Label: ALTABAX- retapamulin ointment




- NDC Code(s): 16110-518-15, 16110-518-30
- Packager: Almirall, LLC
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: New Drug Application
Drug Label Information
Updated June 5, 2023
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use ALTABAX safely and effectively. See full prescribing information for ALTABAX.
ALTABAX (retapamulin ointment), for topical use
Initial U.S. Approval: 2007
INDICATIONS AND USAGE
ALTABAX, a pleuromutilin antibacterial, is indicated for the topical treatment of impetigo due to Staphylococcus aureus (methicillin-susceptible isolates only) or Streptococcus pyogenes in patients aged 9 months or older. (1) Safety in patients younger than 9 months has not been established.
DOSAGE AND ADMINISTRATION
DOSAGE FORMS AND STRENGTHS
10 mg retapamulin per 1g of ointment (1%) in 15- and 30-gram tubes (3)
CONTRAINDICATIONS
None. (4)
WARNINGS AND PRECAUTIONS
ADVERSE REACTIONS
The most common drug-related adverse reaction was application site irritation (less than or equal to 2% of subjects). (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Almirall at 1-866-665-2782 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 6/2023
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Local Irritation
5.2 Not for Systemic or Mucosal Use
5.3 Potential for Microbial Overgrowth
6 ADVERSE REACTIONS
6.1 Clinical Studies Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
12.4 Microbiology
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
15 REFERENCES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
ALTABAX® is indicated for use in adults and pediatric patients aged 9 months and older for the topical treatment of impetigo (up to 100 cm2 in total area in adults or 2% total body surface area in pediatric patients aged 9 months or older) due to Staphylococcus aureus (methicillin-susceptible isolates only) or Streptococcus pyogenes [see Clinical Studies (14)]. Safety in patients younger than 9 months has not been established.
To reduce the development of drug-resistant bacteria and maintain the effectiveness of ALTABAX and other antibacterial drugs, ALTABAX should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria.
-
2 DOSAGE AND ADMINISTRATION
A thin layer of ALTABAX should be applied to the affected area (up to 100 cm2 in total area in adults or 2% total body surface area in pediatric patients aged 9 months or older) twice daily for 5 days. The treated area may be covered with a sterile bandage or gauze dressing if desired [see Patient Counseling Information (17)].
- 3 DOSAGE FORMS AND STRENGTHS
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Local Irritation
In the event of sensitization or severe local irritation from ALTABAX, usage should be discontinued, the ointment wiped off, and appropriate alternative therapy for the infection instituted [see Patient Counseling Information (17)].
5.2 Not for Systemic or Mucosal Use
ALTABAX is not intended for ingestion or for oral, intranasal, ophthalmic, or intravaginal use. The efficacy and safety of ALTABAX on mucosal surfaces have not been established. Epistaxis has been reported with the use of ALTABAX on nasal mucosa.
5.3 Potential for Microbial Overgrowth
The use of antibiotics may promote the selection of nonsusceptible organisms. Should superinfection occur during therapy, appropriate measures should be taken.
Prescribing ALTABAX in the absence of a proven or strongly suspected bacterial infection is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria.
-
6 ADVERSE REACTIONS
6.1 Clinical Studies Experience
Because clinical trials are conducted under varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared with rates in the clinical trials of another drug and may not reflect the rates observed in practice. The adverse reaction information from the clinical trials does, however, provide a basis for identifying the adverse events that appear to be related to drug use and for approximating rates.
The safety profile of ALTABAX was assessed in 2,115 adult and pediatric subjects 9 months and older who used at least one dose from a 5-day, twice-a-day regimen of retapamulin ointment. Control groups included 819 adult and pediatric subjects who used at least one dose of the active control (oral cephalexin), 172 subjects who used an active topical comparator (not available in the US), and 71 subjects who used placebo.
