Label: hypaque sodium- Diatrizoate Meglumine injection, solution
-
Contains inactivated NDC Code(s)
NDC Code(s): 0407-0746-04, 0407-0747-02, 0407-0749-20, 0407-0750-10 - Packager: Amersham Health Inc.
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
Drug Label Information
Updated August 3, 2007
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
- N/A - Section Title Not Found In Database
- SPL UNCLASSIFIED SECTION
-
DESCRIPTION
HYPAQUE meglumine, brand of diatrizoate meglumine, is a water-soluble, radiopaque diagnostic medium. It is a triiodinated benzoic acid derivative containing 47.06 percent organically bound iodine. It is constituted as an iodinated anion (diatrizoate) and a radiolucent cation (meglumine).
HYPAQUE meglumine 60 percent (w/v) is a sterile aqueous solution containing 60 g of the meglumine salt of diatrizoic acid per 100 mL of solution. The solution is a clear-colorless to pale yellow liquid, and the pH is adjusted between 6.5 and 7.7 with diatrizoic acid or meglumine solution. It is a relatively thermostable solution and may be autoclaved without harmful effects, although it should be protected from strong light. The 60 percent solution contains edetate calcium disodium 1:10,000 as a sequestering stabilizing agent. Each 1 mL contains approximately 282 mg of organically bound iodine. The viscosity of the solution is 6.17 cp at 25°C and 4.12 cp at 37°C.
It is hypertonic to blood with an osmolality of 1415 mosm/kg (determined by VPO). A 13 percent solution (w/v) is isotonic.
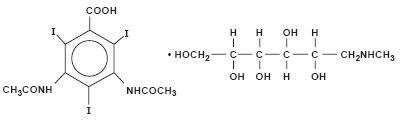
It is a colorless, microcrystalline solid which is readily soluble in water.
It is meglumine 3,5-diacetamido-2,4,6-triiodobenzoate (C11H9I3N2O4 • C7H17NO5) with a molecular weight of 809.13, and has the following structural formula:
-
CLINICAL PHARMACOLOGY
Intravascular injection of a radiopaque diagnostic agent opacifies those vessels in the path of the flow of the contrast medium, permitting radiographic visualization of the internal structures of the human body until significant hemodilution occurs.
At physiologic pH, the water soluble contrast media are completely dissociated into a radiopaque anion and a solubilizing cation. While circulating in tissue fluids, the compound remains ionized. However, it is not metabolized but excreted unchanged in the urine, each diatrizoate molecule remaining "obligated" to its meglumine moiety.
Following intravenous injection, the radiopaque diagnostic agents are immediately diluted in the circulating plasma. Equilibrium is reached with the extracellular compartment at about 10 minutes. Hence, the plasma concentration at 10 minutes is closely related to the dose corrected to body size.
The pharmacokinetics of the intravenously administered radiopaque contrast media are usually best described by a two compartment model with a rapid alpha phase for drug distribution and a slow beta phase for drug elimination. In patients with normal renal function, the alpha and beta half-lives were respectively 30 minutes and 120 minutes for diatrizoate. But in patients with renal functional impairment, the elimination half-life for the beta phase can be prolonged up to several days.
Injectable radiopaque diagnostic agents are excreted either through the liver or through the kidneys. The two excretory pathways are not mutually exclusive, but the main route of excretion seems to be governed by the affinity of the contrast medium for serum albumin. From 0% to 10% of diatrizoate sodium is bound to serum protein.
Diatrizoate salts are excreted unchanged predominantly through the kidneys by glomerular filtration. The amount excreted by the kidney during any period of time is determined by the filtered load; ie, the product of plasma contrast media concentration and glomerular filtration rate. The plasma concentration is dependent upon the dose administered and the body size. The glomerular filtration rate varies with the body size, sex, age, circulatory dynamics, diuretic effect of the drug, and renal function. In patients with normal renal function the maximum urinary concentration of diatrizoate meglumine occurs within 10 minutes with 12 percent of the administered dose being excreted. The mean values of cumulative urinary excretion for diatrizoate meglumine expressed as percentage of administered dose are 38 percent at 60 minutes, 45 percent at 3 hours, and 94 to 100 percent at 24 hours.
Urinary excretion of contrast media is delayed in infants younger than 1 month and in patients with urinary tract obstruction. The urinary iodine concentration is higher with the sodium salt of diatrizoic acid than with the meglumine salt.
The liver and small intestine provide the major alternate route of excretion for diatrizoate. In patients free of severe renal disease, the fecal recovery is less than 2 percent of the administered dose. In patients with severe renal impairment the excretion of these contrast media through the gallbladder and into the small intestine sharply increases; up to 20 percent of the administered dose has been recovered in the feces in 48 hours.
Saliva is a minor secretory pathway for injectable radiopaque diagnostic agents. In patients with normal renal function, minimal amounts of contrast media are secreted unchanged. However, in uremic patients small amounts of free iodides resulting from deiodination prior to administration or in vivo, have been detected in the saliva.
Diatrizoate salts cross the placental barrier in humans by simple diffusion and appear to enter fetal tissue passively. No apparent harm to the fetus was observed when diatrizoate sodium and diatrizoate meglumine were injected intravenously 24 hours prior to delivery. However, abnormal neonatal opacification of the small intestine and colon were detected 4 to 6 days after delivery. Procedures including radiation involve a certain risk related to the exposure of the fetus. (See PRECAUTIONS—General, Pregnancy Category C.)
Injectable radiopaque diagnostic agents are excreted unchanged in human milk. (See PRECAUTIONS-General, Nursing Mothers.)
Computerized Tomography
HYPAQUE meglumine 60 percent can be administered as an intravenous bolus for brain tissue enhancement using computerized tomography. Increased tissue contrast differential for the scan is achieved either because of increased vascular (arterial, venous, or capillary bed) contrast or by blood brain barrier penetration of the medium (or its absence) in certain localized areas of disrupted vascular permeability. The degree of tissue enhancement caused by increased blood contrast is directly related to blood iodine content. However, the degree of enhancement due to extravascular accumulation of iodine resulting from blood brain barrier disruption will depend on the extent of disruption, the blood level of iodine, and the time delay prior to scanning. The nature of the pathology will determine whether an immediate or delayed scan is optimal.
-
INDICATIONS AND USAGE
HYPAQUE meglumine 60 percent is indicated for excretory urography; cerebral angiography; peripheral arteriography; venography; operative, T-tube, or percutaneous transhepatic cholangiography; splenoportography; arthrography; discography; and contrast enhancement of computed tomographic head imaging.
