Label: MOMETASONE FUROATE cream

-
Contains inactivated NDC Code(s)
NDC Code(s): 50090-2179-0 - Packager: A-S Medication Solutions
- This is a repackaged label.
- Source NDC Code(s): 68462-192
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: Abbreviated New Drug Application
Drug Label Information
Updated January 9, 2018
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use mometasone furoate cream safely and effectively. See full prescribing information for mometasone furoate cream.
MOMETASONE FUROATE Cream USP, 0.1% for topical use
Initial U.S. Approval: 1987INDICATIONS AND USAGE
Mometasone furoate cream USP, 0.1% is a corticosteroid indicated for the relief of the inflammatory and pruritic manifestations of corticosteroid-responsive dermatoses in patients ≥2 years of age. (1)
DOSAGE AND ADMINISTRATION
- •
- Apply a thin film to the affected skin areas once daily. (2)
- •
- Discontinue therapy when control is achieved. (2)
- •
- If no improvement is seen within 2 weeks, reassess diagnosis. (2)
- •
- The safety and efficacy of mometasone furoate cream USP, 0.1% in pediatric patients for more than 3 weeks of use have not been established. (2)
- •
- Do not use with occlusive dressings unless directed by a physician. (2)
DOSAGE FORMS AND STRENGTHS
- •
- Cream, 0.1%. (3)
CONTRAINDICATIONS
- •
- None. (4)
WARNINGS AND PRECAUTIONS
- •
- Reversible HPA axis suppression with the potential for glucocorticosteroid insufficiency after withdrawal of treatment, Cushing’s syndrome, and hyperglycemia, may occur due to systemic absorption. Patients applying a topical steroid to a large surface area or to areas under occlusion should be evaluated periodically for evidence of HPA axis suppression. Modify use should HPA axis suppression develop. Pediatric patients may be more susceptible to systemic toxicity. (5.1, 8.4)
ADVERSE REACTIONS
Most common adverse reactions are: burning, pruritus, and skin atrophy. (6)
To report SUSPECTED ADVERSE REACTIONS, contact Glenmark Pharmaceuticals Inc., USA at 1 (888)721-7115] or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 1/2018
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Effects on Endocrine System
5.2 Allergic Contact Dermatitis
5.3 Concomitant Skin Infections
6 ADVERSE REACTIONS
7 DRUG INTERACTIONS
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.3 Nursing Mothers
8.4 Pediatric Use
8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
- 1 INDICATIONS AND USAGE
-
2 DOSAGE AND ADMINISTRATION
Apply a thin film of mometasone furoate cream USP, 0.1% to the affected skin areas once daily. Mometasone furoate cream USP, 0.1% may be used in pediatric patients 2 years of age or older. Since safety and efficacy of mometasone furoate cream USP, 0.1% have not been established in pediatric patients below 2 years of age; use in this age group is not recommended [see Warnings and Precautions (5.1) and Use in Specific Populations (8.4)].
Therapy should be discontinued when control is achieved. If no improvement is seen within 2 weeks, reassessment of diagnosis may be necessary. Safety and efficacy of mometasone furoate cream USP, 0.1% in pediatric patients for more than 3 weeks of use have not been established.
Mometasone furoate cream USP, 0.1% should not be used with occlusive dressings unless directed by a physician. Mometasone furoate cream USP, 0.1% should not be applied in the diaper area if the child still requires diapers or plastic pants, as these garments may constitute occlusive dressing.
Mometasone furoate cream USP, 0.1% is for topical use only. It is not for oral, ophthalmic, or intravaginal use.
Avoid use on the face, groin, or axillae.
- 3 DOSAGE FORMS AND STRENGTHS
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Effects on Endocrine System
Systemic absorption of topical corticosteroids can produce reversible hypothalamic-pituitary-adrenal (HPA) axis suppression with the potential for glucocorticosteroid insufficiency. This may occur during treatment or after withdrawal of treatment. Manifestations of Cushing’s syndrome, hyperglycemia, and glucosuria can also be produced in some patients by systemic absorption of topical corticosteroids while on treatment. Factors that predispose a patient using a topical corticosteroid to HPA axis suppression include the use of high-potency steroids, large treatment surface areas, prolonged use, use of occlusive dressings, altered skin barrier, liver failure and young age.
