Label: LOPINAVIR-RITONAVIR solution

- NDC Code(s): 0527-1947-48
- Packager: Lannett Company, Inc.
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: Abbreviated New Drug Application
Drug Label Information
Updated November 18, 2020
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Medication Guide: HTML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use LOPINAVIR AND RITONAVIR ORAL SOLUTION safely and effectively. See full prescribing information for LOPINAVIR AND RITONAVIR ORAL SOLUTION.
LOPINAVIR AND RITONAVIR oral solution
Initial U.S. Approval: 2000RECENT MAJOR CHANGES
Contraindications (4) 12/2019
INDICATIONS AND USAGE
Lopinavir and ritonavir is an HIV-1 protease inhibitor indicated in combination with other antiretroviral agents for the treatment of HIV-1 infection in adults and pediatric patients (14 days and older). (1)
DOSAGE AND ADMINISTRATION
Oral solution: must be taken with food. (2.1)
Lopinavir and ritonavir oral solution is not recommended for use with polyurethane feeding tubes due to potential incompatibility. Feeding tubes composed of silicone or polyvinyl chloride (PVC) can be used. (2.2)
Adults (2.3):
- Total recommended daily dosage is 800/200 mg given once or twice daily.
- Lopinavir and ritonavir can be given as once daily or twice daily regimen. See Full Prescribing Information for details.
- Lopinavir and ritonavir once daily dosing regimen is not recommended in:
- Adult patients with three or more of the following lopinavir resistance-associated substitutions: L10F/I/R/V, K20M/N/R, L24I, L33F, M36I, I47V, G48V, I54L/T/V, V82A/C/F/S/T, and I84V. (12.4)
- In combination with carbamazepine, phenobarbital, or phenytoin. (7.3)
- In combination with efavirenz, nevirapine, or nelfinavir. (12.3)
- In pregnant women. (2.5, 8.1, 12.3)
Pediatric Patients (14 days and older) (2.4):
- Lopinavir and ritonavir once daily dosing regimen is not recommended in pediatric patients.
- Twice daily dose is based on body weight or body surface area.
Concomitant Therapy in Adults and Pediatric Patients:
- Dose adjustments of lopinavir and ritonavir may be needed when co-administering with efavirenz, nevirapine, or nelfinavir. (2.3, 2.4, 7.3)
- Lopinavir and ritonavir oral solution should not be administered to neonates before a postmenstrual age (first day of the mother’s last menstrual period to birth plus the time elapsed after birth) of 42 weeks and a postnatal age of at least 14 days has been attained (2.4, 5.2)
Pregnancy (2.5):
- 400/100 mg twice daily in pregnant patients with no documented lopinavir-associated resistance substitutions.
- There are insufficient data to recommend a lopinavir and ritonavir dose for pregnant patients with any documented lopinavir and ritonavir-associated resistance substitutions.
- No dose adjustment of lopinavir and ritonavir is required for patients during the postpartum period.
DOSAGE FORMS AND STRENGTHS
- Oral solution: 80 mg lopinavir and 20 mg ritonavir per milliliter (3)
CONTRAINDICATIONS
- Hypersensitivity to lopinavir and ritonavir (e.g., toxic epidermal necrolysis, Stevens-Johnson syndrome, erythema multiforme, urticaria, angioedema) or any of its ingredients, including ritonavir. (4)
- Co-administration with drugs highly dependent on CYP3A for clearance and for which elevated plasma levels may result in serious and/or life-threatening events. (4)
- Co-administration with potent CYP3A inducers where significantly reduced lopinavir plasma concentrations may be associated with the potential for loss of virologic response and possible resistance and cross resistance. (4)
WARNINGS AND PRECAUTIONS
The following have been observed in patients receiving lopinavir and ritonavir:
- The concomitant use of lopinavir and ritonavir and certain other drugs may result in known or potentially significant drug interactions. Consult the full prescribing information prior to and during treatment for potential drug interactions. (5.1, 7.3)
- Toxicity in preterm neonates: Lopinavir and ritonavir oral solution should not be used in preterm neonates in the immediate postnatal period because of possible toxicities. A safe and effective dose of lopinavir and ritonavir oral solution in this patient population has not been established. (2.4, 5.2)
- Pancreatitis: Fatalities have occurred; suspend therapy as clinically appropriate. (5.3)
- Hepatotoxicity: Fatalities have occurred. Monitor liver function before and during therapy, especially in patients with underlying hepatic disease, including hepatitis B and hepatitis C, or marked transaminase elevations. (5.4, 8.6)
- QT interval prolongation and isolated cases of torsade de pointes have been reported although causality could not be established. Avoid use in patients with congenital long QT syndrome, those with hypokalemia, and with other drugs that prolong the QT interval. (5.1, 5.5, 12.3)
- PR interval prolongation may occur in some patients. Cases of second and third degree heart block have been reported. Use with caution in patients with pre-existing conduction system disease, ischemic heart disease, cardiomyopathy, underlying structural heart disease or when administering with other drugs that may prolong the PR interval. (5.1, 5.6, 12.3)
- Patients may develop new onset or exacerbations of diabetes mellitus, hyperglycemia (5.7), immune reconstitution syndrome (5.8), redistribution/accumulation of body fat. (5.10)
- Total cholesterol and triglycerides elevations. Monitor prior to therapy and periodically thereafter. (5.9)
- Hemophilia: Spontaneous bleeding may occur, and additional factor VIII may be required. (5.11)
ADVERSE REACTIONS
Commonly reported adverse reactions to lopinavir and ritonavir included diarrhea, nausea, vomiting, hypertriglyceridemia and hypercholesterolemia. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Lannett Company, Inc. at 1-844-834-0530 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch
DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
Lactation: Breastfeeding not recommended. (8.2)
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 11/2020
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 General Administration Recommendations
2.2 Administering Oral Solution by Feeding Tube
2.3 Dosage Recommendations in Adults
2.4 Dosage Recommendations in Pediatric Patients
2.5 Dosage Recommendations in Pregnancy
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Risk of Serious Adverse Reactions Due to Drug Interactions
5.2 Toxicity in Preterm Neonates
5.3 Pancreatitis
5.4 Hepatotoxicity
5.5 QT Interval Prolongation
5.6 PR Interval Prolongation
5.7 Diabetes Mellitus/Hyperglycemia
5.8 Immune Reconstitution Syndrome
5.9 Lipid Elevations
5.10 Fat Redistribution
5.11 Patients with Hemophilia
5.12 Resistance/Cross-resistance
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
7.1 Potential for Lopinavir and Ritonavir to Affect Other Drugs
7.2 Potential for Other Drugs to Affect Lopinavir
7.3 Established and Other Potentially Significant Drug Interactions
7.4 Drugs with No Observed or Predicted Interactions with Lopinavir and Ritonavir
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Hepatic Impairment
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
12.4 Microbiology
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
14.1 Adult Patients without Prior Antiretroviral Therapy
14.2 Adult Patients with Prior Antiretroviral Therapy
14.3 Other Studies Supporting Approval in Adult Patients
14.4 Pediatric Studies
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
Lopinavir and ritonavir is indicated in combination with other antiretroviral agents for the treatment of HIV-1 infection in adults and pediatric patients 14 days and older.
Limitations of Use:
-
Genotypic or phenotypic testing and/or treatment history should guide the use of lopinavir and ritonavir. The number of baseline lopinavir resistance-associated substitutions affects the virologic response to lopinavir and ritonavir [see Microbiology (12.4)].
-
-
2 DOSAGE AND ADMINISTRATION
2.1 General Administration Recommendations
Lopinavir and ritonavir oral solution must be taken with food.
2.2 Administering Oral Solution by Feeding Tube
Because lopinavir and ritonavir oral solution contains ethanol and propylene glycol, it is not recommended for use with polyurethane feeding tubes due to potential incompatibility. Feeding tubes that are compatible with ethanol and propylene glycol, such as silicone and polyvinyl chloride (PVC) feeding tubes, can be used for administration of lopinavir and ritonavir oral solution. Follow instructions for use of the feeding tube to administer the medicine.
2.3 Dosage Recommendations in Adults
Lopinavir and ritonavir can be given in once daily or twice daily dosing regimen at dosages noted in Tables 1 and 2. Lopinavir and ritonavir once daily dosing regimen is not recommended in:
-
Adult patients with three or more of the following lopinavir resistance-associated substitutions: L10F/I/R/V, K20M/N/R, L24I, L33F, M36I, I47V, G48V, I54L/T/V, V82A/C/F/S/T, and I84V [see Microbiology (12.4)].
-
In combination with carbamazepine, phenobarbital, or phenytoin [see Drug Interactions (7.3)].
-
In combination with efavirenz, nevirapine, or nelfinavir [see Drug Interactions (7.3) and Clinical Pharmacology (12.3)].
-
In pediatric patients younger than 18 years of age [see Dosage and Administration (2.4)].
-
In pregnant women [see Dosage and Administration (2.5), Use in Specific Populations (8.1) and Clinical Pharmacology (12.3)].
Table 1. Recommended Dosage in Adults – Lopinavir and Ritonavir Once Daily Regimen
Lopinavir and Ritonavir Dosage Form
Recommended Dosage
80 mg/20 mg per mL Oral Solution
800 mg/200 mg (10 mL) once daily
Table 2. Recommended Dosage in Adults – Lopinavir and Ritonavir Twice Daily Regimen
Lopinavir and Ritonavir Dosage Form
Recommended Dosage
80 mg/20 mg per mL Oral Solution
400 mg/100 mg (5 mL) twice daily
The dose of lopinavir and ritonavir must be increased when administered in combination with efavirenz, nevirapine or nelfinavir. Table 3 outlines the dosage recommendations for twice daily dosing when lopinavir and ritonavir is taken in combination with these agents.
Table 3. Recommended Dosage in Adults – Lopinavir and Ritonavir Twice Daily Regimen in Combination with Efavirenz, Nevirapine, or Nelfinavir Lopinavir and Ritonavir Dosage Form
Recommended Dosage
80 mg/20 mg per mL Oral Solution
520 mg/130 mg (6.5 mL) twice daily
2.4 Dosage Recommendations in Pediatric Patients
Lopinavir and ritonavir oral solution is not recommended for once daily dosing in pediatric patients younger than 18 years of age. The dose of the oral solution should be administered using the calibrated cup (supplied) or oral dosing syringe.
Lopinavir and ritonavir oral solution is not recommended in neonates before a postmenstrual age (first day of the mother’s last menstrual period to birth plus the time elapsed after birth) of 42 weeks and a postnatal age of at least 14 days has been attained [see Warnings and Precautions (5.2)].
Lopinavir and ritonavir oral solution contains approximately 42% (v/v) ethanol and approximately 15% (w/v) propylene glycol. Total amounts of ethanol and propylene glycol from all medicines that are to be given to pediatric patients 14 days to 6 months of age should be taken into account in order to avoid toxicity from these excipients [see Warnings and Precautions (5.2) and Overdosage (10)].
Pediatric Dosage Calculations
Calculate the appropriate dose of lopinavir and ritonavir for each individual pediatric patient based on body weight (kg) or body surface area (BSA) to avoid underdosing or exceeding the recommended adult dose.
Body surface area (BSA) can be calculated as follows:
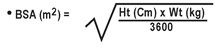
The lopinavir and ritonavir dose can be calculated based on weight or BSA:
Based on Weight:
Patient Weight (kg) × Prescribed lopinavir dose (mg/kg) = Administered lopinavir dose (mg)
Based on BSA:
Patient BSA (m2) × Prescribed lopinavir dose (mg/m2) = Administered lopinavir dose (mg)
If lopinavir and ritonavir oral solution is used, the volume (mL) of lopinavir and ritonavir solution can be determined as follows:
Volume of lopinavir and ritonavir solution (mL) = Administered lopinavir dose (mg) ÷ 80 (mg/mL)
Oral Solution Dosage Recommendation in Pediatric Patients 14 Days to Less Than 18 Years:
Table 4 summarizes the recommended daily dosing regimen for pediatric patients 14 days to less than 18 years of age using the oral solution.
