaluated. Milnacipran hydrochloride should be used with caution in these patients.
Measure blood pressure prior to initiating treatment and periodically monitor blood pressure throughout milnacipran hydrochloride treatment. Treat pre-existing hypertension and other cardiovascular disease before starting therapy with milnacipran hydrochloride. For patients who experience a sustained increase in blood pressure while receiving milnacipran hydrochloride, either reduce the dose or discontinue treatment with milnacipran hydrochloride if clinically warranted.
5.4 Elevated Heart Rate
A double-blind, placebo-controlled ABPM study was conducted to evaluate the effects of milnacipran (up to 200 mg/day) on blood pressure in 321 fibromyalgia patients [see Warnings and Precautions (5.3)]. Information on heart rate was also collected. Following treatment with milnacipran hydrochloride 50 mg BID for three weeks in patients who were normotensive at baseline, the mean increase in mean 24-hour heart rate from baseline was 13 beats per minute. After further treatment with milnacipran hydrochloride 100 mg BID for two weeks, the mean increase from baseline in heart rate was 13 beats per minute.
Similar trends were observed in the clinical trials where milnacipran hydrochloride treatment was associated with mean increases in heart rate of approximately 7 to 8 beats per minute [see Adverse Reactions (6.1)].
Increases in heart rate ≥ 20 beats per minute occurred more frequently in milnacipran hydrochloride-treated patients when compared to placebo (8% in the milnacipran hydrochloride 50 mg BID and 100 mg BID treatment arms versus 0.3% in the placebo arm).
Milnacipran hydrochloride has not been systematically evaluated in patients with a cardiac rhythm disorder.
Measure heart rate prior to initiating treatment and periodically monitor the heart rate throughout milnacipran hydrochloride treatment. Treat pre-existing tachyarrhythmias and other cardiac disease before starting therapy with milnacipran hydrochloride. For patients who experience a sustained increase in heart rate while receiving milnacipran hydrochloride, either reduce the dose or discontinue treatment with milnacipran hydrochloride if clinically warranted.
5.5 Seizures
Milnacipran hydrochloride has not been systematically evaluated in patients with a seizure disorder. In clinical trials evaluating milnacipran hydrochloride in patients with fibromyalgia, seizures/convulsions have not been reported. However, seizures have been reported infrequently in patients treated with milnacipran hydrochloride for disorders other than fibromyalgia. Milnacipran hydrochloride should be prescribed with care in patients with a history of a seizure disorder.
5.6 Hepatotoxicity
In the placebo-controlled fibromyalgia trials, increases in the number of patients treated with milnacipran hydrochloride with mild elevations of ALT or AST (1 to 3 times the upper limit of normal, ULN) were observed. Increases in ALT were more frequently observed in the patients treated with milnacipran hydrochloride 100 mg/day (6%) and milnacipran hydrochloride 200 mg/day (7%), compared to the patients treated with placebo (3%). One patient receiving milnacipran hydrochloride 100 mg/day (0.2%) had an increase in ALT greater than 5 times the upper limit of normal but did not exceed 10 times the upper limit of normal. Increases in AST were more frequently observed in the patients treated with milnacipran hydrochloride 100 mg/day (3%) and milnacipran hydrochloride 200 mg/day (5%) compared to the patients treated with placebo (2%).
The increases of bilirubin observed in the fibromyalgia clinical trials were not clinically significant.
No case met the criteria of elevated ALT > 3x ULN and associated with an increase in bilirubin ≥ 2x ULN.
There have been cases of increased liver enzymes and reports of severe liver injury, including fulminant hepatitis with milnacipran from foreign post-marketing experience. In the cases of severe liver injury, there were significant underlying clinical conditions and/or the use of multiple concomitant medications. Because of underreporting, it is impossible to provide an accurate estimate of the true incidence of these reactions.
Discontinue milnacipran hydrochloride in patients who develop jaundice or other evidence of liver dysfunction. Treatment with milnacipran hydrochloride should not be resumed unless another cause can be established.
Milnacipran hydrochloride should ordinarily not be prescribed to patients with substantial alcohol use or evidence of chronic liver disease.
5.7 Discontinuation of Treatment with Milnacipran Hydrochloride
Withdrawal symptoms have been observed in clinical trials following discontinuation of milnacipran, as with other SNRIs and SSRIs.
During marketing of milnacipran, and other SNRIs and SSRIs, there have been spontaneous reports of adverse events indicative of withdrawal and physical dependence occurring upon discontinuation of these drugs, particularly when discontinuation is abrupt. The adverse events include the following: dysphoric mood, irritability, agitation, dizziness, sensory disturbances (e.g., paresthesias such as electric shock sensations), anxiety, confusion, headache, lethargy, emotional lability, insomnia, hypomania, tinnitus, and seizures. Although these events are generally self-limiting, some have been reported to be severe.
Monitor patients for these symptoms when discontinuing treatment with milnacipran hydrochloride. Milnacipran hydrochloride should be tapered after extended use. Do not abruptly discontinue. If intolerable symptoms occur following a decrease in the dose or upon discontinuation of treatment, then resuming the previously prescribed dose may be considered. Subsequently, the physician may continue decreasing the dose but at a more gradual rate [see Dosage and Administration (2.4)].
5.8 Hyponatremia
Hyponatremia may occur as a result of treatment with SSRIs and SNRIs, including milnacipran hydrochloride. In many cases, this hyponatremia appears to be the result of the syndrome of inappropriate antidiuretic hormone secretion (SIADH). Cases with serum sodium lower than 110 mmol/L have been reported. Elderly patients may be at greater risk of developing hyponatremia with SNRIs, SSRIs, or milnacipran hydrochloride. Also, patients taking diuretics or who are otherwise volume-depleted may be at greater risk [see Geriatric Use (8.5)]. Consider discontinuation of milnacipran hydrochloride in patients with symptomatic hyponatremia.
Signs and symptoms of hyponatremia include headache, difficulty concentrating, memory impairment, confusion, weakness, and unsteadiness, which may lead to falls. Signs and symptoms associated with more severe and/or acute cases have included hallucination, syncope, seizure, coma, respiratory arrest, and death.
5.9 Increased Risk of Bleeding
Drugs that interfere with serotonin reuptake, including milnacipran hydrochloride, may increase the risk of bleeding events. Concomitant use of aspirin, nonsteroidal anti-inflammatory drugs (NSAIDs), warfarin, and other anticoagulants may add to this risk. Case reports and epidemiological studies (case-control and cohort design) have demonstrated an association between use of drugs that interfere with serotonin reuptake and the occurrence of gastrointestinal bleeding. Based on data from published observational studies, exposure to SSRIs, particularly in the month before delivery, has been associated with a less than 2-fold increase in the risk of postpartum hemorrhage [see Use in Specific Populations (8.1)]. Bleeding events related to SSRIs and SNRIs have ranged from ecchymosis, hematoma, epistaxis, and petechiae to life-threatening hemorrhages.
Inform patients about the increased risk of bleeding associated with the concomitant use of milnacipran hydrochloride and NSAIDs, aspirin, or other drugs that affect coagulation [see Drug Interactions (7.7)].
5.10 Activation of Mania
No activation of mania or hypomania was reported in the clinical trials evaluating effects of milnacipran hydrochloride in patients with fibromyalgia. However, those clinical trials excluded patients with current major depressive episode. Activation of mania and hypomania have been reported in patients with mood disorders who were treated with other similar drugs for major depressive disorder. As with these other agents, use milnacipran hydrochloride cautiously in patients with a history of mania.
5.11 Patients with a History of Dysuria
Because of their noradrenergic effect, SNRIs including milnacipran hydrochloride, can affect urethral resistance and micturition. In the controlled fibromyalgia trials, dysuria occurred more frequently in patients treated with milnacipran hydrochloride (1%) than in placebo-treated patients (0.5%). Caution is advised in use of milnacipran hydrochloride in patients with a history of dysuria, notably in male patients with prostatic hypertrophy, prostatitis, and other lower urinary tract obstructive disorders. Male patients are more prone to genitourinary adverse effects, such as dysuria or urinary retention, and may experience testicular pain or ejaculation disorders.
5.12 Sexual Dysfunction
Use of SNRIs, including milnacipran hydrochloride, may cause symptoms of sexual dysfunction [see Adverse Reactions (6.1, 6.2)]. In male patients, SNRI use may result in ejaculatory delay or failure, decreased libido, and erectile dysfunction. In female patients, SNRI use may result in decreased libido and delayed or absent orgasm.
