Label: CHIRHOSTIM- human secretin injection, powder, lyophilized, for solution
CHIRHOSTIM 40- human secretin injection, powder, lyophilized, for solution


- NDC Code(s): 67066-005-01, 67066-007-01
- Packager: ChiRhoClin, Inc.
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: New Drug Application
Drug Label Information
Updated April 2, 2024
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use CHIRHOSTIM® safely and effectively. See full prescribing information for CHIRHOSTIM®.
CHIRHOSTIM® (human secretin) for injection, for intravenous use
Initial U.S. Approval: 2004RECENT MAJOR CHANGES
Dosage and Administration (2.1) 07/2017
Contraindications, removed (4) 07/2017
Warnings and Precautions (5.1, 5.2) 07/2017
INDICATIONS AND USAGE
- ChiRhoStim® is a secretin class hormone indicated for stimulation of:
- pancreatic secretions, including bicarbonate, to aid in the diagnosis of exocrine pancreas dysfunction (1)
- gastrin secretion to aid in the diagnosis of gastrinoma (1)
- pancreatic secretions to facilitate the identification of the ampulla of Vater and the accessory papilla during endoscopic retrograde cholangiopancreatography (ERCP) (1)
(1)
DOSAGE AND ADMINISTRATION
- To avoid an incorrect stimulation test result, discontinue the following drugs for the recommended amount of time prior to administration of ChiRhoStim®:
- anticholinergic drugs: at least 5 half-lives. (2.1, 5.1, 7.1)
- H2-receptor antagonists: at least 2 days. (2.1, 5.2, 7.2)
- proton pump inhibitors (PPIs): consult the prescribing information for specific PPIs. (2.1, 5.2, 7.2)
- The recommended dosage by indication is shown in the table:
(2)
Indication (2)
Recommended Dosage Regimen (2.2) (2)
Stimulation of pancreatic secretions, including bicarbonate, to aid in the diagnosis of exocrine pancreas dysfunction (2)
0.2 mcg/kg by intravenous injection over 1 minute (2)
Stimulation of gastrin secretion to aid in diagnosis of gastrinoma (2)
0.4 mcg/kg by intravenous injection over 1 minute (2)
Stimulation of pancreatic secretions to facilitate the identification of the ampulla of Vater and accessory papilla during endoscopic retrograde cholangiopancreatography (ERCP) (2)
0.2 mcg/kg by intravenous injection over 1 minute (2)
- Determine the number of vials to be reconstituted based on the patient’s weight and prescribed dose (2.2)
- ChiRhoStim® must be reconstituted with 0.9% Sodium Chloride Injection prior to administration (2.2)
- See full prescribing information for complete information on exocrine test methods (2.3)
DOSAGE FORMS AND STRENGTHS
For injection: 16 mcg or 40 mcg of human secretin as a lyophilized powder in single-dose vial for reconstitution (3) (3)
CONTRAINDICATIONS
None (4) (4)
WARNINGS AND PRECAUTIONS
- Hyporesponse to Secretin Stimulation Testing in Patients with Vagotomy, Inflammatory Bowel Disease or Receiving Anticholinergics: Discontinue anticholinergic drugs at least 5 half-lives prior to stimulation testing; consider additional testing and clinical assessments for aid in diagnosis. (2.1, 5.1, 7.1)
- Hyperresponse to Secretin Stimulation Testing: Increased gastrin secretion in patients receiving H 2-receptor antagonists or PPIs falsely suggesting gastrinoma; discontinue co-administered drug prior to stimulation testing. Increased pancreatic secretions in patients with alcoholic or other liver disease masking coexisting pancreatic disease; consider additional testing and clinical assessments for aid in diagnosis. (2.1, 5.2, 7.2)
ADVERSE REACTIONS
Most common adverse reactions (≥2 patients) are nausea, vomiting, flushing, and upset stomach. (6.1) (6)
(6)
To report SUSPECTED ADVERSE REACTIONS, contact ChiRhoClin, Inc. at 1-877-272-4888 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. (6)
(6)
See 17 for PATIENT COUNSELING INFORMATION. (6)
(6)
Revised: 07/2017 (6)
Revised: 7/2017
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
INDICATIONS AND USAGE
DOSAGE AND ADMINISTRATION
DOSAGE FORMS AND STRENGTHS
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
ADVERSE REACTIONS
DRUG INTERACTIONS
DESCRIPTION
CLINICAL PHARMACOLOGY
Mechanism of Action
Pharmacokinetics
CLINICAL STUDIES
REFERENCES
HOW SUPPLIED/STORAGE AND HANDLING
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
INDICATIONS AND USAGE
ChiRhoStim ® is indicated for the stimulation of:
- pancreatic secretions, including bicarbonate, to aid in the diagnosis of pancreatic exocrine dysfunction.