Lopinavir and ritonavir administered in combination with efavirenz, nevirapine, or nelfinavir in patients younger than 6 months of age is not recommended. Total dose of lopinavir and ritonavir oral solution in pediatric patients should not exceed the recommended adult daily dose of 400/100 mg (5mL) twice daily.
Table 4. Lopinavir and Ritonavir Oral Solution Daily Dosage Recommendations in Pediatric Patients 14 days to Less Than 18 Years Without Concomitant Efavirenz, Nevirapine, or Nelfinavir
Patient Age Based on Weight (mg/kg)
Based on BSA (mg/m2) Frequency 14 days to 6 months 16/4 300/75 Given twice daily Older than 6 months to less than 18 years Less than 15 kg 12/3 230/57.5 Given twice daily 15 kg to 40 kg 10/2.5
Concomitant Therapy: Efavirenz, Nevirapine, or Nelfinavir
Dosing recommendations using oral solution
Table 6 provides the dosing recommendations for pediatric patients older than 6 months to less than 18 years of age based on body weight or body surface area for lopinavir and ritonavir oral solution when given in combination with efavirenz, nevirapine, or nelfinavir:
Table 6. Lopinavir and Ritonavir Oral Solution Daily Dosage Recommendations for Pediatric Patients > 6 Months to < 18 Years of Age With Concomitant Efavirenz, Nevirapine, or Nelfinavir Patient Age
Based on Weight
(mg/kg)Based on BSA
(mg/m2)Frequency
> 6 months to < 18 years
<15 kg
13/3.25
300/75
Given twice daily
≥15 kg to 45 kg
11/2.75
2.5 Dosage Recommendations in Pregnancy
Administer 400/100 mg of lopinavir and ritonavir twice daily in pregnant patients with no documented lopinavir-associated resistance substitutions.
-
Once daily lopinavir and ritonavir dosing is not recommended in pregnancy [see Use in Specific Populations (8.1) and Clinical Pharmacology (12.3)].
-
There are insufficient data to recommend dosing in pregnant women with any documented lopinavir-associated resistance substitutions.
-
No dosage adjustment of lopinavir and ritonavir is required for patients during the postpartum period.
-
Avoid use of lopinavir and ritonavir oral solution in pregnant women [see Use in Specific Populations (8.1)].
-
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
-
Lopinavir and ritonavir is contraindicated in patients with previously demonstrated clinically significant hypersensitivity (e.g., toxic epidermal necrolysis, Stevens-Johnson syndrome, erythema multiforme, urticaria, angioedema) to any of its ingredients, including ritonavir.
-
Lopinavir and ritonavir is contraindicated with drugs that are highly dependent on CYP3A for clearance and for which elevated plasma concentrations are associated with serious and/or life-threatening reactions [see Drug Interactions (7.1) and Clinical Pharmacology (12.3)].
- Alpha 1- Adrenoreceptor Antagonist: alfuzosin
- Antianginal: ranolazine
- Antiarrhythmic: dronedarone
- Anti-gout: colchicine
- Antipsychotics: lurasidone, pimozide
- Ergot Derivatives: dihydroergotamine, ergotamine, methylergonovine
- GI Motility Agent: cisapride
- Hepatitis C direct acting antiviral: elbasvir/grazoprevir
- HMG-CoA Reductase Inhibitors: lovastatin, simvastatin
- Microsomal triglyceride transfer protein (MTTP) Inhibitor: lomitapide
- PDE5 Inhibitor: sildenafil (Revatio®) when used for the treatment of pulmonary arterial hypertension
- Sedative/Hypnotics: triazolam, orally administered midazolam
- Lopinavir and ritonavir is contraindicated with drugs that are potent CYP3A inducers where significantly reduced lopinavir plasma concentrations may be associated with the potential for loss of virologic response and possible resistance and cross-resistance [see Drug Interactions (7.2) and Clinical Pharmacology (12.3)].
- Anticancer Agents: apalutamide
- Antimycobacterial: rifampin
- Herbal Products: St. John's Wort (hypericum perforatum)
-
-
5 WARNINGS AND PRECAUTIONS
5.1 Risk of Serious Adverse Reactions Due to Drug Interactions
Initiation of lopinavir and ritonavir, a CYP3A inhibitor, in patients receiving medications metabolized by CYP3A or initiation of medications metabolized by CYP3A in patients already receiving lopinavir and ritonavir, may increase plasma concentrations of medications metabolized by CYP3A. Initiation of medications that inhibit or induce CYP3A may increase or decrease concentrations of lopinavir and ritonavir, respectively. These interactions may lead to:
- Clinically significant adverse reactions, potentially leading to severe, life-threatening, or fatal events from greater exposures of concomitant medications.
- Clinically significant adverse reactions from greater exposures of lopinavir and ritonavir.
- Loss of therapeutic effect of lopinavir and ritonavir and possible development of resistance.
See Table 12 for steps to prevent or manage these possible and known significant drug interactions, including dosing recommendations [see Drug Interactions (7)]. Consider the potential for drug interactions prior to and during lopinavir and ritonavir therapy; review concomitant medications during lopinavir and ritonavir therapy, and monitor for the adverse reactions associated with the concomitant medications [see Contraindications (4) and Drug Interactions (7)].
5.2 Toxicity in Preterm Neonates
Lopinavir and ritonavir oral solution contains the excipients ethanol, approximately 42% (v/v) and propylene glycol, approximately 15% (w/v). When administered concomitantly with propylene glycol, ethanol competitively inhibits the metabolism of propylene glycol, which may lead to elevated concentrations. Preterm neonates may be at increased risk of propylene glycol-associated adverse events due to diminished ability to metabolize propylene glycol, thereby leading to accumulation and potential adverse events. Postmarketing life-threatening cases of cardiac toxicity (including complete AV block, bradycardia, and cardiomyopathy), lactic acidosis, acute renal failure, CNS depression and respiratory complications leading to death have been reported, predominantly in preterm neonates receiving lopinavir and ritonavir oral solution.
Lopinavir and ritonavir oral solution should not be used in preterm neonates in the immediate postnatal period because of possible toxicities. A safe and effective dose of lopinavir and ritonavir oral solution in this patient population has not been established. However, if the benefit of using lopinavir and ritonavir oral solution to treat HIV infection in infants immediately after birth outweighs the potential risks, infants should be monitored closely for increases in serum osmolality and serum creatinine, and for toxicity related to lopinavir and ritonavir oral solution including: hyperosmolality, with or without lactic acidosis, renal toxicity, CNS depression (including stupor, coma, and apnea), seizures, hypotonia, cardiac arrhythmias and ECG changes, and hemolysis. Total amounts of ethanol and propylene glycol from all medicines that are to be given to infants should be taken into account in order to avoid toxicity from these excipients [see Dosage and Administration (2.4) and Overdosage (10)].
5.3 Pancreatitis
Pancreatitis has been observed in patients receiving lopinavir and ritonavir therapy, including those who developed marked triglyceride elevations. In some cases, fatalities have been observed. Although a causal relationship to lopinavir and ritonavir has not been established, marked triglyceride elevations are a risk factor for development of pancreatitis [see Warnings and Precautions (5.9)]. Patients with advanced HIV-1 disease may be at increased risk of elevated triglycerides and pancreatitis, and patients with a history of pancreatitis may be at increased risk for recurrence during lopinavir and ritonavir therapy.
Pancreatitis should be considered if clinical symptoms (nausea, vomiting, abdominal pain) or abnormalities in laboratory values (such as increased serum lipase or amylase values) suggestive of pancreatitis occur. Patients who exhibit these signs or symptoms should be evaluated and lopinavir and ritonavir and/or other antiretroviral therapy should be suspended as clinically appropriate.
5.4 Hepatotoxicity
Patients with underlying hepatitis B or C or marked elevations in transaminase prior to treatment may be at increased risk for developing or worsening of transaminase elevations or hepatic decompensation with use of lopinavir and ritonavir.
There have been postmarketing reports of hepatic dysfunction, including some fatalities. These have generally occurred in patients with advanced HIV-1 disease taking multiple concomitant medications in the setting of underlying chronic hepatitis or cirrhosis. A causal relationship with lopinavir and ritonavir therapy has not been established.
Elevated transaminases with or without elevated bilirubin levels have been reported in HIV-1 mono-infected and uninfected patients as early as 7 days after the initiation of lopinavir and ritonavir in conjunction with other antiretroviral agents. In some cases, the hepatic dysfunction was serious; however, a definitive causal relationship with lopinavir and ritonavir therapy has not been established.
Appropriate laboratory testing should be conducted prior to initiating therapy with lopinavir and ritonavir and patients should be monitored closely during treatment. Increased AST/ALT monitoring should be considered in the patients with underlying chronic hepatitis or cirrhosis, especially during the first several months of lopinavir and ritonavir treatment [see Use in Specific Populations (8.6)].
5.5 QT Interval Prolongation
Postmarketing cases of QT interval prolongation and torsade de pointes have been reported although causality of lopinavir and ritonavir could not be established. Avoid use in patients with congenital long QT syndrome, those with hypokalemia, and with other drugs that prolong the QT interval [see Clinical Pharmacology (12.3)].
5.6 PR Interval Prolongation
Lopinavir and ritonavir prolongs the PR interval in some patients. Cases of second or third degree atrioventricular block have been reported. Lopinavir and ritonavir should be used with caution in patients with underlying structural heart disease, pre-existing conduction system abnormalities, ischemic heart disease or cardiomyopathies, as these patients may be at increased risk for developing cardiac conduction abnormalities.
The impact on the PR interval of co-administration of lopinavir and ritonavir with other drugs that prolong the PR interval (including calcium channel blockers, beta-adrenergic blockers, digoxin and atazanavir) has not been evaluated. As a result, co-administration of lopinavir and ritonavir with these drugs should be undertaken with caution, particularly with those drugs metabolized by CYP3A. Clinical monitoring is recommended [see Clinical Pharmacology (12.3)].
5.7 Diabetes Mellitus/Hyperglycemia
New onset diabetes mellitus, exacerbation of pre-existing diabetes mellitus, and hyperglycemia have been reported during post-marketing surveillance in HIV-1 infected patients receiving protease inhibitor therapy. Some patients required either initiation or dose adjustments of insulin or oral hypoglycemic agents for treatment of these events. In some cases, diabetic ketoacidosis has occurred. In those patients who discontinued protease inhibitor therapy, hyperglycemia persisted in some cases. Because these events have been reported voluntarily during clinical practice, estimates of frequency cannot be made and a causal relationship between protease inhibitor therapy and these events has not been established. Consider monitoring for hyperglycemia, new onset diabetes mellitus or an exacerbation of diabetes mellitus in patients treated with lopinavir and ritonavir.
5.8 Immune Reconstitution Syndrome
Immune reconstitution syndrome has been reported in patients treated with combination antiretroviral therapy, including lopinavir and ritonavir. During the initial phase of combination antiretroviral treatment, patients whose immune system responds may develop an inflammatory response to indolent or residual opportunistic infections (such as Mycobacterium avium infection, cytomegalovirus, Pneumocystis jirovecii pneumonia [PCP], or tuberculosis) which may necessitate further evaluation and treatment.
Autoimmune disorders (such as Graves’ disease, polymyositis, and Guillain-Barré syndrome) have also been reported to occur in the setting of immune reconstitution, however, the time to onset is more variable, and can occur many months after initiation of treatment.
5.9 Lipid Elevations
Treatment with lopinavir and ritonavir has resulted in large increases in the concentration of total cholesterol and triglycerides [see Adverse Reactions (6.1)]. Triglyceride and cholesterol testing should be performed prior to initiating lopinavir and ritonavir therapy and at periodic intervals during therapy. Lipid disorders should be managed as clinically appropriate, taking into account any potential drug-drug interactions with lopinavir and ritonavir and HMG-CoA reductase inhibitors [see Contraindications (4) and Drug Interactions (7.3)].
5.10 Fat Redistribution
Redistribution/accumulation of body fat including central obesity, dorsocervical fat enlargement (buffalo hump), peripheral wasting, facial wasting, breast enlargement, and "cushingoid appearance" have been observed in patients receiving antiretroviral therapy. The mechanism and long-term consequences of these events are currently unknown. A causal relationship has not been established.
