Label: BRAFTOVI- encorafenib capsule




-
NDC Code(s):
70255-025-01,
70255-025-02,
70255-025-03,
70255-025-04, view more70255-025-05, 70255-025-06
- Packager: Array BioPharma Inc.
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: New Drug Application
Drug Label Information
Updated September 18, 2024
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Medication Guide: HTML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use BRAFTOVI safely and effectively. See full prescribing information for BRAFTOVI.
BRAFTOVI® (encorafenib) capsules, for oral use
Initial U.S. Approval: 2018RECENT MAJOR CHANGES
INDICATIONS AND USAGE
BRAFTOVI is a kinase inhibitor indicated:
- •
- in combination with binimetinib, for the treatment of patients with unresectable or metastatic melanoma with a BRAF V600E or V600K mutation, as detected by an FDA-approved test. (1.1, 2.1)
- •
- in combination with cetuximab, for the treatment of adult patients with metastatic colorectal cancer (CRC) with a BRAF V600E mutation, as detected by an FDA-approved test, after prior therapy. (1.2, 2.1)
- •
- in combination with binimetinib, for the treatment of adult patients with metastatic non-small cell lung cancer (NSCLC) with a BRAF V600E mutation, as detected by an FDA-approved test. (1.3, 2.1)
Limitations of Use
BRAFTOVI is not indicated for treatment of patients with wild-type BRAF melanoma, wild-type BRAF CRC, or wild-type BRAF NSCLC. (1.4, 5.2)
DOSAGE FORMS AND STRENGTHS
Capsules: 75 mg. (3)
CONTRAINDICATIONS
None. (4)
WARNINGS AND PRECAUTIONS
- •
- New Primary Malignancies, cutaneous and non-cutaneous: Can occur. Monitor for malignancies and perform dermatologic evaluations prior to, while on therapy, and following discontinuation of treatment. (5.1)
- •
- Tumor Promotion in BRAF Wild-Type Tumors: Increased cell proliferation can occur with BRAF inhibitors. (5.2)
- •
- Cardiomyopathy: Assess left ventricular ejection fraction (LVEF) before initiating treatment with BRAFTOVI and binimetinib, and after one month of treatment, then every 2 to 3 months thereafter. The safety of BRAFTOVI in combination with binimetinib has not been established in patients with LVEF below 50%. (5.3)
- •
- Hepatotoxicity: Monitor liver function tests before and during treatment with BRAFTOVI and binimetinib and as clinically indicated. (5.4)
- •
- Hemorrhage: Major hemorrhagic events can occur in patients receiving BRAFTOVI and binimetinib. (5.5)
- •
- Uveitis: Perform ophthalmologic evaluation at regular intervals and for any visual disturbances. (5.6)
- •
- QT Prolongation: Monitor electrolytes before and during treatment. Correct electrolyte abnormalities and control for cardiac risk factors for QT prolongation. Withhold BRAFTOVI for QTc of 500 ms or greater. (5.7)
- •
- Embryo-Fetal Toxicity: Can cause fetal harm. Advise females with reproductive potential of potential risk to the fetus and to use effective non-hormonal method of contraception. (5.8, 8.1, 8.3)
- •
- Risks Associated with BRAFTOVI as a Single Agent: If binimetinib is temporarily interrupted or permanently discontinued, reduce the dose of BRAFTOVI as recommended. (5.9)
- •
- Risks Associated with Combination Treatment: BRAFTOVI is indicated for use as part of a regimen in combination with binimetinib or cetuximab. (5.10)
ADVERSE REACTIONS
Melanoma: Most common adverse reactions (≥25%) for BRAFTOVI, in combination with binimetinib, are fatigue, nausea, vomiting, abdominal pain, and arthralgia. (6.1)
CRC: Most common adverse reactions (≥25%) for BRAFTOVI, in combination with cetuximab, are fatigue, nausea, diarrhea, dermatitis acneiform, abdominal pain, decreased appetite, arthralgia, and rash. (6.1)
NSCLC: Most common adverse reactions (≥25%) for BRAFTOVI, in combination with binimetinib, are fatigue, nausea, diarrhea, musculoskeletal pain, vomiting, abdominal pain, visual impairment, constipation, dyspnea, rash, and cough. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Pfizer Inc. at 1-800-438-1985 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
- •
- Strong or moderate CYP3A4 inhibitors: Avoid coadministration. If unavoidable, reduce BRAFTOVI dosage. (2.6, 7.1)
- •
- Strong CYP3A4 inducers: Avoid coadministration. (7.1)
- •
- Sensitive CYP3A4 substrates: Avoid coadministration with CYP3A4 substrates (including hormonal contraceptives) for which a decrease in plasma concentration may lead to reduced efficacy of the substrate. (7.2)
- •
- Transporters: Dose reductions of drugs that are substrates of OATP1B1, OATP1B3, or BCRP may be required when used concomitantly with BRAFTOVI. (7.2, 12.3)
USE IN SPECIFIC POPULATIONS
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 9/2024
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
1.1 BRAF V600E or V600K Mutation-Positive Unresectable or Metastatic Melanoma
1.2 BRAF V600E Mutation-Positive Metastatic Colorectal Cancer (CRC)
1.3 BRAF V600E Mutation-Positive Metastatic Non-Small Cell Lung Cancer (NSCLC)
1.4 Limitations of Use
2 DOSAGE AND ADMINISTRATION
2.1 Patient Selection
2.2 Recommended Dosage for BRAF V600E or V600K Mutation-Positive Unresectable or Metastatic Melanoma and for BRAF V600E Mutation-Positive Metastatic Non-Small Cell Lung Cancer (NSCLC)
2.3 Recommended Dosage for BRAF V600E Mutation-Positive Metastatic Colorectal Cancer (CRC)
2.4 Administration
2.5 Dosage Modifications for Adverse Reactions
2.6 Dose Modifications for Coadministration With Strong or Moderate CYP3A4 Inhibitors
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 New Primary Malignancies
5.2 Tumor Promotion in BRAF Wild-Type Tumors
5.3 Cardiomyopathy
5.4 Hepatotoxicity
5.5 Hemorrhage
5.6 Uveitis
5.7 QT Prolongation
5.8 Embryo-Fetal Toxicity
5.9 Risks Associated with BRAFTOVI as a Single Agent
5.10 Risks Associated with Combination Treatment
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
7 DRUG INTERACTIONS
7.1 Effect of Other Drugs on BRAFTOVI
7.2 Effect of BRAFTOVI on Other Drugs
7.3 Drugs That Prolong the QT Interval
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Hepatic Impairment
8.7 Renal Impairment
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
14.1 BRAF V600E or V600K Mutation-Positive Unresectable or Metastatic Melanoma
14.2 BRAF V600E Mutation-Positive Metastatic Colorectal Cancer (CRC)
14.3 BRAF V600E Mutation-Positive Metastatic Non-Small Cell Lung Cancer
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
1.1 BRAF V600E or V600K Mutation-Positive Unresectable or Metastatic Melanoma
BRAFTOVI is indicated, in combination with binimetinib, for the treatment of patients with unresectable or metastatic melanoma with a BRAF V600E or V600K mutation, as detected by an FDA-approved test [see Dosage and Administration (2.1)].
1.2 BRAF V600E Mutation-Positive Metastatic Colorectal Cancer (CRC)
BRAFTOVI is indicated, in combination with cetuximab, for the treatment of adult patients with metastatic colorectal cancer (CRC) with a BRAF V600E mutation, as detected by an FDA-approved test, after prior therapy [see Dosage and Administration (2.1)].
1.3 BRAF V600E Mutation-Positive Metastatic Non-Small Cell Lung Cancer (NSCLC)
BRAFTOVI is indicated, in combination with binimetinib, for the treatment of adult patients with metastatic non-small cell lung cancer (NSCLC) with a BRAF V600E mutation, as detected by an FDA-approved test [see Dosage and Administration (2.1)].
1.4 Limitations of Use
BRAFTOVI is not indicated for treatment of patients with wild-type BRAF melanoma, wild-type BRAF CRC, or wild-type BRAF NSCLC [see Warnings and Precautions (5.2)].
-
2 DOSAGE AND ADMINISTRATION
2.1 Patient Selection
BRAF V600E or V600K Mutation-Positive Unresectable or Metastatic Melanoma
Confirm the presence of a BRAF V600E or V600K mutation in tumor specimens prior to initiating BRAFTOVI [see Warnings and Precautions (5.2), Clinical Studies (14.1)]. Information on FDA-approved tests for the detection of BRAF V600E and V600K mutations in melanoma is available at: http://www.fda.gov/CompanionDiagnostics.
BRAF V600E Mutation-Positive Metastatic Colorectal Cancer (CRC)
Confirm the presence of a BRAF V600E mutation in tumor specimens prior to initiating BRAFTOVI [see Warnings and Precautions (5.2), Clinical Studies (14.2)]. Information on FDA-approved tests for the detection of BRAF V600E mutations in CRC is available at: http://www.fda.gov/CompanionDiagnostics.
BRAF V600E Mutation-Positive Metastatic Non-Small Cell Lung Cancer (NSCLC)
Confirm the presence of a BRAF V600E mutation in tumor or plasma specimens prior to initiating BRAFTOVI [see Warnings and Precautions (5.2), Clinical Studies (14.3)]. If no mutation is detected in a plasma specimen, test tumor tissue. Information on FDA-approved tests for the detection of BRAF V600E mutations in NSCLC is available at: http://www.fda.gov/CompanionDiagnostics.
2.2 Recommended Dosage for BRAF V600E or V600K Mutation-Positive Unresectable or Metastatic Melanoma and for BRAF V600E Mutation-Positive Metastatic Non-Small Cell Lung Cancer (NSCLC)
The recommended dosage of BRAFTOVI is 450 mg (six 75 mg capsules) orally once daily in combination with binimetinib until disease progression or unacceptable toxicity. Refer to the binimetinib prescribing information for recommended binimetinib dosing information.
2.3 Recommended Dosage for BRAF V600E Mutation-Positive Metastatic Colorectal Cancer (CRC)
The recommended dosage of BRAFTOVI is 300 mg (four 75 mg capsules) orally once daily in combination with cetuximab until disease progression or unacceptable toxicity. Refer to the cetuximab prescribing information for recommended cetuximab dosing information.
2.4 Administration
BRAFTOVI may be taken with or without food [see Clinical Pharmacology (12.3)]. Do not take a missed dose of BRAFTOVI within 12 hours of the next dose of BRAFTOVI.
Do not take an additional dose if vomiting occurs after BRAFTOVI administration but continue with the next scheduled dose.
2.5 Dosage Modifications for Adverse Reactions
BRAF V600E or V600K Mutation-Positive Unresectable or Metastatic Melanoma or BRAF V600E Mutation-Positive Metastatic NSCLC
If binimetinib is withheld, reduce BRAFTOVI to a maximum dose of 300 mg (four 75 mg capsules) once daily until binimetinib is resumed [see Warnings and Precautions (5.9)].
Dose reductions for adverse reactions associated with BRAFTOVI are presented in Table 1.
Table 1: Recommended Dose Reductions for BRAFTOVI for Adverse Reactions – Melanoma or NSCLC
Action Recommended Dose First Dose Reduction
300 mg (four 75 mg capsules) orally once daily
Second Dose Reduction
225 mg (three 75 mg capsules) orally once daily
Subsequent Modification
Permanently discontinue if unable to tolerate BRAFTOVI 225 mg (three 75 mg capsules) once daily
BRAF V600E Mutation-Positive Metastatic Colorectal Cancer (CRC)
If cetuximab is discontinued, discontinue BRAFTOVI.
