Label: FILSPARI- sparsentan tablet, film coated


- NDC Code(s): 68974-200-30, 68974-400-30
- Packager: Travere Therapeutics, Inc.
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: New Drug Application
Drug Label Information
Updated February 17, 2023
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Medication Guide: HTML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use FILSPARITM safely and effectively. See full prescribing information for FILSPARITM.
FILSPARITM (sparsentan) tablets, for oral use
Initial U.S. Approval: 2023WARNING: HEPATOTOXICITY and EMBRYO- FETAL TOXICITY
See full prescribing information for complete boxed warning.
- FILSPARI is only available through a restricted distribution program called the FILSPARI Risk Evaluation and Mitigation Strategies (REMS) because of these risks (5.3):
- Some endothelin receptor antagonists have caused elevations of aminotransferases, hepatotoxicity, and liver failure (5.1).
- Measure liver aminotransferases and total bilirubin prior to initiation of treatment and ALT and AST monthly for 12 months, then every 3 months during treatment (2.2, 2.5, 5.1).
- Interrupt treatment and closely monitor patients developing aminotransferase elevations more than 3x Upper Limit of Normal (ULN) (2.2, 2.5).
- Based on animal data, FILSPARI can cause major birth defects if used during pregnancy (4, 5.2, 8.1).
- Pregnancy testing is required before, during, and after treatment (2.2, 4, 5.2, 8.1).
- Patients who can become pregnant must use effective contraception prior to initiation of treatment, during treatment, and for one month after (4, 5.3, 8.1, 8.3).
INDICATIONS AND USAGE
FILSPARI is an endothelin and angiotensin II receptor antagonist indicated to reduce proteinuria in adults with primary immunoglobulin A nephropathy (IgAN) at risk of rapid disease progression, generally a urine protein-to-creatinine ratio (UPCR) ≥1.5 g/g. (1, 12.1).
This indication is approved under accelerated approval based on reduction of proteinuria. It has not been established whether FILSPARI slows kidney function decline in patients with IgAN. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory clinical trial.
DOSAGE AND ADMINISTRATION
- Prior to initiating treatment with FILSPARI, discontinue use of renin- angiotensin-aldosterone system (RAAS) inhibitors, endothelin receptor antagonists (ERAs) or aliskiren (2.1, 4, 7.1).
- Initiate treatment with FILSPARI at 200 mg orally once daily. After 14 days, increase to the recommended dose of 400 mg once daily, as tolerated. When resuming treatment with FILSPARI after an interruption, consider titration of FILSPARI, starting at 200 mg once daily. After 14 days, increase to the recommended dose of 400 mg once daily (2.3).
- Instruct patients to swallow tablets whole with water prior to the morning or evening meal (2.4).
DOSAGE FORMS AND STRENGTHS
Tablets: 200 mg and 400 mg (3)
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
ADVERSE REACTIONS
Most common adverse reactions (≥5%) are peripheral edema , hypotension (including orthostatic hypotension), dizziness, hyperkalemia, and anemia (6.1).
To report SUSPECTED ADVERSE REACTIONS, contact Travere Therapeutics at 1-877-659-5518 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
- Renin-Angiotensin System (RAS) inhibitors and ERAs: Contraindicated. Increased risk of hypotension, hyperkalemia (2.1, 4, 7.1).
- Strong CYP3A inhibitors: Avoid concomitant use. Increased sparsentan exposure (2.6, 7.2, 12.3).
- Moderate CYP3A inhibitors: Monitor adverse reactions. Increased sparsentan exposure (7.2, 12.3).
- Strong CYP3A inducers: Avoid concomitant use. Decreased sparsentan exposure (7.3, 12.3).
- Antacids: Avoid use within 2 hours before or after use of sparsentan. May decrease exposure to sparsentan (7.4, 11).
- Acid reducing agents: Avoid concomitant use. May decrease exposure to sparsentan (7.4).
- Nonsteroidal anti-inflammatory drugs (NSAIDs) including selective cyclooxygenase (COX-2) inhibitors: Monitor for signs of worsening renal function. Increased risk of kidney injury (7.5).
- CYP2B6, 2C9, and 2C19 substrates: Monitor for efficacy of the concurrently administered substrates. Decreased exposure of these substrates (7.6, 12.3).
- Sensitive P-gp and BCRP substrates: Avoid concomitant use. Increased exposure to substrates (7.7, 12.3).
- Agents Increasing Serum Potassium: Increased risk of hyperkalemia, monitor serum potassium frequently (5.6, 7.8).
USE IN SPECIFIC POPULATIONS
- Lactation: Advise not to breastfeed (8.2).
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 2/2023
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: HEPATOTOXICITY and EMBRYO-FETAL TOXICITY
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 General Consideration
2.2 Monitoring
2.3 Recommended Dosage
2.4 Administration
2.5 Dosage Adjustment for Aminotransferase Elevations
2.6 Dosage Modification for Concomitant Use with Strong CYP3A Inhibitors
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Hepatotoxicity
5.2 Embryo-Fetal Toxicity
5.3 FILSPARI REMS
5.4 Hypotension
5.5 Acute Kidney Injury
5.6 Hyperkalemia
5.7 Fluid Retention
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
7 DRUG INTERACTIONS
7.1 Renin-Angiotensin System (RAS) Inhibitors and ERAs
7.2 Strong and Moderate CYP3A Inhibitors
7.3 Strong CYP3A Inducers
7.4 Antacids and Acid Reducing Agents
7.5 Non-Steroidal Anti-Inflammatory Agents (NSAIDs), Including Selective Cyclooxygenase-2 (COX-2) Inhibitors
7.6 CYP2B6, 2C9, and 2C19 Substrates
7.7 P-gp and BCRP Substrates
7.8 Agents Increasing Serum Potassium
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Hepatic Impairment
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, and Impairment of Fertility
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
BOXED WARNING
(What is this?)
WARNING: HEPATOTOXICITY and EMBRYO-FETAL TOXICITY
Because of the risks of hepatotoxicity and birth defects, FILSPARI is available only through a restricted program called the FILSPARI REMS. Under the FILSPARI REMS, prescribers, patients, and pharmacies must enroll in the program [see Warnings and Precautions (5.1, 5.2, 5.3)].
Hepatotoxicity
Some Endothelin Receptor Antagonists (ERAs) have caused elevations of aminotransferases, hepatotoxicity, and liver failure. In clinical studies, elevations in aminotransferases (ALT or AST) of at least 3-times the Upper Limit of Normal (ULN) have been observed in up to 2.5% of FILSPARI-treated patients, including cases confirmed with rechallenge.
Measure transaminases and bilirubin before initiating treatment and monthly for the first 12 months, and then every 3 months during treatment. Interrupt treatment and closely monitor patients who develop aminotransferase elevations more than 3x ULN [see Dosage and Administration (2.3, 2.5), Warning and Precautions (5.1)].
