Label: PIFELTRO- doravirine tablet, film coated

- NDC Code(s): 50090-6237-0
- Packager: A-S Medication Solutions
- This is a repackaged label.
- Source NDC Code(s): 0006-3069
- Category: HUMAN PRESCRIPTION DRUG LABEL
Drug Label Information
Updated October 31, 2023
If you are a healthcare professional or from the pharmaceutical industry please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use PIFELTRO safely and effectively. See full prescribing information for PIFELTRO.
PIFELTRO™ (doravirine) tablets, for oral use
Initial U.S. Approval: 2018RECENT MAJOR CHANGES
INDICATIONS AND USAGE
PIFELTRO, a non-nucleoside reverse transcriptase inhibitor (NNRTI), is indicated in combination with other antiretroviral agents for the treatment of HIV-1 infection in adults and pediatric patients weighing at least 35 kg:
- with no prior antiretroviral treatment history, OR
- to replace the current antiretroviral regimen in those who are virologically-suppressed (HIV-1 RNA less than 50 copies per mL) on a stable antiretroviral regimen with no history of treatment failure and no known substitutions associated with resistance to doravirine. (1)
DOSAGE AND ADMINISTRATION
DOSAGE FORMS AND STRENGTHS
- Tablets: 100 mg doravirine. (3)
CONTRAINDICATIONS
- PIFELTRO is contraindicated when co-administered with drugs that are strong cytochrome P450 (CYP)3A enzyme inducers as significant decreases in doravirine plasma concentrations may occur, which may decrease the effectiveness of PIFELTRO. (4)
WARNINGS AND PRECAUTIONS
- Monitor for Immune Reconstitution Syndrome. (5.2)
ADVERSE REACTIONS
Most common adverse reactions (incidence greater than or equal to 5%, all grades) are nausea, dizziness, headache, fatigue, diarrhea, abdominal pain, and abnormal dreams. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Merck Sharp & Dohme LLC at 1-877-888-4231 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch .
DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 10/2023
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage
2.2 Dosage Adjustment with Rifabutin
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Risk of Adverse Reactions or Loss of Virologic Response Due to Drug Interactions
5.2 Immune Reconstitution Syndrome
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
7 DRUG INTERACTIONS
7.1 Effect of Other Drugs on PIFELTRO
7.2 Effect of PIFELTRO on Other Drugs
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Renal Impairment
8.7 Hepatic Impairment
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
12.4 Microbiology
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
14.1 Clinical Trial Results in Adults with No Antiretroviral Treatment History
14.2 Clinical Trial Results in Virologically-Suppressed Adults
14.3 Clinical Trial Results in Pediatric Patients
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
PIFELTRO™ is indicated in combination with other antiretroviral agents for the treatment of HIV-1 infection in adults and pediatric patients weighing at least 35 kg:
- with no prior antiretroviral treatment history; OR
- to replace the current antiretroviral regimen in those who are virologically-suppressed (HIV-1 RNA less than 50 copies per mL) on a stable antiretroviral regimen with no history of treatment failure and no known substitutions associated with resistance to doravirine [see Clinical Studies (14)].
-
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage
The recommended dosage regimen of PIFELTRO in adults and pediatric patients weighing at least 35 kg is one 100 mg tablet taken orally once daily with or without food [see Clinical Pharmacology (12.3)].
2.2 Dosage Adjustment with Rifabutin
If PIFELTRO is co-administered with rifabutin, increase PIFELTRO dosage to one tablet twice daily (approximately 12 hours apart) for the duration of rifabutin co-administration [see Drug Interactions (7.1) and Clinical Pharmacology (12.3)].
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
PIFELTRO is contraindicated when co-administered with drugs that are strong cytochrome P450 (CYP)3A enzyme inducers as significant decreases in doravirine plasma concentrations may occur, which may decrease the effectiveness of PIFELTRO [see Warnings and Precautions (5.1), Drug Interactions (7.1), and Clinical Pharmacology (12.3)]. These drugs include, but are not limited to, the following:
- the anticonvulsants carbamazepine, oxcarbazepine, phenobarbital, phenytoin
- the androgen receptor inhibitor enzalutamide
- the antimycobacterials rifampin, rifapentine
- the cytotoxic agent mitotane
- St. John's wort (Hypericum perforatum)
-
5 WARNINGS AND PRECAUTIONS
5.1 Risk of Adverse Reactions or Loss of Virologic Response Due to Drug Interactions
The concomitant use of PIFELTRO and certain other drugs may result in known or potentially significant drug interactions, some of which may lead to loss of therapeutic effect of PIFELTRO and possible development of resistance [see Dosage and Administration (2.2), Contraindications (4) and Drug Interactions (7.1)].
See Table 6 for steps to prevent or manage these possible and known significant drug interactions, including dosing recommendations. Consider the potential for drug interactions prior to and during PIFELTRO therapy, review concomitant medications during PIFELTRO therapy, and monitor for adverse reactions.
5.2 Immune Reconstitution Syndrome
Immune reconstitution syndrome has been reported in patients treated with combination antiretroviral therapy. During the initial phase of combination antiretroviral treatment, patients whose immune system responds may develop an inflammatory response to indolent or residual opportunistic infections (such as Mycobacterium avium infection, cytomegalovirus, Pneumocystis jirovecii pneumonia (PCP), or tuberculosis), which may necessitate further evaluation and treatment.
Autoimmune disorders (such as Graves' disease, polymyositis, Guillain-Barré syndrome, and autoimmune hepatitis) have also been reported to occur in the setting of immune reconstitution; however, the time to onset is more variable and can occur many months after initiation of treatment.
-
6 ADVERSE REACTIONS
The following adverse reactions are discussed in other sections of the labeling:
- Immune Reconstitution Syndrome [see Warnings and Precautions (5.2)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Adverse Reactions in Adults with No Antiretroviral Treatment History
The safety assessment of PIFELTRO used in combination with other antiretroviral agents is based on Week 96 data from two Phase 3, randomized, international, multicenter, double-blind, active-controlled trials (DRIVE-FORWARD (Protocol 018) and DRIVE-AHEAD (Protocol 021)).
In DRIVE-FORWARD, 766 adult subjects received either PIFELTRO 100 mg (n=383) or darunavir 800 mg + ritonavir 100 mg (DRV+r) (n=383) once daily, each in combination with emtricitabine/tenofovir disoproxil fumarate (FTC/TDF) or abacavir/lamivudine (ABC/3TC). By Week 96, 2% in the PIFELTRO group and 3% in the DRV+r group had adverse events leading to discontinuation of study medication.
In DRIVE-AHEAD, 728 adult subjects received either DELSTRIGO [doravirine (DOR)/3TC/TDF] (n=364) or efavirenz (EFV)/FTC/TDF once daily (n=364). By Week 96, 3% in the DELSTRIGO group and 7% in the EFV/FTC/TDF group had adverse events leading to discontinuation of study medication.
Adverse reactions reported in greater than or equal to 5% of subjects in any treatment group in DRIVE-FORWARD and DRIVE-AHEAD are presented in Table 1.
Table 1: Adverse Reactions* (All Grades) Reported in ≥5%† of Subjects in Any Treatment Group in Adults with No Antiretroviral Treatment History in DRIVE-FORWARD and DRIVE-AHEAD (Week 96) DRIVE-FORWARD DRIVE-AHEAD PIFELTRO+2 NRTIs‡
Once Daily
N=383DRV+r+2 NRTIs‡
Once Daily
N=383DELSTRIGO
Once Daily
N=364EFV/FTC/TDF
Once Daily
N=364NRTIs = FTC/TDF or ABC/3TC.
