Label: ZYTIGA- abiraterone acetate tablet
ZYTIGA- abiraterone acetate tablet, film coated


- NDC Code(s): 57894-150-12, 57894-150-25, 57894-195-06, 57894-195-15
- Packager: Janssen Biotech, Inc.
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: New Drug Application
Drug Label Information
Updated December 16, 2024
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use ZYTIGA safely and effectively. See full prescribing information for ZYTIGA.
ZYTIGA ®(abiraterone acetate) tablets, for oral use
Initial U.S. Approval: 2011INDICATIONS AND USAGE
DOSAGE AND ADMINISTRATION
Metastatic castration-resistant prostate cancer:
- ZYTIGA 1,000 mg orally once daily with prednisone 5 mg orally twicedaily. ( 2.1)
Metastatic castration-sensitive prostate cancer:
- ZYTIGA 1,000 mg orally once daily with prednisone 5 mg orally oncedaily. ( 2.2)
Patients receiving ZYTIGA should also receive a gonadotropin-releasing hormone (GnRH) analog concurrently or should have had bilateral orchiectomy. ZYTIGA tablets must be taken as a single dose once daily on an empty stomach. Do not eat food 2 hours before and 1 hour after taking ZYTIGA. The tablets must be swallowed whole with water. Do not crush or chew tablets. ( 2.3)
Dose Modification:
- For patients with baseline moderate hepatic impairment (Child-Pugh Class B), reduce the ZYTIGA starting dose to 250 mg once daily. ( 2.4)
- For patients who develop hepatotoxicity during treatment, hold ZYTIGA until recovery. Retreatment may be initiated at a reduced dose. ZYTIGA should be discontinued if patients develop severe hepatotoxicity. ( 2.4)
CONTRAINDICATIONS
None ( 4)
WARNINGS AND PRECAUTIONS
- Mineralocorticoid excess: Closely monitor patients with cardiovascular disease. Control hypertension and correct hypokalemia before treatment. Monitor blood pressure, serum potassium and symptoms of fluid retention at least monthly. ( 5.1)
- Adrenocortical insufficiency: Monitor for symptoms and signs of adrenocortical insufficiency. Increased dosage of corticosteroids may be indicated before, during and after stressful situations. ( 5.2)
- Hepatotoxicity: Can be severe and fatal. Monitor liver function and modify, interrupt, or discontinue ZYTIGA dosing as recommended. ( 5.3)
- Increased fractures and mortality in combination with radium Ra 223 dichloride: Use of ZYTIGA plus prednisone/prednisolone in combination with radium Ra 223 dichloride is not recommended. ( 5.4)
- Embryo-Fetal Toxicity: ZYTIGA can cause fetal harm. Advise males with female partners of reproductive potential to use effective contraception. ( 5.5, 8.1, 8.3)
- Hypoglycemia: Severe hypoglycemia has been reported in patients with pre-existing diabetes who are taking medications containing thiazolidinediones (including pioglitazone) or repaglinide. Monitor blood glucose in patients with diabetes and assess if antidiabetic agent dose modifications are required. ( 5.6)
ADVERSE REACTIONS
The most common adverse reactions (≥10%) are fatigue, arthralgia, hypertension, nausea, edema, hypokalemia, hot flush, diarrhea, vomiting, upper respiratory infection, cough, and headache. ( 6.1)
The most common laboratory abnormalities (>20%) are anemia, elevated alkaline phosphatase, hypertriglyceridemia, lymphopenia, hypercholesterolemia, hyperglycemia, and hypokalemia. ( 6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Janssen Biotech, Inc. at 1-800-526-7736 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
- CYP3A4 Inducers: Avoid concomitant strong CYP3A4 inducers during ZYTIGA treatment. If a strong CYP3A4 inducer must be co-administered, increase the ZYTIGA dosing frequency. ( 2.5, 7.1)
- CYP2D6 Substrates: Avoid co-administration of ZYTIGA with CYP2D6 substrates that have a narrow therapeutic index. If an alternative treatment cannot be used, exercise caution and consider a dose reduction of the concomitant CYP2D6 substrate. ( 7.2)
USE IN SPECIFIC POPULATIONS
- Do not use ZYTIGA in patients with baseline severe hepatic impairment (Child-Pugh Class C). ( 8.6)
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 11/2024
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dose for Metastatic CRPC
2.2 Recommended Dose for Metastatic High-risk CSPC
2.3 Important Administration Instructions
2.4 Dose Modification Guidelines in Hepatic Impairment and Hepatotoxicity
2.5 Dose Modification Guidelines for Strong CYP3A4 Inducers
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Hypokalemia, Fluid Retention, and Cardiovascular Adverse Reactions due to Mineralocorticoid Excess
5.2 Adrenocortical Insufficiency
5.3 Hepatotoxicity
5.4 Increased Fractures and Mortality in Combination with Radium Ra 223 Dichloride
5.5 Embryo-Fetal Toxicity
5.6 Hypoglycemia
6 ADVERSE REACTIONS
6.1 Clinical Trial Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
7.1 Drugs that Inhibit or Induce CYP3A4 Enzymes
7.2 Effects of Abiraterone on Drug Metabolizing Enzymes
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Patients with Hepatic Impairment
8.7 Patients with Renal Impairment
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, and Impairment of Fertility
13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
- 1 INDICATIONS AND USAGE
-
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dose for Metastatic CRPC
The recommended dose of ZYTIGA is 1,000 mg (two 500 mg tablets or four 250 mg tablets) orally once daily with prednisone 5 mg orally twice daily.
2.2 Recommended Dose for Metastatic High-risk CSPC
The recommended dose of ZYTIGA is 1,000 mg (two 500 mg tablets or four 250 mg tablets) orally once daily with prednisone 5 mg administered orally once daily.
2.3 Important Administration Instructions
Patients receiving ZYTIGA should also receive a gonadotropin-releasing hormone (GnRH) analog concurrently or should have had bilateral orchiectomy.
ZYTIGA tablets must be taken as a single dose once daily on an empty stomach. Do not eat food 2 hours before and 1 hour after taking ZYTIGA. The tablets must be swallowed whole with water. Do not crush or chew tablets.
2.4 Dose Modification Guidelines in Hepatic Impairment and Hepatotoxicity
Hepatic Impairment
In patients with baseline moderate hepatic impairment (Child-Pugh Class B), reduce the recommended dose of ZYTIGA to 250 mg once daily. In patients with moderate hepatic impairment monitor ALT, AST, and bilirubin prior to the start of treatment, every week for the first month, every two weeks for the following two months of treatment and monthly thereafter. If elevations in ALT and/or AST greater than 5 × upper limit of normal (ULN) or total bilirubin greater than 3 × ULN occur in patients with baseline moderate hepatic impairment, discontinue ZYTIGA and do not re-treat patients with ZYTIGA [see Use in Specific Populations (8.6)and Clinical Pharmacology (12.3)] .
Do not use ZYTIGA in patients with baseline severe hepatic impairment (Child-Pugh Class C).
Hepatotoxicity
For patients who develop hepatotoxicity during treatment with ZYTIGA (ALT and/or AST greater than 5 × ULN or total bilirubin greater than 3 × ULN), interrupt treatment with ZYTIGA [see Warnings and Precautions (5.3)]. Treatment may be restarted at a reduced dose of 750 mg once daily following return of liver function tests to the patient's baseline or to AST and ALT less than or equal to 2.5 × ULN and total bilirubin less than or equal to 1.5 × ULN .For patients who resume treatment, monitor serum transaminases and bilirubin at a minimum of every two weeks for three months and monthly thereafter.
If hepatotoxicity recurs at the dose of 750 mg once daily, re-treatment may be restarted at a reduced dose of 500 mg once daily following return of liver function tests to the patient's baseline or to AST and ALT less than or equal to 2.5 × ULN and total bilirubin less than or equal to 1.5 × ULN .
If hepatotoxicity recurs at the reduced dose of 500 mg once daily, discontinue treatment with ZYTIGA.
Permanently discontinue ZYTIGA for patients who develop a concurrent elevation of ALT greater than 3 × ULN and total bilirubin greater than 2 × ULN in the absence of biliary obstruction or other causes responsible for the concurrent elevation [see Warnings and Precautions (5.3)] .
2.5 Dose Modification Guidelines for Strong CYP3A4 Inducers
Avoid concomitant strong CYP3A4 inducers (e.g., phenytoin, carbamazepine, rifampin, rifabutin, rifapentine, phenobarbital) during ZYTIGA treatment.
If a strong CYP3A4 inducer must be co-administered, increase the ZYTIGA dosing frequency to twice a day only during the co-administration period (e.g., from 1,000 mg once daily to 1,000 mg twice a day). Reduce the dose back to the previous dose and frequency, if the concomitant strong CYP3A4 inducer is discontinued [see Drug Interactions (7.1)and Clinical Pharmacology (12.3)] .
- 3 DOSAGE FORMS AND STRENGTHS
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Hypokalemia, Fluid Retention, and Cardiovascular Adverse Reactions due to Mineralocorticoid Excess
ZYTIGA may cause hypertension, hypokalemia, and fluid retention as a consequence of increased mineralocorticoid levels resulting from CYP17 inhibition [see Clinical Pharmacology (12.1)] . Monitor patients for hypertension, hypokalemia, and fluid retention at least once a month. Control hypertension and correct hypokalemia before and during treatment with ZYTIGA.
In the combined data from 4 placebo-controlled trials using prednisone 5 mg twice daily in combination with 1,000 mg abiraterone acetate daily, grades 3–4 hypokalemia were detected in 4% of patients on the ZYTIGA arm and 2% of patients on the placebo arm. Grades 3–4 hypertension were observed in 2% of patients each arm and grades 3–4 fluid retention in 1% of patients each arm.