FILSPARI should generally be avoided in patients with elevated aminotransferases (>3x ULN) at baseline because monitoring for hepatotoxicity may be more difficult and these patients may be at increased risk for serious hepatotoxicity [see Dosage and Administration (2.3, 2.5), Warning and Precautions (5.1)]
Embryo-Fetal Toxicity
FILSPARI can cause major birth defects if used by pregnant patients based on animal data [see Warnings and Precautions (5.2), Use in Specific Populations (8.1)]. Therefore, pregnancy testing is required before the initiation of treatment, during treatment, and one month after discontinuation of treatment with FILSPARI. Patients who can become pregnant must use effective contraception before the initiation of treatment, during treatment, and for one month after discontinuation of treatment with FILSPARI [see Dosage and Administration (2.2), Contraindications (4), Warnings and Precautions (5.2), Use in Specific Populations (8.1, 8.3)].
-
1 INDICATIONS AND USAGE
FILSPARI is indicated to reduce proteinuria in adults with primary immunoglobulin A nephropathy (IgAN) at risk of rapid disease progression, generally a urine protein-to-creatinine ratio (UPCR) ≥1.5 g/g.
This indication is approved under accelerated approval based on a reduction of proteinuria [see Clinical Studies (14)]. It has not been established whether FILSPARI slows kidney function decline in patients with IgAN. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory clinical trial.
-
2 DOSAGE AND ADMINISTRATION
2.1 General Consideration
Prior to initiating treatment with FILSPARI, discontinue use of renin-angiotensin-aldosterone system (RAAS) inhibitors, endothelin receptor antagonists (ERAs), and aliskiren [see Contraindications (4), Drug Interactions (7.1)].
2.2 Monitoring
Initiate treatment with FILSPARI only after measuring aminotransferase levels and total bilirubin. Avoid initiation in patients with elevated aminotransferases (>3x ULN). Continue required monitoring monthly for the first 12 months after initiation or restarting following an interruption due to elevated transaminases, then every 3 months during treatment with FILSPARI [see Dosage and Administration (2.2, 2.3, 2.5), Warnings and Precautions (5.1)].
Initiate treatment with FILSPARI in patients who can become pregnant only after confirmation of a negative pregnancy test. Pregnancy tests are required monthly during treatment and one month after discontinuation of treatment with FILSPARI [see Warnings and Precautions (5.2), Use in Specific Populations (8.1, 8.3)].
2.3 Recommended Dosage
Initiate treatment with FILSPARI at 200 mg orally once daily. After 14 days, increase to the recommended dose of 400 mg once daily, as tolerated. When resuming treatment with FILSPARI after an interruption, consider titration of FILSPARI, starting at 200 mg once daily. After 14 days, increase to the recommended dose of 400 mg once daily [see Drug Interactions (7.2)].
2.4 Administration
Instruct patient to swallow tablets whole with water prior to the morning or evening meal. Maintain the same dosing pattern in relationship to meals. If a dose is missed, take the next dose at the regularly scheduled time. Do not take double or extra doses.
2.5 Dosage Adjustment for Aminotransferase Elevations
If aminotransferase levels increase, adjust monitoring and treatment plan according to Table 1.
Do not resume treatment in patients who have experienced clinical symptoms of hepatotoxicity or in patients whose hepatic enzyme levels and bilirubin have not returned to pretreatment levels.
Table 1: Dosage Adjustment and Monitoring in Patients Developing Aminotransferase Elevations >3x ULN ALT = alanine aminotransferase; AST = aspartate aminotransferase; INR = international normalized ratio; ULN = upper limit of normal. ALT/AST levels Treatment and monitoring recommendations >3x and ≤8x ULN Confirm elevation with a repeat measure.
If confirmed, interrupt treatment, and monitor aminotransferase levels and bilirubin at least weekly, and INR as needed, until the levels return to pretreatment values and the patient is asymptomatic.
Do not resume treatment if any of the following occurs without other cause found:
- ALT or AST >3x ULN and total bilirubin >2x ULN or INR >1.5
- ALT or AST >3x ULN, with symptoms of fatigue, nausea, vomiting, right upper quadrant pain or tenderness, fever, rash, and/or eosinophilia (>5% eosinophils)
- ALT or AST >5x ULN for more than 2 weeks
If treatment is resumed, initiate FILSPARI at 200 mg once daily, with reassessment of hepatic enzyme levels and bilirubin within 3 days. Close monitoring is required in these patients [see Dosage and Administration (2.2, 2.3)].
>8x ULN Stop treatment permanently if no other cause found. 2.6 Dosage Modification for Concomitant Use with Strong CYP3A Inhibitors
Avoid concomitant use of strong CYP3A inhibitors with FILSPARI.
If a strong CYP3A inhibitor cannot be avoided, interrupt treatment with FILSPARI [see Drug Interactions (7.2)].
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
Use of FILSPARI is contraindicated in patients who are pregnant [see Dosage and Administration (2.2), Warnings and Precautions (5.1), Use in Specific Populations (8.1)].
Do not coadminister FILSPARI with angiotensin receptor blockers (ARBs), ERAs, or aliskiren [see Dosage and Administration (2.1), Drug Interactions (7.1)].
-
5 WARNINGS AND PRECAUTIONS
5.1 Hepatotoxicity
Elevations in ALT or AST of at least 3-fold ULN have been observed in up to 2.5% of FILSPARI-treated patients, including cases confirmed with rechallenge [see Adverse Reactions (6.1)]. While no concurrent elevations in bilirubin >2-times ULN or cases of liver failure were observed in FILSPARI-treated patients in clinical trials, some endothelin receptor antagonists have caused elevations of aminotransferases, hepatotoxicity, and liver failure. To reduce the risk of potential serious hepatotoxicity, measure serum aminotransferase levels and total bilirubin prior to initiation of treatment and monthly for the first 12 months, then every 3 months during treatment [see Dosage and Administration (2.2)].
Advise patients with symptoms suggesting hepatotoxicity (nausea, vomiting, right upper quadrant pain, fatigue, anorexia, jaundice, dark urine, fever, or itching) to immediately stop treatment with FILSPARI and seek medical attention . If aminotransferase levels are abnormal at any time during treatment, interrupt FILSPARI and monitor as recommended [see Dosage and Administration (2.5)].
Consider re-initiation of FILSPARI only when hepatic enzyme levels and bilirubin return to pretreatment values and only in patients who have not experienced clinical symptoms of hepatotoxicity. [see Dosage and Administration (2.2, 2.5)].
Avoid initiation of FILSPARI in patients with elevated aminotransferases (>3x ULN) prior to drug initiation because monitoring hepatotoxicity in these patients may be more difficult and these patients may be at increased risk for serious hepatotoxicity [see Dosage and Administration (2.2, 2.5) and Warnings and Precautions (5.3)].