It is important for prescribers to inquire about sexual function prior to initiation of milnacipran hydrochloride and to inquire specifically about changes in sexual function during treatment, because sexual function may not be spontaneously reported. When evaluating changes in sexual function, obtaining a detailed history (including timing of symptom onset) is important because sexual symptoms may have other causes, including the underlying psychiatric disorder. Discuss potential management strategies to support patients in making informed decisions about treatment.
5.13 Angle Closure Glaucoma
The pupillary dilation that occurs following use of SNRI drugs including milnacipran hydrochloride may trigger an angle closure attack in a patient with anatomically narrow angles who does not have a patent iridectomy.
5.14 Concomitant Use with Alcohol
In clinical trials, more patients treated with milnacipran hydrochloride developed elevated transaminases than did placebo treated patients [see Warnings and Precautions (5.6)]. Because it is possible that milnacipran may aggravate pre-existing liver disease, milnacipran hydrochloride should not be prescribed to patients with substantial alcohol use or evidence of chronic liver disease.
-
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Patient Exposure
Milnacipran hydrochloride was evaluated in three double-blind placebo-controlled trials involving 2,209 fibromyalgia patients (1,557 patients treated with milnacipran hydrochloride and 652 patients treated with placebo) for a treatment period up to 29 weeks.
The stated frequencies of adverse reactions represent the proportion of individuals who experienced, at least once, a treatment-emergent adverse reaction of the type listed. A reaction was considered treatment emergent if it occurred for the first time or worsened while receiving therapy following baseline evaluation.
Adverse Reactions Leading to Discontinuation
In placebo-controlled trials in patients with fibromyalgia, 23% of patients treated with milnacipran hydrochloride 100 mg/day, 26% of patients treated with milnacipran hydrochloride 200 mg/day discontinued prematurely due to adverse reactions, compared to 12% of patients treated with placebo. The adverse reactions that led to withdrawal in ≥ 1% of patients in the milnacipran hydrochloride treatment group and with an incidence rate greater than that in the placebo treatment group were nausea (milnacipran 6%, placebo 1%), palpitations (milnacipran 3%, placebo 1%), headache (milnacipran 2%, placebo 0%), constipation (milnacipran 1%, placebo 0%), heart rate increased (milnacipran 1%, placebo 0%), hyperhidrosis (milnacipran 1%, placebo 0%), vomiting (milnacipran 1%, placebo 0%), and dizziness (milnacipran 1% and placebo 0.5%). Discontinuation due to adverse reactions was generally more common among patients treated with milnacipran hydrochloride 200 mg/day compared to milnacipran hydrochloride 100 mg/day.
Most Common Adverse Reactions in Placebo Controlled Trials
In the placebo-controlled fibromyalgia patient trials, the most frequently occurring adverse reaction in clinical trials was nausea. The most common adverse reactions (incidence ≥ 5% and twice placebo) in patients treated with milnacipran hydrochloride were constipation, hot flush, hyperhidrosis, vomiting, palpitations, heart rate increased, dry mouth, and hypertension.
Table 4 lists all adverse reactions that occurred in at least 2% of patients treated with milnacipran hydrochloride at either 100 or 200 mg/day and at an incidence greater than that of placebo.
Table 4: Treatment-Emergent Adverse Reaction Incidence in Placebo Controlled Trials in Fibromyalgia Patients (Events Occurring in at Least 2% of All Milnacipran Hydrochloride-Treated Patients and Occurring More Frequently in Either Milnacipran Hydrochloride Treatment Group Than in the Placebo Treatment Group)
System Organ Class–
Preferred TermMilnacipran Hydrochloride
100 mg/day
(n = 623) %Milnacipran Hydrochloride
200 mg/day
(n = 934) %All Milnacipran Hydrochloride
(n = 1,557) %Placebo
(n = 652) %Cardiac Disorders
Palpitations
8
7
7
2
Tachycardia
3
2
2
1
Eye Disorders
Vision blurred
1
2
2
1
Gastrointestinal Disorders
Nausea
35
39
37
20
Constipation
16
15
16
4
Vomiting
6
7
7
2
Dry mouth
5
5
5
2
Abdominal pain
3
3
3
2
General Disorders
Chest pain
3
2
2
2
Chills
1
2
2
0
Chest discomfort
2
1
1
1
Infections
Upper respiratory tract infection
7
6
6
6
Investigations
Heart rate increased
5
6
6
1
Blood pressure increased
3
3
3
1
Metabolism and Nutrition
Disorders
Decreased appetite
1
2
2
0
Nervous System Disorders
Headache
19
17
18
14
Dizziness
11
10
10
6
Migraine
6
4
5
3
Paresthesia
2
3
2
2
Tremor
2
2
2
1
Hypoesthesia
1
2
1
1
Tension headache
2
1
1
1
Psychiatric Disorders
Insomnia
12
12
12
10
Anxiety
5
3
4
4
Respiratory Disorders
Dyspnea
2
2
2
1
Skin Disorders
Hyperhidrosis
8
9
9
2
Rash
3
4
3
2
Pruritus
3
2
2
2
Vascular Disorders
Hot flush
11
12
12
2
Hypertension
7
4
5
2
Flushing
2
3
3
1
Weight Changes
In placebo-controlled fibromyalgia clinical trials, patients treated with milnacipran hydrochloride for up to 3 months experienced a mean weight loss of approximately 0.8 kg in both the milnacipran hydrochloride 100 mg/day and the milnacipran hydrochloride 200 mg/day treatment groups, compared with a mean weight loss of approximately 0.2 kg in placebo-treated patients.
Genitourinary Adverse Reactions in Males
In the placebo-controlled fibromyalgia studies, the following treatment-emergent adverse reactions related to the genitourinary system were observed in at least 2% of male patients treated with milnacipran hydrochloride, and occurred at a rate greater than in placebo-treated male patients: dysuria, ejaculation disorder, erectile dysfunction, ejaculation failure, libido decreased, prostatitis, scrotal pain, testicular pain, testicular swelling, urinary hesitation, urinary retention, urethral pain, and urine flow decreased.
Other Adverse Reactions Observed During Clinical Trials of Milnacipran hydrochloride in Fibromyalgia
Following is a list of frequent (those occurring on one or more occasions in at least 1/100 patients) treatment-emergent adverse reactions reported from 1,824 fibromyalgia patients treated with milnacipran hydrochloride for periods up to 68 weeks. The listing does not include those events already listed in Table 4, those events for which a drug cause was remote, those events which were so general as to be uninformative, and those events reported only once which did not have a substantial probability of being acutely life threatening.
Adverse reactions are categorized by body system and listed in order of decreasing frequency. Adverse reactions of major clinical importance are described in the Warnings and Precautions section (5).
Gastrointestinal Disorders - diarrhea, dyspepsia, gastroesophageal reflux disease, flatulence, abdominal distension
General Disorders - fatigue, peripheral edema, irritability, pyrexia
Infections - urinary tract infection, cystitis
Injury, Poisoning, and Procedural Complications - contusion, fall
Investigations - weight decreased or increased
Metabolism and Nutrition Disorders - hypercholesterolemia
Nervous System Disorders - somnolence, dysgeusia
Psychiatric Disorders - depression, stress
Skin Disorders - night sweats
6.2 Post-marketing Experience
The following additional adverse reactions have been identified from spontaneous reports of milnacipran hydrochloride received worldwide. These adverse reactions have been chosen for inclusion because of a combination of seriousness, frequency of reporting, or potential causal connection to milnacipran hydrochloride. However, because these adverse reactions were reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. These events include:
Blood and Lymphatic System Disorders - leukopenia, neutropenia, thrombocytopenia
Cardiac Disorders - supraventricular tachycardia, Takotsubo cardiomyopathy
Eye Disorders - accommodation disorder
Endocrine Disorders – hyperprolactinemia
Gastrointestinal Disorders - acute pancreatitis
Hepatobiliary Disorders - hepatitis
Metabolism and Nutrition Disorders - anorexia, hyponatremia
Musculoskeletal and Connective Tissue Disorders – rhabdomyolysis
Nervous System Disorders - anosmia, convulsions (including grand mal), hyposmia, loss of consciousness, Parkinsonism
Psychiatric Disorders - aggression, anger, delirium, hallucination, homicidal ideation
Renal and Urinary Disorders - acute renal failure
Reproductive System and Breast Disorders – galactorrhea, decreased libido, delayed or absent orgasm
Skin Disorders - erythema multiforme, Stevens Johnson syndrome
Vascular Disorders - hypertensive crisis
-
7 DRUG INTERACTIONS
Milnacipran undergoes minimal CYP450 related metabolism, with the majority of the dose excreted unchanged in urine (55%) and has a low binding to plasma proteins (13%). In vitro and in vivo studies showed that milnacipran hydrochloride is unlikely to be involved in clinically significant pharmacokinetic drug interactions [see Pharmacokinetics in Special Populations (12.3)].
