Label: DICLOXACILLIN SODIUM capsule

- NDC Code(s): 55289-592-10, 55289-592-20, 55289-592-28, 55289-592-40
- Packager: PD-Rx Pharmaceuticals, Inc.
- This is a repackaged label.
- Source NDC Code(s): 0093-3123
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: Abbreviated New Drug Application
Drug Label Information
Updated September 22, 2023
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
- SPL UNCLASSIFIED SECTION
-
DESCRIPTION
Dicloxacillin sodium, USP is an antibacterial agent of the isoxazolyl penicillin series. It is a penicillinase resistant, acid resistant semisynthetic penicillin suitable for oral administration.
It is monosodium (2 S,5 R,6 R)-6-[3-(2,6-dichlorophenyl)-5-methyl-4-isoxazolecarboxamido]-3,3-dimethyl-7-oxo-4-thia-1-azabicyclo [3.2.0]heptane-2-carboxylate monohydrate, and has following structural formula:
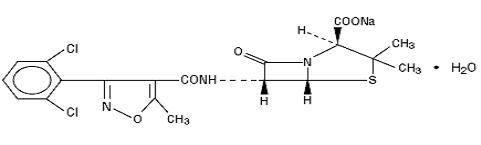
C 19H 16Cl 2N 3NaO 5 S·H 2O MW 510.32
Each capsule for oral administration contains dicloxacillin sodium, USP equivalent to 250 mg or 500 mg of dicloxacillin. The inactive ingredient is Magnesium Stearate. The capsule shells and print constituents contains D&C Yellow #10 Aluminum Lake, FD&C Blue #1 Aluminum Lake, FD&C Blue #1, FD&C Blue #2 Aluminum Lake, FD&C Red #40 Aluminum Lake, D&C Yellow #10, Gelatin, Shellac, Sodium Lauryl Sulfate, Sorbitan Monolaurate, Black Iron Oxide, Titanium Dioxide, Propylene Glycol.
-
CLINICAL PHARMACOLOGY
Microbiology
Mechanism of Action
Penicillinase-resistant penicillins exert a bactericidal action against penicillin-susceptible microorganisms during the state of active multiplication. All penicillins inhibit the biosynthesis of the bacterial cell wall.
Antibacterial Activity
Dicloxacillin sodium has been shown to be active against most isolates of the following microorganisms, both in vitro and in clinical infections as described in the INDICATIONS AND USAGE section.
Gram-positive Bacteria
Staphylococcus spp.
Susceptibility Testing
For specific information regarding susceptibility test interpretive criteria and associated test methods and quality control standards recognized by FDA for this drug, please see: https://www.fda.gov/STIC.
Pharmacokinetics
Dicloxacillin sodium is resistant to destruction by acid.
Absorption of dicloxacillin sodium after oral administration is rapid but incomplete; peak blood levels are achieved in 1 to 1.5 hours. In one study, after ingestion of a single 500 mg oral dose, peak serum concentrations range from 10 to 17 mcg/mL for dicloxacillin.
Oral absorption of dicloxacillin is delayed when the drugs are administered after meals.
Once absorbed, dicloxacillin sodium is 97.9 ± 0.6 percent bound to serum protein, mainly albumin. Dicloxacillin sodium vary in the extent to which they are distributed in the body fluids. With normal doses, insignificant concentrations are found in the cerebrospinal fluid and aqueous humor. Dicloxacillin sodium is found in therapeutic concentrations in the pleural, bile and amniotic fluids.
Dicloxacillin sodiumis rapidly excreted, primarily as unchanged drug in the urine by glomerular filtration and active tubular secretion. The elimination half-life for dicloxacillin is about 0.7 hour. Nonrenal elimination includes hepatic inactivation and excretion in bile.
Dicloxacillin is not dialyzable. Only minimal amounts are removed by hemodialysis or peritoneal dialysis.
-
INDICATIONS AND USAGE
To reduce the development of drug-resistant bacteria and maintain the effectiveness of dicloxacillin sodium capsules and other antibacterial drugs, dicloxacillin sodium capsules should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.