5.2 Embryo-Fetal Toxicity
Based on data from animal reproduction studies, FILSPARI can cause fetal harm when administered to a pregnant patient and is contraindicated during pregnancy. Advise patients who can become pregnant of the potential risk to a fetus. Obtain a pregnancy test prior to initiation of treatment with FILSPARI, monthly during treatment and one month after discontinuation of treatment. Advise patients who can become pregnant to use effective contraception prior to initiation of treatment, during treatment, and for one month after discontinuation of treatment with FILSPARI [see Dosage and Administration (2.2), Warnings and Precautions (5.3) and Use in Specific Populations (8.1, 8.3)].
5.3 FILSPARI REMS
For all patients, FILSPARI is available only through a restricted program under a REMS called the FILSPARI REMS because of the risk of hepatotoxicity and embryo-fetal toxicity [see Contraindications (4), Warnings and Precautions (5.1, 5.2), Use in Specific Populations (8.1, 8.3)].
Important requirements of the FILSPARI REMS include the following:
- Prescribers must be certified with the FILSPARI REMS by enrolling and completing training.
- All patients must enroll in the FILSPARI REMS prior to initiating treatment and comply with monitoring requirements [see Dosage and Administration (2.2, 2.5, 2.6), Warnings and Precautions (5.1, 5.2), Use in Specific Populations (8.3)].
- Pharmacies that dispense FILSPARI must be certified with the FILSPARI REMS and must dispense only to patients who are authorized to receive FILSPARI.
Further information is available at www.filsparirems.com or 1-833-513-1325.
5.4 Hypotension
Hypotension has been observed in patients treated with ARBs and endothelin receptor antagonists (ERAs) and was observed in clinical studies with FILSPARI. In the PROTECT trial, there was a greater incidence of hypotension-associated adverse events, some serious, including dizziness, in patients treated with FILSPARI compared to irbesartan [see Adverse Reactions (6.1)].
In patients at risk for hypotension, consider eliminating or adjusting other antihypertensive medications and maintaining appropriate volume status.
If hypotension develops, despite elimination or reduction of other antihypertensive medications, consider a dose reduction or dose interruption of FILSPARI. A transient hypotensive response is not a contraindication to further dosing of FILSPARI, which can be given once blood pressure has stabilized.
5.5 Acute Kidney Injury
Monitor kidney function periodically. Drugs that inhibit the renin-angiotensin system can cause acute kidney injury. Patients whose kidney function may depend in part on the activity of the renin-angiotensin system (e.g., patients with renal artery stenosis, chronic kidney disease, severe congestive heart failure, or volume depletion) may be at particular risk of developing acute kidney injury on FILSPARI. Consider withholding or discontinuing therapy in patients who develop a clinically significant decrease in kidney function while on FILSPARI.
5.6 Hyperkalemia
Monitor serum potassium periodically and treat appropriately. Patients with advanced kidney disease or taking concomitant potassium-increasing drugs (e.g., potassium supplements, potassium-sparing diuretics), or using potassium-containing salt substitutes are at increased risk for developing hyperkalemia. Dosage reduction or discontinuation of FILSPARI may be required [see Dosage and Administration (2.3), Adverse Reactions (6.1)].
5.7 Fluid Retention
Fluid retention may occur with endothelin receptor antagonists and has been observed in clinical studies with FILSPARI [see Adverse Reactions (6.1)]. FILSPARI has not been evaluated in patients with heart failure.
If clinically significant fluid retention develops, evaluate the patient to determine the cause and the potential need to initiate or modify the dose of diuretic treatment then consider modifying the dose of FILSPARI.
-
6 ADVERSE REACTIONS
Clinically significant adverse reactions that appear in other sections of the label include:
- Hepatotoxicity [see Warnings and Precautions (5.1)]
- Embryo-Fetal Toxicity [see Warnings and Precautions (5.2)]
- Hypotension [see Warnings and Precautions (5.4)]
- Acute Kidney Injury [see Warnings and Precautions (5.5)]
- Hyperkalemia [see Warnings and Precautions (5.6)]
- Fluid Retention [see Warnings and Precautions (5.7)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety of FILSPARI was evaluated in PROTECT (NCT03762850), an ongoing, randomized, double-blind, active-controlled clinical study in adults with IgAN.
The data below reflect FILSPARI exposure in 202 patients with a median duration of 73 weeks (up to 110 weeks).
The most common adverse reactions are presented in Table 2.
Table 2: Adverse Reactions1 Reported in ≥2% in Subjects Treated with FILSPARI 1 Data presented include all Treatment-Emergent Adverse Events reported
2 Elevations in ALT or AST >3-fold ULN reported as Adverse Events of InterestFILSPARI
(N = 202)
n (%)Irbesartan
(N = 202)
n (%)Peripheral edema 29 (14) 19 (9) Hypotension (including orthostatic hypotension) 28 (14) 12 (6) Dizziness 27 (13) 11 (5) Hyperkalemia 27 (13) 21 (10) Anemia 10 (5) 5 (2) Acute kidney injury 9 (4) 2 (1) Transaminase elevations2 5 (2.5) 4 (2) Initiation of FILSPARI may cause an initial small decrease in estimated glomerular filtration rate (eGFR) that occurs within the first 4 weeks of starting therapy and then stabilizes.
The incidence of a hemoglobin decrease >2 g/dL compared to baseline and below the lower limit of normal was greater for the FILSPARI arm (11%) compared to the irbesartan arm (5%). This decrease is thought to be in part due to hemodilution. There were no treatment discontinuations due to anemia or hemoglobin decrease in the PROTECT study.
-
7 DRUG INTERACTIONS
7.1 Renin-Angiotensin System (RAS) Inhibitors and ERAs
Do not coadminister FILSPARI with ARBs, ERAs, or aliskiren [see Dosage and Administration (2.1), Contraindications (4)].
Combined use of these agents is associated with increased risks of hypotension, syncope, hyperkalemia, and changes in renal function (including acute renal failure).
7.2 Strong and Moderate CYP3A Inhibitors
Avoid concomitant use of FILSPARI with strong CYP3A inhibitors. If a strong CYP3A inhibitor cannot be avoided, interrupt treatment with FILSPARI. When resuming treatment with FILSPARI, consider dose titration [see Dosage and Administration (2.3, 2.6), Clinical Pharmacology (12.3)].
Monitor blood pressure, serum potassium, edema, and kidney function regularly when used concomitantly with moderate CYP3A inhibitors [see Warnings and Precautions (5.4, 5.5, 5.6, 5.7)]. No FILSPARI dose adjustment is needed.
Sparsentan is a CYP3A substrate. Concomitant use with a strong CYP3A inhibitor increases sparsentan Cmax and AUC [see Clinical Pharmacology (12.3)], which may increase the risk of FILSPARI adverse reactions.
7.3 Strong CYP3A Inducers
Avoid concomitant use with a strong CYP3A inducer. Sparsentan is a CYP3A substrate. Concomitant use with a strong CYP3A inducer decreases sparsentan Cmax and AUC [see Clinical Pharmacology (12.3)], which may reduce FILSPARI efficacy.