Adverse events rated by investigators as drug-related occurred in 5.5% (116/2,115) of subjects treated with retapamulin ointment, 6.6% (54/819) of subjects receiving cephalexin, and 2.8% (2/71) of subjects receiving placebo. The most common drug-related adverse events (greater than or equal to 1% of subjects) were application site irritation (1.4%) in the retapamulin group, diarrhea (1.7%) in the cephalexin group, and application site pruritus (1.4%) and application site paresthesia (1.4%) in the placebo group.
Adults
The adverse events, regardless of attribution, reported in at least 1% of adults (aged 18 years and older) who received ALTABAX or comparator are presented in Table 1.
Table 1. Adverse Events Reported by ≥1% of Adult Subjects Treated with ALTABAX or Comparator in Phase 3 Clinical Trials Adverse Event ALTABAX
N = 1,527
%Cephalexin
N = 698
%Headache 2.0 2.0 Application site irritation 1.6 <1.0 Diarrhea 1.4 2.3 Nausea 1.2 1.9 Nasopharyngitis 1.2 <1.0 Creatinine phosphokinase increased <1.0 1.0 Pediatrics
The adverse events, regardless of attribution, reported in at least 1% of pediatric subjects aged 9 months to 17 years who received ALTABAX are presented in Table 2.
Table 2. Adverse Events Reported by ≥1% in Pediatric Subjects Aged 9 Months to 17 Years Treated with ALTABAX in Phase 3 Clinical Trials Adverse Event ALTABAX
N = 588
%Cephalexin
N = 121
%Placebo
N = 64
%Application site pruritus 1.9 0 0 Diarrhea 1.7 5.0 0 Nasopharyngitis 1.5 1.7 0 Pruritus 1.5 1.0 1.6 Eczema 1.0 0 0 Headache 1.2 1.7 0 Pyrexia 1.2 <1.0 1.6 Other Adverse Events
Application site pain, erythema, and contact dermatitis were reported in less than 1% of subjects in clinical trials.
6.2 Postmarketing Experience
In addition to reports in clinical trials, the following events have been identified during postmarketing use of ALTABAX. Because these events are reported voluntarily from a population of uncertain size, it is not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
General Disorders and Administration Site Conditions
Application site burning.
Immune System Disorders
Hypersensitivity including angioedema.
-
7 DRUG INTERACTIONS
Coadministration of oral ketoconazole 200 mg twice daily increased retapamulin geometric mean AUC(0-24) and Cmax by 81% after topical application of retapamulin ointment, 1% on the abraded skin of healthy adult males. Due to low systemic exposure to retapamulin following topical application in adults and pediatric patients aged 2 years and older, dosage adjustments for retapamulin are unnecessary in these patients when coadministered with CYP3A4 inhibitors, such as ketoconazole. Based on in vitro P450 inhibition studies and the low systemic exposure observed following topical application of ALTABAX, retapamulin is unlikely to affect the metabolism of other P450 substrates.
Concomitant administration of retapamulin and CYP3A4 inhibitors, such as ketoconazole, has not been studied in pediatric patients. In pediatric subjects aged 2 to 24 months, systemic exposure of retapamulin was higher compared with subjects aged 2 years and older after topical application [see Pharmacokinetics (12.3)]. Based on the higher exposure of retapamulin, it is not recommended to coadminister ALTABAX with strong CYP3A4 inhibitors in patients younger than 24 months.
The effect of concurrent application of ALTABAX and other topical products to the same area of skin has not been studied.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no available data on ALTABAX use in pregnant women to inform any drug associated risk for major birth defects, miscarriage or adverse maternal or fetal outcomes. Retapamulin is negligibly absorbed systemically following topical administration and maternal use is not expected to result in fetal exposure to the retapamulin [see Clinical Pharmacology (12.3)]. Animal reproduction studies were not conducted with ALTABAX. However, in animal studies where retapamulin was administered by oral gavage or intravenous infusion to pregnant rats and rabbits, respectively, during organogenesis, maternal toxicity was seen at doses greater than or equal to 150 mg/kg/day and 7.2 mg/kg/day (8-fold the maximum achievable human exposure based on AUC) for oral and intravenous routes, respectively. The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population the background risk of major birth defects in clinically recognized pregnancies is 2% to 4% and of miscarriage is 15% to 20%, respectively.