Dose reductions for adverse reactions associated with BRAFTOVI are presented in Table 2.
Table 2: Recommended Dose Reductions for BRAFTOVI for Adverse Reactions – CRC Action Recommended Dose First Dose Reduction
225 mg (three 75 mg capsules) orally once daily
Second Dose Reduction
150 mg (two 75 mg capsules) orally once daily
Subsequent Modification
Permanently discontinue if unable to tolerate BRAFTOVI 150 mg (two 75 mg capsules) once daily
BRAF V600E or V600K Mutation-Positive Unresectable or Metastatic Melanoma, BRAF V600E Mutation-Positive Metastatic Colorectal Cancer (CRC), or BRAF V600E Mutation-Positive NSCLC
Dosage modifications for adverse reactions associated with BRAFTOVI are presented in Table 3.
Table 3: Recommended Dosage Modifications for BRAFTOVI for Adverse Reactions Severity of Adverse Reaction* Dose Modification for BRAFTOVI - *
- National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) version 4.03.
- †
- Dose modification of BRAFTOVI when administered with binimetinib or with cetuximab is not recommended for new primary cutaneous malignancies; ocular events other than uveitis, iritis, and iridocyclitis; interstitial lung disease/pneumonitis; creatine phosphokinase (CPK) elevation; rhabdomyolysis; and venous thromboembolism.
New Primary Malignancies [see Warnings and Precautions (5.1)]
Non-Cutaneous RAS Mutation-positive Malignancies
Permanently discontinue BRAFTOVI.
Cardiomyopathy [see Warnings and Precautions (5.3)]
- •
- Symptomatic congestive heart failure or absolute decrease in LVEF of greater than 20% from baseline that is also below LLN
Reduce BRAFTOVI by one dose level [see Dosage and Administration (2.3)].
- •
- If LVEF improves to at least institutional LLN and absolute decrease to less than or equal to 10% compared to baseline, continue BRAFTOVI at the reduced dose [see Dosage and Administration (2.3)].
- •
- If no improvement, withhold BRAFTOVI until improves to at least institutional LLN and absolute decrease to less than or equal to 10% compared to baseline and then resume at the reduced dose or reduce dose an additional dose level.
Hepatotoxicity [see Warnings and Precautions (5.4)]
- •
- Grade 2 AST or ALT increased
Maintain BRAFTOVI dose.
- •
- If no improvement within 4 weeks, withhold BRAFTOVI until improves to Grade 0-1 or to pretreatment/baseline levels and then resume at same dose.
- •
- Grade 3 or 4 AST or ALT increased
Uveitis [see Warnings and Precautions (5.6)]
- •
- Grade 1–3
If Grade 1 or 2 does not respond to specific ocular therapy, or for Grade 3 uveitis, withhold BRAFTOVI for up to 6 weeks.
- •
- If improved, resume at same or reduced dose.
- •
- If not improved, permanently discontinue BRAFTOVI.
- •
- Grade 4
Permanently discontinue BRAFTOVI.
QTc Prolongation [see Warnings and Precautions (5.7)]
- •
- QTcF greater than 500 ms and less than or equal to 60 ms increase from baseline
Withhold BRAFTOVI until QTcF less than or equal to 500 ms. Resume at reduced dose.
- •
- If more than one recurrence, permanently discontinue BRAFTOVI.
- •
- QTcF greater than 500 ms and greater than 60 ms increase from baseline
Permanently discontinue BRAFTOVI.
Dermatologic [other than Hand-foot Skin Reaction (HFSR)] [see Adverse Reactions (6.1)]
- •
- Grade 2
If no improvement within 2 weeks, withhold BRAFTOVI until Grade 0–1. Resume at same dose.
- •
- Grade 3
Withhold BRAFTOVI until Grade 0–1. Resume at same dose if first occurrence or reduce dose if recurrent.
- •
- Grade 4
Permanently discontinue BRAFTOVI.
Other Adverse Reactions (including Hemorrhage) [see Warnings and Precautions (5)] and HFSR [see Adverse Reactions (6.1)]†
- •
- Recurrent Grade 2 or
- •
- First occurrence of any Grade 3
Withhold BRAFTOVI for up to 4 weeks.
- •
- If improves to Grade 0–1 or to pretreatment/baseline level, resume at reduced dose.
- •
- If no improvement, permanently discontinue BRAFTOVI.
- •
- First occurrence of any Grade 4
Permanently discontinue BRAFTOVI or
Withhold BRAFTOVI for up to 4 weeks.- •
- If improves to Grade 0–1 or to pretreatment/baseline level, then resume at reduced dose.
- •
- If no improvement, permanently discontinue BRAFTOVI.
- •
- Recurrent Grade 3
Consider permanently discontinuing BRAFTOVI.
- •
- Recurrent Grade 4
Permanently discontinue BRAFTOVI.
Refer to the binimetinib or cetuximab prescribing information for dose modifications for adverse reactions associated with each product, as appropriate.
2.6 Dose Modifications for Coadministration With Strong or Moderate CYP3A4 Inhibitors
Avoid coadministration of BRAFTOVI with strong or moderate CYP3A4 inhibitors. If coadministration is unavoidable, reduce the BRAFTOVI dose according to the recommendations in Table 4. After the inhibitor has been discontinued for 3 to 5 elimination half-lives, resume the BRAFTOVI dose that was taken prior to initiating the CYP3A4 inhibitor [see Drug Interactions (7.1), Clinical Pharmacology (12.3)].
Table 4: Recommended Dose Reductions for BRAFTOVI for Coadministration With Strong or Moderate CYP3A4 Inhibitors Current Daily Dose* Dose for Coadministration with Moderate CYP3A4 Inhibitor Dose for Coadministration with Strong CYP3A4 Inhibitor - *
- Current daily dose refers to recommended dose of BRAFTOVI based on indication or reductions for adverse reactions based on dosing recommendations in Table 1 (Melanoma) and Table 2 (CRC).
- †
- Encorafenib exposure at the 75 mg QD BRAFTOVI dosage when coadministered with a strong CYP3A4 inhibitor is expected to be higher than at the 150 mg QD dosage in the absence of a CYP3A4 inhibitor and similar to exposure at the 225 mg QD dosage in the absence of a CYP3A4 inhibitor. Monitor patients closely for adverse reactions and use clinical judgement when using BRAFTOVI with strong CYP3A4 inhibitors at the 150 mg dose level.
450 mg
225 mg (three 75 mg capsules)
150 mg (two 75 mg capsules)
300 mg
150 mg (two 75 mg capsules)
75 mg
225 mg
75 mg
75 mg
150 mg
75 mg
75 mg†
- 3 DOSAGE FORMS AND STRENGTHS
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 New Primary Malignancies
New primary malignancies, cutaneous and non-cutaneous, have been observed in patients treated with BRAF inhibitors and can occur with BRAFTOVI.
Cutaneous Malignancies
In COLUMBUS, cutaneous squamous cell carcinoma (cuSCC), including keratoacanthoma (KA), occurred in 2.6%, and basal cell carcinoma occurred in 1.6% of patients who received BRAFTOVI in combination with binimetinib. Median time to first occurrence of cuSCC/KA was 5.8 months (range 1 to 9 months) [see Adverse Reactions (6.1)].
For patients who received BRAFTOVI as a single agent, cuSCC/KA was reported in 8%, basal cell carcinoma in 1%, and a new primary melanoma in 5% of patients.
In BEACON CRC, cuSCC/KA occurred in 1.4% of patients with CRC, and a new primary melanoma occurred in 1.4% of patients who received BRAFTOVI in combination with cetuximab.
In PHAROS, cuSCC and skin papilloma, each occurred in 2% of patients who received BRAFTOVI in combination with binimetinib.
Perform dermatologic evaluations prior to initiating treatment, every 2 months during treatment, and for up to 6 months following discontinuation of treatment. Manage suspicious skin lesions with excision and dermatopathologic evaluation. Dose modification is not recommended for new primary cutaneous malignancies.
Non-Cutaneous Malignancies
Based on its mechanism of action, BRAFTOVI may promote malignancies associated with activation of RAS through mutation or other mechanisms [see Warnings and Precautions (5.2)]. Monitor patients receiving BRAFTOVI for signs and symptoms of non-cutaneous malignancies. Discontinue BRAFTOVI for RAS mutation-positive non-cutaneous malignancies [see Dosage and Administration (2.5)].
5.2 Tumor Promotion in BRAF Wild-Type Tumors
In vitro experiments have demonstrated paradoxical activation of MAP-kinase signaling and increased cell proliferation in BRAF wild-type cells, which are exposed to BRAF inhibitors. Confirm evidence of BRAF V600E or V600K mutation prior to initiating BRAFTOVI [see Indications and Usage (1), Dosage and Administration (2.1)].
5.3 Cardiomyopathy
Cardiomyopathy, manifesting as left ventricular dysfunction associated with symptomatic or asymptomatic decreases in ejection fraction, has been reported in patients treated with BRAFTOVI in combination with binimetinib. In COLUMBUS, evidence of cardiomyopathy (decreased in LVEF below the institutional LLN with an absolute decreased in LVEF ≥10% below baseline as detected by echocardiography or MUGA) occurred in 7% of patients receiving BRAFTOVI plus binimetinib. Grade 3 left ventricular dysfunction occurred in 1.6% of patients. The median time to first occurrence of left ventricular dysfunction (any grade) in patients receiving BRAFTOVI in combination with binimetinib was 3.6 months (range 0 to 21 months). Cardiomyopathy resolved in 87% of patients receiving BRAFTOVI plus binimetinib.
In PHAROS, evidence of cardiomyopathy (decrease in LVEF below the institutional LLN with an absolute decrease in LVEF ≥10% below baseline as detected by echocardiography or MUGA) occurred in 11% of patients receiving BRAFTOVI in combination with binimetinib. Grade 3 left ventricular dysfunction occurred in 1% of patients. Cardiomyopathy resolved in 82% of patients receiving BRAFTOVI plus binimetinib.
Assess ejection fraction by echocardiogram or MUGA scan prior to initiating treatment, one month after initiating treatment, and every 2 to 3 months during treatment. The safety of BRAFTOVI in combination with binimetinib has not been established in patients with baseline ejection fraction that is either below 50% or below the institutional lower limit of normal (LLN). Patients with cardiovascular risk factors should be monitored closely when treated with BRAFTOVI.
Withhold, reduce dose, or permanently discontinue based on severity of adverse reaction [see Dosage and Administration (2.3), Adverse Reactions (6.1)].
5.4 Hepatotoxicity
Hepatotoxicity can occur when BRAFTOVI is administered in combination with binimetinib. In COLUMBUS, the incidence of Grade 3 or 4 increases in liver function laboratory tests in patients receiving BRAFTOVI in combination with binimetinib was 6% for alanine aminotransferase (ALT), 2.6% for aspartate aminotransferase (AST), and 0.5% for alkaline phosphatase. In PHAROS, the incidence of Grade 3 or 4 increases in liver function laboratory tests in patients receiving BRAFTOVI in combination with binimetinib was 10% for AST, 9% for ALT, and 3.2% for alkaline phosphatase.
Monitor liver laboratory tests before initiation of BRAFTOVI, monthly during treatment, and as clinically indicated. Withhold, reduce dose, or permanently discontinue based on severity of adverse reaction [see Dosage and Administration (2.3), Adverse Reactions (6.1)].