Urography
Diatrizoate salts are used in small, medium, and large dose urography (see Dosage and Administration-EXCRETORY UROGRAPHY). Visualization of the urinary tract can be achieved by either direct intravenous bolus injection, intravenous drip infusion, or incidentally following intra-arterial procedures. Visualization of the urinary tract is delayed in infants less than 1 month old, and in patients with urinary tract obstruction (see CLINICAL PHARMACOLOGY).
Contrast Enhancement of Computed Tomographic Head Imaging
Injectable radiopaque contrast media may be used to refine diagnostic precision in areas of the brain which may not otherwise have been satisfactorily visualized.
Tumors
Radiopaque diagnostic agents may be useful to investigate the presence and extent of certain malignancies such as: gliomas including malignant gliomas, glioblastomas, astrocytomas, oligodendrogliomas and gangliomas, ependymomas, medulloblastomas, meningiomas, neuromas, pinealomas, pituitary adenomas, craniopharyngiomas, germinomas, and metastatic lesions.
The usefulness of contrast enhancement for the investigation of the retrobulbar space and in cases of low grade or infiltrative glioma has not been demonstrated.
In calcified lesions, there is less likelihood of enhancement. Following therapy, tumors may show decreased or no enhancement.
The opacification of the inferior vermis following contrast media administration has resulted in false-positive diagnosis in a number of normal studies.
Nonneoplastic Conditions
The use of injectable radiopaque diagnostic agents may be beneficial in the image enhancement of nonneoplastic lesions. Cerebral infarctions of recent onset may be better visualized with contrast enhancement, while some infarctions are obscured if contrast media are used. The use of iodinated contrast media results in contrast enhancement in about 60 percent of cerebral infarctions studied from one to four weeks from the onset of symptoms.
Sites of active infection may also be enhanced following contrast media administration.
Arteriovenous malformations and aneurysms will show contrast enhancement. For these vascular lesions, the enhancement is probably dependent on the iodine content of the circulating blood pool.
Hematomas and intraparenchymal bleeders seldom demonstrate any contrast enhancement. However, in cases of intraparenchymal clot, for which there is no obvious clinical explanation, contrast media administration may be helpful in ruling out the possibility of associated arteriovenous malformation.
Angiography
Diatrizoate salts are used for radiographic studies throughout the cardiovascular system.
Intravascular radiopaque diagnostic agents of high concentration are not recommended for cerebral or spinal angiography (see CONTRAINDICATIONS—General), and contrast agents with the lowest compatible viscosity and higher concentration of iodine (310 mg/mL to 480 mg/mL of bound iodine) must be used for angiocardiography. Contrast media approaching serum ionic content and osmolality have less potential for deleterious effects on the myocardium (see PRECAUTIONS—General, Drug Interactions).
Addition of chelating agents may contribute to toxicity in coronary angiography, and the sodium content of angiographic agents used in coronary arteriography is of crucial importance.
In addition to the following general CONTRAINDICATIONS, WARNINGS, PRECAUTIONS and ADVERSE REACTIONS, there are additional listings in these categories under the particular procedures.
-
CONTRAINDICATION—General
HYPAQUE meglumine 60 percent has no absolute contraindications in its recommended uses (see general WARNINGS and PRECAUTIONS).
Do not use HYPAQUE meglumine 60 percent solution for myelography or for examination of dorsal cysts or sinuses which might communicate with the subarachnoid space. Even a small amount in the subarachnoid space may produce convulsions and result in fatality. Epidural injection is also contraindicated.
Urography and large dose vascular procedures are contraindicated in dehydrated azotemic patients. (See also PRECAUTIONS—General.)
-
WARNINGS—General
SEVERE ADVERSE EVENTS—INADVERTENT INTRATHECAL ADMINISTRATION
Serious adverse reactions have been reported due to the inadvertent intrathecal administration of iodinated contrast media that are not indicated for intrathecal use. These serious adverse reactions include: death, convulsions, cerebral hemorrhage, coma, paralysis, arachnoiditis, acute renal failure, cardiac arrest, seizures, rhabdomyolysis, hyperthermia, and brain edema. Special attention must be given to insure that this drug product is not administered intrathecally.
Ionic iodinated contrast media inhibit blood coagulation, in vitro, more than nonionic contrast media. Nonetheless, it is prudent to avoid prolonged contact of blood with syringes containing ionic contrast media.
Serious, rarely fatal, thromboembolic events causing myocardial infarction and stroke have been reported during angiographic procedures with both ionic and nonionic contrast media. Therefore, meticulous intravascular administration technique is necessary, particularly during angiographic procedures, to minimize thromboembolic events. Numerous factors, including length of procedure, catheter and syringe material, underlying disease state and concomitant medications may contribute to the development of thromboembolic events. For these reasons, meticulous angiographic techniques are recommended including close attention to guidewire and catheter manipulation, use of manifold systems and/or three-way stopcocks, frequent catheter flushing with heparinized saline solutions and minimizing the length of the procedure. The use of plastic syringes in place of glass syringes has been reported to decrease but not eliminate the likelihood of in vitro clotting.
Excretory urography is potentially hazardous in patients with multiple myeloma. In some of those patients, therapeutically resistant anuria resulting in progressive uremia, renal failure and eventually death has followed this procedure. Although neither the contrast agent nor dehydration has been proved separately to be the cause of anuria in myelomatous patients, it has been speculated that the combination of both may be causative. The risk of excretory urography in myelomatous patients is not a contraindication to the procedure; however, they require special precautions. Partial dehydration in the preparation of these patients for the examination is not recommended since this may predispose to the precipitation of myeloma protein in the renal tubules. Myeloma, which occurs most commonly in persons over age 40, should be considered before instituting urographic procedures.
Contrast media may promote sickling in individuals who are homozygous for sickle cell disease when the material is injected intravenously or intra-arterially.
Administration of radiopaque materials to patients known or suspected of having pheochromocytoma should be performed with extreme caution. If, in the opinion of the physician, the possible benefits of such procedures outweigh the considered risks, the procedures may be performed; however, the amount of radiopaque medium injected should be kept to an absolute minimum. The blood pressure should be assessed throughout the procedure and measures for treatment of a hypertensive crisis should be available.
Recent reports of thyroid storm occurring following the intravascular use of iodinated radiopaque diagnostic agents in patients with hyperthyroidism or with an autonomously functioning thyroid nodule suggest that this additional risk be evaluated in such patients before use of HYPAQUE meglumine.