Dicloxacillin is indicated in the treatment of infections caused by penicillinase-producing staphylococci which have demonstrated susceptibility to the drug. Cultures and susceptibility tests should be performed initially to determine the causative organisms and their sensitivity to the drug (see CLINICAL PHARMACOLOGY – Susceptibility Testing) .
Dicloxacillin may be used to initiate therapy in suspected cases of resistant staphylococcal infections prior to the availability of laboratory test results. The penicillinase-resistant penicillins should not be used in infections caused by organisms susceptible to penicillin G. If the susceptibility tests indicate that the infection is due to an organism other than a resistant staphylococcus, therapy should not be continued with a penicillinase-resistant penicillin.
- CONTRAINDICATIONS
-
WARNINGS
Serious and occasionally fatal hypersensitivity (anaphylactic shock with collapse) reactions have occurred in patients receiving penicillin. The incidence of anaphylactic shock in all penicillin-treated patients is between 0.015% and 0.04%. Anaphylactic shock resulting in death has occurred in approximately 0.002% of the patients treated. Although anaphylaxis is more frequent following a parenteral administration, it has occurred in patients receiving oral penicillins.
When penicillin therapy is indicated, it should be initiated only after a comprehensive patient drug and allergy history has been obtained. If an allergic reaction occurs, dicloxacillin should be discontinued and appropriate therapy instituted. Individuals with a history of penicillin hypersensitivity may also experience allergic reactions when treated with a cephalosporin.
Clostridium difficile associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including dicloxacillin sodium, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile.
C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin producing strains of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibiotic use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents.
If CDAD is suspected or confirmed, ongoing antibiotic use not directed against C. difficile may need to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibiotic treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated.
-
PRECAUTIONS
General
Prescribing dicloxacillin sodium capsules in the absence of a proven or strongly suspected bacterial infection or a prophylactic indication is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria.
Dicloxacillin should generally not be administered to patients with a history of sensitivity to any penicillin.
Penicillin should be used with caution in individuals with histories of significant allergies and/or asthma.
There is clinical and laboratory evidence of partial cross-allergenicity among penicillins and other β-lactam antibiotics including cephalosporins, cephamycins, and other 1-oxa-β-lactams. Whenever allergic reactions occur, penicillin should be withdrawn unless, in the opinion of the physician, the condition being treated is life-threatening and amenable only to penicillin therapy.The oral route of administration should not be relied upon in patients with severe illness, or with nausea, vomiting, gastric dilatation, cardiospasm or intestinal hypermotility. Occasionally, patients will not absorb therapeutic amounts of orally administered penicillin.
Information for the Patient
Patients should be counselled that antibacterial drugs including dicloxacillin sodium capsules should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). When dicloxacillin sodium capsules are prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by dicloxacillin sodium capsules or other antibacterial drugs in the future.
Diarrhea is a common problem caused by antibiotics which usually ends when the antibiotic is discontinued. Sometimes after starting treatment with antibiotics, patients can develop watery and bloody stools (with or without stomach cramps and fever) even as late as two or more months after having taken the last dose of the antibiotic. If this occurs, patients should contact their physician as soon as possible.
Patients receiving penicillins should be given the following information and instructions by the physician:
- Patients should be told that penicillin is an antibacterial agent which will work with the body’s natural defenses to control certain types of infections. They should be told that the drug should not be taken if they have had an allergic reaction to any form of penicillin previously, and to inform the physician of any allergies or previous allergic reactions to any drugs they may have had (see WARNINGS).
- Patients who have previously experienced an anaphylactic reaction to penicillin should be instructed to wear a medical identification tag or bracelet.
- Because most antibacterial drugs taken by mouth are best absorbed on an empty stomach, patients should be directed, unless circumstances warrant otherwise, to take penicillin one hour before meals or two hours after eating (see CLINICAL PHARMACOLOGY - Pharmacokinetics).