Fatigue: includes fatigue, asthenia, malaise
Abdominal Pain: includes abdominal discomfort, abdominal pain, abdominal pain lower, abdominal pain upper, epigastric discomfort
Rash: includes rash, rash erythematous, rash generalized, rash macular, rash maculo-papular, rash papular, rash pruritic, rash pustularNausea 7% 8% 5% 7% Headache 6% 3% 4% 5% Fatigue 6% 3% 4% 4% Diarrhea 6% 13% 4% 6% Abdominal Pain 5% 2% 1% 2% Dizziness 3% 2% 7% 32% Rash 2% 3% 2% 12% Abnormal Dreams 1% <1% 5% 10% Insomnia 1% 2% 4% 5% Somnolence 0% <1% 3% 7% The majority (77%) of adverse reactions associated with doravirine occurred at severity Grade 1 (mild).
Neuropsychiatric Adverse Events
For DRIVE-AHEAD, the analysis of subjects with neuropsychiatric adverse events by Week 48 is presented in Table 2. The proportion of subjects who reported one or more neuropsychiatric adverse events was 24% and 57% in the DELSTRIGO and EFV/FTC/TDF groups, respectively.
A statistically significantly lower proportion of DELSTRIGO-treated subjects compared to EFV/FTC/TDF-treated subjects reported neuropsychiatric adverse events by Week 48 in the three pre-specified categories of dizziness, sleep disorders and disturbances, and altered sensorium.
Table 2: DRIVE-AHEAD - Analysis of Subjects with Neuropsychiatric Adverse Events* (Week 48) DELSTRIGO
Once Daily
N=364EFV/FTC/TDF
Once Daily
N=364Treatment Difference
DELSTRIGO - EFV/FTC/TDF
Estimate (95% CI)†- *
- All causality and all grade events were included in the analysis.
- †
- The 95% CIs were calculated using Miettinen and Nurminen's method. Categories pre-specified for statistical testing were dizziness (p <0.001), sleep disorders and disturbances (p <0.001), and altered sensorium (p=0.033).
- ‡
- Predefined using MedDRA preferred terms, including: abnormal dreams, hyposomnia, initial insomnia, insomnia, nightmare, sleep disorder, somnambulism.
- §
- Predefined using MedDRA preferred terms, including: altered state of consciousness, lethargy, somnolence, syncope.
Sleep disorders and disturbances‡ 12% 26% -13.5 (-19.1, -7.9) Dizziness 9% 37% -28.3 (-34.0, -22.5) Altered sensorium§ 4% 8% -3.8 (-7.6, -0.3) Neuropsychiatric adverse events in the pre-defined category of depression and suicide/self-injury were reported in 4% and 7% of subjects, in the DELSTRIGO and EFV/FTC/TDF groups, respectively.
In DRIVE-AHEAD through 48 weeks of treatment, the majority of subjects who reported neuropsychiatric adverse events reported events that were mild to moderate in severity (97% [83/86] and 96% [198/207], in the DELSTRIGO and EFV/FTC/TDF groups, respectively) and the majority of subjects reported these events in the first 4 weeks of treatment (72% [62/86] in the DELSTRIGO group and 86% [177/207] in the EFV/FTC/TDF group).
Neuropsychiatric adverse events led to treatment discontinuation in 1% (2/364) and 1% (5/364) of subjects in the DELSTRIGO and EFV/FTC/TDF groups, respectively. The proportion of subjects who reported neuropsychiatric adverse events through Week 4 was 17% (62/364) in the DELSTRIGO group and 49% (177/364) in the EFV/FTC/TDF group. At Week 48, the prevalence of neuropsychiatric adverse events was 12% (44/364) in the DELSTRIGO group and 22% (81/364) in the EFV/FTC/TDF group. At Week 96, the prevalence of neuropsychiatric adverse events was 13% (47/364) in the DELSTRIGO group and 23% (82/364) in the EFV/FTC/TDF group.
Laboratory Abnormalities
The percentages of subjects with selected laboratory abnormalities (that represent a worsening from baseline) who were treated with PIFELTRO or DRV+r in DRIVE-FORWARD, or DELSTRIGO or EFV/FTC/TDF in DRIVE-AHEAD are presented in Table 3.
Table 3: Selected Laboratory Abnormalities Reported in Adult Subjects with No Antiretroviral Treatment History in DRIVE-FORWARD and DRIVE-AHEAD (Week 96) DRIVE-FORWARD DRIVE-AHEAD Laboratory Parameter Preferred Term (Unit)/Limit PIFELTRO+2 NRTIs
Once Daily
N=383DRV+r+2 NRTIs
Once Daily
N=383DELSTRIGO
Once Daily
N=364EFV/FTC/TDF
Once Daily
N=364Blood Chemistry Each subject is only counted once per parameter at the highest toxicity grade. Only subjects with a baseline value and at least one on-treatment value for a given laboratory parameter are included.
ULN = Upper limit of normal range.
Note: NRTIs = FTC/TDF or ABC/3TC.Total bilirubin 1.1 - < 1.6 × ULN 6% 2% 5% 0% 1.6 - <2.6 × ULN 2% <1% 2% 0% ≥2.6 × ULN <1% 0% 1% <1% Creatinine (mg/dL) >1.3 - 1.8 × ULN or Increase of >0.3 mg/dL above baseline 4% 6% 3% 2% >1.8 × ULN or Increase of ≥1.5 × above baseline 4% 4% 3% 2% Aspartate aminotransferase (IU/L) 2.5 - <5.0 × ULN 5% 4% 3% 3% ≥5.0 × ULN 2% 2% 1% 4% Alanine aminotransferase (IU/L) 2.5 - <5.0 × ULN 4% 2% 4% 4% ≥5.0 × ULN 2% 3% 1% 3% Alkaline phosphatase (IU/L) 2.5 - <5.0 × ULN <1% 1% <1% 1% ≥5.0 × ULN 0% <1% 0% <1% Lipase 1.5 - <3.0 × ULN 7% 6% 6% 4% ≥3.0 × ULN 3% 4% 2% 3% Creatine kinase (IU/L) 6.0 - <10.0 × ULN 3% 3% 3% 3% ≥10.0 × ULN 5% 6% 4% 6% Cholesterol, fasted (mg/dL) ≥300 mg/dL 0% 1% 1% <1% LDL cholesterol, fasted (mg/dL) ≥190 mg/dL <1% 4% <1% 2% Triglycerides, fasted (mg/dL) >500 mg/dL 1% 2% 1% 3% Change in Lipids from Baseline
For DRIVE-FORWARD and DRIVE-AHEAD, changes from baseline at Week 48 in LDL-cholesterol, non-HDL-cholesterol, total cholesterol, triglycerides, and HDL-cholesterol are shown in Table 4. Changes from baseline at Week 96 were similar to those seen at Week 48.
The LDL and non-HDL comparisons were pre-specified and are summarized in Table 4. The differences were statistically significant, showing superiority for doravirine for both parameters. The clinical benefit of these findings has not been demonstrated.