Contrast media administered for cardiac catheterization and angiocardiography may cause cellular injury to circulating lymphocytes. Chromosomal damage in humans includes inhibition of mitosis, increases in the number of micronuclei, and chromosome aberrations. The damages appear to be related to the contrast medium itself rather than to the x-ray radiation. It is to be noted that those agents have not been adequately tested in animal or laboratory systems.
Urography should be performed with caution in patients with severely impaired renal function and patients with combined renal and hepatic disease.
Subcutaneous extravasation, chiefly because of hypertonic cellulitis, causes transitory stinging. If the volume extravasated is small, ill effects are very unlikely. However, if the extravasation is extensive especially in poorly vascularized areas (eg, dorsum of the foot or hand), and especially in the presence of vascular disease, skin slough may occur. Injection of sterile water to dilute or addition of spreading agents to speed absorption have not been successful and may aggravate the condition.
Selective spinal arteriography or arteriography of trunks providing spinal branches can cause mild to severe muscle spasm. However, serious neurologic sequelae, including permanent paralysis, have occasionally been reported. (See also ANGIOGRAPHY, Precaution.)
In patients with subarachnoid hemorrhage, a rare association between contrast administration and clinical deterioration, including convulsions and death, has been reported. Therefore, administration of intravascular iodinated ionic contrast media in these patients should be undertaken with caution.
-
PRECAUTIONS—General
Diagnostic procedures which involve the use of radiopaque diagnostic agents should be carried out under the direction of personnel with the prerequisite training and with a thorough knowledge of the particular procedure to be performed. Appropriate facilities should be available for coping with any complication of the procedure, as well as for emergency treatment of severe reactions to the contrast agent itself. After parenteral administration of a radiopaque agent, competent personnel and emergency facilities should be available for at least 30 to 60 minutes since severe delayed reactions have occurred (see ADVERSE REACTIONS—General).
The possibility of a reaction, including serious, life-threatening, fatal, anaphylactic or cardiovascular reactions should always be considered (see ADVERSE REACTIONS). It is of utmost importance that a course of action be carefully planned in advance for immediate treatment of serious reactions, and that adequate and appropriate personnel be readily available in case of any reaction.
Preparatory dehydration for angiography and CT procedures is unnecessary and may be dangerous, contributing to acute renal failure in infants, young children, the elderly, patients with preexisting renal insufficiency, patients with advanced vascular disease, and diabetic patients. Dehydration in these patients seems to be enhanced by the osmotic diuretic action of urographic agents. Overnight fluid retention for urography may be undesirable and is considered unnecessary when using this relatively high (60%) concentration.
Although azotemia is not a contraindication, the medium should be used with great care in patients with advanced renal destruction associated with severe uremia. (See also EXCRETORY UROGRAPHY, precautions).
Acute renal failure has been reported in diabetic patients with diabetic nephropathy and in susceptible nondiabetic patients (often elderly with preexisting renal disease) following excretory urography. Therefore, careful consideration of the potential risks should be given before performing this radiographic procedure in these patients. (See also, EXCRETORY UROGRAPHY, precautions—Preparatory Dehydration.)
Immediately following surgery, excretory urography should be used with caution in renal transplant recipients.
The possibility of an idiosyncratic reaction in susceptible patients should always be considered (see ADVERSE REACTIONS—General). The susceptible population includes patients with a history of a previous reaction to a contrast medium, patients with a known sensitivity to iodine per se, and patients with a known clinical hypersensitivity: bronchial asthma, hay fever, and food allergies.
The occurrence of severe idiosyncratic reactions has prompted the use of several pretesting methods. However, pretesting cannot be relied upon to predict severe reactions and may itself be hazardous for the patient. It is suggested that a thorough medical history with emphasis on allergy and hypersensitivity, prior to injection of any contrast media, may be more accurate than pretesting in predicting potential adverse reactions.
A positive history of allergies or hypersensitivity does not arbitrarily contraindicate the use of a contrast agent, where a diagnostic procedure is thought essential, but caution should be exercised (see ADVERSE REACTIONS—General). Premedication with antihistamines or corticosteroids to avoid or minimize possible allergic reactions in such patients should be considered. Recent reports indicate that such pretreatment does not prevent serious life-threatening reactions, but may reduce both their incidence and severity.
Due to the transitory increase in the circulatory osmotic load, injections of urographic agents should be used with caution in patients with congestive heart failure. Such patients should be observed for several hours following the procedure to detect delayed hemodynamic disturbances.
General anesthesia may be indicated in the performance of some procedures in young or uncooperative children and in selected adult patients; however, a higher incidence of adverse reactions has been reported in these patients, and may be attributable to the inability of the patient to identify untoward symptoms, or to the hypotensive effect of anesthesia which can reduce cardiac output and increase the duration of exposure to the contrast agent.
Seizure activity is rare (about 0.01%) on intravenous injection of ionic contrast media. However, in the higher doses used for CT in patients with brain metastases the incidence can be much higher (1% to 10%). In these patients prophylactic use of a small parenteral dose of diazepam is suggested immediately before injection when extra high dose CT regimens are employed.
In addition to the general precautions already described, excretory urography, cholangiography, and other uses also have hazards associated with the particular techniques employed. (See INDIVIDUAL INDICATIONS AND USAGE section.)
Information for Patients
Patients receiving injectable radiopaque diagnostic agents should be instructed to:
- Inform the physician if they are pregnant (see CLINICAL PHARMACOLOGY).
- Inform the physician if they are diabetic or if they have multiple myeloma, pheochromocytoma, homozygous sickle cell disease or known thyroid disorder (see WARNINGS—General).
- Inform the physician if they are allergic to any drugs, food, or if they have had any reactions to previous injections of dyes used for x-ray procedures (see PRECAUTIONS—General).
- Inform the physician about any other medications they are currently taking, including nonprescription drugs, before they are administered this drug.
Drug Interactions
Renal toxicity has been reported in a few patients with liver dysfunction who were given oral cholecystographic agents followed by urographic agents. Administration of intravascular urographic agents should therefore be postponed in any patient with a known or suspected hepatic or biliary disorder who has recently received a cholecystographic contrast agent.
Addition of an inotropic agent to contrast agents may produce a paradoxical depressant response which can be deleterious to the ischemic myocardium.
Diphenhydramine hydrochloride may cause precipitation when mixed in the same syringe with HYPAQUE meglumine 60%.
Under certain circumstances (pH, temperature, concentrations, time), diatrizoate solutions are incompatible with promethazine hydrochloride, diphenhydramine hydrochloride, brompheniramine maleate, or papaverine hydrochloride solutions.
Do not prefill plastic syringes with HYPAQUE meglumine 60% for prolonged periods (ie, for several hours or longer) before use.
