Label: CALCITRIOL injection

- NDC Code(s): 68083-316-10
- Packager: Gland Pharma Limited
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: Abbreviated New Drug Application
Drug Label Information
Updated October 10, 2022
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
DESCRIPTION
Calcitriol injection is synthetically manufactured calcitriol and is available as a sterile, isotonic, clear, colorless to yellow, aqueous solution for intravenous injection. Calcitriol Injection, USP is available in 1 mL vials. Each 1 mL contains: Active: Calcitriol, 1 mcg. Inactives: Polysorbate 20, 4 mg; Dibasic Sodium Phosphate, Anhydrous 7.6 mg; Edetate Disodium, Dihydrate 1.1 mg; Monobasic Sodium Phosphate, Monohydrate 1.8 mg; Butylated hydroxyltoluene 0.02 mg; Butylated hydroxyl anisole 0.003 mg; Sodium Chloride 1.5 mg; pH Range is from 6.5 to 8.0 and Water for Injection.
Calcitriol is a crystalline compound which occurs naturally in humans. It is soluble in organic solvents but relatively insoluble in water. Calcitriol is chemically designated (5Z,7E)-9,10 secocholesta-5,7,10(19)-triene-1α,3β,25-triol and has the following structural formula:
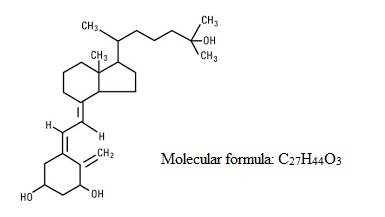
The other names frequently used for calcitriol are 1α,25-dihydroxycholecalciferol,1α,25- dihydroxyvitamin D3,1,25-DHCC,1,25(OH)2D3 and 1,25-diOHC.
-
CLINICAL PHARMACOLOGY
Calcitriol is the active form of vitamin D3 (cholecalciferol). The natural or endogenous supply of vitamin D in man mainly depends on ultraviolet light for conversion of 7-dehydrocholesterol to vitamin D3 in the skin. Vitamin D3 must be metabolically activated in the liver and the kidney before it is fully active on its target tissues. The initial transformation is catalyzed by a vitamin D3-25-hydroxylase enzyme present in the liver, and the product of this reaction is 25-(OH)D3(calcifediol). The latter undergoes hydroxylation in the mitochondria of kidney tissue, and this reaction is activated by the renal 25-hydroxyvitamin D3-1-α-hydroxylase to produce 1,25-(OH)2D3 (calcitriol), the active form of vitamin D3.
The known sites of action of calcitriol are intestine, bone, kidney and parathyroid gland. Calcitriol is the most active known form of vitamin D3 in stimulating intestinal calcium transport. In acutely uremic rats, calcitriol has been shown to stimulate intestinal calcium absorption. In bone, calcitriol, in conjunction with parathyroid hormone, stimulates resorption of calcium; and in the kidney, calcitriol increases the tubular reabsorption of calcium. In vitro and in vivo studies have shown that calcitriol directly suppresses secretion and synthesis of PTH. A vitamin D-resistant state may exist in uremic patients because of the failure of the kidney to adequately convert precursors to the active compound, calcitriol. Calcitriol when administered by bolus injection is rapidly available in the blood stream. Vitamin D metabolites are known to be transported in blood, bound to specific plasma proteins. The pharmacologic activity of an administered dose of calcitriol is about 3 to 5 days. Two metabolic pathways for calcitriol have been identified, conversion to 1,24,25-(OH)3D3 and to calcitroic acid.
- INDICATIONS AND USAGE
- CONTRAINDICATIONS
-
WARNINGS
Since calcitriol is the most potent metabolite of vitamin D available, prescription-based doses of vitamin D and its derivatives should be withheld or used with caution during treatment to avoid the risk of hypercalcemia.
A non-aluminum phosphate-binding compound should be used to control serum phosphorous levels in patients undergoing dialysis.