7.1 Monoamine Oxidase Inhibitors (MAOIs)
The concomitant use of SSRIs and SNRIs, including milnacipran hydrochloride, with MAOIs increases the risk of serotonin syndrome. The use of MAOIs intended to treat psychiatric disorders with milnacipran hydrochloride or within 5 days of stopping treatment with milnacipran hydrochloride is contraindicated. The use of milnacipran hydrochloride within 14 days of stopping an MAOI intended to treat psychiatric disorders is also contraindicated. In addition, do not initiate milnacipran hydrochloride in a patient who is being treated with MAOIs such as linezolid or intravenous methylene blue. No reports involved the administration of methylene blue by other routes (such as oral tablets or local tissue injection). If it is necessary to initiate treatment with a MAOI such as linezolid or intravenous methylene blue in a patient taking milnacipran hydrochloride, discontinue milnacipran hydrochloride before initiating treatment with the MAOI [see Dosage and Administration (2.5, 2.6), Contraindications (4), Drug Interactions (7.1)].
7.2 Serotonergic Drugs
Serotonin syndrome can occur with use of milnacipran hydrochloride and other serotonergic drugs (other SNRIs, SSRIs, triptans, tricyclic antidepressants, opioids, lithium, tryptophan, buspirone, amphetamines, and St. John’s Wort), or with drugs that impair metabolism of serotonin (i.e. monoamine oxidase inhibitors). Advise patients of the signs and symptoms associated with serotonin syndrome and to seek medical care immediately if they experience these symptoms [see Dosage and Administration (2.5, 2.6), Warnings and Precautions (5.2)].
7.3 Triptans
There have been rare post-marketing reports of serotonin syndrome with use of an SSRI and a triptan. If concomitant treatment of milnacipran hydrochloride with a triptan is clinically warranted, careful observation of the patient is advised, particularly during treatment initiation and dose increases [see Warnings and Precautions (5.2)].
7.4 Catecholamines
Milnacipran hydrochloride inhibits the reuptake of norepinephrine. Therefore, concomitant use of milnacipran hydrochloride with epinephrine and norepinephrine may be associated with paroxysmal hypertension and possible arrhythmia [see Warnings and Precautions (5.3, 5.4)].
7.5 CNS-active drugs
Given the primary CNS effects of milnacipran hydrochloride, use caution when it is taken in combination with other centrally acting drugs, including those with a similar mechanism of action.
Clomipramine: In a drug-drug interaction study, an increase in euphoria and postural hypotension was observed in patients who switched from clomipramine to milnacipran hydrochloride.
7.6 Clinically Important Interactions with Select Cardiovascular Agents
Digoxin: Use of milnacipran hydrochloride concomitantly with digoxin may be associated with potentiation of adverse hemodynamic effects. Postural hypotension and tachycardia have been reported in combination therapy with intravenously administered digoxin (1 mg). Avoid co-administration of milnacipran hydrochloride and intravenous digoxin [see Warnings and Precautions (5.3, 5.4)].
Clonidine: Because milnacipran hydrochloride inhibits norepinephrine reuptake, co-administration with clonidine may inhibit clonidine’s anti-hypertensive effect.
7.7 Drugs that Interfere with Hemostasis
Concomitant use of milnacipran hydrochloride with an antiplatelet or anticoagulant drug (e.g., NSAIDs, aspirin, and warfarin) may potentiate the risk of bleeding. This may be due to the effect of milnacipran hydrochloride on the release of serotonin by platelets. Closely monitor for bleeding for patients receiving an antiplatelet or anticoagulant drug when milnacipran hydrochloride is initiated or discontinued [see Warnings and Precautions (5.9)].
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to milnacipran hydrochloride during pregnancy.
Physicians are advised to recommend that pregnant patients taking milnacipran hydrochloride enroll in the milnacipran hydrochloride Pregnancy Registry. Enrollment is voluntary and may be initiated by pregnant patients or their healthcare providers by contacting the registry at X-XXX-XXX-XXXX or by email at xxxxxxxx@xxxxxx.com. Data forms may also be downloaded from the registry website at www.xxxxxxxxxxxx.com.
Risk Summary
Based on data from published observational studies, exposure to SSRIs, particularly in the month before delivery, has been associated with a less than 2-fold increase in the risk of postpartum hemorrhage [see Warnings and Precautions (5.2)].
The available data on milnacipran hydrochloride use in pregnant women are insufficient to evaluate for a drug associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. There are risks associated with exposure to serotonin and norepinephrine reuptake inhibitors (SNRIs) and selective-serotonin reuptake inhibitors (SSRIs), including milnacipran hydrochloride, during pregnancy (see Clinical Considerations). Animal reproduction studies have been performed in rats, rabbits and mice. Milnacipran was shown to increase embryofetal and perinatal lethality in rats and the incidence of a minor skeletal variation in rabbits at doses below (rat) or approximately equal to (rabbit) the maximum recommended human dose (MRHD) of 200 mg/day on a mg/m2 basis. No effects were seen in mice when treated with milnacipran during the period of organogenesis at doses up to 3 times the MHRD on a mg/m2 basis (see Data).
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Consideration
Maternal adverse reactions
Use of milnacipran hydrochloride in the month before delivery may be associated with an increased risk of postpartum hemorrhage [see Warnings and Precautions (5.9)].
Fetal/Neonatal adverse reactions
Neonates exposed to SNRIs or SSRIs, including milnacipran, late in the third trimester have developed complications requiring prolonged hospitalization, respiratory support, and tube feeding. Such complications can arise immediately upon delivery. Reported clinical findings have included respiratory distress, cyanosis, apnea, seizures, temperature instability, feeding difficulty, vomiting, hypoglycemia, hypotonia, hypertonia, hyperreflexia, tremor, jitteriness, irritability, and constant crying. These findings are consistent with either a direct toxic effect of SSRIs and SNRIs or possibly, a drug discontinuation syndrome. It should be noted that, in some cases, the clinical picture is consistent with serotonin syndrome [see Warnings and Precautions (5.2, 5.7)].
Data
Animal Data
Studies were conducted in rats, rabbits and mice with dosing of milnacipran during the period of organogenesis. In rats, milnacipran was shown to increase embryo fetal lethality at doses of 5 mg/kg/day (0.25 times the MRHD on a mg/m2 basis). In rabbits, dose-dependent increases in the incidence of the skeletal variation of an extra single rib were observed in several pups from multiple litters in the absence of maternal toxicity at 15 mg/kg/day (1.5 times the MRHD on a mg/m2 basis). The clinical significance of this finding is unknown. In mice, no embryotoxic or teratogenic effects were seen at doses up to 125 mg/kg/day (3 times the MRHD on a mg/m2 basis).
With peri- and postnatal exposure to oral milnacipran in rats, decreases in viability and body weight were observed on Postpartum Day 4 at a dose of 5 mg/kg/day (approximately 0.25 times the MRHD on a mg/m2 basis). The no-effect dose for maternal and offspring toxicity was 2.5 mg/kg/day (approximately 0.1 times the MRHD on a mg/m2 basis).
8.2 Lactation
Risk Summary
Milnacipran is present in human milk [see Data]. There are no reports on the effects of milnacipran on the breastfed child and on milk production/excretion. However, there are reports of agitation, irritability, poor feeding, and poor weight gain in infants exposed to SSRIs or SNRIs through breast milk (see Clinical Considerations).
The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for milnacipran and any potential adverse effects on the breastfed child from milnacipran or from the underlying maternal conditions.
Clinical Considerations
Monitor infants exposed to milnacipran for agitation, irritability, poor feeding and poor weight gain.