Drug/Laboratory Test Interactions
If any of these studies, which might be affected by contrast media are indicated, it is recommended that they be performed prior to administration of the contrast medium or two or more days afterwards.
Diatrizoate salts interfere with several laboratory urine and blood tests.
Blood Tests
Coagulation: Diatrizoate salts significantly inhibit all stages of coagulation. The fibrinogen concentration, Factors V, VII, and VIII are decreased. Prothrombin time and thromboplastin time are increased.
Platelet aggregation: High levels of plasma diatrizoates inhibit platelet aggregation.
Serum calcium: Diatrizoate salts may decrease serum calcium levels. However, this depletion of serum calcium may also be the result of the addition of chelating agents (edetate disodium) in the preparation of certain contrast media.
Red cell counts: Transitory decreases in red cell counts. Technetium-99m—RBC labeling interference.
Leukocyte counts: Decrease.
Urea nitrogen (BUN): Transitory increase (see CLINICAL PHARMACOLOGY).
Serum creatinine: Transitory increase.
Urine Test
Contrast media which are excreted in the urine, may interfere with some laboratory determinations eg, proteinuria, specific gravity, osmolality, or bacterial cultures.
Thyroid Function Test
Protein-bound iodine (PBI) and total serum organic iodine: Transient increase of both tests following urography have been noticed. The results of PBI and radioactive iodine uptake studies which depend on iodine estimations will not accurately reflect thyroid function for up to 16 days following administration of iodinated urographic media. However, thyroid function tests not depending on iodine estimations, eg, T3 resin uptake or free thyroxine assays are not affected.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term studies in animals have not been performed in order to evaluate carcinogenic potential, mutagenesis, or whether HYPAQUE meglumine 60 percent can affect fertility in males or females.
Pregnancy Category C
Animal reproduction studies have not been conducted with HYPAQUE meglumine 60 percent. It is also not known whether HYPAQUE meglumine 60 percent can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. HYPAQUE meglumine 60 percent should be given to a pregnant woman only if clearly needed. Doses up to 2500 mg/kg in rats, given IV daily, administered during gestation days 6 to 15 revealed no teratogenic abnormalities.
Labor and Delivery
It is not known whether use of these contrast agents during labor or delivery has immediate or delayed adverse effects on the fetus, prolongs the duration of labor or increases the likelihood that forceps delivery or other obstetrical intervention or resuscitation of the newborn will be necessary.
Nursing Mothers
Diatrizoate salts are excreted unchanged in human milk. Because of the potential adverse reactions, although it has not been established that serious adverse reactions occur in nursing infants, caution should be exercised when these intravascular contrast media are administered to a nursing woman.
Pediatric Use
Infants and small children should not have any fluid restriction prior to excretory urography or any other procedures (see PRECAUTIONS—General). Guidelines for pediatric dosages are presented in DOSAGE AND ADMINISTRATION–General.
-
ADVERSE REACTIONS—General
Approximately 95 percent of adverse reactions accompanying the intravascular use of diatrizoate salts are of mild to moderate severity. However, life-threatening reactions and fatalities, mostly of cardiovascular origin, have occurred.
Adverse reactions to injectable contrast media fall into two categories: chemotoxic reactions and idiosyncratic reactions.
Chemotoxic reactions result from the physicochemical properties of the contrast media, the dose, and the speed of injection. All hemodynamic disturbances and injuries to organs or vessels perfused by the contrast medium are included in this category.
Idiosyncratic reactions include all other reactions. They occur more frequently in patients 20 to 40 years old. Idiosyncratic reactions may or may not be dependent on the amount of dose injected, the speed of injection, the mode of injection, and the radiographic procedure. Idiosyncratic reactions are subdivided into minor, intermediate, and severe. The minor reactions are self-limited and of short duration; the severe reactions are life-threatening and treatment is urgent and mandatory.
The reported incidence of adverse reactions to contrast media in patients with a history of allergy are twice that of the general population. Patients with a history of previous reactions to a contrast medium are three times more susceptible than other patients. However, sensitivity to contrast media does not appear to increase with repeated examinations.
Most adverse reactions to injectable contrast media appear within one to three minutes after the start of injection, but delayed reactions may occur.
Adverse reactions are grouped by organ system and listed below by decreasing order of occurrence and with an approximate incidence of occurrence. Significantly more severe reactions are listed before the other reactions regardless of frequency.
Greater Than 1 in 100 Patients
Body as a Whole: Reported incidences of death range from 6.6 per 1 million (0.00066 percent) to 1 in 10,000 patients (0.01 percent). Most deaths occur during injection or 5 to 10 minutes later, the main feature being cardiac arrest with cardiovascular disease as the main aggravating factor.
Isolated reports of hypotensive collapse and shock following urography are found in the literature. The incidence of shock is estimated to occur in 1 out of 20,000 (0.005 percent) patients.
Cardiovascular System: The most frequent adverse reaction to diatrizoate salts is vasodilation (feeling of warmth). The estimated incidence is 49 percent.
Digestive System: Nausea 6 percent, vomiting 3 percent.
Nervous System: Paresthesia 6 percent, dizziness 5 percent.
Respiratory System: Rhinitis 1 percent, increased cough 2 percent.
Skin and Appendages: Urticaria 1 percent.
Pain at the injection site is estimated to occur in about 12 percent of the patients undergoing urography. Pain is usually due to extravasation.
Painful hot erythematous swelling above the venipuncture site was estimated to occur in more than one percent of the patients undergoing phlebography.
Special Senses: Perversion of taste 11 percent.
Urogenital System: Osmotic nephrosis of the proximal tubular cells is estimated to occur in 23 percent of patients following excretory urography.
Less Than 1 in 100 Patients
Other infrequently reported reactions without accompanying incidence rates are listed below, grouped by organ system.
Body as a Whole: Malaria relapse, uremia, high creatinine and BUN (see PRECAUTIONS—General Drug/Laboratory Test Interactions), thrombocytopenia, leukopenia and anemia.
Cardiovascular System: Cerebral hematomas, hemodynamic disturbances, sinus bradycardia, transient electrocardiographic abnormalities, ventricular fibrillation, petechiae, chest pain, cardiac arrest, tachycardia, and cardiorespiratory arrest.
Digestive System: Severe unilateral or bilateral swelling of the parotid and submaxillary glands.
Nervous System: Convulsions, paralysis, coma, speech impairment and severe confusion (see PRECAUTIONS—General).
Respiratory System: Asthma, dyspnea, laryngeal edema, pulmonary edema, bronchospasm, pulmonary embolus and respiratory arrest.