5.11 Patients with Hemophilia
Increased bleeding, including spontaneous skin hematomas and hemarthrosis have been reported in patients with hemophilia type A and B treated with protease inhibitors. In some patients additional factor VIII was given. In more than half of the reported cases, treatment with protease inhibitors was continued or reintroduced. A causal relationship between protease inhibitor therapy and these events has not been established.
5.12 Resistance/Cross-resistance
Because the potential for HIV cross-resistance among protease inhibitors has not been fully explored in lopinavir and ritonavir-treated patients, it is unknown what effect therapy with lopinavir and ritonavir will have on the activity of subsequently administered protease inhibitors [see Microbiology (12.4)].
-
6 ADVERSE REACTIONS
The following adverse reactions are discussed in greater detail in other sections of the labeling.
- QT Interval Prolongation, PR Interval Prolongation [see Warnings and Precautions (5.5, 5.6)]
- Drug Interactions [see Warnings and Precautions (5.1)]
- Pancreatitis [see Warnings and Precautions (5.3)]
- Hepatotoxicity [see Warnings and Precautions (5.4)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reactions rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
Adverse Reactions in Adults
The safety of lopinavir and ritonavir has been investigated in about 2,600 patients in Phase II-IV clinical trials, of which about 700 have received a dose of 800/200 mg (6 capsules or 4 tablets) once daily. Along with nucleoside reverse transcriptase inhibitors (NRTIs), in some studies, lopinavir and ritonavir was used in combination with efavirenz or nevirapine.
In clinical studies the incidence of diarrhea in patients treated with either lopinavir and ritonavir capsules or tablets was greater in those patients treated once daily than in those patients treated twice daily. Any grade of diarrhea was reported by at least half of patients taking once daily lopinavir and ritonavir capsules or tablets. At the time of treatment discontinuation, 4.2-6.3% of patients taking once daily lopinavir and ritonavir and 1.8-3.7% of those taking twice daily lopinavir and ritonavir reported ongoing diarrhea.
Commonly reported adverse reactions to lopinavir and ritonavir included diarrhea, nausea, vomiting, hypertriglyceridemia and hypercholesterolemia. Diarrhea, nausea and vomiting may occur at the beginning of the treatment while hypertriglyceridemia and hypercholesterolemia may occur later. The following have been identified as adverse reactions of moderate or severe intensity (Table 8):
Table 8. Adverse Reactions of Moderate or Severe Intensity Occurring in at Least 0.1% of Adult Patients Receiving Lopinavir and Ritonavir in Combined Phase II/IV Studies (N=2,612) System Organ Class (SOC) and Adverse Reaction
n
%
BLOOD AND LYMPHATIC SYSTEM DISORDERS
anemia*
54
2.1
leukopenia and neutropenia*
44
1.7
lymphadenopathy*
35
1.3
CARDIAC DISORDERS
atherosclerosis such as myocardial infarction*
10
0.4
atrioventricular block*
3
0.1
tricuspid valve incompetence*
3
0.1
EAR AND LABYRINTH DISORDERS
vertigo*
7
0.3
tinnitus
6
0.2
ENDOCRINE DISORDERS
hypogonadism*
16
0.81
EYE DISORDERS
visual impairment*
8
0.3
GASTROINTESTINAL DISORDERS
diarrhea*
510
19.5
nausea
269
10.3
vomiting*
177
6.8
abdominal pain (upper and lower)*
160
6.1
gastroenteritis and colitis*
66
2.5
dyspepsia
53
2.0
pancreatitis*
45
1.7
Gastroesophageal Reflux Disease (GERD)*
40
1.5
hemorrhoids
39
1.5
flatulence
36
1.4
abdominal distension
34
1.3
constipation*
26
1.0
stomatitis and oral ulcers*
24
0.9
duodenitis and gastritis*
20
0.8
gastrointestinal hemorrhage including rectal hemorrhage*
13
0.5
dry mouth
9
0.3
gastrointestinal ulcer*
6
0.2
fecal incontinence
5
0.2
GENERAL DISORDERS AND ADMINISTRATION SITE CONDITIONS
fatigue including asthenia*
198
7.6
HEPATOBILIARY DISORDERS
hepatitis including AST, ALT, and GGT increases*
91
3.5
hepatomegaly
5
0.2
cholangitis
3
0.1
hepatic steatosis
3
0.1
IMMUNE SYSTEM DISORDERS
hypersensitivity including urticaria and angioedema*
70
2.7
immune reconstitution syndrome
3
0.1
INFECTIONS AND INFESTATIONS
upper respiratory tract infection*
363
13.9
lower respiratory tract infection*
202
7.7
skin infections including cellulitis, folliculitis, and furuncle*
86
3.3
METABOLISM AND NUTRITION DISORDERS
hypercholesterolemia*
192
7.4
hypertriglyceridemia*
161
6.2
weight decreased*
61
2.3
decreased appetite
52
2.0
blood glucose disorders including diabetes mellitus*
30
1.1
weight increased*
20
0.8
lactic acidosis*
11
0.4
increased appetite
5
0.2
MUSCULOSKELETAL AND CONNECTIVE TISSUE DISORDERS
musculoskeletal pain including arthralgia and back pain*
166
6.4
myalgia*
46
1.8
muscle disorders such as weakness and spasms*
34
1.3
rhabdomyolysis*
18
0.7
osteonecrosis
3
0.1
NERVOUS SYSTEM DISORDERS
headache including migraine*
165
6.3
insomnia*
99
3.8
neuropathy and peripheral neuropathy*
51
2.0
dizziness*
45
1.7
ageusia*
19
0.7
convulsion*
9
0.3
tremor*
9
0.3
cerebral vascular event*
6
0.2
PSYCHIATRIC DISORDERS
anxiety*
101
3.9
abnormal dreams*
19
0.7
libido decreased
19
0.7
RENAL AND URINARY DISORDERS
renal failure*
31
1.2
hematuria*
20
0.8
nephritis*
3
0.1
REPRODUCTIVE SYSTEM AND BREAST DISORDERS
erectile dysfunction*
34
1.71
menstrual disorders - amenorrhea, menorrhagia*
10
1.72
SKIN AND SUBCUTANEOUS TISSUE DISORDERS
rash including maculopapular rash*
99
3.8
lipodystrophy acquired including facial wasting*
58
2.2
dermatitis/rash including eczema and seborrheic dermatitis*
50
1.9
night sweats*
42
1.6
pruritus*
29
1.1
alopecia
10
0.4
capillaritis and vasculitis*
3
0.1
VASCULAR DISORDERS
hypertension*
47
1.8
deep vein thrombosis*
17
0.7
* Represents a medical concept including several similar MedDRA PTs 1. Percentage of male population (N=2,038)
2. Percentage of female population (N=574)
Laboratory Abnormalities in Adults
The percentages of adult patients treated with combination therapy with Grade 3-4 laboratory abnormalities are presented in Table 9 (treatment-naïve patients) and Table 10 (treatment-experienced patients).
Table 9. Grade 3-4 Laboratory Abnormalities Reported in ≥ 2% of Adult Antiretroviral-Naïve Patients Study 863
(48 Weeks)Study 720
(360 Weeks)Study 730
(48 Weeks)Variable
Limit1
Lopinavir and Ritonavir
400/100 mg
Twice Daily + d4T + 3TC
(N=326)Nelfinavir
750 mg Three Times Daily + d4T + 3TC
(N=327)Lopinavir and Ritonavir
Twice Daily + d4T + 3TC
(N=100)Lopinavir and Ritonavir
Once Daily + TDF + FTC
(N=333)Lopinavir and Ritonavir
Twice Daily + TDF + FTC
(N=331)Chemistry
High
Glucose
>250 mg/dL
2%
2%
4% 0%
<1%
Uric Acid
>12 mg/dL
2%
2%
5%
<1%
1%
SGOT/AST2
>180 U/L
2%
4%
10%
1%
2%
SGPT/ALT2
>215 U/L
4%
4%
11% 1%
1%
GGT
>300 U/L
N/A
N/A
10% N/A
N/A
Total
Cholesterol>300 mg/dL
9%
5%
27% 4%
3%
Triglycerides
>750 mg/dL
9%
1%
29% 3%
6%
Amylase
>2 x ULN
3%
2%
4% N/A
N/A
Lipase
>2 x ULN
N/A
N/A
N/A 3%
5%
Chemistry
Low
Calculated Creatinine Clearance
<50 mL/min
N/A
N/A
N/A 2%
2%
Hematology Low Neutrophils
<0.75 x 109/L
1%
3% 5% 2%
1% 1 ULN = upper limit of the normal range; N/A = Not Applicable. 2 Criterion for Study 730 was >5x ULN (AST/ALT).
Table 10. Grade 3-4 Laboratory Abnormalities Reported in ≥ 2% of Adult Protease Inhibitor-Experienced Patients Study 888
(48 Weeks)Study 9572 and Study 7653
(84-144 Weeks)Study 802
(48 Weeks)Variable
Limit1
Lopinavir and
Ritonavir
400/100 mg Twice Daily + NVP + NRTIs
(N=148)Investigator-Selected Protease Inhibitor(s) + NVP + NRTIs
(N=140)Lopinavir and
Ritonavir
Twice Daily + NNRTI + NRTIs
(N=127)Lopinavir and
Ritonavir
800/200 mg Once Daily
+ NRTIs
(N=300)Lopinavir and
Ritonavir
400/100 mg Twice Daily
+ NRTIs
(N=299)Chemistry
High
Glucose
>250 mg/dL
1%
2%
5%
2%
2%
Total Bilirubin
>3.48 mg/dL
1%
3%
1%
1%
1%
SGOT/AST4
>180 U/L
5%
11%
8%
3%
2%
SGPT/ALT4
>215 U/L
6%
13%
10%
2%
2%
GGT
>300 U/L
N/A
N/A
29%
N/A
N/A
Total
Cholesterol>300 mg/dL
20%
21%
39%
6%
7%
Triglycerides
>750 mg/dL
25%
21%
36%
5%
6%
Amylase
>2 x ULN
4%
8%
8%
4%
4%
Lipase
>2 x ULN
N/A
N/A
N/A
4%
1%
Creatine
Phosphokinase>4 x ULN
N/A
N/A
N/A
4%
5%
Chemistry
Low
Calculated
Creatinine
Clearance<50 mL/min
N/A
N/A
N/A
3%
3%
Inorganic
Phosphorus<1.5 mg/dL
1%
0%
2%
1%
<1%
Hematology
Low
Neutrophils
<0.75 x 109/L
1%
2%
4%
3%
4%
Hemoglobin
<80 g/L
1%
1%
1%
1%
2%
1 ULN = upper limit of the normal range; N/A = Not Applicable. 2 Includes clinical laboratory data from patients receiving 400/100 mg twice daily (n=29) or 533/133 mg twice daily (n=28) for 84 weeks. Patients received lopinavir and ritonavir in combination with NRTIs and efavirenz.
3 Includes clinical laboratory data from patients receiving 400/100 mg twice daily (n=36) or 400/200 mg twice daily (n=34) for 144 weeks. Patients received lopinavir and ritonavir in combination with NRTIs and nevirapine.
4 Criterion for Study 802 was >5x ULN (AST/ALT).
Adverse Reactions in Pediatric Patients
Lopinavir and ritonavir oral solution dosed up to 300/75 mg/m2 has been studied in 100 pediatric patients 6 months to 12 years of age. The adverse reaction profile seen during Study 940 was similar to that for adult patients.
Dysgeusia (22%), vomiting (21%), and diarrhea (12%) were the most common adverse reactions of any severity reported in pediatric patients treated with combination therapy for up to 48 weeks in Study 940. A total of 8 patients experienced adverse reactions of moderate to severe intensity. The adverse reactions meeting these criteria and reported for the 8 subjects include: hypersensitivity (characterized by fever, rash and jaundice), pyrexia, viral infection, constipation, hepatomegaly, pancreatitis, vomiting, alanine aminotransferase increased, dry skin, rash, and dysgeusia. Rash was the only event of those listed that occurred in 2 or more subjects (N=3).