Because of the potential for systemic absorption, use of topical corticosteroids may require that patients be periodically evaluated for HPA axis suppression. This may be done by using the adrenocorticotropic hormone (ACTH) stimulation test.
In a study evaluating the effects of mometasone furoate cream on the HPA axis, 15 grams were applied twice daily for 7 days to six adult subjects with psoriasis or atopic dermatitis. The results show that the drug caused a slight lowering of adrenal corticosteroid secretion.
If HPA axis suppression is noted, an attempt should be made to gradually withdraw the drug, to reduce the frequency of application, or to substitute a less potent corticosteroid. Recovery of HPA axis function is generally prompt upon discontinuation of topical corticosteroids. Infrequently, signs and symptoms of glucocorticosteroid insufficiency may occur, requiring supplemental systemic corticosteroids.
Pediatric patients may be more susceptible to systemic toxicity from equivalent doses due to their larger skin surface to body mass ratios [see Use in Specific Populations (8.4)].
5.2 Allergic Contact Dermatitis
If irritation develops, mometasone furoate cream should be discontinued and appropriate therapy instituted. Allergic contact dermatitis with corticosteroids is usually diagnosed by observing a failure to heal rather than noting a clinical exacerbation as with most topical products not containing corticosteroids. Such an observation should be corroborated with appropriate diagnostic patch testing.
5.3 Concomitant Skin Infections
If concomitant skin infections are present or develop, an appropriate antifungal or antibacterial agent should be used. If a favorable response does not occur promptly, use of mometasone furoate cream should be discontinued until the infection has been adequately controlled
-
6 ADVERSE REACTIONS
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
In controlled clinical trials involving 319 subjects, the incidence of adverse reactions associated with the use of mometasone furoate cream was 1.6%. Reported reactions included burning, pruritus, and skin atrophy. Reports of rosacea associated with the use of mometasone furoate cream have also been received. In controlled clinical trials (n=74) involving pediatric subjects 2 to 12 years of age, the incidence of adverse experiences associated with the use of mometasone furoate cream was approximately 7%. Reported reactions included stinging, pruritus, and furunculosis.
The following adverse reactions were reported to be possibly or probably related to treatment with mometasone furoate cream during clinical trials in 4% of 182 pediatric subjects 6 months to 2 years of age: decreased glucocorticoid levels, 2; paresthesia, 2; folliculitis, 1; moniliasis, 1; bacterial infection, 1; skin depigmentation, 1. The following signs of skin atrophy were also observed among 97 subjects treated with mometasone furoate cream in a clinical trial: shininess, 4; telangiectasia, 1; loss of elasticity, 4; loss of normal skin markings, 4; thinness, 1; and bruising, 1.
The following additional local adverse reactions have been reported with topical corticosteroids, but may occur more frequently with the use of occlusive dressings. These reactions are: irritation, dryness, folliculitis, hypertrichosis, acneiform eruptions, hypopigmentation, perioral dermatitis, allergic contact dermatitis, secondary infection, striae, and miliaria.
- 7 DRUG INTERACTIONS
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Teratogenic Effects Pregnancy Category C:
There are no adequate and well-controlled studies in pregnant women. Therefore, mometasone furoate cream should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Corticosteroids have been shown to be teratogenic in laboratory animals when administered systemically at relatively low dosage levels. Some corticosteroids have been shown to be teratogenic after dermal application in laboratory animals.
When administered to pregnant rats, rabbits, and mice, mometasone furoate increased fetal malformations. The doses that produced malformations also decreased fetal growth, as measured by lower fetal weights and/or delayed ossification. Mometasone furoate also caused dystocia and related complications when administered to rats during the end of pregnancy.
In mice, mometasone furoate caused cleft palate at subcutaneous doses of 60 mcg/kg and above. Fetal survival was reduced at 180 mcg/kg. No toxicity was observed at 20 mcg/kg. (Doses of 20, 60, and 180 mcg/kg in the mouse are approximately 0.01, 0.02, and 0.05 times the estimated maximum clinical topical dose from mometasone furoate cream on a mcg/m2 basis.)
In rats, mometasone furoate produced umbilical hernias at topical doses of 600 mcg/kg and above.A dose of 300 mcg/kg produced delays in ossification, but no malformations. (Doses of 300 and 600 mcg/kg in the rat are approximately 0.2 and 0.4 times the estimated maximum clinical topical dose from mometasone furoate cream on a mcg/m2 basis.)