Data
Human Data
Milnacipran is present in the milk of lactating women treated with milnacipran. In a lactation pharmacokinetic study with milnacipran, a single, oral dose of 50 mg milnacipran hydrochloride tablet was administered to 8 lactating women who were at least 12 weeks postpartum and weaning their infants. The milk/plasma AUC ratio of milnacipran was 1.85 ± 0.38. The maximum estimated weight adjusted daily infant dose for milnacipran from breast milk (assuming mean milk consumption of 150 mL/kg/day) was 5% of the maternal dose based on peak plasma concentrations.
8.4 Pediatric Use
Safety and effectiveness of milnacipran hydrochloride in a fibromyalgia pediatric population below the age of 18 have not been established [see Boxed Warning, Indications and Usage (1), and Warnings and Precautions (5.1)]. The use of milnacipran hydrochloride is not recommended in pediatric patients.
8.5 Geriatric Use
In controlled clinical studies of milnacipran hydrochloride, 402 patients were 60 years or older, and no overall differences in safety and efficacy were observed between these patients and younger patients.
In view of the predominant excretion of unchanged milnacipran via kidneys and the expected decrease in renal function with age, renal function should be considered prior to use of milnacipran hydrochloride in the elderly [see Dosage and Administration (2.2)].
SNRIs, SSRIs, and milnacipran hydrochloride, have been associated with cases of clinically significant hyponatremia in elderly patients, who may be at greater risk for this adverse event [see Warnings and Precautions (5.8)].
-
9 DRUG ABUSE AND DEPENDENCE
9.2 Abuse
Milnacipran did not produce behavioral signs indicative of abuse potential in animal or human studies.
9.3 Dependence
Milnacipran produces physical dependence, as evidenced by the emergence of withdrawal symptoms following drug discontinuation, similar to other SNRIs and SSRIs. These withdrawal symptoms can be severe. Thus, taper milnacipran hydrochloride and do not abruptly discontinue after extended use [see Warnings and Precautions (5.7)].
-
10 OVERDOSAGE
Clinical Presentation
There is limited clinical experience with milnacipran hydrochloride overdose in humans. In clinical trials, cases of acute ingestions up to 1000 mg, alone or in combination with other drugs, were reported with none being fatal.
In post-marketing experience, fatal outcomes have been reported for acute overdoses primarily involving multiple drugs but also with milnacipran hydrochloride only. The most common signs and symptoms included increased blood pressure, cardio-respiratory arrest, changes in the level of consciousness (ranging from somnolence to coma), confusional state, dizziness, and increased hepatic enzymes.
Management of Overdose
There is no specific antidote to milnacipran hydrochloride, but if serotonin syndrome ensues, specific treatment (such as with cyproheptadine and/or temperature control) may be considered. In case of acute overdose, treatment should consist of those general measures employed in the management of overdose with any drug.
Ensure adequate airway, oxygenation, and ventilation and monitor cardiac rhythm and vital signs. Induction of emesis is not recommended. Gastric lavage with a large-bore orogastric tube with appropriate airway protection, if needed, may be indicated if performed soon after ingestion or in symptomatic patients. Because there is no specific antidote for milnacipran hydrochloride, consider symptomatic care and treatment with gastric lavage and activated charcoal as soon as possible for patients who experience a milnacipran hydrochloride overdose.
Due to the large volume of distribution of this drug, forced diuresis, dialysis, hemoperfusion, and exchange transfusion are unlikely to be beneficial.
In managing overdose, consider the possibility of multiple drug involvement. The physician should consider contacting a poison control center for additional information on the treatment of any overdose. Telephone numbers for certified poison control centers are listed in the Physicians’ Desk Reference (PDR).
-
11 DESCRIPTION
Milnacipran hydrochloride is a selective norepinephrine and serotonin reuptake inhibitor; it inhibits norepinephrine uptake with greater potency than serotonin. It is a racemic mixture with the chemical name: (±)-[1R(S),2S(R)]-2-(aminomethyl)-N,N-diethyl-1-phenylcyclopropanecarboxamide hydrochloride. The structural formula is:
Milnacipran hydrochloride is a white to off-white crystalline powder with a melting point of 179°C.
It is freely soluble in water, methanol, ethanol, chloroform, and methylene chloride and sparingly soluble in diethyl ether. It has an empirical formula of C15H23ClN2O and a molecular weight of 282.8 g/mol.
Milnacipran hydrochloride is available for oral administration as film-coated tablets containing 12.5 mg, 25 mg, 50 mg and 100 mg milnacipran hydrochloride. Each tablet also contains carboxymethylcellulose calcium, dibasic calcium phosphate dihydrate, magnesium stearate, povidone, silicon dioxide and talc as inactive ingredients. The film coat contains the following additional inactive ingredients:
12.5 mg:
Erythrosine dye, FD&C Blue #1 Aluminum Lake, hypromellose, polyethylene glycol and titanium dioxide25 mg:
Hypromellose, polyethylene glycol, talc and titanium dioxide50 mg:
Hypromellose, polyethylene glycol, talc and titanium dioxide100 mg:
FD&C Red #40 Aluminum Lake, hypromellose, polyethylene glycol, talc and titanium dioxide -
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
The exact mechanism of the central pain inhibitory action of milnacipran and its ability to improve the symptoms of fibromyalgia in humans are unknown. Preclinical studies have shown that milnacipran is a potent inhibitor of neuronal norepinephrine and serotonin reuptake; milnacipran inhibits norepinephrine uptake with approximately 3-fold higher potency in vitro than serotonin without directly affecting the uptake of dopamine or other neurotransmitters. Milnacipran has no significant affinity for serotonergic (5-HT1-7), α- and β-adrenergic, muscarinic (M1-5), histamine (H1-4), dopamine (D1-5), opiate, benzodiazepine, and γ-aminobutyric acid (GABA) receptors in vitro. Pharmacologic activity at these receptors is hypothesized to be associated with the various anticholinergic, sedative, and cardiovascular effects seen with other psychotropic drugs.
Milnacipran has no significant affinity for Ca++, K+, Na+ and Cl– channels and does not inhibit the activity of human monoamine oxidases (MAO-A and MAO-B) or acetylcholinesterase.
12.2 Pharmacodynamics
Cardiac Electrophysiology
The effect of milnacipran hydrochloride on the QTcF interval was measured in a double-blind placebo-and positive-controlled parallel study in 88 healthy subjects using 600 mg/day milnacipran hydrochloride (3 to 6 times the recommended therapeutic dose for fibromyalgia). After baseline and placebo adjustment, the maximum mean QTcF change was 8 ms (2-sided 90% CI, 3 to 12 ms). This increase is not considered to be clinically significant.
12.3 Pharmacokinetics
Milnacipran is well absorbed after oral administration with an absolute bioavailability of approximately 85% to 90%. The exposure to milnacipran increased proportionally within the therapeutic dose range. It is excreted predominantly unchanged in urine (55%) and has a terminal elimination half-life of about 6 to 8 hours. Steady-state levels are reached within 36 to 48 hours and can be predicted from single-dose data. The active enantiomer, d-milnacipran, has a longer elimination half-life (8 to 10 hours) than the l-enantiomer (4 to 6 hours). There is no interconversion between the enantiomers.
Absorption
Milnacipran hydrochloride is absorbed following oral administration with maximum concentrations (Cmax) reached within 2 to 4 hours post dose. Absorption of milnacipran hydrochloride is not affected by food. The absolute bioavailability is approximately 85% to 90%.
Distribution
The mean volume of distribution of milnacipran following a single intravenous dose to healthy subjects is approximately 400 L.
Plasma protein binding is 13%.
Elimination
Metabolism
Milnacipran and its metabolites are eliminated primarily by renal excretion.
Excretion
Following oral administration of 14C-milnacipran hydrochloride, approximately 55% of the dose was excreted in urine as unchanged milnacipran (24% as l-milnacipran and 31% as d-milnacipran). The l-milnacipran carbamoyl-O-glucuronide was the major metabolite excreted in urine and accounted for approximately 17% of the dose; approximately 2% of the dose was excreted in urine as d-milnacipran carbamoyl-O-glucuronide. Approximately 8% of the dose was excreted in urine as the N-desethyl milnacipran metabolite.
Specific Populations
Geriatric Patients
Cmax and AUC parameters of milnacipran were about 30% higher in elderly (> 65 years) subjects compared with young subjects due to age-related decreases in renal function.
No dosage adjustment is necessary based on age unless renal function is severely impaired [see Dosage and Administration (2.2)].