In LATITUDE (a randomized placebo-controlled, multicenter clinical trial), which used prednisone 5 mg daily in combination with 1,000 mg abiraterone acetate daily, grades 3–4 hypokalemia were detected in 10% of patients on the ZYTIGA arm and 1% of patients on the placebo arm, grades 3–4 hypertension were observed in 20% of patients on the ZYTIGA arm and 10% of patients on the placebo arm. Grades 3–4 fluid retention occurred in 1% of patients each arm [see Adverse Reactions (6)] .
Closely monitor patients whose underlying medical conditions might be compromised by increases in blood pressure, hypokalemia or fluid retention, such as those with heart failure, recent myocardial infarction, cardiovascular disease, or ventricular arrhythmia. In postmarketing experience, QT prolongation and Torsades de Pointes have been observed in patients who develop hypokalemia while taking ZYTIGA.
The safety of ZYTIGA in patients with left ventricular ejection fraction <50% or New York Heart Association (NYHA) Class III or IV heart failure (in COU-AA-301) or NYHA Class II to IV heart failure (in COU-AA-302 and LATITUDE) has not been established because these patients were excluded from these randomized clinical trials [see Clinical Studies (14)] .
5.2 Adrenocortical Insufficiency
Adrenal insufficiency occurred in 0.3% of 2230 patients taking ZYTIGA and in 0.1% of 1763 patients taking placebo in the combined data of the 5 randomized, placebo-controlled clinical studies. Adrenocortical insufficiency was reported in patients receiving ZYTIGA in combination with prednisone, following interruption of daily steroids and/or with concurrent infection or stress.
Monitor patients for symptoms and signs of adrenocortical insufficiency, particularly if patients are withdrawn from prednisone, have prednisone dose reductions, or experience unusual stress. Symptoms and signs of adrenocortical insufficiency may be masked by adverse reactions associated with mineralocorticoid excess seen in patients treated with ZYTIGA. If clinically indicated, perform appropriate tests to confirm the diagnosis of adrenocortical insufficiency. Increased dosage of corticosteroids may be indicated before, during and after stressful situations [see Warnings and Precautions (5.1)].
5.3 Hepatotoxicity
In postmarketing experience, there have been ZYTIGA-associated severe hepatic toxicity, including fulminant hepatitis, acute liver failure and deaths [see Adverse Reactions (6.2)] .
In the combined data of 5 randomized clinical trials, grade 3–4 ALT or AST increases (at least 5 × ULN) were reported in 6% of 2230 patients who received ZYTIGA, typically during the first 3 months after starting treatment. Patients whose baseline ALT or AST were elevated were more likely to experience liver test elevation than those beginning with normal values. Treatment discontinuation due to ALT and AST increases or abnormal hepatic function occurred in 1.1% of 2230 patients taking ZYTIGA. In these clinical trials, no deaths clearly related to ZYTIGA were reported due to hepatotoxicity events.
Measure serum transaminases (ALT and AST) and bilirubin levels prior to starting treatment with ZYTIGA, every two weeks for the first three months of treatment and monthly thereafter. In patients with baseline moderate hepatic impairment receiving a reduced ZYTIGA dose of 250 mg, measure ALT, AST, and bilirubin prior to the start of treatment, every week for the first month, every two weeks for the following two months of treatment and monthly thereafter. Promptly measure serum total bilirubin, AST, and ALT if clinical symptoms or signs suggestive of hepatotoxicity develop. Elevations of AST, ALT, or bilirubin from the patient's baseline should prompt more frequent monitoring. If at any time AST or ALT rise above five times the ULN, or the bilirubin rises above three times the ULN, interrupt ZYTIGA treatment and closely monitor liver function.
Re-treatment with ZYTIGA at a reduced dose level may take place only after return of liver function tests to the patient's baseline or to AST and ALT less than or equal to 2.5 × ULN and total bilirubin less than or equal to 1.5 × ULN [see Dosage and Administration (2.4)] .
Permanently discontinue ZYTIGA for patients who develop a concurrent elevation of ALT greater than 3 × ULN and total bilirubin greater than 2 × ULN in the absence of biliary obstruction or other causes responsible for the concurrent elevation [see Dosage and Administration (2.4)] .
The safety of ZYTIGA re-treatment of patients who develop AST or ALT greater than or equal to 20 × ULN and/or bilirubin greater than or equal to 10 × ULN is unknown.
5.4 Increased Fractures and Mortality in Combination with Radium Ra 223 Dichloride
ZYTIGA plus prednisone/prednisolone is not recommended for use in combination with radium Ra 223 dichloride outside of clinical trials.
The clinical efficacy and safety of concurrent initiation of ZYTIGA plus prednisone/prednisolone and radium Ra 223 dichloride was assessed in a randomized, placebo-controlled multicenter study (ERA-223 trial) in 806 patients with asymptomatic or mildly symptomatic castration-resistant prostate cancer with bone metastases. The study was unblinded early based on an Independent Data Monitoring Committee recommendation.
At the primary analysis, increased incidences of fractures (28.6% vs 11.4%) and deaths (38.5% vs 35.5%) have been observed in patients who received ZYTIGA plus prednisone/prednisolone in combination with radium Ra 223 dichloride compared to patients who received placebo in combination with ZYTIGA plus prednisone/prednisolone.
5.5 Embryo-Fetal Toxicity
The safety and efficacy of ZYTIGA have not been established in females. Based on animal reproductive studies and mechanism of action, ZYTIGA can cause fetal harm and loss of pregnancy when administered to a pregnant female. In animal reproduction studies, oral administration of abiraterone acetate to pregnant rats during organogenesis caused adverse developmental effects at maternal exposures approximately ≥ 0.03 times the human exposure (AUC) at the recommended dose. Advise males with female partners of reproductive potential to use effective contraception during treatment with ZYTIGA and for 3 weeks after the last dose of ZYTIGA [see Use in Specific Populations (8.1, 8.3)] . ZYTIGA should not be handled by females who are or may become pregnant [see How Supplied/Storage and Handling (16)].
5.6 Hypoglycemia
Severe hypoglycemia has been reported when ZYTIGA was administered to patients with pre-existing diabetes receiving medications containing thiazolidinediones (including pioglitazone) or repaglinide [see Drug Interactions (7.2)] . Monitor blood glucose in patients with diabetes during and after discontinuation of treatment with ZYTIGA. Assess if antidiabetic drug dosage needs to be adjusted to minimize the risk of hypoglycemia.
-
6 ADVERSE REACTIONS
The following are discussed in more detail in other sections of the labeling:
- Hypokalemia, Fluid Retention, and Cardiovascular Adverse Reactions due to Mineralocorticoid Excess [see Warnings and Precautions (5.1)] .
- Adrenocortical Insufficiency [see Warnings and Precautions (5.2)] .
- Hepatotoxicity [see Warnings and Precautions (5.3)] .
- Increased Fractures and Mortality in Combination with Radium Ra 223 Dichloride [see Warnings and Precautions (5.4)].
6.1 Clinical Trial Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
Two randomized placebo-controlled, multicenter clinical trials (COU-AA-301 and COU-AA-302) enrolled patients who had metastatic CRPC in which ZYTIGA was administered orally at a dose of 1,000 mg daily in combination with prednisone 5 mg twice daily in the active treatment arms. Placebo plus prednisone 5 mg twice daily was given to patients on the control arm. A third randomized placebo-controlled, multicenter clinical trial (LATITUDE) enrolled patients who had metastatic high-risk CSPC in which ZYTIGA was administered at a dose of 1,000 mg daily in combination with prednisone 5 mg once daily. Placebos were administered to patients in the control arm. Additionally, two other randomized, placebo-controlled trials were conducted in patients with metastatic CRPC. The safety data pooled from 2230 patients in the 5 randomized controlled trials constitute the basis for the data presented in the Warnings and Precautions, Grade 1–4 adverse reactions, and Grade 1–4 laboratory abnormalities. In all trials, a gonadotropin-releasing hormone (GnRH) analog or prior orchiectomy was required in both arms.
In the pooled data, median treatment duration was 11 months (0.1, 43) for ZYTIGA-treated patients and 7.2 months (0.1, 43) for placebo-treated patients. The most common adverse reactions (≥10%) that occurred more commonly (>2%) in the ZYTIGA arm were fatigue, arthralgia, hypertension, nausea, edema, hypokalemia, hot flush, diarrhea, vomiting, upper respiratory infection, cough, and headache. The most common laboratory abnormalities (>20%) that occurred more commonly (≥2%) in the ZYTIGA arm were anemia, elevated alkaline phosphatase, hypertriglyceridemia, lymphopenia, hypercholesterolemia, hyperglycemia, and hypokalemia. Grades 3–4 adverse events were reported for 53% of patients in the ZYTIGA arm and 46% of patients in the placebo arm. Treatment discontinuation was reported in 14% of patients in the ZYTIGA arm and 13% of patients in the placebo arm. The common adverse events (≥1%) resulting in discontinuation of ZYTIGA and prednisone were hepatotoxicity and cardiac disorders.
Deaths associated with treatment-emergent adverse events were reported for 7.5% of patients in the ZYTIGA arm and 6.6% of patients in the placebo arm. Of the patients in the ZYTIGA arm, the most common cause of death was disease progression (3.3%). Other reported causes of death in ≥5 patients included pneumonia, cardio-respiratory arrest, death (no additional information), and general physical health deterioration.
COU-AA-301: Metastatic CRPC Following Chemotherapy
COU-AA-301 enrolled 1195 patients with metastatic CRPC who had received prior docetaxel chemotherapy. Patients were not eligible if AST and/or ALT ≥2.5 × ULN in the absence of liver metastases. Patients with liver metastases were excluded if AST and/or ALT >5 × ULN.
Table 1 shows adverse reactions on the ZYTIGA arm in COU-AA-301 that occurred with a ≥2% absolute increase in frequency compared to placebo or were events of special interest. The median duration of treatment with ZYTIGA with prednisone was 8 months.