Table 4: Mean Change from Baseline in Fasting Lipids in Adult Subjects with No Antiretroviral Treatment History in DRIVE-FORWARD and DRIVE-AHEAD (Week 48) Subjects on lipid-lowering agents at baseline were excluded from these analyses (in DRIVE-FORWARD: PIFELTRO n=12 and DRV+r n=14; in DRIVE-AHEAD: DELSTRIGO n=15 and EFV/FTC/TDF n=10). Subjects initiating a lipid-lowering agent post-baseline had their last fasted on-treatment value (prior to starting the agent) carried forward (in DRIVE-FORWARD: PIFELTRO n=6 and DRV+r n=4; in DRIVE-AHEAD: DELSTRIGO n=3 and EFV/FTC/TDF n=8). DRIVE-FORWARD PIFELTRO+2 NRTIs
Once Daily
N=320DRV+r+2 NRTIs
Once Daily
N=311Laboratory Parameter Preferred Term Baseline Change Baseline Change Difference Estimates (95% CI) LDL-Cholesterol (mg/dL)* 91.4 -4.6 92.3 9.5 -14.4 (-18.0, -10.8) Non-HDL Cholesterol (mg/dL)* 113.6 -5.4 114.5 13.7 -19.4 (-23.4, -15.4) Total Cholesterol (mg/dL)† 157.2 -1.4 157.8 18.0 - Triglycerides (mg/dL)† 111.0 -3.1 113.7 24.5 - HDL-Cholesterol (mg/dL)† 43.6 4.0 43.3 4.3 - DRIVE-AHEAD DELSTRIGO Once Daily
N=320EFV/FTC/TDF Once Daily
N=307Laboratory Parameter Preferred Term Baseline Change Baseline Change Difference Estimates (95% CI) LDL-Cholesterol (mg/dL)* 91.7 -2.1 91.3 8.3 -10.2 (-13.8, -6.7) Non-HDL Cholesterol (mg/dL)* 114.7 -4.1 115.3 12.7 -16.9 (-20.8, -13.0) Total Cholesterol (mg/dL)† 156.8 -2.2 156.8 21.1 - Triglycerides (mg/dL)† 118.7 -12.0 122.6 21.6 - HDL-Cholesterol (mg/dL)† 42.1 1.8 41.6 8.4 - Adverse Reactions in Virologically-Suppressed Adults
The safety of DELSTRIGO in virologically-suppressed adults was based on Week 48 data from 670 subjects in the DRIVE-SHIFT trial (Protocol 024), a randomized, international, multicenter, open-label trial in which virologically-suppressed subjects were switched from a baseline regimen consisting of two NRTIs in combination with a protease inhibitor (PI) plus either ritonavir or cobicistat, or elvitegravir plus cobicistat, or a non-nucleoside reverse transcriptase inhibitor (NNRTI) to DELSTRIGO. Overall, the safety profile in virologically-suppressed adult subjects was similar to that in subjects with no antiretroviral treatment history.
Laboratory Abnormalities
Serum ALT and AST Elevations: In the DRIVE-SHIFT trial, 22% and 16% of subjects in the immediate switch group experienced ALT and AST elevations greater than 1.25 × ULN, respectively, through 48 weeks on DELSTRIGO. For these ALT and AST elevations, no apparent patterns with regard to time to onset relative to switch were observed. One percent of subjects had ALT or AST elevations greater than 5 × ULN through 48 weeks on DELSTRIGO. The ALT and AST elevations were generally asymptomatic and not associated with bilirubin elevations. In comparison, 4% and 4% of subjects in the delayed switch group experienced ALT and AST elevations of greater than 1.25 × ULN through 24 weeks on their baseline regimen.
Change in Lipids from Baseline
Changes from baseline at Week 24 in LDL-cholesterol, non-HDL-cholesterol, total cholesterol, triglycerides, and HDL-cholesterol in subjects on a PI plus ritonavir-based regimen at baseline are shown in Table 5. The LDL and non-HDL comparisons were pre-specified, and the differences were statistically significant, showing superiority for an immediate switch to DELSTRIGO for both parameters. The clinical benefit of these findings has not been demonstrated.
Table 5: Mean Change from Baseline in Fasting Lipids in Adult Virologically-Suppressed Subjects on a PI plus Ritonavir-based Regimen at Baseline in DRIVE-SHIFT (Week 24) Laboratory Parameter Preferred Term DELSTRIGO
(Week 0-24)
Once Daily
N=244PI+ritonavir
(Week 0-24)
Once Daily
N=124Difference Estimates Baseline Change Baseline Change Difference (95% CI) Subjects on lipid-lowering agents at baseline were excluded from these analyses (DELSTRIGO n=26 and PI+ritonavir n=13). Subjects initiating a lipid-lowering agent post-baseline had their last fasted on-treatment value (prior to starting the agent) carried forward (DELSTRIGO n=4 and PI+ritonavir n=2). LDL-Cholesterol (mg/dL)* 108.7 -16.3 110.5 -2.6 -14.5 (-18.9, -10.1) Non-HDL Cholesterol (mg/dL)* 138.6 -24.8 138.8 -2.1 -22.8 (-27.9, -17.7) Total Cholesterol (mg/dL)† 188.5 -26.1 187.4 -0.2 - Triglycerides (mg/dL)† 153.1 -44.4 151.4 -0.4 - HDL-Cholesterol (mg/dL)† 50.0 -1.3 48.5 1.9 - Adverse Reactions in Pediatric Patients
The safety of doravirine as a component of DELSTRIGO was evaluated in 45 HIV-1-infected virologically-suppressed or treatment-naïve pediatric patients 12 to less than 18 years of age through Week 24 in an open-label trial (IMPAACT 2014 (Protocol 027)) [see Clinical Studies (14.3)]. The safety profile in pediatric subjects was similar to that in adults. There were no serious or Grade 3 or 4 adverse reactions. No subjects discontinued due to an adverse event.
-
7 DRUG INTERACTIONS
7.1 Effect of Other Drugs on PIFELTRO
Co-administration of PIFELTRO with a CYP3A inducer decreases doravirine plasma concentrations, which may reduce PIFELTRO efficacy [see Contraindications (4), Warnings and Precautions (5.1), and Clinical Pharmacology (12.3)]. Co-administration of PIFELTRO and drugs that are inhibitors of CYP3A may result in increased plasma concentrations of doravirine.
Table 6 shows significant drug interactions with PIFELTRO.
Table 6: Drug Interactions with PIFELTRO* Concomitant Drug Class:
Drug NameEffect on Concentration Clinical Comment ↑ = increase, ↓ = decrease
All other drug-drug interactions shown are anticipated based on the known metabolic and elimination pathways.Androgen Receptors enzalutamide ↓ doravirine Co-administration is contraindicated with enzalutamide.
At least a 4-week cessation period is recommended prior to initiation of PIFELTRO.Anticonvulsants carbamazepine
oxcarbazepine
phenobarbital
phenytoin↓ doravirine Co-administration is contraindicated with these anticonvulsants.
At least a 4-week cessation period is recommended prior to initiation of PIFELTRO.Antimycobacterials rifampin†
rifapentine↓ doravirine Co-administration is contraindicated with rifampin or rifapentine.
At least a 4-week cessation period is recommended prior to initiation of PIFELTRO.rifabutin† ↓ doravirine Increase PIFELTRO dosage to one tablet twice daily when co-administered with rifabutin [see Dosage and Administration (2.2)]. Cytotoxic Agents mitotane ↓ doravirine Co-administration is contraindicated with mitotane.
At least a 4-week cessation period is recommended prior to initiation of PIFELTRO.HIV Antiviral Agents efavirenz†
etravirine
nevirapine↓ doravirine Use with efavirenz, etravirine, or nevirapine is not recommended. Herbal Products St. John's wort ↓ doravirine Co-administration is contraindicated with St. John's wort.
At least a 4-week cessation period is recommended prior to initiation of PIFELTRO.No clinically significant changes in concentration were observed for doravirine when co-administered with the following agents: dolutegravir, TDF, lamivudine, elbasvir and grazoprevir, ledipasvir and sofosbuvir, ritonavir, ketoconazole, aluminum hydroxide/magnesium hydroxide/simethicone containing antacid, pantoprazole, and methadone [see Clinical Pharmacology (12.3)].
7.2 Effect of PIFELTRO on Other Drugs
No clinically significant changes in concentration were observed for the following agents when co-administered with doravirine: dolutegravir, lamivudine, TDF, elbasvir and grazoprevir, ledipasvir and sofosbuvir, atorvastatin, an oral contraceptive containing ethinyl estradiol and levonorgestrel, metformin, methadone, and midazolam [see Clinical Pharmacology (12.3)].
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in individuals exposed to PIFELTRO during pregnancy. Healthcare providers are encouraged to register patients by calling the Antiretroviral Pregnancy Registry (APR) at 1-800-258-4263.
Risk Summary
No adequate human data are available to establish whether or not PIFELTRO poses a risk to pregnancy outcomes. In animal reproduction studies, no adverse developmental effects were observed when doravirine was administered at exposures ≥8 times the exposure in humans at the recommended human dose (RHD) of PIFELTRO (see Data).
The background rate of major birth defects is 2.7% in a U.S. reference population of the Metropolitan Atlanta Congenital Defects Program (MACDP). The rate of miscarriage is not reported in the APR. The estimated background rate of miscarriage in the clinically recognized pregnancies in the U.S. general population is 15-20%. Methodological limitations of the APR include the use of MACDP as the external comparator group. The MACDP population is not disease-specific, evaluates individuals and infants from the limited geographic area, and does not include outcomes for births that occurred at less than 20 weeks gestation.