Male and Female Patients
Cmax and AUC parameters of milnacipran were about 20% higher in female subjects compared with male subjects. Dosage adjustment based on gender is not necessary.
Patients with Renal Impairment
Milnacipran pharmacokinetics were evaluated following single oral administration of 50 mg milnacipran hydrochloride to subjects with mild (creatinine clearance [CLcr] 50 to 80 mL/min), moderate (CLcr 30 to 49 mL/min), and severe (CLcr 5 to 29 mL/min) renal impairment and to healthy subjects (CLcr > 80 mL/min). The mean AUC0-∞ increased by 16%, 52%, and 199%, and terminal elimination half-life increased by 38%, 41%, and 122% in subjects with mild, moderate, and severe renal impairment, respectively, compared with healthy subjects.
No dosage adjustment is necessary for patients with mild renal impairment. Exercise caution in patients with moderate renal impairment. Dose adjustment is necessary in severe renal impairment patients [see Dosage and Administration (2.2)].
Patients with Hepatic Impairment
Milnacipran pharmacokinetics were evaluated following single oral administration of 50 mg milnacipran hydrochloride to subjects with mild (Child-Pugh A), moderate (Child-Pugh B), and severe (Child-Pugh C) hepatic impairment and to healthy subjects. AUC0-∞ and T1/2; were similar in healthy subjects and subjects with mild and moderate hepatic impairment. However, subjects with severe hepatic impairment had a 31% higher AUC0-∞ and a 55% higher T1/2; than healthy subjects. Exercise caution in patients with severe hepatic impairment.
Drug Interaction Studies
In Vitro Studies
In general, milnacipran, at concentrations that were at least 25 times those attained in clinical trials, did not inhibit human CYP1A2, CYP2A6, CYP2C9, CYP2C19, CYP2D6, CYP2E1, and CYP3A4 or induce human CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, and CYP3A4/5 enzyme systems, indicating a low potential of interactions with drugs metabolized by these enzymes.
In vitro studies have shown that the biotransformation rate of milnacipran by human hepatic microsomes and hepatocytes was low. A low biotransformation was also observed following incubation of milnacipran with cDNA-expressed human CYP1A2, CYP2A6, CYP2B6, CYP2C9, CYP2C19, CYP2D6, CYP2E1, and CYP3A4 isozymes.
In Vivo Studies
The drug interaction studies described in this section were conducted in healthy adult subjects.
Carbamazepine - There were no clinically significant changes in the pharmacokinetics of milnacipran following co-administration of milnacipran hydrochloride (100 mg/day) and carbamazepine (200 mg twice a day). No changes were observed in the pharmacokinetics of carbamazepine or its epoxide metabolite due to co-administration with milnacipran hydrochloride.
Clomipramine - Switching from clomipramine (75 mg once a day) to milnacipran (100 mg/day) without a washout period did not lead to clinically significant changes in the pharmacokinetics of milnacipran. Because an increase in adverse events (e.g., euphoria and postural hypotension) was observed after switching from clomipramine to milnacipran, monitoring of patients during treatment switch is recommended.
Digoxin - There was no pharmacokinetic interaction between milnacipran hydrochloride (200 mg/day) and digoxin (0.2 mg/day Lanoxicaps) following multiple-dose administration to healthy subjects.
Fluoxetine - Switching from fluoxetine (20 mg once a day), a strong inhibitor of CYP2D6 and a moderate inhibitor of CYP2C19, to milnacipran (100 mg/day) without a washout period did not affect the pharmacokinetics of milnacipran.
Lithium - Multiple doses of milnacipran hydrochloride (100 mg/day) did not affect the pharmacokinetics of lithium.
Lorazepam - There was no pharmacokinetic interaction between a single dose of milnacipran hydrochloride (50 mg) and lorazepam (1.5 mg).
Pregabalin - There were no clinically significant changes in the steady-state pharmacokinetics of milnacipran or pregabalin following twice a day co-administration of 50 mg milnacipran and 150 mg pregabalin.
Warfarin - Steady-state milnacipran (200 mg/day) did not affect the pharmacokinetics of R-warfarin and S-warfarin or the pharmacodynamics (as assessed by measurement of prothrombin INR) of a single dose of 25 mg warfarin. The pharmacokinetics of milnacipran hydrochloride were not altered by warfarin.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Dietary administration of milnacipran to rats at doses of 50 mg/kg/day (2 times the MRHD on a mg/m2 basis) for 2 years caused a statistically significant increase in the incidence of thyroid C-cell adenomas and combined adenomas and carcinomas in males. A carcinogenicity study was conducted in Tg.rasH2 mice for 6 months at oral gavage doses of up to 125 mg/kg/day.
Milnacipran did not induce tumors in Tg.rasH2 mice at any dose tested.
Mutagenesis
Milnacipran was not mutagenic in the in vitro bacterial reverse mutation assay (Ames test) or in the L5178Y TK +/-mouse lymphoma forward mutation assay. Milnacipran was also not clastogenic in an in vitro chromosomal aberration test in human lymphocytes or in the in vivo mouse micronucleus assay.
Impairment of Fertility
Although administration of milnacipran to male and female rats had no statistically significant effect on mating or fertility at doses up to 80 mg/kg/day (4 times the MRHD on an mg/m2 basis), there was an apparent dose-related decrease in the fertility index at clinically relevant doses based on body surface area.
13.2 Animal Toxicology and/or Pharmacology
Hepatic Effects
Chronic administration (2 years) of milnacipran to rats at 15 mg/kg (0.6 times the MRHD on an mg/m2 basis) and higher doses showed increased incidences of centrilobular vacuolation of the liver in male rats and eosinophilic foci in male and female rats in the absence of any change in hepatic enzymes. The clinical significance of the finding is not known. Chronic (1 year) administration in the primate at doses up to 25 mg/kg (2 times the MRHD on a mg/m2 basis) did not demonstrate similar evidence of hepatic changes.
Ocular Effects
Chronic (2 years) administration of milnacipran to rats at 15 mg/kg (0.6 times the MRHD on a mg/m2 basis) and higher doses showed increased incidence of keratitis of the eye. One-year studies in the rat and primate did not show this response.
-
14 CLINICAL STUDIES
Management of Fibromyalgia
The efficacy of milnacipran hydrochloride for the management of fibromyalgia was established in two double-blind, placebo-controlled, multicenter studies in adult patients (18 to 74 years of age). Enrolled patients met the American College of Rheumatology (ACR) criteria for fibromyalgia (a history of widespread pain for 3 months and pain present at 11 or more of the 18 specific tender point sites). Approximately 35% of patients had a history of depression. Study 1 was six months in duration and Study 2 was three months in duration.
A larger proportion of patients treated with milnacipran hydrochloride than with placebo experienced a simultaneous reduction in pain from baseline of at least 30% (VAS) and also rated themselves as much improved or very much improved based on the patient global assessment (PGIC). In addition, a larger proportion of patients treated with milnacipran hydrochloride met the criteria for treatment response, as measured by the composite endpoint that concurrently evaluated improvement in pain (VAS), physical function (SF-36 PCS), and patient global assessment (PGIC), in fibromyalgia as compared to placebo.
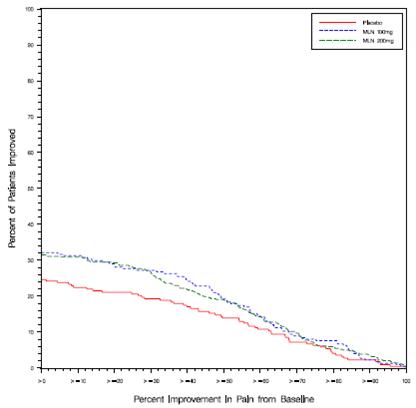
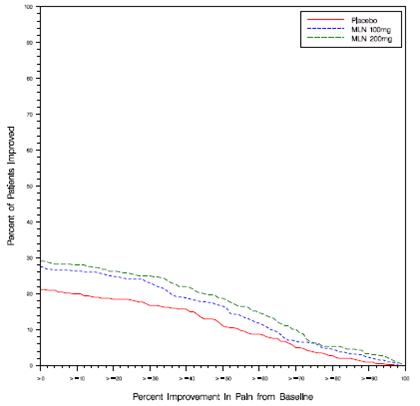
Study 1: This 6-month study compared total daily doses of milnacipran hydrochloride 100 mg and 200 mg to placebo. Patients were enrolled with a minimum mean baseline pain score of ≥ 50 mm on a 100 mm visual analog scale (VAS) ranging from 0 (“no pain”) to 100 (“worst possible pain”). The mean baseline pain score in this trial was 69. The efficacy results for Study 1 are summarized in Figure 1.