Overdosage of any form of vitamin D is dangerous (see also OVERDOSAGE). Progressive hypercalcemia due to overdosage of vitamin D and its metabolites may be so severe as to require emergency attention. Chronic hypercalcemia can lead to generalized vascular calcification, nephrocalcinosis and other soft tissue calcification. The serum calcium times phosphate (Ca x P) product should not be allowed to exceed 70 mg2/dL2. Radiographic evaluation of suspect anatomical regions may be useful in the early detection of this condition.
-
PRECAUTIONS
General
Excessive dosage of calcitriol injection induces hypercalcemia and in some instances hypercalciuria; therefore, early in treatment during dosage adjustment, serum calcium and phosphorus should be determined at least twice weekly. Should hypercalcemia develop, the drug should be discontinued immediately.
Calcitriol injection should be given cautiously to patients on digitalis, because hypercalcemia in such patients may precipitate cardiac arrhythmias.
Information for the Patient
The patient and his or her parents should be informed about adherence to instructions about diet and calcium supplementation and avoidance of the use of unapproved non-prescription drugs, including magnesium-containing antacids. Patients should also be carefully informed about the symptoms of hypercalcemia (see ADVERSE REACTIONS).
Essential Laboratory Tests
Serum calcium, phosphorus, magnesium and alkaline phosphatase and 24-hour urinary calcium and phosphorus should be determined periodically. During the initial phase of the medication, serum calcium and phosphorus should be determined more frequently (twice weekly).
Adynamic bone disease may develop if PTH levels are suppressed to abnormal levels. If biopsy is not being done for other (diagnostic) reasons, PTH levels may be used to indicate the rate of bone turnover. If PTH levels fall below recommended target range (1.5 to 3 times the upper limit of normal), in patients treated with calcitriol injection, the calcitriol injection dose should be reduced or therapy discontinued. Discontinuation of calcitriol therapy may result in rebound effect, therefore, appropriate titration downward to a maintenance dose is recommended.
Drug Interactions
Concomitant use of magnesium-containing preparations should be used with caution or avoided since such use may lead to the development of hypermagnesemia.
Corticosteroids with glucocorticoid activity may counteract the bone and mineral metabolism effects of vitamin D analogues.
Cytochrome P450 enzyme-inducing anticonvulsants such as carbamazepine, phenobarbital and phenytoin may reduce the effects of vitamin D because they increase vitamin D catabolism.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term studies in animals have not been conducted to evaluate the carcinogenic potential of calcitriol injection. Calcitriol was not mutagenic in vitro in the Ames Test nor was oral calcitriol genotoxic in vivo in the Mouse Micronucleus Test. No significant effects on fertility and/or general reproductive performances were observed in a Segment I study in rats using oral calcitriol at doses of up to 0.3 mcg/kg.
Pregnancy
Teratogenic Effects
Pregnancy Category C
Calcitriol has been found to be teratogenic in rabbits when given orally at doses of 0.08 and 0.3 mcg/kg. All 15 fetuses in 3 litters at these doses showed external and skeletal abnormalities. However, none of the other 23 litters (156 fetuses) showed external and skeletal abnormalities compared with controls. Teratogenicity studies in rats at doses up to 0.45 mcg/kg orally showed no evidence of teratogenic potential. There are no adequate and well-controlled studies in pregnant women. Calcitriol injection should be used during pregnancy only if the potential benefits justifies the potential risk to the fetus.
Nonteratogenic Effects
In the rabbit, oral dosages of 0.3 mcg/kg/day administered on days 7 to 18 of gestation resulted in 19% maternal mortality, a decrease in mean fetal body weight and a reduced number of newborns surviving to 24 hours. A study of the effects on orally administered calcitriol on peri- and postnatal development in rats resulted in hypercalcemia in the offspring of dams given calcitriol at doses of 0.08 or 0.3 mcg/kg/day, hypercalcemia and hypophosphatemia in dams given calcitriol at a dose of 0.08 or 0.3 mcg/kg/day and increased serum urea nitrogen in dams given calcitriol at a dose of 0.3 mcg/kg/day. In another study in rats, maternal weight gain was slightly reduced at an oral dose of 0.3 mcg/kg/day administered on days 7 to 15 of gestation.