Skin and Appendages: Extravasation necrosis, urticaria with or without pruritus, mucocutaneous edema, and angioneurotic edema.
Special Senses: Bilateral ocular irritation, lacrimation, itching, conjunctival chemosis, infection, conjunctivitis and unilateral blindness.
Urogenital: Renal failure, pain.
-
OVERDOSAGE
At dosage levels of 1 mL/lb, the incidence of unpleasant side effects increases. At total dosage of 2 mL/lb, administered over a short period of time (eg, 30 minutes), clinical signs of systemic intolerance appear (mostly related to hyperosmolar effects) and are manifest as tremors, irritability, and tachycardia. Above these maximal tolerated dosage levels in otherwise healthy adults, an increasing incidence and severity of dyspnea and pulmonary edema should be expected.
Four cases of overdosage in infants, during urography, are reported. Three of the infants died within 19 hours of the injection. The overdose ranged from slightly above the recommended pediatric dosage to a dose exceeding 19 g/kg. The symptoms of overdosage appeared between 10 minutes to several hours after injection of the contrast medium. Adverse effects were life-threatening, affecting mainly the pulmonary and cardiovascular systems. The symptoms included: cyanosis, bradycardia, acidosis, pulmonary hemorrhage, convulsions, coma, and cardiac arrest. All infants showed a poor visualization of the kidneys and a diffuse opacification of all the tissues and vasculature. Autopsy findings showed acute pulmonary damage and/or edema of subcutaneous tissues. Treatment of an overdose of injectable radiopaque contrast media is directed toward the support of all vital functions, and prompt institution of symptomatic therapy.
The acute intravenous LD50 of diatrizoate meglumine in mice is equivalent in iodine content of 5.3 gI/kg to 8.0 gI/kg and seem to be directly proportional to the rate of injection.
Diatrizoate meglumine is dialyzable.
-
DOSAGE AND ADMINISTRATION—General
Preparation of the patient will vary with preference of the radiologist and the type of radiological procedure performed. Specific radiographic procedures used will depend on the state of the patient and the diagnostic indications. Individual dose should be tailored according to age, body size, and indication for examination. (See INDIVIDUAL INDICATIONS AND USAGE section for specific Dosage and Administration.)
Solutions of radiopaque diagnostic agents for intravascular use should be at body temperature when injected and may need to be warmed before use. In the event that crystallization occurs, the solution may be clarified by placing the vial in a water bath at 40°C to 50°C and shaking it gently for two to three minutes or until the solids redissolve. If the particles still persist, do not use this vial but discard it. The solution should be protected from light and any unused portion remaining in the container should be discarded.
Dilution and withdrawal of the contrast agents should be accomplished under aseptic conditions with sterile syringes.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration. Avoid contaminating catheters, syringes, needles, and contrast media with glove powder or cotton fibers.
Pediatric Dosage
Pediatric doses of injectable radiopaque diagnostic agents are generally determined on a weight basis and should be calculated for each patient individually. (See INDIVIDUAL INDICATIONS AND USAGE section.)
Drug Incompatibilities
Diatrizoate salts are incompatible in vitro with some antihistamines and many other drugs. It is believed that one of the chief causes of in vitro incompatibility is an alteration of pH. Turbidity of solutions of intravascular contrast medium occurs between pH 2.5 and 4.1. Another cause is chemical interaction; therefore, other pharmaceuticals should not be mixed with contrast agents in the same syringe.
-
INDIVIDUAL INDICATIONS AND USAGE
THE FOLLOWING SECTIONS FOR INDIVIDUAL INDICATIONS AND USAGE CONTAIN CONTRAINDICATIONS, WARNINGS, PRECAUTIONS, ADVERSE REACTIONS, AND DOSAGE AND ADMINISTRATION SECTIONS RELATED TO THE SPECIFIC PROCEDURES. HOWEVER, IT SHOULD BE UNDERSTOOD THAT THE INFORMATION IN THE GENERAL SECTIONS IS ALSO LIKELY TO APPLY TO ALL OF THESE SPECIFIC USES.
Hydration—With the possible exception of urography, patients should be fully hydrated prior to the following procedures.
EXCRETORY UROGRAPHY
Diatrizoate salts are used in small, medium, and large dose urography (see Dosage and Administration—EXCRETORY UROGRAPHY). Visualization of the urinary tract can be achieved by either direct intravenous injection, intravenous drip infusion, or sometimes by intramuscular or subcutaneous injections, or incidentally following intra-arterial procedure. Visualization of the urinary tract is delayed in infants less than 1 month old, and in patients with urinary tract obstruction (see CLINICAL PHARMACOLOGY).
Precautions
See PRECAUTIONS—General. Some clinicians consider multiple myeloma a contraindication to excretory urography because of the great possibility of producing transient to fatal renal failure. Others believe that the risk of causing anuria is definite but small. If excretory urography is performed in the presence of multiple myeloma, dehydration should be avoided since it favors protein precipitation in renal tubules.
Although azotemia is not considered a contraindication, care is required in patients with advanced renal failure. The usual preparatory dehydration should be omitted, and urinary output should be observed for one to two days in these patients. Adequate visualization may be difficult or impossible to attain in patients with severely impaired renal and/or hepatic function. Use with extreme caution in patients with concomitant hepatorenal disease.
Because of the possibility of temporary suppression of urine, it is wise to allow an interval of at least 48 hours before excretory urography is repeated in patients with unilateral or bilateral reduction of normal renal function. Inadvertent retrograde cystourethrography can cause malignant hyperthermia, disseminated intravascular coagulation and fatality.
Preparatory Dehydration
Preparatory dehydration is dangerous in infants, young children, the elderly, and azotemic patients (especially those with polyuria, oliguria, diabetes, advanced vascular disease, or preexisting dehydration). The undesirable dehydration in these patients may be accentuated by the osmotic diuretic action of the medium.
Dehydration may improve image quality in patients with adequate renal function particularly if a low dose is used. Dehydration, however, will not improve contrast quality in patients with substantial renal insufficiencies and will increase risk of contrast induced renal damage. Dehydration in these patients is therefore contraindicated.
Dosage and Administration
Intravenous Dosage
Adults: A dose of 30 mL to 60 mL produces excellent shadows in the majority of adults subjected to partial dehydration and effective purgation. In persons of slight build, 20 mL produces adequate shadows. For best results and minimal reactions, the total 30 mL to 60 mL should be injected in one to three minutes and compression may be used. A small intravenous test dose may be administered as a possible aid in determining sensitivity to the medium. (See PRECAUTIONS—General.)
Children: The suggested dosage for children up to 12 years old is presented in the table below. Children older than 12 years may be given an adult dose.