Data
Animal Data
Doravirine was administered orally to pregnant rabbits (up to 300 mg/kg/day on gestation days (GD) 7 to 20) and rats (up to 450 mg/kg/day on GD 6 to 20 and separately from GD 6 to lactation/postpartum day 20). No significant toxicological effects on embryo-fetal (rats and rabbits) or pre/post-natal (rats) development were observed at exposures (AUC) approximately 9 times (rats) and 8 times (rabbits) the exposure in humans at the RHD. Doravirine was transferred to the fetus through the placenta in embryo-fetal studies, with fetal plasma concentrations of up to 40% (rabbits) and 52% (rats) that of maternal concentrations observed on gestation day 20.
8.2 Lactation
Risk Summary
The Centers for Disease Control and Prevention recommend that HIV-1-infected mothers in the United States not breastfeed their infants to avoid risking potential transmission of HIV-1 infection.
It is unknown whether doravirine is present in human milk, affects human milk production, or has effects on the breastfed infant. Doravirine is present in the milk of lactating rats (see Data). Because of the potential for (1) HIV-1 transmission (in HIV-negative infants), (2) developing viral resistance (in HIV-positive infants), and (3) serious adverse reactions in a breastfed infant, instruct mothers not to breastfeed if they are receiving PIFELTRO.
8.4 Pediatric Use
The safety and efficacy of PIFELTRO for the treatment of HIV-1 infection have been established in pediatric patients weighing at least 35 kg [see Indications and Usage (1) and Dosage and Administration (2.1)].
Use of PIFELTRO in this group is supported by evidence from adequate and well-controlled trials in adults and an open-label trial in virologically-suppressed or treatment-naïve pediatric subjects 12 to less than 18 years of age. The safety, efficacy, and exposure of doravirine in these pediatric subjects were similar to that in adults. [see Adverse Reactions (6.1), Clinical Pharmacology (12.3), and Clinical Studies (14.3).]
Safety and efficacy of PIFELTRO in pediatric patients weighing less than 35 kg have not been established.
8.5 Geriatric Use
Clinical trials of PIFELTRO did not include sufficient numbers of subjects aged 65 years and over to determine whether they respond differently from younger subjects. In general, caution should be exercised in the administration of PIFELTRO in elderly patients, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy [see Clinical Pharmacology (12.3)].
8.6 Renal Impairment
No dosage adjustment of PIFELTRO is required in patients with mild, moderate, or severe renal impairment. PIFELTRO has not been adequately studied in patients with end-stage renal disease and has not been studied in dialysis patients [see Clinical Pharmacology (12.3)].
8.7 Hepatic Impairment
No dosage adjustment of PIFELTRO is required in patients with mild (Child-Pugh Class A) or moderate (Child-Pugh Class B) hepatic impairment. PIFELTRO has not been studied in patients with severe hepatic impairment (Child-Pugh Class C) [see Clinical Pharmacology (12.3)].
-
11 DESCRIPTION
PIFELTRO is a film-coated tablet containing doravirine for oral administration.
Doravirine is an HIV-1 non-nucleoside reverse transcriptase inhibitor (NNRTI).
Each tablet contains 100 mg of doravirine as the active ingredient. The tablets include the following inactive ingredients: colloidal silicon dioxide, croscarmellose sodium, hypromellose acetate succinate, lactose monohydrate, magnesium stearate, and microcrystalline cellulose. The tablets are film coated with a coating material containing the following inactive ingredients: hypromellose, lactose monohydrate, titanium dioxide, and triacetin. The coated tablets are polished with carnauba wax.
The chemical name for doravirine is 3-chloro-5-[[1-[(4,5-dihydro-4-methyl-5-oxo-1H-1,2,4-triazol-3-yl)methyl]-1,2-dihydro-2-oxo-4-(trifluoromethyl)-3-pyridinyl]oxy]benzonitrile.
It has a molecular formula of C17H11ClF3N5O3 and a molecular weight of 425.75.
It has the following structural formula:
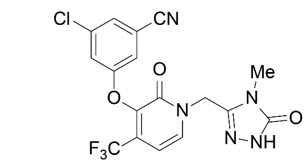
Doravirine is practically insoluble in water.
-
12 CLINICAL PHARMACOLOGY
12.2 Pharmacodynamics
In a Phase 2 trial evaluating doravirine over a dose range of 0.25 to 2 times the recommended dose of PIFELTRO, (in combination with FTC/TDF) in HIV-1-infected subjects with no antiretroviral treatment history, no exposure-response relationship for efficacy was identified for doravirine.
12.3 Pharmacokinetics
Doravirine pharmacokinetics are similar in healthy subjects and HIV-1-infected subjects. Doravirine pharmacokinetics are provided in Table 7.
Table 7: Pharmacokinetic Properties of Doravirine Parameter Doravirine Abbreviations: AUC=area under the time concentration curve; Cmax=maximum concentration; C24=concentration at 24 hours; Tmax time to Cmax; Vdss= volume of distribution at steady state, t1/2=elimination half-life; CL/F=apparent clearance; CLrenal=apparent renal clearance - *
- Doravirine 100 mg once daily to HIV-1-infected subjects
- †
- Presented as geometric mean (%CV: geometric coefficient of variation)
- ‡
- Geometric mean ratio [high-fat meal/fasting] and (90% confidence interval) for PK parameters. High fat meal is approximately 1,000 kcal, 50% fat. The effect of food is not clinically relevant.
- §
- Based on IV dose
General Steady State Exposure*,† AUC0-24
(mcg∙h/mL)16.1 (29) Cmax
(mcg/mL)0.962 (19) C24
(mcg/mL)0.396 (63) Time to Steady State (Days) 2 Accumulation Ratio 1.2 to 1.4 Absorption Absolute Bioavailability 64% Tmax (h) 2 Effect of Food‡ AUC Ratio 1.16 (1.06, 1.26) Cmax Ratio 1.03 (0.89, 1.19) C24 Ratio 1.36 (1.19, 1.55) Distribution Vdss (L)§ 60.5 Plasma Protein Binding 76% Elimination t1/2 (h) 15 CL/F (mL/min)† 106 (35.2) CLrenal (mL/min)† 9.3 (18.6) Metabolism Primary Pathway(s) CYP3A Excretion Major Route of Elimination Metabolism Urine (unchanged) 6% Biliary/Fecal (unchanged) Minor Specific Populations
In adults, no clinically significant difference on the pharmacokinetics of doravirine were observed based on age (18 to 78 years of age), sex, and race/ethnicity, mild to severe renal impairment (creatinine clearance (CLcr) >15 mL/min, estimated by Cockcroft-Gault), or moderate hepatic impairment (Child-Pugh B). The pharmacokinetics of doravirine in patients with end-stage renal disease or undergoing dialysis, or severe hepatic impairment (Child-Pugh C) is unknown.
Patients with Renal Impairment
In a study comparing 8 subjects with severe renal impairment to 8 subjects without renal impairment, the single dose exposure of doravirine was 43% higher in subjects with severe renal impairment. In a population pharmacokinetic analysis, renal function did not have a clinically relevant effect on doravirine pharmacokinetics. Doravirine has not been studied in patients with end-stage renal disease or in patients undergoing dialysis [see Use in Specific Populations (8.6)].
Patients with Hepatic Impairment
No clinically significant difference in the pharmacokinetics of doravirine was observed in subjects with moderate hepatic impairment (Child-Pugh score B) compared to subjects without hepatic impairment. Doravirine has not been studied in subjects with severe hepatic impairment (Child-Pugh score C) [see Use in Specific Populations (8.7)].