- gastrin secretion to aid in the diagnosis of gastrinoma, and
- pancreatic secretions to facilitate the identification of the ampulla of Vater and accessory papilla during endoscopic retrograde cholangiopancreatography (ERCP).
-
DOSAGE AND ADMINISTRATION
2.2 Preparation and Dosage Regimen
The recommended dosage regimen of ChiRhoStim® by indication is shown below in Table 1.
TABLE 1: Dosage by Indication
Indication
Recommended Dosage Regimen
Stimulation of pancreatic secretions, including bicarbonate, to aid in the diagnosis of exocrine pancreas dysfunction
0.2 mcg/kg by intravenous injection over 1 minute
Stimulation of gastrin secretion to aid in diagnosis of gastrinoma
0.4 mcg/kg by intravenous injection over 1 minute
Stimulation of pancreatic secretions to facilitate the identification of the ampulla of Vater and accessory papilla during endoscopic retrograde cholangiopancreatography (ERCP)
0.2 mcg/kg by intravenous injection over 1 minute
Preparation of Recommended Dosage
- ChiRhoStim ® is a lyophilized powder, which requires reconstitution prior to intravenous administration.
- Determine the number of vials needed for the prescribed dosage based on the patient’s weight and recommended dosage. Follow these steps to determine the patient dose:
- Total dose (mcg) = patient’s weight (kg) x prescribed dose (mcg/kg).
- Total injection volume (mL) = total dose (mcg) divided by the concentration of the reconstituted solution (2 mcg/mL).
- Round the total injection volume to the nearest tenth of a mL.
- Total number of vials = total injection volume divided by the vial volume (8 mL).
- To reconstitute one 16 mcg vial:
- Dissolve the contents of the ChiRhoStim ® 16 mcg vial in 8 mL of 0.9% Sodium Chloride Injection, USP, to yield a concentration of 2 mcg/mL.
- Shake vigorously to ensure dissolution.
- Inspect the reconstituted solution visually for particulate matter and discoloration prior to administration. If particulate matter or discoloration is seen, discard the reconstituted solution.
- To reconstitute one 40 mcg vial:
- Dissolve the contents of the ChiRhoStim ® 40 mcg vial in 10 mL of 0.9% Sodium Chloride Injection, USP, to yield a concentration of 4 mcg/mL.
- Shake vigorously to ensure dissolution.
- Inspect the reconstituted solution visually for particulate matter and discoloration prior to administration. If particulate matter or discoloration is seen, discard the reconstituted solution.
- Repeat steps above to reconstitute additional vials, as needed, to administer the total dose.
- Use immediately after reconstitution and discard any unused portion.
2.3 Administration and Test Methods
Stimulation testing with ChiRhoStim ® should only be performed by physicians with sufficient expertise. Ensure that the institution has established normative ranges for pancreatic exocrine response.
Stimulation of Pancreatic Secretions, including Bicarbonate, to Aid in the Diagnosis of Exocrine Pancreas Dysfunction:
Preparation:
- Instruct patients to fast for at least 12 to 15 hours prior to beginning the test.