Pediatric Dosage for Excretory Urography Age Body Weight Dosage Under 2 years up to 10 lb 5 mL to 10 mL 10 to 30 lb 10 mL to 15 mL 2 to 12 years 30 to 60 lb 15 mL to 30 mL over 60 lb 30 mL Preliminary Preparation of Patient
Although clear shadows are often seen in patients who have had no preliminary preparation for urography, the largest percentage of satisfactory films is obtained in patients who abstain from fluids for 12 to 15 hours before the intravenous injection so that partial dehydration results. (See PRECAUTIONS—General concerning dehydration.) Unless contraindicated, a laxative may be taken at bedtime to eliminate gas from the intestine.
Roentgenographic Technique
A preliminary scout film may be obtained before the intravenous injection. Excellent shadows can often be obtained immediately after administration of the radiopaque medium (within a five-minute period). If preliminary preparation has been carried out, the urinary organs are usually best visualized on films exposed 5, 10, or 15 minutes after intravenous injection. If a film of the bladder is required, it is generally taken 25 or 35 minutes after injection.
In patients with impaired renal function, the best shadows may not be obtainable until later (30 minutes or more) because of delayed excretion, and additional film may have to be exposed.
Most urologists and roentgenologists believe that compression immediately above the symphysis (obtained by application of a small hollow rubber ball about the size of a grapefruit or by the rolled bed sheet technique) assures adequate filling of the pelves and ureters, and hence is of great value. Although compression undoubtedly improves the urogram, it also seems to increase the possibility of pyelorenal backflow or reflux by raising the pressure within the urinary tract.
ANGIOGRAPHY
Precautions
Since serious neurologic complications, including quadriplegia, have occasionally been reported following spinal arteriography or selective injection of arterial trunks providing spinal artery branches (usually the thyrocervical, costocervical, subclavian, vertebral, bronchial, intercostal), great care is necessary to avoid entry of a large concentrated bolus of the medium. Thus, a "pilot" dose may establish correct position of the catheter tip. The concentration of the medium should not be over 60 percent. The carefully individualized dose is usually under 5 mL but preferably 3 mL to 4 mL and the number of repeat injections held to a minimum with appropriate intervals between injections. Pain or muscle spasm during the injection may require reevaluation of the procedure.
Angiography should be avoided whenever possible in patients with homocystinuria, because of the risk of inducing thrombosis and embolism.
CEREBRAL ANGIOGRAPHY
Indication
HYPAQUE meglumine 60 percent may be administered for visualization of the cerebral vessels. In as much as cerebral angiography is a highly specialized procedure requiring the use of special techniques, it is recommended that HYPAQUE meglumine 60 percent be used for this purpose only by persons skilled and experienced in carrying out the procedure.
Contraindication
Carotid angiography during the progressive period of a stroke should be avoided, particularly on the left side because of the increased risk of cerebral complications.
Precautions
See PRECAUTIONS—General. Patients in whom cerebral angiography is to be performed should be selected with care.
Although cerebral angiography has been considered contraindicated in patients who have recently experienced cerebral embolism or thrombosis (stroke syndrome), many experts now believe that the diagnostic value of the procedure, when employed early as an aid in locating lesions amenable to operation, outweighs any added risk to the patient. Furthermore, a small number of postangiographic fatalities have been reported, including progressive thrombosis already clinically evident before angiography, in which the procedure did not appear to play any direct role. Patients with severe cerebrovascular disease should be examined primarily by indirect methods of angiography.
In cerebral angiography, every precaution must be taken to prevent untoward reactions. Reactions may vary directly with the concentration of the substance, the amount used, the speed and frequency of injections, and the interval between injections.
In subarachnoid hemorrhage, angiography is expected to be hazardous. In migraine, the procedure can be hazardous because of ischemic complications, particularly if performed during or soon after an attack.
Adverse Reactions
See ADVERSE REACTIONS—General. With any contrast medium introduced into the cerebral vasculature, neurologic complications, including neuromuscular disorders, seizures, loss of consciousness, hemiplegia, unilateral dysesthesias, visual field defect, language disorders (aphasia), amnesia, and respiratory difficulties may occur, particularly when the extent of the intrinsic lesion is unknown. Such untoward reactions are for the most part temporary, although permanent visual field defects have been reported. Some investigators who are experienced in angiographic procedure emphasize the fact that they tend to occur after repeated injections or higher doses of the contrast medium. Other clinicians find that they occur most frequently in elderly patients. Inasmuch as the procedure itself is attended by technical difficulties regardless of the risk the patient presents (eg, mechanical catheter obstruction of the vertebral artery can cause transient blindness), the more experienced the radiologic team, the fewer the complications of any degree that are apt to arise.
Amaurosis can occur following carotid or especially selective vertebral arteriography. It is almost always transitory (4 to 48 hours).
Dosage and Administration
A dose of 8 mL to 12 mL injected at a rate not exceeding the normal flow in the carotid artery (about 5 mL per second) is suggested. The dose may be repeated as indicated; however, an increased risk attends each repeat injection. Children require a smaller dose in proportion to weight. Light anesthesia may be required in these procedures.
PERIPHERAL ARTERIOGRAPHY AND VENOGRAPHY
Indications
HYPAQUE meglumine 60 percent may be administered for peripheral arteriography and for venography.
Precautions
See PRECAUTIONS—General. Extreme caution is advised in considering peripheral arteriography in patients suspected of having thromboangiitis obliterans (Buergers disease) since any procedure (even insertion of a needle or catheter) may induce a severe arterial or venous spasm. Caution is also advisable in patients with severe ischemia associated with ascending infection.
Adverse Reactions
See ADVERSE REACTIONS—General. Soreness in extremities has also been reported.
Adverse reactions observed during peripheral arteriography may sometimes be due to arterial trauma during the procedure (ie, insertion of needle or catheter, subintimal injection, perforation) as well as to the hypertonicity or effect of the medium. Reported adverse reactions include transient arterial spasm, extravasation, hemorrhage, hematoma formation with tamponade, injury to nerves in close proximity to artery, thrombosis, dissecting aneurysm, arteriovenous fistula (eg, with accidental perforation of femoral artery and vein during the needing), and transient leg pain from contraction of calf muscles in femoral arteriography. Transient hypotension has been reported after intra-arterial (brachial) injection of the medium. Also, brachial plexus injury has been reported with axillary artery injections.
During venography in the presence of venous stasis, inflammatory changes and thrombosis may occur. Thrombosis is rare if the vein is irrigated following the injection.
