Label: DUPIXENT- dupilumab injection, solution





-
NDC Code(s):
0024-5911-00,
0024-5911-01,
0024-5911-02,
0024-5911-20, view more0024-5914-00, 0024-5914-01, 0024-5914-02, 0024-5914-20, 0024-5915-00, 0024-5915-01, 0024-5915-02, 0024-5915-20, 0024-5918-00, 0024-5918-01, 0024-5918-02, 0024-5918-20, 0024-5919-00, 0024-5919-01, 0024-5919-02, 0024-5919-20
- Packager: sanofi-aventis U.S. LLC
- Category: HUMAN PRESCRIPTION DRUG LABEL
Drug Label Information
Updated April 12, 2024
If you are a healthcare professional or from the pharmaceutical industry please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use DUPIXENT safely and effectively. See full prescribing information for DUPIXENT.
DUPIXENT® (dupilumab) injection, for subcutaneous use
Initial U.S. Approval: 2017RECENT MAJOR CHANGES
INDICATIONS AND USAGE
DUPIXENT is an interleukin-4 receptor alpha antagonist indicated:
Atopic Dermatitis
- for the treatment of adult and pediatric patients aged 6 months and older with moderate-to-severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. DUPIXENT can be used with or without topical corticosteroids. (1.1)
Asthma
- as an add-on maintenance treatment of adult and pediatric patients aged 6 years and older with moderate-to-severe asthma characterized by an eosinophilic phenotype or with oral corticosteroid dependent asthma. (1.2)
Limitations of Use: Not for the relief of acute bronchospasm or status asthmaticus. (1.2)
Chronic Rhinosinusitis with Nasal Polyposis
- as an add-on maintenance treatment in adult patients with inadequately controlled chronic rhinosinusitis with nasal polyposis (CRSwNP). (1.3)
Eosinophilic Esophagitis
- for the treatment of adult and pediatric patients aged 1 year and older, weighing at least 15 kg, with eosinophilic esophagitis (EoE). (1.4)
Prurigo Nodularis
- for the treatment of adult patients with prurigo nodularis (PN). (1.5)
DOSAGE AND ADMINISTRATION
Atopic Dermatitis
Dosage in Adults (2.3):
- Recommended dosage is an initial dose of 600 mg (two 300 mg injections), followed by 300 mg given every other week (Q2W).
Dosage in Pediatric Patients 6 Months to 5 Years of Age (2.3):
Body Weight Initial and Subsequent Dosage 5 to less than 15 kg 200 mg (one 200 mg injection) every 4 weeks (Q4W) 15 to less than 30 kg 300 mg (one 300 mg injection) every 4 weeks (Q4W) Dosage in Pediatric Patients 6 Years to 17 Years of Age (2.3):
Body Weight Initial Loading Dose Subsequent Dosage* - *
- Q2W – every other week; Q4W – every 4 weeks
15 to less than 30 kg 600 mg (two 300 mg injections) 300 mg Q4W 30 to less than 60 kg 400 mg (two 200 mg injections) 200 mg Q2W 60 kg or more 600 mg (two 300 mg injections) 300 mg Q2W Asthma
Dosage in Adult and Pediatric Patients 12 Years and Older (2.4):
Initial Loading Dose Subsequent Dosage 400 mg (two 200 mg injections) 200 mg every 2 weeks (Q2W) Or 600 mg (two 300 mg injections) 300 mg every 2 weeks (Q2W) Dosage for patients with oral corticosteroid-dependent asthma or with co-morbid moderate-to-severe atopic dermatitis or adults with co-morbid chronic rhinosinusitis with nasal polyposis 600 mg (two 300 mg injections) 300 mg every 2 weeks (Q2W) Dosage in Pediatric Patients 6 to 11 Years of Age (2.4):
Body Weight Initial Dose and Subsequent Dosage 15 to less than 30 kg 300 mg every four weeks (Q4W) ≥30 kg 200 mg every other week (Q2W) For pediatric patients 6 to 11 years old with asthma and co-morbid moderate-to-severe atopic dermatitis, follow the recommended dosage as per Table 2 which includes an initial loading dose. (2.3)
Chronic Rhinosinusitis with Nasal Polyposis (2.5):
- Recommended dosage for adult patients is 300 mg given every other week (Q2W).
Eosinophilic Esophagitis (2.6):
Body Weight Recommended Dosage in Adult and Pediatric Patients 1 Year and Older, Weighing At Least 15 kg 15 to less than 30 kg 200 mg every other week (Q2W) 30 to less than 40 kg 300 mg every other week (Q2W) 40 kg or more 300 mg every week (QW) Prurigo Nodularis (2.7):
- Recommended dosage for adult patients is an initial dose of 600 mg (two 300 mg injections), followed by 300 mg given every other week (Q2W).
DOSAGE FORMS AND STRENGTHS
CONTRAINDICATIONS
Known hypersensitivity to dupilumab or any excipients in DUPIXENT. (4)
WARNINGS AND PRECAUTIONS
- Hypersensitivity: Hypersensitivity reactions including anaphylaxis, serum sickness, angioedema, urticaria, rash, erythema nodosum, and erythema multiforme have occurred. Discontinue DUPIXENT in the event of a hypersensitivity reaction. (5.1)
- Conjunctivitis and Keratitis: Advise patients to report new onset or worsening eye symptoms to their healthcare provider. Consider ophthalmological examination, as appropriate. (5.2)
- Eosinophilic Conditions: Be alert to vasculitic rash, worsening pulmonary symptoms, and/or neuropathy, especially upon reduction of oral corticosteroids. (5.3)
- Reduction of Corticosteroid Dosage: Do not discontinue systemic, topical, or inhaled corticosteroids abruptly upon initiation of DUPIXENT. Decrease steroids gradually, if appropriate. (5.5)
- Arthralgia: Advise patients to report new onset or worsening joint symptoms to their healthcare provider. If symptoms persist or worsen, consider rheumatological evaluation and/or discontinuation of DUPIXENT. (5.7)
- Parasitic (Helminth) Infections: Treat pre-existing helminth infections before initiating DUPIXENT. If patients become infected while receiving DUPIXENT and do not respond to anti-helminth treatment, discontinue DUPIXENT until the infection resolves. (5.8)
- Vaccinations: Avoid use of live vaccines. (5.9)
ADVERSE REACTIONS
Most common adverse reactions are:
- Atopic Dermatitis (incidence ≥1%): injection site reactions, conjunctivitis, blepharitis, oral herpes, keratitis, eye pruritus, other herpes simplex virus infection, dry eye, and eosinophilia. (6.1)
- Asthma (incidence ≥1%): injection site reactions, oropharyngeal pain, and eosinophilia. (6.1)
- Chronic Rhinosinusitis with Nasal Polyposis (incidence ≥1%): injection site reactions, eosinophilia, insomnia, toothache, gastritis, arthralgia, and conjunctivitis. (6.1)
- Eosinophilic Esophagitis (incidence ≥2%): injection site reactions, upper respiratory tract infections, arthralgia, and herpes viral infections. (6.1)
- Prurigo Nodularis (incidence ≥2%): nasopharyngitis, conjunctivitis, herpes infection, dizziness, myalgia, and diarrhea. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Regeneron at 1-844-387-4936 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 4/2024
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
1.1 Atopic Dermatitis
1.2 Asthma
1.3 Chronic Rhinosinusitis with Nasal Polyposis
1.4 Eosinophilic Esophagitis
1.5 Prurigo Nodularis
2 DOSAGE AND ADMINISTRATION
2.1 Important Administration Instructions
2.2 Vaccination Prior to Treatment
2.3 Recommended Dosage for Atopic Dermatitis
2.4 Recommended Dosage for Asthma
2.5 Recommended Dosage for Chronic Rhinosinusitis with Nasal Polyposis
2.6 Recommended Dosage for Eosinophilic Esophagitis
2.7 Recommended Dosage for Prurigo Nodularis
2.8 Missed Doses
2.9 Preparation for Use
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity
5.2 Conjunctivitis and Keratitis
5.3 Eosinophilic Conditions
5.4 Acute Asthma Symptoms or Deteriorating Disease
5.5 Risk Associated with Abrupt Reduction of Corticosteroid Dosage
5.6 Patients with Co-morbid Asthma
5.7 Arthralgia
5.8 Parasitic (Helminth) Infections
5.9 Vaccinations
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
12.6 Immunogenicity
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
14.1 Atopic Dermatitis
14.2 Asthma
14.3 Chronic Rhinosinusitis with Nasal Polyposis
14.4 Eosinophilic Esophagitis
14.5 Prurigo Nodularis
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
1.1 Atopic Dermatitis
DUPIXENT is indicated for the treatment of adult and pediatric patients aged 6 months and older with moderate-to-severe atopic dermatitis (AD) whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. DUPIXENT can be used with or without topical corticosteroids.
1.2 Asthma
DUPIXENT is indicated as an add-on maintenance treatment of adult and pediatric patients aged 6 years and older with moderate-to-severe asthma characterized by an eosinophilic phenotype or with oral corticosteroid dependent asthma [see Clinical Studies (14)].
1.3 Chronic Rhinosinusitis with Nasal Polyposis
DUPIXENT is indicated as an add-on maintenance treatment in adult patients with inadequately controlled chronic rhinosinusitis with nasal polyposis (CRSwNP).
-
2 DOSAGE AND ADMINISTRATION
2.1 Important Administration Instructions
DUPIXENT is administered by subcutaneous injection.
DUPIXENT is intended for use under the guidance of a healthcare provider. Provide proper training to patients and/or caregivers on the preparation and administration of DUPIXENT prior to use according to the "Instructions for Use".
Use of Pre-filled Pen or Pre-filled Syringe
The DUPIXENT pre-filled pen is for use in adult and pediatric patients aged 2 years and older.
The DUPIXENT pre-filled syringe is for use in adult and pediatric patients aged 6 months and older.
A caregiver or patient 12 years of age and older may inject DUPIXENT using the pre-filled syringe or pre-filled pen. In pediatric patients 12 to 17 years of age, administer DUPIXENT under the supervision of an adult. In pediatric patients 6 months to less than 12 years of age, administer DUPIXENT by a caregiver.
Administration Instructions
For AD, asthma, and PN patients taking an initial 600 mg dose, administer each of the two DUPIXENT 300 mg injections at different injection sites.
For AD and asthma patients taking an initial 400 mg dose, administer each of the two DUPIXENT 200 mg injections at different injection sites.
Administer subcutaneous injection into the thigh or abdomen, except for the 2 inches (5 cm) around the navel. The upper arm can also be used if a caregiver administers the injection.
Rotate the injection site with each injection. DO NOT inject DUPIXENT into skin that is tender, damaged, bruised, or scarred.
The DUPIXENT "Instructions for Use" contains more detailed instructions on the preparation and administration of DUPIXENT [see Instructions for Use].
2.2 Vaccination Prior to Treatment
Consider completing all age-appropriate vaccinations as recommended by current immunization guidelines prior to initiating treatment with DUPIXENT [see Warnings and Precautions (5.9)].
2.3 Recommended Dosage for Atopic Dermatitis
Dosage in Adults
The recommended dosage of DUPIXENT for adult patients is an initial dose of 600 mg (two 300 mg injections), followed by 300 mg given every other week (Q2W).
Dosage in Pediatric Patients 6 Months to 5 Years of Age
The recommended dosage of DUPIXENT for pediatric patients 6 months to 5 years of age is specified in Table 1.
Table 1: Dosage of DUPIXENT in Pediatric Patients 6 Months to 5 Years of Age with Atopic Dermatitis Body Weight Initial* and Subsequent Dosage - *
- For pediatric patients 6 months to 5 years of age with AD, no initial loading dose is recommended.
5 to less than 15 kg 200 mg (one 200 mg injection) every 4 weeks (Q4W) 15 to less than 30 kg 300 mg (one 300 mg injection) every 4 weeks (Q4W) Dosage in Pediatric Patients 6 Years to 17 Years of Age
The recommended dosage of DUPIXENT for pediatric patients 6 years to 17 years of age is specified in Table 2.
Table 2: Dosage of DUPIXENT in Pediatric Patients 6 Years to 17 Years of Age with Atopic Dermatitis Body Weight Initial Loading Dose Subsequent Dosage 15 to less than 30 kg 600 mg (two 300 mg injections) 300 mg every 4 weeks (Q4W) 30 to less than 60 kg 400 mg (two 200 mg injections) 200 mg every other week (Q2W) 60 kg or more 600 mg (two 300 mg injections) 300 mg every other week (Q2W) 2.4 Recommended Dosage for Asthma
Dosage in Adult and Pediatric Patients 12 Years and Older
The recommended dosage of DUPIXENT for adult and pediatric patients 12 years of age and older is specified in Table 3.
Table 3: Dosage of DUPIXENT in Adult and Pediatric Patients 12 Years and Older with Asthma Initial Loading Dose Subsequent Dosage 400 mg (two 200 mg injections) 200 mg every 2 weeks (Q2W) Or 600 mg (two 300 mg injections) 300 mg every 2 weeks (Q2W) Dosage for patients with oral corticosteroid-dependent asthma or with co-morbid moderate-to-severe atopic dermatitis or adults with co-morbid chronic rhinosinusitis with nasal polyposis 600 mg (two 300 mg injections) 300 mg every 2 weeks (Q2W) Dosage in Pediatric Patients 6 to 11 Years of Age
The recommended dosage of DUPIXENT for pediatric patients 6 to 11 years of age is specified in Table 4.
Table 4: Dosage of DUPIXENT in Pediatric Patients 6 to 11 Years of Age with Asthma Body Weight Initial* and Subsequent Dosage - *
- For pediatric patients 6 to 11 years of age with asthma, no initial loading dose is recommended.
15 to less than 30 kg 300 mg every four weeks (Q4W) ≥30 kg 200 mg every other week (Q2W) For pediatric patients 6 to 11 years of age with asthma and co-morbid moderate-to-severe AD, follow the recommended dosage as per Table 2 which includes an initial loading dose [see Dosage and Administration (2.3)].
2.5 Recommended Dosage for Chronic Rhinosinusitis with Nasal Polyposis
The recommended dosage of DUPIXENT for adult patients is 300 mg given every other week.
2.6 Recommended Dosage for Eosinophilic Esophagitis
The recommended dosage of DUPIXENT for adult and pediatric patients 1 year of age and older, weighing at least 15 kg, is specified in Table 5.
Table 5: Dosage of DUPIXENT in Adult and Pediatric Patients 1 Year of Age and Older with Eosinophilic Esophagitis Body Weight Recommended Dosage 15 to less than 30 kg 200 mg every other week (Q2W) 30 to less than 40 kg 300 mg every other week (Q2W) 40 kg or more 300 mg every week (QW) 2.7 Recommended Dosage for Prurigo Nodularis
The recommended dosage of DUPIXENT for adult patients is an initial dose of 600 mg (two 300 mg injections) followed by 300 mg given every other week (Q2W).
2.8 Missed Doses
If a weekly dose is missed, administer the dose as soon as possible, and start a new weekly schedule from the date of the last administered dose.
If an every other week dose is missed, administer the injection within 7 days from the missed dose and then resume the patient's original schedule. If the missed dose is not administered within 7 days, wait until the next dose on the original schedule.
If an every 4 week dose is missed, administer the injection within 7 days from the missed dose and then resume the patient's original schedule. If the missed dose is not administered within 7 days, administer the dose, starting a new schedule based on this date.
2.9 Preparation for Use
Before injection, remove DUPIXENT from the refrigerator and allow DUPIXENT to reach room temperature (45 minutes for the 300 mg/2 mL pre-filled syringe or pre-filled pen, and 30 minutes for the 200 mg/1.14 mL pre-filled syringe or pre-filled pen) without removing the needle cap. After removal from the refrigerator, DUPIXENT must be used within 14 days or discarded.
Inspect DUPIXENT visually for particulate matter and discoloration prior to administration. DUPIXENT is a clear to slightly opalescent, colorless to pale yellow solution. Do not use if the liquid contains visible particulate matter, is discolored or cloudy (other than clear to slightly opalescent, colorless to pale yellow). DUPIXENT does not contain preservatives; therefore, discard any unused product remaining in the pre-filled syringe or pre-filled pen.
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
DUPIXENT is contraindicated in patients who have known hypersensitivity to dupilumab or any excipients of DUPIXENT [see Warnings and Precautions (5.1)].
-
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity
Hypersensitivity reactions, including anaphylaxis, serum sickness or serum sickness-like reactions, angioedema, generalized urticaria, rash, erythema nodosum, and erythema multiforme have been reported. If a clinically significant hypersensitivity reaction occurs, institute appropriate therapy and discontinue DUPIXENT [see Adverse Reactions (6.1, 6.2) and Clinical Pharmacology (12.6)].
5.2 Conjunctivitis and Keratitis
Conjunctivitis and keratitis adverse reactions have been reported in clinical trials.
Conjunctivitis and keratitis occurred more frequently in AD subjects who received DUPIXENT compared to those who received placebo. Conjunctivitis was the most frequently reported eye disorder. Most subjects with conjunctivitis or keratitis recovered or were recovering during the treatment period [see Adverse Reactions (6.1)].
Among subjects with asthma, the frequencies of conjunctivitis and keratitis were similar between DUPIXENT and placebo [see Adverse Reactions (6.1)].
In subjects with CRSwNP, the frequency of conjunctivitis was 2% in the DUPIXENT group compared to 1% in the placebo group in the 24-week safety pool; these subjects recovered. There were no cases of keratitis reported in the CRSwNP development program [see Adverse Reactions (6.1)].
Among subjects with EoE, there were no reports of conjunctivitis and keratitis in the DUPIXENT group in placebo-controlled trials [see Adverse Reactions (6.1)].
In subjects with PN, the frequency of conjunctivitis was 4% in the DUPIXENT group compared to 1% in the placebo group; these subjects recovered or were recovering during the treatment period. There were no cases of keratitis reported in the PN development program [see Adverse Reactions (6.1)].
Conjunctivitis and keratitis adverse events have also been reported with DUPIXENT in postmarketing settings, predominantly in AD patients. Some patients reported visual disturbances (e.g., blurred vision) associated with conjunctivitis or keratitis.
Advise patients or their caregivers to report new onset or worsening eye symptoms to their healthcare provider. Consider ophthalmological examination for patients who develop conjunctivitis that does not resolve following standard treatment or signs and symptoms suggestive of keratitis, as appropriate [see Adverse Reactions (6.1)].
5.3 Eosinophilic Conditions
Patients being treated for asthma may present with serious systemic eosinophilia sometimes presenting with clinical features of eosinophilic pneumonia or vasculitis consistent with eosinophilic granulomatosis with polyangiitis, conditions which are often treated with systemic corticosteroid therapy. These events may be associated with the reduction of oral corticosteroid therapy. Healthcare providers should be alert to vasculitic rash, worsening pulmonary symptoms, cardiac complications, and/or neuropathy presenting in their patients with eosinophilia. Cases of eosinophilic pneumonia were reported in adult subjects who participated in the asthma development program and cases of vasculitis consistent with eosinophilic granulomatosis with polyangiitis have been reported with DUPIXENT in adult subjects who participated in the asthma development program as well as in adult subjects with co-morbid asthma in the CRSwNP development program. A causal association between DUPIXENT and these conditions has not been established.
5.4 Acute Asthma Symptoms or Deteriorating Disease
DUPIXENT should not be used to treat acute asthma symptoms or acute exacerbations. Do not use DUPIXENT to treat acute bronchospasm or status asthmaticus. Patients should seek medical advice if their asthma remains uncontrolled or worsens after initiation of treatment with DUPIXENT.
5.5 Risk Associated with Abrupt Reduction of Corticosteroid Dosage
Do not discontinue systemic, topical, or inhaled corticosteroids abruptly upon initiation of therapy with DUPIXENT. Reductions in corticosteroid dose, if appropriate, should be gradual and performed under the direct supervision of a healthcare provider. Reduction in corticosteroid dose may be associated with systemic withdrawal symptoms and/or unmask conditions previously suppressed by systemic corticosteroid therapy.
5.6 Patients with Co-morbid Asthma
Advise patients with co-morbid asthma not to adjust or stop their asthma treatments without consultation with their physicians.
5.7 Arthralgia
Arthralgia has been reported with the use of DUPIXENT with some patients reporting gait disturbances or decreased mobility associated with joint symptoms; some cases resulted in hospitalization [see Adverse Reactions (6.1)]. In postmarketing reports, onset of arthralgia was variable, ranging from days to months after the first dose of DUPIXENT. Some patients' symptoms resolved while continuing treatment with DUPIXENT and other patients recovered or were recovering following discontinuation of DUPIXENT.
Advise patients to report new onset or worsening joint symptoms to their healthcare provider. If symptoms persist or worsen, consider rheumatological evaluation and/or discontinuation of DUPIXENT.
5.8 Parasitic (Helminth) Infections
Patients with known helminth infections were excluded from participation in clinical studies. It is unknown if DUPIXENT will influence the immune response against helminth infections.
Treat patients with pre-existing helminth infections before initiating therapy with DUPIXENT. If patients become infected while receiving treatment with DUPIXENT and do not respond to anti-helminth treatment, discontinue treatment with DUPIXENT until the infection resolves. Adverse reactions of helminth infections (5 cases of enterobiasis and 1 case of ascariasis) were reported in pediatric subjects 6 to 11 years old who participated in the pediatric asthma development program [see Adverse Reactions (6.1)].
5.9 Vaccinations
Consider completing all age-appropriate vaccinations as recommended by current immunization guidelines prior to initiating treatment with DUPIXENT. Avoid use of live vaccines during treatment with DUPIXENT. It is unknown if administration of live vaccines during DUPIXENT treatment will impact the safety or effectiveness of these vaccines. Limited data are available regarding coadministration of DUPIXENT with non-live vaccines [see Clinical Pharmacology (12.2)].
-
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Hypersensitivity [see Warnings and Precautions (5.1)]
- Conjunctivitis and Keratitis [see Warnings and Precautions (5.2)]
- Arthralgia [see Warnings and Precautions (5.7)]
- Parasitic (Helminth) Infections [see Warnings and Precautions (5.8)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Adults with Atopic Dermatitis
Three randomized, double-blind, placebo-controlled, multicenter trials (SOLO 1, SOLO 2, and CHRONOS) and one dose-ranging trial (AD-1021) evaluated the safety of DUPIXENT in subjects with moderate-to-severe AD. The safety population had a mean age of 38 years; 41% of subjects were female, 67% were White, 24% were Asian, and 6% were Black; in terms of co-morbid conditions, 48% of the subjects had asthma, 49% had allergic rhinitis, 37% had food allergy, and 27% had allergic conjunctivitis. In these 4 trials, 1472 subjects were treated with subcutaneous injections of DUPIXENT, with or without concomitant topical corticosteroids (TCS).
A total of 739 subjects were treated with DUPIXENT for at least 1 year in the development program for moderate-to-severe AD.
SOLO 1, SOLO 2, and AD-1021 compared the safety of DUPIXENT monotherapy to placebo through Week 16. CHRONOS compared the safety of DUPIXENT + TCS to placebo + TCS through Week 52.
AD-1225 is a multicenter, open-label extension (OLE) trial which assessed the long-term safety of repeat doses of DUPIXENT through 260 weeks of treatment in adults with moderate-to-severe AD who had previously participated in controlled trials of DUPIXENT or had been screened for SOLO 1 or SOLO 2. The safety data in AD-1225 reflect exposure to DUPIXENT 200 mg QW, 300 mg QW and 300 mg Q2W in 2677 subjects, including 2254 exposed for at least 52 weeks, 1224 exposed for at least 100 weeks, 561 exposed for at least 148 weeks and 179 exposed for at least 260 weeks.
Weeks 0 to 16 (SOLO 1, SOLO 2, CHRONOS, and AD-1021)
In DUPIXENT monotherapy trials (SOLO 1, SOLO 2, and AD-1021) through Week 16, the proportion of subjects who discontinued treatment because of adverse events was 1.9% in both the DUPIXENT 300 mg Q2W and placebo groups. Table 6 summarizes the adverse reactions that occurred at a rate of at least 1% in the DUPIXENT 300 mg Q2W monotherapy groups, and in the DUPIXENT + TCS group, all at a higher rate than in their respective comparator groups during the first 16 weeks of treatment.
Table 6: Adverse Reactions Occurring in ≥1% of the DUPIXENT Monotherapy Group or the DUPIXENT + TCS Group in the Atopic Dermatitis Trials through Week 16 Adverse Reaction DUPIXENT Monotherapy* DUPIXENT + TCS† DUPIXENT
300 mg Q2W‡Placebo DUPIXENT
300 mg Q2W‡ + TCSPlacebo + TCS N=529
n (%)N=517
n (%)N=110
n (%)N=315
n (%)- *
- Pooled analysis of SOLO 1, SOLO 2, and AD-1021.
- †
- Analysis of CHRONOS where subjects were on background TCS therapy.
- ‡
- DUPIXENT 600 mg at Week 0, followed by 300 mg every two weeks.
- §
- Conjunctivitis cluster includes conjunctivitis, allergic conjunctivitis, bacterial conjunctivitis, viral conjunctivitis, giant papillary conjunctivitis, eye irritation, and eye inflammation.
- ¶
- Keratitis cluster includes keratitis, ulcerative keratitis, allergic keratitis, atopic keratoconjunctivitis, and ophthalmic herpes simplex.
- #
- Other herpes simplex virus infection cluster includes herpes simplex, genital herpes, herpes simplex otitis externa, and herpes virus infection, but excludes eczema herpeticum.
Injection site reaction 51 (10) 28 (5) 11 (10) 18 (6) Conjunctivitis§ 51 (10) 12 (2) 10 (9) 15 (5) Blepharitis 2 (<1) 1 (<1) 5 (5) 2 (1) Oral herpes 20 (4) 8 (2) 3 (3) 5 (2) Keratitis¶ 1 (<1) 0 4 (4) 0 Eye pruritus 3 (1) 1 (<1) 2 (2) 2 (1) Other herpes simplex virus infection# 10 (2) 6 (1) 1 (1) 1 (<1) Dry eye 1 (<1) 0 2 (2) 1 (<1) Safety through Week 52 (CHRONOS)
In the DUPIXENT with concomitant TCS trial (CHRONOS) through Week 52, the proportion of subjects who discontinued treatment because of adverse events was 1.8% in DUPIXENT 300 mg Q2W + TCS group and 7.6% in the placebo + TCS group. Two subjects discontinued DUPIXENT because of adverse reactions: atopic dermatitis (1 subject) and exfoliative dermatitis (1 subject).
The safety profile of DUPIXENT + TCS through Week 52 was generally consistent with the safety profile observed at Week 16.
Safety through 260 Weeks (AD-1225)
The long-term safety profile observed in this trial through 260 weeks was generally consistent with the safety profile of DUPIXENT observed in controlled studies.
Pediatric Subjects 12 to 17 Years of Age with Atopic Dermatitis
The safety of DUPIXENT was assessed in a trial of 250 pediatric subjects 12 to 17 years of age with moderate-to-severe AD (AD-1526). The safety profile of DUPIXENT in these subjects through Week 16 was similar to the safety profile seen in adults with AD.
The long-term safety of DUPIXENT was assessed in an open-label extension study in pediatric subjects 12 to 17 years of age with moderate-to-severe AD (AD-1434). The safety profile of DUPIXENT in subjects followed through Week 52 was similar to the safety profile observed at Week 16 in AD-1526. The long-term safety profile of DUPIXENT observed in pediatric subjects 12 to 17 years of age was consistent with that seen in adults with AD.
Pediatric Subjects 6 to 11 Years of Age with Atopic Dermatitis
The safety of DUPIXENT with concomitant TCS was assessed in a trial of 367 pediatric subjects 6 to 11 years of age with severe AD (AD-1652). The safety profile of DUPIXENT + TCS in these subjects through Week 16 was similar to the safety profile from trials in adult and pediatric subjects 12 to 17 years of age with AD.
The long-term safety of DUPIXENT ± TCS was assessed in an open-label extension study of 368 pediatric subjects 6 to 11 years of age with AD (AD-1434). Among subjects who entered this study, 110 (30%) had moderate and 72 (20%) had severe AD at the time of enrollment in AD-1434. The safety profile of DUPIXENT ± TCS in subjects followed through Week 52 was similar to the safety profile observed through Week 16 in AD-1652. The long-term safety profile of DUPIXENT ± TCS observed in pediatric subjects 6 to 11 years of age was consistent with that seen in adult and pediatric subjects 12 to 17 years of age with AD [see Use in Specific Populations (8.4)].
Pediatric Subjects 6 Months to 5 Years of Age with Atopic Dermatitis
The safety of DUPIXENT with concomitant TCS was assessed in a trial of 161 pediatric subjects 6 months to 5 years of age with moderate-to-severe AD (AD-1539). The safety profile of DUPIXENT + TCS in these subjects through Week 16 was similar to the safety profile from trials in adults and pediatric subjects 6 to 17 years of age with AD.
The long-term safety of DUPIXENT ± TCS was assessed in an open-label extension study of 180 pediatric subjects 6 months to 5 years of age with AD (AD-1434). The majority of subjects were treated with DUPIXENT 300 mg every 4 weeks. The safety profile of DUPIXENT ± TCS in subjects followed through Week 52 was similar to the safety profile observed through Week 16 in AD-1539. The long-term safety profile of DUPIXENT ± TCS observed in pediatric subjects 6 months to 5 years of age was consistent with that seen in adults and pediatric subjects 6 to 17 years old with AD. In addition, hand-foot-and-mouth disease was reported in 9 (5%) pediatric subjects and skin papilloma was reported in 4 (2%) pediatric subjects treated with DUPIXENT ± TCS. These cases did not lead to study drug discontinuation [see Use in Specific Populations (8.4)].
Atopic Dermatitis with Hand and/or Foot Involvement
The safety of DUPIXENT was assessed in a 16-week, multicenter, randomized, double-blind, parallel-group, placebo-controlled trial (Liberty-AD-HAFT) in 133 adult and pediatric subjects 12 to 17 years of age with atopic dermatitis with moderate-to-severe hand and/or foot involvement [see Clinical Studies (14)]. In this trial 67 subjects received DUPIXENT, and 66 subjects received placebo. DUPIXENT-treated subjects received the recommended dosage based on their age and body weight [see Dosage and Administration (2.3)]. The safety profile of DUPIXENT in these subjects through Week 16 was consistent with the safety profile from studies in adult and pediatric subjects 6 months of age and older with moderate-to-severe AD.
Asthma
Adults and Pediatric Subjects 12 Years of Age and Older with Asthma
A total of 2888 adult and pediatric subjects 12 to 17 years of age with moderate-to-severe asthma (AS) were evaluated in 3 randomized, placebo-controlled, multicenter trials of 24 to 52 weeks duration (DRI12544, QUEST, and VENTURE). Of these, 2678 had a history of 1 or more severe exacerbations in the year prior to enrollment despite regular use of medium to high-dose inhaled corticosteroids plus an additional controller(s) (DRI12544 and QUEST). A total of 210 subjects with oral corticosteroid-dependent asthma receiving high-dose inhaled corticosteroids plus up to two additional controllers were enrolled (VENTURE). The safety population (DRI12544 and QUEST) was 12-87 years of age, of which 63% were female, and 82% were White. DUPIXENT 200 mg or 300 mg was administered subcutaneously Q2W, following an initial dose of 400 mg or 600 mg, respectively.
In DRI12544 and QUEST, the proportion of subjects who discontinued treatment due to adverse events was 4% of the placebo group, 3% of the DUPIXENT 200 mg Q2W group, and 6% of the DUPIXENT 300 mg Q2W group.
Table 7 summarizes the adverse reactions that occurred at a rate of at least 1% in subjects treated with DUPIXENT and at a higher rate than in their respective comparator groups in DRI12544 and QUEST.
Table 7: Adverse Reactions Occurring in ≥1% of the DUPIXENT Groups in DRI12544 and QUEST and Greater than Placebo (6 Month Safety Pool) Adverse Reaction DRI12544 and QUEST DUPIXENT
200 mg Q2WDUPIXENT
300 mg Q2WPlacebo N=779
n (%)N=788
n (%)N=792
n (%)- *
- Injection site reactions cluster includes erythema, edema, pruritus, pain, and inflammation.
- †
- Eosinophilia = blood eosinophils ≥3,000 cells/mcL or deemed by the investigator to be an adverse event. None met the criteria for serious eosinophilic conditions [see Warnings and Precautions (5.3)].
Injection site reactions* 111 (14%) 144 (18%) 50 (6%) Oropharyngeal pain 13 (2%) 19 (2%) 7 (1%) Eosinophilia† 17 (2%) 16 (2%) 2 (<1%) Injection site reactions were most common with the loading (initial) dose.
The safety profile of DUPIXENT through Week 52 was generally consistent with the safety profile observed at Week 24.
Pediatric Subjects 6 to 11 Years of Age with Asthma
The safety of DUPIXENT was assessed in 405 pediatric subjects 6 to 11 years of age with moderate-to-severe asthma (VOYAGE). The safety profile of DUPIXENT in these subjects through Week 52 was similar to the safety profile from studies in adult and pediatric subjects 12 years of age and older with moderate-to-severe asthma with the addition of helminth infections. Helminth infections were reported in 2.2% (6 subjects) in the DUPIXENT group and 0.7% (1 subject) in the placebo group. The majority of cases were enterobiasis, reported in 1.8% (5 subjects) in the DUPIXENT group and none in the placebo group. There was one case of ascariasis in the DUPIXENT group. All helminth infection cases were mild to moderate and subjects recovered with anti-helminth treatment without DUPIXENT treatment discontinuation.
Chronic Rhinosinusitis with Nasal Polyposis
A total of 722 adult subjects with chronic rhinosinusitis with nasal polyposis (CRSwNP) were evaluated in 2 randomized, placebo-controlled, multicenter trials of 24 to 52 weeks duration (SINUS-24 and SINUS-52). The safety pool consisted of data from the first 24 weeks of treatment from both studies.
In the safety pool, the proportion of subjects who discontinued treatment due to adverse events was 5% of the placebo group and 2% of the DUPIXENT 300 mg Q2W group.
Table 8 summarizes the adverse reactions that occurred at a rate of at least 1% in subjects treated with DUPIXENT and at a higher rate than in their respective comparator group in SINUS-24 and SINUS-52.
Table 8: Adverse Reactions Occurring in ≥1% of the DUPIXENT Group in SINUS-24 and SINUS-52 and Greater than Placebo (24-Week Safety Pool) Adverse Reaction SINUS-24 and SINUS-52 DUPIXENT
300 mg Q2WPlacebo N=440
n (%)N=282
n (%)Injection site reactions* 28 (6%) 12 (4%) Conjunctivitis† 7 (2%) 2 (1%) Arthralgia 14 (3%) 5 (2%) Gastritis 7 (2%) 2 (1%) Insomnia 6 (1%) 0 (<1%) Eosinophilia 5 (1%) 1 (<1%) Toothache 5 (1%) 1 (<1%) The safety profile of DUPIXENT through Week 52 was generally consistent with the safety profile observed at Week 24.
Eosinophilic Esophagitis
Adults and Pediatric Subjects 12 Years of Age and Older with EoE
A total of 239 adult and pediatric subjects 12 years of age and older, weighing at least 40 kg, with EoE were evaluated in a randomized, double-blind, parallel-group, multicenter, placebo-controlled trial, including two 24-week treatment periods (Study EoE-1 Parts A and B) and received either DUPIXENT 300 mg QW or placebo[see Clinical Studies (14.4)].
The proportion of subjects who discontinued treatment due to adverse events was 2% of the placebo group and 2% of the DUPIXENT 300 mg QW group.
Table 9 summarizes the adverse reactions that occurred at a rate of at least 2% in subjects treated with DUPIXENT and at a higher rate than in their respective comparator group in Parts A and B.
Table 9: Adverse Reactions Occurring in ≥2% of Adult and Pediatric Subjects 12 Years of Age and Older with EoE Treated with DUPIXENT in a Placebo-Controlled Trial (Study EoE-1 Parts A and B; 24-Week Safety Pool) Study EoE-1 Parts A and B Adverse Reaction DUPIXENT 300 mg QW
N=122
n (%)Placebo
N=117
n (%)- *
- Injection site reactions are composed of several terms including, but not limited to, injection site swelling, pain, and bruising.
- †
- Upper respiratory tract infections are composed of several terms including, but not limited to, COVID-19, sinusitis, and upper respiratory tract infection.
- ‡
- Herpes viral infections are composed of oral herpes and herpes simplex.
Injection site reactions* 46 (38%) 39 (33%) Upper respiratory tract infections† 22 (18%) 12 (10%) Arthralgia 3 (2%) 1 (1%) Herpes viral infections‡ 3 (2%) 1 (1%) The safety profile of DUPIXENT in 72 pediatric subjects 12 to 17 years of age, weighing at least 40 kg, and adults in Parts A and B was similar.
Pediatric Subjects 1 to 11 Years of Age, Weighing at least 15 kg, with EoE
A total of 61 pediatric subjects 1 to 11 years of age, weighing at least 15 kg, with EoE were evaluated in a randomized, blinded, parallel-group, multicenter trial, including an initial 16-week placebo-controlled treatment period (Study EoE-2 Part A) and a 36-week extended active treatment period (Study EoE-2 Part B). Subjects in Part A received a weight-based dosing regimen of DUPIXENT or placebo [see Clinical Studies (14.4)]. All subjects in Part B completed Part A and received active treatment with weight-based dosing regimens of DUPIXENT in Part B (N=47).
The safety profile of DUPIXENT through Week 16 of Study EoE-2 Part A was generally similar to the safety profile in adult and pediatric subjects 12 years of age and older with EoE. In Part B, a helminth infection was reported in one DUPIXENT-treated subject.
Prurigo Nodularis
A total of 309 adult subjects with prurigo nodularis (PN) were evaluated in two 24-week randomized, double-blind, placebo-controlled, multicenter trials (PRIME and PRIME2). The safety pool included data from the 24-week treatment and 12-week follow-up periods from both trials.
The proportion of subjects who discontinued treatment due to adverse events was 3% of the placebo group and 0% of the DUPIXENT 300 mg Q2W group.
The safety population had a mean age of 49 years; 65% of subjects were female, 56% were White, 34% were Asian, and 6% were Black or African American. Subjects with co-morbid conditions included 43% of subjects with a history of atopy (defined as having a medical history of AD, allergic rhinitis/rhinoconjunctivitis, asthma, or food allergy), 8% of subjects with a history of hypothyroidism and 9% of subjects with a history of diabetes mellitus type 2.
Table 10 summarizes the adverse reactions that occurred at a rate of at least 2% in subjects treated with DUPIXENT and at a higher rate than in their respective comparator group in PRIME and PRIME2.
Table 10: Adverse Reactions Occurring in ≥2% of the DUPIXENT Group in PRIME and PRIME2 and Greater than Placebo Adverse Reaction PRIME and PRIME2 DUPIXENT
300 mg Q2WPlacebo N=152
n (%)N=157
n (%)- *
- Nasopharyngitis includes pharyngitis
- †
- Conjunctivitis includes conjunctivitis and allergic conjunctivitis.
- ‡
- Herpes infection includes oral herpes, genital herpes simplex, herpes zoster and ophthalmic herpes zoster
- §
- Dizziness includes dizziness postural, vertigo and vertigo positional
- ¶
- Myalgia includes musculoskeletal pain and musculoskeletal chest pain
Nasopharyngitis* 8 (5%) 3 (2%) Conjunctivitis† 6 (4%) 2 (1%) Herpes Infection‡ 5 (3%) 0% Dizziness§ 5 (3%) 2 (1%) Myalgia¶ 5 (3%) 2 (1%) Diarrhea 4 (3%) 1 (1%) Specific Adverse Reactions
Conjunctivitis and Keratitis
In adult subjects with AD, conjunctivitis was reported in 10% (34 per 100 subject-years) in the 300 mg Q2W dose group and in 2% of the placebo group (8 per 100 subject-years) during the 16-week treatment period of the monotherapy trials (SOLO 1, SOLO 2, and AD-1021). During the 52-week treatment period of concomitant therapy AD trial (CHRONOS), conjunctivitis was reported in 16% of the DUPIXENT 300 mg Q2W + TCS group (20 per 100 subject-years) and in 9% of the placebo + TCS group (10 per 100 subject-years). During the long-term OLE trial with data through 260 weeks (AD-1225), conjunctivitis was reported in 21% of the DUPIXENT group (12 per 100 subject-years).
In DUPIXENT AD monotherapy trials (SOLO 1, SOLO 2, and AD-1021) through Week 16, keratitis was reported in <1% of the DUPIXENT group (1 per 100 subject-years) and in 0% of the placebo group (0 per 100 subject-years). In the 52-week DUPIXENT + topical corticosteroids (TCS) AD trial (CHRONOS), keratitis was reported in 4% of the DUPIXENT + TCS group (4 per 100 subject-years) and in 2% of the placebo + TCS group (2 per 100 subject-years). Conjunctivitis and keratitis occurred more frequently in AD subjects who received DUPIXENT. Conjunctivitis was the most frequently reported eye disorder. During the long-term OLE trial with data through 260 weeks (AD-1225), keratitis was reported in 3% of the DUPIXENT group (1 per 100 subject-years). Most subjects with conjunctivitis or keratitis recovered or were recovering during the treatment period.
Among subjects with asthma, the frequency of conjunctivitis and keratitis was similar between DUPIXENT and placebo.
In subjects with CRSwNP, the frequency of conjunctivitis was 2% in the DUPIXENT group compared to 1% in the placebo group in the 24-week safety pool; these subjects recovered.
In the 52-week CRSwNP study (SINUS-52), the frequency of conjunctivitis was 3% in the DUPIXENT subjects and 1% in the placebo subjects; all of these subjects recovered. There were no cases of keratitis reported in the CRSwNP development program [see Warnings and Precautions (5.2)].
Among subjects with EoE, there were no reports of conjunctivitis and keratitis in the DUPIXENT group in placebo-controlled trials [see Warnings and Precautions (5.2)]. In the 36-week active treatment extension period of Study EoE-2 Part B, conjunctivitis was reported in 4% of DUPIXENT-treated pediatric subjects with EoE.
Among subjects with PN, the frequency of conjunctivitis was 4% in the DUPIXENT group compared to 1% in the placebo group; all of these subjects recovered or were recovering during the treatment period. There were no cases of keratitis reported in the PN development program [see Warnings and Precautions (5.2)].
Eczema Herpeticum and Herpes Zoster
The rate of eczema herpeticum was similar in the placebo and DUPIXENT groups in the AD trials. The rates remained stable through 260 weeks in the long-term OLE trial (AD-1225).
Herpes zoster was reported in <1% of the DUPIXENT groups (1 per 100 subject-years) and in <1% of the placebo group (1 per 100 subject-years) in the 16-week AD monotherapy trials. In the 52-week DUPIXENT + TCS AD trial, herpes zoster was reported in 1% of the DUPIXENT + TCS group (1 per 100 subject-years) and 2% of the placebo + TCS group (2 per 100 subject-years). During the long-term OLE trial with data through 260 weeks (AD-1225), 2.0% of DUPIXENT-treated subjects reported herpes zoster (0.94 per 100 subject-years of follow up). Among asthma subjects the frequency of herpes zoster was similar between DUPIXENT and placebo. Among subjects with CRSwNP or EoE there were no reported cases of herpes zoster or eczema herpeticum.
Among subjects with PN, herpes zoster and ophthalmic herpes zoster were each reported in <1% of the DUPIXENT group (1 per 100 subject-years) and 0% of the placebo group.
Hypersensitivity Reactions
Hypersensitivity reactions were reported in <1% of DUPIXENT-treated subjects. These included anaphylaxis, serum sickness or serum sickness-like reactions, generalized urticaria, rash, erythema nodosum, and erythema multiforme [see Contraindications (4), Warnings and Precautions (5.1), and Clinical Pharmacology (12.6)].
Eosinophils
DUPIXENT-treated subjects with AD, asthma, and CRSwNP had a greater initial increase from baseline in blood eosinophil count compared to subjects treated with placebo. In adult subjects with AD (SOLO 1, SOLO 2, and AD-1021), the mean and median increases in blood eosinophils from baseline to Week 4 were 100 and 0 cells/mcL, respectively. In pediatric subjects <6 years old with AD, the mean and median increases from baseline to week 4 were 478 and 90 cells/mcL, respectively.
In adult and pediatric subjects 12 years of age and older with asthma (DRI12544 and QUEST), the mean and median increases in blood eosinophils from baseline to Week 4 were 130 and 10 cells/mcL, respectively. In subjects 6 to 11 years of age with asthma (VOYAGE), the mean and median increases in blood eosinophils from baseline to Week 12 were 124 and 0 cells/mcL, respectively.
In adult subjects with CRSwNP (SINUS-24 and SINUS-52), the mean and median increases in blood eosinophils from baseline to Week 16 were 150 and 50 cells/mcL, respectively.
An increase from baseline in blood eosinophil count was not observed in adult and pediatric subjects 12 years of age and older with EoE treated with DUPIXENT as compared to placebo (Study EoE-1). In pediatric subjects 1 to 11 years of age with EoE (Study EoE-2 Part A), blood eosinophil counts were generally consistent with those observed in Study EoE-1.
In subjects with PN (PRIME and PRIME2), the mean and median decrease in blood eosinophils from baseline to Week 4 were 9 and 10 cells/mcL, respectively.
Across the trials for AD, asthma, and CRSwNP indications, the incidence of treatment-emergent eosinophilia (≥500 cells/mcL) was similar in DUPIXENT and placebo groups. In the trials for the PN indication, the incidence of treatment-emergent eosinophilia (≥500 cells/mcL) was lower in DUPIXENT than in the placebo group.
Treatment-emergent eosinophilia (≥5,000 cells/mcL) was reported in <3% of DUPIXENT-treated subjects and <0.5% in placebo-treated subjects (SOLO 1, SOLO 2, and AD-1021; DRI12544, QUEST, and VOYAGE; SINUS-24 and SINUS-52; PRIME and PRIME2). Blood eosinophil counts declined to near baseline or remained below baseline levels (PRIME and PRIME2) during study treatment. In study AD-1539, treatment-emergent eosinophilia (≥5,000 cells/mcL) was reported in 8% of DUPIXENT-treated subjects and 0% in placebo-treated subjects [see Warnings and Precautions (5.3)].
Cardiovascular
In the 1-year placebo-controlled trial in adult and pediatric subjects 12 years of age and older with asthma (QUEST), cardiovascular thromboembolic events (cardiovascular deaths, non-fatal myocardial infarctions, and non-fatal strokes) were reported in 1 (0.2%) of the DUPIXENT 200 mg Q2W group, 4 (0.6%) of the DUPIXENT 300 mg Q2W group, and 2 (0.3%) of the placebo group.
In the 1-year placebo-controlled trial in subjects with AD (CHRONOS), cardiovascular thromboembolic events (cardiovascular deaths, non-fatal myocardial infarctions, and non-fatal strokes) were reported in 1 (0.9%) of the DUPIXENT + TCS 300 mg Q2W group, 0 (0.0%) of the DUPIXENT + TCS 300 mg QW group, and 1 (0.3%) of the placebo + TCS group.
In the 24-week placebo-controlled trial in subjects with CRSwNP (SINUS-24), cardiovascular thromboembolic events (cardiovascular deaths, non-fatal myocardial infarctions, and non-fatal strokes) were reported in 1 (0.7%) of the DUPIXENT group and 0 (0.0%) of the placebo group. In the 1-year placebo-controlled trial in subjects with CRSwNP (SINUS-52), there were no cases of cardiovascular thromboembolic events (cardiovascular deaths, non-fatal myocardial infarctions, and non-fatal strokes) reported in any treatment arm.
In the 24-week placebo-controlled trial in subjects with EoE (Study EoE-1 Parts A and B), there were no cases of cardiovascular thromboembolic events (cardiovascular deaths, non-fatal myocardial infarctions, and non-fatal strokes) reported in any treatment arm.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of DUPIXENT. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Immune system disorders: angioedema [see Warnings and Precautions (5.1)]
Skin and subcutaneous tissue disorders: Facial skin reactions, including erythema, rash, scaling, edema, papules, pruritus, burning, and pain
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to DUPIXENT during pregnancy.
Healthcare providers and patients may call 1-877-311-8972 or go to https://mothertobaby.org/ongoing-study/dupixent/ to enroll in or to obtain information about the registry.
Risk Summary
Available data from case reports and case series with DUPIXENT use in pregnant women have not identified a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. Human IgG antibodies are known to cross the placental barrier; therefore, DUPIXENT may be transmitted from the mother to the developing fetus. There are adverse effects on maternal and fetal outcomes associated with asthma in pregnancy (see Clinical Considerations). In an enhanced pre- and post-natal developmental study, no adverse developmental effects were observed in offspring born to pregnant monkeys after subcutaneous administration of a homologous antibody against interleukin-4-receptor alpha (IL-4Rα) during organogenesis through parturition at doses up to 10-times the maximum recommended human dose (MRHD) (see Data).
The background risk of major birth defects and miscarriage for the indicated populations are unknown. All pregnancies have a background risk of birth defect, loss or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Disease-Associated Maternal and/or Embryo-fetal Risk
In women with poorly or moderately controlled asthma, evidence demonstrates that there is an increased risk of preeclampsia in the mother and prematurity, low birth weight, and small for gestational age in the neonate. The level of asthma control should be closely monitored in pregnant women and treatment adjusted as necessary to maintain optimal control.