Sample Collection: [performed using either the gastroduodenal/Dreiling tube (fluoroscopic) or endoscopic collection method]
-
Gastroduodenal (Dreiling) Tube Collection Method
- Pass a radiopaque, double-lumen gastroduodenal tube through the mouth using a guidewire.
- Under fluoroscopic guidance, place the opening of the proximal lumen in the gastric antrum and the opening of the distal lumen beyond the ampulla of Vater. Confirm the tube positioning and secure the tube.
- Connect both the proximal (gastric) and distal (duodenal) lumens to low intermittent suction, and apply negative pressure of 25 to 40 mmHg to both lumens.
- Collect a sample of the duodenal contents and check the pH of the aspirate to verify tube position. Proceed to next step if the duodenal aspirate has a pH of 6 or higher. If the pH is less than 6, reposition the tube.
- Collect a baseline sample of duodenal fluid for a 15-minute period.
- Administer ChiRhoStim ® at a dose of 0.2 mcg/kg body weight intravenously over 1 minute [see Dosage and Administration (2.2)]. For the 60-minute period following the injection, collect four consecutive 15-minute samples of duodenal fluid. Clear the duodenal lumen of the tube with an injection of air after each 15-minute sample collection. Note that wide variation in aspirate volumes is indicative of incomplete aspiration between samples.
- Endoscopic Collection Method: Endoscopic Pancreatic Function Test (ePFT)
- Administer a topical anesthetic spray to the posterior pharynx and place a bite block in the mouth.
- Perform a standard upper endoscopy by passing the endoscope into the stomach with the patient in the left lateral decubitus position.
- After gastric insufflation, aspirate all gastric fluid through the endoscope and discard.
- Pass the endoscope through the pylorus into small intestine and position the tip of the endoscope at the junction of the second and third portion of the duodenum.
- Aspirate duodenal fluid for several seconds to clear the residual gastric acid from the tube.
- Collect a baseline aspirate of duodenal fluid (3 to 5 mL) from the post-bulbar duodenum.
- Administer ChiRhoStim ® at a dose of 0.2 mcg/kg of body weight intravenously over 1 minute [see Dosage and Administration (2.2)].
- Starting 15 minutes after administration of ChiRhoStim ®, collect 4 timed duodenal fluid aspirates (each 3 to 5 mL) at 15-minute intervals. Keep the patient in the left lateral decubitus position throughout the procedure.
Sample Handling and Interpretation:
- Place fluid specimens on ice for immediate measurement of bicarbonate concentration. If samples will not be analyzed immediately, store fluid at –80°C.
- Peak bicarbonate concentrations of 80 to 130 mEq/L after administration indicate normal pancreatic exocrine function.
Stimulation of Gastrin Secretion to Aid in the Diagnosis of Gastrinoma:
Preparation:
- Instruct patients to fast for at least 12 hours prior to beginning the test.
Sample Collection:
- Before administering ChiRhoStim ®, draw two blood samples for determination of fasting serum gastrin levels (baseline values).
- Administer ChiRhoStim ® at a dose of 0.4 mcg/kg of body weight intravenously over 1 minute [see Dosage and Administration (2.2)].
- Collect post-injection blood samples after 1, 2, 5, 10, and 30 minutes for determination of serum gastrin concentrations.
Sample Interpretation:
- Gastrinoma is strongly suspected in patients who show an increase in serum gastrin concentration of more than 110 picograms (pg) per mL over baseline levels on any of the post injection samples.
Stimulation of Pancreatic Secretions to Facilitate the Identification of the Ampulla of Vater and Accessory Papilla During Endoscopic Retrograde Cholangiopancreatography (ERCP):
When difficulty is encountered by the endoscopist in identifying the ampulla of Vater or in identifying the accessory papilla in patients with pancreas divisum:
- Administer ChiRhoStim ® at a dose of 0.2 mcg/kg of body weight intravenously over 1 minute [see Dosage and Administration (2.2)].
- Visible excretion of pancreatic fluid from the orifices of these papillae will enable their identification and facilitate cannulation.