Pediatric Patients
Mean doravirine exposures were similar in 54 pediatric patients aged 12 to less than 18 years and weighing at least 35 kg who received doravirine or DELSTRIGO in IMPAACT 2014 (Protocol 027) relative to adults following administration of doravirine or DELSTRIGO (Table 8). For pediatric patients weighing ≥ 35 kg and < 45 kg who receive doravirine 100 mg or DELSTRIGO, the population pharmacokinetic model-predicted mean C24 of doravirine was comparable to that achieved in adults, whereas mean AUC0-24 and Cmax of doravirine were 25% and 36% higher than adult values, respectively. However, the predicted AUC0-24 and Cmax increases are not considered clinically significant.
Table 8: Steady State Pharmacokinetics for Doravirine Following Administration of Doravirine or DELSTRIGO in HIV-1-Infected Pediatric Patients Aged 12 to Less than 18 Years and Weighing at Least 35 kg Parameter* Doravirine† Abbreviations: AUC=area under the time concentration curve; Cmax=maximum concentration; C24=concentration at 24 hours AUC0-24
(mcg∙h/mL)16.4 (24) Cmax
(mcg/mL)1.03 (16) C24
(mcg/mL)0.379 (42) Drug Interaction Studies
Doravirine is primarily metabolized by CYP3A, and drugs that induce or inhibit CYP3A may affect the clearance of doravirine. Co-administration of doravirine and drugs that induce CYP3A may result in decreased plasma concentrations of doravirine. Co-administration of doravirine and drugs that inhibit CYP3A may result in increased plasma concentrations of doravirine.
Doravirine is not likely to have a clinically relevant effect on the exposure of medicinal products metabolized by CYP enzymes. Doravirine did not inhibit major drug metabolizing enzymes in vitro, including CYPs 1A2, 2B6, 2C8, 2C9, 2C19, 2D6, 3A4, and UGT1A1 and is not likely to be an inducer of CYP1A2, 2B6, or 3A4. Based on in vitro assays, doravirine is not likely to be an inhibitor of OATP1B1, OATP1B3, P-glycoprotein, BSEP, OAT1, OAT3, OCT2, MATE1, and MATE2K. Drug interaction studies were performed with doravirine and other drugs likely to be co-administered or commonly used as probes for pharmacokinetic interactions. The effects of co-administration with other drugs on the exposure (Cmax, AUC, and C24) of doravirine are summarized in Table 9. A single doravirine 100 mg dose was administered in these studies unless otherwise noted.
Table 9: Drug Interactions: Changes in Pharmacokinetic Parameter Values of Doravirine in the Presence of Co-administered Drug Co-administered Drug Regimen of Co-administered Drug N Geometric Mean Ratio (90% CI) of Doravirine Pharmacokinetics with/without Co-administered Drug (No Effect=1.00) AUC* Cmax C24 CI = confidence interval; QD = once daily; BID = twice daily - *
- AUC0-∞ for single-dose, AUC0-24 for once daily.
- †
- Changes in doravirine pharmacokinetic values are not clinically relevant.
- ‡
- Doravirine 100 mg BID resulted in similar pharmacokinetic values when compared to 100 mg QD without rifabutin.
- §
- A single doravirine 50 mg dose (0.5 times the recommended approved dose) was administered.
- ¶
- The first day following the cessation of efavirenz therapy and initiation of doravirine 100 mg QD.
- #
- 14 days following the cessation of efavirenz therapy and initiation of doravirine 100 mg QD.
Azole Antifungal Agents ketoconazole† 400 mg QD 10 3.06 (2.85, 3.29) 1.25 (1.05, 1.49) 2.75 (2.54, 2.98) Antimycobacterials rifampin 600 mg QD 10 0.12 (0.10, 0.15) 0.43 (0.35, 0.52) 0.03 (0.02, 0.04) rifabutin 300 mg QD 12 0.50 (0.45, 0.55) 0.99 (0.85, 1.15) 0.32 (0.28, 0.35) 300 mg QD‡ 15 1.03 (0.94, 1.14) 0.97 (0.87, 1.08) 0.98 (0.88, 1.10) HIV Antiviral Agents ritonavir†,§ 100 mg BID 8 3.54 (3.04, 4.11) 1.31 (1.17, 1.46) 2.91 (2.33, 3.62) efavirenz 600 mg QD¶ 17 0.38 (0.33, 0.45) 0.65 (0.58, 0.73) 0.15 (0.10, 0.23) 600 mg QD# 17 0.68 (0.58, 0.80) 0.86 (0.77, 0.97) 0.50 (0.39, 0.64) Based on drug interaction studies conducted with doravirine, no clinically significant drug interactions have been observed following the co-administration of doravirine and the following drugs: dolutegravir, ritonavir, TDF, lamivudine, elbasvir and grazoprevir, ledipasvir and sofosbuvir, ketoconazole, aluminum hydroxide/magnesium hydroxide/simethicone containing antacid, pantoprazole, atorvastatin, an oral contraceptive containing ethinyl estradiol and levonorgestrel, metformin, methadone, and midazolam.
12.4 Microbiology
Mechanism of Action
Doravirine is a pyridinone non-nucleoside reverse transcriptase inhibitor of HIV-1 and inhibits HIV-1 replication by non-competitive inhibition of HIV-1 reverse transcriptase (RT). The inhibitory concentration at 50% (IC50) of doravirine for RNA-dependent DNA polymerization of recombinant wild-type HIV-1 RT in a biochemical assay was 12.2±2.0 nM (n=3). Doravirine does not inhibit the human cellular DNA polymerases α, β, and mitochondrial DNA polymerase γ.
Antiviral Activity in Cell Culture
Doravirine exhibited an EC50 value of 12.0±4.4 nM against wild-type laboratory strains of HIV-1 when tested in the presence of 100% normal human serum (NHS) using MT4-GFP reporter cells and a median EC50 value for HIV-1 subtype B primary isolates (n=118) of 4.1 nM (range: 1.0 nM-16.0 nM). Doravirine demonstrated antiviral activity against a broad panel of primary HIV-1 isolates (A, A1, AE, AG, B, BF, C, D, G, H) with EC50 values ranging from 1.2 nM to 10.0 nM.
Antiviral Activity in Combination with other HIV Antiviral Agents
The antiviral activity of doravirine in cell culture was not antagonistic when combined with the NNRTIs delavirdine, efavirenz, etravirine, nevirapine, or rilpivirine; the NRTIs abacavir, didanosine, emtricitabine, lamivudine, stavudine, tenofovir DF, or zidovudine; the PIs darunavir or indinavir; the gp41 fusion inhibitor enfuvirtide; the CCR5 co-receptor antagonist maraviroc; or the integrase strand transfer inhibitor raltegravir.
Resistance
In Cell Culture
Doravirine-resistant strains were selected in cell culture starting from wild-type HIV-1 of different origins and subtypes, as well as NNRTI-resistant HIV-1. Observed emergent amino acid substitutions in RT included: V106A, V106I, V106M, V108I, H221Y, F227C, F227I, F227L, F227V, M230I, L234I, P236L, and Y318F. The V106A, V106M, V108I, H221Y, F227C, M230I, P236L, and Y318F substitutions conferred 3.4-fold to 70-fold reductions in susceptibility to doravirine. Y318F in combination with V106A, V106M, V108I, and F227C conferred greater decreases in susceptibility to doravirine than Y318F alone, which conferred a 10-fold reduction in susceptibility to doravirine.
In Clinical Trials
Clinical Trial Results in Adults with No Antiretroviral Treatment History
In the doravirine treatment arms of the DRIVE-FORWARD and DRIVE-AHEAD trials (n=747) through Week 96, 13 subjects showed the emergence of doravirine resistance-associated substitutions in their HIV among 36 (36%) subjects in the resistance analysis subset (subjects with HIV-1 RNA greater than 400 copies per mL at virologic failure or early study discontinuation and having post-baseline resistance samples). Emergent doravirine resistance-associated substitutions in RT included one or more of the following: V90G/I, A98G, V106A, V106I, V106M/T, V108I, E138G, Y188L, H221Y, P225H, P225L, P225P/S, F227C, F227C/R, Y318Y/F and Y318Y/S. Eight of 13 (62%) subjects with emergent doravirine resistance-associated substitutions showed doravirine phenotypic resistance and most of them had at least a 100-fold reduction in doravirine susceptibility (range >95- to >211–fold reduction in doravirine susceptibility). The other 5 virologic failures who had only amino acid mixtures of NNRTI resistance substitutions showed doravirine phenotypic fold-changes of less than 2-fold. Of the 36 subjects in the resistance analysis subset, 10 subjects (28%) developed genotypic and/or phenotypic resistance to the other drugs (abacavir, emtricitabine, lamivudine, or tenofovir) in the regimens of the DRIVE-FORWARD and DRIVE-AHEAD trials. The resistance-associated substitutions that emerged were RT M41L (n=1), A62A/V (n=1), K65R (n=2), T69T/A (n=1), V75V/I (n=1), and M184I or V (n=7).