Data
Animal Data
In an enhanced pre- and post-natal development toxicity study, pregnant cynomolgus monkeys were administered weekly subcutaneous doses of homologous antibody against IL-4Rα up to 10 times the MRHD (on a mg/kg basis of 100 mg/kg/week) from the beginning of organogenesis to parturition. No treatment-related adverse effects on embryo-fetal toxicity or malformations, or on morphological, functional, or immunological development were observed in the infants from birth through 6 months of age.
8.2 Lactation
Risk Summary
There are no data on the presence of dupilumab in human milk, the effects on the breastfed infant, or the effects on milk production. Maternal IgG is known to be present in human milk. The effects of local gastrointestinal exposure and limited systemic exposure to dupilumab on the breastfed infant are unknown. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for DUPIXENT and any potential adverse effects on the breastfed child from DUPIXENT or from the underlying maternal condition.
8.4 Pediatric Use
Atopic Dermatitis
The safety and effectiveness of DUPIXENT have been established in pediatric patients 6 months of age and older with moderate-to-severe AD, whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable [see Clinical Studies (14.1)].
Use of DUPIXENT in this age group is supported by data from the following clinical trials:
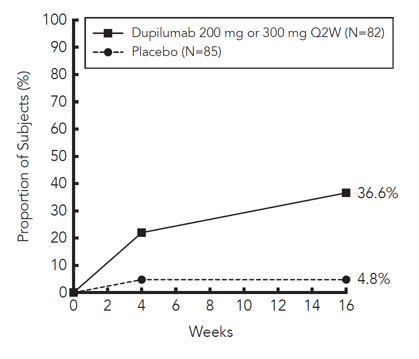
- AD-1526 which included 251 pediatric subjects 12 to 17 years of age with moderate-to-severe AD. Of the 251 subjects, 82 were treated with DUPIXENT 200 mg Q2W (<60 kg) or 300 mg Q2W (≥60 kg) and 85 were treated with matching placebo
- AD-1652 which included 367 pediatric subjects 6 to 11 years of age with severe AD. Of the 367 subjects, 120 were treated with DUPIXENT 300 mg Q4W + TCS (15 to <30 kg) or 200 mg Q2W + TCS (≥30 kg) and 123 were treated with matching placebo + TCS
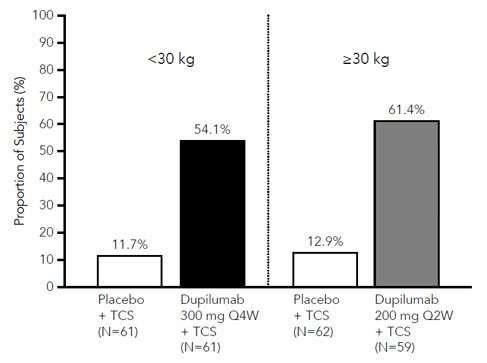
- AD-1539 which included 162 pediatric subjects 6 months to 5 years of age with moderate-to-severe AD. Of the 162 subjects, 83 were treated with DUPIXENT 200 mg Q4W + TCS (5 to <15 kg) or 300 mg Q4W + TCS (15 to <30 kg) and 79 subjects were assigned to be treated with matching placebo + TCS
- AD-1434, an open-label extension study that enrolled 275 pediatric subjects 12 to 17 years of age treated with DUPIXENT ± TCS, 368 pediatric subjects 6 to 11 years of age treated with DUPIXENT ± TCS, and 180 pediatric subjects 6 months to 5 years of age treated with DUPIXENT ± TCS
- Liberty-AD-HAFT which included 27 pediatric subjects 12 to 17 years of age with atopic dermatitis with moderate-to-severe hand and/or foot involvement treated with DUPIXENT (N=14) or matching placebo (N=13)
The safety and effectiveness were generally consistent between pediatric and adult patients [see Adverse Reactions (6.1) and Clinical Studies (14.1)]. In addition, hand-foot-and-mouth disease was reported in 9 (5%) pediatric subjects and skin papilloma was reported in 4 (2%) pediatric subjects 6 months to 5 years of age treated with DUPIXENT ± TCS in AD-1434. These cases did not lead to study drug discontinuation [see Adverse Reactions (6.1)].
Safety and effectiveness in pediatric patients younger than 6 months of age with AD have not been established.
Asthma
The safety and effectiveness of DUPIXENT for an add-on maintenance treatment in patients with moderate-to-severe asthma characterized by an eosinophilic phenotype or with oral corticosteroid dependent asthma have been established in pediatric patients 6 years of age and older. Use of DUPIXENT for this indication is supported by evidence from adequate and well-controlled studies in adult and pediatric patients 6 years and older [see Clinical Studies (14.2)].
Pediatric Subjects 12 to 17 Years of Age:
A total of 107 pediatric subjects 12 to 17 years of age with moderate-to-severe asthma were enrolled in QUEST and received either 200 mg (N=21) or 300 mg (N=18) DUPIXENT (or matching placebo either 200 mg [N=34] or 300 mg [N=34]) Q2W. Asthma exacerbations and lung function were assessed in both pediatric subjects 12 to 17 years of age and adults. For both the 200 mg and 300 mg Q2W doses, improvements in FEV1 (LS mean change from baseline at Week 12) were observed (0.36 L and 0.27 L, respectively). For the 200 mg Q2W dose, subjects had a reduction in the rate of severe exacerbations that was consistent with adults. Dupilumab exposure was higher in pediatric subjects 12 to 17 years of age than that in adults at the respective dose level which was mainly accounted for by difference in body weight [see Clinical Pharmacology (12.3)].
The adverse event profile in pediatric subjects 12 to 17 years of age was generally similar to the adults [see Adverse Reactions (6.1)].
Pediatric Subjects 6 to 11 Years of Age:
A total of 408 pediatric subjects 6 to 11 years of age with moderate-to-severe asthma were enrolled in VOYAGE, which evaluated doses of 100 mg Q2W or 200 mg Q2W. Improvement in asthma exacerbations and lung function were demonstrated [see Clinical Studies (14.2)]. The effectiveness of DUPIXENT 300 mg Q4W in subjects 6 to 11 years of age with body weight 15 to <30 kg was extrapolated from efficacy of 100 mg Q2W in VOYAGE with support from population pharmacokinetic analyses showing higher drug exposure levels with 300 mg Q4W [see Clinical Pharmacology (12.3)]. Subjects who completed the treatment period of the VOYAGE study could participate in the open-label extension study (LTS14424). Eighteen subjects (≥15 to <30 kg) out of 365 subjects were exposed to 300 mg Q4W in this study, and the safety profile in these eighteen subjects was consistent with that seen in VOYAGE. Additional safety for DUPIXENT 300 mg Q4W is based upon available safety information from the pediatric AD indication [see Adverse Reactions (6.1) and Clinical Pharmacology (12.3)].
Safety and effectiveness in pediatric patients younger than 6 years of age with asthma have not been established.
CRSwNP
Safety and effectiveness in pediatric patients younger than 18 years of age with CRSwNP have not been established.
EoE
The safety and effectiveness of DUPIXENT for the treatment of EoE have been established in pediatric subjects 1 year of age and older, weighing at least 15 kg. Use of DUPIXENT in this population is supported by an adequate well-controlled study in adults and 72 pediatric subjects 12 to 17 years of age (Study EoE-1), a clinical study in 61 pediatric subjects 1 to 11 years of age (Study EoE-2), and pharmacokinetic data in adult and pediatric subjects 1 to 17 years of age. The safety of DUPIXENT in pediatric subjects 1 to 17 years of age was similar to adults [see Adverse Reactions (6.1), Clinical Pharmacology (12.3), and Clinical Studies (14.4)].
Safety and effectiveness in pediatric patients younger than 1 year of age, or weighing less than 15 kg, with EoE have not been established.
8.5 Geriatric Use
Of the 1539 subjects with AD exposed to DUPIXENT in a dose-ranging study and placebo-controlled trials, 70 subjects were 65 years or older. Clinical trials of DUPIXENT in AD did not include sufficient numbers of subjects aged 65 years and over to determine whether they respond differently from younger subjects [see Clinical Pharmacology (12.3)].
Of the 1977 subjects with asthma exposed to DUPIXENT, a total of 240 subjects were 65 years or older. Efficacy and safety in this age group was similar to the overall study population.
Of the 440 subjects with CRSwNP exposed to DUPIXENT, a total of 79 subjects were 65 years or older. Efficacy and safety in this age group were similar to the overall study population.
Clinical studies of DUPIXENT in EoE did not include sufficient numbers of subjects aged 65 years and over to determine whether they respond differently from younger adult subjects.
Of the 152 subjects with PN exposed to DUPIXENT, a total of 37 were 65 years or older including 8 subjects 75 years or older. Clinical trials did not include a sufficient number of subjects 65 years of age and older to determine whether they respond differently from younger adult subjects.
- 10 OVERDOSAGE
-
11 DESCRIPTION
Dupilumab, an interleukin-4 receptor alpha antagonist, is a human monoclonal antibody of the IgG4 subclass that binds to the IL-4Rα subunit and inhibits IL-4 and IL-13 signaling. Dupilumab has an approximate molecular weight of 147 kDa.
Dupilumab is produced by recombinant DNA technology in Chinese Hamster Ovary cell suspension culture.
DUPIXENT (dupilumab) Injection is supplied as a sterile, preservative-free, clear to slightly opalescent, colorless to pale yellow solution for subcutaneous injection. DUPIXENT is provided as either a single-dose pre-filled syringe with needle shield or a single-dose pre-filled pen in a siliconized Type-1 clear glass syringe. The needle cap is not made with natural rubber latex.
Each 300 mg pre-filled syringe or pre-filled pen delivers 300 mg dupilumab in 2 mL which also contains L-arginine hydrochloride (10.5 mg), L-histidine (6.2 mg), polysorbate 80 (4 mg), sodium acetate (2 mg), sucrose (100 mg), and water for injection, pH 5.9.
Each 200 mg pre-filled syringe or pre-filled pen delivers 200 mg dupilumab in 1.14 mL which also contains L-arginine hydrochloride (12 mg), L-histidine (3.5 mg), polysorbate 80 (2.3 mg), sodium acetate (1.2 mg), sucrose (57 mg), and water for injection, pH 5.9.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Dupilumab is a human monoclonal IgG4 antibody that inhibits interleukin-4 (IL-4) and interleukin-13 (IL-13) signaling by specifically binding to the IL-4Rα subunit shared by the IL-4 and IL-13 receptor complexes. Dupilumab inhibits IL-4 signaling via the Type I receptor and both IL-4 and IL-13 signaling through the Type II receptor.
Inflammation driven by IL-4 and IL-13 is an important component in the pathogenesis of asthma, AD, CRSwNP, EoE, and PN. Multiple cell types that express IL-4Rα (e.g., mast cells, eosinophils, macrophages, lymphocytes, epithelial cells, goblet cells) and inflammatory mediators (e.g., histamine, eicosanoids, leukotrienes, cytokines, chemokines) are involved in inflammation. Blocking IL-4Rα with dupilumab inhibits IL-4 and IL-13 cytokine-induced inflammatory responses, including the release of proinflammatory cytokines, chemokines, nitric oxide, and IgE. The mechanism of dupilumab action has not been definitively established.
12.2 Pharmacodynamics
Consistent with inhibition of IL-4 and IL-13 signaling, dupilumab treatment decreased certain biomarkers of inflammation. In asthma subjects, fractional exhaled nitric oxide (FeNO) and circulating concentrations of eotaxin-3, total IgE, allergen specific IgE, TARC, and periostin were decreased relative to placebo. Reductions in these biomarkers were comparable for the 300 mg Q2W and 200 mg Q2W regimens. These markers were near maximal suppression after 2 weeks of treatment, except for IgE which declined more slowly. These effects were sustained throughout treatment. The median percent reduction from baseline in total IgE concentrations with dupilumab treatments was 52% at Week 24 (DRI12544) and 70% at Week 52 (QUEST). For FeNO, the mean percent reduction from baseline at Week 2 was 35% and 24% in DRI12544 and QUEST, respectively, and in the overall safety population, the mean FeNO level decreased to 20 ppb.
Antibody Response to Non-Live Vaccines During DUPIXENT Treatment
In a clinical study, adult subjects with AD were treated once weekly for 16 weeks with 300 mg of DUPIXENT (twice the recommended dosing frequency). After 12 weeks of administration, subjects received a Tdap vaccine and a meningococcal polysaccharide vaccine. Antibody responses to tetanus toxoid and serogroup C meningococcal polysaccharide were assessed 4 weeks later. Antibody responses to both tetanus toxoid and serogroup C meningococcal polysaccharide were similar in DUPIXENT-treated and placebo-treated subjects. Antibody responses to the other active components of both vaccines were not assessed. Antibody responses to other non-live vaccines were also not assessed.
12.3 Pharmacokinetics
The pharmacokinetics of dupilumab is similar in subjects with AD, asthma, CRSwNP, EoE and PN.
Absorption
Following an initial subcutaneous (SC) dose of 600 mg, 400 mg, or 300 mg, dupilumab reached peak mean ± SD concentrations (Cmax) of 70.1±24.1 mcg/mL, 41.8±12.4 mcg/mL, or 30.5±9.39 mcg/mL, respectively, by approximately 1 week post dose. Steady-state concentrations were achieved by Week 16 following the administration of 600 mg starting dose and 300 mg dose either weekly or Q2W, or 400 mg starting dose and 200 mg dose Q2W, or 300 mg Q2W without a loading dose. Across clinical trials, the mean ± SD steady-state trough concentrations ranged from 60.3±35.1 mcg/mL to 80.2±35.3 mcg/mL for 300 mg administered Q2W, from 173±75.9 mcg/mL to 195±71.7 mcg/mL for 300 mg administered weekly, and from 29.2±18.7 to 36.5±22.2 mcg/mL for 200 mg administered Q2W.
The bioavailability of dupilumab following a SC dose is similar between AD, asthma, CRSwNP, EoE, and PN subjects, ranging between 61% and 64%.
Elimination
The metabolic pathway of dupilumab has not been characterized. As a human monoclonal IgG4 antibody, dupilumab is expected to be degraded into small peptides and amino acids via catabolic pathways in the same manner as endogenous IgG. After the last steady-state dose of 300 mg QW, 300 mg Q2W, 200 mg Q2W, 300 mg Q4W, or 200 mg Q4W dupilumab, the median times to non-detectable concentration (<78 ng/mL) ranged from 9 to 13 weeks in adults and pediatric subjects 12 to 17 years of age. Population pharmacokinetic analyses indicate the median times to non-detectable concentration are approximately 1.5 times (up to 19 weeks) and 2.5 times (up to 32 weeks) longer in pediatric subjects 6 to 11 years of age and pediatric subjects 6 months to 5 years of age, respectively.
Dose Linearity
Dupilumab exhibited nonlinear target-mediated pharmacokinetics with exposures increasing in a greater than dose-proportional manner. The systemic exposure increased by 30-fold when the dose increased 8-fold following a single dose of dupilumab from 75 mg to 600 mg (i.e., 0.25-times to 2-times the recommended dose).
Immunogenicity
Development of antibodies to dupilumab was associated with lower serum dupilumab concentrations. A few subjects who had high antibody titers also had no detectable serum dupilumab concentrations.
Specific Populations
Age
Based on population pharmacokinetic analysis, age did not affect dupilumab clearance in adults and in pediatric subjects 6 to 17 years of age. In pediatric subjects 6 months to 5 years of age, clearance increased with age.
Geriatric Patients
In subjects who are 65 years and older, the mean ± SD steady-state trough concentrations of dupilumab were 69.4±31.4 mcg/mL and 166±62.3 mcg/mL, respectively, for 300 mg administered Q2W and weekly, and 39.7±21.7 mcg/mL for 200 mg administered Q2W.
Pediatric Patients
Atopic Dermatitis
For pediatric subjects 12 to 17 years of age with AD receiving every other week dosing (Q2W) with either 200 mg (<60 kg) or 300 mg (≥60 kg), the mean ± SD steady-state trough concentration of dupilumab was 54.5±27.0 mcg/mL.
For pediatric subjects 6 to 11 years of age with AD receiving every other week dosing (Q2W) with 200 mg (≥30 kg) or every four week dosing (Q4W) with 300 mg (<30 kg), mean ± SD steady-state trough concentration was 86.0±34.6 mcg/mL and 98.7±33.2 mcg/mL, respectively.
For pediatric subjects 6 months to 5 years of age with AD receiving every four week dosing (Q4W) with 300 mg (≥15 to <30 kg) or 200 mg (≥5 to <15 kg), the mean ± SD steady-state trough concentration was 110±42.8 mcg/mL and 109±50.8 mcg/mL, respectively.
Asthma
A total of 107 pediatric subjects 12 to 17 years of age with asthma were enrolled in QUEST. The mean ± SD steady-state trough concentrations of dupilumab were 107±51.6 mcg/mL and 46.7±26.9 mcg/mL, respectively, for 300 mg or 200 mg administered Q2W.
In VOYAGE, dupilumab pharmacokinetics was investigated in 270 subjects with moderate-to-severe asthma following subcutaneous administration of either 100 mg Q2W (for 91 pediatric subjects weighing <30 kg) or 200 mg Q2W (for 179 pediatric subjects weighing ≥30 kg). The mean ± SD steady-state trough concentration was 58.4±28.0 mcg/mL and 85.1±44.9 mcg/mL, respectively. Simulation of a 300 mg Q4W subcutaneous dose in pediatric subjects 6 to 11 years of age with body weight of ≥15 to <30 kg resulted in predicted steady-state trough concentrations (98.7±41.0 mcg/L) and average concentrations higher than the observed trough concentrations and average concentrations of 100 mg Q2W (<30 kg).
Eosinophilic Esophagitis
In Study EoE-1, dupilumab pharmacokinetics were investigated in 35 pediatric subjects 12 to 17 years of age, weighing at least 40 kg, with EoE, receiving 300 mg QW. The mean ± SD steady-state trough concentration of dupilumab was 227±95.3 mcg/mL.
In Study EoE-2 Part A, dupilumab pharmacokinetics were investigated in 20 pediatric subjects 1 to 11 years of age with EoE receiving the following weight-based dosing regimens: ≥15 to <30 kg (200 mg Q2W) and ≥30 to <40 kg (300 mg Q2W). At Week 16, the mean ± SD steady-state trough concentration of dupilumab was 174±66.2 mcg/mL.
The systemic exposure in pediatric subjects 1 to 11 years of age with a body weight ≥40 kg receiving 300 mg QW is expected to be comparable to adult and pediatric subjects 12 years and older with a body weight ≥40 kg. The systemic exposure in pediatric subjects 12 to 17 years of age with a body weight <40 kg receiving 300 mg Q2W is expected to be comparable to pediatric subjects 6 to 11 years of age.
Drug Interaction Studies
An effect of dupilumab on the PK of co-administered medications is not expected. Based on the population analysis, commonly co-administered medications had no effect on DUPIXENT pharmacokinetics in subjects with moderate-to-severe asthma.
Cytochrome P450 Substrates
The effects of dupilumab on the pharmacokinetics of midazolam (metabolized by CYP3A4), warfarin (metabolized by CYP2C9), omeprazole (metabolized by CYP2C19), metoprolol (metabolized by CYP2D6), and caffeine (metabolized by CYP1A2) were evaluated in a study with 12-13 evaluable subjects with AD (a SC loading dose of 600 mg followed by 300 mg SC weekly for six weeks). No clinically significant changes in AUC were observed. The largest effect was observed for metoprolol (CYP2D6) with an increase in AUC of 29%.
12.6 Immunogenicity
The observed incidence of anti-drug antibodies is highly dependent on the sensitivity and specificity of the assay. Differences in assay methods preclude meaningful comparisons of the incidence of anti-drug antibodies in the studies described below with the incidence of anti-drug antibodies in other studies, including those of DUPIXENT or of other dupilumab products.
Atopic Dermatitis
Approximately 6% of subjects with AD who received DUPIXENT 300 mg Q2W for 52 weeks developed antibodies to DUPIXENT; approximately 2% exhibited persistent ADA responses, and approximately 1% had neutralizing antibodies. Similar results were observed in pediatric subjects 6 months to 11 years of age with AD who received either DUPIXENT 200 mg Q2W, 200 mg Q4W, or 300 mg Q4W.
Approximately 16% of pediatric subjects 12 to 17 years of age with AD who received DUPIXENT 300 mg or 200 mg Q2W for 16 weeks developed antibodies to DUPIXENT; approximately 3% exhibited persistent ADA responses, and approximately 5% had neutralizing antibodies.
Asthma
Approximately 5% of subjects with asthma who received DUPIXENT 300 mg Q2W for 52 weeks developed antibodies to DUPIXENT; approximately 2% exhibited persistent ADA responses, and approximately 2% had neutralizing antibodies. Similar results were observed in pediatric subjects 6 to 11 years of age with asthma who received either DUPIXENT 100 mg Q2W or 200 mg Q2W up to 52 weeks.
Approximately 9% of subjects with asthma who received DUPIXENT 200 mg Q2W for 52 weeks developed antibodies to DUPIXENT; approximately 4% exhibited persistent ADA responses, and approximately 4% had neutralizing antibodies.
Chronic Rhinosinusitis with Nasal Polyposis
Approximately 5% of subjects with CRSwNP who received DUPIXENT 300 mg Q2W for 52 weeks developed antibodies to DUPIXENT; approximately 2% exhibited persistent ADA responses, and approximately 3% had neutralizing antibodies.
Eosinophilic Esophagitis
Approximately 1% of subjects with EoE who received DUPIXENT 300 mg QW for 52 weeks developed antibodies to DUPIXENT; no subjects exhibited persistent ADA responses or had neutralizing antibodies. Similar results were observed in pediatric subjects 1 to 11 years of age with EoE administered either DUPIXENT 200 mg Q2W or 300 mg Q2W for 52 weeks.
Prurigo Nodularis
Approximately 8% of subjects with PN who received DUPIXENT 300 mg Q2W for 24 weeks developed antibodies to DUPIXENT; approximately 1% exhibited persistent ADA responses, and approximately 3% had neutralizing antibodies.
The antibody titers detected in subjects who received DUPIXENT were mostly low. In subjects who received DUPIXENT, development of high titer antibodies to DUPIXENT was associated with lower serum dupilumab concentrations [see Clinical Pharmacology (12.3)].
Two adult subjects with AD who experienced high titer antibody responses developed serum sickness or serum sickness-like reactions during DUPIXENT therapy [see Warnings and Precautions (5.1)].
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Animal studies have not been conducted to evaluate the carcinogenic or mutagenic potential of dupilumab.
No effects on fertility parameters such as reproductive organs, menstrual cycle length, or sperm analysis were observed in sexually mature mice that were subcutaneously administered a homologous antibody against IL-4Rα at doses up to 200 mg/kg/week.
-
14 CLINICAL STUDIES
14.1 Atopic Dermatitis
Adults with Atopic Dermatitis
Three randomized, double-blind, placebo-controlled trials (SOLO 1 (NCT02277743), SOLO 2 (NCT02277769), and CHRONOS (NCT02260986)) enrolled a total of 2119 adult subjects 18 years of age and older with moderate-to-severe AD not adequately controlled by topical medication(s). Disease severity was defined by an Investigator's Global Assessment (IGA) score ≥3 in the overall assessment of AD lesions on a severity scale of 0 to 4, an Eczema Area and Severity Index (EASI) score ≥16 on a scale of 0 to 72, and a minimum body surface area involvement of ≥10%. At baseline, 59% of subjects were male, 67% were White, 52% of subjects had a baseline IGA score of 3 (moderate AD), and 48% of subjects had a baseline IGA of 4 (severe AD). The baseline mean EASI score was 33 and the baseline weekly averaged Peak Pruritus Numeric Rating Scale (NRS) was 7 on a scale of 0-10.
In all three trials, subjects in the DUPIXENT group received subcutaneous injections of DUPIXENT 600 mg at Week 0, followed by 300 mg every other week (Q2W). In the monotherapy trials (SOLO 1 and SOLO 2), subjects received DUPIXENT or placebo for 16 weeks.
In the concomitant therapy trial (CHRONOS), subjects received DUPIXENT or placebo with concomitant topical corticosteroids (TCS) and as needed topical calcineurin inhibitors for problem areas only, such as the face, neck, intertriginous and genital areas for 52 weeks.
All three trials assessed the primary endpoint, the change from baseline to Week 16 in the proportion of subjects with an IGA 0 (clear) or 1 (almost clear) and at least a 2-point improvement. Other endpoints included the proportion of subjects with EASI-75 (improvement of at least 75% in EASI score from baseline), and reduction in itch as defined by at least a 4-point improvement in the Peak Pruritus NRS from baseline to Week 16.
Clinical Response at Week 16 (SOLO 1, SOLO 2, and CHRONOS)
The results of the DUPIXENT monotherapy trials (SOLO 1 and SOLO 2) and the DUPIXENT with concomitant TCS trial (CHRONOS) are presented in Table 11.
Table 11: Efficacy Results of DUPIXENT with or without Concomitant TCS at Week 16 (FAS) in Adult Subjects 18 Years of Age and Older with Moderate-to-Severe AD SOLO 1 SOLO 2 CHRONOS DUPIXENT
300 mg Q2WPlacebo DUPIXENT
300 mg Q2WPlacebo DUPIXENT
300 mg Q2W + TCSPlacebo + TCS Number of subjects randomized (FAS)* 224 224 233 236 106 315 IGA 0 or 1†,‡ 38% 10% 36% 9% 39% 12% EASI-75‡ 51% 15% 44% 12% 69% 23% EASI-90‡ 36% 8% 30% 7% 40% 11% Number of subjects with baseline Peak Pruritus NRS score ≥4 213 212 225 221 102 299 Peak Pruritus NRS
(≥4-point improvement)‡41% 12% 36% 10% 59% 20% Figure 1: Proportion of Adult Subjects 18 Years of Age and Older with Moderate-to-Severe AD with ≥4-point Improvement on the Peak Pruritus NRS in SOLO 1* and SOLO 2* Studies (FAS)† SOLO 1 SOLO 2 
In CHRONOS, of the 421 subjects, 353 had been on study for 52 weeks at the time of data analysis. Of these 353 subjects, responders at Week 52 represent a mixture of subjects who maintained their efficacy from Week 16 (e.g., 53% of DUPIXENT IGA 0 or 1 responders at Week 16 remained responders at Week 52) and subjects who were non-responders at Week 16 who later responded to treatment (e.g., 24% of DUPIXENT IGA 0 or 1 non-responders at Week 16 became responders at Week 52). Results of supportive analyses of the 353 subjects in the DUPIXENT with concomitant TCS trial (CHRONOS) are presented in Table 12.
Table 12: Efficacy Results (IGA 0 or 1) of DUPIXENT with Concomitant TCS at Week 16 and 52 in Adult Subjects 18 Years of Age and Older with Moderate-to-Severe AD DUPIXENT
300 mg Q2W + TCSPlacebo + TCS - *
- In CHRONOS, of the 421 randomized and treated subjects, 68 subjects (16%) had not been on study for 52 weeks at the time of data analysis.
- †
- Responder was defined as a subject with an IGA 0 or 1 ("clear" or "almost clear") and a reduction of ≥2 points on a 0-4 IGA scale.
- ‡
- Subjects who received rescue treatment or with missing data were considered as non-responders.
Number of Subjects* 89 264 Responder†,‡ at Week 16 and 52 22% 7% Responder at Week 16 but Non-responder at Week 52 20% 7% Non-responder at Week 16 and Responder at Week 52 13% 6% Non-responder at Week 16 and 52 44% 80% Overall Responder†,‡ Rate at Week 52 36% 13% Treatment effects in subgroups (weight, age, gender, race, and prior treatment, including immunosuppressants) in SOLO 1, SOLO 2, and CHRONOS were generally consistent with the results in the overall study population.
In SOLO 1, SOLO 2, and CHRONOS, a third randomized treatment arm of DUPIXENT 300 mg QW did not demonstrate additional treatment benefit over DUPIXENT 300 mg Q2W.
Subjects in SOLO 1 and SOLO 2 who had an IGA 0 or 1 with a reduction of ≥2 points were re-randomized into SOLO CONTINUE (NCT02395133). SOLO CONTINUE evaluated multiple DUPIXENT monotherapy dose regimens for maintaining treatment response. The study included subjects randomized to continue with DUPIXENT 300 mg Q2W (62 subjects) or switch to placebo (31 subjects) for 36 weeks. IGA 0 or 1 responses at Week 36 were as follows: 33 (53%) in the Q2W group and 3 (10%) in the placebo group.
Pediatric Subjects 12 to 17 Years of Age with Atopic Dermatitis
The efficacy of DUPIXENT monotherapy in pediatric subjects 12 to 17 years of age was evaluated in a multicenter, randomized, double-blind, placebo-controlled trial (AD-1526; NCT03054428) in 251 pediatric subjects 12 to 17 years of age, with moderate-to-severe AD defined by an IGA score ≥3 (scale of 0 to 4), an EASI score ≥16 (scale of 0 to 72), and a minimum BSA involvement of ≥10%. Eligible subjects enrolled into this trial had previous inadequate response to topical medication.
Subjects in the DUPIXENT group with baseline weight of <60 kg received an initial dose of 400 mg at Week 0, followed by 200 mg Q2W for 16 weeks. Subjects with baseline weight of ≥60 kg received an initial dose of 600 mg at Week 0, followed by 300 mg Q2W for 16 weeks. Subjects were permitted to receive rescue treatment at the discretion of the investigator. Subjects who received rescue treatment were considered non-responders.
In AD-1526, the mean age was 14.5 years, the median weight was 59.4 kg, 41% of subjects were female, 63% were White, 15% were Asian, and 12% were Black. At baseline, 46% of subjects had an IGA score of 3 (moderate AD), 54% had an IGA score of 4 (severe AD), the mean BSA involvement was 57%, and 42% had received prior systemic immunosuppressants. Also, at baseline, the mean EASI score was 36, and the weekly averaged Peak Pruritus NRS was 8 on a scale of 0-10. Overall, 92% of subjects had at least one co-morbid allergic condition; 66% had allergic rhinitis, 54% had asthma, and 61% had food allergies.
The primary endpoint was the proportion of subjects with an IGA 0 (clear) or 1 (almost clear) and at least a 2-point improvement from baseline to Week 16. Other evaluated outcomes included the proportion of subjects with EASI-75 or EASI-90 (improvement of at least 75% or 90% in EASI from baseline, respectively), and reduction in itch as measured by the Peak Pruritus NRS (≥4-point improvement).
The efficacy results at Week 16 for AD-1526 are presented in Table 13.
Table 13: Efficacy Results of DUPIXENT in AD-1526 at Week 16 (FAS)* in Pediatric Subjects 12 to 17 Years of Age with Moderate-to-Severe AD DUPIXENT†
200 mg (<60 kg) or 300 mg (≥60 kg) Q2W
N=82*Placebo
N=85*- *
- Full Analysis Set (FAS) includes all subjects randomized.
- †
- At Week 0, subjects received 400 mg (baseline weight <60 kg) or 600 mg (baseline weight ≥60 kg) of DUPIXENT.
- ‡
- Responder was defined as a subject with an IGA 0 or 1 ("clear" or "almost clear") and a reduction of ≥2 points on a 0-4 IGA scale.
- §
- Subjects who received rescue treatment or with missing data were considered as non-responders (59% and 21% in the placebo and DUPIXENT arms, respectively).
IGA 0 or 1‡,§ 24% 2% EASI-75§ 42% 8% EASI-90§ 23% 2% Peak Pruritus NRS (≥4-point improvement)§ 37% 5% A greater proportion of subjects randomized to DUPIXENT achieved an improvement in the Peak Pruritus NRS compared to placebo (defined as ≥4-point improvement at Week 4). See Figure 2.
Pediatric Subjects 6 to 11 Years of Age with Atopic Dermatitis
The efficacy and safety of DUPIXENT use concomitantly with TCS in pediatric subjects was evaluated in a multicenter, randomized, double-blind, placebo-controlled trial (AD-1652; NCT03345914) in 367 subjects 6 to 11 years of age, with AD defined by an IGA score of 4 (scale of 0 to 4), an EASI score ≥21 (scale of 0 to 72), and a minimum BSA involvement of ≥15%. Eligible subjects enrolled into this trial had previous inadequate response to topical medication. Enrollment was stratified by baseline weight (<30 kg; ≥30 kg).
Subjects in the DUPIXENT Q4W + TCS group received an initial dose of 600 mg on Day 1, followed by 300 mg Q4W from Week 4 to Week 12, regardless of weight. Subjects in the DUPIXENT Q2W + TCS group with baseline weight of <30 kg received an initial dose of 200 mg on Day 1, followed by 100 mg Q2W from Week 2 to Week 14, and subjects with baseline weight of ≥30 kg received an initial dose of 400 mg on Day 1, followed by 200 mg Q2W from Week 2 to Week 14. Subjects were permitted to receive rescue treatment at the discretion of the investigator. Subjects who received rescue treatment were considered non-responders.
In AD-1652, the mean age was 8.5 years, the median weight was 29.8 kg, 50% of subjects were female, 69% were White, 17% were Black, and 8% were Asian. At baseline, the mean BSA involvement was 58%, and 17% had received prior systemic non-steroidal immunosuppressants. Also, at baseline the mean EASI score was 37.9, and the weekly average of daily worst itch score was 7.8 on a scale of 0-10. Overall, 92% of subjects had at least one co-morbid allergic condition; 64% had food allergies, 63% had other allergies, 60% had allergic rhinitis, and 47% had asthma.
The primary endpoint was the proportion of subjects with an IGA 0 (clear) or 1 (almost clear) at Week 16. Other evaluated outcomes included the proportion of subjects with EASI-75 or EASI-90 (improvement of at least 75% or 90% in EASI from baseline, respectively), and reduction in itch as measured by the Peak Pruritus NRS (≥4-point improvement).
Table 14 presents the results by baseline weight strata for the approved dose regimens.
Table 14: Efficacy Results of DUPIXENT with Concomitant TCS in AD-1652 at Week 16 (FAS)* in Pediatric Subjects 6 to 11 Years of Age with AD DUPIXENT
300 mg Q4W† + TCSPlacebo + TCS DUPIXENT
200 mg Q2W‡ + TCSPlacebo + TCS (N=61) (N=61) (N=59) (N=62) <30 kg <30 kg ≥30 kg ≥30 kg - *
- Full Analysis Set (FAS) includes all subjects randomized.
- †
- At Day 1, subjects received 600 mg of DUPIXENT.
- ‡
- At Day 1, subjects received 200 mg (baseline weight <30 kg) or 400 mg (baseline weight ≥30 kg) of DUPIXENT.
- §
- Responder was defined as a subject with an IGA 0 or 1 ("clear" or "almost clear").
- ¶
- Subjects who received rescue treatment or with missing data were considered as non-responders.
IGA 0 or 1§,¶ 30% 13% 39% 10% EASI-75¶ 75% 28% 75% 26% EASI-90¶ 46% 7% 36% 8% Peak Pruritus NRS (≥4-point improvement)¶ 54% 12% 61% 13% A greater proportion of subjects randomized to DUPIXENT + TCS achieved an improvement in the Peak Pruritus NRS compared to placebo + TCS (defined as ≥4-point improvement at Week 16). See Figure 3.
Pediatric Subjects 6 Months to 5 Years of Age with Atopic Dermatitis
The efficacy and safety of DUPIXENT use concomitantly with TCS in pediatric subjects was evaluated in a multicenter, randomized, double-blind, placebo-controlled trial (AD-1539; NCT03346434) in 162 subjects 6 months to 5 years of age, with moderate-to-severe AD defined by an IGA score ≥3 (scale of 0 to 4), an EASI score ≥16 (scale of 0 to 72), and a minimum BSA involvement of ≥10%. Eligible subjects enrolled into this trial had previous inadequate response to topical medication. Enrollment was stratified by baseline weight (≥5 to <15 kg and ≥15 to <30 kg).
Subjects in the DUPIXENT Q4W + TCS group with baseline weight of ≥5 to <15 kg received an initial dose of 200 mg on Day 1, followed by 200 mg Q4W from Week 4 to Week 12, and subjects with baseline weight of ≥15 to <30 kg received an initial dose of 300 mg on Day 1, followed by 300 mg Q4W from Week 4 to Week 12. Subjects were permitted to receive rescue treatment at the discretion of the investigator. Subjects who received rescue treatment were considered non-responders.
In AD-1539, the mean age was 3.8 years, the median weight was 16.5 kg, 39% of subjects were female, 69% were White, 19% were Black, and 6% were Asian. At baseline, the mean BSA involvement was 58%, and 29% of subjects had received prior systemic immunosuppressants. Also, at baseline the mean EASI score was 34.1, and the weekly average of daily worst scratch/itch score was 7.6 on a scale of 0-10. Overall, 81.4% of subjects had at least one co-morbid allergic condition; 68.3% had food allergies, 52.8% had other allergies, 44.1% had allergic rhinitis, and 25.5% had asthma.
The primary endpoint was the proportion of subjects with an IGA 0 (clear) or 1 (almost clear) at Week 16. Other evaluated outcomes included the proportion of subjects with EASI-75 or EASI-90 (improvement of at least 75% or 90% in EASI from baseline, respectively), and reduction in itch as measured by the Worst Scratch/Itch NRS (≥4-point improvement).
The efficacy results at Week 16 for AD-1539 are presented in Table 15.
Table 15: Efficacy Results of DUPIXENT with Concomitant TCS in AD-1539 at Week 16 (FAS)* in Pediatric Subjects 6 Months to 5 Years of Age with Moderate-to-Severe AD DUPIXENT
+ TCS
200 mg (5 to <15 kg) or 300 mg (15 to <30 kg) Q4W†Placebo
+ TCSDifference vs. Placebo (95 % CI) (N=83)* (N=79)* CI = confidence interval - *
- Full Analysis Set (FAS) includes all subjects randomized.
- †
- At Day 1, subjects received 200 mg (5 to <15 kg) or 300 mg (15 to <30 kg) of DUPIXENT.
- ‡
- Responder was defined as a subject with an IGA 0 or 1 ("clear" or "almost clear").
- §
- Subjects who received rescue treatment (63% and 19% in the placebo and DUPIXENT arms, respectively) or with missing data were considered as non-responders.
IGA 0 or 1‡,§ 28% 4% 24% (13%, 34%) EASI-75§ 53% 11% 42% (29%, 55%) EASI-90§ 25% 3% 23% (12%, 33%) Worst Scratch/Itch NRS (≥4-point improvement)§ 48% 9% 39% (26%, 52%) Atopic Dermatitis with Hand and/or Foot Involvement
The efficacy and safety of DUPIXENT was evaluated in a 16-week, multicenter, randomized, double-blind, parallel-group, placebo-controlled trial (Liberty-AD-HAFT; NCT04417894) in 133 adult and pediatric subjects 12 to 17 years of age with atopic dermatitis with moderate-to-severe hand and/or foot involvement, defined by an established diagnosis of atopic dermatitis and screening to rule out irritant and allergic contact dermatitis through history and appropriate patch testing, and by an IGA (hand and foot) score ≥3 (scale of 0 to 4) and a hand and foot Peak Pruritus Numeric Rating Scale (NRS) score for maximum itch intensity ≥4 (scale of 0 to 10). Fifty-three (53) percent (N=70/133) of the subjects also had moderate-to-severe AD outside of the hands or feet (IGA global ≥3). Eligible subjects had previous inadequate response or intolerance to treatment of hand and/or foot dermatitis with topical AD medications. In this trial 67 subjects received DUPIXENT, and 66 subjects received placebo. DUPIXENT-treated subjects received the recommended dosage based on their age and body weight [see Dosage and Administration (2.3)]. Subjects were not allowed concomitant use of topical treatments for AD on the hands and feet during the trial, but were allowed the use of topical treatments for AD on other parts of the body with certain restrictions.
In Liberty-AD-HAFT, 38% of subjects were male, 80% were White, 13% were Asian, and 5% were Black or African American. For ethnicity, 4% were identified as Hispanic or Latino and 96% were identified as not Hispanic or Latino. Seventy-two (72) percent (N=96/133) of subjects had a baseline IGA (hand and foot) score of 3 (atopic dermatitis with moderate hand and/or foot involvement), and 28% (N=37/133) of subjects had a baseline IGA (hand and foot) score of 4 (atopic dermatitis with severe hand and/or foot involvement). The baseline weekly averaged hand and foot Peak Pruritus NRS score was 7.1.
The primary endpoint was the proportion of subjects with an IGA hand and foot score of 0 (clear) or 1 (almost clear) at Week 16. The key secondary endpoint was reduction of itch as measured by the hand and foot Peak Pruritus NRS (≥4-point improvement).
The efficacy results at Week 16 for Liberty-AD-HAFT are presented in Table 16.
Table 16: Efficacy Results of DUPIXENT in Liberty-AD-HAFT at Week 16 (FAS)* in Adult and Pediatric Subjects 12 to 17 Years of Age with AD with Moderate-to-Severe Hand and/or Foot Involvement DUPIXENT
200/300 mg Q2W†Placebo Difference vs. Placebo (95 % CI) (N=67)* (N=66)* CI = confidence interval - *
- Full Analysis Set (FAS) includes all subjects randomized.
- †
- Adults received a loading dose of DUPIXENT 600 mg SC followed by 300 mg SC Q2W. Pediatric subjects 12 to 17 years of age received a loading dose of DUPIXENT 600 mg SC followed by 300 mg SC Q2W (for body weight ≥60 kg) or a loading dose of DUPIXENT 400 mg SC followed by 200 mg SC Q2W (for body weight <60 kg).
- ‡
- Responder was defined as a subject with an IGA 0 or 1 ("clear" or "almost clear").
- §
- Subjects who received rescue treatment (21% and 3% in the placebo and DUPIXENT arms, respectively) or with missing data were considered as non-responders.
IGA (hand and foot) 0 or 1‡,§ 40% 17% 24% (9%, 38%) Improvement (reduction) of weekly averaged hand and foot Peak Pruritus NRS ≥4§ 52% 14% 39% (24%, 53%) 14.2 Asthma
The asthma development program for patients aged 12 years and older included three randomized, double-blind, placebo-controlled, parallel-group, multicenter trials (DRI12544 (NCT01854047), QUEST (NCT02414854), and VENTURE (NCT02528214)) of 24 to 52 weeks in treatment duration which enrolled a total of 2888 subjects. Subjects enrolled in DRI12544 and QUEST were required to have a history of 1 or more asthma exacerbations that required treatment with systemic corticosteroids or emergency department visit or hospitalization for the treatment of asthma in the year prior to trial entry. Subjects enrolled in VENTURE required dependence on daily oral corticosteroids in addition to regular use of high-dose inhaled corticosteroids plus an additional controller(s). In all 3 trials, subjects were enrolled without requiring a minimum baseline blood eosinophil count. In QUEST and VENTURE, subjects with screening blood eosinophil level of >1500 cells/mcL (<1.3%) were excluded. DUPIXENT was administered as add-on to background asthma treatment. Subjects continued background asthma therapy throughout the duration of the studies, except in VENTURE in which OCS dose was tapered as described below.
DRI12544
DRI12544 was a 24-week dose-ranging study which included 776 adult subjects (18 years of age and older). DUPIXENT compared with placebo was evaluated in adult subjects with moderate-to-severe asthma on a medium or high-dose inhaled corticosteroid and a long acting beta agonist. Subjects were randomized to receive either 200 mg (N=150) or 300 mg (N=157) DUPIXENT every other week (Q2W) or 200 mg (N=154) or 300 mg (N=157) DUPIXENT every 4 weeks following an initial dose of 400 mg, 600 mg or placebo (N=158), respectively. The primary endpoint was mean change from baseline to Week 12 in FEV1 (L) in subjects with baseline blood eosinophils ≥300 cells/mcL. Other endpoints included percent change from baseline in FEV1 and annualized rate of severe asthma exacerbation events during the 24-week placebo-controlled treatment period. Results were evaluated in the overall population and subgroups based on baseline blood eosinophil count (≥300 cells/mcL and <300 cells/mcL). Additional secondary endpoints included responder rates in the patient reported Asthma Control Questionnaire (ACQ-5) and Asthma Quality of Life Questionnaire, Standardized Version (AQLQ(S)) scores.
QUEST
QUEST was a 52-week study which included 1902 adult and pediatric subjects (12 years of age and older). DUPIXENT compared with placebo was evaluated in 107 pediatric subjects 12 to 17 years of age and 1795 adult subjects with moderate-to-severe asthma on a medium or high-dose inhaled corticosteroid (ICS) and a minimum of one and up to two additional controller medications. Subjects were randomized to receive either 200 mg (N=631) or 300 mg (N=633) DUPIXENT Q2W (or matching placebo for either 200 mg [N=317] or 300 mg [N=321] Q2W) following an initial dose of 400 mg, 600 mg or placebo, respectively. The primary endpoints were the annualized rate of severe exacerbation events during the 52-week placebo-controlled period and change from baseline in pre-bronchodilator FEV1 at Week 12 in the overall population (unrestricted by minimum baseline blood eosinophils count). Additional secondary endpoints included annualized severe exacerbation rates and FEV1 in subjects with different baseline levels of blood eosinophils as well as responder rates in the ACQ-5 and AQLQ(S) scores.
VENTURE
VENTURE was a 24-week oral corticosteroid-reduction study in 210 adult and pediatric subjects 15 years of age and older with asthma who required daily oral corticosteroids in addition to regular use of high dose inhaled corticosteroids plus an additional controller. After optimizing the OCS dose during the screening period, subjects received 300 mg DUPIXENT (N=103) or placebo (N=107) once Q2W for 24 weeks following an initial dose of 600 mg or placebo. Subjects continued to receive their existing asthma medicine during the study; however, their OCS dose was reduced every 4 weeks during the OCS reduction phase (Week 4-20), as long as asthma control was maintained. The primary endpoint was the percent reduction of oral corticosteroid dose at Weeks 20 to 24 compared with the baseline dose, while maintaining asthma control in the overall population (unrestricted by minimum baseline blood eosinophils count). Additional secondary endpoints included the annualized rate of severe exacerbation events during treatment period and responder rate in the ACQ-5 and AQLQ(S) scores.
The demographics and baseline characteristics of these 3 trials are provided in Table 17 below.
Table 17: Demographics and Baseline Characteristics of Asthma Trials Parameter DRI12544
(N=776)QUEST
(N=1902)VENTURE
(N=210)ICS = inhaled corticosteroid; FEV1 = Forced expiratory volume in 1 second; AD = atopic dermatitis; NP = nasal polyposis; AR = allergic rhinitis; FeNO = fraction of exhaled nitric oxide Mean age (years) (SD) 49 (13) 48 (15) 51 (13) % Female 63 63 61 % White 78 83 94 Duration of Asthma (years), mean (± SD) 22 (15) 21 (15) 20 (14) Never smoked (%) 77 81 81 Mean exacerbations in previous year (± SD) 2.2 (2.1) 2.1 (2.2) 2.1 (2.2) High dose ICS use (%) 50 52 89 Pre-dose FEV1 (L) at baseline (± SD) 1.84 (0.54) 1.78 (0.60) 1.58 (0.57) Mean percent predicted FEV1 at baseline (%) (± SD) 61 (11) 58 (14) 52 (15) % Reversibility (± SD) 27 (15) 26 (22) 19 (23) Atopic Medical History % Overall
(AD %, NP %, AR %)73
(8, 11, 62)78
(10, 13, 69)72
(8, 21, 56)Mean FeNO ppb (± SD) 39 (35) 35 (33) 38 (31) Mean total IgE IU/mL (± SD) 435 (754) 432 (747) 431 (776) Mean baseline blood Eosinophil count (± SD) cells/mcL 350 (430) 360 (370) 350 (310) Exacerbations
DRI12544 and QUEST evaluated the frequency of severe asthma exacerbations defined as deterioration of asthma requiring the use of systemic corticosteroids for at least 3 days or hospitalization or emergency room visit due to asthma that required systemic corticosteroids. In the primary analysis population (subjects with baseline blood eosinophil count of ≥300 cells/mcL in DRI12544 and the overall population in QUEST), subjects receiving either DUPIXENT 200 mg or 300 mg Q2W had significant reductions in the rate of asthma exacerbations compared to placebo. In the overall population in QUEST, the rate of severe exacerbations was 0.46 and 0.52 for DUPIXENT 200 mg Q2W and 300 mg Q2W, respectively, compared to matched placebo rates of 0.87 and 0.97. The rate ratio of severe exacerbations compared to placebo was 0.52 (95% CI: 0.41, 0.66) and 0.54 (95% CI: 0.43, 0.68) for DUPIXENT 200 mg Q2W and 300 mg Q2W, respectively. Results in subjects with baseline blood eosinophil counts ≥300 cells/mcL in DRI12544 and QUEST are shown in Table 18.
Response rates by baseline blood eosinophils and baseline FeNO for QUEST are shown for the overall population in Figure 4 and Figure 5, respectively. Elevation of FeNO can be a marker of the eosinophilic asthma phenotype when supported by clinical data. Pre-specified subgroup analyses of DRI12544 and QUEST demonstrated that there were greater reductions in severe exacerbations in subjects with higher baseline blood eosinophil levels (≥150 cells/mcL) or FeNO (≥25 ppb). In QUEST, reductions in exacerbations were significant in the subgroup of subjects with baseline blood eosinophils ≥150 cells/mcL. In subjects with baseline blood eosinophil count <150 cells/mcL and FeNO <25 ppb, similar severe exacerbation rates were observed between DUPIXENT and placebo.
In QUEST, the estimated rate ratio of exacerbations leading to hospitalizations and/or emergency room visits versus placebo was 0.53 (95% CI: 0.28, 1.03) and 0.74 (95% CI: 0.32, 1.70) with DUPIXENT 200 mg or 300 mg Q2W, respectively.
Table 18: Rate of Severe Exacerbations in DRI12544 and QUEST Trial Treatment Baseline Blood EOS ≥300 cells/mcL
(primary analysis population, DRI12544)N Rate
(95% CI)Rate Ratio
(95% CI)DRI12544 DUPIXENT
200 mg Q2W65 0.30
(0.13, 0.68)0.29
(0.11, 0.76)DUPIXENT
300 mg Q2W64 0.20
(0.08, 0.52)0.19
(0.07, 0.56)Placebo 68 1.04
(0.57, 1.90)QUEST DUPIXENT
200 mg Q2W264 0.37
(0.29, 0.48)0.34
(0.24, 0.48)Placebo 148 1.08
(0.85, 1.38)DUPIXENT
300 mg Q2W277 0.40
(0.32, 0.51)0.33
(0.23, 0.45)Placebo 142 1.24
(0.97, 1.57)Figure 4: Relative Risk in Annualized Event Rate of Severe Exacerbations across Baseline Blood Eosinophil Count (cells/mcL) in Subjects with Moderate-to-Severe Asthma (QUEST)
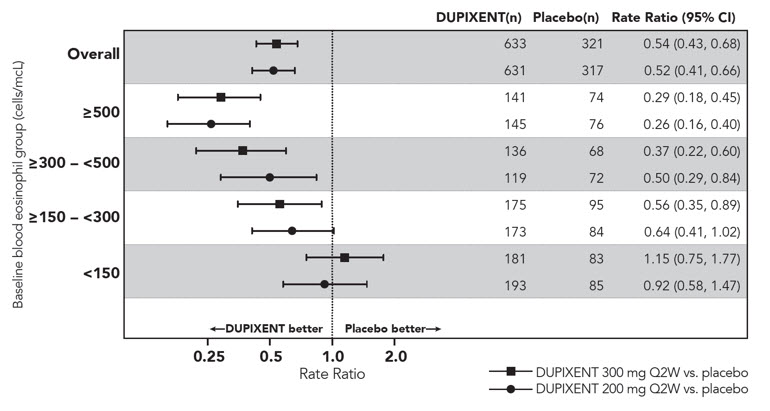
Figure 5: Relative Risk in Annualized Event Rate of Severe Exacerbations across Baseline FeNO Group (ppb) in Subjects with Moderate-to-Severe Asthma (QUEST)
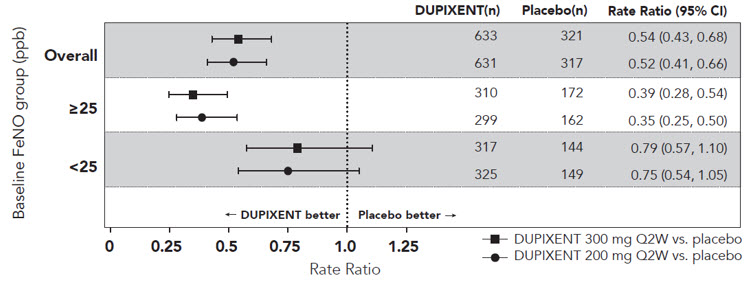
The time to first exacerbation was longer for the subjects receiving DUPIXENT compared to placebo in QUEST (Figure 6).
Lung Function
Significant increases in pre-bronchodilator FEV1 were observed at Week 12 for DRI12544 and QUEST in the primary analysis populations (subjects with baseline blood eosinophil count of ≥300 cells/mcL in DRI12544 and the overall population in QUEST). In the overall population in QUEST, the FEV1 LS mean change from baseline was 0.32 L (21%) and 0.34 L (23%) for DUPIXENT 200 mg Q2W and 300 mg Q2W, respectively, compared to matched placebo means of 0.18 L (12%) and 0.21 L (14%). The mean treatment difference versus placebo was 0.14 L (95% CI: 0.08, 0.19) and 0.13 L (95% CI: 0.08, 0.18) for DUPIXENT 200 mg Q2W and 300 mg Q2W, respectively. Results in subjects with baseline blood eosinophil counts ≥300 cells/mcL in DRI12544 and QUEST are shown in Table 19.