- DOSAGE FORMS AND STRENGTHS
- CONTRAINDICATIONS
- WARNINGS AND PRECAUTIONS
-
ADVERSE REACTIONS
6.1 Clinical Trials Experience
Because clinical trials are conducted under varying conditions, adverse reaction rates observed during the clinical trials of a drug cannot always be directly compared to the rates observed during the clinical trials of another drug and may not reflect the adverse reaction rates observed in practice.
The data described below reflect exposure to ChiRhoStim® in 531 patients from an open-label clinical trial. The population consisted of patients aged 1 to 91 years, 185 males, 346 females, 480 Caucasians, 31 Blacks, 12 American Indians, 6 Hispanics, and 2 Asians with known or suspected diseases of the exocrine pancreas including chronic pancreatitis and pancreatic cancer. Most patients received a single dose of ChiRhoStim® in a dose range of 0.2 mcg/kg to 0.4 mcg/kg. The most common adverse reactions (reported in at least 2 patients in the trial) are listed in Table 2.
TABLE 2
Adverse Reactions in at Least 2 Patients Treated with a Single-Dose of ChiRhoStim® in a Clinical Trial
Adverse Reaction
ChiRhoStim®
Number of Patients
N = 531
Nausea
9
Vomiting
3
Flushing
2
Upset stomach
2
-
DRUG INTERACTIONS
7.1 Hyporesponse with Anticholinergics
The concomitant use anticholinergic drugs may cause a hyporesponse to stimulation testing with ChiRhoStim ®. Discontinue anticholinergic drugs at least 5 half-lives before administering ChiRhoStim ®[see Dosage and Administration (2.1)].
7.2 Hyperresponse of Gastrin Secretion with H 2-Receptor Antagonists and PPIs
The concomitant use of H 2-receptor antagonists or PPIs may cause a hyperresponse in gastrin secretion in response to stimulation testing with ChiRhoStim ®, falsely suggesting gastrinoma.
Discontinue H 2-receptor antagonists at least 2 days before administering ChiRhoStim ® to aid in the diagnosis of gastrinoma.
The time it takes for serum gastrin concentrations to return to baseline following discontinuation of PPIs is specific to the individual drug. Consult the prescribing information of each specific PPI before administering ChiRhoStim ® to aid in the diagnosis of gastrinoma.
-
USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no available data (either clinical studies or postmarketing reports) of use of synthetic human secretin in pregnant women. Animal reproduction studies have not been conducted with synthetic human secretin.
The estimated background risk of major birth defects and miscarriage for the indicated populations are unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
8.2 Lactation
Risk Summary
There are no data on the presence of synthetic human secretin in human or animal milk, the effects of synthetic human secretin on the breastfed infant, or the effects of synthetic human secretin on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for ChiRhoStim ® and any potential adverse effects on the breastfed infant from ChiRhoStim ® or from the underlying maternal condition.
8.4 Pediatric Use
The safety and effectiveness of ChiRhoStim ® in pediatric patients have not been established.
8.5 Geriatric Use
Among the 531 patients who have received ChiRhoStim ® in a clinical trial, 11% were 65 years of age or older and 5% were 75 years of age or older. No overall differences in safety, pharmacologic response, or diagnostic effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and the younger patients, but greater sensitivity of some older individuals cannot be ruled out.
-
DESCRIPTION
ChiRhoStim ® is a pure sterile, nonpyrogenic, lyophilized white cake powder acetate salt of secretin, a peptide hormone. ChiRhoStim ® has an amino acid sequence identical to the naturally occurring hormone consisting of 27 amino acids. Synthetic human secretin is chemically defined as follows:
Molecular Weight 3039.44
Empirical Formula: C 130H 220N 44O 39
CAS # 108153-74-8
Structural Formula:
His-Ser-Asp-Gly-Thr-Phe-Thr-Ser-Glu-Leu-Ser-Arg-Leu-Arg-Glu-Gly-Ala-Arg-Leu-Gln-Arg-Leu-Leu-Gln-Gly-Leu-Val-NH 2
The standard unit of biological activity for ChiRhoStim ® is the clinical unit (CU). (3) One (1) CU of secretin biological activity is equal to 0.2 micrograms (mcg) of human secretin.