Table 1: Adverse Reactions due to ZYTIGA in COU-AA-301 ZYTIGA with Prednisone
(N=791)Placebo with Prednisone
(N=394)System/Organ Class All Grades * Grade 3–4 All Grades Grade 3–4 Adverse reaction % % % % - *
- Adverse events graded according to CTCAE version 3.0.
- †
- Includes terms Arthritis, Arthralgia, Joint swelling, and Joint stiffness.
- ‡
- Includes terms Muscle spasms, Musculoskeletal pain, Myalgia, Musculoskeletal discomfort, and Musculoskeletal stiffness.
- §
- Includes terms Edema, Edema peripheral, Pitting edema, and Generalized edema.
- ¶
- Includes all fractures with the exception of pathological fracture.
- #
- Includes terms Arrhythmia, Tachycardia, Atrial fibrillation, Supraventricular tachycardia, Atrial tachycardia, Ventricular tachycardia, Atrial flutter, Bradycardia, Atrioventricular block complete, Conduction disorder, and Bradyarrhythmia.
- Þ
- Includes terms Angina pectoris, Chest pain, and Angina unstable. Myocardial infarction or ischemia occurred more commonly in the placebo arm than in the ZYTIGA arm (1.3% vs. 1.1% respectively).
- ß
- Includes terms Cardiac failure, Cardiac failure congestive, Left ventricular dysfunction, Cardiogenic shock, Cardiomegaly, Cardiomyopathy, and Ejection fraction decreased.
Musculoskeletal and connective tissue disorders Joint swelling/discomfort † 30 4.2 23 4.1 Muscle discomfort ‡ 26 3.0 23 2.3 General disorders Edema § 27 1.9 18 0.8 Vascular disorders Hot flush 19 0.3 17 0.3 Hypertension 8.5 1.3 6.9 0.3 Gastrointestinal disorders Diarrhea 18 0.6 14 1.3 Dyspepsia 6.1 0 3.3 0 Infections and infestations Urinary tract infection 12 2.1 7.1 0.5 Upper respiratory tract infection 5.4 0 2.5 0 Respiratory, thoracic and mediastinal disorders Cough 11 0 7.6 0 Renal and urinary disorders Urinary frequency 7.2 0.3 5.1 0.3 Nocturia 6.2 0 4.1 0 Injury, poisoning and procedural complications Fractures ¶ 5.9 1.4 2.3 0 Cardiac disorders Arrhythmia # 7.2 1.1 4.6 1.0 Chest pain or chest discomfort Þ 3.8 0.5 2.8 0 Cardiac failure ß 2.3 1.9 1.0 0.3 Table 2 shows laboratory abnormalities of interest from COU-AA-301.
Table 2: Laboratory Abnormalities of Interest in COU-AA-301 ZYTIGA with Prednisone (N=791) Placebo with Prednisone
(N=394)Laboratory Abnormality All Grades (%) Grade 3–4 (%) All Grades (%) Grade 3–4 (%) Hypertriglyceridemia 63 0.4 53 0 High AST 31 2.1 36 1.5 Hypokalemia 28 5.3 20 1.0 Hypophosphatemia 24 7.2 16 5.8 High ALT 11 1.4 10 0.8 High Total Bilirubin 6.6 0.1 4.6 0 COU-AA-302: Metastatic CRPC Prior to Chemotherapy
COU-AA-302 enrolled 1088 patients with metastatic CRPC who had not received prior cytotoxic chemotherapy. Patients were ineligible if AST and/or ALT ≥2.5 × ULN and patients were excluded if they had liver metastases.
Table 3 shows adverse reactions on the ZYTIGA arm in COU-AA-302 that occurred in ≥5% of patients with a ≥2% absolute increase in frequency compared to placebo. The median duration of treatment with ZYTIGA with prednisone was 13.8 months.
Table 3: Adverse Reactions in ≥5% of Patients on the ZYTIGA Arm in COU-AA-302 ZYTIGA with Prednisone (N=542) Placebo with Prednisone (N=540) System/Organ Class All Grades * Grade 3–4 All Grades Grade 3–4 Adverse reaction % % % % General disorders Fatigue 39 2.2 34 1.7 Edema † 25 0.4 21 1.1 Pyrexia 8.7 0.6 5.9 0.2 Musculoskeletal and connective tissue disorders Joint swelling/discomfort ‡ 30 2.0 25 2.0 Groin pain 6.6 0.4 4.1 0.7 Gastrointestinal disorders Constipation 23 0.4 19 0.6 Diarrhea 22 0.9 18 0.9 Dyspepsia 11 0.0 5.0 0.2 Vascular disorders Hot flush 22 0.2 18 0.0 Hypertension 22 3.9 13 3.0 Respiratory, thoracic and mediastinal disorders Cough 17 0.0 14 0.2 Dyspnea 12 2.4 9.6 0.9 Psychiatric disorders Insomnia 14 0.2 11 0.0 Injury, poisoning and procedural complications Contusion 13 0.0 9.1 0.0 Falls 5.9 0.0 3.3 0.0 Infections and infestations Upper respiratory tract infection 13 0.0 8.0 0.0 Nasopharyngitis 11 0.0 8.1 0.0 Renal and urinary disorders Hematuria 10 1.3 5.6 0.6 Skin and subcutaneous tissue disorders Rash 8.1 0.0 3.7 0.0 Table 4 shows laboratory abnormalities that occurred in greater than 15% of patients, and more frequently (>5%) in the ZYTIGA arm compared to placebo in COU-AA-302.
Table 4: Laboratory Abnormalities in >15% of Patients in the ZYTIGA Arm of COU-AA-302 ZYTIGA with Prednisone
(N=542)Placebo with Prednisone
(N=540)Laboratory Abnormality Grade 1–4
%Grade 3–4
%Grade 1–4
%Grade 3–4
%- *
- Based on non-fasting blood draws
Hematology Lymphopenia 38 8.7 32 7.4 Chemistry Hyperglycemia * 57 6.5 51 5.2 High ALT 42 6.1 29 0.7 High AST 37 3.1 29 1.1 Hypernatremia 33 0.4 25 0.2 Hypokalemia 17 2.8 10 1.7 LATITUDE: Patients with Metastatic High-risk CSPC
LATITUDE enrolled 1199 patients with newly-diagnosed metastatic, high-risk CSPC who had not received prior cytotoxic chemotherapy. Patients were ineligible if AST and/or ALT ≥2.5 × ULN or if they had liver metastases. All the patients received GnRH analogs or had prior bilateral orchiectomy during the trial. The median duration of treatment with ZYTIGA and prednisone was 24 months.
Table 5 shows adverse reactions on the ZYTIGA arm that occurred in ≥5% of patients with a ≥2% absolute increase in frequency compared to those on the placebos arm.
Table 5: Adverse Reactions in ≥5% of Patients on the ZYTIGA Arm in LATITUDE * ZYTIGA with Prednisone
(N=597)Placebos
(N=602)System/Organ Class
Adverse reactionAll Grades †
%Grade 3–4
%All Grades
%Grade 3–4
%Vascular disorders Hypertension 37 20 13 10 Hot flush 15 0.0 13 0.2 Metabolism and nutrition disorders Hypokalemia 20 10 3.7 1.3 Investigations Alanine aminotransferase increased ‡ 16 5.5 13 1.3 Aspartate aminotransferase increased ‡ 15 4.4 11 1.5 Infections and infestations Urinary tract infection 7.0 1.0 3.7 0.8 Upper respiratory tract infection 6.7 0.2 4.7 0.2 Nervous system disorders Headache 7.5 0.3 5.0 0.2 Respiratory, Thoracic and Mediastinal Disorders Cough § 6.5 0.0 3.2 0 Table 6 shows laboratory abnormalities that occurred in >15% of patients, and more frequently (>5%) in the ZYTIGA arm compared to placebos.
Table 6: Laboratory Abnormalities in >15% of Patients in the ZYTIGA Arm of LATITUDE ZYTIGA with Prednisone
(N=597)Placebos
(N=602)Laboratory Abnormality Grade 1–4
%Grade 3–4
%Grade 1–4
%Grade 3–4
%Hematology Lymphopenia 20 4.1 14 1.8 Chemistry Hypokalemia 30 9.6 6.7 1.3 Elevated ALT 46 6.4 45 1.3 Elevated total bilirubin 16 0.2 6.2 0.2 Cardiovascular Adverse Reactions
In the combined data of 5 randomized, placebo-controlled clinical studies, cardiac failure occurred more commonly in patients on the ZYTIGA arm compared to patients on the placebo arm (2.6% versus 0.9%). Grade 3–4 cardiac failure occurred in 1.3% of patients taking ZYTIGA and led to 5 treatment discontinuations and 4 deaths. Grade 3–4 cardiac failure occurred in 0.2% of patients taking placebo. There were no treatment discontinuations and two deaths due to cardiac failure in the placebo group.
In the same combined data, the majority of arrhythmias were grade 1 or 2. There was one death associated with arrhythmia and three patients with sudden death in the ZYTIGA arms and five deaths in the placebo arms. There were 7 (0.3%) deaths due to cardiorespiratory arrest in the ZYTIGA arms and 2 (0.1%) deaths in the placebo arms. Myocardial ischemia or myocardial infarction led to death in 3 patients in the placebo arms and 3 deaths in the ZYTIGA arms.
6.2 Postmarketing Experience
The following additional adverse reactions have been identified during post approval use of ZYTIGA with prednisone. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Respiratory, Thoracic and Mediastinal Disorders:non-infectious pneumonitis.
Musculoskeletaland Connective Tissue Disorders:myopathy, including rhabdomyolysis.
Hepatobiliary Disorders:fulminant hepatitis, including acute hepatic failure and death.
Cardiac Disorders:QT prolongation and Torsades de Pointes (observed in patients who developed hypokalemia or had underlying cardiovascular conditions).
