Label: TIOPRONIN tablet, delayed release

- NDC Code(s): 60219-2009-9
- Packager: Amneal Pharmaceuticals NY LLC
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: Abbreviated New Drug Application
Drug Label Information
Updated May 18, 2023
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use TIOPRONIN DELAYED-RELEASE TABLETS safely and effectively. See full prescribing information for TIOPRONIN DELAYED-RELEASE TABLETS.
TIOPRONIN delayed-release tablets, for oral use
Initial U.S. Approval: 1988INDICATIONS AND USAGE
Tiopronin delayed-release tablets are a reducing and complexing thiol indicated, in combination with high fluid intake, alkali, and diet modification, for the prevention of cystine stone formation in adults and pediatric patients 9 years of age and older with severe homozygous cystinuria, who are not responsive to these measures alone. (1)
DOSAGE AND ADMINISTRATION
- The recommended initial dosage in adult patients is 800 mg/day. In clinical studies, the average dosage was about 1,000 mg/day. (2.1)
- The recommended initial dosage in pediatric patients 9 years of age and older is 15 mg/kg/day. Avoid dosages greater than 50 mg/kg per day in pediatric patients. (5.1, 8.4)
- Measure urinary cystine 1 month after initiation of tiopronin delayed-release tablets and every 3 months thereafter. (2.3)
- Administer tiopronin delayed-release tablets in 3 divided doses at the same times each day, with or without food. Maintain a routine pattern with regard to meals. (2.1)
- Tiopronin delayed-release tablets can be crushed and mixed with applesauce. For preparation and administration instructions, see the full prescribing information. (2.2)
DOSAGE FORMS AND STRENGTHS
Tablets: 300 mg. (3)
CONTRAINDICATIONS
- Hypersensitivity to tiopronin or any component of tiopronin delayed-release tablets. (4)
WARNINGS AND PRECAUTIONS
- Proteinuria, including nephrotic syndrome, and membranous nephropathy, has been reported with tiopronin use. Pediatric patients receiving greater than 50 mg/kg of tiopronin per day may be at increased risk for proteinuria. (2.1, 5.1, 8.4)
- Hypersensitivity reactions have been reported during tiopronin treatment. (4, 5.2)
ADVERSE REACTIONS
Most common adverse reactions (≥ 10%) are nausea, diarrhea or soft stools, oral ulcers, rash, fatigue, fever, arthralgia, proteinuria, and emesis. (6)
To report SUSPECTED ADVERSE REACTIONS, contact Amneal Pharmaceuticals at 1-877-835-5472 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
USE IN SPECIFIC POPULATIONS
- Lactation: Breastfeeding is not recommended. (8.2)
- Geriatric: Choose dose carefully and monitor renal function in the elderly. (8.5)
Additional pediatric use information is approved for Mission Pharmacal Company’s THIOLA EC (tiopronin) delayed-release tablets. However, due to Mission Pharmacal Company’s marketing exclusivity rights, this drug product is not labeled with that information.
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 5/2023
- The recommended initial dosage in adult patients is 800 mg/day. In clinical studies, the average dosage was about 1,000 mg/day. (2.1)
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage
2.2 Preparation and Administration Instructions
2.3 Monitoring
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Proteinuria
5.2 Hypersensitivity Reactions
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Post-marketing Experience
7 DRUG INTERACTIONS
7.1 Alcohol
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
Tiopronin delayed-release tablets are indicated, in combination with high fluid intake, alkali, and diet modification, for the prevention of cystine stone formation in adults and pediatric patients 9 years of age and older with severe homozygous cystinuria, who are not responsive to these measures alone.
Additional pediatric use information is approved for Mission Pharmacal Company’s THIOLA EC (tiopronin) delayed-release tablets. However, due to Mission Pharmacal Company’s marketing exclusivity rights, this drug product is not labeled with that information.
-
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage
Adults: The recommended initial dosage in adult patients is 800 mg/day. In clinical studies, the average dosage was about 1,000 mg/day.
Pediatrics: The recommended initial dosage in pediatric patients 9 years of age and older is 15 mg/kg/day. Avoid dosages greater than 50 mg/kg per day in pediatric patients [see Warnings and Precautions (5.1), Use in Specific Populations (8.4)].