DIRECT CHOLANGIOGRAPHY
Contraindication
Percutaneous transhepatic cholangiography is contraindicated in patients with coagulation defects and prolonged prothrombin times until normal, or near normal, coagulation is achieved (eg, with vitamin K).
Precautions
In the presence of acute pancreatitis, direct cholangiography, if necessary, should be employed with caution, injecting no more than 5 mL to 10 mL without undue pressure.
Percutaneous transhepatic cholangiography should only be attempted when compatible blood for potential transfusions is in readiness and emergency surgical measures are available. The patient should be carefully monitored for at least 24 hours to insure prompt detection of bile leakage and hemorrhage. Cholespastic premedication, as with morphine, should be avoided. Respiratory movements should be controlled during introduction of the needle.
Adverse Reactions
Adverse reactions may often be attributed to injection pressure or excessive volume of the medium, resulting in overdistention. Such pressure may produce a sensation of epigastric fullness, followed by moderate pain in the back or right upper abdominal quadrant, which will subside when injection is stopped.
Hepatobiliary reflux of the medium may cause a pancholangitis or hepatitis which is usually transitory. Retrograde spread of the infection may produce liver abscess or septicemia. Pancreatic duct reflux may cause a transitory increase in serum amylase for a period of 6 to 18 hours without ill effects. Rarely it may cause pancreatitis.
In percutaneous transhepatic cholangiography, some discomfort is common, but severe pain is unusual. Complications of the procedure are often serious and have been reported in four to six percent of patients. These reactions have included bile leakage and peritonitis, which are more likely to occur in patients with obstructions that cause unrelieved high biliary pressure. Bleeding (sometimes massive with exsanguination) may occur, especially in patients with clotting abnormalities. Blood-bile fistula, manifested by an early urogram (within 2 minutes) has been reported. Hypotension with fever and chills, as manifestations of septicemia, have occurred. Tension pneumothorax, cholangitis, and bacteremia have been reported.
Dosage and Administration
The solution should be warmed to body temperature before administration. The injection is made slowly without undue pressure, taking great care to avoid introducing bubbles.
Operative—If no resistance is encountered, from 10 mL to 15 mL (sometimes up to 25 mL) of a 30 to 60 percent solution is injected or instilled into the cystic duct or common bile duct, as indicated. In patients with obstructive jaundice, 40 mL to 50 mL of the medium may be injected indirectly into the gallbladder after aspiration of its contents.
Postexploratory or completion T tube cholangiography may also be performed after exploration of the common bile duct.
Postoperative—Delayed cholangiograms are usually made from the fifth to the tenth postoperative day prior to removal of the T tube.
Percutaneous transhepatic cholangiography is recommended for carefully selected patients for the differential diagnosis of jaundice due to extrahepatic biliary obstruction or parenchymal disease. The procedure is only employed where oral or intravenous cholangiography and other procedures have failed to provide the necessary information. In obstructive cases, percutaneous transhepatic cholangiography is used to determine the cause and site of the obstruction to help plan surgery. The technique may also be of value in avoiding laparotomy in poor risk jaundice patients since failure to enter a duct suggests hepatocellular disease. Careful attention to technique is essential for the success and safety of the procedure. The procedure is usually performed under local anesthesia following analgesic premedication (eg, 100 mg meperidine intramuscularly).
As the needle is advanced or withdrawn, a bile duct may be located by frequent aspiration for bile or mucus into a syringe filled with normal saline. As much bile as possible is aspirated. The usual dose of HYPAQUE meglumine 60 percent is 20 mL to 40 mL but the range can be from 10 mL to 60 mL depending on degree of biliary dilatation present. The injection may be repeated for exposures in different planes. If a duct is not readily located by aspiration, entry may be established by the injection of successive small doses of 1 mL or 2 mL of the medium under x-ray observation as the needle is withdrawn. If a duct is not located after three or four attempts, the procedure should be abandoned. Inability to enter a duct strongly suggests hepatocellular disease.
SPLENOPORTOGRAPHY
Indication
Splenoportography is usually performed under mild preoperative sedation and under local anesthesia.
Contraindications
Splenoportography should not be performed on any patient for whom splenectomy is contraindicated, since complications of the procedure at times make splenectomy necessary. Other contraindications include prolonged prothrombin time or other coagulation defects, significant thrombocytopenia, and any condition which may increase the possibility of rupture of the spleen.
Precautions
Prior gastrointestinal x-ray examination should include particular attention to the lower esophageal area. A hematologic survey, including prothrombin time and platelet count, should be performed. To minimize risk of bleeding, manipulation during or after entry of the needle should be avoided. Caution is advised in patients whose spleen has recently become tender and palpable.
Following splenoportography, the patient should lie on his left side for several hours and should be closely observed for 24 hours for signs of internal bleeding.
Adverse Reactions
Internal bleeding is the most common serious complication of splenoportography. Although leakage of up to 300 mL of blood is apparently not uncommon, sometimes blood transfusions and, rarely, splenectomy, may be required to control hemorrhage. Peritoneal extravasation may cause transient diaphragmatic irritation or mild to moderate transient pain which may sometimes be referred to the shoulder, the periumbilical region, or other areas. Because of the proximity of the pleural cavity, accidental pneumothorax has been known to occur. Inadvertent injection of the medium into other nearby structures is not likely to cause untoward consequences.
Dosage and Administration
A preliminary small "pilot" dose is injected to confirm splenic entry, followed usually by rapid injection of 20 mL to 25 mL of HYPAQUE meglumine 60 percent. Rapid serial exposures are started with the injection of the dose and continued until contrast is observed in the entire portal system.
ARTHROGRAPHY
Indications
Arthrography may be helpful in the diagnosis of posttraumatic or degenerative joint diseases, synovial rupture, the visualization of communicating bursae or cysts, and in meniscography. However, the technique is of little value unless the arthrograms are interpreted by well-trained personnel.
Precautions
See PRECAUTIONS—General. A strict, aseptic technique is required to avoid introducing infection.
Adverse Reactions
See ADVERSE REACTIONS—General. Injection of HYPAQUE meglumine 60 percent into the joint usually causes immediate but transient discomfort. However, delayed, severe, or persistent pain may occur occasionally. Severe pain often results from undue use of pressure or the injection of large volumes. Joint swelling after injection is rare. Effusion, occasionally requiring aspiration, can occur in patients with rheumatoid arthritis.