Improvements in FEV1 by baseline blood eosinophils and baseline FeNO for QUEST are shown in Figure 7 and 8, respectively. Subgroup analysis of DRI12544 and QUEST demonstrated greater improvement in subjects with higher baseline blood eosinophils (≥150 cells/mcL) or FeNO (≥25 ppb). In subjects with baseline blood eosinophil count <150 cells/mcL and FeNO <25 ppb, similar differences in FEV1 were observed between DUPIXENT and placebo.
Mean changes in FEV1 over time in QUEST are shown in Figure 9.
Table 19: Mean Change from Baseline and Difference vs Placebo in Pre-Bronchodilator FEV1 at Week 12 in Subjects with Moderate-to-Severe Asthma (DRI12544 and QUEST) Trial Treatment Baseline Blood EOS ≥300 cells/mcL
(primary analysis population, DRI12544)N LS Mean Change from baseline
L (%)LS Mean Difference vs. placebo
(95% CI)DRI12544 DUPIXENT
200 mg Q2W65 0.43 (25.9) 0.26
(0.11, 0.40)DUPIXENT
300 mg Q2W64 0.39 (25.8)
0.21
(0.06, 0.36)Placebo 68 0.18 (10.2) QUEST DUPIXENT
200 mg Q2W264 0.43 (29.0) 0.21
(0.13, 0.29)Placebo 148 0.21 (15.6) DUPIXENT
300 mg Q2W277 0.47 (32.5) 0.24
(0.16, 0.32)Placebo 142 0.22 (14.4) Figure 7: LS Mean Difference in Change from Baseline vs Placebo to Week 12 in Pre-Bronchodilator FEV1 across Baseline Blood Eosinophil Counts (cells/mcL) in Subjects with Moderate-to-Severe Asthma (QUEST)
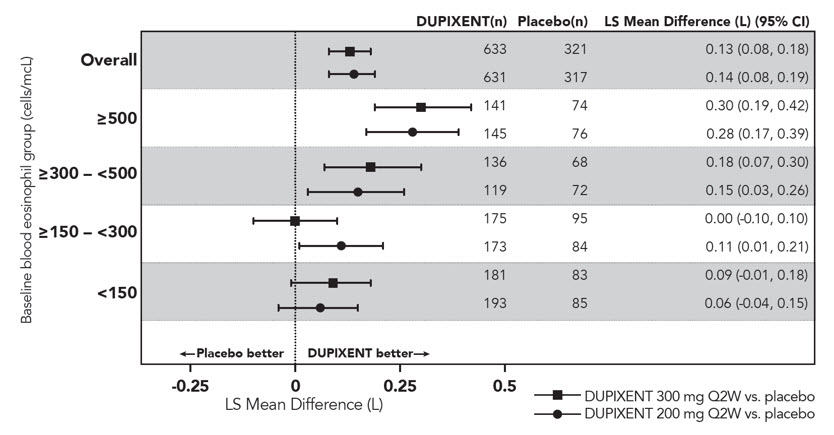
Figure 8: LS Mean Difference in Change from Baseline vs Placebo to Week 12 in Pre-bronchodilator FEV1 across Baseline FeNO (ppb) in Subjects with Moderate-to-Severe Asthma (QUEST)
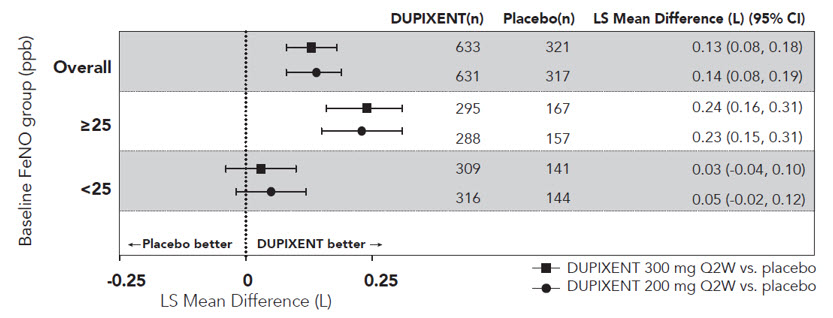
Figure 9: Mean Change from Baseline in Pre-Bronchodilator FEV1 (L) Over Time in Subjects with Moderate-to-Severe Asthma with Baseline Blood Eosinophils ≥300 cells/mcL (QUEST)
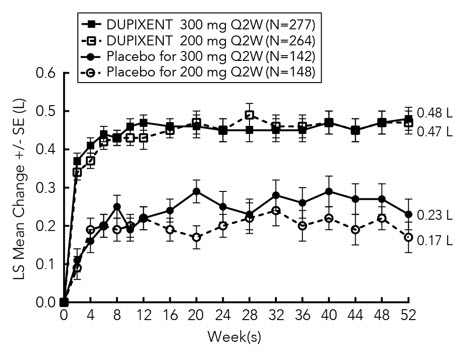
Additional Secondary Endpoints
ACQ-5 and AQLQ(S) were assessed in QUEST at 52 weeks. The responder rate was defined as an improvement in score of 0.5 or more (scale range 0-6 for ACQ-5 and 1-7 for AQLQ(S)).
- The ACQ-5 responder rate for DUPIXENT 200 mg and 300 mg Q2W in the overall population was 69% vs 62% placebo (odds ratio 1.37; 95% CI: 1.01, 1.86) and 69% vs 63% placebo (odds ratio 1.28; 95% CI: 0.94, 1.73), respectively; and the AQLQ(S) responder rates were 62% vs 54% placebo (odds ratio 1.61; 95% CI: 1.17, 2.21) and 62% vs 57% placebo (odds ratio 1.33; 95% CI: 0.98, 1.81), respectively.
- The ACQ-5 responder rate for DUPIXENT 200 mg and 300 mg Q2W in subjects with baseline blood eosinophils ≥300 cells/mcL was 75% vs 67% placebo (odds ratio: 1.46; 95% CI: 0.90, 2.35) and 71% vs 64% placebo (odds ratio: 1.39; 95% CI: 0.88, 2.19), respectively; and the AQLQ(S) responder rates were 71% vs 55% placebo (odds ratio: 2.02; 95% CI: 1.24, 3.32) and 65% vs 55% placebo (odds ratio: 1.79; 95% CI: 1.13, 2.85), respectively.
Oral Corticosteroid Reduction (VENTURE)
VENTURE evaluated the effect of DUPIXENT on reducing the use of maintenance oral corticosteroids. The baseline mean oral corticosteroid dose was 12 mg in the placebo group and 11 mg in the group receiving DUPIXENT. The primary endpoint was the percent reduction from baseline of the final oral corticosteroid dose at Week 24 while maintaining asthma control.
Compared with placebo, subjects receiving DUPIXENT achieved greater reductions in daily maintenance oral corticosteroid dose, while maintaining asthma control. The mean percent reduction in daily OCS dose from baseline was 70% (median 100%) in subjects receiving DUPIXENT (95% CI: 60%, 80%) compared to 42% (median 50%) in subjects receiving placebo (95% CI: 33%, 51%). Reductions of 50% or higher in the OCS dose were observed in 82 (80%) subjects receiving DUPIXENT compared to 57 (53%) in those receiving placebo. The proportion of subjects with a mean final dose less than 5 mg at Week 24 was 72% for DUPIXENT and 37% for placebo (odds ratio 4.48 95% CI: 2.39, 8.39). A total of 54 (52%) subjects receiving DUPIXENT versus 31 (29%) subjects in the placebo group had a 100% reduction in their OCS dose.
In this 24-week trial, asthma exacerbations (defined as a temporary increase in oral corticosteroid dose for at least 3 days) were lower in subjects receiving DUPIXENT compared with those receiving placebo (annualized rate 0.65 and 1.60 for the DUPIXENT and placebo group, respectively; rate ratio 0.41 [95% CI 0.26, 0.63]) and improvement in pre-bronchodilator FEV1 from baseline to Week 24 was greater in subjects receiving DUPIXENT compared with those receiving placebo (LS mean difference for DUPIXENT versus placebo of 0.22 L [95% CI: 0.09 to 0.34 L]). Effects on lung function and on oral steroid and exacerbation reduction were similar irrespective of baseline blood eosinophil levels. The ACQ-5 and AQLQ(S) were also assessed in VENTURE and showed improvements similar to those in QUEST.
Pediatric Subjects 6 to 11 Years of Age with Asthma
The efficacy and safety of DUPIXENT in pediatric subjects was evaluated in a 52-week multicenter, randomized, double-blind, placebo-controlled study (VOYAGE; NCT02948959) in 408 subjects 6 to 11 years of age, with moderate-to-severe asthma on a medium or high-dose ICS and a second controller medication or high-dose ICS alone. Subjects were required to have a history of 1 or more asthma exacerbation(s) that required treatment with systemic corticosteroids or emergency department visit or hospitalization for the treatment of asthma in the year prior to trial entry. Subjects were randomized to DUPIXENT (N=273) or matching placebo (N=135) every other week based on body weight <30 kg (100 mg Q2W) or ≥30 kg (200 mg Q2W). The effectiveness of DUPIXENT 300 mg Q4W was extrapolated from efficacy of 100 mg Q2W in VOYAGE with support from population pharmacokinetic analyses showing higher drug exposure levels with 300 mg Q4W [see Pediatric Use (8.4) and Pharmacokinetics (12.3)].
The primary endpoint was the annualized rate of severe asthma exacerbation events during the 52-week placebo-controlled period. Severe asthma exacerbations were defined as deterioration of asthma requiring the use of systemic corticosteroids for at least 3 days or hospitalization or emergency room visit due to asthma that required systemic corticosteroids. The key secondary endpoint was the change from baseline in pre-bronchodilator FEV1 percent predicted at Week 12. Additional secondary endpoints included mean change from baseline and responder rates in the ACQ-7-IA (Asthma Control Questionnaire-7-Interviewer Administered) and PAQLQ(S)-IA (Pediatric Asthma Quality of Life Questionnaire with Standardized Activities Interviewer Administered) scores.
The demographics and baseline characteristics for VOYAGE are provided in Table 20 below.
Table 20: Demographics and Baseline Characteristics for VOYAGE Parameter VOYAGE
(N=408)ICS = inhaled corticosteroid; FEV1 = Forced expiratory volume in 1 second; AD = atopic dermatitis; AR = allergic rhinitis; FeNO = fraction of exhaled nitric oxide Mean age (years) (SD) 9 (2) % Female 36 % White 88 Mean body weight (kg) 36 Mean exacerbations in previous year (± SD) 2.4 (2.2) High dose ICS use (%) 44 Pre-dose FEV1 (L) at baseline (± SD) 1.48 (0.41) Mean percent predicted FEV1 (%) (±SD) 78 (15) Mean % Reversibility (± SD) 20 (21) Atopic Medical History % Overall
(AD %, AR %)92
(36, 82)Mean FeNO ppb (± SD) 28 (24) % subjects with FeNO ppb ≥20 50 Median total IgE IU/mL (±SD) 792 (1093) Mean baseline Eosinophil count (± SD) cells/mcL 502 (395) DUPIXENT significantly reduced the annualized rate of severe asthma exacerbation events during the 52-week treatment period compared to placebo in populations with an eosinophilic phenotype as indicated by elevated blood eosinophils and/or the population with elevated FeNO. Subgroup analyses for results of DUPIXENT treatment based upon either baseline eosinophil level or baseline FeNO level were similar to the pediatric (12 to 17 years of age) and adult trials and are described for the adult and pediatric (12 to 17 years of age) asthma population above. In subjects with baseline blood eosinophil count <150 cells/mcL and FeNO <20 ppb, similar severe asthma exacerbation rates were observed between DUPIXENT and placebo.
Significant improvements in percent predicted pre-bronchodilator FEV1 were observed at Week 12. Significant improvements in percent predicted FEV1 were observed as early as Week 2 and were maintained through Week 52 in VOYAGE (Figure 10).
The efficacy results for VOYAGE are presented in Table 21.
Table 21: Efficacy Results of DUPIXENT in VOYAGE Treatment EOS ≥300 cells/mcL* Annualized Severe Exacerbations Rate over 52 Weeks N Rate
(95% CI)Rate Ratio
(95% CI)DUPIXENT
100 mg Q2W† (<30 kg)/
200 mg Q2W (≥30 kg)175 0.24
(0.16, 0.35)
0.35
(0.22, 0.56)Placebo 84 0.67
(0.47, 0.95)Mean Change from Baseline in Percent Predicted FEV1 at Week 12 N LS mean Δ from Baseline LS mean difference vs. Placebo (95% CI) DUPIXENT
100 mg Q2W† (<30 kg)/
200 mg Q2W (≥30 kg)168 10.15 5.32
(1.76, 8.88)Placebo 80 4.83 Figure 10: Mean Change from Baseline in Percent Predicted Pre-bronchodilator FEV1 (L) Over Time in Pediatric Subjects 6 to 11 Years of Age in VOYAGE (Baseline Blood Eosinophils ≥300 cells/mcL)
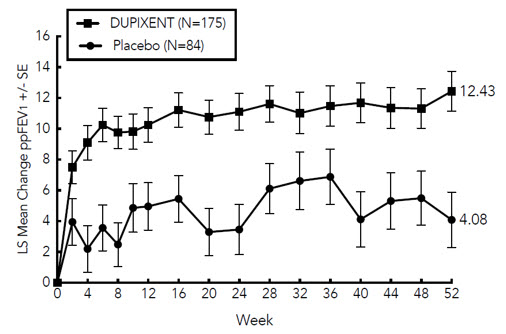
Improvements were also observed for ACQ-7-IA and PAQLQ(S)-IA at Week 24 and were sustained at Week 52. Greater responder rates were observed for ACQ-7-IA and PAQLQ(S)-IA compared to placebo at Week 24. The responder rate was defined as an improvement in score of 0.5 or more (scale range 0-6 for ACQ-7-IA and 1-7 for PAQLQ(S)-IA). In the subgroup of subjects with baseline blood eosinophil count ≥300 cells/mcL, DUPIXENT led to a higher proportion of subjects with a response in ACQ-7-IA (80.6% versus 64.3% for placebo) with an OR of 2.79 (95% CI: 1.43, 5.44), and in PAQLQ(S)-IA (72.8% versus 63.0% for placebo) with an OR of 1.84 (95% CI: 0.92, 3.65) at Week 24.
14.3 Chronic Rhinosinusitis with Nasal Polyposis
The chronic rhinosinusitis with nasal polyposis (CRSwNP) development program included two randomized, double-blind, parallel-group, multicenter, placebo-controlled studies (SINUS-24 (NCT02912468) and SINUS-52 (NCT02898454)) in 724 adult subjects 18 years of age and older on background intranasal corticosteroids (INCS). These studies included subjects with CRSwNP despite prior sino-nasal surgery or treatment with, or who were ineligible to receive or were intolerant to, systemic corticosteroids in the past 2 years. Subjects with chronic rhinosinusitis without nasal polyposis were not included in these trials. Rescue with systemic corticosteroids or surgery was allowed during the studies at the investigator's discretion. In SINUS-24, a total of 276 subjects were randomized to receive either 300 mg DUPIXENT (N=143) or placebo (N=133) every other week for 24 weeks. In SINUS-52, 448 subjects were randomized to receive either 300 mg DUPIXENT (N=150) every other week for 52 weeks, 300 mg DUPIXENT (N=145) every other week until Week 24 followed by 300 mg DUPIXENT every 4 weeks until Week 52, or placebo (N=153). All subjects had evidence of sinus opacification on the Lund Mackay (LMK) sinus CT scan and 73% to 90% of subjects had opacification of all sinuses. Subjects were stratified based on their histories of prior surgery and co-morbid asthma/nonsteroidal anti-inflammatory drug exacerbated respiratory disease (NSAID-ERD). A total of 63% of subjects reported previous sinus surgery, with a mean number of 2.0 prior surgeries, 74% used systemic corticosteroids in the previous 2 years with a mean number of 1.6 systemic corticosteroid courses in the previous 2 years, 59% had co-morbid asthma, and 28% had NSAID-ERD.
The co-primary efficacy endpoints were change from baseline to Week 24 in bilateral endoscopic nasal polyps score (NPS; 0-8 scale) as graded by central blinded readers, and change from baseline to Week 24 in nasal congestion/obstruction score averaged over 28 days (NC; 0-3 scale), as determined by subjects using a daily diary. For NPS, polyps on each side of the nose were graded on a categorical scale (0=no polyps; 1=small polyps in the middle meatus not reaching below the inferior border of the middle turbinate; 2=polyps reaching below the lower border of the middle turbinate; 3=large polyps reaching the lower border of the inferior turbinate or polyps medial to the middle turbinate; 4=large polyps causing complete obstruction of the inferior nasal cavity). The total score was the sum of the right and left scores. Nasal congestion was rated daily by the subjects on a 0 to 3 categorical severity scale (0=no symptoms; 1=mild symptoms; 2=moderate symptoms; 3=severe symptoms).
In both studies, key secondary end-points at Week 24 included change from baseline in: LMK sinus CT scan score, daily loss of smell, and 22-item sino-nasal outcome test (SNOT-22). The LMK sinus CT scan score evaluated the opacification of each sinus using a 0 to 2 scale (0=normal; 1=partial opacification; 2=total opacification) deriving a maximum score of 12 per side and a total maximum score of 24 (higher scores indicate more opacification). Loss of smell was scored reflectively by the subject every morning on a 0-3 scale (0=no symptoms, 1=mild symptoms, 2=moderate symptoms, 3=severe symptoms). SNOT-22 includes 22 items assessing symptoms and symptom impact associated with CRSwNP with each item scored from 0 (no problem) to 5 (problem as bad as it can be) with a global score ranging from 0 to 110. SNOT-22 had a 2 week recall period. In the pooled efficacy results, the reduction in the proportion of subjects rescued with systemic corticosteroids and/or sino-nasal surgery (up to Week 52) were evaluated.
The demographics and baseline characteristics of these 2 trials are provided in Table 22 below.
Table 22: Demographics and Baseline Characteristics of CRSwNP Trials Parameter SINUS-24
(N=276)SINUS-52
(N=448)SD = standard deviation; AM = morning; NPS = nasal polyps score; SNOT-22 = 22-item sino-nasal outcome test; NSAID-ERD = asthma/nonsteroidal anti-inflammatory drug exacerbated respiratory disease - *
- Higher scores indicate greater disease severity
Mean age (years) (SD) 50 (13) 52 (12) % Male 57 62 Mean CRSwNP duration (years) (SD) 11 (9) 11 (10) Subjects with ≥1 prior surgery (%) 72 58 Subjects with systemic corticosteroid use in the previous 2 years (%) 65 80 Mean Bilateral endoscopic NPS* (SD), range 0-8 5.8 (1.3) 6.1 (1.2) Mean Nasal congestion (NC) score* (SD), range 0-3 2.4 (0.6) 2.4 (0.6) Mean LMK sinus CT total score* (SD), range 0-24 19 (4.4) 18 (3.8) Mean loss of smell score *(AM), (SD) range 0-3 2.7 (0.5) 2.8 (0.5) Mean SNOT-22 total score* (SD), range 0-110 49.4 (20.2) 51.9 (20.9) Mean blood eosinophils (cells/mcL) (SD) 440 (330) 430 (350) Mean total IgE IU/mL (SD) 212 (276) 240 (342) Atopic Medical History
% Overall75 82 Asthma (%) 58 60 NSAID-ERD (%) 30 27 Clinical Response (SINUS-24 and SINUS-52)
The results for primary endpoints in CRSwNP studies are presented in Table 23.
Table 23: Results of the Primary Endpoints in CRSwNP Trials SINUS-24 SINUS-52 Placebo
(n=133)DUPIXENT
300 mg Q2W
(n=143)LS mean difference vs. Placebo (95% CI) Placebo
(n=153)DUPIXENT
300 mg Q2W
(n=295)LS mean difference vs. Placebo (95% CI) Primary Endpoints at Week 24 Scores Baseline mean LS mean change Baseline mean LS mean change Baseline mean LS mean change Baseline mean LS mean change A reduction in score indicates improvement.
NPS = nasal polyps score; NC = nasal congestion/obstructionNPS 5.86 0.17 5.64 -1.89 -2.06
(-2.43, -1.69)5.96 0.10 6.18 -1.71 -1.80
(-2.10, -1.51)NC 2.45 -0.45 2.26 -1.34 -0.89
(-1.07, -0.71)2.38 -0.38 2.46 -1.25 -0.87
(-1.03, -0.71)Statistically significant efficacy was observed in SINUS-52 with regard to improvement in bilateral endoscopic NPS score at week 24 and week 52 (see Figure 11).
Figure 11: LS Mean Change from Baseline in Bilateral Nasal Polyps Score (NPS) up to Week 52 in Subjects 18 Years of Age and Older with CRSwNP (SINUS-52 - ITT Population)
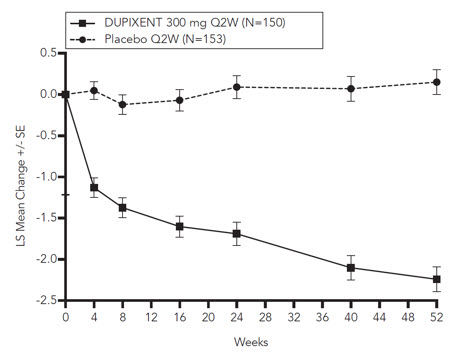
Similar results were seen in SINUS-24 at Week 24. In the post-treatment period when subjects were off DUPIXENT, the treatment effect diminished over time (see Figure 12).
Figure 12: LS Mean Change from Baseline in Bilateral Nasal Polyps Score (NPS) up to Week 48 in Subjects 18 Years of Age and Older with CRSwNP (SINUS-24 - ITT Population)
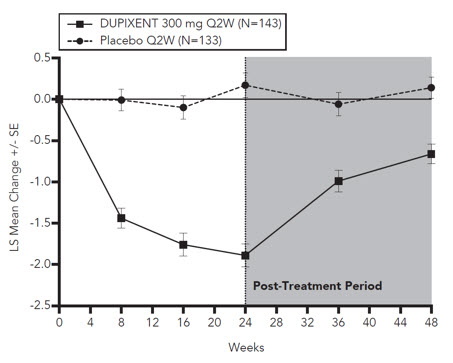
At Week 52, the LS mean difference for nasal congestion in the DUPIXENT group versus placebo was -0.98 (95% CI -1.17, -0.79). In both studies, significant improvements in nasal congestion were observed as early as the first assessment at Week 4. The LS mean difference for nasal congestion at Week 4 in the DUPIXENT group versus placebo was -0.41 (95% CI: -0.52, -0.30) in SINUS-24 and -0.37 (95% CI: -0.46, -0.27) in SINUS-52.
A significant decrease in the LMK sinus CT scan score was observed. The LS mean difference for LMK sinus CT scan score at Week 24 in the DUPIXENT group versus placebo was -7.44 (95% CI: -8.35, -6.53) in SINUS-24 and -5.13 (95% CI: -5.80, -4.46) in SINUS-52. At Week 52, in SINUS-52 the LS mean difference for LMK sinus CT scan score in the DUPIXENT group versus placebo was -6.94 (95% CI: -7.87, -6.01).
Dupilumab significantly improved the loss of smell compared to placebo. The LS mean difference for loss of smell at Week 24 in the DUPIXENT group versus placebo was -1.12 (95% CI: -1.31, -0.93) in SINUS-24 and -0.98 (95% CI: -1.15, -0.81) in SINUS-52. At Week 52, the LS mean difference for loss of smell in the DUPIXENT group versus placebo was -1.10 (95% CI -1.31, -0.89). In both studies, significant improvements in daily loss of smell severity were observed as early as the first assessment at Week 4.
Dupilumab significantly decreased sino-nasal symptoms as measured by SNOT-22 compared to placebo. The LS mean difference for SNOT-22 at Week 24 in the DUPIXENT group versus placebo was -21.12 (95% CI: -25.17, -17.06) in SINUS-24 and -17.36 (95% CI: -20.87, -13.85) in SINUS-52. At Week 52, the LS mean difference in the DUPIXENT group versus placebo was -20.96 (95% CI -25.03, -16.89).
In the pre-specified multiplicity-adjusted pooled analysis of two studies, treatment with DUPIXENT resulted in significant reduction of systemic corticosteroid use and need for sino-nasal surgery versus placebo (HR of 0.24; 95% CI: 0.17, 0.35) (see Figure 13). The proportion of subjects who required systemic corticosteroids was reduced by 74% (HR of 0.26; 95% CI: 0.18, 0.38). The total number of systemic corticosteroid courses per year was reduced by 75% (RR of 0.25; 95% CI: 0.17, 0.37). The proportion of subjects who required surgery was reduced by 83% (HR of 0.17; 95% CI: 0.07, 0.46).
Figure 13: Kaplan Meier Curve for Time to First Systemic Corticosteroid Use and/or Sino-Nasal Surgery During Treatment Period in Subjects 18 Years of Age and Older with CRSwNP (SINUS-24 and SINUS-52 Pooled - ITT Population)
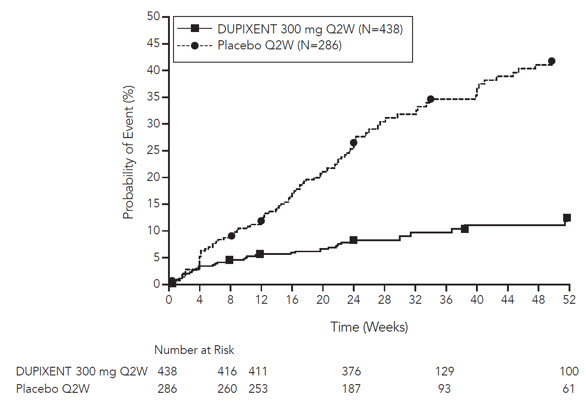
The effects of DUPIXENT on the primary endpoints of NPS and nasal congestion and the key secondary endpoint of LMK sinus CT scan score were consistent in subjects with prior surgery and without prior surgery.
In subjects with co-morbid asthma, improvements in pre-bronchodilator FEV1 were similar to subjects in the asthma program.
14.4 Eosinophilic Esophagitis
Adult and Pediatric Subjects 12 Years of Age and Older with EoE
A single randomized, double-blind, parallel-group, multicenter, placebo-controlled trial, including two 24-week treatment periods (Study EoE-1 Parts A and B) was conducted in adult and pediatric subjects 12 years of age and older, weighing at least 40 kg, with EoE (NCT03633617). In both parts, subjects were randomized to receive 300 mg DUPIXENT every week or placebo. Eligible subjects had ≥15 intraepithelial eosinophils per high-power field (eos/hpf) following a treatment course of a proton pump inhibitor (PPI) either prior to or during the screening period and symptoms of dysphagia as measured by the Dysphagia Symptom Questionnaire (DSQ). At baseline, 43% of subjects in Part A and 37% of subjects in Part B had a history of prior esophageal dilations.
Demographics and baseline characteristics were similar in Parts A and B. A total of 81 subjects (61 adults and 20 pediatric subjects) were enrolled in Part A and 159 subjects (107 adults and 52 pediatric subjects) were enrolled in Part B. The mean age in years was 32 years (range 13 to 62 years) in Part A and 28 years (range 12 to 66 years) in Part B. The majority of subjects were male (60% in Part A and 68% in Part B) and White (96% in Part A and 90% in Part B). The mean baseline DSQ score (SD) was 33.6 (12.4) in Part A and 37.2 (10.7) in Part B.
The coprimary efficacy endpoints in Parts A and B were the (1) proportion of subjects achieving histological remission defined as peak esophageal intraepithelial eosinophil count of ≤6 eos/hpf at Week 24; and (2) the absolute change in the subject-reported DSQ score from baseline to Week 24.
Efficacy results for Parts A and B are presented in Table 24.
Table 24: Efficacy Results of DUPIXENT at Week 24 in Adult and Pediatric Subjects 12 Years of Age and Older with EoE (Study EoE-1 Parts A and B) Study EoE-1 Part A Study EoE-1 Part B DUPIXENT 300 mg QW* Placebo* Difference vs. Placebo
(95% CI)*DUPIXENT 300 mg QW* Placebo* Difference vs. Placebo
(95% CI)*N = 42 N = 39 N = 80 N = 79 - *
- For histological remission, the difference in percentages is estimated using the Cochran Mantel Haenszel method, adjusting for randomization stratification factors. For absolute change in DSQ score, the LS mean changes, standard errors, and differences are estimated using an ANCOVA model with treatment group, randomization stratification factors, and baseline measurement as covariates.
- †
- Total biweekly DSQ scores range from 0 to 84; higher scores indicate greater frequency and severity of dysphagia
Co-primary Endpoints Proportion of subjects achieving histological remission (peak esophageal intraepithelial eosinophil count ≤6 eos/hpf), n (%) 25
(59.5)2
(5.1)57.0
(40.9, 73.1)47
(58.8)5
(6.3)53.5
(41.2, 65.8)Absolute change from baseline in DSQ score (0-84†), LS mean (SE) -21.9
(2.5)-9.6
(2.8)-12.3
(-19.1, -5.5)-23.8
(1.9)-13.9
(1.9)-9.9
(-14.8, -5.0)In Parts A and B, a greater proportion of subjects randomized to DUPIXENT achieved histological remission (peak esophageal intraepithelial eosinophil count ≤6 eos/hpf) compared to placebo. Treatment with DUPIXENT also resulted in a significant improvement in LS mean change in DSQ score compared to placebo at Week 24. The results of the anchor-based analyses that incorporated the subjects' perspectives indicated that the observed improvement in dysphagia from Parts A and B is representative of a clinically meaningful within-subject improvement.
Pediatric Subjects 1 to 11 Years of Age, Weighing at Least 15 kg, with EoE
The efficacy and safety of DUPIXENT was evaluated in pediatric subjects 1 to 11 years of age, weighing at least 15 kg, with EoE in a randomized, blinded, parallel-group, multicenter trial (Study EoE-2 Parts A and B; NCT04394351). Eligible subjects had ≥15 intraepithelial eosinophils per high-power field (eos/hpf) despite a treatment course of a proton pump inhibitor (PPI) either prior to or during the screening period and a history of EoE signs and symptoms. Part A evaluated weight-based dosing regimens of DUPIXENT, 200 mg Q2W (≥15 to <30 kg) and 300 mg Q2W (≥30 to <60 kg), or placebo in 61 subjects during the 16-week treatment period.
The recommended dosage of 300 mg QW for pediatric subjects 1 to 11 years of age weighing ≥40 kg is based on modeled pharmacokinetic data to provide comparable exposures to the 300 mg QW dosage in adult and pediatric subjects 12 years of age and older weighing ≥40 kg with EoE [see Dosage and Administration (2.6) and Pharmacokinetics (12.3)].
Forty-seven subjects who completed Part A were evaluated in the 36-week extended active treatment period (Study EoE-2 Part B). All subjects in Part B were treated with the weight-based dosing regimens of DUPIXENT described for Part A.
Of the total subjects evaluated in Part A, the mean age was 8 years, the median weight was 28 kg, and 75% were male. Seven percent identified as Hispanic or Latino; 85% identified as White, 12% as Black, 2% as Asian, and 2% identified as another racial subgroup.
The primary efficacy endpoint in Part A was the proportion of subjects achieving histological remission defined as peak esophageal intraepithelial eosinophil count of ≤6 eos/hpf at Week 16.
Efficacy results for Part A are presented in Table 25.
Table 25: Efficacy Results of DUPIXENT at Week 16 in Subjects 1 to 11 Years of Age with EoE, Weighing at Least 15 kg (Study EoE-2 Part A) DUPIXENT*
N=32Placebo
N=29Difference vs Placebo
(95% CI)- *
- DUPIXENT was evaluated at tiered dosing regimens based on body weight: ≥15 to <30 kg (200 mg Q2W) and ≥30 to <60 kg (300 mg Q2W). The 300 mg Q2W dosing regimen is lower than the recommended dosage of DUPIXENT in subjects ≥40 kg [see Dosage and Administration (2.6)].
- †
- The difference in percentages is estimated using the Mantel-Haenszel method, adjusting for baseline weight group (≥15 to <30 kg and ≥30 to <60 kg).
Proportion of subjects achieving histological remission (peak esophageal intraepithelial eosinophil count ≤6 eos/hpf), n (%)† 21
(65.6)1
(3.4)62.0
(44.00, 79.95)In Part B, histological remission was achieved at Week 52 in 17/32 subjects treated with DUPIXENT in Parts A and B and 8/15 subjects treated with placebo in Part A and DUPIXENT in Part B.
In Study EoE-2 Part A, an observer-reported outcome, the Pediatric EoE Sign/Symptom Questionnaire-Caregiver (PESQ-C), was used to measure signs of EoE. A greater decrease in the proportion of days with 1 or more signs of EoE (based on the PESQ-C) was observed for subjects treated with DUPIXENT compared to placebo after 16 weeks of treatment.
14.5 Prurigo Nodularis
The prurigo nodularis (PN) development program included two 24-week randomized, double-blind, placebo-controlled, multicenter, parallel-group trials (PRIME (NCT04183335) and PRIME 2 (NCT04202679)) in 311 adult subjects 18 years of age and older with pruritus (WI-NRS ≥ 7 on a scale of 0 to 10) and greater than or equal to 20 nodular lesions. PRIME and PRIME 2 assessed the effect of DUPIXENT on pruritus improvement as well as its effect on PN lesions.
In these two trials, subjects received either subcutaneous DUPIXENT 600 mg (two 300 mg injections) on day 1, followed by 300 mg once every other week (Q2W) for 24 weeks, or matching placebo.
In these trials, the mean age was 49.5 years, the median weight was 71 kg, 65% of subjects were female, 57% were White, 6% were Black, and 34% were Asian. At baseline, the mean Worst Itch-Numeric Rating Scale (WI-NRS) was 8.5, 66% had 20 to 100 nodules (moderate), and 34% had greater than 100 nodules (severe). Eleven percent (11%) of subjects were taking stable doses of antidepressants at baseline and were instructed to continue taking these medications during the trial. Forty-three percent (43%) had a history of atopy (defined as having a medical history of AD, allergic rhinitis/rhinoconjunctivitis, asthma, or food allergy).
The WI-NRS is comprised of a single item, rated on a scale from 0 ("no itch") to 10 ("worst imaginable itch"). Subjects were asked to rate the intensity of their worst pruritus (itch) over the past 24 hours using this scale. The Investigator's Global Assessment for Prurigo Nodularis-Stage (IGA PN-S) is a scale that measures the approximate number of nodules using a 5-point scale from 0 (clear) to 4 (severe).
Efficacy was assessed with the proportion of subjects with improvement (reduction) in WI-NRS by ≥4 points, the proportion of subjects with IGA PN-S 0 or 1 (the equivalent of 0-5 nodules), and the proportion of subjects who achieved a response in both WI-NRS and IGA PN-S per the criteria described above.
The efficacy results for PRIME and PRIME2 are presented in Table 26 and Figures 14, 15, and 16.
Table 26: Efficacy Results of DUPIXENT in PRIME and PRIME2 PRIME PRIME2 Placebo
(N=76)DUPIXENT
300 mg Q2W
(N=75)Difference (95% CI) for DUPIXENT vs. Placebo Placebo
(N=82)DUPIXENT
300 mg Q2W
(N=78)Difference (95% CI) for DUPIXENT vs. Placebo Proportion of subjects with both an improvement (reduction) in WI-NRS by ≥4 points from baseline to Week 24 and an IGA PN-S 0 or 1 at Week 24* 9.2% 38.7% 29.6%
(16.4, 42.8)8.5% 32.1% 25.5%
(13.1, 37.9)Proportion of subjects with improvement (reduction) in WI-NRS by ≥4 points from baseline at Week 24* 18.4% 60.0% 42.7%
(27.8, 57.7)19.5% 57.7% 42.6%
(29.1, 56.1)Proportion of subjects with IGA PN-S 0 or 1 at Week 24* 18.4% 48.0% 28.3%
(13.4, 43.2)15.9% 44.9% 30.8%
(16.4, 45.2)Proportion of subjects with improvement (reduction) in WI-NRS by ≥4 points from baseline at Week 12* 15.8%† 44.0%† 29.2%
(14.5, 43.8)†22.0% 37.2% 16.8%
(2.3, 31.2)Figure 14: Proportion of Adult Subjects with PN with Both WI-NRS ≥4-point Improvement and IGA PN-S 0 or 1 Over Time in PRIME and PRIME2
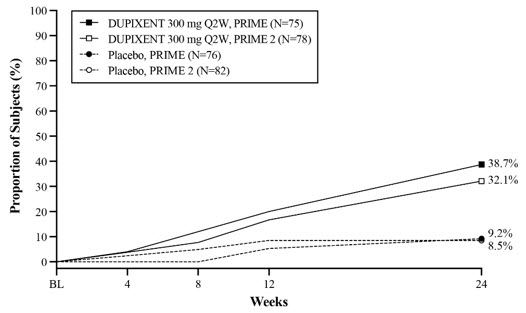
Figure 15: Proportion of Adult Subjects with PN with WI-NRS ≥4-point Improvement Over Time in PRIME and PRIME2
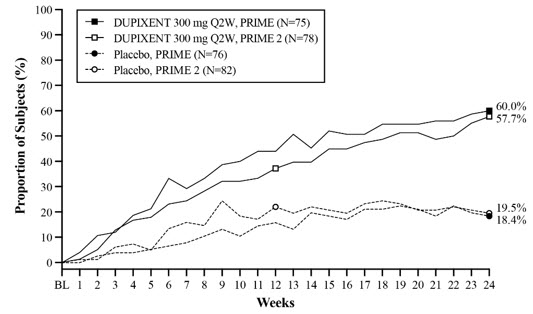
Figure 16: Proportion of Adult Subjects with IGA PN-S 0 or 1 Over Time in PRIME and PRIME 2
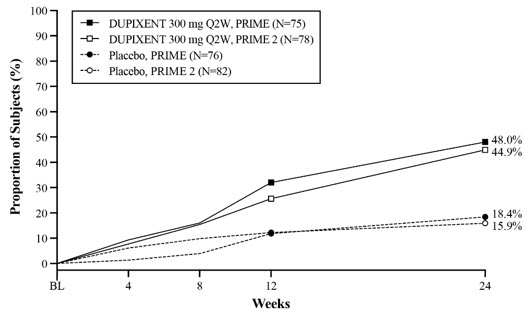
The efficacy data did not show differential treatment effect across demographic subgroups.
-
16 HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
DUPIXENT (dupilumab) Injection is a clear to slightly opalescent, colorless to pale yellow solution, supplied in single-dose pre-filled syringes with needle shield or pre-filled pens.
The pre-filled syringe with needle shield is designed to deliver:
- 300 mg of DUPIXENT in 2 mL solution (NDC 0024-5914-00)
- 200 mg of DUPIXENT in 1.14 mL solution (NDC 0024-5918-00)
The pre-filled pen is designed to deliver:
- 300 mg of DUPIXENT in 2 mL solution (NDC 0024-5915-00)
- 200 mg of DUPIXENT in 1.14 mL solution (NDC 0024-5919-00)
DUPIXENT is available in cartons containing 2 pre-filled syringes with needle shield or 2 pre-filled pens.
Pack Size 300 mg/2 mL Pre-filled Syringe with Needle Shield 200 mg/1.14 mL Pre-filled Syringe with Needle Shield Pack of 2 syringes NDC 0024-5914-01 NDC 0024-5918-01 Pack Size 300 mg/2 mL Pre-filled Pen 200 mg/1.14 mL Pre-filled Pen Pack of 2 pens NDC 0024-5915-02 NDC 0024-5919-02 Storage and Handling
DUPIXENT is sterile and preservative-free. Discard any unused portion.
Store refrigerated at 2°C to 8°C (36°F to 46°F) in the original carton to protect from light.
If necessary, DUPIXENT may be kept at room temperature up to 25°C (77°F) for a maximum of 14 days. Do not store above 25°C (77°F). After removal from the refrigerator, DUPIXENT must be used within 14 days or discarded.
Do not expose DUPIXENT to heat or direct sunlight.
Do NOT freeze. Do NOT shake.
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information and Instructions for Use).
Pregnancy Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to DUPIXENT during pregnancy. Encourage participation and advise patients about how they may enroll in the registry [see Use in Specific Populations (8.1)].
Administration Instructions
Provide proper training to patients and/or caregivers on proper subcutaneous injection technique, including aseptic technique, and the preparation and administration of DUPIXENT prior to use. Advise patients to follow sharps disposal recommendations [see Dosage and Administration (2.1) and Instructions for Use].
Hypersensitivity
Advise patients to discontinue DUPIXENT and to seek immediate medical attention if they experience any symptoms of systemic hypersensitivity reactions [see Warnings and Precautions (5.1)].
Conjunctivitis and Keratitis
Advise patients to consult their healthcare provider if new onset or worsening eye symptoms develop [see Warnings and Precautions (5.2)].
Eosinophilic Conditions
Advise patients to notify their healthcare provider if they present with clinical features of eosinophilic pneumonia or vasculitis consistent with eosinophilic granulomatosis with polyangiitis [see Warnings and Precautions (5.3)].
Not for Acute Asthma Symptoms or Deteriorating Disease
Inform patients that DUPIXENT does not treat acute asthma symptoms or acute exacerbations. Inform patients to seek medical advice if their asthma remains uncontrolled or worsens after initiation of treatment with DUPIXENT [see Warnings and Precautions (5.4)].
Reduction in Corticosteroid Dosage
Inform patients to not discontinue systemic or inhaled corticosteroids except under the direct supervision of a healthcare provider. Inform patients that reduction in corticosteroid dose may be associated with systemic withdrawal symptoms and/or unmask conditions previously suppressed by systemic corticosteroid therapy [see Warnings and Precautions (5.5)].
Patients with Co-morbid Asthma
Advise patients with co-morbid asthma not to adjust or stop their asthma treatment without talking to their healthcare providers [see Warnings and Precautions (5.6)].
Arthralgia
Advise patients to report new onset or worsening joint symptoms to their healthcare provider [see Warnings and Precautions (5.7)].
Parasitic (Helminth) Infections
Advise patients to notify their healthcare provider if they present with clinical features consistent with helminthic infection [see Warnings and Precautions (5.8)].
Vaccinations
Advise patients that vaccination with live vaccines is not recommended immediately prior to and while they are receiving DUPIXENT. Instruct patients to inform their healthcare provider that they are taking DUPIXENT prior to a potential vaccination [see Warnings and Precautions (5.9)].
-
SPL UNCLASSIFIED SECTION
Manufactured by:
Regeneron Pharmaceuticals, Inc.
Tarrytown, NY 10591
U.S. License No. 1760
Marketed by:
sanofi-aventis U.S. LLC (Bridgewater, NJ 08807) and
Regeneron Pharmaceuticals, Inc. (Tarrytown, NY 10591)
For patent information: www.dupixent-patents.com
DUPIXENT® is a registered trademark of Sanofi Biotechnology
© 2024 Regeneron Pharmaceuticals, Inc. / sanofi-aventis U.S. LLC. All rights reserved.
-
PATIENT PACKAGE INSERT
This Patient Information has been approved by the U.S. Food and Drug Administration. Revised: January 2024 Patient Information
DUPIXENT® (DU-pix-ent)
(dupilumab)
injection, for subcutaneous useWhat is DUPIXENT?
DUPIXENT is a prescription medicine used:- to treat adults and children 6 months of age and older with moderate-to-severe eczema (atopic dermatitis or AD) that is not well controlled with prescription therapies used on the skin (topical), or who cannot use topical therapies. DUPIXENT can be used with or without topical corticosteroids.
- with other asthma medicines for the maintenance treatment of moderate-to-severe asthma in adults and children 6 years of age and older whose asthma is not controlled with their current asthma medicines. DUPIXENT helps prevent severe asthma attacks (exacerbations) and can improve your breathing. DUPIXENT may also help reduce the amount of oral corticosteroids you need while preventing severe asthma attacks and improving your breathing. DUPIXENT is not used to treat sudden breathing problems.
- with other medicines for the maintenance treatment of chronic rhinosinusitis with nasal polyposis (CRSwNP) in adults whose disease is not controlled.
- to treat adults and children 1 year of age and older with eosinophilic esophagitis (EoE), who weigh at least 33 pounds (15 kg).
- to treat adults with prurigo nodularis (PN).
- DUPIXENT works by blocking two proteins that contribute to a type of inflammation that plays a major role in atopic dermatitis, asthma, chronic rhinosinusitis with nasal polyposis, eosinophilic esophagitis, and prurigo nodularis.
- It is not known if DUPIXENT is safe and effective in children with atopic dermatitis under 6 months of age.
- It is not known if DUPIXENT is safe and effective in children with asthma under 6 years of age.
- It is not known if DUPIXENT is safe and effective in children with chronic rhinosinusitis with nasal polyposis under 18 years of age.
- It is not known if DUPIXENT is safe and effective in children with eosinophilic esophagitis under 1 year of age, or who weigh less than 33 pounds (15 kg).
- It is not known if DUPIXENT is safe and effective in children with prurigo nodularis under 18 years of age.
Do not use DUPIXENT if you are allergic to dupilumab or to any of the ingredients in DUPIXENT. See the end of this Patient Information leaflet for a complete list of ingredients in DUPIXENT. Before using DUPIXENT, tell your healthcare provider about all your medical conditions, including if you: - have eye problems.
- have a parasitic (helminth) infection.
- are scheduled to receive any vaccinations. You should not receive a "live vaccine" right before and during treatment with DUPIXENT.
- are pregnant or plan to become pregnant. It is not known whether DUPIXENT will harm your unborn baby.
Pregnancy Exposure Registry. There is a pregnancy exposure registry for women who use DUPIXENT during pregnancy. The purpose of this registry is to collect information about the health of you and your baby. Your healthcare provider can enroll you in this registry. You may also enroll yourself or get more information about the registry by calling 1-877-311-8972 or going to https://mothertobaby.org/ongoing-study/dupixent/. - are breastfeeding or plan to breastfeed. It is not known whether DUPIXENT passes into your breast milk.
Especially tell your healthcare provider if you:- are taking oral, topical, or inhaled corticosteroid medicines
- have asthma and use an asthma medicine
- have atopic dermatitis, chronic rhinosinusitis with nasal polyposis, eosinophilic esophagitis, or prurigo nodularis and also have asthma
How should I use DUPIXENT? - See the detailed "Instructions for Use" that comes with DUPIXENT for information on how to prepare and inject DUPIXENT and how to properly store and throw away (dispose of) used DUPIXENT pre-filled syringes and pre-filled pens.
- Use DUPIXENT exactly as prescribed by your healthcare provider.
- Your healthcare provider will tell you how much DUPIXENT to inject and how often to inject it.
- DUPIXENT comes as a single-dose pre-filled syringe with needle shield or as a pre-filled pen.
- The DUPIXENT pre-filled pen is only for use in adults and children 2 years of age and older.
- The DUPIXENT pre-filled syringe is for use in adults and children 6 months of age and older.
- DUPIXENT is given as an injection under the skin (subcutaneous injection).
- If your healthcare provider decides that you or a caregiver can give the injections of DUPIXENT, you or your caregiver should receive training on the right way to prepare and inject DUPIXENT. Do not try to inject DUPIXENT until you have been shown the right way by your healthcare provider. In children 12 years of age and older, it is recommended that DUPIXENT be given by or under the supervision of an adult. In children 6 months to less than 12 years of age, DUPIXENT should be given by a caregiver.
- If your dose schedule is every week and you miss a dose of DUPIXENT: Give the DUPIXENT injection as soon as possible and start a new every week dose schedule from the time you remember to take your DUPIXENT injection.
- If your dose schedule is every other week and you miss a dose of DUPIXENT: Give the DUPIXENT injection within 7 days from the missed dose, then continue with your original schedule. If the missed dose is not given within 7 days, wait until the next scheduled dose to give your DUPIXENT injection.
- If your dose schedule is every 4 weeks and you miss a dose of DUPIXENT: Give the DUPIXENT injection within 7 days from the missed dose, then continue with your original schedule. If the missed dose is not given within 7 days, start a new every 4 week dose schedule from the time you remember to take your DUPIXENT injection.
- If you inject too much DUPIXENT, call your healthcare provider or Poison Help line at 1-800-222-1222 or go to the nearest hospital emergency room right away.
- Your healthcare provider may prescribe other medicines to use with DUPIXENT. Use the other prescribed medicines exactly as your healthcare provider tells you to.
What are the possible side effects of DUPIXENT?
DUPIXENT can cause serious side effects, including:- Allergic reactions. DUPIXENT can cause allergic reactions that can sometimes be severe. Stop using DUPIXENT and tell your healthcare provider or get emergency help right away if you get any of the following signs or symptoms:
- breathing problems or wheezing
- fast pulse
- fever
- general ill feeling
- swollen lymph nodes
- swelling of the face, lips, mouth, tongue, or throat
- hives
- itching
- nausea or vomiting
- fainting, dizziness, feeling lightheaded
- joint pain
- skin rash
- cramps in your stomach-area
- Eye problems. Tell your healthcare provider if you have any new or worsening eye problems, including eye pain or changes in vision, such as blurred vision. Your healthcare provider may send you to an ophthalmologist for an eye exam if needed.
- Inflammation of your blood vessels. Rarely, this can happen in people with asthma who receive DUPIXENT. This may happen in people who also take a steroid medicine by mouth that is being stopped or the dose is being lowered. It is not known whether this is caused by DUPIXENT. Tell your healthcare provider right away if you have:
- rash
- worsening shortness of breath
- persistent fever
- chest pain
- a feeling of pins and needles or numbness of your arms or legs
- Joint aches and pain. Joint aches and pain can happen in people who use DUPIXENT. Some people have had trouble walking or moving due to their joint symptoms, and in some cases needed to be hospitalized. Tell your healthcare provider about any new or worsening joint symptoms. Your healthcare provider may stop DUPIXENT if you develop joint symptoms.
- injection site reactions
- upper respiratory tract infections
- eye and eyelid inflammation, including redness, swelling, and itching, sometimes with blurred vision
- dry eye
- herpes virus infections
- common cold symptoms (nasopharyngitis)
- cold sores in your mouth or on your lips
- high count of a certain white blood cell (eosinophilia)
- dizziness
- muscle pain
- diarrhea
- pain in the throat (oropharyngeal pain)
- gastritis
- joint pain (arthralgia)
- trouble sleeping (insomnia)
- toothache
- parasitic (helminth) infections
The following additional side effects have been reported with DUPIXENT: - facial rash or redness
These are not all of the possible side effects of DUPIXENT.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.How should I store DUPIXENT? - Store DUPIXENT in the refrigerator at 36ºF to 46ºF (2ºC to 8ºC).
- Store DUPIXENT in the original carton to protect from light.
- DUPIXENT can be stored at room temperature up to 77°F (25°C) up to 14 days. Throw away (dispose of) any DUPIXENT that has been left at room temperature for longer than 14 days.
- Do not heat or put DUPIXENT into direct sunlight.
- Do not freeze. Do not shake.
General information about the safe and effective use of DUPIXENT.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use DUPIXENT for a condition for which it was not prescribed. Do not give DUPIXENT to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about DUPIXENT that is written for health professionals.What are the ingredients in DUPIXENT?
Active ingredient: dupilumab
Inactive ingredients: L-arginine hydrochloride, L-histidine, polysorbate 80, sodium acetate, sucrose, and water for injection.
Manufactured by: Regeneron Pharmaceuticals, Inc., Tarrytown, NY 10591 U.S. License No. 1760
Marketed by: sanofi-aventis U.S. LLC (Bridgewater, NJ 08807) and Regeneron Pharmaceuticals, Inc. (Tarrytown, NY 10591)
DUPIXENT® is a registered trademark of Sanofi Biotechnology / © 2024 Regeneron Pharmaceuticals, Inc. / sanofi-aventis U.S. LLC. All rights reserved.
For more information about DUPIXENT, go to www.DUPIXENT.com or call 1-844-DUPIXENT (1-844-387-4936). -
INSTRUCTIONS FOR USEDUPIXENT® (DU-pix-ent)(dupilumab)injection, for subcutaneous useSingle-Dose Pre-filled Syringe with Needle Shield
Read this Instructions for Use before using the DUPIXENT Pre-filled Syringe. Do not inject yourself or someone else until you have been shown how to inject DUPIXENT. Your healthcare provider can show you or your caregiver how to prepare and inject a dose of DUPIXENT before you try to do it yourself the first time. Keep these instructions for future use. Call your healthcare provider if you have any questions.
This device is a Single-Dose Pre-filled Syringe (called "DUPIXENT Syringe" in these instructions). It contains 300 mg of DUPIXENT for injection under the skin (subcutaneous injection).
The parts of the DUPIXENT Syringe are shown below:
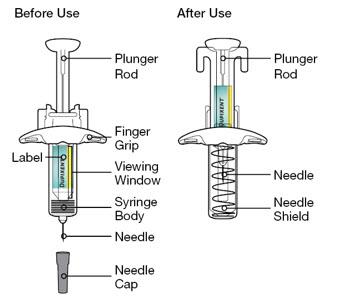
Important Information - Read all of the instructions carefully before using the DUPIXENT Syringe.
- Ask your healthcare provider how often you will need to inject the medicine.
- In children 12 years of age and older, it is recommended that DUPIXENT be administered by or under supervision of an adult.
- In children 6 months to less than 12 years of age, DUPIXENT should be given by a caregiver.
- Rotate the injection site each time you inject.
- Do not use the DUPIXENT Syringe if it has been dropped on a hard surface or damaged.
- Do not use the DUPIXENT Syringe if the Needle Cap is missing or not securely attached.
- Do not touch the Plunger Rod until you are ready to inject.
- Do not inject through clothes.
- Do not get rid of any air bubble in the DUPIXENT Syringe.
- To reduce the risk of accidental needle sticks, each pre-filled syringe has a Needle Shield that is automatically activated to cover the needle after you have given your injection.
- Do not pull back on the Plunger Rod at any time.
- Do not remove the Needle Cap until just before you give the injection.
- Throw away (dispose of) the used DUPIXENT Single-Dose Pre-filled Syringe right away after use. See "Step 13: Dispose" below.
- Do not re-use a DUPIXENT Single-Dose Pre-filled Syringe.
How should I store DUPIXENT? - Keep DUPIXENT Syringes and all medicines out of the reach of children.
- Store DUPIXENT Syringes in the refrigerator between 36°F to 46°F (2°C to 8°C).
- Store DUPIXENT Syringes in the original carton to protect them from light.
- DUPIXENT Syringes can be stored at room temperature up to 77°F (25°C) up to 14 days. Throw away (dispose of) any DUPIXENT Syringes that have been left at room temperature for longer than 14 days.
- Do not shake the DUPIXENT Syringe.
- Do not heat the DUPIXENT Syringe.
- Do not freeze the DUPIXENT Syringe.
- Do not put the DUPIXENT Syringe into direct sunlight.
Step 1: Remove
Remove the DUPIXENT Syringe from the carton by holding the middle of the Syringe Body.
 Do not pull off the Needle Cap until you are ready to inject.
Do not use the DUPIXENT Syringe if it has been dropped on a hard surface or damaged.
Do not pull off the Needle Cap until you are ready to inject.
Do not use the DUPIXENT Syringe if it has been dropped on a hard surface or damaged.
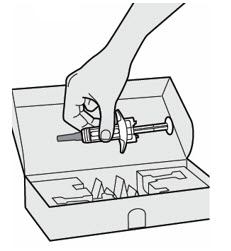
Step 2: Prepare
Ensure you have the following:
- the DUPIXENT Pre-filled Syringe
- 1 alcohol wipe*
- 1 cotton ball or gauze*
- a sharps disposal container* (See Step 13)
*Items not included in the carton
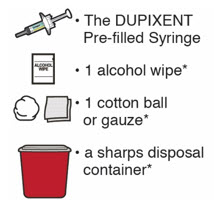
Step 3: Check
When you receive your DUPIXENT Syringes, always check to see that:
- you have the correct medicine and dose.
- the expiration date on the Single-Dose Pre-filled Syringe has not passed.
Do not use the DUPIXENT Syringe if the expiration date has passed.
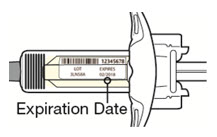
Step 4: Inspect
Look at the medicine through the Viewing Window on the DUPIXENT Syringe:
Check to see if the liquid is clear and colorless to pale yellow.
Note: You may see an air bubble, this is normal.
Do not use the DUPIXENT Syringe if the liquid is discolored or cloudy, or if it contains visible flakes or particles.
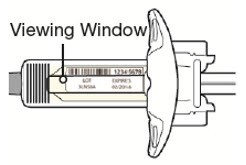
Step 5: Wait 45 minutes
Lay the DUPIXENT Syringe on a flat surface and let it naturally warm to room temperature for at least 45 minutes.
Do not heat the DUPIXENT Syringe.
Do not put the DUPIXENT Syringe into direct sunlight.
Do not keep DUPIXENT Syringes at room temperature for more than 14 days. Throw away (dispose of) any DUPIXENT Syringes that have been left at room temperature for longer than 14 days.
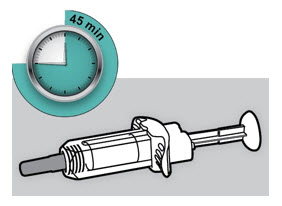
Step 6: Choose your injection site
- You can inject into your thigh or stomach, except for the 2 inches (5 cm) around your belly button (navel).
- If a caregiver injects your dose, they can also use the outer area of the upper arm.
- Choose a different site each time you inject DUPIXENT.
Do not inject into skin that is tender, damaged, bruised or scarred.
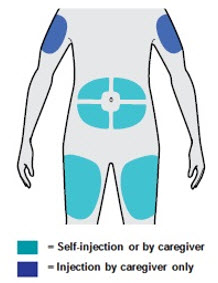
Step 7: Clean
Wash your hands.
Clean the injection site with an alcohol wipe.
Let your skin dry before injecting.
Do not touch the injection site again or blow on it before the injection.