In the DRV/r treatment arm of the DRIVE-FORWARD trial (n=383) through Week 96, no subjects showed the emergence of darunavir resistance-associated substitutions among 15 subjects with resistance data and 2 of the subjects had emergent genotypic or phenotypic resistance to lamivudine or tenofovir. In the EFV/FTC/TDF treatment arm of the DRIVE-AHEAD trial (n=364) through Week 96, 15 subjects showed the emergence of efavirenz resistance-associated substitutions among 25 (60%) subjects in the resistance analysis subset and genotypic resistance to emtricitabine or tenofovir developed in 5 evaluable subjects; emergent resistance-associated substitutions were RT K65R (n=1), D67G/K70E (n=1), L74V/V75M/V118I (n=1), M184I or V (n=5), and K219K/E (n=1).
Clinical Trial Results in Virologically-Suppressed Adults
In the DRIVE-SHIFT clinical trial [see Clinical Studies (14.2)], there were 6 subjects in the immediate switch group (n=447) and 2 subjects in the delayed switch group (n=209) who met the protocol-defined virologic failure criteria (confirmed HIV-1 RNA ≥ 50 copies/mL). Two of the 6 virologic failure subjects in the immediate switch group had available resistance data and neither developed detectable genotypic or phenotypic resistance to doravirine, lamivudine, or tenofovir during treatment with DELSTRIGO. One of the two virologic failure subjects in the delayed switch group who had available resistance data developed the RT M184M/I substitution and phenotypic resistance to emtricitabine and lamivudine during treatment with their baseline regimen.
Cross-Resistance
Cross-resistance has been observed among NNRTIs. Treatment-emergent doravirine resistance-associated substitutions can confer cross-resistance to efavirenz, etravirine, nevirapine, and rilpivirine. Of the 8 virologic failure subjects who developed doravirine phenotypic resistance, all had phenotypic resistance to nevirapine, 6 had phenotypic resistance to efavirenz, 4 had phenotypic resistance to rilpivirine, and 4 had resistance to etravirine in the Monogram PhenoSense assay. Of the 11 virologic failure subjects in DRIVE-AHEAD phenotypically resistant to efavirenz, 2 (18%) had decreased susceptibility to doravirine (18- and 36-fold).
The treatment-emergent doravirine resistance-associated substitution Y318F did not confer reduced susceptibility to efavirenz, etravirine, or rilpivirine.
A panel of 96 diverse clinical isolates containing NNRTI resistance-associated substitutions was evaluated for susceptibility to doravirine. Clinical isolates containing the Y188L substitution alone or in combination with K103N or V106I, V106A in combination with G190A and F227L, or E138K in combination with Y181C and M230L showed greater than 100-fold reduced susceptibility to doravirine.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Doravirine was not carcinogenic in long-term oral carcinogenicity studies in mice and rats at exposures up to 6 and 7 times, respectively, the human exposures at the RHD. A statistically significant incidence of thyroid parafollicular cell adenoma and carcinoma seen only in female rats at the high dose was within the range observed in historical controls.
-
14 CLINICAL STUDIES
14.1 Clinical Trial Results in Adults with No Antiretroviral Treatment History
The efficacy of PIFELTRO is based on the analyses of 96-week data from two randomized, multicenter, double-blind, active controlled Phase 3 trials (DRIVE-FORWARD, NCT02275780 and DRIVE-AHEAD, NCT02403674) in HIV-1-infected subjects with no antiretroviral treatment history (n=1494).
In DRIVE-FORWARD, 766 subjects were randomized and received at least 1 dose of either PIFELTRO once daily or darunavir 800 mg + ritonavir 100 mg (DRV+r) once daily each in combination with emtricitabine/tenofovir DF (FTC/TDF) or abacavir/lamivudine (ABC/3TC) selected by the investigator. At baseline, the median age of subjects was 33 years, 16% were female, 27% were non-white, 4% had hepatitis B and/or C virus co-infection, 10% had a history of AIDS, 20% had HIV-1 RNA greater than 100,000 copies/mL, 86% had CD4+ T-cell count greater than 200 cells/mm3, 13% received ABC/3TC, and 87% received FTC/TDF; these characteristics were similar between treatment groups.
In DRIVE-AHEAD, 728 subjects were randomized and received at least 1 dose of either DELSTRIGO (DOR/3TC/TDF) or EFV 600 mg/FTC 200 mg/TDF 300 mg once daily. At baseline, the median age of subjects was 31 years, 15% were female, 52% were non-white, 3% had hepatitis B or C co-infection, 14% had a history of AIDS, 21% had HIV-1 RNA greater than 100,000 copies/mL, and 88% had CD4+ T-cell count greater than 200 cells/mm3; these characteristics were similar between treatment groups.
Week 96 outcomes for DRIVE-FORWARD and DRIVE-AHEAD are provided in Table 10. Side-by-side tabulation is to simplify presentation; direct comparisons across trials should not be made due to differing trial designs.
In DRIVE-FORWARD, the mean CD4+ T-cell counts in the PIFELTRO and DRV+r groups increased from baseline by 224 and 207 cells/mm3, respectively.
In DRIVE-AHEAD, the mean CD4+ T-cell counts in the DELSTRIGO and EFV/FTC/TDF groups increased from baseline by 238 and 223 cells/mm3, respectively.
Table 10: Virologic Outcome in DRIVE-FORWARD and DRIVE-AHEAD at Week 96 in HIV-1 Adults with No Antiretroviral Treatment History Outcome DRIVE-FORWARD DRIVE-AHEAD PIFELTRO + 2 NRTIs
Once DailyDRV+r + 2 NRTIs
Once DailyDELSTRIGO
Once DailyEFV/FTC/TDF
Once DailyN=383 N=383 N=364 N=364 Note: NRTIs = FTC/3TC or ABC/3TC. - *
- The 95% CIs for the treatment differences were calculated using stratum-adjusted Mantel-Haenszel method.
- †
- Includes subjects who discontinued study drug or study before Week 96 for lack or loss of efficacy and subjects with HIV-1 RNA equal to or above 50 copies/mL in the Week 96 window.
- ‡
- Includes subjects who discontinued because of adverse event (AE) or death if this resulted in no virologic data in the Week 96 window.
- §
- Other Reasons include: lost to follow-up, non-compliance with study drug, physician decision, pregnancy, protocol deviation, screen failure, withdrawal by subject.
- ¶
- Does not include subjects whose ethnicity or viral subtypes were unknown.