Lopinavir and ritonavir oral solution dosed at 300/75 mg/m2 has been studied in 31 pediatric patients 14 days to 6 months of age. The adverse reaction profile in Study 1030 was similar to that observed in older children and adults. No adverse reaction was reported in greater than 10% of subjects. Adverse drug reactions of moderate to severe intensity occurring in 2 or more subjects included decreased neutrophil count (N=3), anemia (N=2), high potassium (N=2), and low sodium (N=2).
Lopinavir and ritonavir oral solution and soft gelatin capsules dosed at higher than recommended doses including 400/100 mg/m2 (without concomitant NNRTI) and 480/120 mg/m2 (with concomitant NNRTI) have been studied in 26 pediatric patients 7 to 18 years of age in Study 1038. Patients also had saquinavir mesylate added to their regimen at Week 4. Rash (12%), blood cholesterol abnormal (12%) and blood triglycerides abnormal (12%) were the only adverse reactions reported in greater than 10% of subjects. Adverse drug reactions of moderate to severe intensity occurring in 2 or more subjects included rash (N=3), blood triglycerides abnormal (N=3), and electrocardiogram QT prolonged (N=2). Both subjects with QT prolongation had additional predisposing conditions such as electrolyte abnormalities, concomitant medications, or pre-existing cardiac abnormalities.
Laboratory Abnormalities in Pediatric Patients
The percentages of pediatric patients treated with combination therapy including lopinavir and ritonavir with Grade 3-4 laboratory abnormalities are presented in Table 11.
Table 11. Grade 3-4 Laboratory Abnormalities Reported in ≥ 2% Pediatric Patients in Study 940 Variable
Limit1
Lopinavir and Ritonavir
Twice Daily + RTIs
(N=100)Chemistry
High
Sodium
>149 mEq/L
3%
Total Bilirubin
≥3.0 x ULN
3%
SGOT/AST
>180 U/L
8%
SGPT/ALT
>215 U/L
7%
Total Cholesterol
>300 mg/dL
3%
Amylase
>2.5 x ULN
7%2
Chemistry
Low
Sodium
<130 mEq/L
3%
Hematology
Low
Platelet Count
<50 x 109/L
4%
Neutrophils
<0.40 x 109/L
2%
1 ULN = upper limit of the normal range. 2 Subjects with Grade 3-4 amylase confirmed by elevations in pancreatic amylase.
6.2 Postmarketing Experience
The following adverse reactions have been reported during postmarketing use of lopinavir and ritonavir. Because these reactions are reported voluntarily from a population of unknown size, it is not possible to reliably estimate their frequency or establish a causal relationship to lopinavir and ritonavir exposure.
Body as a Whole
Redistribution/accumulation of body fat has been reported [see Warnings and Precautions (5.10)].
Cardiovascular
Bradyarrhythmias. First-degree AV block, second-degree AV block, third-degree AV block, QTc interval prolongation, torsades (torsade) de pointes [see Warnings and Precautions (5.5, 5.6)].
Renal and Urinary Disorders
Nephrolithiasis
Skin and Appendages
Toxic epidermal necrolysis (TEN), Stevens-Johnson syndrome and erythema multiforme.
-
7 DRUG INTERACTIONS
7.1 Potential for Lopinavir and Ritonavir to Affect Other Drugs
Lopinavir and ritonavir is an inhibitor of CYP3A and may increase plasma concentrations of agents that are primarily metabolized by CYP3A. Agents that are extensively metabolized by CYP3A and have high first pass metabolism appear to be the most susceptible to large increases in AUC (> 3-fold) when co-administered with lopinavir and ritonavir. Thus, co-administration of lopinavir and ritonavir with drugs highly dependent on CYP3A for clearance and for which elevated plasma concentrations are associated with serious and/or life-threatening events is contraindicated. Co-administration with other CYP3A substrates may require a dose adjustment or additional monitoring as shown in Table 12.
Additionally, lopinavir and ritonavir induces glucuronidation.
Published data suggest that lopinavir is an inhibitor of OATP1B1.
These examples are a guide and not considered a comprehensive list of all possible drugs that may interact with lopinavir and ritonavir. The healthcare provider should consult appropriate references for comprehensive information.
7.2 Potential for Other Drugs to Affect Lopinavir
Lopinavir and ritonavir is a CYP3A substrate; therefore, drugs that induce CYP3A may decrease lopinavir plasma concentrations and reduce lopinavir and ritonavir’s therapeutic effect. Although not observed in the lopinavir and ritonavir/ketoconazole drug interaction study, co-administration of lopinavir and ritonavir and other drugs that inhibit CYP3A may increase lopinavir plasma concentrations.
7.3 Established and Other Potentially Significant Drug Interactions
Table 12 provides a listing of established or potentially clinically significant drug interactions. Alteration in dose or regimen may be recommended based on drug interaction studies or predicted interaction [see Contraindications (4), Warnings and Precautions (5.1), Clinical Pharmacology (12.3)] for magnitude of interaction.
Table 12. Established and Other Potentially Significant Drug Interactions Concomitant Drug Class:
Drug Name
Effect on Concentration of Lopinavir or Concomitant Drug
Clinical Comments
HIV-1 Antiviral Agents
HIV-1 Protease Inhibitor:
fosamprenavir/ritonavir
↓amprenavir
↓lopinavir
An increased rate of adverse reactions has been observed with co-administration of these medications. Appropriate doses of the combinations with respect to safety and efficacy have not been established.
HIV-1 Protease Inhibitor:
indinavir*
↑ indinavir
Decrease indinavir dose to 600 mg twice daily, when co-administered with lopinavir and ritonavir 400/100 mg twice daily. Lopinavir and ritonavir once daily has not been studied in combination with indinavir.
HIV-1 Protease Inhibitor:
nelfinavir*
↑ nelfinavir
↑ M8 metabolite of nelfinavir
↓ lopinavir
Lopinavir and ritonavir once daily in combination with nelfinavir is not recommended [see Dosage and Administration (2)].
HIV-1 Protease Inhibitor:
ritonavir*
↑ lopinavir
Appropriate doses of additional ritonavir in combination with lopinavir and ritonavir with respect to safety and efficacy have not been established.
HIV-1 Protease Inhibitor:
saquinavir
↑ saquinavir
The saquinavir dose is 1000 mg twice daily, when co-administered with lopinavir and ritonavir 400/100 mg twice daily. Lopinavir and ritonavir once daily has not been studied in combination with saquinavir.
HIV-1 Protease Inhibitor:
tipranavir*
↓ lopinavir
Co-administration with tipranavir (500 mg twice daily) and ritonavir (200 mg twice daily) is not recommended.
HIV CCR5 – Antagonist:
maraviroc*
↑ maraviroc
When co-administered, patients should receive 150 mg twice daily of maraviroc. For further details see complete prescribing information for maraviroc.
Non-nucleoside Reverse Transcriptase Inhibitors:
efavirenz*,
nevirapine*
↓ lopinavir
Increase the dose of lopinavir and ritonavir tablets to 500/125 mg when lopinavir and ritonavir tablet is co-administered with efavirenz or nevirapine. Lopinavir and ritonavir once daily in combination with efavirenz or nevirapine is not recommended [see Dosage and Administration (2)].
Non-nucleoside Reverse Transcriptase Inhibitor:
delavirdine
↑ lopinavir
Appropriate doses of the combination with respect to safety and efficacy have not been established.
Nucleoside Reverse Transcriptase Inhibitor:
didanosine
For lopinavir and ritonavir oral solution, it is recommended that didanosine be administered on an empty stomach; therefore, didanosine should be given one hour before or two hours after lopinavir and ritonavir oral solution (given with food).
Nucleoside Reverse Transcriptase Inhibitor:
tenofovir disoproxil fumarate*
↑ tenofovir
Patients receiving lopinavir and ritonavir and tenofovir should be monitored for adverse reactions associated with tenofovir.
Nucleoside Reverse Transcriptase Inhibitors:
abacavir
zidovudine
↓ abacavir
↓ zidovudine
The clinical significance of this potential interaction is unknown.
Other Agents
Alpha 1- Adrenoreceptor Antagonist:
alfuzosin↑ alfuzosin Contraindicated due to potential hypotension [see Contraindications (4)]. Antianginal:
ranolazine↑ ranolazine Contraindicated due to potential for serious and/or life-threatening reactions [see Contraindications (4)]. Antiarrhythmics: dronedarone
↑ dronedarone Contraindicated due to potential for cardiac arrhythmias [see Contraindications (4)]. Antiarrhythmics e.g. amiodarone,
bepridil,
lidocaine (systemic),
quinidine↑ antiarrhythmics Caution is warranted and therapeutic concentration monitoring (if available) is recommended for antiarrhythmics when co-administered with lopinavir and ritonavir. Anticancer Agents:
abemaciclib,
apalutamide,
encorafenib,
ibrutinib,
ivosidenib,
dasatinib,
neratinib,
nilotinib,
venetoclax,
vinblastine,
vincristine
↑ anticancer agents
↓ lopinavir/ritonavir#
Apalutamide is contraindicated due to potential for loss of virologic response and possible resistance to lopinavir and ritonavir or to the class of protease inhibitors [see Contraindications (4)].
Avoid co-administration of encorafenib or ivosidenib with lopinavir and ritonavir due to potential risk of serious adverse events such as QT interval prolongation. If co-administration of encorafenib with lopinavir and ritonavir cannot be avoided, modify dose as recommended in encorafenib USPI. If co-administration of ivosidenib with lopinavir and ritonavir cannot be avoided, reduce ivosidenib dose to 250 mg once daily.
Avoid use of neratinib, venetoclax or ibrutinib with lopinavir and ritonavir.
For vincristine and vinblastine, consideration should be given to temporarily withholding the ritonavir-containing antiretroviral regimen in patients who develop significant hematologic or gastrointestinal side effects when lopinavir and ritonavir is administered concurrently with vincristine or vinblastine. If the antiretroviral regimen must be withheld for a prolonged period, consideration should be given to initiating a revised regimen that does not include a CYP3A or P-gp inhibitor.
A decrease in the dosage or an adjustment of the dosing interval of nilotinib and dasatinib may be necessary for patients requiring co-administration with strong CYP3A inhibitors such as lopinavir and ritonavir. Please refer to the nilotinib and dasatinib prescribing information for dosing instructions.
Anticoagulants:
warfarin,
rivaroxaban
↑↓ warfarin
↑ rivaroxaban
Concentrations of warfarin may be affected. Initial frequent monitoring of the INR during lopinavir and ritonavir and warfarin co-administration is recommended.
Avoid concomitant use of rivaroxaban and lopinavir and ritonavir. Co-administration of lopinavir and ritonavir and rivaroxaban may lead to risk of increased bleeding.
Anticonvulsants:
carbamazepine,
phenobarbital,
phenytoin
↓ lopinavir
↓ phenytoin
Lopinavir and ritonavir may be less effective due to decreased lopinavir plasma concentrations in patients taking these agents concomitantly and should be used with caution.
Lopinavir and ritonavir once daily in combination with carbamazepine, phenobarbital, or phenytoin is not recommended.
In addition, co-administration of phenytoin and lopinavir and ritonavir may cause decreases in steady-state phenytoin concentrations. Phenytoin levels should be monitored when co-administering with lopinavir and ritonavir.
Anticonvulsants:
lamotrigine,
valproate
↓ lamotrigine
↓ or ↔ valproate
A dose increase of lamotrigine or valproate may be needed when co-administered with lopinavir and ritonavir and therapeutic concentration monitoring for lamotrigine may be indicated; particularly during dosage adjustments.
Antidepressant:
bupropion
↓ bupropion
↓ active metabolite,
hydroxybupropion
Patients receiving lopinavir and ritonavir and bupropion concurrently should be monitored for an adequate clinical response to bupropion.
Antidepressant:
trazodone
↑ trazodone
Adverse reactions of nausea, dizziness, hypotension and syncope have been observed following co-administration of trazodone and ritonavir. A lower dose of trazodone should be considered.