Additional pediatric use information is approved for Mission Pharmacal Company’s THIOLA EC (tiopronin) delayed-release tablets. However, due to Mission Pharmacal Company’s marketing exclusivity rights, this drug product is not labeled with that information.
Administer tiopronin delayed-release tablets in 3 divided doses at the same times each day, with or without food. Maintain a routine pattern with regard to meals.
Consider starting tiopronin delayed-release tablets at a lower dosage in patients with history of severe toxicity to d-penicillamine.
2.2 Preparation and Administration Instructions
For patients who cannot swallow the tablet whole, tiopronin delayed-release tablets can be crushed and mixed with applesauce. Administration of tiopronin delayed-release tablets with other liquids or foods has not been studied and is not recommended.
Preparation and Administration of Tiopronin Delayed-Release Tablets Mixed in Applesauce
For patients who can swallow semi-solid food, tiopronin delayed-release tablets can be crushed and mixed with applesauce:
- Crush the tiopronin delayed-release tablet in a clean pill crusher or mortar and pestle. Always crush one tablet at a time.
- Measure approximately one tablespoon of applesauce and transfer it into a container with the crushed tiopronin delayed-release tablet.
- Mix the crushed tiopronin delayed-release tablet in the applesauce until the powder is well dispersed.
- Administer the entire tiopronin delayed-release tablet-applesauce mixture to the patient’s mouth immediately. However, if this is not possible, the mixture can be stored in a refrigerator for up to 2 hours after adding the crushed tablet to the applesauce. Discard any mixture that has not been given within 2 hours.
- To assure that any leftover applesauce mixture from the container is recovered, add tap water to the same container, mix, and have the patient drink the water.
2.3 Monitoring
Measure urinary cystine 1 month after starting tiopronin delayed-release tablets and every 3 months thereafter. Adjust tiopronin delayed-release tablets dosage to maintain urinary cystine concentration less than 250 mg/L.
Assess for proteinuria before treatment and every 3 to 6 months during treatment [see Warnings and Precautions (5.1)].
Discontinue tiopronin delayed-release tablets in patients who develop proteinuria, and monitor urinary protein and renal function. Consider restarting tiopronin delayed-release tablets treatment at a lower dosage after resolution of proteinuria.
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
Tiopronin delayed-release tablets are contraindicated in patients with hypersensitivity to tiopronin or any other components of tiopronin delayed-release tablets [see Warnings and Precautions (5.2)].
-
5 WARNINGS AND PRECAUTIONS
5.1 Proteinuria
Proteinuria, including nephrotic syndrome, and membranous nephropathy, have been reported with tiopronin use. Pediatric patients receiving greater than 50 mg/kg of tiopronin per day may be at increased risk for proteinuria [see Dosage and Administration (2.3), Adverse Reactions (6.1, 6.2), Use in Specific Populations (8.4)]. Monitor patients for the development of proteinuria and discontinue therapy in patients who develop proteinuria [see Dosage and Administration (2.3)].
5.2 Hypersensitivity Reactions
Hypersensitivity reactions (drug fever, rash, fever, arthralgia and lymphadenopathy) have been reported [see Contraindications (4)].
-
6 ADVERSE REACTIONS
The following adverse reactions are discussed in greater detail in other sections of the labeling:
- Proteinuria [see Warnings and Precautions (5.1)]
- Hypersensitivity [see Warnings and Precautions (5.2)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, the adverse reaction rates observed in the clinical trials of the drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Adverse reactions occurring at an incidence of ≥ 5% in an uncontrolled trial in 66 patients with cystinuria age 9 to 68 years are shown in the table below. Patients in group 1 had previously been treated with d-penicillamine; those in group 2 had not. Of those patients who had stopped taking d-penicillamine due to toxicity (34 out of 49 patients in group 1), 22 were able to continue treatment with tiopronin. In those without prior history of d-penicillamine treatment, 6% developed reactions of sufficient severity to require tiopronin withdrawal.
Table 1 presents adverse reactions ≥ 5% in either treatment group occurring in this trial.