In rabbits, mometasone furoate caused multiple malformations (e.g., flexed front paws, gallbladder agenesis, umbilical hernia, hydrocephaly) at topical doses of 150 mcg/kg and above (approximately 0.2 times the estimated maximum clinical topical dose from mometasone furoate cream on a mcg/m2 basis). In an oral study, mometasone furoate increased resorptions and caused cleft palate and/or head malformations (hydrocephaly and domed head) at 700 mcg/kg. At 2800 mcg/kg most litters were aborted or resorbed. No toxicity was observed at 140 mcg/kg. (Doses of 140, 700, and 2800 mcg/kg in the rabbit are approximately 0.2, 0.9, and 3.6 times the estimated maximum clinical topical dose from mometasone furoate cream on a mcg/m2 basis.)
When rats received subcutaneous doses of mometasone furoate throughout pregnancy or during the later stages of pregnancy, 15 mcg/kg caused prolonged and difficult labor and reduced the number of live births, birth weight, and early pup survival. Similar effects were not observed at 7.5 mcg/kg. (Doses of 7.5 and 15 mcg/kg in the rat are approximately 0.005 and 0.01 times the estimated maximum clinical topical dose from mometasone furoate cream on a mcg/m2 basis.)
8.3 Nursing Mothers
Systemically administered corticosteroids appear in human milk and could suppress growth, interfere with endogenous corticosteroid production, or cause other untoward effects. It is not known whether topical administration of corticosteroids could result in sufficient systemic absorption to produce detectable quantities in human milk. Because many drugs are excreted in human milk, caution should be exercised when mometasone furoate cream is administered to a nursing woman.
8.4 Pediatric Use
Mometasone furoate cream may be used with caution in pediatric patients 2 years of age or older, although the safety and efficacy of drug use for longer than 3 weeks have not been established. Since safety and efficacy of mometasone furoate cream have not been established in pediatric patients below 2 years of age, its use in this age group is not recommended.
In a pediatric trial, 24 atopic dermatitis subjects, of whom 19 subjects were age 2 to 12 years, were treated with mometasone furoate cream once daily. The majority of subjects cleared within 3 weeks. Mometasone furoate cream caused HPA axis suppression in approximately 16% of pediatric subjects ages 6 to 23 months, who showed normal adrenal function by Cortrosyn test before starting treatment, and were treated for approximately 3 weeks over a mean body surface area of 41% (range 15%-94%). The criteria for suppression were: basal cortisol level of ≤5 mcg/dL, 30-minute post-stimulation level of ≤18 mcg/dL, or an increase of <7 mcg/dL. Follow-up testing 2 to 4 weeks after trial completion, available for 5 of the subjects, demonstrated suppressed HPA axis function in 1 subject, using these same criteria. Long-term use of topical corticosteroids has not been studied in this population [see Clinical Pharmacology (12.2)].
Because of a higher ratio of skin surface area to body mass, pediatric patients are at a greater risk than adults of HPA axis suppression and Cushing’s syndrome when they are treated with topical corticosteroids. They are, therefore, also at greater risk of adrenal insufficiency during and/or after withdrawal of treatment. Pediatric patients may be more susceptible than adults to skin atrophy, including striae, when they are treated with topical corticosteroids. Pediatric patients applying topical corticosteroids to greater than 20% of body surface are at higher risk of HPA axis suppression.
HPA axis suppression, Cushing’s syndrome, linear growth retardation, delayed weight gain, and intracranial hypertension have been reported in pediatric patients receiving topical corticosteroids. Manifestations of adrenal suppression in children include low plasma cortisol levels and an absence of response to ACTH stimulation. Manifestations of intracranial hypertension include bulging fontanelles, headaches, and bilateral papilledema.
Mometasone furoate cream should not be used in the treatment of diaper dermatitis.
8.5 Geriatric Use
Clinical studies of mometasone furoate cream included 190 subjects who were 65 years of age and over and 39 subjects who were 75 years of age and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients. However, greater sensitivity of some older individuals cannot be ruled out.
-
10 OVERDOSAGE
Topically applied mometasone furoate cream can be absorbed in sufficient amounts to produce systemic effects [see Warnings and Precautions (5.1)].