Anti-infective:
clarithromycin
↑ clarithromycin
For patients with renal impairment, adjust clarithromycin dose as follows:
• For patients on lopinavir and ritonavir with CLCR 30 to 60 mL/min the dose of clarithromycin should be reduced by 50%.
• For patients on lopinavir and ritonavir with CLCR < 30 mL/min the dose of clarithromycin should be decreased by 75%.
No dose adjustment for patients with normal renal function is necessary.
Antifungals:
ketoconazole*,
itraconazole,
voriconazole
isavuconazonium sulfate*
↑ ketoconazole
↑ itraconazole
↓ voriconazole
↑ isavuconazonium
High doses of ketoconazole (>200 mg/day) or itraconazole (> 200 mg/day) are not recommended.
The co-administration of voriconazole and lopinavir and ritonavir should be avoided unless an assessment of the benefit/risk to the patient justifies the use of voriconazole.
Isavuconazonium and lopinavir and ritonavir should be co-administered with caution. Alternative antifungal therapies should be considered in these patients.
Anti-gout:
colchicine
↑ colchicine
Contraindicated due to potential for serious and/or life-threatening reactions in patients with renal and/or hepatic impairment [see Contraindications (4)].
For patients with normal renal or hepatic function:
Treatment of gout flares-co-administration of colchicine in patients on lopinavir and ritonavir:
0.6 mg (1 tablet) x 1 dose, followed by 0.3 mg (half tablet) 1 hour later. Dose to be repeated no earlier than 3 days.
Prophylaxis of gout flares-co-administration of colchicine in patients on lopinavir and ritonavir:
If the original colchicine regimen was 0.6 mg twice a day, the regimen should be adjusted to 0.3 mg once a day.
If the original colchicine regimen was 0.6 mg once a day, the regimen should be adjusted to 0.3 mg once every other day.
Treatment of familial Mediterranean fever (FMF)-co-administration of colchicine in patients on lopinavir and ritonavir:
Maximum daily dose of 0.6 mg (may be given as 0.3 mg twice a day).
Antimycobacterial: rifampin ↓ lopinavir Contraindicated due to potential loss of virologic response and possible resistance to lopinavir and ritonavir or to the class of protease inhibitors or other co-administered antiretroviral agents [see Contraindications (4)]. Antimycobacterial: bedaquiline
↑ bedaquiline
Bedaquiline should only be used with lopinavir and ritonavir if the benefit of co-administration outweighs the risk. Antimycobacterial:
rifabutin*
↑ rifabutin and rifabutin metabolite
Dosage reduction of rifabutin by at least 75% of the usual dose of 300 mg/day is recommended (i.e., a maximum dose of 150 mg every other day or three times per week). Increased monitoring for adverse reactions is warranted in patients receiving the combination. Further dosage reduction of rifabutin may be necessary.
Antiparasitic:
atovaquone
↓ atovaquone
Clinical significance is unknown; however, increase in atovaquone doses may be needed.
Antipsychotics:
lurasidone
pimozide↑ lurasidone
↑ pimozideContraindicated due to potential for serious and/or life-threatening reactions [see Contraindications (4)].
Contraindicated due to potential for serious and/or life-threatening reactions such as cardiac arrhythmias [see Contraindications (4)].
Antipsychotics: quetiapine
↑ quetiapine Initiation of lopinavir and ritonavir in patients taking quetiapine: Consider alternative antiretroviral therapy to avoid increases in quetiapine exposures. If coadministration is necessary, reduce the quetiapine dose to 1/6 of the current dose and monitor for quetiapine-associated adverse reactions. Refer to the quetiapine prescribing information for recommendations on adverse reaction monitoring.
Initiation of quetiapine in patients taking lopinavir and ritonavir:
Refer to the quetiapine prescribing information for initial dosing and titration of quetiapine.
Contraceptive:
ethinyl estradiol*
↓ ethinyl estradiol Because contraceptive steroid concentrations may be altered when lopinavir and ritonavir is co-administered with oral contraceptives or with the contraceptive patch, alternative methods of nonhormonal contraception are recommended. Dihydropyridine Calcium Channel Blockers: e.g. felodipine,
nifedipine,
nicardipine
↑ dihydropyridine calcium channel blockers
Clinical monitoring of patients is recommended and a dose reduction of the dihydropyridine calcium channel blocker may be considered. Disulfiram/metronidazole Lopinavir and ritonavir oral solution contains ethanol, which can produce disulfiram-like reactions when co-administered with disulfiram or other drugs that produce this reaction (e.g., metronidazole). Endothelin Receptor Antagonists:
bosentan
↑ bosentan
Co-administration of bosentan in patients on lopinavir and ritonavir:
In patients who have been receiving lopinavir and ritonavir for at least 10 days, start bosentan at 62.5 mg once daily or every other day based upon individual tolerability.
Co-administration of lopinavir and ritonavir in patients on bosentan:
Discontinue use of bosentan at least 36 hours prior to initiation of lopinavir and ritonavir.
After at least 10 days following the initiation of lopinavir and ritonavir, resume bosentan at 62.5 mg once daily or every other day based upon individual tolerability.
Ergot Derivatives: dihydroergotamine, ergotamine, methylergonovine
↑ ergot derivatives Contraindicated due to potential for acute ergot toxicity characterized by peripheral vasospasm and ischemia of the extremities and other tissues [see Contraindications (4)].
GI Motility Agent: cisapride ↑ cisapride Contraindicated due to potential for cardiac arrhythmias [see Contraindications (4)]. GnRH Receptor Antagonists: elagolix ↑ elagolix
↓ lopinavir/ritonavirConcomitant use of elagolix 200 mg twice daily and lopinavir and ritonavir for more than 1 month is not recommended due to potential risk of adverse events such as bone loss and hepatic transaminase elevations. Limit concomitant use of elagolix 150 mg once daily and lopinavir and ritonavir to 6 months. Hepatitis C direct acting antiviral: elbasvir/grazoprevir
↑
elbasvir/grazoprevir
Contraindicated due to increased risk of alanine transaminase (ALT) elevations [see Contraindications (4)].
Hepatitis C direct acting antivirals:
boceprevir*
glecaprevir/pibrentasvir
simeprevir
sofosbuvir/velpatasvir/ voxilaprevir
ombitasvir/paritaprevir/
ritonavir and dasabuvir*
↓ lopinavir
↓ boceprevir
↓ ritonavir
↑ glecaprevir
↑ pibrentasvir
↑ simeprevir
↑ sofosbuvir
↑ velpatasvir
↑ voxilaprevir
↑ ombitasvir
↑ paritaprevir
↑ ritonavir
↔ dasabuvir
It is not recommended to co-administer lopinavir and ritonavir and boceprevir, glecaprevir/pibrentasvir, simeprevir, sofosbuvir/velpatasvir/voxilaprevir, or ombitasvir/paritaprevir/ritonavir and dasabuvir.
Herbal Products:
St. John's Wort (hypericum perforatum)↓ lopinavir Contraindicated due to potential for loss of virologic response and possible resistance to lopinavir and ritonavir or to the class of protease inhibitors [see Contraindications (4)]. Lipid-modifying agents
HMG-CoA Reductase Inhibitors:
lovastatin
simvastatin
atorvastatin
rosuvastatin
Microsomal triglyceride transfer protein (MTTP) Inhibitor: lomitapide↑ lovastatin
↑ simvastatin
↑ atorvastatin
↑ rosuvastatin
↑ lomitapideContraindicated due to potential for myopathy including rhabdomyolysis [see Contraindications (4)].
Use atorvastatin with caution and at the lowest necessary dose. Titrate rosuvastatin dose carefully and use the lowest necessary dose; do not exceed rosuvastatin 10 mg/day.
Lomitapide is a sensitive substrate for CYP3A4 metabolism. CYP3A4 inhibitors increase the exposure of lomitapide, with strong inhibitors increasing exposure approximately 27-fold.
Concomitant use of moderate or strong CYP3A4 inhibitors with lomitapide is contraindicated due to potential for hepatotoxicity [see Contraindications (4)].
Immunosuppressants: e.g.
cyclosporine,
tacrolimus,
sirolimus↑
immunosuppressants
Therapeutic concentration monitoring is recommended for immunosuppressant agents when co-administered with lopinavir and ritonavir. Kinase Inhibitors:
fostamatinib (also see anticancer agents above)↑ fostamatinib
metabolite R406Monitor for toxicities of R406 such as hepatotoxicity and neutropenia. Fostamatinib dose reduction may be required. Long-acting beta-adrenoceptor Agonist:
salmeterol
↑ salmeterol
Concurrent administration of salmeterol and lopinavir and ritonavir is not recommended. The combination may result in increased risk of cardiovascular adverse events associated with salmeterol, including QT prolongation, palpitations and sinus tachycardia.
Narcotic Analgesics:
methadone,*fentanyl
↓ methadone
↑ fentanyl
Dosage of methadone may need to be increased when co-administered with lopinavir and ritonavir.
Careful monitoring of therapeutic and adverse effects (including potentially fatal respiratory depression) is recommended when fentanyl is concomitantly administered with lopinavir and ritonavir.
PDE5 inhibitors:
avanafil,
sildenafil,
tadalafil,
vardenafil
↑ avanafil
↑ sildenafil
↑ tadalafil
↑ vardenafil
Sildenafil when used for the treatment of pulmonary arterial hypertension (Revatio®) is contraindicated due to the potential for sildenafil-associated adverse events, including visual abnormalities, hypotension, prolonged erection, and syncope [see Contraindications (4)].
Do not use lopinavir and ritonavir with avanafil because a safe and effective avanafil dosage regimen has not been established.
Particular caution should be used when prescribing sildenafil, tadalafil, or vardenafil in patients receiving lopinavir and ritonavir. Co-administration of lopinavir and ritonavir with these drugs may result in an increase in PDE5 inhibitor associated adverse reactions including hypotension, syncope, visual changes and prolonged erection.
Use of PDE5 inhibitors for pulmonary arterial hypertension (PAH):
Sildenafil (Revatio®) is contraindicated [see Contraindications (4)].
The following dose adjustments are recommended for use of tadalafil (Adcirca®) with lopinavir and ritonavir:
Co-administration of ADCIRCA in patients on lopinavir and ritonavir:
In patients receiving lopinavir and ritonavir for at least one week, start ADCIRCA at 20 mg once daily. Increase to 40 mg once daily based upon individual tolerability.
Co-administration of lopinavir and ritonavir in patients on ADCIRCA:
Avoid use of ADCIRCA during the initiation of lopinavir and ritonavir. Stop ADCIRCA at least 24 hours prior to starting lopinavir and ritonavir. After at least one week following the initiation of lopinavir and ritonavir, resume ADCIRCA at 20 mg once daily. Increase to 40 mg once daily based upon individual tolerability.
Use of PDE5 inhibitors for erectile dysfunction:
It is recommended not to exceed the following doses:
• Sildenafil: 25 mg every 48 hours
• Tadalafil: 10 mg every 72 hours
• Vardenafil: 2.5 mg every 72 hours
Use with increased monitoring for adverse events.
Sedative/Hypnotics: triazolam, orally administered midazolam ↑ triazolam
↑ midazolamContraindicated due to potential for prolonged or increased sedation or respiratory depression [see Contraindications (4)]. Sedative/Hypnotics: parenterally administered midazolam ↑ midazolam If lopinavir and ritonavir is co-administered with parenteral midazolam, close clinical monitoring for respiratory depression and/or prolonged sedation should be exercised and dosage adjustment should be considered. Systemic/Inhaled/ Nasal/Ophthalmic
Corticosteroids: e.g.,
betamethasone
budesonide
ciclesonide dexamethasone fluticasone methylprednisolone mometasone
prednisone
triamcinolone↓ lopinavir
↑ glucocorticoidsCo-administration with oral dexamethasone or other systemic corticosteroids that induce CYP3A may result in loss of therapeutic effect and development of resistance to lopinavir. Consider alternative corticosteroids. Co-administration with corticosteroids whose exposures are significantly increased by strong CYP3A inhibitors can increase the risk for Cushing’s syndrome and adrenal suppression.