ChiRhoStim ® is available in two strengths:
As a 10 mL single-dose vial which contains 16 mcg of purified synthetic human secretin, 1.5 mg of L-cysteine hydrochloride, 20 mg of mannitol, and 9 mg of sodium chloride. When reconstituted in 8 mL of Sodium Chloride Injection USP, each mL of solution contains 2 mcg synthetic human secretin for intravenous use. The pH of the reconstituted solution has a range of 3 to 6.5.
As a 10 mL single-dose vial which contains 40 mcg of purified synthetic human secretin, 3.75 mg of L-cysteine hydrochloride, 50 mg of mannitol, and 22.5 mg of sodium chloride per vial. When reconstituted in 10 mL of Sodium Chloride Injection USP, each mL of solution contains 4 mcg synthetic human secretin for intravenous use. The pH of the reconstituted solution has a range of 3 to 6.5.
-
CLINICAL PHARMACOLOGY
Mechanism of Action
12.1 Mechanism of Action
The primary action of ChiRhoStim ® is to stimulate pancreatic ductal cells to secrete pancreas fluid in large volumes that contain bicarbonate.
Secretin is a hormone that is normally released from the duodenum upon exposure of the proximal intestinal lumen to gastric acid, fatty acids and amino acids. Secretin is released from enterochromaffin cells in the intestinal mucosa. Secretin receptors have been identified in the pancreas, stomach, liver, colon and other tissues. When secretin binds to secretin receptors on pancreatic duct cells it opens cystic fibrosis transmembrane conductance regulator (CFTR) channels, leading to secretion of bicarbonate-rich-pancreatic fluid. Secretin may also work through vagal-vagal neural pathways since stimulation of the efferent vagus nerve stimulates bicarbonate secretion and atropine blocks secretin-stimulated pancreatic secretion.
Pharmacokinetics
12.3 Pharmacokinetics
The pharmacokinetic profile for synthetic human secretin was evaluated in 12 healthy subjects following a single-dose of human secretin administered as a 0.4 mcg/kg intravenous bolus. The plasma concentrations of human secretin declined to baseline concentrations within 90 to 120 minutes. The elimination half-life of synthetic human secretin is 45 minutes. The clearance of synthetic human secretin is 580.9 ± 51.3 mL/min and the volume of distribution is 2.7 liters.
-
CLINICAL STUDIES
14.1 Stimulation of Pancreatic Secretions, Including Bicarbonate to Aid in the Diagnosis of Exocrine Pancreas Dysfunction
ChiRhoStim® administered intravenously stimulates the exocrine pancreas to secrete pancreatic juice, which can assist in the diagnosis of exocrine pancreas dysfunction. Normal ranges for pancreatic secretory response to intravenous secretin in patients with defined pancreatic disease have been shown to vary. One source of variation is related to the inter-investigator differences in operative technique.In two studies, a total of 18 patients with a documented history of chronic pancreatitis were given 0.2 mcg/kg synthetic human secretin (sHS), 0.2 mcg/kg synthetic porcine secretin (sPS), and 1 CU/kg (equal to 0.2 mcg/kg for biologically derived secretin (bPS)) in a crossover design. The results appear in Figures 1 and 2. In another study, 35 healthy subjects were given sHS at a dose of 0.2 mcg/kg. The results appear in Figures 1 and 2.