Figure 1 shows the proportion of patients achieving various degrees of improvement in pain from baseline to the 3-month time point and who concurrently rated themselves globally improved (PGIC score of 1 or 2). Patients who did not complete the 3-month assessment were assigned 0% improvement. More patients in the milnacipran hydrochloride treatment arms experienced at least a 30% reduction in pain from baseline (VAS) and considered themselves globally improved (PGIC) than did patients in the placebo arm. Treatment with milnacipran hydrochloride 200 mg/day did not confer greater benefit than treatment with milnacipran hydrochloride 100 mg/day.
Figure 1: Patients Achieving Various Levels of Pain Relief with Concurrent Ratings of Being Much or Very Much Improved on the PGIC - Study 1
Study 2: This 3-month study compared total daily doses of milnacipran hydrochloride 100 mg and 200 mg to placebo. Patients were enrolled with a minimum mean baseline pain score of ≥ 40 mm on a 100-mm VAS ranging from 0 (“no pain”) to 100 (“worst possible pain”). The mean baseline pain score in this trial was 65. The efficacy results for Study 2 are summarized in Figure 2.
Figure 2 shows the proportion of patients achieving various degrees of improvement in pain from baseline to the 3-month time point and who concurrently rated themselves globally improved (PGIC score of 1 or 2). Patients who did not complete the 3-month assessment were assigned 0% improvement. More patients in the milnacipran hydrochloride treatment arms experienced at least a 30% reduction in pain from baseline (VAS) and considered themselves globally improved (PGIC) than did patients in the placebo arm. Treatment with milnacipran hydrochloride 200 mg/day did not confer greater benefit than treatment with milnacipran hydrochloride 100 mg/day.
Figure 2: Patients Achieving Various Levels of Pain Relief with Concurrent Ratings of Being Much or Very Much Improved on the PGIC - Study 2
In both studies, some patients who rated themselves as globally “much” or “very much” improved experienced a decrease in pain as early as week 1 of treatment with a stable dose of milnacipran hydrochloride that persisted throughout these studies.
-
16 HOW SUPPLIED/STORAGE AND HANDLING
Milnacipran hydrochloride tablets, 12.5 mg are supplied as blue color, round shaped, biconvex, film-coated tablets, debossed with “AN” on one side and “091” on the other side.
Bottles of 60: NDC 65162-091-06
Milnacipran hydrochloride tablets, 25 mg are supplied as white to off-white, round shaped, biconvex, film-coated tablets, debossed with “AN” on one side and “092” on the other side.
Bottles of 60: NDC 65162-092-06
Milnacipran hydrochloride tablets, 50 mg are supplied as white to off-white, oval-shaped, biconvex, film-coated tablets, debossed with “AN” on one side and “093” on the other side.
Bottles of 60: NDC 65162-093-06
Bottles of 500: NDC 65162-093-50
Milnacipran hydrochloride tablets, 100 mg are supplied as pink color, oval-shaped, biconvex, film-coated tablets, debossed with “AN” on one side and “094” on the other side.
Bottles of 60: NDC 65162-094-06
Bottles of 500: NDC 65162-094-50
Storage
Store at 20° to 25°C (68° to 77°F); excursions permitted between 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature].
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Advise patients of the following issues and to alert their prescriber if these occur while taking milnacipran hydrochloride:
Clinical Worsening and Suicide Risk
Advise patients, their families, and their caregivers that patients with depression may be at increased risk for clinical worsening and/or suicidal ideation if they stop taking anti-depressant medication, change the dose, or start a new medication.
Encourage patients, their families, and their caregivers to be alert to the emergence of anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania, or other unusual changes in behavior, worsening of depression, and suicidal ideation, especially early during treatment with milnacipran hydrochloride or other drugs that inhibit the reuptake of norepinephrine and/or serotonin, and when the dose is adjusted up or down. Advise families and caregivers to observe for the emergence of such symptoms on a day-to-day basis, since changes may be abrupt and to report such symptoms to the patient’s prescriber or health professional, especially if they are severe, abrupt in onset, or were not part of the patient’s presenting symptoms [see Boxed Warning and Warnings and Precautions (5.1)].
Serotonin Syndrome
Inform patients about the risk of serotonin syndrome with use of milnacipran hydrochloride as well as the increased risk when taken concomitantly with other serotonergic drugs including triptans, tricyclic antidepressants, opioids, lithium, tryptophan, buspirone, amphetamines and St. John’s Wort, and with drugs that impair metabolism of serotonin (in particular MAOIs, both those intended to treat psychiatric disorders and also others, such as linezolid) [see Warnings and Precautions (5.2), Drug Interactions (7.2)].
Advise patients of the signs and symptoms associated with serotonin syndrome and to seek medical care immediately if they experience these symptoms.
Elevated Blood Pressure and Heart Rate
Advise patients that milnacipran hydrochloride may increase their blood pressure and heart rate and that they should have their blood pressure and heart rate monitored at regular intervals when receiving treatment with milnacipran hydrochloride [see Warnings and Precautions (5.3, 5.4)].
Increased Risk of Bleeding
Advise patients that the concomitant use of drugs that interfere with serotonin reuptake, including milnacipran hydrochloride, and NSAIDs, aspirin, or anticoagulants has been associated with an increased risk of abnormal bleeding [see Warnings and Precautions (5.9)].
Angle Closure Glaucoma
Advise patients that taking milnacipran hydrochloride can cause mild pupillary dilation which, in susceptible individuals, can lead to an episode of angle closure glaucoma [see Warnings and Precautions (5.13)].
Ability to Drive and Use Machinery
Advise patients not to operate machinery or drive motor vehicles until they are reasonably certain that milnacipran hydrochloride treatment does not affect their ability to engage in such activities.
Alcohol
Inform patients of the risks associated with drinking alcohol while taking milnacipran hydrochloride [see Warnings and Precautions (5.6, 5.14)].
Sexual Dysfunction
Advise patients that use of milnacipran hydrochloride may cause symptoms of sexual dysfunction in both male and female patients. Inform patients that they should discuss any changes in sexual function and potential management strategies with their healthcare provider [see Warnings and Precautions (5.12)].
Discontinuation
Advise patients that withdrawal symptoms can occur when discontinuing treatment with milnacipran hydrochloride, particularly when discontinuation is abrupt [see Warnings and Precautions (5.7)].
Missing a Dose
Advise patients that if they miss a dose, they should skip the missed dose and take the next dose at their regular time.
Pregnancy Registry
Advise patients that there is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to milnacipran hydrochloride during pregnancy [see Use in Specific Populations (8.1)].
Pregnancy
- Advise pregnant women to notify their healthcare provider if they become pregnant or intend to become pregnant during treatment with milnacipran hydrochloride.
- Advise patients that milnacipran hydrochloride may increase the risk of neonatal complications requiring prolonged hospitalization, respiratory support, and tube feeding.
Lactation
Advise breastfeeding women using milnacipran to monitor infants for sedation, agitation, irritability, poor feeding, and poor weight gain and to seek medical care if they notice these signs [see Use in Specific Populations (8.2)].
Manufactured by:
Amneal Pharmaceuticals Pvt. Ltd.
Ahmedabad 382220, INDIADistributed by:
Amneal Pharmaceuticals LLC
Bridgewater, NJ 08807Rev. 03-2024-05
-
MEDICATION GUIDE
FDA-Approved Medication Guide
Milnacipran Hydrochloride (mil naʹ si pran hyeʺ droe klorʹ ide) Tablets
Milnacipran hydrochloride tablets are not used to treat depression, but it acts like medicines that are used to treat depression (antidepressants) and other psychiatric disorders.
Read the Medication Guide that comes with milnacipran hydrochloride tablets before you start taking it and each time you get a refill. There may be new information. This Medication Guide does not take the place of talking to your healthcare provider about your medical condition or treatment. Talk with your healthcare provider if there is something you do not understand or want to learn more about.
What is the most important information I should know about milnacipran hydrochloride tablets?
Milnacipran hydrochloride tablets and antidepressant medicines may cause serious side effects, including:
1. Suicidal thoughts or actions:
- Milnacipran hydrochloride tablets and antidepressant medicines may increase suicidal thoughts or actions in some children, teenagers, and young adults within the first few months of treatment or when the dose is changed.