Alternative corticosteroids including beclomethasone and prednisolone (whose PK and/or PD are less affected by strong CYP3A inhibitors relative to other studied steroids) should be considered, particularly for long-term use.* see Clinical Pharmacology (12.3) for magnitude of interaction.
# refers to interaction with apalutamide.
7.4 Drugs with No Observed or Predicted Interactions with Lopinavir and Ritonavir
Drug interaction or clinical studies reveal no clinically significant interaction between lopinavir and ritonavir and desipramine (CYP2D6 probe), etravirine, pitavastatin, pravastatin, stavudine, lamivudine, omeprazole, raltegravir, ranitidine, or rilpivirine.
Based on known metabolic profiles, clinically significant drug interactions are not expected between lopinavir and ritonavir and dapsone, trimethoprim/sulfamethoxazole, azithromycin, erythromycin, or fluconazole.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to lopinavir and ritonavir during pregnancy. Physicians are encouraged to register patients by calling the Antiretroviral Pregnancy Registry at 1-800-258-4263.
Risk Summary
Available data from the Antiretroviral Pregnancy Registry show no difference in the risk of overall major birth defects compared to the background rate for major birth defects of 2.7% in the U.S. reference population of the Metropolitan Atlanta Congenital Defects Program (MACDP) (see Data). The estimated background rate of miscarriage in clinically recognized pregnancies in the U.S. general population is 15-20%. The background risk for major birth defects and miscarriage for the indicated population is unknown. Methodological limitations of the APR include the use of MACDP as the external comparator group. The MACDP population is not disease-specific, evaluates women and infants from a limited geographic area, and does not include outcomes for births that occurred at <20 weeks gestation (see Data). No treatment-related malformations were observed when lopinavir in combination with ritonavir was administered to pregnant rats or rabbits; however embryonic and fetal developmental toxicities occurred in rats administered maternally toxic doses.
Clinical Considerations
Dose Adjustments During Pregnancy and the Postpartum Period
Administer 400/100 mg of lopinavir and ritonavir twice daily in pregnant patients with no documented lopinavir-associated resistance substitutions [see Dosage and Administration (2.5) and Clinical Pharmacology (12.3)]. There are insufficient data to recommend lopinavir and ritonavir dosing for pregnant patients with any documented lopinavir-associated resistance substitutions. No dose adjustment of lopinavir and ritonavir is required for patients during the postpartum period.
Once daily lopinavir and ritonavir dosing is not recommended in pregnancy.
Avoid use of lopinavir and ritonavir oral solution during pregnancy due to the ethanol content. Lopinavir and ritonavir oral solution contains the excipients ethanol, approximately 42% (v/v) and propylene glycol, approximately 15% (w/v).
Data
Human Data
Lopinavir and ritonavir was evaluated in 12 HIV-infected pregnant women in an open-label pharmacokinetic trial [see Clinical Pharmacology (12.3)]. No new trends in the safety profile were identified in pregnant women dosed with lopinavir and ritonavir compared to the safety described in non-pregnant adults, based on the review of these limited data.
Antiretroviral Pregnancy Registry Data: Based on prospective reports from the Antiretroviral Pregnancy Registry (APR) of over 3,000 exposures to lopinavir containing regimens (including over 1,000 exposed in the first trimester), there was no difference between lopinavir and overall birth defects compared with the background birth defect rate of 2.7% in the U.S. reference population of the Metropolitan Atlanta Congenital Defects Program. The prevalence of birth defects in live births was 2.1% (95% CI: 1.4%-3.0%) following first-trimester exposure to lopinavir-containing regimens and 3.0% (95% CI: 2.4%-3.8%) following second and third trimester exposure to lopinavir-containing regimens. Based on prospective reports from the APR of over 5,000 exposures to ritonavir containing regimens (including over 2,000 exposures in the first trimester) there was no difference between ritonavir and overall birth defects compared with the U.S. background rate (MACDP). The prevalence of birth defects in live births was 2.2% (95% CI: 1.7%-2.8%) following first-trimester exposure to ritonavir-containing regimens and 2.9% (95% CI: 2.4%-3.6%) following second and third trimester exposure to ritonavir-containing regimens. For both lopinavir and ritonavir, sufficient numbers of first trimester exposures have been monitored to detect at least a 1.5 fold increase in risk of overall birth defects and a 2 fold increase in risk of birth defects in the cardiovascular and genitourinary systems.
Animal Data
Embryonic and fetal developmental toxicities (early resorption, decreased fetal viability, decreased fetal body weight, increased incidence of skeletal variations and skeletal ossification delays) occurred in rats administered lopinavir in combination with ritonavir (on gestation days 6-17) at a maternally toxic dosage. Based on AUC measurements, the drug exposures in rats at the toxic doses were approximately 0.7 times (for lopinavir) and 1.8 times (for ritonavir) the exposures in humans at the recommended therapeutic dose (400/100 mg twice daily). In a pre- and post-natal study in rats, a developmental toxicity (a decrease in survival in pups between birth and postnatal Day 21) occurred.
No embryonic and fetal developmental toxicities were observed in rabbits administered lopinavir in combination with ritonavir (on gestation days 6-18) at a maternally toxic dosage. Based on AUC measurements, the drug exposures in rabbits at the toxic doses were approximately 0.6 times (for lopinavir) and similar to (for ritonavir) the exposures in humans at the recommended therapeutic dose (400/100 mg twice daily).
8.2 Lactation
Risk Summary
The Centers for Disease Control and Prevention recommend that HIV-1 infected mothers not breastfeed their infants to avoid risking postnatal transmission of HIV-1. Because of the potential for: 1) HIV transmission (in HIV-negative infants), 2) developing viral resistance (in HIV-positive infants), and 3) adverse reactions in the breastfed infant, instruct mothers not to breastfeed if they are receiving lopinavir and ritonavir.
8.3 Females and Males of Reproductive Potential
Contraception
Use of lopinavir and ritonavir may reduce the efficacy of combined hormonal contraceptives. Advise patients using combined hormonal contraceptives to use an effective alternative contraceptive method or an additional barrier method of contraception [see Drug Interactions (7.3)].
8.4 Pediatric Use
The safety, efficacy, and pharmacokinetic profiles of lopinavir and ritonavir in pediatric patients below the age of 14 days have not been established. Lopinavir and ritonavir should not be administered once daily in pediatric patients.
An open-label, multi-center, dose-finding trial was performed to evaluate the pharmacokinetic profile, tolerability, safety and efficacy of lopinavir and ritonavir oral solution containing lopinavir 80 mg/mL and ritonavir 20 mg/mL at a dose of 300/75 mg/m2 twice daily plus two NRTIs in HIV-infected infants ≥14 days and < 6 months of age. Results revealed that infants younger than 6 months of age generally had lower lopinavir AUC12 than older children (6 months to 12 years of age), however, despite the lower lopinavir drug exposure observed, antiviral activity was demonstrated as reflected in the proportion of subjects who achieved HIV-1 RNA <400 copies/mL at Week 24 [see Adverse Reactions (6.2), Clinical Pharmacology (12.3), Clinical Studies (14.4)].
Safety and efficacy in pediatric patients > 6 months of age was demonstrated in a clinical trial in 100 patients. The clinical trial was an open-label, multicenter trial evaluating the pharmacokinetic profile, tolerability, safety, and efficacy of lopinavir and ritonavir oral solution containing lopinavir 80 mg/mL and ritonavir 20 mg/mL in 100 antiretroviral naïve and experienced pediatric patients ages 6 months to 12 years. Dose selection for patients 6 months to 12 years of age was based on the following results. The 230/57.5 mg/m2 oral solution twice daily regimen without nevirapine and the 300/75 mg/m2 oral solution twice daily regimen with nevirapine provided lopinavir plasma concentrations similar to those obtained in adult patients receiving the 400/100 mg twice daily regimen (without nevirapine) [see Adverse Reactions (6.2), Clinical Pharmacology (12.3), Clinical Studies (14.4)].
A prospective multicenter, open-label trial evaluated the pharmacokinetic profile, tolerability, safety and efficacy of high-dose lopinavir and ritonavir with or without concurrent NNRTI therapy (Group 1: 400/100 mg/m2 twice daily + ≥ 2 NRTIs; Group 2: 480/120 mg/m2 twice daily + ≥ 1 NRTI + 1 NNRTI) in 26 children and adolescents ≥ 2 years to < 18 years of age who had failed prior therapy. Patients also had saquinavir mesylate added to their regimen. This strategy was intended to assess whether higher than approved doses of lopinavir and ritonavir could overcome protease inhibitor cross-resistance. High doses of lopinavir and ritonavir exhibited a safety profile similar to those observed in previous trials; changes in HIV-1 RNA were less than anticipated; three patients had HIV-1 RNA <400 copies/mL at Week 48. CD4+ cell count increases were noted in the eight patients who remained on treatment for 48 weeks [see Adverse Reactions (6.2), Clinical Pharmacology (12.3)].
8.5 Geriatric Use
Clinical studies of lopinavir and ritonavir did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. In general, appropriate caution should be exercised in the administration and monitoring of lopinavir and ritonavir in elderly patients reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
8.6 Hepatic Impairment
Lopinavir and ritonavir is principally metabolized by the liver; therefore, caution should be exercised when administering this drug to patients with hepatic impairment, because lopinavir concentrations may be increased [see Warnings and Precautions (5.4) and Clinical Pharmacology (12.3)].
-
10 OVERDOSAGE
Overdoses with lopinavir and ritonavir oral solution have been reported. One of these reports described fatal cardiogenic shock in a 2.1 kg infant who received a single dose of 6.5 mL of lopinavir and ritonavir oral solution (520 mg lopinavir, approximately 10-fold above the recommended lopinavir dose) nine days prior. The following events have been reported in association with unintended overdoses in preterm neonates: complete AV block, cardiomyopathy, lactic acidosis, and acute renal failure [see Warnings and Precautions (5.2)]. Healthcare professionals should be aware that lopinavir and ritonavir oral solution is highly concentrated and therefore, should pay special attention to accurate calculation of the dose of lopinavir and ritonavir, transcription of the medication order, dispensing information and dosing instructions to minimize the risk for medication errors and overdose. This is especially important for infants and young children.
Lopinavir and ritonavir oral solution contains approximately 42% (v/v) ethanol and approximately 15% (w/v) propylene glycol. Ingestion of the product over the recommended dose by an infant or a young child could result in significant toxicity and could potentially be lethal.
Human experience of acute overdosage with lopinavir and ritonavir is limited. Treatment of overdose with lopinavir and ritonavir should consist of general supportive measures including monitoring of vital signs and observation of the clinical status of the patient. There is no specific antidote for overdose with lopinavir and ritonavir. If indicated, elimination of unabsorbed drug should be achieved by gastric lavage. Administration of activated charcoal may also be used to aid in removal of unabsorbed drug. Since lopinavir is highly protein bound, dialysis is unlikely to be beneficial in significant removal of the drug. However, dialysis can remove both ethanol and propylene glycol in the case of overdose with lopinavir and ritonavir oral solution.
-
11 DESCRIPTION
Lopinavir and Ritonavir Oral Solution USP is a co-formulation of lopinavir and ritonavir. Lopinavir is an inhibitor of the HIV-1 protease. As co-formulated in lopinavir and ritonavir, ritonavir inhibits the CYP3A-mediated metabolism of lopinavir, thereby providing increased plasma levels of lopinavir.
Lopinavir is chemically designated as [1S-[1R*,(R*), 3R*, 4R*]]-N-[4-[[(2,6-dimethylphenoxy)acetyl]amino]-3-hydroxy-5-phenyl-1-(phenylmethyl)pentyl]tetrahydro-alpha-(1-methylethyl)-2-oxo-1(2H)-pyrimidineacetamide. Its molecular formula is C37H48N4O5, and its molecular weight is 628.80. Lopinavir is a white to light tan powder. It is freely soluble in methanol and ethanol, soluble in isopropanol and practically insoluble in water. Lopinavir has the following structural formula:
Ritonavir is chemically designated as 10-hydroxy-2-methyl-5-(1-methylethyl)-1-[2-(1-methylethyl)-4-thiazolyl]-3,6-dioxo-8,11-bis(phenylmethyl)-2,4,7,12-tetraazatridecan-13-oic acid, 5-thiazolylmethyl ester, [5S-(5R*,8R*,10R*,11R*)]. Its molecular formula is C37H48N6O5S2, and its molecular weight is 720.95. Ritonavir is a white to light tan powder. It is freely soluble in methanol and ethanol, soluble in isopropanol and practically insoluble in water. Ritonavir has the following structural formula:
Lopinavir and ritonavir oral solution is available for oral administration as 80 mg lopinavir and 20 mg ritonavir per milliliter with the following inactive ingredients: bubble gum flavor, ethanol, glycerin, high fructose corn syrup, malic acid, polyoxyl 40 hydrogenated castor oil, povidone, propylene glycol, sodium hydroxide, sucralose, and water.