Immune System Disorders – Hypersensitivity:anaphylactic reactions (severe allergic reactions that include, but are not limited to difficulty swallowing or breathing, swollen face, lips, tongue or throat, or an itchy rash (urticaria)).
-
7 DRUG INTERACTIONS
7.1 Drugs that Inhibit or Induce CYP3A4 Enzymes
Based on in vitrodata, ZYTIGA is a substrate of CYP3A4.
In a dedicated drug interaction trial, co-administration of rifampin, a strong CYP3A4 inducer, decreased exposure of abiraterone by 55%. Avoid concomitant strong CYP3A4 inducers during ZYTIGA treatment. If a strong CYP3A4 inducer must be co-administered, increase the ZYTIGA dosing frequency [see Dosage and Administration (2.5)and Clinical Pharmacology (12.3)] .
In a dedicated drug interaction trial, co-administration of ketoconazole, a strong inhibitor of CYP3A4, had no clinically meaningful effect on the pharmacokinetics of abiraterone [see Clinical Pharmacology (12.3)] .
7.2 Effects of Abiraterone on Drug Metabolizing Enzymes
ZYTIGA is an inhibitor of the hepatic drug-metabolizing enzymes CYP2D6 and CYP2C8. In a CYP2D6 drug-drug interaction trial, the C maxand AUC of dextromethorphan (CYP2D6 substrate) were increased 2.8- and 2.9-fold, respectively, when dextromethorphan was given with abiraterone acetate 1,000 mg daily and prednisone 5 mg twice daily. Avoid co-administration of abiraterone acetate with substrates of CYP2D6 with a narrow therapeutic index (e.g., thioridazine). If alternative treatments cannot be used, consider a dose reduction of the concomitant CYP2D6 substrate drug [see Clinical Pharmacology (12.3)] .
In a CYP2C8 drug-drug interaction trial in healthy subjects, the AUC of pioglitazone (CYP2C8 substrate) was increased by 46% when pioglitazone was given together with a single dose of 1,000 mg abiraterone acetate. Therefore, patients should be monitored closely for signs of toxicity related to a CYP2C8 substrate with a narrow therapeutic index if used concomitantly with ZYTIGA [see Clinical Pharmacology (12.3)and Warnings and Precautions (5.6)] .
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
The safety and efficacy of ZYTIGA have not been established in females. Based on findings from animal studies and the mechanism of action, ZYTIGA can cause fetal harm and potential loss of pregnancy.
There are no human data on the use of ZYTIGA in pregnant women. In animal reproduction studies, oral administration of abiraterone acetate to pregnant rats during organogenesis caused adverse developmental effects at maternal exposures approximately ≥ 0.03 times the human exposure (AUC) at the recommended dose (see Data).
Data
Animal Data
In an embryo-fetal developmental toxicity study in rats, abiraterone acetate caused developmental toxicity when administered at oral doses of 10, 30 or 100 mg/kg/day throughout the period of organogenesis (gestational days 6–17). Findings included embryo-fetal lethality (increased post implantation loss and resorptions and decreased number of live fetuses), fetal developmental delay (skeletal effects) and urogenital effects (bilateral ureter dilation) at doses ≥10 mg/kg/day, decreased fetal ano-genital distance at ≥30 mg/kg/day, and decreased fetal body weight at 100 mg/kg/day. Doses ≥10 mg/kg/day caused maternal toxicity. The doses tested in rats resulted in systemic exposures (AUC) approximately 0.03, 0.1 and 0.3 times, respectively, the AUC in patients.
8.3 Females and Males of Reproductive Potential
Contraception
Males
Based on findings in animal reproduction studies and its mechanism of action, advise males with female partners of reproductive potential to use effective contraception during treatment and for 3 weeks after the final dose of ZYTIGA [see Use in Specific Populations (8.1)] .
Infertility
Based on animal studies, ZYTIGA may impair reproductive function and fertility in males of reproductive potential [see Nonclinical Toxicology (13.1)].
8.4 Pediatric Use
Safety and effectiveness of ZYTIGA in pediatric patients have not been established.
8.5 Geriatric Use
Of the total number of patients receiving ZYTIGA in randomized clinical trials, 70% of patients were 65 years and over and 27% were 75 years and over. No overall differences in safety or effectiveness were observed between these elderly patients and younger patients. Other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
8.6 Patients with Hepatic Impairment
The pharmacokinetics of abiraterone were examined in subjects with baseline mild (N=8) or moderate (N=8) hepatic impairment (Child-Pugh Class A and B, respectively) and in 8 healthy control subjects with normal hepatic function. The systemic exposure (AUC) of abiraterone after a single oral 1,000 mg dose of ZYTIGA increased by approximately 1.1-fold and 3.6-fold in subjects with mild and moderate baseline hepatic impairment, respectively compared to subjects with normal hepatic function.
In another trial, the pharmacokinetics of abiraterone were examined in subjects with baseline severe (N=8) hepatic impairment (Child-Pugh Class C) and in 8 healthy control subjects with normal hepatic function. The systemic exposure (AUC) of abiraterone increased by approximately 7-fold and the fraction of free drug increased 2-fold in subjects with severe baseline hepatic impairment compared to subjects with normal hepatic function.
No dosage adjustment is necessary for patients with baseline mild hepatic impairment. In patients with baseline moderate hepatic impairment (Child-Pugh Class B), reduce the recommended dose of ZYTIGA to 250 mg once daily. Do not use ZYTIGA in patients with baseline severe hepatic impairment (Child-Pugh Class C). If elevations in ALT or AST >5 × ULN or total bilirubin >3 × ULN occur in patients with baseline moderate hepatic impairment, discontinue ZYTIGA treatment [see Dosage and Administration (2.4)and Clinical Pharmacology (12.3)] .
For patients who develop hepatotoxicity during treatment, interruption of treatment and dosage adjustment may be required [see Dosage and Administration (2.4), Warnings and Precautions (5.3), and Clinical Pharmacology (12.3)].
8.7 Patients with Renal Impairment
No dosage adjustment is necessary for patients with renal impairment [see Clinical Pharmacology (12.3)] .
- 10 OVERDOSAGE
-
11 DESCRIPTION
Abiraterone acetate, the active ingredient of ZYTIGA ® is the acetyl ester of abiraterone. Abiraterone is an inhibitor of CYP17 (17α-hydroxylase/C17,20-lyase). Each ZYTIGA tablet contains either 250 mg or 500 mg of abiraterone acetate. Abiraterone acetate is designated chemically as (3β)-17-(3-pyridinyl) androsta-5,16-dien-3-yl acetate and its structure is:
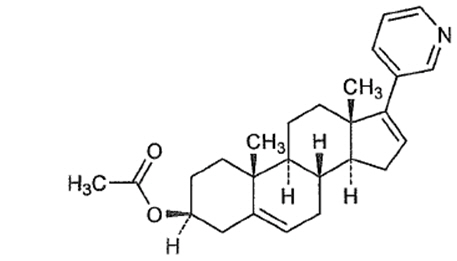
Abiraterone acetate is a white to off-white, non-hygroscopic, crystalline powder. Its molecular formula is C 26H 33NO 2 and it has a molecular weight of 391.55. Abiraterone acetate is a lipophilic compound with an octanol-water partition coefficient of 5.12 (Log P) and is practically insoluble in water. The pKa of the aromatic nitrogen is 5.19.
ZYTIGA tablets are available in 500 mg film-coated tablets and 250 mg uncoated tablets with the following inactive ingredients:
- 500 mg film-coated tablets: colloidal silicon dioxide, croscarmellose sodium, hypromellose, lactose monohydrate, magnesium stearate, silicified microcrystalline cellulose, and sodium lauryl sulfate. The coating, Opadry ®II Purple, contains iron oxide black, iron oxide red, polyethylene glycol, polyvinyl alcohol, talc, and titanium dioxide.
- 250 mg uncoated tablets: colloidal silicon dioxide, croscarmellose sodium, lactose monohydrate, magnesium stearate, microcrystalline cellulose, povidone, and sodium lauryl sulfate.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Abiraterone acetate (ZYTIGA) is converted in vivo to abiraterone, an androgen biosynthesis inhibitor, that inhibits 17 α-hydroxylase/C17,20-lyase (CYP17). This enzyme is expressed in testicular, adrenal, and prostatic tumor tissues and is required for androgen biosynthesis.
CYP17 catalyzes two sequential reactions: 1) the conversion of pregnenolone and progesterone to their 17α-hydroxy derivatives by 17α-hydroxylase activity and 2) the subsequent formation of dehydroepiandrosterone (DHEA) and androstenedione, respectively, by C17, 20 lyase activity. DHEA and androstenedione are androgens and are precursors of testosterone. Inhibition of CYP17 by abiraterone can also result in increased mineralocorticoid production by the adrenals [see Warnings and Precautions (5.1)] .
Androgen sensitive prostatic carcinoma responds to treatment that decreases androgen levels. Androgen deprivation therapies, such as treatment with GnRH agonists or orchiectomy, decrease androgen production in the testes but do not affect androgen production by the adrenals or in the tumor.
ZYTIGA decreased serum testosterone and other androgens in patients in the placebo-controlled clinical trial. It is not necessary to monitor the effect of ZYTIGA on serum testosterone levels.
Changes in serum prostate specific antigen (PSA) levels may be observed but have not been shown to correlate with clinical benefit in individual patients.
12.2 Pharmacodynamics
Cardiac Electrophysiology
In a multi-center, open-label, single-arm trial, 33 patients with metastatic CRPC received ZYTIGA orally at a dose of 1,000 mg once daily at least 1 hour before or 2 hours after a meal in combination with prednisone 5 mg orally twice daily. Assessments up to Cycle 2 Day 2 showed no large changes in the QTc interval (i.e., >20 ms) from baseline. However, small increases in the QTc interval (i.e., <10 ms) due to abiraterone acetate cannot be excluded due to study design limitations.