The offspring of a woman administered oral calcitriol at 17 to 36 mcg/day during pregnancy manifested mild hypercalcemia in the first 2 days of life which returned to normal at day 3.
Nursing Mothers
It is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from calcitriol, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use
The safety and effectiveness of calcitriol injection were examined in a 12-week randomized, doubleblind, placebo-controlled study of 35 pediatric patients, aged 13 to 18 years, with end-stage renal disease on hemodialysis. Sixty-six percent of the patients were male, 57% were African-American, and nearly all had received some form of vitamin D therapy prior to the study. The initial dose of calcitriol was 0.5 mcg, 1.0 mcg, or 1.5 mcg, 3 times per week, based on baseline iPTH level of less than 500 pg/mL, 500-1000 pg/mL, or greater than 1000 pg/mL, respectively. The dose of calcitriol was adjusted in 0.25 mcg increments based on the levels of serum iPTH, calcium, and Ca x P. The mean baseline levels of iPTH were 769 pg/mL for the 16 calcitriol-treated patients and 897 pg/mL for the 19 placebo-treated subjects. The mean weekly dose of calctiriol ranged from 1.0 mcg to 1.4 mcg. In the primary efficacy analysis, 7 of 16 (44%) subjects in the calcitriol group had 2 consecutive 30% decreases from baseline iPTH compared with 3 to 19 (16%) patients in the placebo group (95% CI for the difference between groups -6%, 62%). One calcitriol-treated patient experienced transient hypercalcemia (>11.0 mg/dL), while 6 of 16 (38%) calcitriol-treated patients vs. 2 of 19 (11%) placebo-treated patients experienced Ca x P>75.
Geriatric Use
Clinical studies of calcitriol injection did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosage range, reflecting greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
-
ADVERSE REACTIONS
Adverse effects of calcitriol injection are, in general, similar to those encountered with excessive vitamin D intake. The early and late signs and symptoms of vitamin D intoxication associated with hypercalcemia include:
Early
Weakness, headache, somnolence, nausea, vomiting, dry mouth, constipation, muscle pain, bone pain, metallic taste, anorexia, abdominal pain and epigastric discomfort.
Late
Polyuria, polydipsia, anorexia, weight loss, nocturia, conjunctivitis (calcific) pancreatitis, photophobia, rhinorrhea, pruritus, hyperthermia, decreased libido, elevated BUN, albuminuria, hypercholesterolemia, elevated SGOT and SGPT, ectopic calcification, hypertension, cardiac arrhythmias, nephrocalcinosis, sensory disturbance, dehydration, apathy, and, rarely, overt psychosis.
Occasional mild pain on injection has been observed.
-
OVERDOSAGE
Administration of calcitriol injection to patients in excess of their requirements can cause hypercalcemia, hypercalciuria and hyperphosphatemia. High intake of calcium and phosphate concomitant with calcitriol injection may lead to similar abnormalities (see WARNINGS, PRECAUTIONS and ADVERSE REACTIONS).
Treatment of Hypercalcemia and Overdosage in Patients on Hemodialysis
General treatment of hypercalcemia (greater than 1 mg/dL above the upper limit of normal range) consists of immediate discontinuation of calcitriol injection therapy, institution of a low calcium diet and withdrawal of calcium supplements. Serum calcium levels should be determined daily until normocalcemia ensues. Hypercalcemia usually resolves in two to seven days. When serum calcium levels have returned to within normal limits, Calcitriol Injection therapy may be reinstituted at a dose 0.5 mcg less than prior therapy. Serum calcium levels should be obtained at least twice weekly after all dosage changes.
Persistent or markedly elevated serum calcium levels may be corrected by dialysis against a calciumfree dialysate.