5.5 Hemorrhage
In COLUMBUS, hemorrhage occurred in 19% of patients receiving BRAFTOVI in combination with binimetinib; Grade 3 or greater hemorrhage occurred in 3.2% of patients. The most frequent hemorrhagic events were gastrointestinal, including rectal hemorrhage (4.2%), hematochezia (3.1%), and hemorrhoidal hemorrhage (1%). Fatal intracranial hemorrhage in the setting of new or progressive brain metastases occurred in 1.6% of patients.
In BEACON CRC, hemorrhage occurred in 19% of patients receiving BRAFTOVI in combination with cetuximab; Grade 3 or higher hemorrhage occurred in 1.9% of patients, including fatal gastrointestinal hemorrhage in 0.5% of patients. The most frequent hemorrhagic events were epistaxis (6.9%), hematochezia (2.3%), and rectal hemorrhage (2.3%).
In PHAROS, hemorrhage occurred in 12% of patients receiving BRAFTOVI in combination with binimetinib including fatal hemorrhage intracranial (1%); Grade 3 or 4 hemorrhage occurred in 4.1% of patients. The most frequent hemorrhagic events were anal hemorrhage and hemothorax (2% each).
Withhold, reduce dose, or permanently discontinue based on severity of adverse reaction [see Dosage and Administration (2.5), Adverse Reactions (6.1)].
5.6 Uveitis
Uveitis, including iritis and iridocyclitis, has been reported in patients treated with BRAFTOVI in combination with binimetinib. In COLUMBUS, the incidence of uveitis among patients treated with BRAFTOVI in combination with binimetinib was 4%. In PHAROS, the incidence of uveitis among patients treated with BRAFTOVI in combination with binimetinib was 1%.
Assess for visual symptoms at each visit. Perform an ophthalmologic evaluation at regular intervals and for new or worsening visual disturbances, and to follow new or persistent ophthalmologic findings. Withhold, reduce dose, or permanently discontinue based on severity of adverse reaction [see Dosage and Administration (2.5), Adverse Reactions (6.1)].
5.7 QT Prolongation
BRAFTOVI is associated with dose-dependent QTc interval prolongation in some patients [see Clinical Pharmacology (12.2)]. In COLUMBUS, an increase in QTcF to >500 ms was measured in 0.5% (1/192) of patients who received BRAFTOVI in combination with binimetinib. In PHAROS, an increase in QTcF to >500 ms was measured in 2.1% (2/95) of patients who received BRAFTOVI in combination with binimetinib.
Monitor patients who already have or who are at significant risk of developing QTc prolongation, including patients with known long QT syndromes, clinically significant bradyarrhythmias, severe or uncontrolled heart failure and those taking other medicinal products associated with QT prolongation. Correct hypokalemia and hypomagnesemia prior to and during BRAFTOVI administration. Withhold, reduce dose, or permanently discontinue for QTc >500 ms [see Dosage and Administration (2.5), Adverse Reactions (6.1)].
5.8 Embryo-Fetal Toxicity
Based on its mechanism of action, BRAFTOVI can cause fetal harm when administered to a pregnant woman. Encorafenib produced embryo-fetal developmental changes in rats and rabbits and was an abortifacient in rabbits at doses greater than or equal to those resulting in exposures approximately 26 (in the rat) and 178 (in the rabbit) times the human exposure at the recommended dose of 450 mg, with no clear findings at lower doses.
Advise pregnant women and females of reproductive potential of the potential risk to a fetus. Advise females of reproductive potential to use an effective, non-hormonal method of contraception since BRAFTOVI can render hormonal contraceptives ineffective, during treatment and for 2 weeks after the last dose of BRAFTOVI [see Use in Specific Populations (8.1, 8.3)].
5.9 Risks Associated with BRAFTOVI as a Single Agent
BRAFTOVI when used as a single agent is associated with an increased risk of certain adverse reactions compared to when BRAFTOVI is used in combination with binimetinib. In COLUMBUS, Grades 3 or 4 dermatologic reactions occurred in 21% of patients treated with BRAFTOVI single agent compared to 2% of patients treated with BRAFTOVI in combination with binimetinib [see Warnings and Precautions (5.1), Adverse Reactions (6.1)].
If binimetinib is temporarily interrupted or permanently discontinued, reduce the dose of BRAFTOVI as recommended [see Dosage and Administration (2.5)].
-
6 ADVERSE REACTIONS
The following adverse reactions are described elsewhere in the labeling:
- •
- New Primary Malignancies [see Warnings and Precautions (5.1)]
- •
- Tumor Promotion in BRAF Wild-Type Tumors [see Warnings and Precautions (5.2)]
- •
- Cardiomyopathy [see Warnings and Precautions (5.3)]
- •
- Hepatotoxicity [see Warnings and Precautions (5.4)]
- •
- Hemorrhage [see Warnings and Precautions (5.5)]
- •
- Uveitis [see Warnings and Precautions (5.6)]
- •
- QT Prolongation [see Warnings and Precautions (5.7)]
- •
- Embryo-Fetal Toxicity [see Warnings and Precautions (5.8)]
- •
- Risks Associated with BRAFTOVI as a Single Agent [see Warnings and Precautions (5.9)]
- •
- Risks Associated with Combination Treatment [see Warnings and Precautions (5.10)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
BRAF V600E or V600K Mutation-Positive Unresectable or Metastatic Melanoma
The safety of BRAFTOVI in combination with binimetinib is described in 192 patients with BRAF V600 mutation-positive unresectable or metastatic melanoma who received BRAFTOVI (450 mg once daily) in combination with binimetinib (45 mg twice daily) in a randomized open-label, active-controlled trial (COLUMBUS).
The COLUMBUS trial [see Clinical Studies (14.1)] excluded patients with a history of Gilbert's syndrome, abnormal left ventricular ejection fraction, prolonged QTc (>480 ms), uncontrolled hypertension, and history or current evidence of retinal vein occlusion. The median duration of exposure was 11.8 months for patients treated with BRAFTOVI in combination with binimetinib and 6.2 months for patients treated with vemurafenib.
The most common (≥25%) adverse reactions in patients receiving BRAFTOVI in combination with binimetinib were fatigue, nausea, vomiting, abdominal pain, and arthralgia.
Adverse reactions leading to dose interruptions of BRAFTOVI occurred in 30% of patients receiving BRAFTOVI in combination with binimetinib; the most common were nausea (7%), vomiting (7%), and pyrexia (4%). Adverse reactions leading to dose reductions of BRAFTOVI occurred in 14% of patients receiving BRAFTOVI in combination with binimetinib; the most common were arthralgia (2%), fatigue (2%), and nausea (2%). Five percent (5%) of patients receiving BRAFTOVI in combination with binimetinib experienced an adverse reaction that resulted in permanent discontinuation of BRAFTOVI; the most common were hemorrhage in 2% and headache in 1% of patients.
Table 5 and Table 6 present adverse drug reactions and laboratory abnormalities, respectively, identified in COLUMBUS. The COLUMBUS trial was not designed to demonstrate a statistically significant difference in adverse reaction rates for BRAFTOVI in combination with binimetinib, as compared to vemurafenib, for any specific adverse reaction listed in Table 5.
Table 5: Adverse Reactions Occurring in ≥10% of Patients Receiving BRAFTOVI in Combination With Binimetinib in COLUMBUS* Adverse Reaction BRAFTOVI
with binimetinib
N=192Vemurafenib
N=186All
Grades
(%)Grades
3 and 4†
(%)All Grades
(%)Grades
3 and 4
(%)General Disorders and Administration Site Conditions
Fatigue‡
43
3
46
6
Pyrexia‡
18
4
30
0
Gastrointestinal Disorders
Nausea
41
2
34
2
Vomiting‡
30
2
16
1
Abdominal pain‡
28
4
16
1
Constipation
22
0
6
1
Musculoskeletal and Connective Tissue Disorders
Arthralgia‡
26
1
46
6
Myopathy‡
23
0
22
1
Pain in extremity
11
1
13
1
Skin and Subcutaneous Tissue Disorders
Hyperkeratosis‡
23
1
49
1
Rash‡
22
1
53
13
Dry skin‡
16
0
26
0
Alopecia‡
14
0
38
0
Pruritus‡
13
1
21
1
Nervous System Disorders
Headache‡
22
2
20
1
Dizziness‡
15
3
4
0
Peripheral neuropathy‡
12
1
13
2
Vascular Disorders
Hemorrhage‡
19
3
9
2
BRAFTOVI when used as a single agent increases the risk of certain adverse reactions compared to BRAFTOVI in combination with binimetinib. In patients receiving BRAFTOVI 300 mg orally once daily as a single agent, the following adverse reactions were observed at a higher rate (≥5%) compared to patients receiving BRAFTOVI in combination with binimetinib: palmar-plantar erythrodysesthesia syndrome (51% vs. 7%), hyperkeratosis (57% vs. 23%), dry skin (38% vs. 16%), erythema (16% vs. 7%), rash (41% vs. 22%), alopecia (56% vs. 14%), pruritus (31% vs. 13%), arthralgia (44% vs. 26%), myopathy (33% vs. 23%), back pain (15% vs. 9%), dysgeusia (13% vs. 6%), and acneiform dermatitis (8% vs. 3%).
Other clinically important adverse reactions occurring in <10% of patients who received BRAFTOVI in combination with binimetinib were:
Nervous system disorders: Facial paresis
Gastrointestinal disorders: Pancreatitis
Skin and subcutaneous tissue disorders: Panniculitis, Photosensitivity
Immune system disorders: Drug hypersensitivity
Table 6: Laboratory Abnormalities Occurring in ≥10% (All Grades) of Patients Receiving BRAFTOVI in Combination With Binimetinib in COLUMBUS* Laboratory Abnormality BRAFTOVI
with binimetinib*
N=192Vemurafenib*
N=186All
Grades
(%)Grades
3 and 4
(%)All
Grades
(%)Grades
3 and 4
(%)- *
- Grades per National Cancer Institute CTCAE v4.03.
Hematology
Anemia
36
3.6
34
2.2
Leukopenia
13
0
10
0.5
Lymphopenia
13
2.1
30
7
Neutropenia
13
3.1
4.8
0.5
Chemistry
Increased Creatinine
93
3.6
92
1.1
Increased Gamma Glutamyl Transferase
45
11
34
4.8
Increased ALT
29
6
27
2.2
Increased AST
27
2.6
24
1.6
Hyperglycemia
28
5
20
2.7
Increased Alkaline Phosphatase
21
0.5
35
2.2
Hyponatremia
18
3.6
15
0.5
Hypermagnesemia
10
1.0
26
0.5
BRAF V600E Mutation-Positive Metastatic Colorectal Cancer (CRC)
The safety of BRAFTOVI 300 mg once daily in combination with cetuximab (400 mg/m2 initial dose, followed by 250 mg/m2 weekly) was evaluated in 216 patients with BRAF V600E mutation-positive metastatic CRC in a randomized, open-label, active-controlled trial (BEACON CRC). The BEACON CRC trial [see Clinical Studies (14.2)] excluded patients with a history of Gilbert's syndrome, abnormal left ventricular ejection fraction, prolonged QTc (>480 ms), uncontrolled hypertension, and history or current evidence of retinal vein occlusion. The median duration of exposure was 4.4 months for patients treated with BRAFTOVI in combination with cetuximab and 1.6 months for patients treated with either irinotecan or infusional 5-fluorouracil (5-FU)/folinic acid (FA)/irinotecan (FOLFIRI) in combination with cetuximab.