FIGURE 1
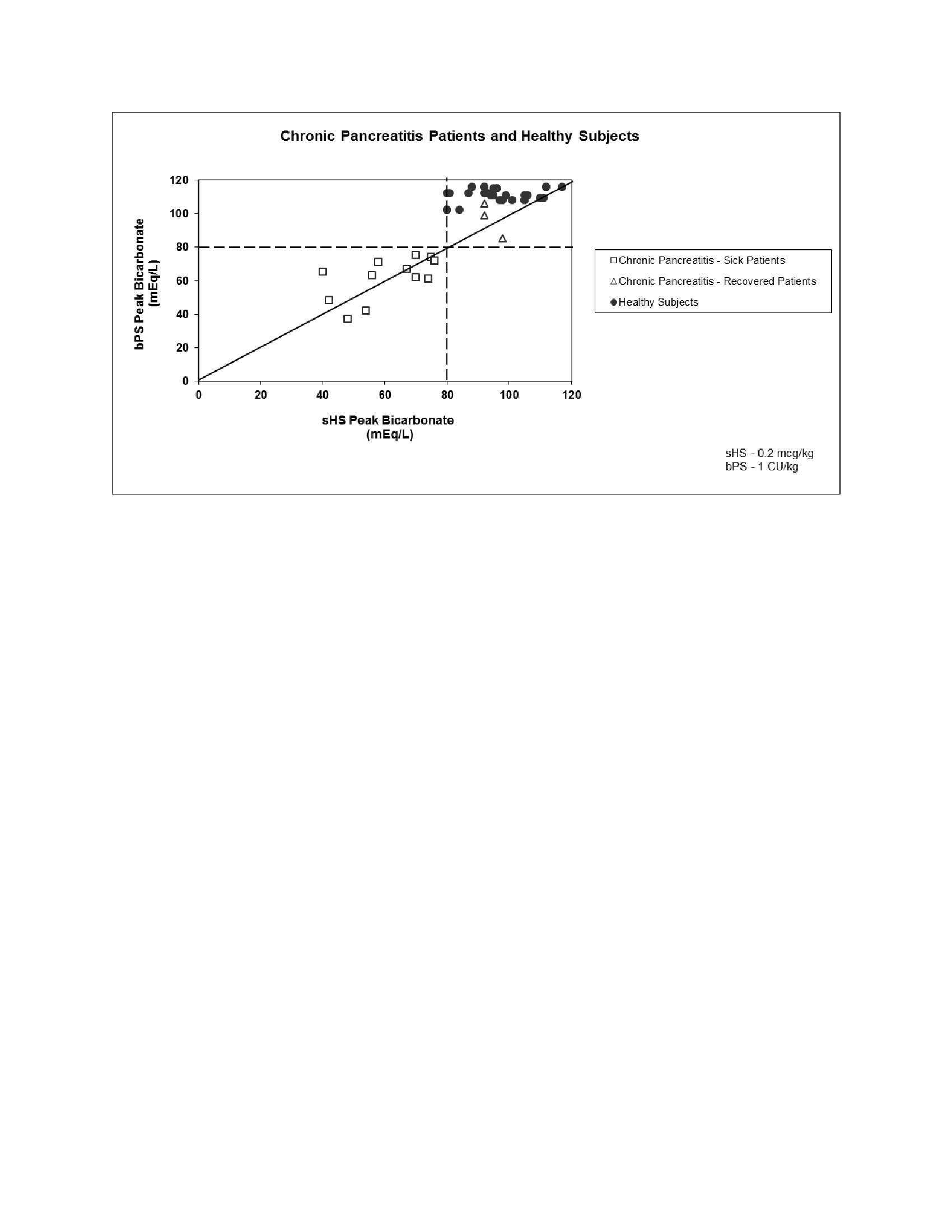 FIGURE 2
FIGURE 2
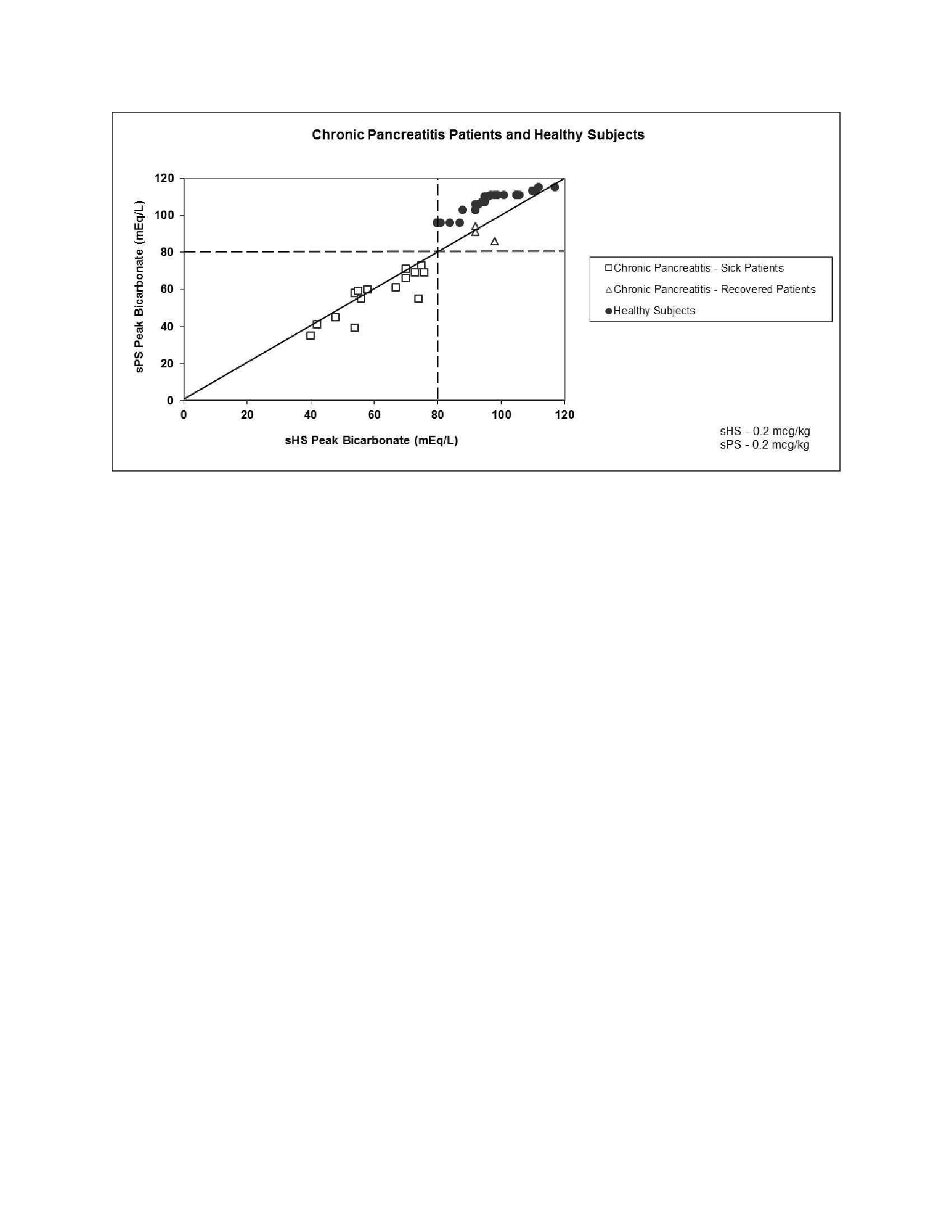 The values obtained for Figures 1 and 2 were performed by investigators skilled in performing secretin stimulation testing and are to be taken only as guidelines. These results should not be generalized to results of secretin stimulation testing conducted in other laboratories. However, a volume response of less than 2 mL/kg/hr, bicarbonate concentration of less than 80 mEq/L, and a bicarbonate output of less than 0.2 mEq/kg/hr are consistent with impaired pancreatic function.
The values obtained for Figures 1 and 2 were performed by investigators skilled in performing secretin stimulation testing and are to be taken only as guidelines. These results should not be generalized to results of secretin stimulation testing conducted in other laboratories. However, a volume response of less than 2 mL/kg/hr, bicarbonate concentration of less than 80 mEq/L, and a bicarbonate output of less than 0.2 mEq/kg/hr are consistent with impaired pancreatic function.