- Depression or other serious mental illnesses are the most important causes of suicidal thoughts or actions. Watch for these changes and call your healthcare provider right away if you notice:
- New or sudden changes, in mood, behavior, thoughts, or feelings, especially if severe.
- Pay particular attention to such changes when milnacipran hydrochloride tablets are started or when the dose is changed.
- Keep all follow-up visits with your healthcare provider and call between visits if you are worried about symptoms.
Call your healthcare provider right away or go to the nearest hospital emergency room if you have any of the following symptoms, especially if they are new, worse, or worry you:
- attempts to commit suicide
- acting on dangerous impulses
- acting aggressive, being angry, or violent
- thoughts about suicide or dying
- new or worse depression
- new or worse anxiety or panic attacks
- feeling agitated, restless, angry or irritable
- trouble sleeping (insomnia)
- an increase in activity or talking more than what is normal for you
- other unusual changes in behavior or mood
Call your healthcare provider right away or go to the nearest hospital emergency room if you have any symptoms of the serious side effects listed below:
2. Serotonin Syndrome. This condition can be life-threatening, symptoms may include:
- agitation, hallucinations, coma or other changes in mental status
- coordination problems or muscle twitching (overactive reflexes)
- sweating or fever
- diarrhea
- muscle rigidity
- dizziness
- tremor
Symptoms such as racing heartbeat, high or low blood pressure, nausea, vomiting, and flushing are common with milnacipran hydrochloride tablets. Call your healthcare provider right away if you get these symptoms and they are severe or if they happen with any of the symptoms of serotonin syndrome listed above.
3. Increase in blood pressure or heart rate: Milnacipran hydrochloride tablets may increase your blood pressure or heart rate. Check your blood pressure and heart rate before you start and during treatment with milnacipran hydrochloride tablets. Before taking milnacipran hydrochloride tablets, tell your healthcare provider if you have high blood pressure or problems with your heart or blood vessels (cardiovascular disease).
4. Seizures or convulsions.
5. Liver problems. Symptoms of liver problems may include:
- itching
- right upper abdominal pain
- dark urine
- yellowing of your skin or eyes
- enlarged liver
- increased liver enzymes
6. Low salt (sodium) levels in the blood. Elderly people may be at greater risk for this. Symptoms may include:
- headache
- weakness or feeling unsteady
- confusion, problems concentrating or thinking or memory problems
7. Abnormal bleeding: Milnacipran hydrochloride tablets and other similar medicines (antidepressants) may increase your risk of bleeding or bruising, especially if you take the blood thinner warfarin (Coumadin, Jantoven), a nonsteroidal anti-inflammatory drug (NSAID), or aspirin.
8. Manic episodes
- greatly increased energy
- severe trouble sleeping
- racing thoughts
- reckless behavior
- unusually grand ideas
- excessive happiness or irritability
- talking more or faster than usual
9. Problems with urination
- decreased urine flow
- unable to pass any urine
Men may be more likely to have these symptoms, and may develop pain in their testicles or have problems with ejaculation.
10. Visual problems
- eye pain
- changes in vision
- swelling or redness in or around eye
Only some people are at risk for these problems. You may want to undergo an eye examination to see if you are at risk and receive preventative treatment if you are.
11. Sexual problems (dysfunction). Taking serotonin and norepinephrine reuptake inhibitors (SNRIs), including milnacipran hydrochloride, may cause sexual problems.
Symptoms in males may include
- Delayed ejaculation or inability to have an ejaculation
- Decreased sex drive
- Problems getting or keeping an erection
Symptoms in females may include
- Decreased sex drive
- Delayed orgasm or inability to have an orgasm
Talk to your healthcare provider if you develop any changes in your sexual function or if you have any questions or concerns about sexual problems during treatment with milnacipran hydrochloride. There may be treatments your healthcare provider can suggest.
Do not stop milnacipran hydrochloride tablets without first talking to your healthcare provider.
Stopping milnacipran hydrochloride tablets too quickly may cause symptoms, some serious, including:
- anxiety, irritability, or confusion
- feeling tired or problems sleeping
- headache, dizziness, seizures
- electric shock-like sensations, ringing in ears
What are milnacipran hydrochloride tablets?
Milnacipran hydrochloride tablets are prescription medicine used to manage fibromyalgia. It is important to talk with your healthcare provider about the risks of treating fibromyalgia and also the risks of not treating it. You should discuss all treatment choices with your healthcare provider.
It is not known if milnacipran hydrochloride tablets are safe and effective in children.
Who should not take milnacipran hydrochloride tablets?
Do not take milnacipran hydrochloride tablets if you:
-
take a Monoamine Oxidase Inhibitor (MAOI). Ask your healthcare provider or pharmacist if you are not sure if you take an MAOI, including the antibiotic linezolid.
- Do not take an MAOI within 5 days of stopping milnacipran hydrochloride tablets unless your healthcare provider tells you to.
- Do not start milnacipran hydrochloride tablets if you stopped taking an MAOI in the last 14 days unless your healthcare provider tells you to.
-
People who take milnacipran hydrochloride tablets close in time to an MAOI may have serious or even life-threatening side effects. Get medical help right away if you have any of these symptoms:
- high fever
- uncontrolled muscle spasms
- stiff muscles
- rapid changes in heart rate or blood pressure
- confusion
- loss of consciousness (pass out)
What should I tell my healthcare provider before taking milnacipran hydrochloride tablets?
Before starting milnacipran hydrochloride tablets, tell your healthcare provider if you:
- have heart problems or high blood pressure
- have liver problems
- have kidney problems
- have or had seizures or convulsions
- have bipolar disorder or mania
- have low sodium levels in your blood
- have or had bleeding problems
- drink alcohol. Talk to your healthcare provider about how often and how much alcohol you drink.
- have any other medical conditions
- are pregnant or plan to become pregnant. It is not known if milnacipran hydrochloride tablets will harm your unborn baby.
Pregnancy registry: There is a pregnancy registry for women who take milnacipran hydrochloride during pregnancy. The purpose of the registry is to collect information about the health of you and your baby. You may talk to your healthcare provider about how you can take part in this registry, or you may call the Registry directly at X-XXX-XXX-XXXX or go to www.XXXXXXXXXXXXX.com.
- are breastfeeding or plan to breastfeed. Milnacipran hydrochloride can pass into your breast milk and may harm your baby. Talk to your healthcare provider about the best way to feed your baby while taking milnacipran hydrochloride tablets.
Tell your healthcare provider about all the medicines that you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. Milnacipran hydrochloride tablets and some medicines may interact with each other, may not work as well, or may cause serious side effects.
Especially tell your healthcare provider if you take:
- triptans used to treat migraine headache
- medicines used to treat mood, anxiety, psychotic or thought disorders, including tricyclics, lithium, buspirone, SSRIs, SNRIs or MAOIs
- tramadol, fentanyl, meperidine, methadone, or other opioids
- amphetamines
- the blood thinner warfarin (Coumadin, Jantoven)
- non-steroidal anti-inflammatory drug (NSAID) (like ibuprofen, naproxen or aspirin)
- over-the-counter supplements such as tryptophan or St. John’s Wort
Ask your healthcare provider for a list of these medicines if you are not sure.
Your healthcare provider or pharmacist can tell you if it is safe to take milnacipran hydrochloride tablets with your other medicines. Do not start or stop any medicine while taking milnacipran hydrochloride tablets without talking to your healthcare provider first.
How should I take milnacipran hydrochloride tablets?
- Take milnacipran hydrochloride tablets exactly as your healthcare provider tells you.
- Your healthcare provider will slowly increase your dose to find the dose that is right for you.
- On the first day of treatment, you will take 1 dose of milnacipran hydrochloride tablets as prescribed.
- After your first dose, your healthcare provider will tell you how much milnacipran hydrochloride tablets to take and when to take it, usually 2 times each day.
- You may take milnacipran hydrochloride tablets with or without food. Taking milnacipran hydrochloride tablets with food may help you tolerate it better.
- If you miss a dose, skip the missed dose and take the next dose at your regular time.
- Tell your healthcare provider if you feel that your condition is not improving during treatment with milnacipran hydrochloride tablets.
- If you take too much milnacipran hydrochloride tablets, call your healthcare provider or go to the nearest hospital emergency room right away.
What should I avoid while taking milnacipran hydrochloride tablets?