Step 8: Remove Needle Cap
Hold the DUPIXENT Syringe in the middle of the Syringe Body with the Needle pointing away from you and pull off the Needle Cap.
Do not put the Needle Cap back on.
Do not touch the Needle.
Inject your medicine right away after removing the Needle Cap.
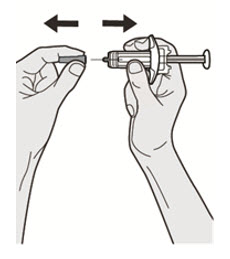
Step 9: Pinch
Pinch a fold of skin at the injection site (thigh or stomach, except 2 inches around your belly button, or outer area of the upper arm if injected by your caregiver). The figure below shows an example of pinching a fold of skin on your stomach.
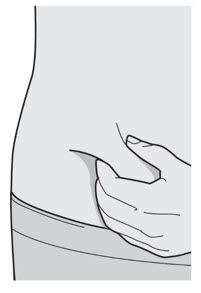
Step 10: Insert
Insert the Needle completely into the fold of the skin at about a 45° angle.
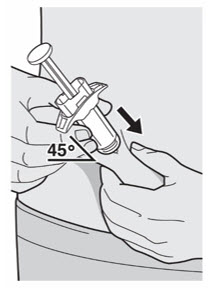
Step 11: Push
Relax the pinch.
Push the Plunger Rod down slowly and steadily as far as it will go until the DUPIXENT Syringe is empty.
Note: You will feel some resistance. This is normal.
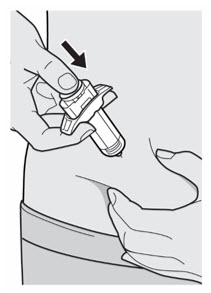
Step 12: Release and Remove
Lift your thumb to release the Plunger Rod until the Needle is covered by the Needle Shield and then remove the Syringe from the injection site.
Lightly press a cotton ball or gauze on the injection site if you see any blood.
Do not put the Needle Cap back on.
Do not rub your skin after the injection.
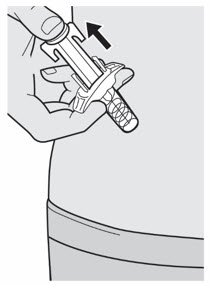
Put your used Needles, DUPIXENT Syringes, and Needle Caps in a FDA-cleared sharps disposal container right away after use.
Do not dispose of (throw away) Needles, DUPIXENT Syringes, and Needle Caps in your household trash.
If you do not have a FDA-cleared sharps disposal container, you may use a household container that is:
- made of a heavy-duty plastic,
- can be closed with a tight-fitting, puncture-resistant lid, without sharps being able to come out,
- upright and stable during use,
- leak-resistant, and
- properly labeled to warn of hazardous waste inside the container
When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to dispose of your sharps disposal container. There may be state or local laws about how you should throw away used Needles and Syringes.
For more information about safe sharps disposal, and for specific information about sharps disposal in the state that you live in, go to the FDA's website at: http://www.fda.gov/safesharpsdisposal
Do not dispose of your used sharps disposal container in your household trash unless your community guidelines permit this. Do not recycle your used sharps disposal container.
Do not put the Needle Cap back on.
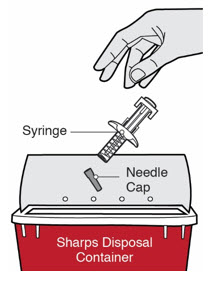