A physician or institution planning to perform secretin stimulation testing as an aid to the diagnosis of pancreatic disease should begin by assessing enough normal subjects (greater than 5) to develop proficiency in proper techniques and to generate normal response ranges for the commonly assessed parameters for pancreatic exocrine response to ChiRhoStim®.
In three crossover studies evaluating 21 different patients with a documented history of chronic pancreatitis, sHS was compared to sPS and bPS at a dose of 0.2 mcg/kg for each drug. All of the patients treated with these drugs had peak bicarbonate concentrations of less than 80 mEq/L.
Pancreatic secretory response to intravenous synthetic human secretin in 35 healthy subjects demonstrated a mean peak bicarbonate concentration of 100 mEq/L and a mean total volume over one hour of 260.7 mL. All 35 subjects had peak bicarbonate concentrations greater than or equal to 80 mEq/L.
14.2 Stimulation of Gastrin Secretion to Aid in the Diagnosis of Gastrinoma
ChiRhoStim® administered intravenously stimulates gastrin release in patients with gastrinoma (Zollinger-Ellison Syndrome), whereas no or only small changes in serum gastrin concentrations occur in healthy subjects and in patients with duodenal ulcer disease. Discriminant analysis was used to establish secretin stimulation testing as an aid in the diagnosis of gastrinoma. An increase from basal levels of greater than or equal to 110 pg/mL was the optimal point separating positive and negative tests. This gastrin response is the basis for the use of secretin as a provocative test in the evaluation of patients in whom gastrinoma is a diagnostic consideration.
In a three way crossover study, 6 patients with tissue confirmed gastrinoma received synthetic human secretin (ChiRhoStim®), synthetic porcine secretin and biologically derived porcine secretin at a dose of 0.4 mcg/kg for each drug. Serum gastrin levels were reported to be greater than 110 pg/mL for all secretin products tested after stimulation. Testing of ChiRhoStim® in 12 healthy subjects demonstrated completely negative results for gastrinoma.
14.3 Stimulation of Pancreatic Secretion to Facilitate Identification of the Ampulla of Vater and the Accessory Papilla During Endoscopic Retrograde Cholangiopancreatography (ERCP)
In a randomized, placebo controlled crossover study in 24 patients with pancreas divisum undergoing ERCP, ChiRhoStim® at a dose of 0.2 mcg/kg resulted in 16 of 24 successful cannulations of the minor duct compared to 2 of 24 for placebo.
-
REFERENCES
- Gardner TB, Purich ED and Gordon SR. Pancreatic Duct Compliance After Secretin Stimulation. A Novel Endoscopic Ultrasound Diagnostic Tool for Chronic Pancreatitis. Pancreas. 2012 Mar;41(2):290-94.
- Jorpes, E. and Mutt V. On the biological assay of secretin. The reference standard. Acta Physiol Scand. 1966 Mar;66(3):316-25.
- HOW SUPPLIED/STORAGE AND HANDLING
- PATIENT COUNSELING INFORMATION
- PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
CHIRHOSTIM
human secretin injection, powder, lyophilized, for solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:67066-005 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SECRETIN HUMAN (UNII: A0426J905J) (SECRETIN HUMAN - UNII:A0426J905J) SECRETIN HUMAN 16 ug in 8 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:67066-005-01 8 mL in 1 VIAL, SINGLE-USE; Type 0: Not a Combination Product 08/01/2004 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA021256 08/01/2004 CHIRHOSTIM 40
human secretin injection, powder, lyophilized, for solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:67066-007 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SECRETIN HUMAN (UNII: A0426J905J) (SECRETIN HUMAN - UNII:A0426J905J) SECRETIN HUMAN 40 ug in 10 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:67066-007-01 10 mL in 1 VIAL, SINGLE-USE; Type 0: Not a Combination Product 06/21/2007 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA021256 06/01/2007 Labeler - ChiRhoClin, Inc. (036663672) Establishment Name Address ID/FEI Business Operations ChiRhoClin, Inc. 036663672 manufacture(67066-007) Establishment Name Address ID/FEI Business Operations Bell-More Laboratories, Inc. 074932856 manufacture(67066-005)