-
11 DESCRIPTION
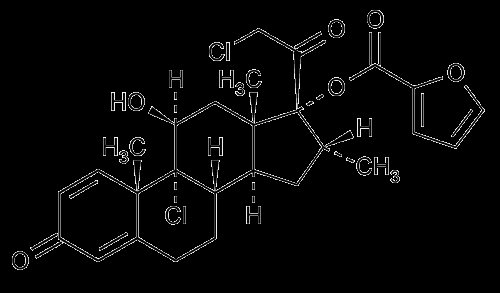
Mometasone furoate cream USP, 0.1% contains mometasone furoate USP for topical use. Mometasone furoate USP is a synthetic corticosteroid with anti-inflammatory activity.
Chemically, mometasone furoate USP is 9α,21-dichloro-11β,17-dihydroxy-16α-methylpregna-1,4-diene-3,20-dione 17-(2-furoate), with the empirical formula C27H30CI2O6, a molecular weight of 521.43 and the following structural formula:
Mometasone furoate USP is a white to off-white powder, soluble in acetone and methylene chloride.
Each gram of mometasone furoate cream USP, 0.1% contains: 1 mg mometasone furoate USP in a cream base of hexylene glycol, phosphoric acid, propylene glycol stearate (55% monoester), stearyl alcohol and ceteareth-20, titanium dioxide, aluminum starch octenylsuccinate (Gamma Irradiated), white wax, white petrolatum, and purified water.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Like other topical corticosteroids, mometasone furoate has anti-inflammatory, antipruritic, and vasoconstrictive properties. The mechanism of the anti-inflammatory activity of the topical steroids, in general, is unclear. However, corticosteroids are thought to act by the induction of phospholipase A2 inhibitory proteins, collectively called lipocortins. It is postulated that these proteins control the biosynthesis of potent mediators of inflammation such as prostaglandins and leukotrienes by inhibiting the release of their common precursor arachidonic acid. Arachidonic acid is released from membrane phospholipids by phospholipase A2.
12.2 Pharmacodynamics
Studies performed with mometasone furoate cream indicate that it is in the medium range of potency as compared with other topical corticosteroids.
In a study evaluating the effects of mometasone furoate cream on the HPA axis, 15 grams were applied twice daily for 7 days to six adult subjects with psoriasis or atopic dermatitis.The cream was applied without occlusion to at least 30% of the body surface. The results showed that the drug caused a slight lowering of adrenal corticosteroid secretion [see Warnings and Precautions (5.1)].
Ninety-seven pediatric subjects ages 6 to 23 months with atopic dermatitis were enrolled in an open-label HPA axis safety study. Mometasone furoate cream was applied once daily for approximately 3 weeks over a mean body surface area of 41% (range 15%-94%). In approximately 16% of subjects who showed normal adrenal function by Cortrosyn test before starting treatment, adrenal suppression was observed at the end of treatment with mometasone furoate cream. The criteria for suppression were: basal cortisol level of ≤5 mcg/dL, 30-minute post-stimulation level of ≤18 mcg/dL, or an increase of <7 mcg/dL. Follow-up testing 2 to 4 weeks after stopping treatment, available for 5 of the subjects, demonstrated suppressed HPA axis function in one subject, using these same criteria [see Use in Specific Populations (8.4)].
12.3 Pharmacokinetics
The extent of percutaneous absorption of topical corticosteroids is determined by many factors including the vehicle and the integrity of the epidermal barrier. Studies in humans indicate that approximately 0.4% of the applied dose of mometasone furoate cream enters the circulation after 8 hours of contact on normal skin without occlusion. Inflammation and/or other disease processes in the skin may increase percutaneous absorption.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term animal studies have not been performed to evaluate the carcinogenic potential of mometasone furoate cream. Long-term carcinogenicity studies of mometasone furoate were conducted by the inhalation route in rats and mice. In a 2-year carcinogenicity study in Sprague Dawley rats, mometasone furoate demonstrated no statistically significant increase of tumors at inhalation doses up to 67 mcg/kg (approximately 0.04 times the estimated maximum clinical topical dose from mometasone furoate cream on a mcg/m2 basis). In a 19-month carcinogenicity study in Swiss CD-1 mice, mometasone furoate demonstrated no statistically significant increase in the incidence of tumors at inhalation doses up to 160 mcg/kg (approximately 0.05 times the estimated maximum clinical topical dose from mometasone furoate cream on a mcg/m2 basis).