Manufactured by: Regeneron Pharmaceuticals, Inc. Tarrytown, NY 10591
U.S. License No. 1760Marketed by: sanofi-aventis U.S. LLC (Bridgewater, NJ 08807) and Regeneron Pharmaceuticals, Inc. (Tarrytown, NY 10591)
DUPIXENT® is a registered trademark of Sanofi Biotechnology© 2023 Regeneron Pharmaceuticals, Inc. / sanofi-aventis U.S. LLC. All rights reserved.
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Revised: July 2023
-
INSTRUCTIONS FOR USEDUPIXENT® (DU-pix-ent)(dupilumab)injection, for subcutaneous useSingle-Dose Pre-filled Syringe with Needle Shield
Read this Instructions for Use before using the DUPIXENT Pre-filled Syringe. Do not inject yourself or someone else until you have been shown how to inject DUPIXENT. Your healthcare provider can show you or your caregiver how to prepare and inject a dose of DUPIXENT before you try to do it yourself the first time. Keep these instructions for future use. Call your healthcare provider if you have any questions.
This device is a Single-Dose Pre-filled Syringe (called "DUPIXENT Syringe" in these instructions). It contains 200 mg of DUPIXENT for injection under the skin (subcutaneous injection).
The parts of the DUPIXENT Syringe are shown below:
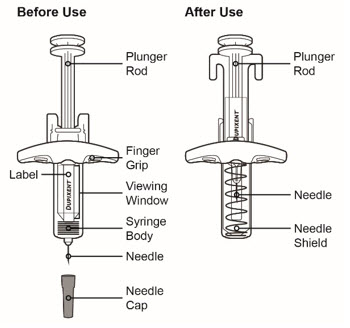
Important Information - Read all of the instructions carefully before using the DUPIXENT Syringe.
- Ask your healthcare provider how often you will need to inject the medicine.
- In children 12 years of age and older, it is recommended that DUPIXENT be administered by or under supervision of an adult.
- In children 6 months to less than 12 years of age, DUPIXENT should be given by a caregiver.
- Rotate the injection site each time you inject.
- Do not use the DUPIXENT Syringe if it has been dropped on a hard surface or damaged.
- Do not use the DUPIXENT Syringe if the Needle Cap is missing or not securely attached.
- Do not touch the Plunger Rod until you are ready to inject.
- Do not inject through clothes.
- Do not get rid of any air bubble in the DUPIXENT Syringe.
- To reduce the risk of accidental needle sticks, each pre-filled syringe has a Needle Shield that is automatically activated to cover the needle after you have given your injection.
- Do not pull back on the Plunger Rod at any time.
- Do not remove the Needle Cap until just before you give the injection.
- Throw away (dispose of) the used DUPIXENT Single-Dose Pre-filled Syringe right away after use. See "Step 13: Dispose" below.
- Do not re-use a DUPIXENT Single-Dose Pre-filled Syringe.
How should I store DUPIXENT? - Keep DUPIXENT Syringes and all medicines out of the reach of children.
- Store DUPIXENT Syringes in the refrigerator between 36°F to 46°F (2°C to 8°C).
- Store DUPIXENT Syringes in the original carton to protect them from light.
- DUPIXENT Syringes can be stored at room temperature up to 77°F (25°C) up to 14 days. Throw away (dispose of) any DUPIXENT Syringes that have been left at room temperature for longer than 14 days.
- Do not shake the DUPIXENT Syringe.
- Do not heat the DUPIXENT Syringe.
- Do not freeze the DUPIXENT Syringe.
- Do not put the DUPIXENT Syringe into direct sunlight.
Step 1: Remove
Remove the DUPIXENT Syringe from the carton by holding the middle of the Syringe Body.
 Do not pull off the Needle Cap until you are ready to inject.
Do not use the DUPIXENT Syringe if it has been dropped on a hard surface or damaged.
Do not pull off the Needle Cap until you are ready to inject.
Do not use the DUPIXENT Syringe if it has been dropped on a hard surface or damaged.
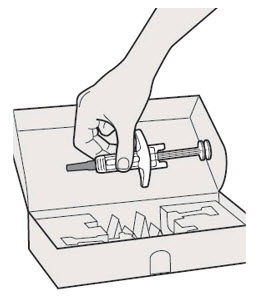
Step 2: Prepare
Ensure you have the following:
- the DUPIXENT Pre-filled Syringe
- 1 alcohol wipe*
- 1 cotton ball or gauze*
- a sharps disposal container* (See Step 13)
*Items not included in the carton
Step 3: Check
When you receive your DUPIXENT Syringes, always check to see that:
- you have the correct medicine and dose.
- the expiration date on the Single-Dose Pre-filled Syringe has not passed.
Do not use the DUPIXENT Syringe if the expiration date has passed.
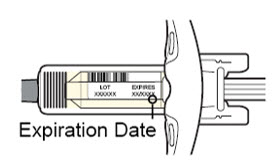
Step 4: Inspect
Look at the medicine through the Viewing Window on the DUPIXENT Syringe:
Check to see if the liquid is clear and colorless to pale yellow.
Note: You may see an air bubble, this is normal.
Do not use the DUPIXENT Syringe if the liquid is discolored or cloudy, or if it contains visible flakes or particles.
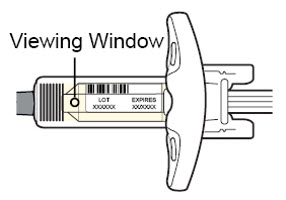
Step 5: Wait 30 minutes
Lay the DUPIXENT Syringe on a flat surface and let it naturally warm to room temperature for at least 30 minutes.
Do not heat the DUPIXENT Syringe.
Do not put the DUPIXENT Syringe into direct sunlight.
Do not keep DUPIXENT Syringes at room temperature for more than 14 days. Throw away (dispose of) any DUPIXENT Syringes that have been left at room temperature for longer than 14 days.
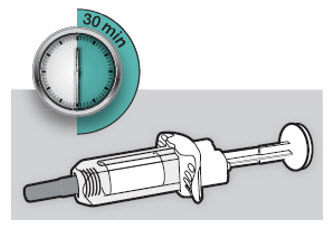
Step 6: Choose your injection site
- You can inject into your thigh or stomach, except for the 2 inches (5 cm) around your belly button (navel).
- If a caregiver injects your dose, they can also use the outer area of the upper arm.
- Choose a different site each time you inject DUPIXENT.
Do not inject into skin that is tender, damaged, bruised or scarred.
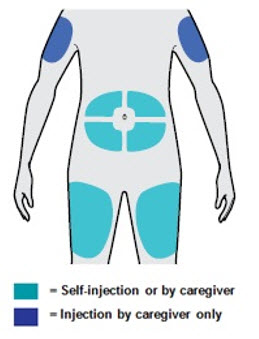
Step 7: Clean
Wash your hands.
Clean the injection site with an alcohol wipe.
Let your skin dry before injecting.
Do not touch the injection site again or blow on it before the injection.