7.4 Antacids and Acid Reducing Agents
Administer FILSPARI 2 hours before or after administration of antacids. Avoid concomitant use of acid reducing agents (histamine H2 receptor antagonist and PPI proton pump inhibitor) with FILSPARI. Sparsentan exhibits pH-dependent solubility [see Description (11)]. Antacids or acid reducing agents may decrease sparsentan exposure which may reduce FILSPARI efficacy.
7.5 Non-Steroidal Anti-Inflammatory Agents (NSAIDs), Including Selective Cyclooxygenase-2 (COX-2) Inhibitors
Monitor for signs of worsening renal function with concomitant use with NSAIDs (including selective COX-2 inhibitors). In patients with volume depletion (including those on diuretic therapy) or with impaired kidney function, concomitant use of NSAIDs (including selective COX-2 inhibitors) with drugs that antagonize the angiotensin II receptor may result in deterioration of kidney function, including possible kidney failure [see Warnings and Precautions (5.5)]. These effects are usually reversible.
7.6 CYP2B6, 2C9, and 2C19 Substrates
Monitor for efficacy of the concurrently administered CYP2B6, 2C9, and 2C19 substrates and consider dosage adjustment in accordance with the Prescribing Information. Sparsentan is an inducer of CYP2B6, 2C9, and 2C19. Sparsentan decreases exposure of these substrates [see Clinical Pharmacology (12.3)], which may reduce efficacy related to these substrates.
7.7 P-gp and BCRP Substrates
Avoid concomitant use of sensitive substrates of P-gp and BCRP with FILSPARI. Sparsentan is an inhibitor of P-gp and BCRP. Sparsentan may increase exposure of these transporter substrates [see Clinical Pharmacology (12.3)], which may increase the risk of adverse reactions related to these substrates.
7.8 Agents Increasing Serum Potassium
Monitor serum potassium frequently in patients treated with FILSPARI and other agents that increase serum potassium. Concomitant use of FILSPARI with potassium-sparing diuretics, potassium supplements, potassium-containing salt substitutes, or other drugs that raise serum potassium levels may result in hyperkalemia [see Warnings and Precautions (5.6)].
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Based on data from animal reproductive toxicity studies, FILSPARI can cause fetal harm, including birth defects and fetal death, when administered to a pregnant patient and is contraindicated during pregnancy [see Contraindications (4)]. Available data from reports of pregnancy in clinical trials with FILSPARI are insufficient to identify a drug-associated risk of major birth defects, miscarriage, or other adverse maternal or fetal outcomes. In animal reproduction studies, oral administration of sparsentan to pregnant rats throughout organogenesis at 10-times the maximum recommended human dose (MRHD) in mg/day caused teratogenic effects in rats, including craniofacial malformations, skeletal abnormalities, increased embryo-fetal lethality, and reduced fetal weights (see Data). Advise pregnant patients of the potential risk to the fetus.
The background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
In embryo-fetal development studies in pregnant rats and rabbits, teratogenicity and/or developmental toxicity were observed, which were attributed to the antagonism of endothelin type A (ETA) and angiotensin II type 1 (AT1) receptors.
In pregnant rats, oral administration of sparsentan throughout organogenesis at doses of 80, 160, and 240 mg/kg/day resulted in dose-dependent teratogenic effects in the form of craniofacial malformations, skeletal abnormalities, increased embryo-fetal lethality, and reduced fetal weights at all doses tested. The area under the curve (AUC) at the lowest dose tested (80 mg/kg/day) was approximately 10 times the AUC at the MRHD of 400 mg/day. In pregnant rabbits, oral administration of sparsentan throughout organogenesis at doses of 2.5, 10 and 40 mg/kg/day resulted in maternal death and abortions at 10 and 40 mg/kg/day which provided exposures approximately 0.1 times and 0.2 times the AUC at the MRHD, respectively. An increase in fetal variation (supernumerary cervical ribs) occurred at the high dose of 40 mg/kg/day.
In the pre- and postnatal development study in rats, oral administration of sparsentan during pregnancy and the lactational period at doses of 5, 20, or 80 mg/kg/day resulted in maternal death, body weight loss/reduced body weight gain, and adverse clinical signs at 80 mg/kg/day. An increase in pup deaths occurred at 80 mg/kg/day (approximately 10 times the AUC at MRHD) during the neonatal period through weaning, and decreased growth occurred at ≥ 20 mg/kg/day (approximately 2.6 times the AUC at the MRHD) after weaning. The NOAEL for pre- and postnatal development in rats was 5 mg/kg/day, approximately 0.7 times the AUC at the MRHD.
8.2 Lactation
There are no data on the presence of sparsentan in human milk, the effects on the breastfed infant, or the effect on milk production. Because of the potential for adverse reactions, such as hypotension in breastfed infants, advise patients not to breastfeed during treatment with FILSPARI.
8.3 Females and Males of Reproductive Potential
Based on data from animal reproductive toxicity studies, FILSPARI can cause fetal harm, including birth defects and fetal death, when administered to a pregnant patient and is contraindicated during pregnancy [see Contraindications (4), Use in Specific Populations (8.1)].
Pregnancy Testing
Verify that patients who can become pregnant are not pregnant prior to initiating FILSPARI, monthly during treatment, and one month after discontinuation of treatment. The patient should contact their physician immediately for pregnancy testing if onset of menses is delayed or pregnancy is suspected. If the pregnancy test is positive, the physician and patient must discuss the risks to their pregnancy and the fetus.Contraception
Patients who can become pregnant using FILSPARI must use an effective method of contraception prior to initiation of treatment, during treatment, and for one month after discontinuation of treatment with FILSPARI to prevent pregnancy [see Warnings and Precautions (5.2)].8.4 Pediatric Use
The safety and efficacy of FILSPARI in pediatric patients have not been established.
-
10 OVERDOSAGE
There is no experience with overdose with FILSPARI. Sparsentan has been given in doses up to 1600 mg/day in healthy volunteers, or up to 400 mg/day in patients. Overdose of FILSPARI may result in decreased blood pressure. In the event of an overdose, standard supportive measures should be taken, as required. Dialysis is unlikely to be effective because sparsentan is highly protein-bound.
-
11 DESCRIPTION
FILSPARI (sparsentan) is an endothelin and angiotensin II receptor antagonist. The chemical name of sparsentan is 2-[4-[(2-butyl-4-oxo-1,3-diazaspiro[4.4]non-1-en-3-yl)methyl]-2-(ethoxymethyl)phenyl]-N-(4,5-dimethyl-1,2-oxazol-3-yl)benzenesulfonamide.
Sparsentan is a white to off-white powder, which is practically insoluble in water. Sparsentan has pH-dependent solubility, with intrinsic solubility of 1.48 and 0.055 mg/mL under pH 1.2 and 6.8, respectively. Sparsentan has a molecular weight of 592.76 g/mol, a molecular formula of C32H40N4O5S, and the following structure:
FILSPARI is available as film-coated 200 mg and 400 mg strength immediate release tablets for oral administration.