- Patients should be told to take the entire course of therapy prescribed, even if fever and other symptoms have stopped (see PRECAUTIONS - General).
- If any of the following reactions occur, stop taking your prescription and notify the physician: shortness of breath, wheezing, skin rash, mouth irritation, black tongue, sore throat, nausea, vomiting, diarrhea, fever, swollen joints or any unusual bleeding or bruising (see ADVERSE REACTIONS).
- Do not take any additional medications without physician approval, including nonprescription drugs such as antacids, laxatives or vitamins.
Laboratory Tests
Bacteriologic studies to determine the causative organisms and their susceptibility to the penicillinase-resistant penicillins should be performed (see CLINICAL PHARMACOLOGY - Microbiology). In the treatment of suspected staphylococcal infections, therapy should be changed to another active agent if culture tests fail to demonstrate the presence of staphylococci.
Periodic assessment of organ system function, including renal, hepatic and hematopoietic, should be made during prolonged therapy with the penicillinase-resistant penicillins.
Blood cultures, white blood cell and differential cell counts should be obtained prior to initiation of therapy and at least weekly during therapy with penicillinase-resistant penicillins.
Periodic urinalysis, blood urea nitrogen and creatinine determinations should be performed during therapy with the penicillinase-resistant penicillins and dosage alterations should be considered if these values become elevated. If any impairment of renal function is suspected or known to exist, a reduction in the total dosage should be considered and blood levels monitored to avoid possible neurotoxic reactions (see DOSAGE AND ADMINISTRATION).
AST (SGOT) and ALT (SGPT) values should be obtained periodically during therapy to monitor for possible liver function abnormalities.
Drug Interactions
Tetracycline, a bacteriostatic antibiotic, may antagonize the bactericidal effect of penicillin and concurrent use of these drugs should be avoided.
Probenecid administered concomitantly with penicillins increases and prolongs serum penicillin levels (see DOSAGE AND ADMINISTRATION).
Penicillinase-resistant penicillins, like other penicillins, are physically and/or chemically incompatible with aminoglycosides and can inactivate the drugs in vitro. In vitro mixing of penicillins and aminoglycosides should be avoided during concomitant therapy and the drugs should be administered separately. Penicillins can inactivate aminoglycosides in vitro in serum samples from patients receiving both drugs, which could produce falsely decreased results in serum aminoglycoside assays of the serum samples.
Dicloxacillin may reduce the anticoagulant response to dicumarol and warfarin. Careful monitoring of prothrombin times is suggested during concomitant therapy, and dosage of the anticoagulant should be adjusted as required. The mechanism of this possible interaction is unclear, but may be due to hepatic enzyme induction.
Carcinogenesis, Mutagenesis, Impairment of Fertility
No long-term animal studies have been conducted with these drugs.
Studies on reproduction (nafcillin) in rats and rabbits reveal no fetal or maternal abnormalities before conception and continuously through weaning (one generation).
Pregnancy
Reproduction studies performed in the mouse, rat and rabbit have revealed no evidence of impaired fertility or harm to the fetus due to the penicillinase-resistant penicillins. Human experience with the penicillins during pregnancy has not shown any positive evidence of adverse effects on the fetus. There are, however, no adequate or well-controlled studies in pregnant women showing conclusively that harmful effects of these drugs on the fetus can be excluded. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.
Nursing Mothers
Penicillins are excreted in breast milk. Caution should be exercised when penicillins are administered to a nursing woman.
Pediatric Use
Because of incompletely developed renal function in newborns, penicillinase-resistant penicillins (especially methicillin) may not be completely excreted, with abnormally high blood levels resulting. Frequent monitoring of blood levels is advisable in this group, with dosage adjustments when necessary. All newborns treated with penicillins should be monitored closely for clinical and laboratory evidence of toxic or adverse effects (see DOSAGE AND ADMINISTRATION). Experience in the neonatal period is limited. Therefore a dose for the newborn is not recommended.