- Do not drive or operate machinery until you know how milnacipran hydrochloride tablets affect you. Milnacipran hydrochloride tablets may make you less alert and affect your reaction time.
What are the possible side effects of milnacipran hydrochloride tablets?
Milnacipran hydrochloride tablets may cause side effects, some serious, including:
- See “What is the most important information I should know about milnacipran hydrochloride tablets?”
The most common side effects of milnacipran hydrochloride tablets include:
- nausea
- headache
- constipation
- dizziness
- trouble sleeping
- hot flush
- increased sweating
- vomiting
- irregular heartbeat (palpitations)
- heart rate increased
- dry mouth
- high blood pressure (hypertension)
Tell your healthcare provider if you have any side effect that bothers you or that does not go away.
These are not all the possible side effects of milnacipran hydrochloride tablets. For more information, ask your healthcare provider or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store milnacipran hydrochloride tablets?
- Store at room temperature 20° to 25°C (68° to 77°F); excursions permitted between 15° to 30°C (59° to 86°F).
Keep milnacipran hydrochloride tablets and all medicines out of the reach of children.
General information about the safe and effective use of milnacipran hydrochloride tablets
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use milnacipran hydrochloride tablets for a condition for which it was not prescribed. Do not give milnacipran hydrochloride tablets to other people, even if they have the same condition. It may harm them.
You may ask your healthcare provider or pharmacist for information about milnacipran hydrochloride tablets that is written for health professionals.
For more information call 1-877-835-5472 or go to www.amneal.com.
What are the ingredients in milnacipran hydrochloride tablets?
Active ingredient: milnacipran hydrochloride
Inactive ingredients: carboxymethylcellulose calcium, dibasic calcium phosphate dihydrate, magnesium stearate, povidone, silicon dioxide and talc.
The film coat contains the inactive ingredients:
12.5 mg tablets: Erythrosine dye, FD&C Blue #1 Aluminum Lake, hypromellose, polyethylene glycol and titanium dioxide
25 mg tablets: Hypromellose, polyethylene glycol, talc and titanium dioxide
50 mg tablets: Hypromellose, polyethylene glycol, talc and titanium dioxide
100 mg tablets: FD&C Red #40 Aluminum Lake, hypromellose, polyethylene glycol, talc and titanium dioxide
This Medication Guide has been approved by the U.S. Food and Drug Administration.
*All trademarks are the property of their respective owners.
Manufactured by:
Amneal Pharmaceuticals Pvt. Ltd.
Ahmedabad 382220, INDIADistributed by:
Amneal Pharmaceuticals LLC
Bridgewater, NJ 08807Rev. 03-2024-05
Dispense with Medication Guide available at:
documents.amneal.com/mg/milnacipran-hcl.pdf
-
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
NDC 65162-091-06
Milnacipran Hydrochloride tablets, 12.5 mg
Rx only
60 Tablets
Amneal Pharmaceuticals LLC
NDC 65162-092-06
Milnacipran Hydrochloride tablets, 25 mg
Rx only
60 Tablets
Amneal Pharmaceuticals LLC
-
INGREDIENTS AND APPEARANCE
MILNACIPRAN HCL
milnacipran hcl tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:65162-091 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength MILNACIPRAN HYDROCHLORIDE (UNII: RNZ43O5WW5) (MILNACIPRAN - UNII:G56VK1HF36) MILNACIPRAN HYDROCHLORIDE 12.5 mg Inactive Ingredients Ingredient Name Strength CARBOXYMETHYLCELLULOSE CALCIUM (UNII: UTY7PDF93L) CALCIUM PHOSPHATE, DIBASIC, DIHYDRATE (UNII: O7TSZ97GEP) MAGNESIUM STEARATE (UNII: 70097M6I30) POVIDONE (UNII: FZ989GH94E) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) TALC (UNII: 7SEV7J4R1U) FD&C RED NO. 3 (UNII: PN2ZH5LOQY) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) HYPROMELLOSES (UNII: 3NXW29V3WO) POLYETHYLENE GLYCOL, UNSPECIFIED (UNII: 3WJQ0SDW1A) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color blue Score no score Shape ROUND Size 5mm Flavor Imprint Code AN;091 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:65162-091-06 60 in 1 BOTTLE; Type 0: Not a Combination Product 01/31/2014 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA205081 01/31/2014 MILNACIPRAN HCL
milnacipran hcl tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:65162-092 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength MILNACIPRAN HYDROCHLORIDE (UNII: RNZ43O5WW5) (MILNACIPRAN - UNII:G56VK1HF36) MILNACIPRAN HYDROCHLORIDE 25 mg Inactive Ingredients Ingredient Name Strength CARBOXYMETHYLCELLULOSE CALCIUM (UNII: UTY7PDF93L) CALCIUM PHOSPHATE, DIBASIC, DIHYDRATE (UNII: O7TSZ97GEP) MAGNESIUM STEARATE (UNII: 70097M6I30) POVIDONE (UNII: FZ989GH94E) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) TALC (UNII: 7SEV7J4R1U) HYPROMELLOSES (UNII: 3NXW29V3WO) POLYETHYLENE GLYCOL, UNSPECIFIED (UNII: 3WJQ0SDW1A) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color white (off-white) Score no score Shape ROUND Size 6mm Flavor Imprint Code AN;092 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:65162-092-06 60 in 1 BOTTLE; Type 0: Not a Combination Product 01/31/2014 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA205081 01/31/2014 MILNACIPRAN HCL
milnacipran hcl tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:65162-093 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength MILNACIPRAN HYDROCHLORIDE (UNII: RNZ43O5WW5) (MILNACIPRAN - UNII:G56VK1HF36) MILNACIPRAN HYDROCHLORIDE 50 mg Inactive Ingredients Ingredient Name Strength CARBOXYMETHYLCELLULOSE CALCIUM (UNII: UTY7PDF93L) CALCIUM PHOSPHATE, DIBASIC, DIHYDRATE (UNII: O7TSZ97GEP) MAGNESIUM STEARATE (UNII: 70097M6I30) POVIDONE (UNII: FZ989GH94E) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) TALC (UNII: 7SEV7J4R1U) HYPROMELLOSES (UNII: 3NXW29V3WO) POLYETHYLENE GLYCOL, UNSPECIFIED (UNII: 3WJQ0SDW1A) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color white (off-white) Score no score Shape OVAL Size 11mm Flavor Imprint Code AN;093 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:65162-093-06 60 in 1 BOTTLE; Type 0: Not a Combination Product 01/31/2014 2 NDC:65162-093-50 500 in 1 BOTTLE; Type 0: Not a Combination Product 01/31/2014 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA205081 01/31/2014 MILNACIPRAN HCL
milnacipran hcl tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:65162-094 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength MILNACIPRAN HYDROCHLORIDE (UNII: RNZ43O5WW5) (MILNACIPRAN - UNII:G56VK1HF36) MILNACIPRAN HYDROCHLORIDE 100 mg Inactive Ingredients Ingredient Name Strength CARBOXYMETHYLCELLULOSE CALCIUM (UNII: UTY7PDF93L) CALCIUM PHOSPHATE, DIBASIC, DIHYDRATE (UNII: O7TSZ97GEP) MAGNESIUM STEARATE (UNII: 70097M6I30) POVIDONE (UNII: FZ989GH94E) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) TALC (UNII: 7SEV7J4R1U) HYPROMELLOSES (UNII: 3NXW29V3WO) POLYETHYLENE GLYCOL, UNSPECIFIED (UNII: 3WJQ0SDW1A) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FD&C RED NO. 40 (UNII: WZB9127XOA) Product Characteristics Color pink Score no score Shape OVAL Size 13mm Flavor Imprint Code AN;094 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:65162-094-06 60 in 1 BOTTLE; Type 0: Not a Combination Product 01/31/2014 2 NDC:65162-094-50 500 in 1 BOTTLE; Type 0: Not a Combination Product 01/31/2014 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA205081 01/31/2014 Labeler - Amneal Pharmaceuticals LLC (123797875) Establishment Name Address ID/FEI Business Operations Amneal Pharmaceuticals Private Limited 915076126 analysis(65162-091, 65162-092, 65162-093, 65162-094) , label(65162-091, 65162-092, 65162-093, 65162-094) , manufacture(65162-091, 65162-092, 65162-093, 65162-094) , pack(65162-091, 65162-092, 65162-093, 65162-094)