The inactive ingredients in FILSPARI are colloidal silicon dioxide, lactose anhydrous, magnesium stearate, silicified microcrystalline cellulose, and sodium starch glycolate. Film-coating is composed of macrogol/polyethylene glycol, polyvinyl alcohol-partially hydrolyzed, talc, and titanium dioxide.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Sparsentan is a single molecule with antagonism of the endothelin type A receptor (ETAR) and the angiotensin II type 1 receptor (AT1R). Sparsentan has high affinity for both the ETAR (Ki= 12.8 nM) and the AT1R (Ki=0.36 nM), and greater than 500-fold selectivity for these receptors over the endothelin type B and angiotensin II subtype 2 receptors. Endothelin-1 and angiotensin II are thought to contribute to the pathogenesis of IgAN via the ETAR and AT1R, respectively.
12.2 Pharmacodynamics
Dose-response information is not available. At the recommended dose regimen, no statistically significant exposure-response (E-R) relationship was identified between sparsentan exposure and the percentage reduction from baseline in UPCR at Week 36 over the observed sparsentan exposure range. No clinically meaningful E-R relationships were observed for hypotension of any grade and peripheral edema worst grade. A statistically significant relationship was observed between sparsentan exposures and the incidence of hyperkalemia of any grade.
In a randomized, positive-, and placebo-controlled study in healthy subjects, sparsentan caused QTcF prolongation with maximal mean effect of 8.8 msec (90% CI: 5.9, 11.8) at 800 mg and 8.1 msec (90% CI: 5.2, 11.0) at 1600 mg. The underlying mechanism behind the observed QTc prolongation is unknown but is unlikely to be mediated via direct inhibition of hERG channels. At the recommended dose, no clinically relevant QTc prolongation (i.e., > 20 msec) is expected.
12.3 Pharmacokinetics
The pharmacokinetics of sparsentan are presented as geometric mean (% coefficient of variation) unless otherwise specified. The Cmax and AUC of sparsentan increase less than proportionally following administration of single doses of 200 mg to 1600 mg. Sparsentan showed time-dependent pharmacokinetics which may be related to the drug inducing its own metabolism over time. Steady-state plasma levels are reached within 7 days with no accumulation of exposure at the approved recommended dosage. Following a single oral dose of 400 mg sparsentan, the mean Cmax and AUC are 6.97 μg/mL and 83 μg×h/mL, respectively. Following daily doses of 400 mg sparsentan, the steady-state mean Cmax and AUC are 6.47 μg/mL and 63.6 μg×h/mL, respectively.
Following a single oral dose of 400 mg sparsentan, the median (minimum to maximum) time to peak plasma concentration is approximately 3 hours (2 to 8 hours).
Sparsentan AUC and Cmax increased by 22% and 108%, respectively, following administration of a single oral 800 mg dose with a high fat, high calorie meal (1000 kcal, 50% fat) [see Dosage and Administration (2.4)]. No clinically significant differences in sparsentan pharmacokinetics were observed following administration of a single 200 mg dose with a high fat, high calorie meal.
The apparent volume of distribution at steady state is 61.4 L at the approved recommended dosage.
Sparsentan is >99% bound to human plasma proteins.
The clearance of sparsentan is time-dependent which may be related to the drug inducing its own metabolism over time. The apparent clearance (CL/F) of sparsentan is 3.88 L/h following the initial 400 mg dose then increases to 5.11 L/h at steady state.
The half-life of sparsentan is estimated to be 9.6 hours at steady state.
Cytochrome P450 3A is the major isozyme responsible for the metabolism of sparsentan.
After a single dose of radiolabeled sparsentan 400 mg to healthy subjects, approximately 80% of the dose was recovered in feces (9% unchanged) and 2% in urine (negligible amount unchanged). 82% of the dosed radioactivity was recovered within a 10-day collection period.
No clinically significant differences in the pharmacokinetics of sparsentan were observed based on age (18 – 73 years), sex, race, mild to moderate renal impairment (eGFR 30 to 89 mL/min/1.73 m2), or mild to moderate hepatic impairment (Child-Pugh class A or B). Patients with severe hepatic impairment (Child-Pugh class C) and eGFR <30 mL/min/1.73 m2 have not been studied.
Clinical Studies and Model-Informed Approaches
Effect of Other Drugs on Sparsentan
Strong CYP3A inhibitors: Concomitant use with itraconazole (strong CYP3A inhibitor) increased sparsentan Cmax by 25% and AUC by 174%.
Moderate CYP3A inhibitors: Concomitant use with cyclosporine (moderate CYP3A inhibitor) increased sparsentan Cmax by 41% and AUC by 70%.
Strong CYP3A inducers: Coadministration of rifampin (strong CYP3A inducer) is predicted to decrease sparsentan Cmax by 23% and AUC0-inf by 47% at steady state.
Effect of Sparsentan on Other Drugs
No clinically significant differences in the pharmacokinetics of midazolam (sensitive CYP3A4 substrate) or pitavastatin (OATP1B1, OATP1B3, P-gp, and BCRP substrate) were observed when co-administered with sparsentan. In addition, sparsentan had no clinically significant effect on serum creatinine levels (an endogenous biomarker of OAT2, OCT2, MATE1, and MATE2K) or on 6β hydroxycortisol (an endogenous biomarker of OAT3).
CYP2B6 substrates: Concomitant use with sparsentan decreased the exposure of bupropion (CYP2B6 substrate) Cmax by 32% and AUC by 33%.
CYP Enzymes: Sparsentan is a substrate of CYP3A. Sparsentan is both an inhibitor and inducer of CYP3A and an inducer of CYP2B6, CYP2C9, and CYP2C19.
Transporters: Sparsentan is a substrate of P-gp and BCRP but is not a substrate of OATP1B1 or OATP1B3. Sparsentan is an inhibitor of P-gp, BCRP, OATP1B3 and OAT3 but does not inhibit MRP, OATP1B1, NTCP, OCT2, OAT1, MATE1, or MATE2K at relevant concentrations.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, and Impairment of Fertility
Carcinogenesis: In the two-year rat carcinogenicity study, there was no evidence of increased incidence of neoplasia in male rats orally administered at 15 mg/kg/day (the only dose evaluated) and in female rats orally administered up to 240 mg/kg/day, which provided an exposure approximately 0.7 times and 26 times the AUC at the MRHD, respectively. In the 26-week transgenic mouse study, there was no evidence of increased incidence of neoplasia in male and female mice orally administered sparsentan at doses up to 600 mg/kg/day.
Mutagenesis: There was no evidence of mutagenicity or clastogenicity for sparsentan in in vitro bacteria reverse mutation and chromosomal aberration assays, or in an in vivo rat micronucleus study.
Impairment of fertility: In a fertility and early embryonic development study in rats, oral administration of sparsentan at doses of 20, 80, and 320 mg/kg/day for at least 36 (females) and 49 (males) days did not result in any adverse effects on estrous cycles, mating, fertility, sperm evaluation, or pregnancy incidence at doses up to 320 mg/kg/day, which provided approximately 10 and 14 times the AUC at the MRHD for males and females, respectively. Male reproductive organ toxicity was not evident in chronic toxicity studies with sparsentan at exposures up to 10 times and 1.3 times the AUC at the MRHD in rats and monkeys, respectively.