Table 1: Adverse Reactions Occurring in One or More Patients
System Organ Class
Adverse Reaction
Group 1
Previously treated with d-penicillamine
(N = 49)Group 2
Naïve to d-penicillamine
(N = 17)Blood and Lymphatic System Disorders
anemia
1 (2%)
1 (6%)
Gastrointestinal Disorders
nausea
12 (25%)
2 (12%)
emesis
5 (10%)
–
diarrhea/soft stools
9 (18%)
1 (6%)
abdominal pain
–
1 (6%)
oral ulcers
6 (12%)
3 (18%)
General Disorders and Administration Site Conditions
fever
4 (8%)
–
weakness
2 (4%)
2 (12%)
fatigue
7 (14%)
–
peripheral (edema)
3 (6%)
1 (6%)
chest pain
–
1 (6%)
Metabolism and Nutrition Disorders
anorexia
4 (8%)
–
Musculoskeletal and Connective Tissue Disorders
arthralgia
–
2 (12%)
Renal and Urinary Disorders
proteinuria
5 (10%)
1 (6%)
impotence
–
1 (6%)
Respiratory, Thoracic and Mediastinal Disorders
cough
–
1 (6%)
Skin and Subcutaneous Tissue Disorders
rash
7 (14%)
2 (12%)
ecchymosis
3 (6%)
–
pruritus
2 (4%)
1 (6%)
urticaria
4 (8%)
–
skin wrinkling
3 (6%)
1 (6%)
Taste Disturbance
A reduction in taste perception may develop. It is believed to be the result of chelation of trace metals by tiopronin. Hypogeusia is often self-limited.
6.2 Post-marketing Experience
Adverse reactions have been reported from the literature, as well as during post-approval use of tiopronin. Because the post-approval reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to tiopronin exposure.
Adverse reactions reported during the post-marketing use of tiopronin are listed by body system in Table 2.
Table 2: Adverse Reactions Reported for Tiopronin Pharmacovigilance by System Organ Class and Preferred Term
System Organ Class
Preferred Term
Cardiac Disorders
congestive heart failure
Ear and Labyrinth Disorder
vertigo
Gastrointestinal Disorders
abdominal discomfort; abdominal distension; abdominal pain; chapped lips; diarrhea; dry mouth; dyspepsia; eructation; flatulence; gastrointestinal disorder; gastroesophageal reflux disease; nausea; vomiting; jaundice; liver transaminitis
General Disorders and Administration Site Conditions
asthenia; chest pain; fatigue; malaise; pain; peripheral swelling; pyrexia; swelling
Investigations
glomerular filtration rate decreased; weight increased
Metabolism and Nutrition Disorders
decreased appetite; dehydration; hypophagia
Musculoskeletal and Connective Tissue Disorders
arthralgia; back pain; flank pain; joint swelling; limb discomfort; musculoskeletal discomfort; myalgia; neck pain; pain in extremity
Nervous System Disorders
ageusia; burning sensation; dizziness; dysgeusia; headache; hypoesthesia
Renal and Urinary Disorders
nephrotic syndrome; proteinuria; renal failure
Skin and Subcutaneous Tissue Disorders
dry skin; hyperhidrosis; pemphigus foliaceus; pruritus; rash; rash pruritic; skin irritation; skin texture abnormal; skin wrinkling; urticaria
-
7 DRUG INTERACTIONS
7.1 Alcohol
Tiopronin is released faster from tiopronin delayed-release tablets in the presence of alcohol and the risk for adverse events associated with tiopronin delayed-release tablets when taken with alcohol is unknown. Avoid alcohol consumption 2 hours before and 3 hours after taking tiopronin delayed-release tablets [see Clinical Pharmacology (12.3)].
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Available published case report data with tiopronin have not identified a drug-associated risk for major birth defects, miscarriage, or adverse maternal or fetal outcomes. Renal stones in pregnancy may result in adverse pregnancy outcomes (see Clinical Considerations). In animal reproduction studies, there were no adverse developmental outcomes with oral administration of tiopronin to pregnant mice and rats during organogenesis at doses up to 2 times a 2 grams/day human dose (based on mg/m2). The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies are 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Disease-associated maternal and/or embryo/fetal risk
Renal stones in pregnancy may increase the risk of adverse pregnancy outcomes, such as preterm birth and low birth weight.
Data
Animal Data
No findings of fetal malformations could be attributed to the drug in reproduction studies in mice and rats at doses up to 2 times the highest recommended human dose of 2 grams/day (based on mg/m2).