HIV-1 RNA <50 copies/mL 72% 65% 77% 74% Treatment Differences (95% CI) * 7.5% (1.0%, 14.1%) 3.8% (-2.4%, 10.0%) HIV-1 RNA ≥ 50 copies/mL† 17% 20% 15% 12% No Virologic Data at Week 96 Window 11% 15% 7% 14% Discontinued study due to AE or Death‡ 2% 4% 3% 8% Discontinued study for Other Reasons§ 7% 9% 4% 5% On study but missing data in window 2% 3% 1% 1% Proportion (%) of Subjects With HIV-1 RNA <50 copies/mL at Week 96 by Baseline and Demographic Category Gender Male 72% (N = 319) 67% (N = 326) 78% (N = 305) 73% (N = 311) Female 73% (N = 64) 54% (N = 57) 75% (N = 59) 75% (N = 53) Race White 78% (N = 280) 68% (N = 280) 80% (N = 176) 74% (N = 170) Non-White 58% (N = 103) 57% (N = 102) 76% (N = 188) 74% (N = 194) Ethnicity¶ Hispanic or Latino 76% (N = 93) 63% (N = 86) 81% (N = 126) 77% (N = 119) Not Hispanic or Latino 71% (N = 284) 66% (N = 290) 76% (N = 238) 72% (N = 239) NRTI Background Therapy FTC/TDF 71% (N = 333) 64% (N = 335) - - ABC/3TC 80% (N = 50) 67% (N = 48) - - Baseline HIV-1 RNA (copies/mL) ≤100,000 copies/mL 75% (N = 300) 66% (N = 309) 80% (N = 291) 77% (N = 282) >100,000 copies/mL 61% (N = 83) 59% (N = 73) 67% (N = 73) 62% (N = 82) CD4+ T-cell Count (cells/mm3) ≤200 cells/mm3 62% (N = 42) 51% (N = 67) 59% (N = 44) 70% (N = 46) >200 cells/mm3 74% (N = 341) 68% (N = 316) 80% (N = 320) 74% (N = 318) Viral Subtype¶ Subtype B 71% (N = 266) 66% (N = 272) 80% (N = 232) 72% (N = 253) Subtype Non-B 75% (N = 117) 62% (N = 111) 73% (N = 130) 77% (N = 111) 14.2 Clinical Trial Results in Virologically-Suppressed Adults
The efficacy of switching from a baseline regimen consisting of two NRTIs in combination with a PI plus either ritonavir or cobicistat, or elvitegravir plus cobicistat, or an NNRTI to DELSTRIGO was evaluated in a randomized, open-label trial (DRIVE-SHIFT, NCT02397096), in virologically-suppressed HIV-1-infected adults. Subjects must have been virologically-suppressed (HIV-1 RNA < 50 copies/mL) on their baseline regimen for at least 6 months prior to trial entry, with no history of virologic failure. Subjects were randomized to either switch to DELSTRIGO at baseline (n = 447, Immediate Switch Group (ISG)), or stay on their baseline regimen until Week 24, at which point they switched to DELSTRIGO (n = 223, Delayed Switch Group (DSG)).
At baseline, the median age of subjects was 43 years, 16% were female, and 24% were Non-White, 21% were of Hispanic or Latino ethnicity, 3% had hepatitis B and/or C virus co-infection, 17% had a history of AIDS, 96% had CD4+ T-cell count greater than or equal to 200 cells/mm3, 70% were on a regimen containing a PI plus ritonavir, 24% were on a regimen containing an NNRTI, 6% were on a regimen containing elvitegravir plus cobicistat, and 1% were on a regimen containing a PI plus cobicistat; these characteristics were similar between treatment groups.
Virologic outcome results are shown in Table 11.
Table 11: Virologic Outcomes in DRIVE-SHIFT in HIV-1 Virologically-Suppressed Subjects Who Switched to DELSTRIGO Outcome DELSTRIGO
Once Daily ISG
Week 48
N=447Baseline Regimen
DSG
Week 24
N=223- *
- Includes subjects who discontinued study drug or study before Week 48 for ISG or before Week 24 for DSG for lack or loss of efficacy and subjects with HIV-1 RNA ≥50 copies/mL in the Week 48 window for ISG and in the Week 24 window for DSG.
- †
- The 95% CI for the treatment difference was calculated using stratum-adjusted Mantel-Haenszel method.
- ‡
- Assessed using a non-inferiority margin of 4%.
- §
- Includes subjects who discontinued because of adverse event (AE) or death if this resulted in no virologic data on treatment during the specified window.
- ¶
- Other reasons include: lost to follow-up, non-compliance with study drug, physician decision, protocol deviation, withdrawal by subject.
- #
- Baseline Regimen = PI plus either ritonavir or cobicistat (specifically atazanavir, darunavir, or lopinavir), or elvitegravir plus cobicistat, or NNRTI (specifically efavirenz, nevirapine, or rilpivirine), each administered with two NRTIs.
HIV-1 RNA ≥ 50 copies/mL* 2% 1% ISG-DSG, Difference (95% CI) †‡ 0.7% (-1.3%, 2.6%) HIV-1 RNA <50 copies/mL 91% 95% No Virologic Data Within the Time Window 8% 4% Discontinued study due to AE or Death§ 3% <1% Discontinued study for Other Reasons¶ 4% 4% On study but missing data in window 0 0 Proportion (%) of Subjects With HIV-1 RNA <50 copies/mL by Baseline and Demographic Category Age (years) < 50 90% (N = 320) 95% (N = 157) ≥ 50 94% (N = 127) 94% (N = 66) Gender Male 91% (N = 372) 94% (N = 194) Female 91% (N = 75) 100% (N = 29) Race White 90% (N = 344) 95% (N = 168) Non-White 93% (N = 103) 93% (N = 55) Ethnicity Hispanic or Latino 88% (N = 99) 91% (N = 45) Not Hispanic or Latino 91% (N = 341) 95% (N = 175) CD4+ T-cell Count (cells/mm3) <200 cells/mm3 85% (N = 13) 75% (N = 4) ≥200 cells/mm3 91% (N = 426) 95% (N = 216) Baseline Regimen# PI plus either ritonavir or cobicistat 90% (N=316) 94% (N=156) elvitegravir plus cobicistat or NNRTI 93% (N=131) 96% (N=67) 14.3 Clinical Trial Results in Pediatric Patients
The efficacy of DELSTRIGO (DOR/3TC/TDF) was evaluated in cohort 2 of an open-label, single-arm 2-cohort trial in HIV-1-infected pediatric patients 12 to less than 18 years of age (IMPAACT 2014 (Protocol 027), NCT03332095). In cohort 1, virologically-suppressed subjects (n=9) received a single 100 mg dose of PIFELTRO followed by intensive PK sampling. In cohort 2, virologically-suppressed subjects (n=43) were switched to DELSTRIGO and treatment-naïve subjects (n=2) were started on DELSTRIGO.
In cohort 2, at baseline the median age of subjects was 15 years (range: 12 to 17), the median weight was 52 kg (range: 45 to 80), 58% were female, 78% were Asian and 22% were Black, and the median CD4+ T-cell count was 713 cells per mm3 (range 84 to 1397). After switching to DELSTRIGO, 95% (41/43) of virologically-suppressed subjects remained suppressed (HIV-1 RNA <50 copies/mL) at Week 24. One of the two treatment-naïve subjects achieved HIV-1 RNA <50 copies/mL at Week 24. The other treatment-naïve subject met the protocol-defined virologic failure criteria (defined as 2 consecutive plasma HIV-1 RNA test results ≥200 copies/mL at or after Week 24) and was evaluated for the development of resistance; no emergence of genotypic or phenotypic resistance to doravirine, lamivudine, or tenofovir was detected.
- 16 HOW SUPPLIED/STORAGE AND HANDLING
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Drug Interactions
Inform patients that PIFELTRO may interact with certain other drugs; therefore, advise patients to report to their healthcare provider the use of any other prescription or nonprescription medication or herbal products, including St. John's wort [see Contraindications (4), Warnings and Precautions (5.1), and Drug Interactions (7.1)].
For patients concomitantly receiving rifabutin, take one tablet of PIFELTRO twice daily (approximately 12 hours apart) [see Dosage and Administration (2.2)].
Immune Reconstitution Syndrome
Inform patients that in some patients with advanced HIV infection (AIDS), signs and symptoms of inflammation from previous infections may occur soon after anti-HIV treatment is started. It is believed that these symptoms are due to an improvement in the body's immune response, enabling the body to fight infections that may have been present with no obvious symptoms. Advise patients to inform their healthcare provider immediately of any symptoms of infection [see Warnings and Precautions (5.2)].