Mometasone furoate increased chromosomal aberrations in an in vitro Chinese hamster ovary cell assay, but did not increase chromosomal aberrations in an in vitro Chinese hamster lung cell assay. Mometasone furoate was not mutagenic in the Ames test or mouse lymphoma assay, and was not clastogenic in an in vivo mouse micronucleus assay, a rat bone marrow chromosomal aberration assay, or a mouse male germ-cell chromosomal aberration assay. Mometasone furoate also did not induce unscheduled DNA synthesis in vivo in rat hepatocytes.
In reproductive studies in rats, impairment of fertility was not produced in male or female rats by subcutaneous doses up to 15 mcg/kg (approximately 0.01 times the estimated maximum clinical topical dose from mometasone furoate cream, on a mcg/m2 basis)
-
14 CLINICAL STUDIES
The safety and efficacy of the mometasone furoate cream for the treatment of corticosteroid-responsive dermatoses were evaluated in two randomized, double-blind, vehicle-controlled clinical trials, one in psoriasis and one in atopic dermatitis. A total 366 subjects (12-81 years of age), of whom 177 received mometasone furoate cream and 181 subjects received vehicle cream, were evaluated in these trials. Mometasone furoate cream or the vehicle cream were applied once daily for 21 days.
The two trials showed mometasone furoate cream is effective in the treatment of psoriasis and atopic dermatitis.
- 16 HOW SUPPLIED/STORAGE AND HANDLING
-
17 PATIENT COUNSELING INFORMATION
Inform patients of the following:
- •
- Use mometasone furoate cream as directed by the physician. It is for external use only.
- •
- Avoid contact with the eyes.
- •
- Do not use mometasone furoate cream on the face, underarms, or groin areas unless directed by the physician.
- •
- Do not use mometasone furoate cream for any disorder other than that for which it was prescribed.
- •
- The treated skin area should not be bandaged or otherwise covered or wrapped so as to be occlusive, unless directed by the physician.
- •
- Report any signs of local adverse reactions to the physician.
- •
- Advise patients not to use mometasone furoate cream in the treatment of diaper dermatitis. Do not apply mometasone furoate cream in the diaper area, as diapers or plastic pants may constitute occlusive dressing.
- •
- Discontinue therapy when control is achieved. If no improvement is seen within 2 weeks, contact the physician.
- •
- Do not use other corticosteroid-containing products with mometasone furoate cream without first consulting with the physician.
Manufactured by:
Glenmark Pharmaceuticals Ltd.
Village Kishanpura, Baddi Nalagarh Road
District : Solan, Himachal Pradesh - 173205, IndiaManufactured for:
Glenmark Pharmaceuticals Inc., USA
Mahwah, NJ 07430Questions? 1 (888)721-7115
www.glenmarkpharma.com/usaSeptember 2014
- Mometasone Furoate
-
INGREDIENTS AND APPEARANCE
MOMETASONE FUROATE
mometasone furoate creamProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:50090-2179(NDC:68462-192) Route of Administration TOPICAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength MOMETASONE FUROATE (UNII: 04201GDN4R) (MOMETASONE - UNII:8HR4QJ6DW8) MOMETASONE FUROATE 1 mg in 1 g Inactive Ingredients Ingredient Name Strength HEXYLENE GLYCOL (UNII: KEH0A3F75J) PHOSPHORIC ACID (UNII: E4GA8884NN) PROPYLENE GLYCOL MONOSTEARATE (UNII: MZM1I680W0) STEARYL ALCOHOL (UNII: 2KR89I4H1Y) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) WHITE WAX (UNII: 7G1J5DA97F) PETROLATUM (UNII: 4T6H12BN9U) WATER (UNII: 059QF0KO0R) ALUMINUM STARCH OCTENYLSUCCINATE (UNII: I9PJ0O6294) POLYOXYL 20 CETOSTEARYL ETHER (UNII: YRC528SWUY) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:50090-2179-0 45 g in 1 TUBE; Type 0: Not a Combination Product 10/24/2015 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA078541 05/28/2008 Labeler - A-S Medication Solutions (830016429) Establishment Name Address ID/FEI Business Operations A-S Medication Solutions 830016429 RELABEL(50090-2179)