8.2 Lactation
Risk Summary
There are no data available on the presence of retapamulin in human milk, its effects on the breastfed infant or its effects on milk production. However, breastfeeding is not expected to result in exposure of the child to the drug due to the negligible systemic absorption of retapamulin in humans following topical administration of ALTABAX [see Clinical Pharmacology (12.3)].
The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for ALTABAX and any potential adverse effects on the breastfed infant from ALTABAX or from the underlying maternal condition.
8.4 Pediatric Use
The safety and effectiveness of ALTABAX in the treatment of impetigo have been established in pediatric patients aged 9 months to 17 years. Use of ALTABAX in pediatric patients (9 months to 17 years of age) is supported by evidence from adequate and well-controlled trials of ALTABAX in which 588 pediatric subjects received at least one dose of retapamulin ointment, 1% [see Adverse Reactions (6.1), Clinical Studies (14)]. The magnitude of efficacy and the safety profile of ALTABAX in pediatric subjects 9 months and older were similar to those in adults.
The safety and effectiveness of ALTABAX in pediatric patients younger than 9 months have not been established. An open-label clinical trial of topical treatment with ALTABAX (twice daily for 5 days) was conducted in subjects aged 2 to 24 months. Plasma samples were obtained from 79 subjects. In these pediatric subjects, systemic exposure of retapamulin was higher compared with subjects aged 2 to 17 years. Furthermore, a higher proportion of pediatric subjects aged 2 to 9 months had measurable concentrations (greater than 0.5 ng per mL) of retapamulin compared with subjects aged 9 to 24 months [see Pharmacokinetics (12.3)]. The highest levels were seen in subjects aged 2 to 6 months [see Pharmacokinetics (12.3)]. The use of retapamulin is not indicated in pediatric patients younger than 9 months.
8.5 Geriatric Use
Of the total number of subjects in the adequate and well-controlled trials of ALTABAX, 234 subjects were aged 65 years and older, of whom 114 subjects were aged 75 years and older. No overall differences in effectiveness or safety were observed between these subjects and younger adult subjects.
- 10 OVERDOSAGE
-
11 DESCRIPTION
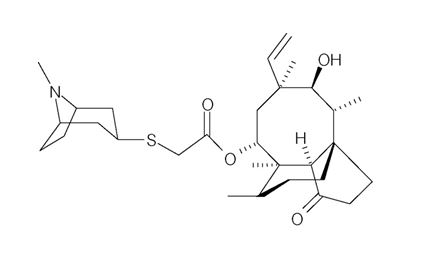
ALTABAX contains retapamulin, a semisynthetic pleuromutilin antibiotic. The chemical name of retapamulin is acetic acid, [[(3-exo)-8-methyl-8-azabicyclo[3.2.1]oct-3-yl]thio]-, (3aS,4R,5S,6S,8R,9R,9aR,10R)-6-ethenyldecahydro-5-hydroxy-4,6,9,10-tetramethyl-1-oxo-3a,9-propano-3aH-cyclopentacycloocten-8-yl ester. Retapamulin, a white to pale-yellow crystalline solid, has a molecular formula of C30H47NO4S, and a molecular weight of 517.78. The chemical structure is:
Each gram of ointment for dermatological use contains 10 mg of retapamulin in white petrolatum.
-
12 CLINICAL PHARMACOLOGY
12.2 Pharmacodynamics
In post-hoc analyses of manually over-read 12-lead ECGs from healthy subjects (N = 103), no significant effects on QT/QTc intervals were observed after topical application of retapamulin ointment on intact and abraded skin. Due to the low systemic exposure to retapamulin with topical application, QT prolongation in patients is unlikely [see Clinical Pharmacology (12.3)].