Dosage and Administration
The procedure is usually performed with analgesic premedication and under local anesthesia. The amount of HYPAQUE meglumine 60 percent injected depends solely on the capacity of the joint. The damaged joint may require doses greatly exceeding those for normal joints. As much fluid as possible should first be aspirated from the joint; then, the medium should be injected gently to avoid overdistention of the joint capsule. Passive manipulation is sometimes used to disperse the medium in the joint. Sometimes, a 1 mL or 2 mL test dose is injected; immediate pain may indicate extravasation or extracapsular injection which, if confirmed by x-ray, requires relocation of the needle.
A single injection is usually adequate for multiple exposures. Contrast is good during the first 10 minutes after injection, adequate at 10 to 15 minutes, and begins to fade at 15 to 25 minutes.
The following approximate volumes have been used in normal adult joints:
- Knee, shoulder, hip—5 mL to 15 mL
- Temporomandibular—0.5 mL
- Other—1 mL to 4 mL
"Double contrast arthrography," using a mixture of the medium and air or a dilution of HYPAQUE meglumine 60 percent to a 30 percent concentration, has been employed.
DISCOGRAPHY
Indications
Cervical discography is a more hazardous procedure than lumbar discography, and the interpretation of the cervical discograms is more difficult.
The injected medium gradually diffuses throughout the disc and is absorbed rapidly. In a normal disc, good contrast is evident for 10 to 15 minutes. In a ruptured disc, the medium is absorbed more rapidly. Aspiration of the medium on completion of discography is considered unnecessary.
Contraindication
Discography is contraindicated when there is infection or open injury near the region to be examined.
Warning
Inadvertent subarachnoid injection must be avoided since even the small dose of the medium used in discography might result in convulsions and death. The onset of signs of pain, cramps, or convulsions (requiring anesthesia) may occur within minutes to an hour.
Precautions
A strict, aseptic technique is required to avoid introducing infection. The examination should be postponed if local or systemic infection is present. In cervical discography, care should be taken to avoid contamination of the disc by inadvertent puncture of the esophagus. Laceration of the disc by use of a needle that has become barbed by forceful impingement on a vertebra, should be avoided. The patient should be cautioned not to move during introduction of the needle.
Adverse Reactions
In the normal disc, only minor discomfort will occur during injection. More discomfort will result if excessive pressure or volume is used. Pain is unusual and may indicate extravasation.
In the damaged disc, however, the injection can cause pain, sometimes severe, which mimics the symptoms. Transient backache or headache, as in lumbar puncture, often occurs. Extravasation from the disc into the lateral recesses and extradurally into the spinal canal or local soft tissue does not usually cause adverse effects.
During discography extreme care is advised to avoid inadvertent intrathecal injection since the injection of even small amounts of the contrast medium may cause convulsions, permanent sequelae, or fatality. Should the accident occur, the patient should be placed upright to confine the hyperbaric solution to a low level, anesthesia may be required to control convulsions, and if there is evidence of a large dose having been administered, a careful cerebrospinal fluid exchange-washout should be considered.
Dosage and Administration
Discography is usually performed with parenteral analgesia or sedation, and under local anesthesia. To minimize disc and tissue trauma, a two-needle technique is usually employed. An 18 to 20 gauge needle is used to penetrate to the disc and then a very fine (25 or 26 gauge) lumbar puncture-type needle is inserted through the needle to penetrate the disc.
Because of the resistance encountered, it is difficult to inject more than 0.2 mL to 0.3 mL of HYPAQUE meglumine 60 percent into a normal disc. Occasionally, however, a cervical disc can accept up to 0.5 mL and a lumbar disc, 1 mL (rarely, 2 mL) before resistance is encountered. Mild discomfort with little or no frank pain may indicate a normal disc.
In ruptured and some abnormal discs, 1 mL to 2 mL or more can be introduced without resistance; and, particularly if only one disc has pathology, the patient usually experiences pain, sometimes severe, with distribution characteristic of his symptoms. To minimize the amount of HYPAQUE extravasated, no more than 2 mL is injected in any one disc.
The procedure should be planned so that the duration of the discogram allows multiple exposures with a single dose. It has been recommended for diagnostic reasons that the procedure (injection and discogram) be performed on one disc at a time. Injection of a number of discs under suspicion, however, may be performed as part of one procedure.
CONTRAST ENHANCEMENT OF COMPUTED TOMOGRAPHIC HEAD IMAGING
Precautions
Metastatic Brain Lesions: Large doses of contrast media should be avoided in patients with suspected metastatic brain lesions. Intravenous administration of large doses to these patients is more likely to result in convulsions; however, these occurrences are rare. This has been attributed to tissue accumulation of the medium in the presence of blood brain barrier disruption caused by disease. Appropriate measures for seizure management should be immediately available.
Convulsion. (See PRECAUTIONS—General.)
-
HOW SUPPLIED
Vials of 50 mL, rubber stoppered, box of 25 (NDC 0407-0746-04).
Vials of 100 mL, rubber stoppered, box of 10 (NDC 0407-0747-02).
Box of 10 calibrated 200 mL dilution bottles with hangers containing 150 mL HYPAQUE meglumine 60%; rubber stoppered (NDC 0407-0749-20).
Box of 10 calibrated 200 mL dilution bottles with hangers containing 200 mL HYPAQUE meglumine 60%; rubber stoppered (NDC 0407-0750-10).
Protect from light. Store at 15°C to 30°C (59° F to 86°F).
- SPL UNCLASSIFIED SECTION
-
INGREDIENTS AND APPEARANCE
HYPAQUE SODIUM
diatrizoate meglumine injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:0407-0746 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Diatrizoate Meglumine (UNII: 3X9MR4N98U) (diatrizoic acid - UNII:5UVC90J1LK) 60 g in 100 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:0407-0746-04 25 in 1 BOX 1 50 mL in 1 VIAL HYPAQUE SODIUM
diatrizoate meglumine injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:0407-0747 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Diatrizoate Meglumine (UNII: 3X9MR4N98U) (diatrizoic acid - UNII:5UVC90J1LK) 60 g in 100 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:0407-0747-02 10 in 1 BOX 1 100 mL in 1 VIAL HYPAQUE SODIUM
diatrizoate meglumine injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:0407-0749 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Diatrizoate Meglumine (UNII: 3X9MR4N98U) (diatrizoic acid - UNII:5UVC90J1LK) 60 g in 100 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:0407-0749-20 10 in 1 BOX 1 150 mL in 1 BOTTLE HYPAQUE SODIUM
diatrizoate meglumine injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:0407-0750 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Diatrizoate Meglumine (UNII: 3X9MR4N98U) (diatrizoic acid - UNII:5UVC90J1LK) 60 g in 100 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:0407-0750-10 10 in 1 BOX 1 200 mL in 1 BOTTLE Labeler - Amersham Health Inc.