Geriatric Use
Clinical studies of dicloxacillin sodium capsules did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
-
Postmarketing
Experience
Rare reports have been received during postmarketing surveillance of esophageal burning, esophagitis, and esophageal ulceration, particularly after ingestion of dicloxacillin capsules with an insufficient quantity of water and/or before going to bed. To minimize the risk of developing such events, dicloxacillin should be taken with at least 4 fluid ounces (120 mL) of water and dicloxacillin should NOT be taken in the supine position or immediately before going to bed.
-
ADVERSE REACTIONS
Hypersensitive Reactions
The reported incidence of allergic reactions to penicillin ranges from 0.7% to 10% (see WARNINGS). Sensitization is usually the result of treatment, but some individuals have had immediate reactions to penicillin when first treated. In such cases, it is thought that the patients may have had prior exposure to the drug via trace amounts present in milk and vaccines.
Two types of allergic reactions to penicillin are noted clinically, immediate and delayed.
Immediate reactions usually occur within 20 minutes of administration and range in severity from urticaria and pruritus to angioneurotic edema, laryngospasm, bronchospasm, hypotension, vascular collapse and death. Such immediate anaphylactic reactions are very rare (see WARNINGS) and usually occur after parenteral therapy, but have occurred in patients receiving oral therapy. Another type of immediate reaction, an accelerated reaction, may occur between 20 minutes and 48 hours after administration and may include urticaria, pruritus and fever. Although laryngeal edema, laryngospasm and hypotension occasionally occur, fatality is uncommon.
Delayed allergic reactions to penicillin therapy usually occur after 48 hours and sometimes as late as two to four weeks after initiation of therapy. Manifestations of this type of reaction include serum sickness-like symptoms (i.e., fever, malaise, urticaria, myalgia, arthralgia, abdominal pain) and various skin rashes.
Gastrointestinal Reactions
Nausea, vomiting, diarrhea, stomatitis, black or hairy tongue and other symptoms of gastrointestinal irritation may occur, especially during oral penicillin therapy.
Pseudomembranous colitis has been reported with the use of dicloxacillin. Therefore, it is important to consider its diagnosis in patients who develop diarrhea in association with dicloxacillin use.
Reports have been received during postmarketing surveillance of esophageal burning, esophagitis, and esophageal ulceration, particularly after ingestion of dicloxacillin capsules with an insufficient quantity of water and/or before going to bed (see PRECAUTIONS and DOSAGE AND ADMINISTRATION).
Nervous System Reactions
Neurotoxic reactions similar to those observed with penicillin G (e.g., lethargy, confusion, twitching, multifocal myoclonus, localized or generalized epileptiform seizures) may occur with large intravenous doses of the penicillinase-resistant penicillins, especially with patients with renal insufficiency.
Renal Reactions
Renal tubular damage and interstitial nephritis have been associated with the administration of methicillin sodium and, infrequently, with the administration of nafcillin and oxacillin. Manifestations of this reaction may include rash, fever, eosinophilia, hematuria, proteinuria and renal insufficiency. Methicillin-induced nephropathy does not appear to be dose-related and is generally reversible upon prompt discontinuation of therapy.
Hematologic Reactions
Eosinophilia, hemolytic anemia, agranulocytosis, neutropenia, leukopenia, granulocytopenia, thrombocytopenia, and bone marrow depression have been associated with the use of penicillinase-resistant penicillins.
Hepatic Reactions
Hepatotoxicity, characterized by fever, nausea and vomiting associated with abnormal liver function tests, mainly elevated AST (SGOT) levels, has been associated with the use of oxacillin and cloxacillin. Chloestatic hepatitis has been reported rarely. Asymptomatic, transient increases in serum concentrations of alkaline phosphatase, AST (SGOT), and ALT (SGPT) have been reported.
-
DOSAGE AND ADMINISTRATION
Concurrent administration of the penicillinase-resistant penicillins and probenecid increases and prolongs serum penicillin levels.
Probenecid decreases the apparent volume of distribution and slows the rate of excretion by competitively inhibiting renal tubular secretion of penicillin. Penicillin-probenecid therapy is generally limited to those infections where very high serum levels of penicillin are necessary.