12.3 Pharmacokinetics
Following administration of abiraterone acetate, the pharmacokinetics of abiraterone have been studied in healthy subjects and in patients with metastatic CRPC. In vivo, abiraterone acetate is converted to abiraterone. In clinical studies, abiraterone acetate plasma concentrations were below detectable levels (<0.2 ng/mL) in >99% of the analyzed samples.
Absorption
Following oral administration of abiraterone acetate to patients with metastatic CRPC, the median time to reach maximum plasma abiraterone concentrations is 2 hours. Abiraterone accumulation is observed at steady-state, with a 2-fold higher exposure (steady-state AUC) compared to a single 1,000 mg dose of abiraterone acetate.
At the dose of 1,000 mg daily in patients with metastatic CRPC, steady-state values (mean ± SD) of C max were 226 ± 178 ng/mL and of AUC were 993 ± 639 ng.hr/mL. No major deviation from dose proportionality was observed in the dose range of 250 mg to 1,000 mg. However, the exposure was not significantly increased when the dose was doubled from 1,000 to 2,000 mg (8% increase in the mean AUC).
Effect of Food
Systemic exposure of abiraterone is increased when abiraterone acetate is administered with food. In healthy subjects abiraterone C max and AUC 0–∞ were approximately 7- and 5-fold higher, respectively, when a single dose of abiraterone acetate was administered with a low-fat meal (7% fat, 300 calories) and approximately 17- and 10-fold higher, respectively, when a single dose of abiraterone acetate was administered with a high-fat (57% fat, 825 calories) meal compared to overnight fasting. Abiraterone AUC 0–∞ was approximately 7-fold or 1.6-fold higher, respectively, when a single dose of abiraterone acetate was administered 2 hours after or 1 hour before a medium fat meal (25% fat, 491 calories) compared to overnight fasting.
Systemic exposures of abiraterone in patients with metastatic CRPC, after repeated dosing of abiraterone acetate were similar when abiraterone acetate was taken with low-fat meals for 7 days and increased approximately 2-fold when taken with high-fat meals for 7 days compared to when taken at least 2 hours after a meal and at least 1 hour before a meal for 7 days.
Given the normal variation in the content and composition of meals, taking ZYTIGA with meals has the potential to result in increased and highly variable exposures.
Distribution
Abiraterone is highly bound (>99%) to the human plasma proteins, albumin and alpha-1 acid glycoprotein. The apparent steady-state volume of distribution (mean ± SD) is 19,669 ± 13,358 L.
Elimination
In patients with metastatic CRPC, the mean terminal half-life of abiraterone in plasma (mean ± SD) is 12 ± 5 hours.
Metabolism
Following oral administration of 14C-abiraterone acetate as capsules, abiraterone acetate is hydrolyzed to abiraterone (active metabolite). The conversion is likely through esterase activity (the esterases have not been identified) and is not CYP mediated. The two main circulating metabolites of abiraterone in human plasma are abiraterone sulphate (inactive) and N-oxide abiraterone sulphate (inactive), which account for about 43% of exposure each. CYP3A4 and SULT2A1 are the enzymes involved in the formation of N-oxide abiraterone sulphate and SULT2A1 is involved in the formation of abiraterone sulphate.
Excretion
Following oral administration of 14C-abiraterone acetate, approximately 88% of the radioactive dose is recovered in feces and approximately 5% in urine. The major compounds present in feces are unchanged abiraterone acetate and abiraterone (approximately 55% and 22% of the administered dose, respectively).
Specific Populations
Patients with Hepatic Impairment
The pharmacokinetics of abiraterone was examined in subjects with baseline mild (N=8) or moderate (N=8) hepatic impairment (Child-Pugh Class A and B, respectively) and in 8 healthy control subjects with normal hepatic function. Systemic exposure to abiraterone after a single oral 1,000 mg dose given under fasting conditions increased approximately 1.1-fold and 3.6-fold in subjects with mild and moderate baseline hepatic impairment, respectively. The mean half-life of abiraterone is prolonged to approximately 18 hours in subjects with mild hepatic impairment and to approximately 19 hours in subjects with moderate hepatic impairment.
In another trial, the pharmacokinetics of abiraterone were examined in subjects with baseline severe (N=8) hepatic impairment (Child-Pugh Class C) and in 8 healthy control subjects with normal hepatic function. The systemic exposure (AUC) of abiraterone increased by approximately 7-fold in subjects with severe baseline hepatic impairment compared to subjects with normal hepatic function. In addition, the mean protein binding was found to be lower in the severe hepatic impairment group compared to the normal hepatic function group, which resulted in a two-fold increase in the fraction of free drug in patients with severe hepatic impairment .
Patients with Renal Impairment
The pharmacokinetics of abiraterone were examined in patients with end-stage renal disease (ESRD) on a stable hemodialysis schedule (N=8) and in matched control subjects with normal renal function (N=8). In the ESRD cohort of the trial, a single 1,000 mg ZYTIGA dose was given under fasting conditions 1 hour after dialysis, and samples for pharmacokinetic analysis were collected up to 96 hours post dose. Systemic exposure to abiraterone after a single oral 1,000 mg dose did not increase in subjects with end-stage renal disease on dialysis, compared to subjects with normal renal function .
Drug Interaction Studies
Clinical Studies
Effect of Other Drugs on ZYTIGA
Effect of ZYTIGA on Other Drugs
CYP2D6 substrates: The C max and AUC of dextromethorphan (CYP2D6 substrate) were increased 2.8- and 2.9-fold, respectively when dextromethorphan 30 mg was given with abiraterone acetate 1,000 mg daily (plus prednisone 5 mg twice daily). The AUC for dextrorphan, the active metabolite of dextromethorphan, increased approximately 1.3 fold.
In Vitro Studies
Cytochrome P450 (CYP) Enzymes:Abiraterone is a substrate of CYP3A4 and has the potential to inhibit CYP1A2, CYP2D6, CYP2C8 and to a lesser extent CYP2C9, CYP2C19 and CYP3A4/5.
Transporter Systems: In vitro studies show that at clinically relevant concentrations, abiraterone acetate and abiraterone are not substrates of P-glycoprotein (P-gp) and that abiraterone acetate is an inhibitor of P-gp. In vitro, abiraterone and its major metabolites were shown to inhibit the hepatic uptake transporter OATP1B1. There are no clinical data available to confirm transporter based interaction.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, and Impairment of Fertility
A two-year carcinogenicity study was conducted in rats at oral abiraterone acetate doses of 5, 15, and 50 mg/kg/day for males and 15, 50, and 150 mg/kg/day for females. Abiraterone acetate increased the combined incidence of interstitial cell adenomas and carcinomas in the testes at all dose levels tested. This finding is considered to be related to the pharmacological activity of abiraterone. Rats are regarded as more sensitive than humans to developing interstitial cell tumors in the testes. Abiraterone acetate was not carcinogenic in female rats at exposure levels up to 0.8 times the human clinical exposure based on AUC. Abiraterone acetate was not carcinogenic in a 6-month study in the transgenic (Tg.rasH2) mouse.
Abiraterone acetate and abiraterone was not mutagenic in an in vitro microbial mutagenesis (Ames) assay or clastogenic in an in vitro cytogenetic assay using primary human lymphocytes or an in vivo rat micronucleus assay.
In repeat-dose toxicity studies in male rats (13- and 26-weeks) and monkeys (39-weeks), atrophy, aspermia/hypospermia, and hyperplasia in the reproductive system were observed at ≥50 mg/kg/day in rats and ≥250 mg/kg/day in monkeys and were consistent with the antiandrogenic pharmacological activity of abiraterone. These effects were observed in rats at systemic exposures similar to humans and in monkeys at exposures approximately 0.6 times the AUC in humans.
In a fertility study in male rats, reduced organ weights of the reproductive system, sperm counts, sperm motility, altered sperm morphology and decreased fertility were observed in animals dosed for 4 weeks at ≥30 mg/kg/day orally. Mating of untreated females with males that received 30 mg/kg/day oral abiraterone acetate resulted in a reduced number of corpora lutea, implantations and live embryos and an increased incidence of pre-implantation loss. Effects on male rats were reversible after 16 weeks from the last abiraterone acetate administration.
In a fertility study in female rats, animals dosed orally for 2 weeks until day 7 of pregnancy at ≥30 mg/kg/day had an increased incidence of irregular or extended estrous cycles and pre-implantation loss (300 mg/kg/day). There were no differences in mating, fertility, and litter parameters in female rats that received abiraterone acetate. Effects on female rats were reversible after 4 weeks from the last abiraterone acetate administration.
The dose of 30 mg/kg/day in rats is approximately 0.3 times the recommended dose of 1,000 mg/day based on body surface area.
In 13- and 26-week studies in rats and 13- and 39-week studies in monkeys, a reduction in circulating testosterone levels occurred with abiraterone acetate at approximately one half the human clinical exposure based on AUC. As a result, decreases in organ weights and toxicities were observed in the male and female reproductive system, adrenal glands, liver, pituitary (rats only), and male mammary glands. The changes in the reproductive organs are consistent with the antiandrogenic pharmacological activity of abiraterone acetate.
13.2 Animal Toxicology and/or Pharmacology
A dose-dependent increase in cataracts was observed in rats after daily oral abiraterone acetate administration for 26 weeks starting at ≥50 mg/kg/day (similar to the human clinical exposure based on AUC). In a 39-week monkey study with daily oral abiraterone acetate administration, no cataracts were observed at higher doses (2 times greater than the clinical exposure based on AUC).
-
14 CLINICAL STUDIES
The efficacy and safety of ZYTIGA with prednisone was established in three randomized placebo-controlled international clinical studies. All patients in these studies received a GnRH analog or had prior bilateral orchiectomy. Patients with prior ketoconazole treatment for prostate cancer and a history of adrenal gland or pituitary disorders were excluded from these trials. Concurrent use of spironolactone was not allowed during the study period.