Dosing Instructions
Advise patients to take PIFELTRO every day at a regularly scheduled time with or without food. Inform patients that it is important not to miss or skip doses as it can result in development of resistance. If a patient forgets to take PIFELTRO, tell the patient to take the missed dose right away, unless it is almost time for the next dose. Advise the patient not to take 2 doses at one time and to take the next dose at the regularly scheduled time.
Pregnancy Registry
Inform patients that there is an antiretroviral pregnancy registry to monitor fetal outcomes in pregnant individuals exposed to PIFELTRO [see Use in Specific Populations (8.1)].
Lactation
Instruct mothers with HIV-1 infection not to breastfeed because HIV-1 can be passed to the baby in breast milk [see Use in Specific Populations (8.2)].
-
SPL UNCLASSIFIED SECTION
Manufactured for: Merck Sharp & Dohme LLC
Rahway, NJ 07065, USAFor patent information: www.msd.com/research/patent
The trademarks depicted herein are owned by their respective companies.
Copyright © 2018-2022 Merck & Co., Inc., Rahway, NJ, USA, and its affiliates.
All rights reserved.uspi-mk1439-t-2206r005
-
PATIENT PACKAGE INSERT
Patient Information
PIFELTRO™ (pih-FEL-tro)
(doravirine)
tabletsWhat is PIFELTRO? PIFELTRO is a prescription medicine that is used together with other HIV-1 medicines to treat Human Immunodeficiency Virus-1 (HIV-1) infection in adults and children who weigh at least 77 pounds (35 kg): - who have not received HIV-1 medicines in the past, or
- to replace their current HIV-1 medicines for people whose healthcare provider determines that they meet certain requirements.
It is not known if PIFELTRO is safe and effective in children who weigh less than 77 pounds (35 kg).
Who should not take PIFELTRO?Do not take PIFELTRO if you take any of the following medicines: - carbamazepine
- oxcarbazepine
- phenobarbital
- phenytoin
- enzalutamide
- rifampin
- rifapentine
- mitotane
- St. John's wort
Ask your healthcare provider or pharmacist if you are not sure if your medicine is one that is listed above. If you have taken any of the medicines in the past 4 weeks, talk to your healthcare provider or pharmacist before starting treatment with PIFELTRO.
What should I tell my healthcare provider before treatment with PIFELTRO?Before treatment with PIFELTRO, tell your healthcare provider about all of your medical conditions, including if you: - are pregnant or plan to become pregnant. It is not known if PIFELTRO can harm your unborn baby. Tell your healthcare provider if you become pregnant during treatment with PIFELTRO.
Pregnancy Registry: There is a pregnancy registry for people who take PIFELTRO during pregnancy. The purpose of this registry is to collect information about the health of you and your baby. Talk to your healthcare provider about how you can take part in this registry. - are breastfeeding or plan to breastfeed. Do not breastfeed if you take PIFELTRO.
- You should not breastfeed if you have HIV-1 because of the risk of passing HIV-1 to your baby.
- It is not known if PIFELTRO can pass into your breast milk.
- Talk with your healthcare provider about the best way to feed your baby.
- Some medicines interact with PIFELTRO. Keep a list of your medicines to show your healthcare provider and pharmacist.
- Tell your healthcare provider if you have taken rifabutin in the past 4 weeks.
- You can ask your healthcare provider or pharmacist for a list of medicines that interact with PIFELTRO.
- Do not start taking a new medicine without telling your healthcare provider. Your healthcare provider can tell you if it is safe to take PIFELTRO with other medicines.
- Take PIFELTRO every day exactly as your healthcare provider tells you to take it.
- Take PIFELTRO 1 time each day, at about the same time every day.
- If you take the medicine rifabutin during treatment with PIFELTRO, take PIFELTRO 2 times each day, about 12 hours apart, as prescribed by your healthcare provider. You may not have enough doravirine in your blood if you take rifabutin during treatment with PIFELTRO.
- Take PIFELTRO with or without food.
- Do not change your dose or stop taking PIFELTRO without talking to your healthcare provider. Stay under a healthcare provider's care when taking PIFELTRO.
- It is important that you do not miss or skip doses of PIFELTRO.
- If you miss a dose of PIFELTRO, take it as soon as you remember. If it is almost time for your next dose, skip the missed dose and take the next dose at your regular time. Do not take 2 doses of PIFELTRO at the same time.
- If you have any questions, call your healthcare provider or pharmacist.
- When your PIFELTRO supply starts to run low, get more from your healthcare provider or pharmacy. This is very important because the amount of virus in your blood may increase if the medicine is stopped for even a short time. The virus may develop resistance to PIFELTRO and become harder to treat.
PIFELTRO can cause serious side effects, including: - Changes in your immune system (Immune Reconstitution Syndrome) can happen when you start taking HIV-1 medicines. Your immune system may get stronger and begin to fight infections that have been hidden in your body for a long time. Tell your healthcare provider right away if you start having any new symptoms after starting your HIV-1 medicine.
- nausea
- dizziness
- headache
- tiredness
- diarrhea
- stomach (abdominal) pain
- abnormal dreams
These are not all the possible side effects of PIFELTRO.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store PIFELTRO?- Store PIFELTRO tablets at room temperature between 68°F to 77°F (20°C to 25°C).
- Keep PIFELTRO in the original bottle.
- Do not take the tablets out of the bottle to store in another container, such as a pill box.
- Keep the bottle tightly closed to protect PIFELTRO from moisture.
- The PIFELTRO bottle contains a desiccant to help keep your medicine dry (protect it from moisture). Keep the desiccant in the bottle. Do not eat the desiccant.
General information about the safe and effective use of PIFELTRO.Medicines are sometimes prescribed for purposes other than those listed in the Patient Information leaflet. Do not use PIFELTRO for a condition for which it was not prescribed. Do not give PIFELTRO to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about PIFELTRO that is written for healthcare professionals.
What are the ingredients in PIFELTRO?Active ingredient: doravirine.
Inactive ingredients: colloidal silicon dioxide, croscarmellose sodium, hypromellose acetate succinate, lactose monohydrate, magnesium stearate, and microcrystalline cellulose. The tablet film coating contains hypromellose, lactose monohydrate, titanium dioxide and triacetin. The coated tablets are polished with carnauba wax. -
SPL UNCLASSIFIED SECTION
Manufactured for: Merck Sharp & Dohme LLC
Rahway, NJ 07065, USAU.S. License No. 0002
For patent information: www.msd.com/research/patent
The trademarks depicted herein are owned by their respective companies.
Copyright © 2018-2022 Merck & Co., Inc., Rahway, NJ, USA, and its affiliates.
All rights reserved.usppi-mk1439-t-2206r003
For more information, go to www.PIFELTRO.com or call 1-877-888-4231.
This Patient Information has been approved by the U.S. Food and Drug Administration. Revised: 06/2022
- doravirine tablet
-
INGREDIENTS AND APPEARANCE
PIFELTRO
doravirine tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:50090-6237(NDC:0006-3069) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength DORAVIRINE (UNII: 913P6LK81M) (DORAVIRINE - UNII:913P6LK81M) DORAVIRINE 100 mg Inactive Ingredients Ingredient Name Strength silicon dioxide (UNII: ETJ7Z6XBU4) croscarmellose sodium (UNII: M28OL1HH48) hypromellose acetate succinate 06081224 (3 MM2/S) (UNII: 6N003M473W) microcrystalline cellulose (UNII: OP1R32D61U) magnesium stearate (UNII: 70097M6I30) carnauba wax (UNII: R12CBM0EIZ) hypromellose, unspecified (UNII: 3NXW29V3WO) lactose monohydrate (UNII: EWQ57Q8I5X) titanium dioxide (UNII: 15FIX9V2JP) triacetin (UNII: XHX3C3X673) Product Characteristics Color WHITE Score no score Shape OVAL Size 19mm Flavor Imprint Code logo;700 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:50090-6237-0 30 in 1 BOTTLE; Type 0: Not a Combination Product 11/21/2022 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA210806 07/20/2018 Labeler - A-S Medication Solutions (830016429) Establishment Name Address ID/FEI Business Operations A-S Medication Solutions 830016429 RELABEL(50090-6237)