Oral preparations of the penicillinase-resistant penicillins should not be used as initial therapy in serious, life-threatening infections (see PRECAUTIONS - General). Oral therapy with the penicillinase-resistant penicillins may be used to follow up the previous use of a parenteral agent as soon as the clinical condition warrants.
RECOMMENDED DOSAGES FOR DICLOXACILLIN SODIUM IN MILD TO MODERATE AND SEVERE INFECTIONS DRUG
ADULTS
CHILDREN
Mild to Moderate
Severe
Mild to Moderate
Severe
Dicloxacillin
125 mg every
6 hours
250 mg every
6 hours
12.5 mg/kg/day 1 in equally divided doses every 6 hours
25 mg/kg/day 1 in equally divided doses every 6 hours
1. Patients weighing less than 40 kg (88 lbs)
Dicloxacillin is best absorbed when taken on an empty stomach, and should be administered at least 1 hour before or 2 hours after meals. Dicloxacillin should be taken with at least 4 fluid ounces (120 mL) of water and should not be taken in the supine position or immediately before going to bed (see PRECAUTIONS).
-
HOW SUPPLIED
Dicloxacillin Sodium Capsules USP are available as follows:
250 mg: Each capsule contains dicloxacillin sodium monohydrate equivalent to 250 mg dicloxacillin (anhydrous), with green colored cap and light green colored body, imprinted "TEVA" on the cap and “3123” on the body, available in:
NDC 55289-592-10 Bottles of 10 capsules
NDC 55289-592-20 Bottles of 20 capsules
NDC 55289-592-28 Bottles of 28 capsules
NDC 55289-592-40 Bottles of 40 capsules
Store at 20° to 25°C (68° to 77°F) [See USP Controlled Room Temperature].
Dispense in a tight, light-resistant container as defined in the USP, with a child-resistant closure (as required).
KEEP THIS AND ALL MEDICATIONS OUT OF THE REACH OF CHILDREN.
- Package/Label Display Panel
-
INGREDIENTS AND APPEARANCE
DICLOXACILLIN SODIUM
dicloxacillin sodium capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:55289-592(NDC:0093-3123) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength DICLOXACILLIN SODIUM (UNII: 4HZT2V9KX0) (DICLOXACILLIN - UNII:COF19H7WBK) DICLOXACILLIN 250 mg Inactive Ingredients Ingredient Name Strength MAGNESIUM STEARATE (UNII: 70097M6I30) D&C YELLOW NO. 10 ALUMINUM LAKE (UNII: CQ3XH3DET6) FD&C BLUE NO. 1 ALUMINUM LAKE (UNII: J9EQA3S2JM) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) FD&C BLUE NO. 2--ALUMINUM LAKE (UNII: 4AQJ3LG584) FD&C RED NO. 40 (UNII: WZB9127XOA) D&C YELLOW NO. 10 (UNII: 35SW5USQ3G) GELATIN (UNII: 2G86QN327L) SHELLAC (UNII: 46N107B71O) SODIUM LAURYL SULFATE (UNII: 368GB5141J) SORBITAN MONOLAURATE (UNII: 6W9PS8B71J) FERROSOFERRIC OXIDE (UNII: XM0M87F357) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) Product Characteristics Color green (light green) , green Score no score Shape CAPSULE Size 18mm Flavor Imprint Code TEVA;3123 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:55289-592-10 10 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 01/20/2011 2 NDC:55289-592-20 20 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 01/20/2011 3 NDC:55289-592-28 28 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 01/20/2011 4 NDC:55289-592-40 40 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 01/20/2011 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA062286 09/30/1990 Labeler - PD-Rx Pharmaceuticals, Inc. (156893695) Registrant - PD-Rx Pharmaceuticals, Inc. (156893695) Establishment Name Address ID/FEI Business Operations PD-Rx Pharmaceuticals, Inc. 156893695 repack(55289-592)