Step 8: Remove Needle Cap
Hold the DUPIXENT Syringe in the middle of the Syringe Body with the Needle pointing away from you and pull off the Needle Cap.
Do not put the Needle Cap back on.
Do not touch the Needle.
Inject your medicine right away after removing the Needle Cap.
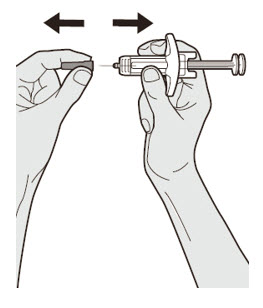
Step 9: Pinch
Pinch a fold of skin at the injection site (thigh or stomach, except 2 inches around your belly button, or outer area of the upper arm if injected by your caregiver). The figure below shows an example of pinching a fold of skin on your stomach.
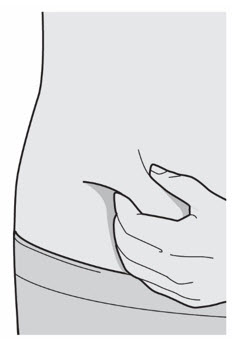
Step 10: Insert
Insert the Needle completely into the fold of the skin at about a 45° angle.
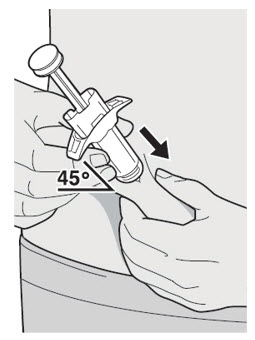
Step 11: Push
Relax the pinch.
Push the Plunger Rod down slowly and steadily as far as it will go until the DUPIXENT Syringe is empty.
Note: You will feel some resistance. This is normal.