COU-AA-301: Patients with metastatic CRPC who had received prior docetaxel chemotherapy
In COU-AA-301 (NCT00638690), a total of 1195 patients were randomized 2:1 to receive either ZYTIGA orally at a dose of 1,000 mg once daily in combination with prednisone 5 mg orally twice daily (N=797) or placebo once daily plus prednisone 5 mg orally twice daily (N=398). Patients randomized to either arm were to continue treatment until disease progression (defined as a 25% increase in PSA over the patient's baseline/nadir together with protocol-defined radiographic progression and symptomatic or clinical progression), initiation of new treatment, unacceptable toxicity or withdrawal.
The following patient demographics and baseline disease characteristics were balanced between the treatment arms. The median age was 69 years (range 39–95) and the racial distribution was 93% Caucasian, 3.6% Black, 1.7% Asian, and 1.6% Other. Eighty-nine percent of patients enrolled had an ECOG performance status score of 0–1 and 45% had a Brief Pain Inventory-Short Form score of ≥4 (patient's reported worst pain over the previous 24 hours). Ninety percent of patients had metastases in bone and 30% had visceral involvement. Seventy percent of patients had radiographic evidence of disease progression and 30% had PSA-only progression. Seventy percent of patients had previously received one cytotoxic chemotherapy regimen and 30% received two regimens.
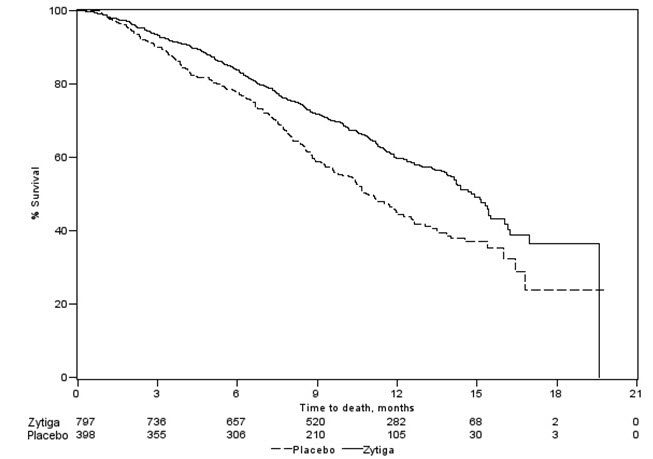
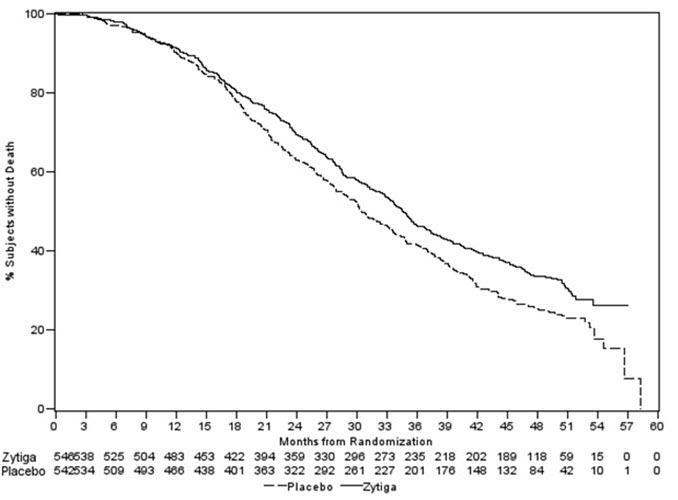
The protocol pre-specified interim analysis was conducted after 552 deaths and showed a statistically significant improvement in overall survival (OS) in patients treated with ZYTIGA with prednisone compared to patients in the placebo with prednisone arm (Table 7 and Figure 1). An updated survival analysis was conducted when 775 deaths (97% of the planned number of deaths for final analysis) were observed. Results from this analysis were consistent with those from the interim analysis (Table 7).
Table 7: Overall Survival of Patients Treated with Either ZYTIGA or Placebo in Combination with Prednisone in COU-AA-301 (Intent-to-Treat Analysis) ZYTIGA with Prednisone
(N=797)Placebo with Prednisone
(N=398)- *
- p-value is derived from a log-rank test stratified by ECOG performance status score (0–1 vs. 2), pain score (absent vs. present), number of prior chemotherapy regimens (1 vs. 2), and type of disease progression (PSA only vs. radiographic).
- †
- Hazard Ratio is derived from a stratified proportional hazards model. Hazard ratio <1 favors ZYTIGA with prednisone.
Primary Survival Analysis Deaths (%) 333 (42%) 219 (55%) Median survival (months)
(95% CI)14.8 (14.1, 15.4) 10.9 (10.2, 12.0) p-value * <0.0001 Hazard ratio (95% CI) † 0.646 (0.543, 0.768) Updated Survival Analysis Deaths (%) 501 (63%) 274 (69%) Median survival (months)
(95% CI)15.8 (14.8, 17.0) 11.2 (10.4, 13.1) Hazard ratio (95% CI) † 0.740 (0.638, 0.859) Figure 1: Kaplan-Meier Overall Survival Curves in COU-AA-301 (Intent-to-Treat Analysis)
COU-AA-302: Patients with metastatic CRPC who had not received prior cytotoxic chemotherapy
In COU-AA-302 (NCT00887198), 1088 patients were randomized 1:1 to receive either ZYTIGA orally at a dose of 1,000 mg once daily (N=546) or Placebo orally once daily (N=542). Both arms were given concomitant prednisone 5 mg twice daily. Patients continued treatment until radiographic or clinical (cytotoxic chemotherapy, radiation or surgical treatment for cancer, pain requiring chronic opioids, or ECOG performance status decline to 3 or more) disease progression, unacceptable toxicity or withdrawal. Patients with moderate or severe pain, opiate use for cancer pain, or visceral organ metastases were excluded.
Patient demographics were balanced between the treatment arms. The median age was 70 years. The racial distribution of patients treated with ZYTIGA was 95% Caucasian, 2.8% Black, 0.7% Asian and 1.1% Other. The ECOG performance status was 0 for 76% of patients, and 1 for 24% of patients. Co-primary efficacy endpoints were overall survival and radiographic progression-free survival (rPFS). Baseline pain assessment was 0–1 (asymptomatic) in 66% of patients and 2–3 (mildly symptomatic) in 26% of patients as defined by the Brief Pain Inventory-Short Form (worst pain over the last 24 hours).
Radiographic progression-free survival was assessed with the use of sequential imaging studies and was defined by bone scan identification of 2 or more new bone lesions with confirmation (Prostate Cancer Working Group 2 criteria) and/or modified Response Evaluation Criteria In Solid Tumors (RECIST) criteria for progression of soft tissue lesions. Analysis of rPFS utilized centrally-reviewed radiographic assessment of progression.
The planned final analysis for OS, conducted after 741 deaths (median follow up of 49 months) demonstrated a statistically significant OS improvement in patients treated with ZYTIGA with prednisone compared to those treated with placebo with prednisone (Table 8 and Figure 2). Sixty-five percent of patients on the ZYTIGA arm and 78% of patients on the placebo arm used subsequent therapies that may prolong OS in metastatic CRPC. ZYTIGA was used as a subsequent therapy in 13% of patients on the ZYTIGA arm and 44% of patients on the placebo arm.
Table 8: Overall Survival of Patients Treated with Either ZYTIGA or Placebo in Combination with Prednisone in COU-AA-302 (Intent-to-Treat Analysis) ZYTIGA with Prednisone
(N=546)Placebo with Prednisone
(N=542)Overall Survival Deaths 354 (65%) 387 (71%) Median survival (months)
(95% CI)34.7 (32.7, 36.8) 30.3 (28.7, 33.3) p-value * 0.0033 Hazard ratio †(95% CI) 0.81 (0.70, 0.93) Figure 2: Kaplan Meier Overall Survival Curves in COU-AA-302
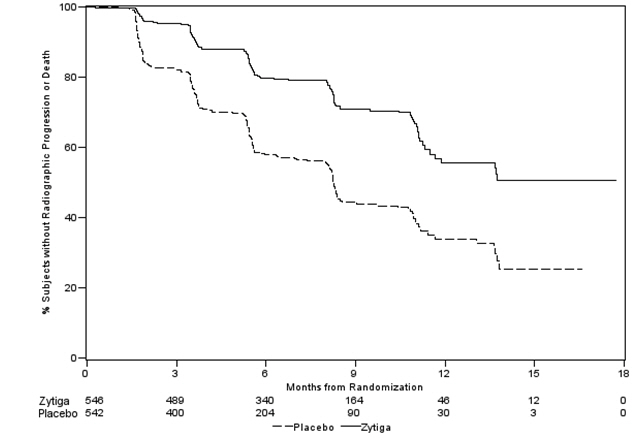
At the pre-specified rPFS analysis, 150 (28%) patients treated with ZYTIGA with prednisone and 251 (46%) patients treated with placebo with prednisone had radiographic progression. A significant difference in rPFS between treatment groups was observed (Table 9 and Figure 3).
Table 9: Radiographic Progression-free Survival of Patients Treated with Either ZYTIGA or Placebo in Combination with Prednisone in COU-AA-302 (Intent-to-Treat Analysis) ZYTIGA with Prednisone
(N=546)Placebo with Prednisone
(N=542)NR=Not reached. Radiographic Progression-free Survival Progression or death 150 (28%) 251 (46%) Median rPFS (months)
(95% CI)NR
(11.66, NR)8.28
(8.12, 8.54)p-value * <0.0001 Hazard ratio †(95% CI) 0.425 (0.347, 0.522) Figure 3: Kaplan Meier Curves of Radiographic Progression-free Survival in COU-AA-302 (Intent-to-Treat Analysis)
The primary efficacy analyses are supported by the following prospectively defined endpoints. The median time to initiation of cytotoxic chemotherapy was 25.2 months for patients in the ZYTIGA arm and 16.8 months for patients in the placebo arm (HR=0.580; 95% CI: [0.487, 0.691], p < 0.0001).