Treatment of Accidental Overdosage of Calcitriol Injection
The treatment of acute accidental overdosage of calcitriol injection should consist of general supportive measures. Serial serum electrolyte determinations (especially calcium), rate of urinary calcium excretion and assessment of electrocardiographic abnormalities due to the hypercalcemia should be obtained. Such monitoring is critical in patients receiving digitalis. Discontinuation of supplemental calcium and low calcium diet are also indicated in accidental overdosage. Due to the relatively short duration of the pharmacological action of calcitriol, further measures are probably unnecessary. Should, however, persistent and markedly elevated serum calcium levels occur, there are a variety of therapeutic alternatives which may be considered, depending on the patients' underlying condition. These include the use of drugs such as phosphates and corticosteroids as well as measures to induce an appropriate forced diuresis. The use of peritoneal dialysis against a calcium-free dialysate has also been reported.
-
DOSAGE AND ADMINISTRATION
Calcitriol injection is for intravenous injection only.
The optimal dose of calcitriol injection must be carefully determined for each patient.
The effectiveness of calcitriol injection therapy is predicated on the assumption that each patient is receiving an adequate and appropriate daily intake of calcium. The RDA for calcium in adults is 800 mg. To ensure that each patient receives an adequate daily intake of calcium, the physician should either prescribe a calcium supplement or instruct the patient in proper dietary measures.
The recommended initial dose of Calcitriol Injection, depending on the severity of the hypocalcemia and/or secondary hyperparathyroidism, is 1 mcg (0.02 mcg/kg) to 2 mcg administered intravenously three times weekly, approximately every other day. Doses as small as 0.5 mcg and as large as 4 mcg three times weekly have been used as an initial dose. If a satisfactory response is not observed, the dose may be increased by 0.5 to 1 mcg at two to four week intervals. During this titration period, serum calcium and phosphorus levels should be obtained at least twice weekly. If hypercalcemia or a serum calcium times phosphate product greater than 70 is noted, the drug should be immediately discontinued until these parameters are appropriate. Then, the calcitriol injection dose should be reinitiated at a lower dose. Doses may need to be reduced as the PTH levels decrease in response to the therapy. Thus, incremental dosing must be individualized and commensurate with PTH, serum calcium and phosphorus levels. The following is a suggested approach in dose titration:
PTH Levels Calcitriol Injection Dose the same or increasing increase decreasing by < 30% increase decreasing by > 30%, < 60% maintain decreasing by > 60% decrease one and one-half to three times the
upper limit of normalmaintain
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
Discard unused portion. - How Supplied
- PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
CALCITRIOL
calcitriol injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:68083-316 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength CALCITRIOL (UNII: FXC9231JVH) (CALCITRIOL - UNII:FXC9231JVH) CALCITRIOL 1 ug in 1 mL Inactive Ingredients Ingredient Name Strength POLYSORBATE 20 (UNII: 7T1F30V5YH) 4 mg in 1 mL BUTYLATED HYDROXYTOLUENE (UNII: 1P9D0Z171K) 0.02 mg in 1 mL BUTYLATED HYDROXYANISOLE (UNII: REK4960K2U) 0.003 mg in 1 mL SODIUM CHLORIDE (UNII: 451W47IQ8X) 1.5 mg in 1 mL SODIUM PHOSPHATE, DIBASIC, ANHYDROUS (UNII: 22ADO53M6F) 7.6 mg in 1 mL SODIUM PHOSPHATE, MONOBASIC, MONOHYDRATE (UNII: 593YOG76RN) 1.8 mg in 1 mL EDETATE DISODIUM (UNII: 7FLD91C86K) 1.1 mg in 1 mL WATER (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:68083-316-10 10 in 1 CARTON 02/03/2020 1 1 mL in 1 VIAL; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA211030 02/03/2020 Labeler - Gland Pharma Limited (918601238) Establishment Name Address ID/FEI Business Operations Gland Pharma Limited 918601238 ANALYSIS(68083-316) , MANUFACTURE(68083-316) , PACK(68083-316)