12.3 Pharmacokinetics
Absorption
In a trial of healthy adult subjects, retapamulin ointment, 1% was applied once daily to intact skin (800 cm2 surface area) and to abraded skin (200 cm2 surface area) under occlusion for up to 7 days. Systemic exposure following topical application of retapamulin through intact and abraded skin was low. Three percent of blood samples obtained on Day 1 after topical application to intact skin had measurable retapamulin concentrations (lower limit of quantitation 0.5 ng per mL); thus Cmax values on Day 1 could not be determined. Eighty-two percent of blood samples obtained on Day 7 after topical application to intact skin and 97% and 100% of blood samples obtained after topical application to abraded skin on Days 1 and 7, respectively, had measurable retapamulin concentrations. The median Cmax value in plasma after application to 800 cm2 of intact skin was 3.5 ng per mL on Day 7 (range: 1.2 to 7.8 ng per mL). The median Cmax value in plasma after application to 200 cm2 of abraded skin was 11.7 ng per mL on Day 1 (range: 5.6 to 22.1 ng per mL) and 9.0 ng per mL on Day 7 (range: 6.7 to 12.8 ng per mL).
Plasma samples were obtained from 380 adult subjects and 136 pediatric subjects (aged 2 to 17 years) who were receiving topical treatment with ALTABAX topically twice daily. Eleven percent had measurable retapamulin concentrations (lower limit of quantitation 0.5 ng per mL), of which the median concentration was 0.8 ng per mL. The maximum measured retapamulin concentration in adults was 10.7 ng per mL and in pediatric subjects (aged 2 to 17 years) was 18.5 ng per mL.
A single plasma sample was obtained from 79 pediatric subjects (aged 2 to 24 months) who were receiving topical treatment with ALTABAX twice daily. Forty-six percent had measurable retapamulin concentrations greater than 0.5 ng per mL) compared with 7% in pediatric subjects aged 2 to 17 years. A higher proportion (69%) of pediatric subjects aged 2 to 9 months had measurable concentrations of retapamulin compared with subjects aged 9 to 24 months (32%). Among pediatric subjects aged 2 to 9 months (n = 29), 4 subjects had retapamulin concentrations that were higher (greater than or equal to 26.9 ng per mL) than the maximum concentration observed in pediatric subjects aged 2 to 17 years (18.5 ng per mL). Among pediatric subjects aged 9 to 24 months (n = 50), 1 subject had a retapamulin concentration that was higher (95.1 ng per mL) than the maximum level observed in pediatric subjects aged 2 to 17 years.
Distribution
Retapamulin is approximately 94% bound to human plasma proteins, and the protein binding is independent of concentration. The apparent volume of distribution of retapamulin has not been determined in humans.
Metabolism
In vitro studies with human hepatocytes showed that the main routes of metabolism were mono-oxygenation and di-oxygenation. In vitro studies with human liver microsomes demonstrated that retapamulin is extensively metabolized to numerous metabolites, of which the predominant routes of metabolism were mono-oxygenation and N-demethylation. The major enzyme responsible for metabolism of retapamulin in human liver microsomes was cytochrome P450 3A4 (CYP3A4).
Elimination
Retapamulin elimination in humans has not been investigated due to low systemic exposure after topical application.
12.4 Microbiology
Retapamulin is a semisynthetic derivative of the compound pleuromutilin, which is isolated through fermentation from Clitopilus passeckerianus (formerly Pleurotus passeckerianus). In vitro activity of retapamulin against isolates of Staphylococcus aureus as well as Streptococcus pyogenes has been demonstrated.
Antimicrobial Mechanism of Action
Retapamulin selectively inhibits bacterial protein synthesis by interacting at a site on the 50S subunit of the bacterial ribosome through an interaction that is different from that of other antibiotics. This binding site involves ribosomal protein L3 and is in the region of the ribosomal P site and peptidyl transferase center. By virtue of binding to this site, pleuromutilins inhibit peptidyl transfer, block P-site interactions, and prevent the normal formation of active 50S ribosomal subunits. Retapamulin is bacteriostatic against Staphylococcus aureus and Streptococcus pyogenes at the retapamulin in vitro minimum inhibitory concentration (MIC) for these organisms. At concentrations 1,000 times the in vitro MIC, retapamulin is bactericidal against these same organisms. Although cross-resistance between retapamulin and other antibacterial classes (such as clindamycin and oxazolidones) exist, isolates resistant to these classes may be susceptible to retapamulin.