Lopinavir and ritonavir oral solution contains approximately 42% (v/v) ethanol and approximately 15% (w/v) propylene glycol.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Lopinavir and ritonavir is a fixed-dose combination of HIV-1 antiviral drugs lopinavir [see Microbiology (12.4)] and ritonavir. As co-formulated in lopinavir and ritonavir, ritonavir inhibits the CYP3A-mediated metabolism of lopinavir, thereby providing increased plasma levels of lopinavir.
12.2 Pharmacodynamics
Cardiac Electrophysiology
The effect of lopinavir and ritonavir on QTcF interval was evaluated in a placebo and active (moxifloxacin 400 mg once daily) controlled crossover study in 39 healthy adults. The maximum mean time-matched (95% upper confidence bound) differences in QTcF interval from placebo after baseline-correction were 5.3 (8.1) and 15.2 (18.0) mseconds (msec) for 400/100 mg twice daily and supratherapeutic 800/200 mg twice daily lopinavir and ritonavir, respectively. Lopinavir and ritonavir 800/200 mg twice daily resulted in a Day 3 mean Cmax approximately 2-fold higher than the mean Cmax observed with the approved once daily and twice daily lopinavir and ritonavir doses at steady state. The maximum mean (95% upper confidence bound) difference from placebo in the PR interval after baseline-correction were 24.9 (21.5, 28.3) and 31.9 (28.5, 35.3) msec for 400/100 mg twice daily and supratherapeutic 800/200 mg twice daily lopinavir and ritonavir, respectively [see Warnings and Precautions (5.5, 5.6)].
12.3 Pharmacokinetics
The pharmacokinetic properties of lopinavir are summarized in Table 13. The steady-state pharmacokinetic parameters of lopinavir are summarized in Table 14. Under fed conditions, lopinavir concentrations were similar following administration of lopinavir and ritonavir tablets to capsules with less pharmacokinetic variability. Under fed conditions (500 kcal, 25% from fat), lopinavir concentrations were similar following administration of lopinavir and ritonavir capsules and oral solution.
Table 13. Pharmacokinetic Properties of Lopinavir
Absorption
Tmax (hr)a
4.4 ± 0.8
Effect of meal
(relative to fasting)
Tablet
Oral Solution↑ 19%b
↑ 130%b
Distribution
% Bound to human plasma proteins
> 98
Vd/Fa (L)
16.9
Metabolism
Metabolism
CYP3A
Elimination
Major route of elimination
hepatic
t1/2 (h)a
6.9 ± 2.2
% of dose excreted in urine
10.4 ± 2.3
% of dose excreted in feces
82.6 ± 2.5
a. Lopinavir and ritonavir tablet
b. Changes in AUC values
Table 14. Steady-State Pharmacokinetic Parameters of Lopinavir, Mean ± SD
Pharmacokinetic Parameter Twice Dailya Once Dailyb Cmax (µg/mL) 9.8 ± 3.7 11.8 ± 3.7 Cmin (µg/mL) 5.5 ± 2.7 1.7 ± 1.6 AUCtau (µg●h/mL) 92.6 ± 36.7 154.1 ± 61.4 a. 19 HIV-1 subjects, lopinavir and ritonavir 400/100 mg twice daily
b. 24 HIV-1 subjects, lopinavir and ritonavir 800/200 mg + emtricitabine 200 mg + tenofovir DF 300 mgSpecific Populations
Gender, Race and Age
No gender or race related pharmacokinetic differences have been observed in adult patients. Lopinavir pharmacokinetics have not been studied in elderly patients.
Pediatric Patients
The 230/57.5 mg/m2 twice daily regimen without nevirapine and the 300/75 mg/m2 twice daily regimen with nevirapine provided lopinavir plasma concentrations similar to those obtained in adult patients receiving the 400/100 mg twice daily regimen without nevirapine.
Table 15. Lopinavir Pharmacokinetic Data from Pediatric Clinical Trials, Mean ± SD
Cmax(μg/mL)
Cmin (μg/mL)
AUC12(μg•hr/m)
Age ≥ 14 Days to < 6 Weeks Cohort (N = 9):
5.17 ± 1.84a
1.40 ± 0.48a
43.39 ± 14.80a
Age ≥ 6 Weeks to < 6 Months Cohort (N = 18):
9.39 ± 4.91a
1.95 ± 1.80a
74.50 ± 37.87a
Age ≥ 6 Months to ≤ 12 years Cohort (N = 24):
8.2 ± 2.9b
3.4 ± 2.1b
72.6 ± 31.1b
10.0 ± 3.3c
3.6 ± 3.5c
85.8 ± 36.9c
a. Lopinavir and ritonavir oral solution 300/75 mg/m2 twice daily without concomitant NNRTI therapy
b. Lopinavir and ritonavir oral solution 230/57.5 mg/m2 twice daily without nevirapine (n=12)
c. Lopinavir and ritonavir oral solution 300/75 mg/m2 twice daily with nevirapine (n=12)
Pregnancy
The C12h values of lopinavir were lower during the second and third trimester by approximately 40% as compared to post-partum in 12 HIV-infected pregnant women received lopinavir and ritonavir 400 mg/100 mg twice daily. Yet this decrease is not considered clinically relevant in patients with no documented lopinavir and ritonavir-associated resistance substitutions receiving 400 mg/100 mg twice daily [see Use in Specific Populations (8.1)].
Renal Impairment
Lopinavir pharmacokinetics have not been studied in patients with renal impairment; however, since the renal clearance of lopinavir is negligible, a decrease in total body clearance is not expected in patients with renal impairment.
Hepatic Impairment
Multiple dosing of lopinavir and ritonavir 400/100 mg twice daily to HIV-1 and HCV co-infected patients with mild to moderate hepatic impairment (n = 12) resulted in a 30% increase in lopinavir AUC and 20% increase in Cmax compared to HIV-1 infected subjects with normal hepatic function (n = 12). Additionally, the plasma protein binding of lopinavir was statistically significantly lower in both mild and moderate hepatic impairment compared to controls (99.09 vs. 99.31%, respectively). Lopinavir and ritonavir has not been studied in patients with severe hepatic impairment [see Warnings and Precautions (5.4) and Use in Specific Populations (8.6)].
Drug Interactions
Lopinavir and ritonavir is an inhibitor of the P450 isoform CYP3A in vitro. Lopinavir and ritonavir does not inhibit CYP2D6, CYP2C9, CYP2C19, CYP2E1, CYP2B6 or CYP1A2 at clinically relevant concentrations.
Lopinavir and ritonavir has been shown in vivo to induce its own metabolism and to increase the biotransformation of some drugs metabolized by cytochrome P450 enzymes and by glucuronidation.
The effects of co-administration of lopinavir and ritonavir on the AUC, Cmax and Cmin are summarized in Table 16 (effect of other drugs on lopinavir) and Table 17 (effect of lopinavir and ritonavir on other drugs). For information regarding clinical recommendations, see Table 12 in Drug Interactions (7).
Table 16. Drug Interactions: Pharmacokinetic Parameters for Lopinavir in the Presence of the Co-administered Drug for Recommended Alterations in Dose or Regimen
Co-administered Drug
Dose of Co-administered Drug
(mg)
Dose of Lopinavir and
Ritonavir
(mg)
n
Ratio (in combination with Co-administered drug/alone) of Lopinavir Pharmacokinetic Parameters (90% CI); No Effect = 1.00
Cmax
AUC
Cmin
Efavirenz1
600 at bedtime
400/100 capsule twice daily
11, 73
0.97
(0.78, 1.22)
0.81
(0.64, 1.03)
0.61
(0.38, 0.97)
600 at bedtime
500/125 tablet
twice daily
19
1.12
(1.02, 1.23)
1.06
(0.96, 1.17)
0.90
(0.78, 1.04)
600 at bedtime
600/150 tablet
twice daily
23
1.36
(1.28, 1.44)
1.36
(1.28, 1.44)
1.32
(1.21, 1.44)
Etravirine
200 twice daily
400/100 mg twice day (tablets)
16
0.89
(0.82-0.96)
0.87
(0.83-0.92)
0.80
(0.73-0.88)
Fosamprenavir2
700 twice daily plus ritonavir 100 twice daily
400/100 capsule twice daily
18
1.30
(0.85, 1.47)
1.37
(0.80, 1.55)
1.52
(0.72, 1.82)
Ketoconazole
200 single dose
400/100 capsule twice daily
12
0.89
(0.80, 0.99)
0.87
(0.75, 1.00)
0.75
(0.55, 1.00)
Nelfinavir
1000 twice daily
400/100 capsule twice daily
13
0.79
(0.70, 0.89)
0.73
(0.63, 0.85)
0.62
(0.49, 0.78)
Nevirapine
200 twice daily
steady-state
400/100 capsule twice daily
22, 193
0.81
(0.62, 1.05)
0.73
(0.53, 0.98)
0.49
(0.28, 0.74)
7 mg/kg or 4 mg/kg once daily;
twice daily
1 wk5
(> 1 yr) 300/75 mg/m2
oral solution
twice daily
12, 153
0.86
(0.64, 1.16)
0.78
(0.56, 1.09)
0.45
(0.25, 0.81)
Ombitasvir/
paritaprevir/
ritonavir+
dasabuvir2
25/150/100 +
dasabuvir 400
400/100 tablet
twice daily
6
0.87
(0.76, 0.99)
0.94
(0.81, 1.10)
1.15
(0.93, 1.42)
Omeprazole
40 once daily, 5 d
400/100 tablet twice daily, 10 d
12
1.08
(0.99, 1.17)
1.07
(0.99, 1.15)
1.03
(0.90, 1.18)
40 once daily, 5 d
800/200 tablet once daily, 10 d
12
0.94
(0.88, 1.00)
0.92
(0.86, 0.99)
0.71
(0.57, 0.89)
Pravastatin
20 once daily, 4 d
400/100 capsule twice daily, 14 d
12
0.98
(0.89, 1.08)
0.95
(0.85, 1.05)
0.88
(0.77, 1.02)
Ranitidine
150 single dose
400/100 tablet twice daily, 10 d
12
0.99
(0.95, 1.03)
0.97
(0.93, 1.01)
0.90
(0.85, 0.95)
150 single dose
800/200 tablet once daily, 10 d
10
0.97
(0.95, 1.00)
0.95
(0.91, 0.99)
0.82
(0.74, 0.91)
Rifabutin
150 once daily
400/100 capsule twice daily
14
1.08
(0.97, 1.19)
1.17
(1.04, 1.31)
1.20
(0.96, 1.65)
Rifampin
600 once daily
400/100 capsule twice daily
22
0.45
(0.40, 0.51)
0.25
(0.21, 0.29)
0.01
(0.01, 0.02)
600 once daily
800/200 capsule twice daily
10
1.02
(0.85, 1.23)
0.84
(0.64, 1.10)
0.43
(0.19, 0.96)
600 once daily
400/400 capsule twice daily
9
0.93
(0.81, 1.07)
0.98
(0.81, 1.17)
1.03
(0.68, 1.56)
Rilpivirine
150 once daily
400/100 twice daily (capsules)
15
0.96
(0.88-1.05)
0.99
(0.89-1.10)
0.89
(0.73-1.08)
Ritonavir
100 twice daily
400/100 capsule twice daily
8, 213
1.28
(0.94, 1.76)
1.46
(1.04, 2.06)
2.16
(1.29, 3.62)
Tipranavir/
ritonavir
500/200 twice daily
400/100 capsule twice daily
21
693
0.53
(0.40, 0.69)
0.45
(0.32, 0.63)
0.30
(0.17, 0.51)
0.484
(0.40, 0.58)
1 Reference for comparison is lopinavir/ritonavir 400/100 mg twice daily without efavirenz. 2 Data extracted from the U.S. prescribing information of co-administered drugs.