The most common (≥25%) adverse reactions in patients receiving BRAFTOVI in combination with cetuximab were fatigue, nausea, diarrhea, dermatitis acneiform, abdominal pain, decreased appetite, arthralgia, and rash.
Adverse reactions leading to dose interruptions of BRAFTOVI occurred in 33% of patients receiving BRAFTOVI in combination with cetuximab; the most common were vomiting (4%), fatigue (4%), nausea (4%), pyrexia (3%), and diarrhea (3%). Adverse reactions leading to dose reductions of BRAFTOVI occurred in 9% of patients receiving BRAFTOVI in combination with cetuximab; the most common were fatigue (2%), arthralgia (2%), and peripheral neuropathy (2%). Ten percent (10%) of patients receiving BRAFTOVI in combination with cetuximab experienced an adverse reaction that resulted in permanent discontinuation of BRAFTOVI. None of the adverse reactions leading to permanent discontinuation of BRAFTOVI occurred in more than one patient (>0.5%).
Table 7 and Table 8 present adverse drug reactions and laboratory abnormalities, respectively, identified in BEACON CRC.
Table 7: Adverse Reactions Occurring in ≥10% of Patients Receiving BRAFTOVI in Combination With Cetuximab in BEACON CRC* Adverse Reaction BRAFTOVI
with cetuximab
N=216Irinotecan with cetuximab or FOLFIRI with cetuximab
N=193All
Grades
(%)≥ Grade 3†
(%)All
Grades
(%)≥ Grade 3
(%)General Disorders and Administration Site Conditions
Fatigue‡
51
7
50
8
Pyrexia‡
17
1
15
1
Gastrointestinal Disorders
Nausea
34
1
41
1
Diarrhea‡
33
2
48
10
Abdominal pain‡
30
4
32
5
Vomiting
21
1
29
3
Constipation
15
0
18
1
Metabolism and Nutrition Disorders
Decreased appetite
27
1
27
3
Musculoskeletal and Connective Tissue Disorders
Arthralgia‡
27
1
3
0
Myopathy‡
15
1
4
0
Pain in extremity
10
0
1
0
Skin and Subcutaneous Tissue Disorders
Dermatitis acneiform‡
32
1
43
3
Rash‡
26
0
26
2
Pruritus‡
14
0
6
0
Melanocytic nevus
14
0
0
0
Dry skin‡
13
0
12
1
Nervous System Disorders
Headache‡
20
0
3
0
Peripheral neuropathy‡
12
1
6
0
Vascular Disorders
Hemorrhage‡
19
2
9
0
Psychiatric Disorders
Insomnia‡
13
0
6
0
Other clinically important adverse reactions occurring in <10% of patients who received BRAFTOVI in combination with cetuximab were:
Gastrointestinal disorders: Pancreatitis
Table 8: Laboratory Abnormalities Occurring in ≥10% (All Grades) of Patients Receiving BRAFTOVI in Combination With Cetuximab in BEACON CRC* Laboratory Abnormality† BRAFTOVI
with cetuximabIrinotecan with cetuximab or FOLFIRI with cetuximab All
Grades
(%)Grades
3 and 4
(%)All
Grades
(%)Grades
3 and 4
(%)Hematology
Anemia
34
4
48
5
Lymphopenia
24
7
35
5
Increased Activated Partial Thromboplastin Time
13
1
7
1
Chemistry
Hypomagnesemia
19
0
22
1
Increased Alkaline Phosphatase
18
4
30
7
Increased ALT
17
0
29
3
Increased AST
15
1
22
2
Hypokalemia
12
3
32
5
Hyponatremia
11
2
13
2
BRAF V600E Mutation-Positive Metastatic Non-Small Cell Lung Cancer (NSCLC)
The safety of BRAFTOVI in combination with binimetinib was evaluated in 98 patients with BRAF V600E mutation-positive metastatic NSCLC who received BRAFTOVI (450 mg once daily) in combination with binimetinib (45 mg twice daily) in an open-label, single-arm trial (PHAROS).
The PHAROS trial [see Clinical Studies (14.3)] excluded patients with abnormal left ventricular ejection fraction, prolonged QTc (>480 ms), uncontrolled hypertension, and history or current evidence of retinal vein occlusion. The median duration of treatment for BRAFTOVI and binimetinib was 9.2 and 8.4 months, respectively.
The most common (≥25%) adverse reactions in patients receiving BRAFTOVI were fatigue, nausea, diarrhea, musculoskeletal pain, vomiting, abdominal pain, visual impairment, constipation, dyspnea, rash, and cough.
Adverse reactions leading to dose interruptions of BRAFTOVI occurred in 59% of patients receiving BRAFTOVI; the most common (≥5%) were diarrhea (17%); nausea (13%); musculoskeletal pain, fatigue (8% each); AST increased (7%); ALT increased, anemia, hemorrhage, vomiting (6% each); and acute kidney injury (5%). Adverse reactions leading to dose reductions of BRAFTOVI occurred in 30% of patients receiving BRAFTOVI; the most common (≥5%) were diarrhea, nausea (8% each); AST increased and fatigue (5% each). A total of 16% of patients receiving BRAFTOVI experienced an adverse reaction that resulted in permanent discontinuation of BRAFTOVI; the most common (≥2%) were diarrhea, musculoskeletal pain (3.1% each); fatigue, rash, nausea, visual impairment, and vomiting (2% each). None of the other adverse reactions leading to permanent discontinuation of BRAFTOVI occurred in more than 1 patient.
Serious adverse reactions occurred in 38% of patients who received BRAFTOVI in combination with binimetinib. Serious adverse reactions occurring in ≥2% of patients were hemorrhage (6%); diarrhea (4.1%); anemia, dyspnea, pneumonia (3.1% each); arrhythmia, device related infection, edema, myocardial infarction, and pleural effusion (2% each). Fatal adverse reactions occurred in 2% of patients who received BRAFTOVI (450 mg once daily) in combination with binimetinib, including intracranial hemorrhage and myocardial infarction (1% each).
Table 9 and Table 10 present adverse drug reactions and laboratory abnormalities, respectively, identified in PHAROS.
Table 9: Adverse Reactions Occurring in ≥10% of Patients Receiving BRAFTOVI in Combination with Binimetinib in PHAROS* - *
- Grades per National Cancer Institute CTCAE v4.03.
- †
- One Grade 5 adverse reaction of hemorrhage occurred.
- ‡
- Fatigue includes fatigue, asthenia.
- §
- Edema includes edema peripheral, generalized edema, swelling, localized edema, face edema.
- ¶
- Diarrhea includes diarrhea, colitis.
- #
- Abdominal pain includes abdominal pain, abdominal pain upper, abdominal discomfort, epigastric discomfort.
- Þ
- Visual impairment includes vision blurred, visual impairment, vitreous floaters, photophobia, visual acuity reduced, photopsia.
- ß
- Musculoskeletal pain includes back pain, arthralgia, pain in extremity, myalgia, musculoskeletal chest pain, non-cardiac chest pain, neck pain.
- à
- Rash includes rash, rash macular, rash maculo-papular, rash papular, rash pustular, dermatitis acneiform, palmar-plantar erythrodysesthesia syndrome, eczema, skin exfoliation.
- è
- Pruritis includes pruritus, pruritus genital.
- ð
- Dyspnea includes dyspnea, dyspnea exertional.
- ø
- Cough includes cough, productive cough.
- ý
- Dizziness includes dizziness, balance disorder.
- £
- Hemorrhage includes anal hemorrhage, hemothorax, gastrointestinal hemorrhage, hematochezia, hematuria, hemoptysis, hemorrhage intracranial, hyphema, small intestinal hemorrhage, upper gastrointestinal hemorrhage, vaginal hemorrhage.
- ¥
- Left ventricular dysfunction/cardiomyopathy includes ejection fraction decreased, cardiac failure, cardiac failure congestive.
Adverse Reaction
BRAFTOVI
with binimetinib
N=98All
Grades
(%)
Grades 3 and 4†
(%)
General Disorders and Administration Site Conditions
Fatigue‡
61
8
Edema§
23
1
Pyrexia
22
0
Gastrointestinal Disorders
Nausea
58
3.1
Diarrhea¶
52
7
Vomiting
37
1
Abdominal pain#
32
1
Constipation
27
0
Eye Disorders
Visual impairmentÞ
29
2
Musculoskeletal and Connective Tissue Disorders
Musculoskeletal painß
48
4.1
Skin and Subcutaneous Tissue Disorders
Rashà
27
3.1
Pruritisè
16
0
Dry skin
13
0
Alopecia
12
0
Respiratory, Thoracic and Mediastinal Disorders
Dyspneað
27
8
Coughø
26
0
Nervous System Disorders
Dizzinessý
17
1
Headache
11
0
Metabolism and Nutrition Disorders
Decreased appetite
14
1
Vascular Disorders
12
4.1
Hypertension
10
5
Cardiac Disorders
Left ventricular dysfunction/cardiomyopathy¥
11
1
Investigations
Weight increased
11
1
Psychiatric Disorders
Insomnia
10
0
Other clinically important adverse reactions occurring in <10% of patients who received BRAFTOVI in combination with binimetinib were:
Nervous system disorders: Peripheral neuropathy, Dysgeusia, Facial paresis
Gastrointestinal disorders: Pancreatitis
Skin and subcutaneous tissue disorders: Hyperkeratosis, Erythema, Photosensitivity
Immune system disorders: Drug hypersensitivity
Table 10: Laboratory Abnormalities Occurring in ≥10% (All Grades) of Patients Receiving BRAFTOVI with Binimetinib* Laboratory Abnormality†
BRAFTOVI with binimetinib
All
Grades
(%)
Grades
3 and 4
(%)
Hematology
Anemia
47
11
Lymphopenia
24
6
Thrombocytopenia
20
1.1
Leukopenia
12
0
Neutropenia
12
1.1
Chemistry
Increased creatinine
91
3.2
Hyperglycemia
48
6
Increased creatine kinase
41
3.3
Lipase increased
40
14
Increased ALT
34
9
Hypoalbuminemia
32
0
Increased AST
31
10
Increased alkaline phosphatase
31
3.2
Hyperkalemia
31
2.1
Hyponatremia
26
11
Serum amylase increased
22
1.1
Hypocalcemia
12
2.1
-
7 DRUG INTERACTIONS
7.1 Effect of Other Drugs on BRAFTOVI
Strong or Moderate CYP3A4 Inhibitors
Coadministration of BRAFTOVI with a strong or moderate CYP3A4 inhibitor increases encorafenib plasma concentrations [see Clinical Pharmacology (12.3)] and may increase encorafenib adverse reactions. Avoid coadministration of BRAFTOVI with strong or moderate CYP3A4 inhibitors, including grapefruit juice. If coadministration is unavoidable, reduce the BRAFTOVI dose [see Dosage and Administration (2.6)].
Strong CYP3A4 Inducers
Coadministration of BRAFTOVI with a strong CYP3A4 inducer may decrease encorafenib plasma concentrations [see Clinical Pharmacology (12.3)] and may decrease encorafenib efficacy. Avoid coadministration of BRAFTOVI with strong CYP3A4 inducers.