The median time to opiate use for prostate cancer pain was not reached for patients receiving ZYTIGA and was 23.7 months for patients receiving placebo (HR=0.686; 95% CI: [0.566, 0.833], p=0.0001). The time to opiate use result was supported by a delay in patient reported pain progression favoring the ZYTIGA arm.
LATITUDE: Patients with metastatic high-risk CSPC
In LATITUDE (NCT01715285), 1199 patients with metastatic high-risk CSPC were randomized 1:1 to receive either ZYTIGA orally at a dose of 1,000 mg once daily with prednisone 5 mg once daily (N=597) or placebos orally once daily (N=602). High-risk disease was defined as having at least two of three risk factors at baseline: a total Gleason score of ≥8, presence of ≥3 lesions on bone scan, and evidence of measurable visceral metastases. Patients with significant cardiac, adrenal, or hepatic dysfunction were excluded. Patients continued treatment until radiographic or clinical disease progression, unacceptable toxicity, withdrawal or death. Clinical progression was defined as the need for cytotoxic chemotherapy, radiation or surgical treatment for cancer, pain requiring chronic opioids, or ECOG performance status decline to ≥3.
Patient demographics were balanced between the treatment arms. The median age was 67 years among all randomized subjects. The racial distribution of patients treated with ZYTIGA was 69% Caucasian, 2.5% Black, 21% Asian, and 8.1% Other. The ECOG performance status was 0 for 55%, 1 for 42%, and 2 for 3.5% of patients. Baseline pain assessment was 0–1 (asymptomatic) in 50% of patients, 2–3 (mildly symptomatic) in 23% of patients, and ≥4 in 28% of patients as defined by the Brief Pain Inventory-Short Form (worst pain over the last 24 hours).
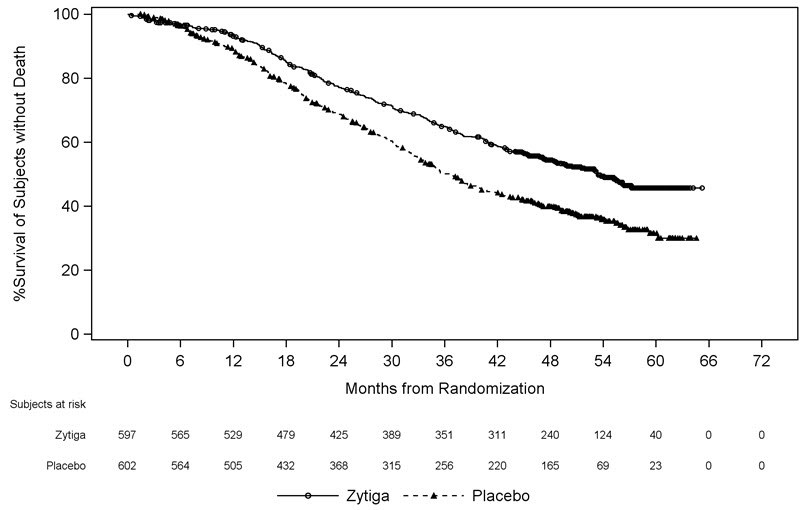
A major efficacy outcome was overall survival. The pre-specified interim analysis after 406 deaths showed a statistically significant improvement in OS in patients on ZYTIGA with prednisone compared to those on placebos. Twenty-one percent of patients on the ZYTIGA arm and 41% of patients on the placebos arm received subsequent therapies that may prolong OS in metastatic CRPC. An updated survival analysis was conducted when 618 deaths were observed. The median follow-up time was 52 months. Results from this analysis were consistent with those from the pre-specified interim analysis (Table 10 and Figure 4). At the updated analysis, 29% of patients on the ZYTIGA arm and 45% of patients on the placebos arm received subsequent therapies that may prolong OS in metastatic CRPC.
Table 10: Overall Survival of Patients Treated with Either ZYTIGA or Placebos in LATITUDE (Intent-to-Treat Analysis) ZYTIGA with Prednisone
(N=597)Placebos
(N=602)NE=Not estimable Overall Survival * Deaths (%) 169 (28%) 237 (39%) Median survival (months)
(95% CI)NE (NE, NE) 34.7 (33.1, NE) p-value † <0.0001 Hazard ratio (95% CI) ‡ 0.62 (0.51, 0.76) Updated Overall Survival Deaths (%) 275 (46%) 343 (57%) Median survival (months)
(95% CI)53.3
(48.2, NE)36.5
(33.5, 40.0)Hazard ratio (95% CI) ‡ 0.66 (0.56, 0.78) Figure 4: Kaplan-Meier Plot of Overall Survival; Intent-to-treat Population in LATITUDE Updated Analysis
The major efficacy outcome was supported by a statistically significant delay in time to initiation of chemotherapy for patients in the ZYTIGA arm compared to those in the placebos arm. The median time to initiation of chemotherapy was not reached for patients on ZYTIGA with prednisone and was 38.9 months for patients on placebos (HR = 0.44; 95% CI: [0.35, 0.56], p < 0.0001).
-
16 HOW SUPPLIED/STORAGE AND HANDLING
ZYTIGA ® (abiraterone acetate) Tablets are available in the strengths and packages listed below:
-
ZYTIGA
® 500 mg film-coated Tablets
Purple, oval-shaped tablets debossed with "AA" one side and "500" on the other side.
NDC 57894-195-06, 60 tablets available in child-resistant high-density polyethylene bottles -
ZYTIGA®250 mg uncoated Tablets
White to off-white, oval-shaped tablets debossed with "AA250" on one side.
NDC 57894-150-12, 120 tablets available in child-resistant high-density polyethylene bottles
Storage and Handling
Store at 20 °C to 25 °C (68 °F to 77 °F); excursions permitted in the range from 15 °C to 30 °C (59 °F to 86 °F) [see USP Controlled Room Temperature].
Keep out of reach of children.
Based on its mechanism of action, ZYTIGA may harm a developing fetus. Women who are pregnant or women who may be pregnant should not handle ZYTIGA 250 mg uncoated tablets or other ZYTIGA tablets if broken, crushed, or damaged without protection, e.g., gloves [see Use in Specific Populations (8.1)] .
-
ZYTIGA
® 500 mg film-coated Tablets
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information)
Hypokalemia, Fluid Retention, and Cardiovascular Adverse Reactions
- Inform patients that ZYTIGA is associated with hypertension, hypokalemia, and peripheral edema that may lead to QT prolongation and Torsades de Pointes in patients who develop hypokalemia while taking ZYTIGA. Advise patients that their blood pressure, serum potassium and signs and symptoms of fluid retention will be monitored clinically at least monthly. Advise patients to adhere to corticosteroids and to report symptoms of hypertension, hypokalemia, or edema to their healthcare provider [see Warnings and Precautions (5.1)] .
Adrenocortical Insufficiency
- Inform patients that ZYTIGA with prednisone is associated with adrenal insufficiency. Advise patients to report symptoms of adrenocortical insufficiency to their healthcare provider [see Warnings and Precautions (5.2)] .
Hepatotoxicity
- Inform patients that ZYTIGA is associated with severe hepatotoxicity. Inform patients that their liver function will be monitored using blood tests. Advise patients to immediately report symptoms of hepatotoxicity to their healthcare provider [see Warnings and Precautions (5.3)] .
Hypoglycemia
- Inform patients that severe hypoglycemia has been reported when ZYTIGA was administered to patients with pre-existing diabetes who were receiving medications containing thiazolidinediones (including pioglitazone) or repaglinide, antidiabetic drugs. Advise patients with diabetes to monitor glucose levels during and after treatment with ZYTIGA [see Warnings and Precautions (5.6)and Drug Interactions (7.2)].
Use in Combination with Radium Ra 223 Dichloride
- Advise patients that radium Ra 223 dichloride showed an increase in mortality and an increased rate of fracture when used in combination with ZYTIGA plus prednisone/prednisolone. Inform patients to speak with their healthcare provider about any other medications or treatment they are currently taking for prostate cancer [see Warnings and Precautions (5.4)] .
Dosing and Administration
- Inform patients that ZYTIGA is taken once daily with prednisone (once or twice daily according to their healthcare provider's instructions) and to not interrupt or stop either of these medications without consulting their healthcare provider.
- Inform patients receiving GnRH therapy that they need to maintain this treatment during the course of treatment with ZYTIGA.
- Instruct patients to take ZYTIGA tablets as a single dose once daily on an empty stomach. Instruct patients to not eat food 2 hours before and 1 hour after taking ZYTIGA. ZYTIGA taken with food causes increased exposure and may result in adverse reactions. Instruct patients to swallow tablets whole with water and not to crush or chew the tablets [see Dosage and Administration (2.3)] .
- Inform patients that if they miss a dose of ZYTIGA or prednisone, they should take their normal dose the following day. If more than one daily dose is skipped, inform patients to contact their healthcare provider [see Dosage and Administration (2.3)] .
Embryo-Fetal Toxicity
- Inform patients that ZYTIGA may harm a developing fetus and can cause loss of pregnancy.
- Advise males with female partners of reproductive potential to use effective contraception during treatment and for 3 weeks after the final dose of ZYTIGA [see Use in Specific Populations (8.1)] .
- Advise females who are pregnant or women who may be pregnant not to handle ZYTIGA 250 mg uncoated tablets or other ZYTIGA tablets if broken, crushed, or damaged without protection, e.g., gloves [see Use in Specific Populations (8.1)and How Supplied/Storage and Handling (16)] .