Mechanisms of Decreased Susceptibility to Retapamulin
In vitro, 2 mechanisms that cause reduced susceptibility to retapamulin have been identified, specifically, mutations in ribosomal protein L3, the presence of Cfr rRNA methyltransferase or the presence of an efflux mechanism. Decreased susceptibility of S. aureus to retapamulin (highest retapamulin MIC was 2 mcg per mL) develops slowly in vitro via multistep mutations in L3 after serial passage in sub-inhibitory concentrations of retapamulin. There was no apparent treatment-associated reduction in susceptibility to retapamulin in the Phase 3 clinical program. The clinical significance of these findings is not known.
Other
Based on in vitro broth microdilution susceptibility testing, no differences were observed in susceptibility of S. aureus to retapamulin whether the isolates were methicillin-resistant or methicillin-susceptible. Retapamulin susceptibility did not correlate with clinical success rates in patients with methicillin-resistant S. aureus. The reason for this is not known but may have been influenced by the presence of particular strains of S. aureus possessing certain virulence factors, such as Panton-Valentine Leukocidin (PVL). In the case of treatment failure associated with S. aureus (regardless of methicillin susceptibility), the presence of strains possessing additional virulence factors (such as PVL) should be considered.
Retapamulin has been shown to be active against the following microorganisms, both in vitro and in clinical trials [see Indications and Usage (1)].
Aerobic and Facultative Gram-Positive Bacteria: Staphylococcus aureus (methicillin-susceptible isolates only); Streptococcus pyogenes.
Susceptibility Testing
The clinical microbiology laboratory should provide cumulative results of the in vitro susceptibility test results for antimicrobial drugs used in local hospitals and practice areas to the physician as periodic reports that describe the susceptibility profile of nosocomial and community-acquired pathogens. These reports should aid the physician in selecting the most effective antimicrobial.
Susceptibility Testing Techniques:
Dilution Techniques: Quantitative methods can be used to determine the MIC of retapamulin that will inhibit the growth of the bacteria being tested. The MIC provides an estimate of the susceptibility of bacteria to retapamulin. The MIC should be determined using a standardized procedure.1,2 Standardized procedures are based on a dilution method (broth or agar) or equivalent with standardized inoculum concentrations and standardized concentrations of retapamulin powder.
Diffusion Techniques: Quantitative methods that require measurement of zone diameters also provide reproducible estimates of the susceptibility of bacteria to antimicrobial compounds. One such standardized procedure requires the use of standardized inoculum concentrations.2,3 This procedure uses paper disks impregnated with 2 mcg of retapamulin to test the susceptibility of microorganisms to retapamulin.
Susceptibility Test Interpretive Criteria: In vitro susceptibility test interpretive criteria for retapamulin have not been determined for this topical antimicrobial. The relation of the in vitro MIC and/or disk diffusion susceptibility test results to clinical efficacy of retapamulin against the bacteria tested should be monitored.
Quality Control Parameters for Susceptibility Testing: In vitro susceptibility test quality control parameters were developed for retapamulin so that laboratories that test the susceptibility of bacterial isolates to retapamulin can determine if the susceptibility test is performing correctly. Standardized dilution techniques and diffusion methods require the use of laboratory control microorganisms to monitor the technical aspects of the laboratory procedures. Standard retapamulin powder should provide the following MIC and a 2-mcg retapamulin disk should produce the following zone diameters with the indicated quality control strains in Table 3.