-
14 CLINICAL STUDIES
The effect of FILSPARI on proteinuria was assessed in a randomized, double-blind, active-controlled, multicenter, global study (PROTECT, NCT03762850) in adults with biopsy-proven IgAN, eGFR ≥30 mL/min/1.73 m2, and total urine protein ≥1.0 g/day on a maximized stable dose of RAS inhibitor treatment that was at least 50% of maximum labeled dose. Patients with other glomerulopathies or those who had been recently treated with systemic immunosuppressants were excluded.
Patients were randomized (1:1) to either FILSPARI (400 mg once daily following 200 mg once daily for 14 days) or irbesartan (300 mg once daily following 150 mg once daily for 14 days). Rescue immunosuppressive treatment could be initiated per investigator discretion during the trial, but use of SGLT2 inhibitors was prohibited.
The 281 patients who reached week 36 had a mean age of 46 years (range 18 to 76 years); 69% were male, 62% White, 35% Asian, and 1% Black or African American. Approximately 77% had a history of hypertension, 12% diabetes or impaired fasting glucose, and 53% hematuria. Mean (SD) baseline eGFR was 56 (24) mL/min/1.73 m2.
The primary endpoint was the relative change from baseline in UPCR at Week 36 (Table 3). The mean percent change from baseline over time is displayed in Figure 1.
Table 3: Ratio of Geometric Mean (GM) of UPCR at Week 36 Relative to Baseline (PROTECT, IAS) *Adjusted GM of UPCR was based on MMRM stratified by screening eGFR and total urine protein excretion. MMRM analysis includes UPCR data during the double-blind period up to week 36 from the first 281 randomized and treated subjects at the interim analysis. Baseline was defined as the last non-missing observation on or prior to the start of dosing.
Missing data were imputed using multiple imputation under the missing at random assumption. Data observed while on randomized treatment and after treatment discontinuation were included in the analysis regardless of treatment discontinuation and initiation of rescue therapy (treatment policy strategy). Rescue immunosuppressive treatment was initiated in 1.4% and 5.7% of FILSPARI and irbesartan patients, respectively.
Abbreviations: CI=confidence interval; GM=geometric mean; GMPC=geometric mean percent change; IAS=interim analysis set; MMRM=mixed model repeated measures; N=number of subjects in each group; n=number of subjects with available data at the time of analysis; UPCR=urine protein-to-creatinine ratio.FILSPARI
N=141Irbesartan
N=140Adjusted GM of UPCR*, g/g Baseline 1.2 (n=141) 1.2 (n=140) Week 36 0.7 (n=135) 1.0 (n=128) Adjusted GMPC from Baseline in UPCR at Week 36 (95% CI) ‑45% (-51%, -38%) ‑15% (-24%, -4%) FILSPARI versus Irbesartan: Ratio of adjusted GM relative to baseline at week 36 (95% CI) 0.65 (0.55, 0.77) p-value <0.0001 Figure 1: Percent Change from Baseline in UPCR by Visit (PROTECT, IAS) Adjusted GMPC of UPCR relative to baseline were based on the same MMRM analysis as used in Table 3. Counts in axis table represent number of subjects with UPCR data by visit and treatment group.
BL=baseline; CI=confidence interval; FIL=FILSPARI; GMPC=geometric mean percent change; Irb=irbesartan; IAS=interim analysis data set; MMRM=mixed model repeated measures; N=number of subjects in each group; UPCR=urine protein-to-creatinine ratio.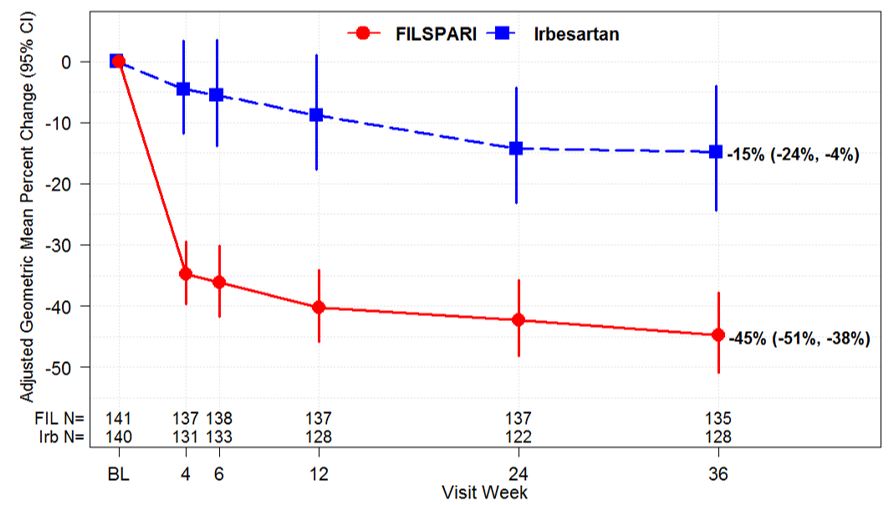
The treatment effect on UPCR at Week 36 was consistent across subgroups such as age, sex, race, and baseline eGFR and proteinuria levels.
-
16 HOW SUPPLIED/STORAGE AND HANDLING
FILSPARI is supplied in bottles of 30 film-coated tablets.
- 200 mg tablets are film-coated, modified oval, white to off-white, debossed with “105” on one side and plain on the other side, available in bottles of 30 tablets with child-resistant caps (NDC 68974-200-30).
- 400 mg tablets are film-coated, modified oval, white to off-white, debossed with “021” on one side and plain on the other side, available in bottles of 30 tablets with child-resistant caps (NDC 68974-400-30).
Store at 20°C to 25°C (68°F to 77°F), excursions permitted to 15°C to 30°C (59°F to 86°F). Store FILSPARI in its original container.
-
17 PATIENT COUNSELING INFORMATION
Advise patients to read the FDA-approved patient labeling (Medication Guide).
Advise the patient that FILSPARI is only available through a restricted access program called the FILSPARI REMS.
As a component of the FILSPARI REMS, prescribers must review the contents of the FILSPARI Medication Guide with the patient before initiating FILSPARI.
Instruct patients that the risks associated with FILSPARI include:
Hepatotoxicity
Advise patients with symptoms suggesting hepatotoxicity (nausea, vomiting, right upper quadrant pain, fatigue, anorexia, jaundice, dark urine, fever, or itching) to immediately stop taking FILSPARI and seek medical attention [see Dosage and Administration (2.2, 2.3, 2.5), Warnings and Precautions (5.1)].
Educate and counsel patients who can become pregnant about the need to use reliable methods of contraception prior to treatment with FILSPARI, during treatment and for one month after treatment discontinuation. Patients who can become pregnant must have pregnancy tests prior to treatment with FILSPARI, monthly during treatment, and one month after treatment discontinuation [see Dosage and Administration (2.2, 2.3, 2.5)), Contraindications (4), Warnings and Precautions (5.2), Use in Specific Populations (8.1, 8.3)].