Infertility
- Advise male patients that ZYTIGA may impair fertility [see Use in Specific Populations (8.3)] .
- SPL UNCLASSIFIED SECTION
-
PATIENT PACKAGE INSERT
This Patient Information has been approved by the U.S. Food and Drug Administration. Revised: 11/2024 PATIENT INFORMATION
ZYTIGA ®( Zye- tee- ga)
(abiraterone acetate)
tabletsWhat is ZYTIGA?
ZYTIGA is a prescription medicine that is used along with prednisone. ZYTIGA is used to treat men with prostate cancer that has spread to other parts of the body.
It is not known if ZYTIGA is safe and effective in females or children.Before taking ZYTIGA, tell your healthcare provider about all of your medical conditions, including if you: - have heart problems
- have liver problems
- have diabetes
- have a history of adrenal problems
- have a history of pituitary problems
- are receiving any other treatment for prostate cancer
- are pregnant or plan to become pregnant. ZYTIGA can cause harm to your unborn baby and loss of pregnancy (miscarriage). Females who are or may become pregnant should not handle ZYTIGA uncoated tablets or other ZYTIGA tablets if broken, crushed, or damaged without protection, such as gloves.
- have a partner who is pregnant or may become pregnant.
- Males who have female partners who are able to become pregnant should use effective birth control (contraception) during treatment with ZYTIGA and for 3 weeks after the last dose of ZYTIGA.
- are breastfeeding or plan to breastfeed. It is not known if ZYTIGA passes into your breastmilk.
You should not start or stop any medicine before you talk with the healthcare provider that prescribed ZYTIGA.
Know the medicines you take. Keep a list of them with you to show to your healthcare provider and pharmacist when you get a new medicine.How should I take ZYTIGA? - Take ZYTIGA and prednisone exactly as your healthcare provider tells you.
- Take your prescribed dose of ZYTIGA 1 time a day.
- Your healthcare provider may change your dose if needed.
- Do not change or stop taking your prescribed dose of ZYTIGA or prednisone without talking with your healthcare provider first.
- Take ZYTIGA tablets as a single dose one time a day on an empty stomach. Do not eat food 2 hours before and 1 hour after taking ZYTIGA.
- Do not take ZYTIGA with food.Taking ZYTIGA with food may cause more of the medicine to be absorbed by the body than is needed and this may cause side effects.
- Swallow ZYTIGA tablets whole. Do not crush or chew tablets.
- Take ZYTIGA tablets with water.
- If you miss a dose of ZYTIGA or prednisone, take your prescribed dose the following day. If you miss more than 1 dose, tell your healthcare provider right away.
- Your healthcare provider will do blood tests to check for side effects.
What are the possible side effects of ZYTIGA?
ZYTIGA may cause serious side effects including:-
High blood pressure (hypertension), low blood potassium levels (hypokalemia), fluid retention (edema), and irregular heartbeats can happen during treatment with ZYTIGA. This can be life threatening. To decrease the chance of this happening, you must take prednisone with ZYTIGA exactly as your healthcare provider tells you. Your healthcare provider will check your blood pressure, do blood tests to check your potassium levels, and check for any signs and symptoms of fluid retention every month during treatment with ZYTIGA.
Tell your healthcare provider if you get any of the following symptoms:
- dizziness
- fast or irregular heartbeats
- feel faint or lightheaded
- headache
- confusion
- muscle weakness
- pain in your legs
- swelling in your legs or feet
- Adrenal problems may happen if you stop taking prednisone, get an infection, or are under stress.
-
Severe liver problems. You may develop changes in liver function blood tests. Your healthcare provider will do blood tests to check your liver before treatment with ZYTIGA and during treatment with ZYTIGA. Liver failure may occur, which can lead to death. Tell your healthcare provider right away if you notice any of the following changes:
- yellowing of the skin or eyes
- darkening of the urine
- severe nausea or vomiting
- Increased risk of bone fracture and death when ZYTIGA and prednisone or prednisolone, is used in combination with a type of radiation called radium Ra 223 dichloride. Tell your healthcare provider about any other treatments you are taking for prostate cancer.
- Severe low blood sugar (hypoglycemia). Severe low blood sugar with ZYTIGA can happen in people who have diabetes and take certain antidiabetic medicines. You and your healthcare provider should check your blood sugar levels regularly during treatment with ZYTIGA and after you stop treatment. Your healthcare provider may also need to change the dose of your antidiabetic medicines. Signs and symptoms of low blood sugar may include.
- headache
- drowsiness
- weakness
- dizziness
- confusion
- irritability
- hunger
- fast heartbeat
- sweating
- feeling jittery
The most common side effects of ZYTIGA include: - feeling very tired
- joint pain
- high blood pressure
- nausea
- swelling in your legs or feet
- low blood potassium levels
- hot flushes
- diarrhea
- vomiting
- infected nose, sinuses, or throat (cold)
- cough
- headache
- low red blood cells (anemia)
- high blood cholesterol and triglycerides
- high blood sugar levels
- certain other abnormal blood tests
ZYTIGA may cause fertility problems in males, which may affect the ability to father children. Talk to your healthcare provider if you have concerns about fertility.
These are not all the possible side effects of ZYTIGA. Call your healthcare provider for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.How should I store ZYTIGA? - Store ZYTIGA at room temperature between 68 °F to 77 °F (20 °C to 25 °C).
General information about the safe and effective use of ZYTIGA.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use ZYTIGA for a condition for which it was not prescribed. Do not give ZYTIGA to other people, even if they have the same symptoms that you have. It may harm them.
You can ask your healthcare provider or pharmacist for information about ZYTIGA that is written for health professionals.What are the ingredients of ZYTIGA?
Active ingredient: abiraterone acetate
Inactive ingredients:
500 mg film-coated tablets: colloidal silicon dioxide, croscarmellose sodium, hypromellose, lactose monohydrate, magnesium stearate, silicified microcrystalline cellulose, and sodium lauryl sulfate. The film-coating contains iron oxide black, iron oxide red, polyethylene glycol, polyvinyl alcohol, talc, and titanium dioxide.
250 mg uncoated tablets: colloidal silicon dioxide, croscarmellose sodium, lactose monohydrate, magnesium stearate, microcrystalline cellulose, povidone, and sodium lauryl sulfate.
Manufactured for: Janssen Biotech, Inc., Horsham, PA 19044, USA
For more information, call Janssen Biotech, Inc. at 1-800-526-7736 or go to www.Zytiga.com.
For patent information: www.janssenpatents.com
© Johnson & Johnson and its affiliates 2011, 2017, 2024 - PRINCIPAL DISPLAY PANEL - 250 mg Tablet Bottle Label
- PRINCIPAL DISPLAY PANEL - 500 mg Tablet Bottle Label
-
INGREDIENTS AND APPEARANCE
ZYTIGA
abiraterone acetate tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:57894-150 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength ABIRATERONE ACETATE (UNII: EM5OCB9YJ6) (ABIRATERONE - UNII:G819A456D0) ABIRATERONE ACETATE 250 mg Inactive Ingredients Ingredient Name Strength LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) POVIDONE, UNSPECIFIED (UNII: FZ989GH94E) SODIUM LAURYL SULFATE (UNII: 368GB5141J) MAGNESIUM STEARATE (UNII: 70097M6I30) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) Product Characteristics Color white (white to off-white) Score no score Shape OVAL Size 16mm Flavor Imprint Code AA250 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:57894-150-12 120 in 1 BOTTLE; Type 0: Not a Combination Product 04/28/2011 2 NDC:57894-150-25 120 in 1 BOTTLE; Type 0: Not a Combination Product 09/01/2015 08/31/2018 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA202379 04/28/2011 ZYTIGA
abiraterone acetate tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:57894-195 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength ABIRATERONE ACETATE (UNII: EM5OCB9YJ6) (ABIRATERONE - UNII:G819A456D0) ABIRATERONE ACETATE 500 mg Inactive Ingredients Ingredient Name Strength MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) HYPROMELLOSE 2910 (15 MPA.S) (UNII: 36SFW2JZ0W) LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) MAGNESIUM STEARATE (UNII: 70097M6I30) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) SODIUM LAURYL SULFATE (UNII: 368GB5141J) POLYVINYL ALCOHOL, UNSPECIFIED (UNII: 532B59J990) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) POLYETHYLENE GLYCOL 3350 (UNII: G2M7P15E5P) TALC (UNII: 7SEV7J4R1U) FERRIC OXIDE RED (UNII: 1K09F3G675) FERROSOFERRIC OXIDE (UNII: XM0M87F357) WATER (UNII: 059QF0KO0R) Product Characteristics Color purple Score no score Shape OVAL Size 20mm Flavor Imprint Code AA;500 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:57894-195-06 60 in 1 BOTTLE; Type 0: Not a Combination Product 04/17/2017 2 NDC:57894-195-15 60 in 1 BOTTLE; Type 0: Not a Combination Product 04/17/2017 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA202379 04/17/2017 Labeler - Janssen Biotech, Inc. (099091753) Establishment Name Address ID/FEI Business Operations Patheon, Inc. 240769596 manufacture(57894-150, 57894-195) , analysis(57894-150, 57894-195) , pack(57894-150, 57894-195) Establishment Name Address ID/FEI Business Operations Janssen Pharmaceutica NV 400345889 api manufacture(57894-150, 57894-195) Establishment Name Address ID/FEI Business Operations Janssen-Cilag S.p.A. 542797928 pack(57894-150, 57894-195) Establishment Name Address ID/FEI Business Operations Patheon France S.A.S. 543127229 manufacture(57894-150, 57894-195) , analysis(57894-150, 57894-195) Establishment Name Address ID/FEI Business Operations Ajinomoto Omnichem 400344443 api manufacture(57894-150, 57894-195) Establishment Name Address ID/FEI Business Operations Johnson & Johnson Private Limited 677603030 analysis(57894-150, 57894-195)