Step 12: Release and Remove
Lift your thumb to release the Plunger Rod until the Needle is covered by the Needle Shield and then remove the Syringe from the injection site.
Lightly press a cotton ball or gauze on the injection site if you see any blood.
Do not put the Needle Cap back on.
Do not rub your skin after the injection.
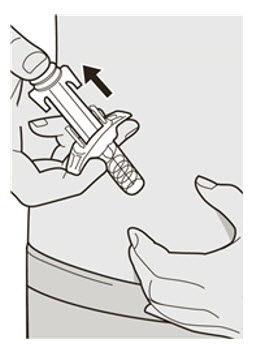
Put your used Needles, DUPIXENT Syringes, and Needle Caps in a FDA-cleared sharps disposal container right away after use.
Do not dispose of (throw away) Needles, DUPIXENT Syringes, and Needle Caps in your household trash.
If you do not have a FDA-cleared sharps disposal container, you may use a household container that is:
- made of a heavy-duty plastic,
- can be closed with a tight-fitting, puncture-resistant lid, without sharps being able to come out,
- upright and stable during use,
- leak-resistant, and
- properly labeled to warn of hazardous waste inside the container
When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to dispose of your sharps disposal container. There may be state or local laws about how you should throw away used Needles and Syringes.
For more information about safe sharps disposal, and for specific information about sharps disposal in the state that you live in, go to the FDA's website at: http://www.fda.gov/safesharpsdisposal
Do not dispose of your used sharps disposal container in your household trash unless your community guidelines permit this. Do not recycle your used sharps disposal container.
Do not put the Needle Cap back on.
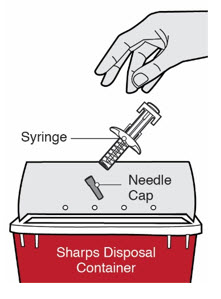

Manufactured by: Regeneron Pharmaceuticals, Inc. Tarrytown, NY 10591
U.S. License No. 1760Marketed by: sanofi-aventis U.S. LLC (Bridgewater, NJ 08807) and Regeneron Pharmaceuticals, Inc. (Tarrytown, NY 10591)
DUPIXENT® is a registered trademark of Sanofi Biotechnology© 2023 Regeneron Pharmaceuticals, Inc. / sanofi-aventis U.S. LLC. All rights reserved.
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Revised: July 2023
-
INSTRUCTIONS FOR USE
Instructions for Use
DUPIXENT® (DU-pix-ent)
(dupilumab)
injection, for subcutaneous use
Single-Dose Pre-filled Pen (300 mg/2 mL)This Instructions for Use contains information on how to inject DUPIXENT.
Read this Instructions for Use before using the DUPIXENT Pre-filled Pen. Do not inject yourself or someone else until you have been shown how to inject DUPIXENT. Your healthcare provider can show you or your caregiver how to prepare and inject a dose of DUPIXENT before you try to do it yourself for the first time. Keep this Instructions for Use. Call your healthcare provider if you have any questions.
This DUPIXENT Pre-filled Pen is only for use in adults and children aged 2 years and older.
This DUPIXENT Pre-filled Pen is a single-dose device. It contains 300 mg of DUPIXENT for injection under the skin (subcutaneous injection).
The parts of the DUPIXENT Pre-filled Pen are shown below:
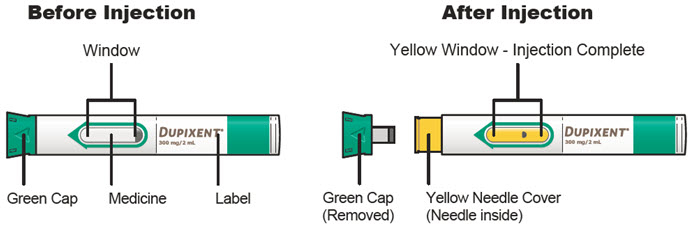
Important Information - Read all of the instructions carefully before using the DUPIXENT Pre-filled Pen.
- Ask your healthcare provider how often you will need to inject the medicine.
- In children 12 years of age and older, it is recommended that DUPIXENT be administered by or under supervision of an adult.
- In children 2 years to less than 12 years of age, DUPIXENT should be given by a caregiver.
- Choose a different injection site for each injection.
- Do not press or touch the Yellow Needle Cover with your fingers.
- Do not inject through clothes.
- Do not remove the Green Cap until just before you give the injection.
- Do not try to put the Green Cap back on the DUPIXENT Pre-filled Pen.
- Throw away (dispose of) the used DUPIXENT Pre-filled Pen right away after use.
- Do not re-use a DUPIXENT Pre-filled Pen.
Storing DUPIXENT - Store unused DUPIXENT Pre-filled Pens in the refrigerator between 36ºF to 46ºF (2ºC to 8ºC).
- Store DUPIXENT Pre-filled Pens in the original carton to protect from light.
- If necessary, you may keep DUPIXENT Pre-filled Pens at room temperature up to 77ºF (25ºC) for up to 14 days.
- Do not store DUPIXENT Pre-filled Pens at room temperature more than 77ºF (25ºC).
- After removing a DUPIXENT Pre-filled Pen from the refrigerator, it must be used within 14 days or thrown away (disposed of).
- Do not shake the DUPIXENT Pre-filled Pen at any time.
- Do not heat the DUPIXENT Pre-filled Pen.
- Do not freeze the DUPIXENT Pre-filled Pen.
- Do not put the DUPIXENT Pre-filled Pen into direct sunlight.
- Keep DUPIXENT Pre-filled Pens and all medicines out of the reach of children.
A. Get ready to inject A1. Gather supplies Find a clean, flat work surface. Make sure you have the following supplies:
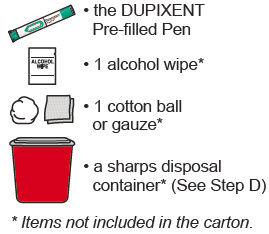
A2. Check the Pen - Do not use the DUPIXENT Pre-filled Pen if it has been damaged.
- Do not use the DUPIXENT Pre-filled Pen if the Green Cap is missing or not securely attached.
- Do not use the DUPIXENT Pre-filled Pen if the Window is yellow before use.

A3. Look at the Label - Check to be sure that you have the correct Medicine and dose.
- Check the expiration date.
-
 Do not use the DUPIXENT Pre-filled Pen if the expiration date has passed.
Do not use the DUPIXENT Pre-filled Pen if the expiration date has passed.

A4. Check the Medicine - Look at the Medicine through the Window: it should be clear and colorless to pale yellow.
- Note: You may see an air bubble, this is normal.
-
 Do not use the DUPIXENT Pre-filled Pen if the liquid is discolored or cloudy, or if it contains visible flakes or particles.
Do not use the DUPIXENT Pre-filled Pen if the liquid is discolored or cloudy, or if it contains visible flakes or particles.

A5. Wait 45 minutes - Lay the DUPIXENT Pre-filled Pen on a flat surface and let it warm up at room temperature less than 77ºF (25ºC) for at least 45 minutes.
-
 Do not heat the DUPIXENT Pre-filled Pen in a microwave, hot water or direct sunlight.
Do not heat the DUPIXENT Pre-filled Pen in a microwave, hot water or direct sunlight.

B. Choose and prepare your injection site B1. Wash your hands well with soap and water 
B2. Choose an injection site - Thigh
- Stomach except for the 2 inches (5 cm) around your belly button (navel).
- A caregiver can also inject in the outer area of the upper arm.
- Choose a different site for each injection.
-
 Do not inject into skin that is tender, damaged, has bruises or scars, or into areas with visible veins.
Do not inject into skin that is tender, damaged, has bruises or scars, or into areas with visible veins. -
 Do not inject through clothes.
Do not inject through clothes.
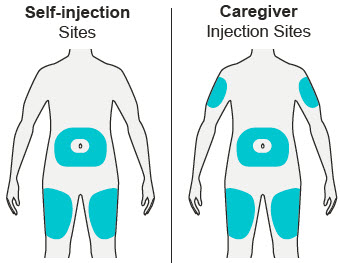
B3. Prepare the injection site - Clean the injection site with an alcohol wipe.
- Let the skin dry before injecting.
-
 Do not touch the injection site again or blow on it before the injection.
Do not touch the injection site again or blow on it before the injection.
C. Give the injection C1. Remove Green Cap - Remove the Green Cap by pulling it straight off, as shown. Do not twist the Green Cap off.
- Do not remove the Green Cap until you are ready to inject.
- Do not press or touch the Yellow Needle Cover with your fingers. The Needle is inside.
-
 Do not put the Green Cap back on the DUPIXENT Pre-filled Pen after you have removed it.
Do not put the Green Cap back on the DUPIXENT Pre-filled Pen after you have removed it.
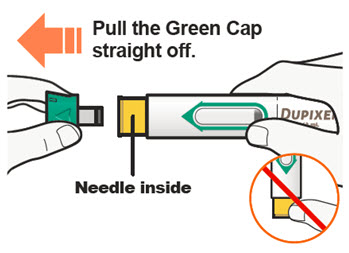
C2. Pinch Skin and Place 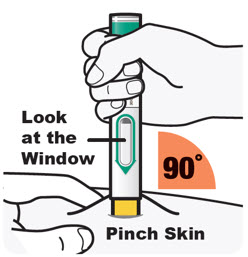
Pinch the skin before and during the injection. - Hold the DUPIXENT Pre-filled Pen as shown so that you can see the Window. Place the Yellow Needle Cover on the skin.
- Place the Yellow Needle Cover on the skin at approximately a 90-degree angle.
- Pinching is not needed for adults and children aged 12 years and older.
C3. Press down ➜ Watch Window turn fully yellow ➜ Then count to 5 
Press and hold the DUPIXENT Pre-filled Pen firmly against the skin until you cannot see the Yellow Needle Cover. - There will be a "click" when the injection starts, and
- The Window will start to turn yellow.
- Keep pressing the DUPIXENT Pre-filled Pen against the skin.
Keep pressing the DUPIXENT Pre-filled Pen against the skin and watch the window:
- The Window will turn completely yellow, and
- You will hear a 2nd "click".
- Keep pressing the DUPIXENT Pre-filled Pen against the skin.
Keep pressing the DUPIXENT Pre-filled Pen against the skin and count to 5 to make sure you get your full dose. Pinching of the skin is not needed for adults and children aged 12 years and older. C4. Remove - After you have completed the injection pull straight up to remove DUPIXENT Pre-filled Pen from the skin. The Yellow Needle Cover will cover the needle.
- If you see any blood at the site, lightly dab a cotton ball or gauze pad.
-
 Do not rub the skin after the injection.
Do not rub the skin after the injection. - If the Window does not turn completely Yellow, or if it looks like medicine is still coming out of the pen, you may not have received a full dose. Dispose of (throw away) the pen and contact your healthcare provider right away.
-
 Do not give a second dose without speaking to your healthcare provider.
Do not give a second dose without speaking to your healthcare provider.

D. Dispose of used DUPIXENT Pre-filled Pen This Instructions for Use has been approved by the U.S. Food and Drug Administration. Revised: July 2023 How to Dispose of (throw away) DUPIXENT Pre-filled Pen:
Put the used DUPIXENT Pre-filled Pens and Green Caps in a FDA-cleared sharps disposal container right away after use.
 Do not dispose of (throw away) DUPIXENT Pre-filled Pens and Green Caps in your household trash.
Do not dispose of (throw away) DUPIXENT Pre-filled Pens and Green Caps in your household trash.
If you do not have a FDA-cleared sharps disposal container, you may use a household container that is:
- made of a heavy-duty plastic,
- can be closed with a tightfitting, puncture-resistant lid, without sharps being able to come out,
- upright and stable during use,
- leak-resistant, and
- properly labeled to warn of hazardous waste inside the container.
For more information about safe sharps disposal, and for specific information about sharps disposal in the state that you live in, go to the FDA's website at: http://www.fda.gov/safesharpsdisposal
 Do not dispose of your used sharps disposal container in your household trash unless your community guidelines permit this.
Do not dispose of your used sharps disposal container in your household trash unless your community guidelines permit this.
 Do not recycle your used sharps disposal container.
Do not recycle your used sharps disposal container.
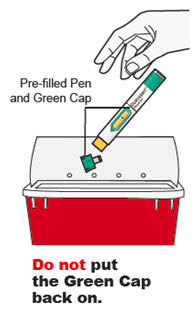
Keep your sharps disposal container out of the reach of children.
Manufactured by:
Regeneron Pharmaceuticals, Inc.
Tarrytown, NY 10591
U.S. License No. 1760
Marketed by:
sanofi-aventis U.S. LLC (Bridgewater, NJ 08807) and
Regeneron Pharmaceuticals, Inc. (Tarrytown, NY 10591)
DUPIXENT® is a registered trademark of Sanofi Biotechnology
© 2023 Regeneron Pharmaceuticals, Inc. / sanofi-aventis U.S. LLC. All rights reserved. -
Instructions for Use
DUPIXENT® (DU-pix-ent)
(dupilumab)
injection, for subcutaneous use
Single-Dose Pre-filled Pen (200 mg/1.14 mL)This Instructions for Use contains information on how to inject DUPIXENT.
Read this Instructions for Use before using the DUPIXENT Pre-filled Pen. Do not inject yourself or someone else until you have been shown how to inject DUPIXENT. Your healthcare provider can show you or your caregiver how to prepare and inject a dose of DUPIXENT before you try to do it yourself for the first time. Keep this Instructions for Use. Call your healthcare provider if you have any questions.
This DUPIXENT Pre-filled Pen is only for use in adults and children aged 2 years and older.
This DUPIXENT Pre-filled Pen is a single-dose device. It contains 200 mg of DUPIXENT for injection under the skin (subcutaneous injection).
The parts of the DUPIXENT Pre-filled Pen are shown below:
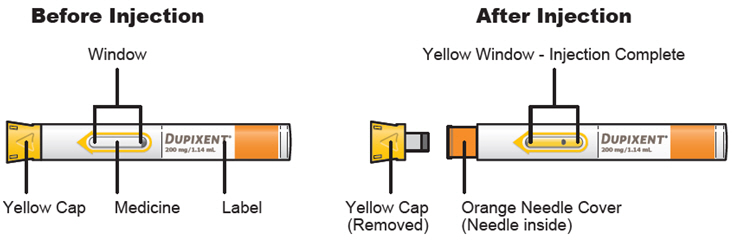
Important Information - Read all of the instructions carefully before using the DUPIXENT Pre-filled Pen.
- Ask your healthcare provider how often you will need to inject the medicine.
- In children 12 years of age and older, it is recommended that DUPIXENT be administered by or under supervision of an adult.
- In children 2 years to less than 12 years of age, DUPIXENT should be given by a caregiver.
- Choose a different injection site for each injection.
- Do not press or touch the Orange Needle Cover with your fingers.
- Do not inject through clothes.
- Do not remove the Yellow Cap until just before you give the injection.
- Do not try to put the Yellow Cap back on the DUPIXENT Pre-filled Pen.
- Throw away (dispose of) the used DUPIXENT Pre-filled Pen right away after use.
- Do not re-use a DUPIXENT Pre-filled Pen.
Storing DUPIXENT - Store unused DUPIXENT Pre-filled Pens in the refrigerator between 36°F to 46°F (2°C to 8°C).
- Store DUPIXENT Pre-filled Pens in the original carton to protect from light.
- If necessary, you may keep DUPIXENT Pre-filled Pens at room temperature up to 77°F (25°C) for up to 14 days.
- Do not store DUPIXENT Pre-filled Pens at room temperature more than 77°F (25°C).
- After removing a DUPIXENT Pre-filled Pen from the refrigerator, it must be used within 14 days or thrown away (disposed of).
- Do not shake the DUPIXENT Pre-filled Pen at any time.
- Do not heat the DUPIXENT Pre-filled Pen.
- Do not freeze the DUPIXENT Pre-filled Pen.
- Do not put the DUPIXENT Pre-filled Pen into direct sunlight.
- Keep DUPIXENT Pre-filled Pens and all medicines out of the reach of children.
A. Get ready to inject A1. Gather supplies Find a clean, flat work surface. Make sure you have the following supplies:
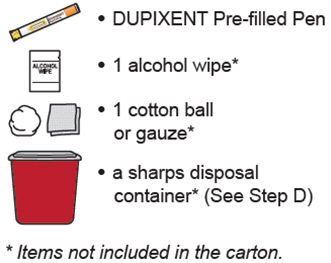
A2. Check the Pen - Do not use the DUPIXENT Pre-filled Pen if it has been damaged.
- Do not use the DUPIXENT Pre-filled Pen if the Yellow Cap is missing or not securely attached.
- Do not use the DUPIXENT Pre-filled Pen if the Window is yellow before use.


A3. Look at the Label - Check to be sure that you have the correct Medicine and dose.
- Check the expiration date.
-
 Do not use the DUPIXENT Pre-filled Pen if the expiration date has passed.
Do not use the DUPIXENT Pre-filled Pen if the expiration date has passed.

A4. Check the Medicine - Look at the Medicine through the Window: it should be clear and colorless to pale yellow.
- Note: You may see an air bubble, this is normal.
-
 Do not use the DUPIXENT Pre-filled Pen if the liquid is discolored or cloudy, or if it contains visible flakes or particles.
Do not use the DUPIXENT Pre-filled Pen if the liquid is discolored or cloudy, or if it contains visible flakes or particles.

A5. Wait 30 minutes - Lay the DUPIXENT Pre-filled Pen on a flat surface and let it warm up at room temperature less than 77°F (25°C) for at least 30 minutes.
-
 Do not heat the DUPIXENT Pre-filled Pen in a microwave, hot water or direct sunlight.
Do not heat the DUPIXENT Pre-filled Pen in a microwave, hot water or direct sunlight.