Patients should be instructed to immediately contact their physician if they suspect they may be pregnant. Patients should seek additional contraceptive advice from a gynecologist or similar expert as needed.
Educate and counsel patients who can become pregnant on the use of emergency contraception in the event of unprotected sex or contraceptive failure.
Advise patients to contact their gynecologist or healthcare provider if they want to change the form of birth control which is used to ensure that another acceptable form of birth control is selected.
Advise the patient that FILSPARI is available only from certified pharmacies that are enrolled in the FILSPARI REMS.
Patients must sign the FILSPARI REMS Patient Enrollment Form to confirm that they understand the risks of FILSPARI.
Advise patients not to breastfeed during treatment with FILSPARI [see Use in Specific Populations (8.2)].
Advise patients to inform their healthcare provider of all concomitant medications, including prescription medications, over-the-counter drugs, vitamins/supplements, herbal products, and grapefruit [see Contraindications (4), Warnings and Precautions (5.4, 5.5, 5.6, 5.7), Drug Interactions (7)].
Other Risks Associated with FILSPARI
Inform patients of other risks associated with FILSPARI, including:
- Hypotension: Advise patients to remain hydrated [see Warnings and Precautions (5.4)].
- Hyperkalemia: Advise patients not to use potassium supplements or salt substitutes that contain potassium without consulting their healthcare provider [see Warnings and Precautions (5.6)].
Advise patients to take the full daily dose with water prior to the morning or evening meal. Maintain the same dosing pattern in relationship to meals. If a dose is missed, take the next dose at the regularly scheduled time. Do not take double or extra doses [see Dosage and Administration (2.4)].
Distributed by Travere Therapeutics, Inc., San Diego, CA 92130
FILSPARI is a registered trademark of Travere Therapeutics, Inc.
-
MEDICATION GUIDE
Medication Guide
FILSPARITM (fil spah’ ree)
(sparsentan)
tabletsWhat is the most important information I should know about FILSPARI?
FILSPARI is only available through the FILSPARI REMS Program. Before you begin taking FILSPARI, you must read and agree to all of the instructions in the FILSPARI REMS Program.
FILSPARI can cause serious side effects, including:
Liver problems.
-
FILSPARI can cause changes in liver tests. Some medicines that are like FILSPARI can cause liver failure. Your healthcare provider will do blood tests to check your liver before starting treatment with FILSPARI, monthly for the first 12 months, and then every 3 months during treatment. Your healthcare provider may temporarily stop or permanently stop treatment with FILSPARI if you have changes in your liver tests.
Tell your healthcare provider right away if you develop any of the following signs of liver problems during treatment with FILSPARI:
- nausea or vomiting
- pain on the upper right side of your stomach area
- tiredness
- loss of appetite
- yellowing of your skin or the white part of your eyes (jaundice)
- dark “tea-colored” urine
- fever
- itching
Serious birth defects.
FILSPARI can cause serious birth defects if taken during pregnancy.
- Patients who can become pregnant must not be pregnant when they start taking FILSPARI or become pregnant during treatment with FILSPARI or for 1 month after stopping treatment with FILSPARI.
- Patients who can become pregnant must have a negative pregnancy test before starting FILSPARI and must have a monthly negative pregnancy test during treatment and 1 month after stopping treatment with FILSPARI.
- Patients who can become pregnant are those who:
- have entered puberty, even if they have not started their menstrual period, and
- have a uterus, and
- have not gone through menopause. Menopause means that you have not had a menstrual period for at least 12 months for natural reasons, or that you have had your ovaries removed.
- Patients who cannot become pregnant are those who:
- have not yet entered puberty, or
- do not have a uterus, or
- have gone through menopause. Menopause means that you have not had a menstrual period for at least 12 months for natural reasons, or that you have had your ovaries removed, or
- are infertile for any other medical reason and this infertility is permanent and cannot be reversed.
- Patients who can become pregnant are those who:
Patients who can become pregnant must use effective birth control during treatment with FILSPARI and for 1 month after stopping FILSPARI because the medicine may still be in your body.
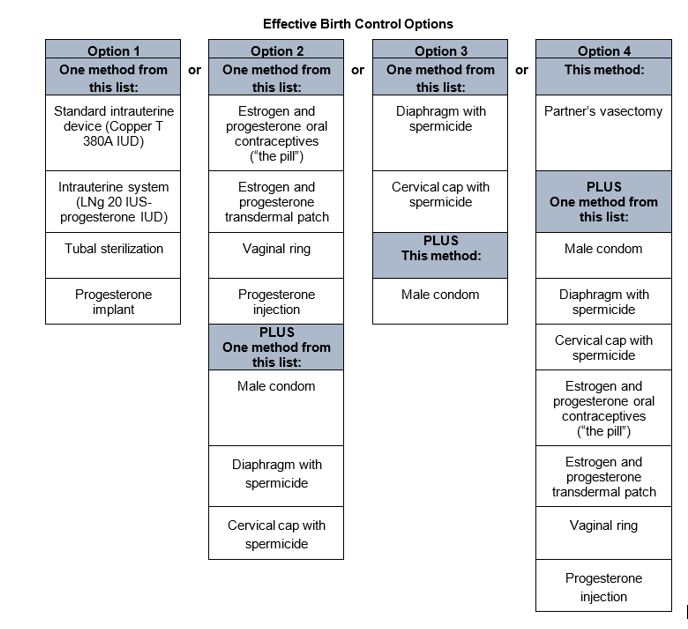
- If you have had a tubal sterilization or have an IUD (intrauterine device) or progesterone implant, these methods may be used alone, and no other form of birth control is needed.
- Talk with your healthcare provider or gynecologist (a healthcare provider who specializes in reproduction) to find out about options for effective forms of birth control that you may use to prevent pregnancy during treatment with FILSPARI.
- If you decide that you want to change the form of birth control that you use, talk with your healthcare provider or gynecologist to be sure that you choose another effective form of birth control.
See the chart below for acceptable birth control options during treatment with FILSPARI.
- Do not have unprotected sex. Talk to your healthcare provider or pharmacist right away if you have unprotected sex or if you think your birth control has failed. Your healthcare provider may talk with you about using emergency birth control.
- Tell your healthcare provider right away if you miss a menstrual period or think you may be pregnant.
What is FILSPARI?
FILSPARI is a prescription medicine used to reduce levels of protein in the urine (proteinuria) in adults with a kidney disease called primary immunoglobulin A nephropathy (IgAN), who are at risk of their disease progressing quickly.
It is not known if FILSPARI is safe and effective in children.
Do not take FILSPARI if you:
- are pregnant, plan to become pregnant, or become pregnant during treatment with FILSPARI. FILSPARI can cause serious birth defects. (See “What is the most important information I should know about FILSPARI?”)