7.2 Effect of BRAFTOVI on Other Drugs
Sensitive CYP3A4 Substrates
BRAFTOVI is a strong CYP3A4 inducer at steady-state. Concomitant use of BRAFTOVI may decrease the plasma concentrations of CYP3A4 substrates (including hormonal contraceptives), [see Clinical Pharmacology (12.3)], which may reduce the efficacy of these substrates. Avoid the coadministration of BRAFTOVI with CYP3A4 substrates for which a decrease in plasma concentration may lead to reduced efficacy of the substrate. If the coadministration cannot be avoided, see the CYP3A4 substrate product labeling for recommendations.
OATP1B1, OATP1B3, or BCRP Substrates
Coadministration of BRAFTOVI with OATP1B1, OATP1B3, or BCRP substrates can result in increased concentrations of the substrates, and may increase toxicity of these agents. When used in combination, monitor patients closely for signs and symptoms of increased exposure and consider adjusting the dose of these substrates [see Clinical Pharmacology (12.3)].
7.3 Drugs That Prolong the QT Interval
BRAFTOVI is associated with dose-dependent QTc interval prolongation [see Warnings and Precautions (5.7), Clinical Pharmacology (12.2)]. Avoid coadministration of BRAFTOVI with drugs known to prolong the QT/QTc interval.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Based on its mechanism of action, BRAFTOVI can cause fetal harm when administered to a pregnant woman [see Clinical Pharmacology (12.1)]. There are no available clinical data on the use of BRAFTOVI during pregnancy. In animal reproduction studies, encorafenib produced embryo-fetal developmental changes in rats and rabbits and was an abortifacient in rabbits at doses greater than or equal to those resulting in exposures approximately 26 (in the rat) and 178 (in the rabbit) times the human exposure at the clinical dose of 450 mg, with no clear findings at lower doses (see Data). Advise pregnant women and females of reproductive potential of the potential risk to a fetus.
In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Animal Data
In reproductive toxicity studies, administration of encorafenib to rats during the period of organogenesis resulted in maternal toxicity, decreased fetal weights, and increased incidence of total skeletal variations at a dose of 20 mg/kg/day (approximately 26 times the human exposure based on area under the concentration-time curve [AUC] at the recommended clinical dose of 450 mg once daily). In pregnant rabbits, administration of encorafenib during the period of organogenesis resulted in maternal toxicity, decreased fetal body weights, increased incidence of total skeletal variations and increased post-implantation loss, including total loss of pregnancy at a dose of 75 mg/kg/day (approximately 178 times the human exposure based on AUC at the recommended clinical dose of 450 mg once daily). While formal placental transfer studies have not been performed, encorafenib exposure in the fetal plasma of both rats and rabbits was up to 1.7% and 0.8%, respectively, of maternal exposure.
8.2 Lactation
Risk Summary
There are no data on the presence of encorafenib or its metabolites in human milk or the effects of encorafenib on the breastfed child, or the effects on milk production. Because of the potential for serious adverse reactions in a breastfed child from BRAFTOVI, advise women not to breastfeed during treatment with BRAFTOVI and for 2 weeks after the last dose.
8.3 Females and Males of Reproductive Potential
BRAFTOVI can cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)].
Pregnancy Testing
Verify the pregnancy status of females of reproductive potential prior to initiating BRAFTOVI [see Use in Specific Populations (8.1)].
Contraception
Females
Advise females of reproductive potential to use effective contraception during treatment with BRAFTOVI and for 2 weeks after the last dose. Counsel patients to use a non-hormonal method of contraception since BRAFTOVI has the potential to render hormonal contraceptives ineffective [see Drug Interactions (7.2)].
Infertility
Males
Based on findings in male rats at doses approximately 13 times the human exposure at the 450 mg clinical dose, use of BRAFTOVI may impact fertility in males [see Nonclinical Toxicology (13.1)].
8.4 Pediatric Use
The safety and effectiveness of BRAFTOVI have not been established in pediatric patients.
8.5 Geriatric Use
Of the 690 patients with BRAF mutation-positive melanoma who received BRAFTOVI in combination with binimetinib across multiple clinical trials, 20% were aged 65 to 74 years and 8% were aged 75 years and older [see Clinical Studies (14.1)].
Of the 216 patients with BRAF V600E mutation-positive metastatic CRC who received BRAFTOVI in combination with cetuximab, 62 (29%) were 65 years of age to up to 75 years of age, while 20 (9%) were 75 years of age and over [see Clinical Studies (14.2)].
Of the 98 patients with BRAF V600E mutation-positive metastatic NSCLC who received BRAFTOVI with binimetinib, 62 (63%) were 65 years of age and over and 20 (20%) were 75 years and over [see Clinical Studies (14.3)].
No overall differences in the safety or effectiveness of BRAFTOVI plus binimetinib or BRAFTOVI plus cetuximab were observed in older patients as compared to younger patients.
8.6 Hepatic Impairment
No BRAFTOVI dosage adjustment is recommended in patients with mild hepatic impairment (Child-Pugh Class A) [see Clinical Pharmacology (12.3)]. A recommended dosage has not been established in patients with moderate (Child-Pugh Class B) or severe (Child-Pugh Class C) hepatic impairment.
8.7 Renal Impairment
No BRAFTOVI dosage adjustment is recommended in patients with mild to moderate renal impairment (CLcr 30 to <90 mL/min) [see Clinical Pharmacology (12.3)]. A recommended dosage has not been established in patients with severe renal impairment (CLcr <30 mL/min).
- 10 OVERDOSAGE
-
11 DESCRIPTION
Encorafenib is a kinase inhibitor. The chemical name is methyl N-{(2S)-1-[(4-{3-[5-chloro-2-fluoro-3-(methanesulfonamido)phenyl]-1-(propan-2-yl)-1H-pyrazol-4-yl}pyrimidin-2-yl)amino]propan-2-yl}carbamate. The molecular formula is C22H27ClFN7O4S and the molecular weight is 540 daltons. The chemical structure of encorafenib is shown below:
Encorafenib is a white to almost white powder. In aqueous media, encorafenib is slightly soluble at pH 1, very slightly soluble at pH 2, and insoluble at pH 3 and higher.
BRAFTOVI (encorafenib) capsules for oral use contain 75 mg of encorafenib with the following inactive ingredients: copovidone, poloxamer 188, microcrystalline cellulose, succinic acid, crospovidone, colloidal silicon dioxide, magnesium stearate (vegetable origin). The capsule shell contains gelatin, titanium dioxide, iron oxide red, iron oxide yellow, ferrosoferric oxide, monogramming ink (pharmaceutical glaze, ferrosoferric oxide, propylene glycol).
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Encorafenib is a kinase inhibitor that targets BRAF V600E, as well as wild-type BRAF and CRAF in in vitro cell-free assays with IC50 values of 0.35, 0.47, and 0.3 nM, respectively. Mutations in the BRAF gene, such as BRAF V600E, can result in constitutively activated BRAF kinases that may stimulate tumor cell growth. Encorafenib was also able to bind to other kinases in vitro including JNK1, JNK2, JNK3, LIMK1, LIMK2, MEK4, and STK36 and reduce ligand binding to these kinases at clinically achievable concentrations (≤0.9 µM).
Encorafenib inhibited in vitro growth of tumor cell lines expressing BRAF V600 E, D, and K mutations. In mice implanted with tumor cells expressing BRAF V600E, encorafenib induced tumor regressions associated with RAF/MEK/ERK pathway suppression.
Encorafenib and binimetinib target two different kinases in the RAS/RAF/MEK/ERK pathway. Compared with either drug alone, coadministration of encorafenib and binimetinib resulted in greater anti-proliferative activity in vitro in BRAF mutation-positive cell lines and greater anti-tumor activity with respect to tumor growth inhibition in BRAF V600E mutant human melanoma xenograft studies in mice. Additionally, the combination of encorafenib and binimetinib delayed the emergence of resistance in BRAF V600E mutant human melanoma xenografts in mice compared to either drug alone. In a BRAF V600E mutant NSCLC patient-derived xenograft model in mice, coadministration of encorafenib and binimetinib resulted in greater anti-tumor activity compared to binimetinib alone, with respect to tumor growth inhibition. Increased tumor growth delay after dosing cessation was also observed with the coadmnistration compared to either drug alone.
In the setting of BRAF-mutant CRC, induction of EGFR-mediated MAPK pathway activation has been identified as a mechanism of resistance to BRAF inhibitors. Combinations of a BRAF inhibitor and agents targeting EGFR have been shown to overcome this resistance mechanism in nonclinical models. Coadministration of encorafenib and cetuximab had an anti-tumor effect greater than either drug alone, in a mouse model of colorectal cancer with mutated BRAF V600E.
12.2 Pharmacodynamics
Cardiac Electrophysiology
A dedicated study to evaluate the QT prolongation potential of BRAFTOVI has not been conducted. BRAFTOVI is associated with dose-dependent QTc interval prolongation. Based on a central tendency analysis of QTc in a study of adult patients with melanoma who received the recommended dose of BRAFTOVI in combination with binimetinib, the largest mean (90% CI) QTcF change from baseline (ΔQTcF) was 18 (14 to 22) ms [see Warnings and Precautions (5.7)].
12.3 Pharmacokinetics
The pharmacokinetics of encorafenib were studied in healthy subjects and patients with solid tumors, including advanced and unresectable or metastatic cutaneous melanoma harboring a BRAF V600E or V600K mutation, BRAF V600E mutation-positive metastatic CRC. After a single dose, systemic exposure of encorafenib was dose proportional over the dose range of 50 mg to 700 mg (0.1 to 1.6 times the maximum recommended dose of 450 mg). After once-daily dosing, systemic exposure of encorafenib was less than dose proportional over the dose range of 50 mg to 800 mg (0.1 to 1.8 times the maximum recommended dose of 450 mg). Steady-state was reached within 15 days, with exposure being 50% lower compared to Day 1; intersubject variability (CV%) of AUC ranged from 12% to 69%.
Absorption
The median Tmax of encorafenib is 2 hours. At least 86% of the dose is absorbed.
Effect of Food
Following administration of a single dose of BRAFTOVI 100 mg (0.2 times the maximum recommended dose of 450 mg) with a high-fat, high-calorie meal (consisting of approximately 150 calories from protein, 350 calories from carbohydrates, and 500 calories from fat) the mean maximum encorafenib concentration (Cmax) decreased by 36% and there was no effect on AUC.
Distribution
The geometric mean (CV%) of apparent volume of distribution is 164 L (70%). The protein binding of encorafenib is 86% in vitro. The blood-to-plasma concentration ratio is 0.58.
Elimination
The mean (CV%) terminal half-life (t1/2) of encorafenib is 3.5 hours (17%), and the apparent clearance is 14 L/h (54%) at day 1, increasing to 32 L/h (59%) at steady-state at the maximum recommended dose of 450 mg.
Specific Populations
No clinically significant differences in the pharmacokinetics of encorafenib were observed based on age (19 to 94 years), sex, body weight (34 to 168 kg), mild hepatic impairment (Child-Pugh Class A), and mild or moderate renal impairment (CLcr 30 to <90 mL/min). The effect of race or ethnicity, moderate or severe hepatic impairment (Child-Pugh Class B or C), and severe renal impairment (CLcr <30 mL/min) on encorafenib pharmacokinetics have not been studied.
Drug Interaction Studies
Clinical Studies
CYP3A4 Inhibitors: Coadministration of posaconazole (strong CYP3A4 inhibitor) or diltiazem (moderate CYP3A4 inhibitor) increased AUC of encorafenib by 3- and 2-fold, respectively, and increased Cmax by 68% and 45%, respectively, after a single dose of 50 mg BRAFTOVI (0.1 times the maximum recommended dose of 450 mg).