8.2 Lactation
Risk Summary
There are no data on the presence of tiopronin in either human or animal milk or on the effects of the breastfed child. A published study suggests that tiopronin may suppress milk production. Because of the potential for serious adverse reactions, including nephrotic syndrome, advise patients that breastfeeding is not recommended during treatment with tiopronin delayed-release tablets.
8.4 Pediatric Use
Tiopronin delayed-release tablets are indicated in pediatric patients 9 years of age and older with severe homozygous cystinuria, in combination with high fluid intake, alkali, and diet modification, for the prevention of cystine stone formation who are not responsive to these measures alone. This indication is based on safety and efficacy data from a trial in patients 9 years to 68 years of age and clinical experience. Proteinuria, including nephrotic syndrome, has been reported in pediatric patients. Pediatric patients receiving greater than 50 mg/kg tiopronin per day may be at greater risk [see Dosage and Administration (2.1, 2.3), Warnings and Precautions (5.1) and Adverse Reactions (6.1)].
Tiopronin delayed-release tablets are not approved for use in pediatric patients weighing less than 20 kg [see Dosage and Administration (2.1)].
Additional pediatric use information is approved for Mission Pharmacal Company’s THIOLA EC (tiopronin) delayed-release tablets. However, due to Mission Pharmacal Company’s marketing exclusivity rights, this drug product is not labeled with that information.
8.5 Geriatric Use
This drug is known to be substantially excreted by the kidney, and the risk of adverse reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
- 10 OVERDOSAGE
-
11 DESCRIPTION
Tiopronin delayed-release tablets are a reducing and cystine-binding thiol drug (CBTD) for oral use. Tiopronin is N-(2-Mercaptopropionyl) glycine and has the following structure:
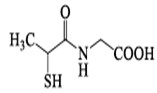
Tiopronin has the molecular formula C5H9NO3S and a molecular weight of 163.19 g/mol. In this drug product tiopronin exists as a dl racemic mixture.
Tiopronin is a white to off-white color crystalline powder, which is freely soluble in water.
Each tiopronin delayed-release tablet contains 300 mg of tiopronin. The inactive ingredients in tiopronin delayed-release tablets include lactose monohydrate, hydroxypropyl cellulose, hydroxypropyl cellulose (low substitute), magnesium stearate, hydroxypropyl methylcellulose E5, methacrylic acid and ethyl acrylate copolymer (Eudragit L 100-55), talc, triethyl citrate.
Each tablet is imprinted with red pharmaceutical ink which contains: alcohol, butyl alcohol, FD & C Red # 40, propylene glycol, shellac and titanium dioxide.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
The goal of therapy is to reduce urinary cystine concentration below its solubility limit. Tiopronin is an active reducing agent which undergoes thiol-disulfide exchange with cystine to form a mixed disulfide of tiopronin-cysteine. From this reaction, a water-soluble mixed disulfide is formed and the amount of sparingly soluble cystine is reduced.
12.2 Pharmacodynamics
The decrement in urinary cystine produced by tiopronin is generally proportional to the dose. A reduction in urinary cystine of 250 mg/day to 350 mg/day at tiopronin dosage of 1 g/day, and a decline of approximately 500 mg/day at a dosage of 2 g/day, might be expected. Tiopronin has a rapid onset and offset of action, showing a fall in cystine excretion on the first day of administration and a rise on the first day of drug withdrawal.
12.3 Pharmacokinetics
Absorption
Tiopronin Delayed-Release Tablets
When tiopronin immediate-release tablets and tiopronin delayed-release tablets single doses were given to fasted healthy subjects, the median time to peak plasma levels (Tmax) was 1 (range: 0.5 to 2.1) and 3 (range: 1.0 to 6.0) hours, respectively. The peak exposure (Cmax) and total exposure (AUC0-t) of tiopronin from tiopronin delayed-release tablets were decreased by 22% and 7% respectively compared to tiopronin immediate-release tablets.
When tiopronin delayed-release tablets were administered crushed in applesauce, the median time to peak plasma levels of tiopronin (Tmax) was 1 hour (range: 0.5 to 2.0) compared to 3.1 hours (range: 1.5 to 4.0) when administered as intact EC tablets.
When tiopronin delayed-release tablets were administered crushed in applesauce, the maximum concentration (Cmax) and exposure (AUC0-t) to tiopronin were increased by 38% and 14%, respectively, compared to tiopronin delayed-release tablets administered intact.