-
are taking any of these medicines:
- an angiotensin receptor blocker, or
- an endothelin receptor antagonist, or
- aliskiren.
Before taking FILSPARI, tell your healthcare provider about all of your medical conditions, including if you have:
- high blood pressure or heart problems
- liver problems
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, herbal supplements, and grapefruit. FILSPARI and other medicines may affect each other and cause side effects. Do not start any new medicine until you check with your healthcare provider.
Especially tell your healthcare provider if you take:
- nonsteroidal anti-inflammatory drugs (NSAIDs)
- potassium-containing medicines, potassium supplements or salt substitutes containing potassium
- blood pressure medicines
How should I take FILSPARI?
- FILSPARI will be provided to you by a certified pharmacy. Your healthcare provider will give you complete details.
- Take FILSPARI exactly as your healthcare provider tells you to take it. Do not stop taking FILSPARI unless your healthcare provider tells you.
- Your healthcare provider may change your dose, temporarily stop, or permanently stop treatment with FILSPARI if you develop side effects.
- Swallow FILSPARI whole with water before your morning or evening meal. Take your dose with the same meal each day.
- If you miss a dose, take the next dose at the regularly scheduled time. Do not take 2 doses at the same time or take extra doses.
- Talk to your healthcare provider before using antacid medicines because they may affect how FILSPARI works.
- If you take too much FILSPARI, call your healthcare provider or go to the nearest hospital emergency room right away.
What should I avoid while taking FILSPARI?
- Do not get pregnant while taking FILSPARI. (See the serious birth defects section of the Medication Guide above called “What is the most important information I should know about FILSPARI?”) If you miss a menstrual period, or think you might be pregnant, call your healthcare provider right away.
- It is not known if FILSPARI passes into your breast milk. You should not breastfeed if you are taking FILSPARI. Talk to your healthcare provider about the best way to feed your baby during treatment with FILSPARI.
What are the possible side effects of FILSPARI?
FILSPARI can cause serious side effects, including:
- Liver problems. See “What is the most important information I should know about FILSPARI?”
- Serious birth defects. See “What is the most important information I should know about FILSPARI?”
- Low blood pressure. Low blood pressure is common during treatment with FILSPARI and can also be serious. Tell your healthcare provider if you feel dizzy, light-headed, or faint. Stay hydrated during treatment with FILSPARI.
- Worsening of Kidney function. Your healthcare provider will check your kidney function during treatment with FILSPARI.
- Increased potassium in your blood. This is common during treatment with FILSPARI and can also be serious. Your healthcare provider will check your potassium blood level during treatment with FILSPARI.
- Fluid retention. FILSPARI can cause your body to hold too much water. Tell your healthcare provider right away if you have any unusual weight gain or swelling of your ankles or legs.
- swelling of hands, legs, ankles and feet (peripheral edema)
- dizziness
- low red blood cells (anemia)
These are not all the possible side effects of FILSPARI.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store FILSPARI?
- Store FILSPARI at room temperature between 68°F to 77°F (20°C to 25°C).
- Store FILSPARI in the original container.
- The bottle has a child-resistant closure.
General information about the safe and effective use of FILSPARI
Medicines are sometimes prescribed for purposes other than those listed in the Medication Guide. Do not use FILSPARI for a condition for which it was not prescribed. Do not give FILSPARI to other people, even if they have the same symptoms that you have. It may harm them. You can ask your healthcare provider or pharmacist for information about FILSPARI that is written for health professionals.
What are the ingredients in FILSPARI?
Active ingredient: sparsentan
Inactive ingredients: colloidal silicon dioxide, lactose anhydrous, magnesium stearate, silicified microcrystalline cellulose, and sodium starch glycolate. Tablets are film coated with material containing macrogol/polyethylene glycol, polyvinyl alcohol-partially hydrolyzed, talc, and titanium dioxide.
Distributed by Travere Therapeutics, Inc., San Diego, CA 92130
FILSPARI is a registered trademark of Travere Therapeutics, Inc.
For more information, go to www.FILSPARI.com or call 1-877-659-5518.This Medication Guide has been approved by the U.S. Food and Drug Administration. Issued: February 2023 -
FILSPARI can cause changes in liver tests. Some medicines that are like FILSPARI can cause liver failure. Your healthcare provider will do blood tests to check your liver before starting treatment with FILSPARI, monthly for the first 12 months, and then every 3 months during treatment. Your healthcare provider may temporarily stop or permanently stop treatment with FILSPARI if you have changes in your liver tests.
- PRINCIPAL DISPLAY PANEL - 200 mg Tablet Bottle Label
- PRINCIPAL DISPLAY PANEL - 400 mg Tablet Label
-
INGREDIENTS AND APPEARANCE
FILSPARI
sparsentan tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:68974-200 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SPARSENTAN (UNII: 9242RO5URM) (SPARSENTAN - UNII:9242RO5URM) SPARSENTAN 200 mg Inactive Ingredients Ingredient Name Strength ANHYDROUS LACTOSE (UNII: 3SY5LH9PMK) SODIUM STARCH GLYCOLATE TYPE A (UNII: H8AV0SQX4D) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) MAGNESIUM STEARATE (UNII: 70097M6I30) CELLULOSE, MICROCRYSTALLINE (UNII: OP1R32D61U) POLYETHYLENE GLYCOL, UNSPECIFIED (UNII: 3WJQ0SDW1A) POLYVINYL ALCOHOL, UNSPECIFIED (UNII: 532B59J990) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color WHITE Score no score Shape ROUND Size 13mm Flavor Imprint Code 105 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:68974-200-30 30 in 1 BOTTLE; Type 0: Not a Combination Product 02/17/2023 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA216403 02/17/2023 FILSPARI
sparsentan tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:68974-400 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SPARSENTAN (UNII: 9242RO5URM) (SPARSENTAN - UNII:9242RO5URM) SPARSENTAN 400 mg Inactive Ingredients Ingredient Name Strength ANHYDROUS LACTOSE (UNII: 3SY5LH9PMK) SODIUM STARCH GLYCOLATE TYPE A (UNII: H8AV0SQX4D) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) MAGNESIUM STEARATE (UNII: 70097M6I30) CELLULOSE, MICROCRYSTALLINE (UNII: OP1R32D61U) POLYETHYLENE GLYCOL, UNSPECIFIED (UNII: 3WJQ0SDW1A) POLYVINYL ALCOHOL, UNSPECIFIED (UNII: 532B59J990) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color WHITE Score no score Shape ROUND Size 18mm Flavor Imprint Code 021 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:68974-400-30 30 in 1 BOTTLE; Type 0: Not a Combination Product 02/17/2023 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA216403 02/17/2023 Labeler - Travere Therapeutics, Inc. (965454502) Registrant - Travere Therapeutics, Inc. (965454502) Establishment Name Address ID/FEI Business Operations Travere Therapeutics, Inc. 965454502 LABEL(68974-200, 68974-400) Establishment Name Address ID/FEI Business Operations Catalent CTS, LLC 962674474 manufacture(68974-200, 68974-400)