Strong CYP3A4 Inducers: The effect of a strong CYP3A4 inducer on encorafenib exposure has not been studied [see Drug Interactions (7.1)].
Moderate CYP3A4 Inducers: Repeat dose administration of BRAFTOVI 450 mg once daily and binimetinib 45 mg twice daily with modafinil, a moderate CYP3A4 inducer, decreased encorafenib steady-state AUC by 24% and Cmax by 20%, compared to BRAFTOVI alone.
Effect of encorafenib on CYP3A4 Substrates: Repeat dose administration of BRAFTOVI 450 mg once daily and binimetinib 45 mg twice daily with a single dose of midazolam 2 mg, a sensitive CYP3A4 substrate, decreased midazolam AUC by 82% and Cmax by 74% relative to midazolam 2 mg alone.
Effect of encorafenib on Other CYP Substrates: There was no clinically significant effect of repeat dose administration of BRAFTOVI 450 mg once daily and binimetinib 45 mg twice daily on the exposure of substrates of CYP1A2, CYP2B6, CYP2C9, CYP2C19, and CYP2D6.
Proton Pump Inhibitors: No clinically significant differences in encorafenib pharmacokinetics were observed when coadministered with rabeprazole.
Binimetinib: No clinically significant differences in the pharmacokinetics of binimetinib (UGT1A1 substrate) were observed when coadministered with BRAFTOVI (UGT1A1 inhibitor).
In Vitro Studies
Transporters: Encorafenib is a substrate of P-glycoprotein (P-gp) but not of breast cancer resistance protein (BCRP), multidrug resistance-associated protein 2 (MRP2), organic anion transporting polypeptide (OATP1B1, OATP1B3) or organic cation transporter (OCT1) at clinically relevant plasma concentrations.
Encorafenib is an inhibitor of P-gp, BCRP, OCT2, organic anion transporter (OAT1, OAT3), OATP1B1, and OATP1B3, but not of OCT1 or MRP2 at clinically relevant plasma concentrations.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies with encorafenib have not been conducted. Encorafenib was not genotoxic in studies evaluating reverse mutations in bacteria, chromosomal aberrations in mammalian cells, or micronuclei in bone marrow of rats.
No dedicated fertility studies were performed with encorafenib in animals. In a general toxicology study in rats, decreased testes and epididymis weights, tubular degeneration in testes, and oligospermia in epididymides were observed at doses approximately 13 times the human exposure at the 450 mg clinical dose based on AUC. No effects on reproductive organs were observed in either sex in any of the non-human primate toxicity studies.
13.2 Animal Toxicology and/or Pharmacology
Adverse histopathology findings of hyperplasia and hyperkeratosis occurred in the stomach of rats at encorafenib doses of 20 mg/kg/day (approximately 14 times the human exposure at the 450 mg clinical dose based on AUC) or greater, in both 4 and 13-week studies.
-
14 CLINICAL STUDIES
14.1 BRAF V600E or V600K Mutation-Positive Unresectable or Metastatic Melanoma
BRAFTOVI in combination with binimetinib was evaluated in a randomized, active-controlled, open-label, multicenter trial (COLUMBUS; NCT01909453). Eligible patients were required to have BRAF V600E or V600K mutation-positive unresectable or metastatic melanoma, as detected using the bioMerieux THxID™BRAF assay. Patients were permitted to have received immunotherapy in the adjuvant setting and one prior line of immunotherapy for unresectable locally advanced or metastatic disease. Prior use of BRAF inhibitors or MEK inhibitors was prohibited. Randomization was stratified by American Joint Committee on Cancer (AJCC) Stage (IIIB, IIIC, IVM1a or IVM1b, versus IVM1c), Eastern Cooperative Oncology Group (ECOG) performance status (0 versus 1), and prior immunotherapy for unresectable or metastatic disease (yes versus no).
Patients were randomized (1:1:1) to receive BRAFTOVI 450 mg once daily in combination with binimetinib 45 mg twice daily (BRAFTOVI in combination with binimetinib), BRAFTOVI 300 mg once daily, or vemurafenib 960 mg twice daily. Treatment continued until disease progression or unacceptable toxicity. Only the results of the approved dosing (BRAFTOVI 450 mg in combination with binimetinib 45 mg) are described below.
The major efficacy outcome measure was progression-free survival (PFS), as assessed by a blinded independent central review, to compare BRAFTOVI in combination with binimetinib with vemurafenib. Additional efficacy outcome measures included overall survival (OS), as well as objective response rate (ORR) and duration of response (DoR) which were assessed by central review.
A total of 577 patients were randomized, 192 to the BRAFTOVI in combination with binimetinib arm, 194 to the BRAFTOVI arm, and 191 to the vemurafenib arm. Of the 383 patients randomized to either the BRAFTOVI in combination with binimetinib or the vemurafenib arms, the median age was 56 years (20 to 89 years), 59% were male, 91% were White, and 72% had baseline ECOG performance status of 0. Ninety-five percent (95%) had metastatic disease, 65% were Stage IVM1c, and 4% received prior CTLA-4, PD-1, or PD-L1 directed antibodies. Twenty-eight percent (28%) had elevated baseline serum lactate dehydrogenase (LDH), 45% had ≥3 organs with tumor involvement at baseline, and 3% had brain metastases. Based on centralized testing, 100% of patients' tumors tested positive for BRAF mutations; BRAF V600E (88%), BRAF V600K (11%), or both (<1%).
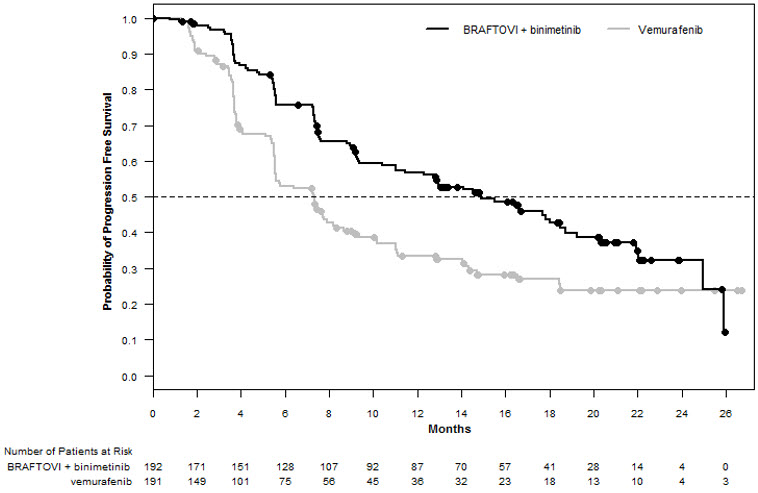
BRAFTOVI in combination with binimetinib demonstrated a statistically significant improvement in PFS compared to vemurafenib. Efficacy results are summarized in Table 11 and Figure 1.
Table 11: Efficacy Results for COLUMBUS BRAFTOVI with
binimetinib
N=192Vemurafenib
N=191CI = Confidence interval; CR = Complete response; DoR = Duration of response; HR = Hazard ratio; NE = Not estimable; ORR = Overall response rate; OS = Overall survival; PFS = Progression-free survival; PR = Partial response. - *
- Estimated with Cox proportional hazard model adjusted by the following stratification factors: American Joint Committee on Cancer (AJCC) Stage (IIIB, IIIC, IVM1a or IVM1b, versus IVM1c) and Eastern Cooperative Oncology Group (ECOG) performance status (0 versus 1).
- †
- Log-rank test adjusted by the same stratification factors.
- ‡
- Based on a cutoff date of 82.4 months after the date of the PFS analysis.
Progression-Free Survival
Number of events (%)
98 (51)
106 (55)
Progressive disease
88 (46)
104 (54)
Death
10 (5)
2 (1)
Median PFS, months (95% CI)
14.9 (11.0, 18.5)
7.3 (5.6, 8.2)
HR (95% CI)*
0.54 (0.41, 0.71)
P-value†
<0.0001
Overall Survival‡
Number of events (%)
139 (72)
147 (77)
Median OS, months (95% CI)
33.6 (24.4, 39.2)
16.9 (14.0, 24.5)
HR (95% CI)*
0.67 (0.53, 0.84)
Overall Response Rate
ORR (95% CI)
63% (56%, 70%)
40% (33%, 48%)
CR
8%
6%
PR
55%
35%
Duration of Response
Median DoR, months (95% CI)
16.6 (12.2, 20.4)
12.3 (6.9, 16.9)
Figure 1: Kaplan-Meier Curves for Progression-Free Survival in COLUMBUS
14.2 BRAF V600E Mutation-Positive Metastatic Colorectal Cancer (CRC)
BRAFTOVI in combination with cetuximab was evaluated in a randomized, active-controlled, open-label, multicenter trial (BEACON CRC; NCT02928224). Eligible patients were required to have BRAF V600E mutation-positive metastatic colorectal cancer (CRC), as detected using the Qiagen therascreen BRAF V600E RGQ polymerase chain reaction (PCR) Kit, with disease progression after 1 or 2 prior regimens. Other key eligibility criteria included absence of prior treatment with a RAF, MEK, or EGFR inhibitor, eligibility to receive cetuximab per local labeling with respect to tumor RAS status, and ECOG performance status (PS) 0–1. Randomization was stratified by Eastern Cooperative Oncology Group (ECOG) performance status (0 versus 1), prior use of irinotecan (yes versus no), and cetuximab product used (US-licensed versus EU-approved).
Patients were randomized 1:1:1 to one of the following treatment arms:
- •
- BRAFTOVI 300 mg orally once daily in combination with cetuximab (BRAFTOVI/cetuximab arm)
- •
- BRAFTOVI 300 mg orally once daily in combination with binimetinib and cetuximab
- •
- Irinotecan with cetuximab or FOLFIRI with cetuximab (control arm)
The dosage of cetuximab in all patients was 400 mg/m2 intravenously for the first dose followed by 250 mg/m2 weekly.
Patients in the control arm received cetuximab with either irinotecan 180 mg/m2 intravenously on Days 1 and 15 of each 28-day cycle or FOLFIRI intravenously (irinotecan 180 mg/m2 on Days 1 and 15; folinic acid 400 mg/m2 on Days 1 and 15; then fluorouracil 400 mg/m2 bolus on Days 1 and 15 followed by fluorouracil 2400 mg/m2/day by continuous infusion over 2 days).
Treatment continued until disease progression or unacceptable toxicity. Only the results of the approved regimen (BRAFTOVI in combination with cetuximab) are described below.
The major efficacy outcome measure was overall survival (OS). Additional efficacy outcome measures included progression-free survival (PFS), overall response rate (ORR), and duration of response (DoR) as assessed by blinded independent central review (BICR). OS and PFS were assessed in all randomized patients. ORR and DoR were assessed in the subset of the first 220 patients included in the randomized portion of the BRAFTOVI/cetuximab and control arm of the study.
A total of 220 patients were randomized to the BRAFTOVI/cetuximab arm and 221 to the control arm. Of these 441 patients, the median age was 61 years; 53% were female; 80% were White and 15% were Asian. Fifty percent (50%) had baseline ECOG performance status of 0; 66% received 1 prior therapy and 34% received 2; 93% received prior oxaliplatin and 52% received prior irinotecan.