Food Effects
Administration of the tiopronin delayed-release tablet with food decreases Cmax of tiopronin by 13% and AUC0-t by 25% compared to tiopronin delayed-release tablets administered in a fasted state.
Since the drug is dosed to effect, the study results support administration of tiopronin delayed-release tablets with or without food; administer at the same time each day with a routine pattern with regard to meals.
Elimination
Excretion
When tiopronin is given orally, up to 48% of dose appears in urine during the first 4 hours and up to 78% by 72 hours.
Drug Interactions
Alcohol
An in vitro dissolution study was conducted to evaluate the impact of alcohol (5%, 10%, 20%, and 40%) on the dose dumping of tiopronin delayed-release tablets. The study results showed that the addition of alcohol to the dissolution media increases the dissolution rate of tiopronin delayed-release tablets in the acidic media of 0.1 N HCl [see Drug Interactions (7.1)].
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Long-term carcinogenicity studies in animals have not been performed.
Mutagenesis
Tiopronin was not genotoxic in the chromosomal aberration, sister chromatid exchange, and in vivo micronucleus assays.
Impairment of Fertility
High doses of tiopronin in experimental animals have been shown to interfere with maintenance of pregnancy and viability of the fetus. In 2 published male fertility studies in rats, tiopronin at 20 mg/kg/day intramuscular (IM) for 60 days induced reductions in testis, epididymis, vas deferens, and accessory sex glands weights and in the count and motility of cauda epididymal sperm.
-
16
HOW
SUPPLIED/STORAGE AND HANDLING
Tiopronin Delayed-Release Tablets, 300 mg are supplied as round, white to off-white tablet imprinted with “L6” on one side with red ink and blank on the other side.
They are available as follows:
Bottles of 90 with child-resistant closure: NDC 60219-2009-9
Store at 20° to 25°C (68° to 77°F); excursions permitted between 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature].
Keep this and all medications out of the reach of children.
-
17 PATIENT COUNSELING INFORMATION
Administration Instructions
For patients who cannot swallow the tablet whole, the tiopronin delayed-release tablets can be crushed and mixed with applesauce [see Dosage and Administration (2.2)] for preparation and administration instructions.
Lactation
Advise women that breastfeeding is not recommended during treatment with tiopronin delayed-release tablets [see Use in Specific Populations (8.2)].
Manufactured by:
Amneal Pharmaceuticals Pvt. Ltd.
Oral Solid Dosage Unit
Ahmedabad 382213, INDIADistributed by:
Amneal Pharmaceuticals LLC
Bridgewater, NJ 08807Rev. 05-2023-01
- PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
TIOPRONIN
tiopronin tablet, delayed releaseProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:60219-2009 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength TIOPRONIN (UNII: C5W04GO61S) (TIOPRONIN - UNII:C5W04GO61S) TIOPRONIN 300 mg Inactive Ingredients Ingredient Name Strength ALCOHOL (UNII: 3K9958V90M) BUTYL ALCOHOL (UNII: 8PJ61P6TS3) FD&C RED NO. 40 (UNII: WZB9127XOA) HYDROXYPROPYL CELLULOSE, UNSPECIFIED (UNII: 9XZ8H6N6OH) HYDROXYPROPYL CELLULOSE, LOW SUBSTITUTED (UNII: 2165RE0K14) HYPROMELLOSE 2910 (5 MPA.S) (UNII: R75537T0T4) MAGNESIUM STEARATE (UNII: 70097M6I30) LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) METHACRYLIC ACID AND ETHYL ACRYLATE COPOLYMER (UNII: NX76LV5T8J) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) SHELLAC (UNII: 46N107B71O) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) TRIETHYL CITRATE (UNII: 8Z96QXD6UM) Product Characteristics Color white (white to off-white) Score no score Shape ROUND Size 11mm Flavor Imprint Code L6 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:60219-2009-9 90 in 1 BOTTLE; Type 0: Not a Combination Product 08/16/2023 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA216278 08/16/2023 Labeler - Amneal Pharmaceuticals NY LLC (123797875) Registrant - Amneal Pharmaceuticals of New York, LLC (123797875) Establishment Name Address ID/FEI Business Operations Amneal Pharmaceuticals Private Limited 650762060 analysis(60219-2009) , label(60219-2009) , manufacture(60219-2009) , pack(60219-2009)