Table 3. Acceptable Quality Control Ranges for Retapamulin NA = Not applicable.
a This quality control range is applicable using cation-adjusted Mueller-Hinton broth with 2% to 5% lysed horse blood.
b This quality control limit is applicable using Mueller-Hinton agar with 5% sheep blood.Microorganism MIC Range
(mcg/mL)Disk Diffusion Zone Diameter (mm) Staphylococcus aureus ATCC 29213 0.06-0.25 NA Staphylococcus aureus ATCC 25923 NA 23-30 Streptococcus pneumoniae ATCC 49619 0.06-0.5a 13-19b -
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term studies in animals to evaluate carcinogenic potential have not been conducted with retapamulin.
Retapamulin showed no genotoxicity when evaluated in vitro for gene mutation and/or chromosomal effects in the mouse lymphoma cell assay, in cultured human peripheral blood lymphocytes, or when evaluated in vivo in a rat micronucleus test.
No evidence of impaired fertility was found in male or female rats given retapamulin 50, 150, or 450 mg per kg per day orally.
-
14 CLINICAL STUDIES
ALTABAX was evaluated in a placebo-controlled trial that enrolled adult and pediatric subjects aged 9 months and older for treatment of impetigo up to 100 cm2 in total area (up to 10 lesions) or a total body surface area not exceeding 2%. The majority of subjects enrolled (164/210, 78%) were under the age of 13. The trial was a double-blind, randomized, multi-center, parallel-group comparison of the safety of ALTABAX and placebo ointment, both applied twice daily for 5 days. Subjects were randomized to ALTABAX or placebo (2:1). Subjects with underlying skin disease (e.g., pre-existing eczematous dermatitis) or skin trauma, with clinical evidence of secondary infection, were excluded from these trials. In addition, subjects with any systemic signs and symptoms of infection (such as fever) were excluded from the trial. Clinical success was defined as the absence of treated lesions, or treated lesions had become dry without crusts with or without erythema compared with baseline, or had improved (defined as a decline in the size of the affected area, number of lesions or both) such that no further antimicrobial therapy was required. The intent-to-treat clinical (ITTC) population consisted of all randomized subjects who took at least 1 dose of trial medication. The clinical per protocol (PPC) population included all ITTC subjects who satisfied the inclusion/exclusion criteria and subsequently adhered to the protocol. The intent-to-treat bacteriological (ITTB) population consisted of all randomized subjects who took at least 1 dose of trial medication and had a pathogen identified at trial entry. The bacteriological per protocol (PPB) population included all ITTB subjects who satisfied the inclusion/exclusion criteria and subsequently adhered to the protocol.
Table 4 presents the results for clinical response at end of therapy (2 days after treatment) and follow-up (9 days after treatment), by analysis population.
Table 4. Clinical Response at End of Therapy and at Follow-Up by Analysis Population n = number with clinical success outcome, N = number in analysis population, PPC = Clinical Per Protocol Population, ITTC = Clinical Intent to Treat Population, PPB = Bacteriological Per Protocol Population, ITTB = Bacteriological Intent to Treat Population. Analysis
PopulationALTABAX Placebo Difference
in Success
Rates (%)95% CI
(%)n/N Success
Rate (%)n/N Success
Rate (%)End of Therapy PPC 111/124 89.5 33/62 53.2 36.3 (22.8, 49.8) ITTC 119/139 85.6 37/71 52.1 33.5 (20.5, 46.5) PPB 96/107 89.7 26/52 50.0 39.7 (25.0, 54.5) ITTB 101/114 88.6 28/57 49.1 39.5 (25.2, 53.7) Follow-Up PPC 98/119 82.4 25/58 43.1 39.2 (24.8, 53.7) ITTC 105/139 75.5 28/71 39.4 36.1 (22.7, 49.5) PPB 86/102 84.3 18/48 37.5 46.8 (31.4, 62.2) ITTB 91/114 79.8 19/57 33.3 46.5 (32.2, 60.8) Table 5 presents the clinical success at end of therapy and follow-up by baseline pathogen.