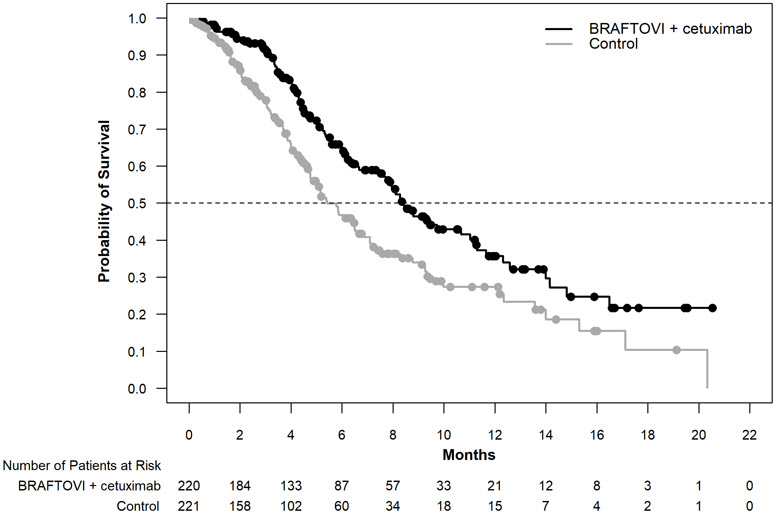
BRAFTOVI in combination with cetuximab demonstrated a statistically significant improvement in OS, ORR, and PFS compared to the active comparator. Efficacy results are summarized in Table 12 and Figure 2.
Table 12: Efficacy Results From BEACON CRC BRAFTOVI with cetuximab
N = 220Irinotecan with cetuximab or FOLFIRI with cetuximab
N = 221CI = Confidence interval; CR = Complete response; DoR = Duration of response; HR = Hazard ratio; NR = Not reached; ORR = Overall response rate; OS = Overall survival; PFS = Progression-free survival; PR = Partial response. - *
- Stratified by ECOG PS, source of cetuximab (US-licensed versus EU-approved) and prior irinotecan use at randomization.
- †
- Stratified Cox proportional hazard model.
- ‡
- Stratified log-rank test, tested at alpha level of 0.0084.
- §
- BRAFTOVI/cetuximab arm (n=113) and control arm (n=107).
- ¶
- Cochran-Mantel-Haenszel test; tested at alpha level of 0.05.
- #
- Stratified log-rank test, tested at alpha level of 0.0234.
Overall Survival
Number of Events (%)
93 (42)
114 (52)
Median OS, months (95% CI)
8.4 (7.5, 11.0)
5.4 (4.8, 6.6)
0.60 (0.45, 0.79)
0.0003
Overall Response Rate (per BICR)
ORR (95% CI)§
20% (13%, 29%)
2% (0%, 7%)
CR
5%
0%
PR
15%
2%
<0.0001
Median DoR, months (95% CI)
6.1 (4.1, 8.3)
NR (2.6, NR)
Progression Free Survival (per BICR)
Number of events (%)
133 (60)
128 (58)
Progressive disease
110 (50)
101 (46)
Death
23 (10)
27 (12)
Median PFS, months (95% CI)
4.2 (3.7, 5.4)
1.5 (1.4, 1.7)
0.40 (0.31, 0.52)
<0.0001
Figure 2: Kaplan-Meier Curves for Overall Survival in BEACON CRC
14.3 BRAF V600E Mutation-Positive Metastatic Non-Small Cell Lung Cancer
BRAFTOVI in combination with binimetinib was evaluated in an open-label, multicenter, single-arm study in patients with BRAF V600E mutation-positive metastatic non-small cell lung cancer (NSCLC) (PHAROS; NCT03915951). Eligible patients had a diagnosis of histologically-confirmed metastatic NSCLC with BRAF V600E mutation that was treatment-naïve or had been previously treated with 1 prior line of systemic therapy in the metastatic setting (platinum-based chemotherapy and/or anti-PD-1/PD-L1 therapies), age 18 years or older, Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0 or 1, and measurable disease as defined by Response Evaluation Criteria in Solid Tumors (RECIST) v1.1. Prior use of BRAF inhibitors or MEK inhibitors was not allowed.
Patients received BRAFTOVI 450 mg once daily and binimetinib 45 mg orally twice daily until disease progression or unacceptable toxicity. The major efficacy outcome measures were objective response rate (ORR) per RECIST v1.1 and duration of response (DoR) as assessed by independent review committee (IRC).
In the efficacy population, BRAF V600E mutation status was determined by prospective local testing using tumor tissue (78%) or blood (22%) specimens. Of the 98 patients with BRAF V600E mutation, 6 patients were enrolled into the trial based on testing of their tumor tissue specimens with the FoundationOne CDx tissue test. Of the remaining 92 patients enrolled based on local testing, 68 patients had their tumor tissue specimens retrospectively confirmed as having BRAF V600E positive status by the FoundationOne CDx tissue test. The remaining patients had either BRAF V600E negative status (n=5) or had unevaluable results (n=19) by the FoundationOne CDx tissue test. In addition, plasma samples from 81 out of 98 patients were retrospectively tested using the FoundationOne Liquid CDx assay. Of the 81 patients, 48 were confirmed positive for BRAF V600E, while 33 patients were BRAF V600E mutation negative by FoundationOne Liquid CDx assay. The remaining 17 samples had unevaluable results with FoundationOne Liquid CDx assay.
The efficacy population included 59 treatment-naïve patients and 39 previously-treated patients. Among these 98 patients, the median age was 70 years (range: 47 to 86); 53% female; 88% White, 7% Asian, 3% Black or African American, and 1% American Indian or Alaska Native; 99% were not Hispanic or Latino; 13% were current smokers and 57% were former smokers; 73% had ECOG PS of 1; and 97% had adenocarcinoma. All patients had metastatic disease, and 8% had brain metastases at baseline.
Efficacy results for patients with BRAF V600E mutation-positive metastatic NSCLC are summarized in Table 13.
Table 13: Efficacy Results for PHAROS CI = Confidence interval; CR = Complete response; DoR = Duration of response; N = Number of patients; NE = Not estimable; ORR = Objective response rate; PR = Partial response. - *
- Assessed by Independent Central Review (ICR).
BRAFTOVI with binimetinib
Efficacy Parameter
Treatment naïve
(N=59)
Previously treated
(N=39)
Objective Response Rate*
ORR (95% CI)
75% (62, 85)
46% (30, 63)
CR
15%
10%
PR
59%
36%
Duration of Response*
N=44
N=18
Median DoR, months (95% CI)
NE (23.1, NE)
16.7 (7.4, NE)
% with DoR ≥6 months
75%
67%
% with DoR ≥12 months
59%
33%
-
16 HOW SUPPLIED/STORAGE AND HANDLING
BRAFTOVI (encorafenib) is supplied as 75 mg hard gelatin capsules.
75 mg: stylized "A" on beige cap and "LGX 75mg" on white body, available in cartons (NDC 70255-025-01) containing two bottles of 90 capsules each (NDC 70255-025-02) and cartons (NDC 70255-025-03) containing two bottles of 60 capsules each (NDC 70255-025-04).
Store at 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C and 30°C (59°F and 86°F) [see USP Controlled Room Temperature]. Do not use if safety seal under cap is broken or missing. Dispense in original bottle. Do not remove desiccant. Protect from moisture. Keep container tightly closed.
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Inform patients of the following:
New Primary Malignancies
Advise patients that BRAFTOVI increases the risk of developing new primary cutaneous and non-cutaneous malignancies. Advise patients to contact their healthcare provider immediately for change in or development of new skin lesions [see Warnings and Precautions (5.1)].
Tumor Promotion in BRAF Wild-Type Tumors
Advise patients of the need to confirm BRAF V600E or V600K mutation prior to initiating BRAFTOVI [see Warnings and Precautions (5.2)].
Cardiomyopathy
Advise patients to report any symptoms of heart failure to their healthcare provider [see Warnings and Precautions (5.3)].
Hepatotoxicity
Advise patients that serial testing of serum liver tests (ALT, AST, bilirubin) is recommended during treatment with BRAFTOVI. Instruct patients to report symptoms of liver dysfunction including jaundice, dark urine, nausea, vomiting, loss of appetite, fatigue, bruising, or bleeding [see Warnings and Precautions (5.4)].
Hemorrhage
Advise patients to notify their healthcare provider immediately with any symptoms suggestive of hemorrhage, such as unusual bleeding [see Warnings and Precautions (5.5)].
Uveitis
Advise patients to contact their healthcare provider if they experience any changes in their vision [see Warnings and Precautions (5.6)].
QT Prolongation
Advise patients that BRAFTOVI can cause QTc interval prolongation and to inform their physician if they have any QTc interval prolongation symptoms, such as syncope [see Warnings and Precautions (5.7)].
Embryo-Fetal Toxicity
- •
- Advise females with reproductive potential of the potential risk to a fetus. Advise females to contact their healthcare provider if they become pregnant, or if pregnancy is suspected, during treatment with BRAFTOVI [see Warnings and Precautions (5.8), Use in Specific Populations (8.1)].
- •
- Advise females of reproductive potential to use effective non-hormonal contraception during treatment with BRAFTOVI and for 2 weeks after the last dose [Use in Specific Populations (8.3)].
Lactation
Advise women not to breastfeed during treatment with BRAFTOVI and for 2 weeks after the last dose [see Use in Specific Populations (8.2)].
Infertility
Advise males of reproductive potential that BRAFTOVI may impair fertility [see Use in Specific Populations (8.3)].
Drug Interactions
Coadministration of BRAFTOVI with a strong or moderate CYP3A inhibitor may increase encorafenib concentrations; coadministration of BRAFTOVI with a strong CYP3A inducer may decrease encorafenib concentrations. Advise patients that they may need to avoid certain medications while taking BRAFTOVI and to inform their healthcare provider of all concomitant medications, including prescription medicines, over-the-counter drugs, vitamins, and herbal products. Advise patients to avoid grapefruit and grapefruit juice while taking BRAFTOVI [see Drug Interactions (7.1)].
-
SPL UNCLASSIFIED SECTION
This product's labeling may have been updated. For the most recent prescribing information, please visit www.pfizer.com.
Distributed by:
Array BioPharma Inc., a wholly owned subsidiary of Pfizer Inc.
3200 Walnut Street
Boulder, CO 80301© 2023 Array BioPharma Inc. All rights reserved.
BRAFTOVI® is a registered trademark of Array BioPharma Inc. in the United States and various other countries.
LAB-1428-4.0
-
MEDICATION GUIDE
This Medication Guide has been approved by the U.S. Food and Drug Administration. Revised: 10/2023 MEDICATION GUIDE
BRAFTOVI® (braf-TOE-vee)
(encorafenib)
capsulesImportant information: BRAFTOVI is used with other medicines, either binimetinib or cetuximab. Read the Medication Guide that comes with binimetinib if used with binimetinib and talk to your healthcare provider about cetuximab if used with cetuximab.
What is the most important information I should know about BRAFTOVI?
BRAFTOVI may cause serious side effects, including:- •
-
Risk of new skin cancers. BRAFTOVI when used alone, or with binimetinib or cetuximab, may cause skin cancers called cutaneous squamous cell carcinoma or basal cell carcinoma.
Talk to your healthcare provider about your risk for these cancers.
Check your skin and tell your healthcare provider right away about any skin changes, including a:
- o
- new wart
- o
- skin sore or reddish bump that bleeds or does not heal
- o
- change in size or color of a mole
- Your healthcare provider should check your skin before treatment with BRAFTOVI, every 2 months during treatment, and for up to 6 months after you stop treatment with BRAFTOVI to look for any new skin cancers.