B. Choose and prepare your injection site B1. Wash your hands well with soap and water 
B2. Choose an injection site - Thigh
- Stomach except for the 2 inches (5 cm) around your belly button (navel).
- A caregiver can also inject in the outer area of the upper arm.
- Choose a different site for each injection.
-
 Do not inject into skin that is tender, damaged, has bruises or scars, or into areas with visible veins.
Do not inject into skin that is tender, damaged, has bruises or scars, or into areas with visible veins. -
 Do not inject through clothes.
Do not inject through clothes.
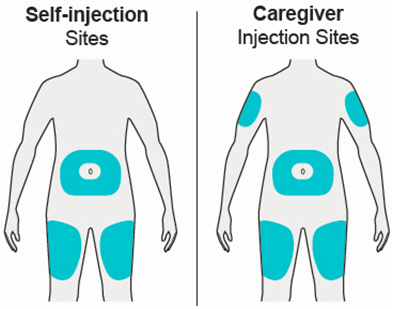
B3. Prepare the injection site - Clean the injection site with an alcohol wipe.
- Let the skin dry before injecting.
-
 Do not touch the injection site again or blow on it before the injection.
Do not touch the injection site again or blow on it before the injection.
C. Give the injection C1. Remove Yellow Cap - Remove the Yellow Cap by pulling it straight off, as shown. Do not twist the Yellow Cap off.
- Do not remove the Yellow Cap until you are ready to inject.
- Do not press or touch the Orange Needle Cover with your fingers. The Needle is inside.
-
 Do not put the Yellow Cap back on the DUPIXENT Pre-filled Pen after you have removed it.
Do not put the Yellow Cap back on the DUPIXENT Pre-filled Pen after you have removed it.
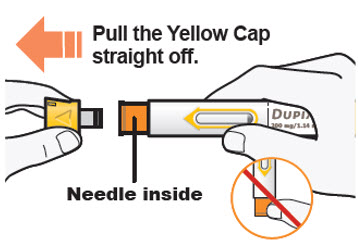
C2. Pinch Skin and Place 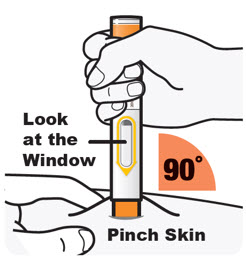
Pinch the skin before and during the injection. - Hold the DUPIXENT Pre-filled Pen as shown so that you can see the Window. Place the Orange Needle Cover on the skin.
- Place the Orange Needle Cover on the skin at approximately a 90-degree angle.
- Pinching is not needed for adults and children aged 12 years and older.
C3. Press down ➜ Watch Window turn fully yellow ➜ Then count to 5 
Press and hold the DUPIXENT Pre-filled Pen firmly against the skin until you cannot see the Orange Needle Cover. - There will be a "click" when the injection starts, and
- The Window will start to turn yellow.
- Keep pressing the DUPIXENT Pre-filled Pen against the skin.
Keep pressing the DUPIXENT Pre-filled Pen against the skin and watch the window:
- The Window will turn completely yellow, and
- You will hear a 2nd "click".
- Keep pressing the DUPIXENT Pre-filled Pen against the skin.
Keep pressing the DUPIXENT Pre-filled Pen against the skin and count to 5 to make sure you get your full dose. Pinching of the skin is not needed for adults and children aged 12 years and older. C4. Remove - After you have completed the injection pull straight up to remove DUPIXENT Pre-filled Pen from the skin. The Orange Needle Cover will cover the needle.
- If you see any blood at the site, lightly dab a cotton ball or gauze pad.
-
 Do not rub the skin after the injection.
Do not rub the skin after the injection. - If the Window does not turn completely Yellow, or if it looks like medicine is still coming out of the pen, you may not have received a full dose. Dispose of (throw away) the pen and contact your healthcare provider right away.
-
 Do not give a second dose without speaking to your healthcare provider.
Do not give a second dose without speaking to your healthcare provider.
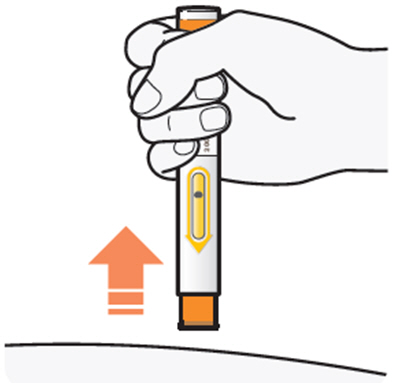
D. Dispose of used DUPIXENT Pre-filled Pen This Instructions for Use has been approved by the U.S. Food and Drug Administration. Revised: July 2023 How to Dispose of (throw away) DUPIXENT Pre-filled Pen:
Put the used DUPIXENT Pre-filled Pens and Yellow Caps in a FDA-cleared sharps disposal container right away after use.
 Do not dispose of (throw away) DUPIXENT Pre-filled Pens and Yellow Caps in your household trash.
Do not dispose of (throw away) DUPIXENT Pre-filled Pens and Yellow Caps in your household trash.
If you do not have a FDA-cleared sharps disposal container, you may use a household container that is:
- made of a heavy-duty plastic,
- can be closed with a tightfitting, puncture-resistant lid, without sharps being able to come out,
- upright and stable during use,
- leak-resistant, and
- properly labeled to warn of hazardous waste inside the container.
For more information about safe sharps disposal, and for specific information about sharps disposal in the state that you live in, go to the FDA's website at: http://www.fda.gov/safesharpsdisposal
 Do not dispose of your used sharps disposal container in your household trash unless your community guidelines permit this.
Do not dispose of your used sharps disposal container in your household trash unless your community guidelines permit this.
 Do not recycle your used sharps disposal container.
Do not recycle your used sharps disposal container.
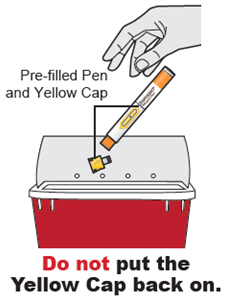
Keep your sharps disposal container out of the reach of children.
Manufactured by:
Regeneron Pharmaceuticals, Inc.
Tarrytown, NY 10591
U.S. License No. 1760
Marketed by:
sanofi-aventis U.S. LLC (Bridgewater, NJ 08807) and
Regeneron Pharmaceuticals, Inc. (Tarrytown, NY 10591)
DUPIXENT® is a registered trademark of Sanofi Biotechnology
© 2023 Regeneron Pharmaceuticals, Inc. / sanofi-aventis U.S. LLC. All rights reserved. -
INSTRUCTIONS FOR USE DUPIXENT® (DU-pix-ent) (dupilumab) injection, for subcutaneous use Single-Dose Pre-filled Syringe with Needle Shield
Read this Instructions for Use before using the DUPIXENT Pre-filled Syringe. Do not inject the child until you have been shown how to inject DUPIXENT. Your healthcare provider can show you how to prepare and inject a dose of DUPIXENT before you try to do it yourself the first time. Keep these instructions for future use. Call your healthcare provider if you have any questions.
This device is a Single-Dose Pre-filled Syringe (called "DUPIXENT Syringe" in these instructions). It contains 100 mg of DUPIXENT for injection under the skin (subcutaneous injection).
The parts of the DUPIXENT Syringe are shown below:
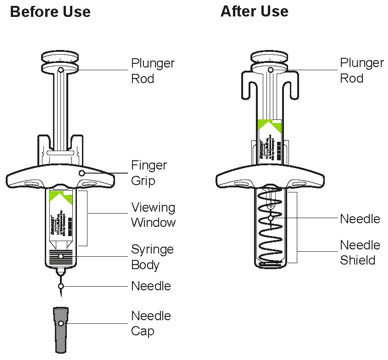
Important Information - Read all of the instructions carefully before using the DUPIXENT Syringe.
- Ask your healthcare provider how often you will need to inject the medicine.
- In children 6 months to less than 12 years of age, DUPIXENT should be given by a caregiver.
- Rotate the injection site each time you inject.
- Do not use the DUPIXENT Syringe if it has been dropped on a hard surface or damaged.
- Do not use the DUPIXENT Syringe if the Needle Cap is missing or not securely attached.
- Do not touch the Plunger Rod until you are ready to inject.
- Do not inject through clothes.
- Do not get rid of any air bubble in the DUPIXENT Syringe.
- To reduce the risk of accidental needle sticks, each pre-filled syringe has a Needle Shield that is automatically activated to cover the needle after you have given the injection.
- Do not pull back on the Plunger Rod at any time.
- Do not remove the Needle Cap until just before you give the injection.
- Throw away (dispose of) the used DUPIXENT Single-Dose Pre-filled Syringe right away after use. See "Step 13: Dispose" below.
- Do not re-use a DUPIXENT Single-Dose Pre-filled Syringe.
How should I store DUPIXENT? - Keep DUPIXENT Syringes and all medicines out of the reach of children.
- Store DUPIXENT Syringes in the refrigerator between 36°F to 46°F (2°C to 8°C).
- Store DUPIXENT Syringes in the original carton to protect them from light.
- DUPIXENT Syringes can be stored at room temperature up to 77°F (25°C) up to 14 days. Throw away (dispose of) any DUPIXENT Syringes that have been left at room temperature for longer than 14 days.
- Do not shake the DUPIXENT Syringe.
- Do not heat the DUPIXENT Syringe.
- Do not freeze the DUPIXENT Syringe.
- Do not put the DUPIXENT Syringe into direct sunlight.
Step 1: Remove
Remove the DUPIXENT Syringe from the carton by holding the middle of the Syringe Body.
 Do not pull off the Needle Cap until you are ready to inject.
Do not pull off the Needle Cap until you are ready to inject.
 Do not use the DUPIXENT Syringe if it has been dropped on a hard surface or damaged.
Do not use the DUPIXENT Syringe if it has been dropped on a hard surface or damaged.
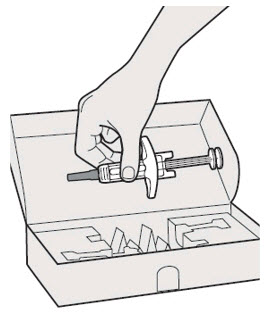
Step 2: Prepare
Ensure you have the following:
- the DUPIXENT Pre-filled Syringe
- 1 alcohol wipe*
- 1 cotton ball or gauze*
- a sharps disposal container* (See Step 13)
*Items not included in the carton
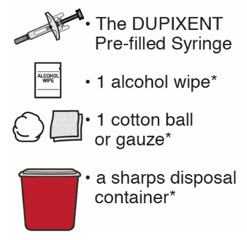
Step 3: Check
When you receive the DUPIXENT Syringes, always check to see that:
- you have the correct medicine and dose.
- the expiration date on the Single-Dose Pre-filled Syringe has not passed.
 Do not use the DUPIXENT Syringe if the expiration date has passed.
Do not use the DUPIXENT Syringe if the expiration date has passed.
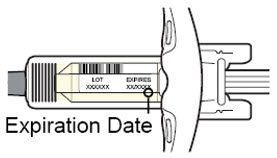
Step 4: Inspect
Look at the medicine through the Viewing Window on the DUPIXENT Syringe:
Check to see if the liquid is clear and colorless to pale yellow.
Note: You may see an air bubble, this is normal.
 Do not use the DUPIXENT Syringe if the liquid is discolored or cloudy, or if it contains visible flakes or particles.
Do not use the DUPIXENT Syringe if the liquid is discolored or cloudy, or if it contains visible flakes or particles.
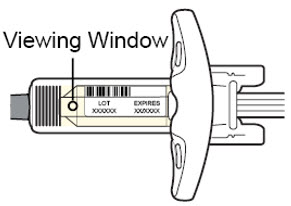
Step 5: Wait 30 minutes
Lay the DUPIXENT Syringe on a flat surface and let it naturally warm to room temperature for at least 30 minutes.
 Do not heat the DUPIXENT Syringe.
Do not heat the DUPIXENT Syringe.
 Do not put the DUPIXENT Syringe into direct sunlight.
Do not put the DUPIXENT Syringe into direct sunlight.
 Do not keep DUPIXENT Syringes at room temperature for more than 14 days. Throw away (dispose of) any DUPIXENT Syringes that have been left at room temperature for longer than 14 days.
Do not keep DUPIXENT Syringes at room temperature for more than 14 days. Throw away (dispose of) any DUPIXENT Syringes that have been left at room temperature for longer than 14 days.
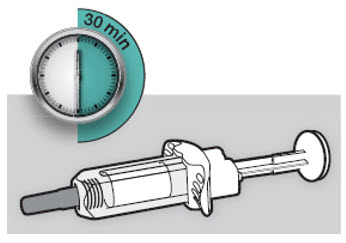
Step 6: Choose the injection site
- You can inject into the thigh, outer area of the upper arm or stomach, except for the 2 inches (5 cm) around the belly button (navel).
- Choose a different site each time you inject DUPIXENT.
 Do not inject into skin that is tender, damaged, bruised or scarred.
Do not inject into skin that is tender, damaged, bruised or scarred.
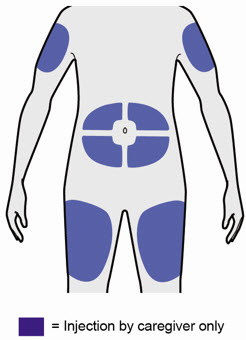
Step 7: Clean
Wash your hands.
Clean the injection site with an alcohol wipe.
Let the skin dry before injecting.
 Do not touch the injection site again or blow on it before the injection.
Do not touch the injection site again or blow on it before the injection.

Step 8: Remove Needle Cap
Hold the DUPIXENT Syringe in the middle of the Syringe Body with the Needle pointing away from you and pull off the Needle Cap.
 Do not put the Needle Cap back on.
Do not put the Needle Cap back on.
 Do not touch the Needle.
Do not touch the Needle.
Inject the medicine right away after removing the Needle Cap.
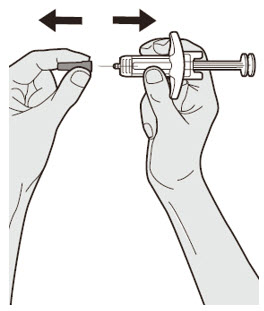
Step 9: Pinch
Pinch a fold of skin at the injection site (thigh or stomach, except 2 inches around the belly button, or outer area of the upper arm). The figure below shows an example of pinching a fold of skin on the stomach.
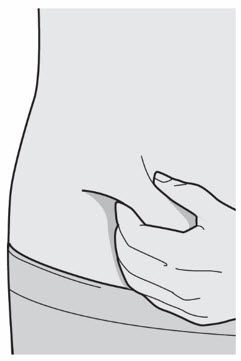
Step 10: Insert
Insert the Needle completely into the fold of the skin at about a 45° angle.
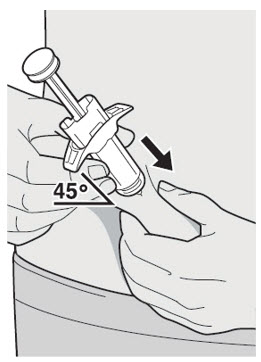
Step 11: Push
Relax the pinch.
Push the Plunger Rod down slowly and steadily as far as it will go until the DUPIXENT Syringe is empty.
Note: You will feel some resistance. This is normal.

Step 12: Release and Remove
Lift your thumb to release the Plunger Rod until the Needle is covered by the Needle Shield and then remove the Syringe from the injection site.
Lightly press a cotton ball or gauze on the injection site if you see any blood.
 Do not put the Needle Cap back on.
Do not put the Needle Cap back on.
 Do not rub the skin after the injection.
Do not rub the skin after the injection.

Put used Needles, DUPIXENT Syringes, and Needle Caps in a FDA-cleared sharps disposal container right away after use.
 Do not dispose of (throw away) Needles, DUPIXENT Syringes, and Needle Caps in your household trash.
Do not dispose of (throw away) Needles, DUPIXENT Syringes, and Needle Caps in your household trash.
If you do not have a FDA-cleared sharps disposal container, you may use a household container that is:
- made of a heavy-duty plastic,
- can be closed with a tight-fitting, puncture-resistant lid, without sharps being able to come out,
- upright and stable during use,
- leak-resistant, and
- properly labeled to warn of hazardous waste inside the container
When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to dispose of your sharps disposal container. There may be state or local laws about how you should throw away used Needles and Syringes.
For more information about safe sharps disposal, and for specific information about sharps disposal in the state that you live in, go to the FDA's website at: http://www.fda.gov/safesharpsdisposal
Do not dispose of your used sharps disposal container in your household trash unless your community guidelines permit this. Do not recycle your used sharps disposal container.
 Do not put the Needle Cap back on.
Do not put the Needle Cap back on.
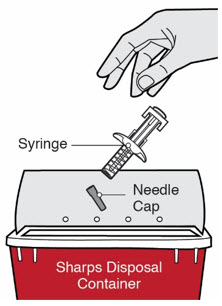

Manufactured by: Regeneron Pharmaceuticals, Inc. Tarrytown, NY 10591
U.S. License No. 1760Marketed by: sanofi-aventis U.S. LLC (Bridgewater, NJ 08807) and Regeneron Pharmaceuticals,
Inc. (Tarrytown, NY 10591)
DUPIXENT® is a registered trademark of Sanofi Biotechnology© 2023 Regeneron Pharmaceuticals, Inc. / sanofi-aventis U.S. LLC. All rights reserved.
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Revised: July 2023
-
PRINCIPAL DISPLAY PANEL - 300 mg/2 mL Syringe Carton - 5914
NDC 0024-5914-01
Rx Only
DUPIXENT®
(dupilumab)
Injection300 mg/2 mL (150 mg/mL)
For Subcutaneous Use Only.
300 mg/2 mL
2
Single-dose
Pre-filled Syringes
with Needle ShieldKeep out of reach of children. Do not use after
expiration. Do not use if seal is broken or damaged.Store refrigerated at 36° to 46°F (2° to 8°C) in the original carton.
Dosage and Administration: See package insert for dosage information and directions for use.sanofi | REGENERON
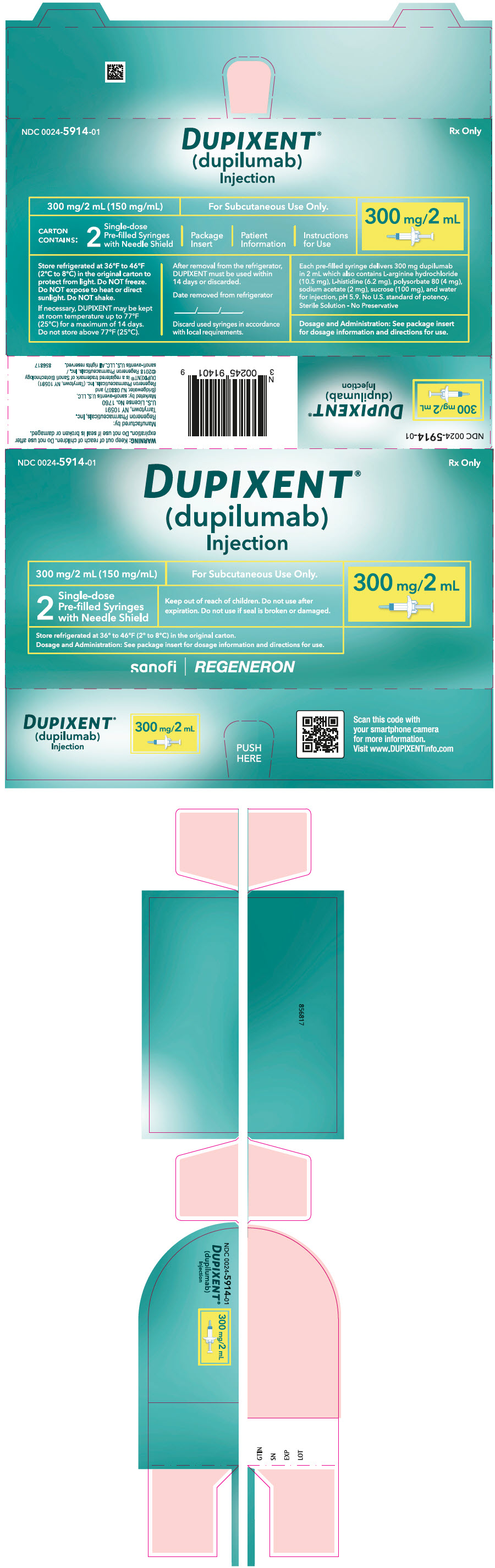
-
PRINCIPAL DISPLAY PANEL - 200 mg/1.14 mL Syringe Carton
NDC 0024-5918-01
Rx Only
DUPIXENT®
(dupilumab)
Injection200 mg/1.14 mL (175 mg/mL)
For Subcutaneous Use Only.
200 mg/1.14 mL
2
Single-dose
Pre-filled Syringes
with Needle ShieldKeep out of reach of children. Do not use after
expiration. Do not use if seal is broken or damaged.Store refrigerated at 36° to 46°F (2° to 8°C) in the original carton.
Dosage and Administration: See package insert for dosage information and directions for use.sanofi | REGENERON
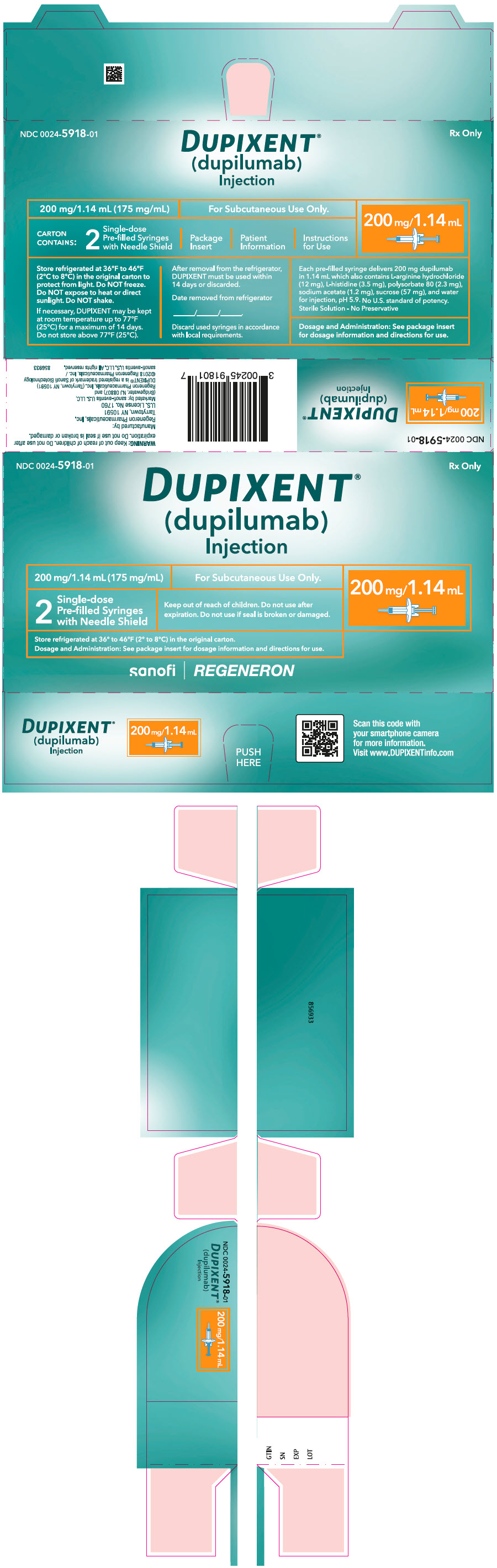
-
PRINCIPAL DISPLAY PANEL - 300 mg/2 mL Pre-filled Pen Carton
NDC 0024-5915-02
Rx Only
DUPIXENT®
(dupilumab)
Injection
Single-dose Pre-filled Pen300 mg/2 mL (150 mg/mL)
For Subcutaneous Use Only.
2
Single-dose
Pre-filled PensKeep out of reach of children. Do not use
after expiration. Do not use if seal is broken
or damaged.Store refrigerated at 36° to 46°F (2° to 8°C) in the original carton.
Do NOT freeze. Do NOT heat.
Dosage and Administration: See package insert for dosage information
and directions for use.300 mg/2 mL
sanofi | REGENERON
-
PRINCIPAL DISPLAY PANEL - 200 mg/1.14 mL Pre-filled Pen Carton
NDC 0024-5919-02
Rx Only
DUPIXENT®
(dupilumab)
Injection
Single-dose Pre-filled Pen200 mg/1.14 mL (175 mg/mL)
For Subcutaneous Use Only.
2
Single-dose
Pre-filled PensKeep out of reach of children. Do not use after
expiration. Do not use if seal is broken or damaged.Store refrigerated at 36° to 46°F (2° to 8°C) in
the original carton. Do not freeze. Do not heat.
Dosage and Administration: See package insert
for dosage information and directions for use.200 mg/1.14 mL
sanofi | REGENERON
-
PRINCIPAL DISPLAY PANEL - 100 mg/0.67 mL Syringe Carton
NDC 0024-5911-02
Rx Only
DUPIXENT®
(dupilumab)
Injection100 mg/0.67 mL (150 mg/mL)
For Subcutaneous Use Only.
2
Single-dose
Pre-filled Syringes
with Needle ShieldKeep out of reach of children. Do not use after
expiration. Do not use if seal is broken or damaged.Store refrigerated at 36° to 46°F (2° to 8°C) in the original carton.
Dosage and Administration: See package insert for dosage information and directions for use.100 mg/0.67 mL
sanofi | REGENERON
-
INGREDIENTS AND APPEARANCE
DUPIXENT
dupilumab injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:0024-5914 Route of Administration SUBCUTANEOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Dupilumab (UNII: 420K487FSG) (Dupilumab - UNII:420K487FSG) Dupilumab 300 mg in 2 mL Inactive Ingredients Ingredient Name Strength ARGININE HYDROCHLORIDE (UNII: F7LTH1E20Y) HISTIDINE (UNII: 4QD397987E) polysorbate 80 (UNII: 6OZP39ZG8H) sodium acetate (UNII: 4550K0SC9B) sucrose (UNII: C151H8M554) water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:0024-5914-01 2 in 1 CARTON 03/28/2017 1 NDC:0024-5914-00 2 mL in 1 SYRINGE, GLASS; Type 3: Prefilled Biologic Delivery Device/System (syringe, patch, etc.) 2 NDC:0024-5914-02 2 in 1 CARTON 07/01/2018 2 NDC:0024-5914-20 2 mL in 1 SYRINGE, GLASS; Type 3: Prefilled Biologic Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA761055 03/28/2017 DUPIXENT
dupilumab injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:0024-5918 Route of Administration SUBCUTANEOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Dupilumab (UNII: 420K487FSG) (Dupilumab - UNII:420K487FSG) Dupilumab 200 mg in 1.14 mL Inactive Ingredients Ingredient Name Strength ARGININE HYDROCHLORIDE (UNII: F7LTH1E20Y) HISTIDINE (UNII: 4QD397987E) polysorbate 80 (UNII: 6OZP39ZG8H) sodium acetate (UNII: 4550K0SC9B) sucrose (UNII: C151H8M554) water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:0024-5918-01 2 in 1 CARTON 10/19/2018 1 NDC:0024-5918-00 1.14 mL in 1 SYRINGE, GLASS; Type 3: Prefilled Biologic Delivery Device/System (syringe, patch, etc.) 2 NDC:0024-5918-02 2 in 1 CARTON 10/19/2018 2 NDC:0024-5918-20 1.14 mL in 1 SYRINGE, GLASS; Type 3: Prefilled Biologic Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA761055 10/19/2018 DUPIXENT
dupilumab injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:0024-5915 Route of Administration SUBCUTANEOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Dupilumab (UNII: 420K487FSG) (Dupilumab - UNII:420K487FSG) Dupilumab 300 mg in 2 mL Inactive Ingredients Ingredient Name Strength ARGININE HYDROCHLORIDE (UNII: F7LTH1E20Y) HISTIDINE (UNII: 4QD397987E) polysorbate 80 (UNII: 6OZP39ZG8H) sodium acetate (UNII: 4550K0SC9B) sucrose (UNII: C151H8M554) water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:0024-5915-02 2 in 1 CARTON 06/19/2020 1 NDC:0024-5915-00 2 mL in 1 SYRINGE, GLASS; Type 3: Prefilled Biologic Delivery Device/System (syringe, patch, etc.) 2 NDC:0024-5915-20 2 in 1 CARTON 06/19/2020 2 NDC:0024-5915-01 2 mL in 1 SYRINGE, GLASS; Type 3: Prefilled Biologic Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA761055 06/19/2020 DUPIXENT
dupilumab injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:0024-5919 Route of Administration SUBCUTANEOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Dupilumab (UNII: 420K487FSG) (Dupilumab - UNII:420K487FSG) Dupilumab 200 mg in 1.14 mL Inactive Ingredients Ingredient Name Strength ARGININE HYDROCHLORIDE (UNII: F7LTH1E20Y) HISTIDINE (UNII: 4QD397987E) polysorbate 80 (UNII: 6OZP39ZG8H) sodium acetate (UNII: 4550K0SC9B) sucrose (UNII: C151H8M554) water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:0024-5919-02 2 in 1 CARTON 06/14/2021 1 NDC:0024-5919-00 1.14 mL in 1 SYRINGE, GLASS; Type 3: Prefilled Biologic Delivery Device/System (syringe, patch, etc.) 2 NDC:0024-5919-20 2 in 1 CARTON 06/14/2021 2 NDC:0024-5919-01 1.14 mL in 1 SYRINGE, GLASS; Type 3: Prefilled Biologic Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA761055 06/14/2021 DUPIXENT
dupilumab injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:0024-5911 Route of Administration SUBCUTANEOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Dupilumab (UNII: 420K487FSG) (Dupilumab - UNII:420K487FSG) Dupilumab 100 mg in 0.67 mL Inactive Ingredients Ingredient Name Strength ARGININE HYDROCHLORIDE (UNII: F7LTH1E20Y) HISTIDINE (UNII: 4QD397987E) polysorbate 80 (UNII: 6OZP39ZG8H) sodium acetate (UNII: 4550K0SC9B) sucrose (UNII: C151H8M554) water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:0024-5911-02 2 in 1 CARTON 10/20/2021 07/31/2026 1 NDC:0024-5911-00 0.67 mL in 1 SYRINGE, GLASS; Type 3: Prefilled Biologic Delivery Device/System (syringe, patch, etc.) 2 NDC:0024-5911-20 2 in 1 CARTON 10/20/2021 07/31/2026 2 NDC:0024-5911-01 0.67 mL in 1 SYRINGE, GLASS; Type 3: Prefilled Biologic Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA761055 10/20/2021 Labeler - sanofi-aventis U.S. LLC (824676584) Establishment Name Address ID/FEI Business Operations Regeneron Pharmaceuticals, Inc. 945589711 API MANUFACTURE(0024-5914, 0024-5918, 0024-5915, 0024-5919, 0024-5911) , ANALYSIS(0024-5914, 0024-5918, 0024-5915, 0024-5919, 0024-5911) Establishment Name Address ID/FEI Business Operations Sanofi-Winthrop Industrie 297730488 ANALYSIS(0024-5914, 0024-5918, 0024-5915, 0024-5919, 0024-5911) , MANUFACTURE(0024-5914, 0024-5918, 0024-5915, 0024-5919, 0024-5911) , LABEL(0024-5914, 0024-5918, 0024-5911) , PACK(0024-5914, 0024-5918, 0024-5911) Establishment Name Address ID/FEI Business Operations Sanofi-Aventis Deutschland GmbH 313218430 ANALYSIS(0024-5914, 0024-5918, 0024-5915, 0024-5919, 0024-5911) , MANUFACTURE(0024-5915, 0024-5919) , LABEL(0024-5915, 0024-5919) , PACK(0024-5915, 0024-5919) Establishment Name Address ID/FEI Business Operations Regeneron Ireland Designated Activity Company 986063166 API MANUFACTURE(0024-5914, 0024-5918, 0024-5915, 0024-5919, 0024-5911) , ANALYSIS(0024-5914, 0024-5918, 0024-5915, 0024-5919, 0024-5911) Establishment Name Address ID/FEI Business Operations Genzyme Ireland Limited 985127419 ANALYSIS(0024-5914, 0024-5915) , MANUFACTURE(0024-5914, 0024-5915) , LABEL(0024-5914) , PACK(0024-5914)