Table 5. Clinical Response at End of Therapy and Follow-Up for Subjects with Staphylococcus aureus and Streptococcus pyogenes at Baseline in the Per Protocol Bacteriological Population (PPB) n/N = Number of clinical successes/number of pathogens isolated at baseline. Pathogen ALTABAX Placebo n/N Success Rate (%) n/N Success Rate (%) End of Therapy Staphylococcus aureus
(Methicillin-susceptible)79/88 89.8 25/48 52.1 Streptococcus pyogenes 29/32 90.6 3/7 42.9 Follow-Up Staphylococcus aureus
(Methicillin-susceptible)71/84 84.5 19/44 43.2 Streptococcus pyogenes 29/32 90.6 2/6 33.3 Examination of age and gender subgroups did not identify differences in response to ALTABAX among these groups. The majority of subjects entered into this trial were classified as white/Caucasian or of Asian heritage; when response rates by racial subgroups were viewed across trials, differences in response to ALTABAX were not identified.
-
15 REFERENCES
- Clinical and Laboratory Standards Institute (CLSI). Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria that Grow Aerobically; Eleventh Edition. CLSI document M07-A11. Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087, USA, 2018.
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing; Twenty-ninth Edition. CLSI supplement M100-S29. Wayne, PA: Clinical Laboratory Standards Institute; 2019.
- CLSI. Performance Standards for Antimicrobial Disk Diffusion Susceptibility Tests; Thirteenth Edition. CLSI Document M02-A13. Wayne, PA: Clinical Laboratory Standards Institute; 2018.
- 16 HOW SUPPLIED/STORAGE AND HANDLING
-
17 PATIENT COUNSELING INFORMATION
Patients using ALTABAX and/or their guardians should receive the following information and instructions:
- Use ALTABAX as directed by the healthcare practitioner. As with any topical medication, patients and caregivers should wash their hands after application if the hands are not the area for treatment.
- ALTABAX is for external use only. Do not swallow ALTABAX or use it in the eyes, on the mouth or lips, inside the nose, or inside the female genital area.
- The treated area may be covered by a sterile bandage or gauze dressing, if desired. This may also be helpful for infants and young children who accidentally touch or lick the lesion site. A bandage will protect the treated area and avoid accidental transfer of ointment to the eyes or other areas.
- Use the medication for the full time recommended by the healthcare practitioner, even though symptoms may have improved.
- Notify the healthcare practitioner if there is no improvement in symptoms within 3 to 4 days after starting use of ALTABAX.
- ALTABAX may cause reactions at the site of application of the ointment. Inform the healthcare practitioner if the area of application worsens in irritation, redness, itching, burning, swelling, blistering, or oozing.
ALTABAX is a registered trademark of Almirall, S.A.
Almirall
Manufactured for: Almirall, LLC, Malvern, PA 19355
© 2019 Almirall, LLC. All rights reserved.
- PRINCIPAL DISPLAY PANEL - NDC: 16110-518-15 - 15 g Tube Label
- PRINCIPAL DISPLAY PANEL - NDC: 16110-518-15 - 15 g Carton Label
- PRINCIPAL DISPLAY PANEL - NDC: 16110-518-30 - 30 g Tube Label
- PRINCIPAL DISPLAY PANEL - NDC: 16110-518-30 - 30 g Carton Label
-
INGREDIENTS AND APPEARANCE
ALTABAX
retapamulin ointmentProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:16110-518 Route of Administration TOPICAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength RETAPAMULIN (UNII: 4MG6O8991R) (RETAPAMULIN - UNII:4MG6O8991R) RETAPAMULIN 10 mg in 1 g Inactive Ingredients Ingredient Name Strength PETROLATUM (UNII: 4T6H12BN9U) Product Characteristics Color WHITE Score Shape Size Flavor Imprint Code Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:16110-518-15 1 in 1 CARTON 05/01/2016 1 15 g in 1 TUBE; Type 0: Not a Combination Product 2 NDC:16110-518-30 1 in 1 CARTON 05/01/2016 2 30 g in 1 TUBE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA022055 05/01/2016 Labeler - Almirall, LLC (605425912)