- Your healthcare provider should also check for cancers that may not occur on the skin. Tell your healthcare provider about any new symptoms that develop during treatment with BRAFTOVI.
- See "What are the possible side effects of BRAFTOVI?" for more information about side effects.
What is BRAFTOVI?
BRAFTOVI is a prescription medicine used:- •
- in combination with a medicine called binimetinib to treat people with a type of skin cancer called melanoma:
- o
- that has spread to other parts of the body or cannot be removed by surgery, and
- o
- that has a certain type of abnormal "BRAF" gene
- •
- in combination with a medicine called cetuximab, for the treatment of adults with cancer of your colon or rectum (colorectal cancer):
- o
- that has been previously treated, and
- o
- that has spread to other parts of the body, and
- o
- that has a certain type of abnormal "BRAF" gene
- •
- in combination with a medicine called binimetinib to treat adults with a type of lung cancer called non-small cell lung cancer (NSCLC):
- o
- that has spread to other parts of the body, and
- o
- that has a certain type of abnormal “BRAF” gene
BRAFTOVI should not be used to treat people with wild-type BRAF melanoma, wild-type BRAF colorectal cancer, or wild-type BRAF NSCLC. Your healthcare provider will perform a test to make sure that BRAFTOVI is right for you.
It is not known if BRAFTOVI is safe and effective in children.Before taking BRAFTOVI, tell your healthcare provider about all of your medical conditions, including if you:
- •
- have had bleeding problems
- •
- have eye problems
- •
- have heart problems, including a condition called long QT syndrome
- •
- have been told that you have low blood levels of potassium, calcium, or magnesium
- •
- have liver or kidney problems
- •
- are pregnant or plan to become pregnant. BRAFTOVI can harm your unborn baby.
- o
- Females who are able to become pregnant should use effective non-hormonal birth control (contraception) during treatment with BRAFTOVI and for 2 weeks after the last dose of BRAFTOVI. Birth control methods that contain hormones (such as birth control pills, injections or transdermal systems) may not work as well during treatment with BRAFTOVI.
- o
- Talk to your healthcare provider about birth control methods that may be right for you during this time.
- o
- Your healthcare provider will do a pregnancy test before you start taking BRAFTOVI. Tell your healthcare provider right away if you become pregnant or think you might be pregnant during treatment with BRAFTOVI.
- •
- are breastfeeding or plan to breastfeed. It is not known if BRAFTOVI passes into your breast milk. Do not breastfeed during treatment with BRAFTOVI and for 2 weeks after the last dose of BRAFTOVI. Talk to your healthcare provider about the best way to feed your baby during this time.
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements.
BRAFTOVI and certain other medicines can affect each other, causing side effects or affecting how BRAFTOVI or the other medicines work.
Know the medicines you take. Keep a list of them to show your healthcare provider and pharmacist when you get a new medicine.How should I take BRAFTOVI?
- •
- Take BRAFTOVI exactly as your healthcare provider tells you. Do not change your dose or stop taking BRAFTOVI unless your healthcare provider tells you to.
- •
- For melanoma and NSCLC, BRAFTOVI is given in combination with binimetinib. Take BRAFTOVI by mouth one time each day.
- •
- For colorectal cancer, take BRAFTOVI by mouth one time each day. You will also receive cetuximab through a vein in your arm (intravenously) given by your healthcare provider.
- •
- BRAFTOVI may be taken with or without food.
- •
- Avoid grapefruit during treatment with BRAFTOVI. Grapefruit products may increase the amount of BRAFTOVI in your body.
- •
- If you miss a dose of BRAFTOVI, take it as soon as you remember. If it is within 12 hours of your next scheduled dose, take your next dose at your regular time. Do not make up for the missed dose.
- •
- Do not take an extra dose if you vomit after taking your scheduled dose. Take your next dose at your regular time.
- •
- If you stop treatment with binimetinib or cetuximab, talk to your healthcare provider about your BRAFTOVI treatment. Your BRAFTOVI dose may need to be changed or stopped.
What are the possible side effects of BRAFTOVI?
BRAFTOVI may cause serious side effects, including:
See "What is the most important information I should know about BRAFTOVI?"- •
-
Heart problems, including heart failure. BRAFTOVI, when taken with binimetinib, can cause heart problems. Your healthcare provider will check your heart function before and during treatment with BRAFTOVI. Tell your healthcare provider right away if you get any of the following signs and symptoms of a heart problem:
- o
- feeling like your heart is pounding or racing
- o
- shortness of breath
- o
- swelling in your hands, ankles legs or feet
- o
- feeling faint or lightheaded
- •
- Liver problems. BRAFTOVI, when taken with binimetinib, can cause liver problems. Your healthcare provider will perform blood tests to check your liver function before and during treatment with BRAFTOVI. Tell your healthcare provider if you get any of the following signs and symptoms of a liver problem:
- o
- yellowing of your skin or your eyes
- o
- dark or brown (tea-colored) urine
- o
- nausea or vomiting
- o
- loss of appetite
- o
- tiredness
- o
- bruising
- o
- bleeding
- •
-
Bleeding problems. BRAFTOVI, when taken with binimetinib or cetuximab, can cause serious bleeding problems, including in your stomach or brain, that can lead to death. Tell your healthcare provider and get medical help right away if you develop any signs of bleeding, including:
- o
- headaches, dizziness, or feeling weak
- o
- cough up blood or blood clots
- o
- vomit blood or your vomit looks like “coffee grounds”
- o
- red or black stools that look like tar
- •
-
Eye problems. BRAFTOVI, when taken with binimetinib, can cause eye problems. Your healthcare provider should perform an eye exam regularly. Tell your healthcare provider right away if you develop any new or worsening symptoms of eye problems, including:
- o
- blurred vision, loss of vision, or other vision changes
- o
- see colored dots
- o
- see halos (blurred outline around objects)
- o
- eye pain, swelling, or redness
- •
- Changes in the electrical activity of your heart called QT prolongation. QT prolongation can cause irregular heartbeats that can be life threatening. Your healthcare provider should do tests before you start taking BRAFTOVI with binimetinib or cetuximab and during your treatment to check your body salts (electrolytes). Tell your healthcare provider right away if you feel faint, lightheaded, dizzy or if you feel your heart beating irregularly or fast during treatment with BRAFTOVI and binimetinib or cetuximab. These symptoms may be related to QT prolongation.
Your healthcare provider may change your dose, temporarily stop, or permanently stop treatment with BRAFTOVI if you have certain side effects.
The most common side effects of BRAFTOVI when taken in combination with binimetinib for melanoma include:
- •
- fatigue
- •
- nausea
- •
- vomiting
- •
- abdominal pain
- •
- pain or swelling of your joints (arthralgia)
The most common side effects of BRAFTOVI when taken in combination with cetuximab for colorectal cancer include:
- •
- fatigue
- •
- nausea
- •
- diarrhea
- •
- acne-like rash (dermatitis acneiform)
- •
- stomach-area (abdominal) pain
- •
- decreased appetite
- •
- pain or swelling of your joints (arthralgia)
- •
- rash
The most common side effects of BRAFTOVI when taken in combination with binimetinib for NSCLC include:
- •
- fatigue
- •
- nausea
- •
- diarrhea
- •
- muscle or joint pain
- •
- vomiting
- •
- stomach-area (abdominal) pain
- •
- blurred vision, loss of vision, or other vision changes
- •
- constipation
- •
- shortness of breath
- •
- rash
- •
- cough
BRAFTOVI may cause fertility problems in males. Talk to your healthcare provider if this is a concern for you.
These are not all of the possible side effects of BRAFTOVI.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
You may also report side effects to Pfizer Inc. at 1-800-438-1985.
How should I store BRAFTOVI?
- •
- Store BRAFTOVI at room temperature between 68°F to 77°F (20°C to 25°C).
- •
- Store BRAFTOVI in the original bottle.
- •
- Keep the BRAFTOVI bottle tightly closed and protect it from moisture.
- •
- BRAFTOVI comes with a desiccant packet in the bottle to help protect your medicine from moisture. Do not remove the desiccant packet from the bottle.
Keep BRAFTOVI and all medicines out of the reach of children.
General information about the safe and effective use of BRAFTOVI.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use BRAFTOVI for a condition for which it was not prescribed. Do not give BRAFTOVI to other people, even if they have the same symptoms that you have. It may harm them. You can ask your healthcare provider or pharmacist for information about BRAFTOVI that is written for health professionals.What are the ingredients in BRAFTOVI?
Active ingredient: encorafenib
Inactive ingredients: copovidone, poloxamer 188, microcrystalline cellulose, succinic acid, crospovidone, colloidal silicon dioxide, and magnesium stearate of vegetable origin
Capsule shell: gelatin, titanium dioxide, iron oxide red, iron oxide yellow, ferrosoferric oxide, monogramming ink (pharmaceutical glaze, ferrosoferric oxide, propylene glycol)
Distributed by: Array BioPharma Inc., a wholly owned subsidiary of Pfizer Inc. Boulder, Colorado 80301.
BRAFTOVI® is a registered trademark of Array BioPharma Inc. in the United States and various other countries.
LAB-1429-3.0
For more information, go to www.BRAFTOVIMEKTOVI.com or call 1-844-792-7729.
© 2022 Array BioPharma Inc. All rights reserved. - PRINCIPAL DISPLAY PANEL - 75 mg Capsule Bottle Label - 025-02
- PRINCIPAL DISPLAY PANEL - 75 mg Capsule Bottle Carton
- PRINCIPAL DISPLAY PANEL - 75 mg Capsule Bottle Label - 025-06
- PRINCIPAL DISPLAY PANEL - 75 mg Capsule Bottle Label - 025-05
-
INGREDIENTS AND APPEARANCE
BRAFTOVI
encorafenib capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:70255-025 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength ENCORAFENIB (UNII: 8L7891MRB6) (ENCORAFENIB - UNII:8L7891MRB6) ENCORAFENIB 75 mg Inactive Ingredients Ingredient Name Strength COPOVIDONE K25-31 (UNII: D9C330MD8B) POLOXAMER 188 (UNII: LQA7B6G8JG) MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) SUCCINIC ACID (UNII: AB6MNQ6J6L) CROSPOVIDONE, UNSPECIFIED (UNII: 2S7830E561) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) MAGNESIUM STEARATE (UNII: 70097M6I30) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FERRIC OXIDE RED (UNII: 1K09F3G675) FERRIC OXIDE YELLOW (UNII: EX438O2MRT) FERROSOFERRIC OXIDE (UNII: XM0M87F357) SHELLAC (UNII: 46N107B71O) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) Product Characteristics Color PINK (beige) , WHITE Score no score Shape CAPSULE Size 23mm Flavor Imprint Code A;LGX;75mg Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:70255-025-01 2 in 1 CARTON 06/27/2018 1 NDC:70255-025-02 90 in 1 BOTTLE; Type 0: Not a Combination Product 2 NDC:70255-025-03 2 in 1 CARTON 06/27/2018 2 NDC:70255-025-04 60 in 1 BOTTLE; Type 0: Not a Combination Product 3 NDC:70255-025-06 60 in 1 BOTTLE; Type 0: Not a Combination Product 08/03/2020 4 NDC:70255-025-05 90 in 1 BOTTLE; Type 0: Not a Combination Product 08/03/2020 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA210496 06/27/2018 Labeler - Array BioPharma Inc. (004047838) Registrant - Pfizer Inc (113480771)