3 Parallel group design
4 Drug levels obtained at 8-16 hours post dose
N/A = Not available.
Table 17. Drug Interactions: Pharmacokinetic Parameters for Co-administered Drug in the Presence of Lopinavir and Ritonavir for Recommended Alterations in Dose or Regimen
Co-administered Drug
Dose of Co-administered Drug
(mg)
Dose of Lopinavir and
Ritonavir
(mg)
n
Ratio (in combination with Lopinavir and Ritonavir/alone) of Co-administered Drug Pharmacokinetic Parameters (90% CI); No Effect = 1.00
Cmax
AUC
Cmin
Bedaquiline1
400 single dose
400/100 twice daily
N/A
N/A
1.22
(1.11, 1.34)
N/A
Efavirenz
600 at bedtime
400/100
capsule twice daily
11, 123
0.91
(0.72, 1.15)
0.84
(0.62, 1.15)
0.84
(0.58, 1.20)
Elbasvir/
grazoprevir1
50 once daily
400/100
twice daily
10
2.87
(2.29, 3.58)
3.71
(3.05, 4.53)
4.58
(3.72, 5.64)
200 once daily
13
7.31
(5.65, 9.45)
12.86
(10.25, 16.13)
21.70
(12.99, 36.25)
Ethinyl
Estradiol
35 µg once daily
(Ortho Novum®)
400/100
capsule twice daily
12
0.59
(0.52, 0.66)
0.58
(0.54, 0.62)
0.42
(0.36, 0.49)
Etravirine
200 twice daily
400/100 tablet twice day
16
0.70
(0.64-0.78)
0.65
(0.59-0.71)
0.55
(0.49-0.62)
Fosamprenavir1
700 twice daily plus ritonavir 100 twice daily
400/100
capsule twice daily
18
0.42
(0.30, 0.58)
0.37
(0.28, 0.49)
0.35
(0.27, 0.46)
Indinavir
600 twice daily combo nonfasting vs. 800 three times daily alone fasting
400/100
capsule twice daily
13
0.71
(0.63, 0.81)
0.91
(0.75, 1.10)
3.47
(2.60, 4.64)
Ketoconazole
200 single dose
400/100
capsule twice daily
12
1.13
(0.91, 1.40)
3.04
(2.44, 3.79)
N/A
Maraviroc1
300 twice daily
400/100
twice daily
11
1.97
(1.66, 2.34)
3.95
(3.43, 4.56)
9.24
(7.98, 10.7)
Methadone
5 single dose
400/100
capsule twice daily
11
0.55
(0.48, 0.64)
0.47
(0.42, 0.53)
N/A
Nelfinavir
1000 twice daily combo vs. 1250 twice daily alone
400/100
capsule twice daily
13
0.93
(0.82, 1.05)
1.07
(0.95, 1.19)
1.86
(1.57, 2.22)
M8 metabolite
2.36
(1.91, 2.91)
3.46
(2.78, 4.31)
7.49
(5.85, 9.58)
Nevirapine
200 once daily twice daily
400/100
capsule twice daily
5,
63
1.05
(0.72, 1.52)
1.08
(0.72, 1.64)
1.15
(0.71, 1.86)
Norethindrone
1 once daily
(Ortho Novum®)
400/100
capsule twice daily
12
0.84
(0.75, 0.94)
0.83
(0.73, 0.94)
0.68
(0.54, 0.85)
Ombitasvir/
paritaprevir/
ritonavir+
dasabuvir1
25/150/100 +
dasabuvir 400
400/100
tablet twice
daily
6
1.14
(1.01, 1.28)
1.17
(1.07, 1.28)
1.24
(1.14, 1.34)
2.04
(1.30, 3.20)
2.17
(1.63, 2.89)
2.36
(1.00, 5.55)
1.55
(1.16, 2.09)
2.05
(1.49, 2.81)
5.25
(3.33, 8.28)
0.99
(0.75, 1.31)
0.93
(0.75, 1.15)
0.68
(0.57, 0.80)
Pitavastatin1
4 once daily
400/100 tablet twice daily
23
0.96
(0.84-1.10)
0.80
(0.73-0.87)
N/A
Pravastatin
20 once daily
400/100 capsule twice daily
12
1.26
(0.87, 1.83)
1.33
(0.91, 1.94)
N/A
Rifabutin
150 once daily combo vs. 300 once daily alone
400/100 capsule twice daily
12
2.12
(1.89, 2.38)
3.03
(2.79, 3.30)
4.90
(3.18, 5.76)
25-O-desacetyl rifabutin
23.6
(13.7, 25.3)
47.5
(29.3, 51.8)
94.9
(74.0, 122)
Rifabutin + 25-O-desacetyl rifabutin
3.46
(3.07, 3.91)
5.73
(5.08, 6.46)
9.53
(7.56, 12.01)
Rilpivirine
150 once daily
400/100 capsules twice daily
15
1.29
(1.18-1.40)
1.52
(1.36-1.70)
1.74
(1.46-2.08)
Rosuvastatin2
20 once daily
400/100 tablet twice daily
15
4.66
(3.4, 6.4)
2.08
(1.66, 2.6)
1.04
(0.9, 1.2)
Tenofovir
alafenamide1
10 once daily
800/200
tablet once daily
10
2.19
(1.72, 2.79)
1.47
(1.17, 1.85)
N/A
Tenofovir
disoproxil
fumarate1
300 once daily
400/100 capsule twice daily
24
No
Change
1.32
(1.26, 1.38)
1.51
(1.32, 1.66)
1 Data extracted from the U.S. prescribing information of co-administered drugs. 2 Kiser, et al. J Acquir Immune Defic Syndr. 2008 Apr 15; 47(5):570-8.
3 Parallel group design
N/A = Not available.
12.4 Microbiology
Mechanism of Action
Lopinavir, an inhibitor of the HIV-1 protease, prevents cleavage of the viral Gag-Pol polyprotein, resulting in the production of immature, non-infectious viral particles.
Antiviral Activity
In the absence of human serum, the mean 50% effective concentration (EC50) values of lopinavir against five different HIV-1 subtype B laboratory strains in lymphoblastic cell lines ranged from 10-27 nM (0.006-0.017 µg/mL, 1 µg/mL = 1.6 µM), and ranged from 4-11 nM (0.003-0.007 µg/mL) against several HIV-1 subtype B clinical isolates in peripheral blood lymphocytes (n = 6). In the presence of 50% human serum, the mean EC50 values of lopinavir against these five HIV-1 laboratory strains ranged from 65-289 nM (0.04-0.18 µg/mL), representing a 7 to 11-fold attenuation. The EC50 values of lopinavir against three different HIV-2 strains ranged from 12-180 nM (0.008-113 μg/mL).
Resistance
HIV-1 isolates with reduced susceptibility to lopinavir have been selected in cell culture. The presence of ritonavir does not appear to influence the selection of lopinavir-resistant viruses in cell culture.
In a study of 653 antiretroviral treatment-naïve patients (Study 863), plasma viral isolates from each patient on treatment with plasma HIV-1 RNA >400 copies/mL at Week 24, 32, 40 and/or 48 were analyzed. No specific amino acid substitutions could be associated with resistance to lopinavir and ritonavir in the virus from 37 evaluable loninavir and ritonavir-treated patients. The selection of resistance to lopinavir and ritonavir in antiretroviral treatment-naïve pediatric patients (Study 940) appears to be consistent with that seen in adult patients (Study 863).
Resistance to lopinavir and ritonavir has been noted to emerge in patients treated with other protease inhibitors prior to lopinavir and ritonavir therapy. In studies of 227 antiretroviral treatment-naïve and protease inhibitor experienced patients, isolates from 4 of 23 patients with quantifiable (>400 copies/mL) viral RNA following treatment with lopinavir and ritonavir for 12 to 100 weeks displayed significantly reduced susceptibility to lopinavir compared to the corresponding baseline viral isolates. All four of these patients had previously received treatment at least one protease inhibitor and had at least 4 substitutions associated with protease inhibitor resistance immediately prior to lopinavir and ritonavir therapy. Following viral rebound, isolates from these patients all contained additional substitutions, some of which are recognized to be associated with protease inhibitor resistance.
Cross-resistance - Nonclinical Studies
Varying degrees of cross-resistance have been observed among HIV-1 protease inhibitors. The antiviral activity in cell culture of lopinavir against clinical isolates from patients previously treated with a single protease inhibitor was determined (Table 18).
Table 18. Susceptibility Reduction to Lopinavir Against Isolates from Patients Previously Treated With a Single Protease Inhibitor
Susceptibility reduced by >4 fold
Susceptibility reduced to LPV
Indinavir (n=16)
5.7 fold
Nelfinavir (n=13)
<4 fold
Ritonavir (n=3)
8.32 fold
Saquinavir (n=4)
<4 fold
Isolates from patients previously treated with two or more protease inhibitors showed greater reductions in susceptibility to lopinavir, as described in the following section.
Clinical Studies - Antiviral Activity of Lopinavir and Ritonavir in Patients with Previous Protease Inhibitor Therapies
The clinical relevance of reduced susceptibility in cell culture to lopinavir has been examined by assessing the virologic response to lopinavir and ritonavir therapy in treatment-experienced patients, with respect to baseline viral genotype in three studies and baseline viral phenotype in one study.
Virologic response to lopinavir and ritonavir has been shown to be affected by the presence of three or more of the following amino acid substitutions in protease at baseline: L10F/I/R/V, K20M/N/R, L24I, L33F, M36I, I47V, G48V, I54L/T/V, V82A/C/F/S/T, and I84V. Table 19 shows the 48-week virologic response (HIV-1 RNA <400 copies/mL) according to the number of the above protease inhibitor resistance-associated substitutions at baseline in studies 888 and 765 [see Clinical Studies (14.2) and (14.3)] and study 957 (see below). Once daily administration of lopinavir and ritonavir for adult patients with three or more of the above substitutions is not recommended.
Table 19. Virologic Response (HIV-1 RNA <400 copies/mL) at Week 48 by Baseline Lopinavir and Ritonavir Susceptibility and by Number of Protease Substitutions Associated with Reduced Response to Lopinavir and Ritonavir1 Number of protease inhibitor substitutions at baseline1
Study 888 (Single protease inhibitor-experienced2, NNRTI-naïve) n=130
Study 765 (Single protease inhibitor-experienced3, NNRTI-naïve) n=56
Study 957 (Multiple protease inhibitor-experienced4, NNRTI-naïve) n=50
0-2
76/103 (74%)
34/45 (76%)
19/20 (95%)
3-5
13/26 (50%)
8/11 (73%)
18/26 (69%)
6 or more
0/1 (0%)
N/A
1/4 (25%)
1 Substitutions considered in the analysis included L10F/I/R/V, K20M/N/R, L24I, L33F, M36I, I47V, G48V, I54L/T/V, V82A/C/F/S/T, and I84V. 2 43% indinavir, 42% nelfinavir, 10% ritonavir, 15% saquinavir.
3 41% indinavir, 38% nelfinavir, 4% ritonavir, 16% saquinavir.
4 86% indinavir, 54% nelfinavir, 80% ritonavir, 70% saquinavir.
Virologic response to lopinavir and ritonavir therapy with respect to phenotypic susceptibility to lopinavir at baseline was examined in Study 957. In this study 56 NNRTI-naïve patients with HIV-1 RNA >1,000 copies/mL despite previous therapy with at least two protease inhibitors selected from indinavir, nelfinavir, ritonavir, and saquinavir were randomized to receive one of two doses of lopinavir and ritonavir in combination with efavirenz and nucleoside reverse transcriptase inhibitors (NRTIs). The EC50 values of lopinavir against the 56 baseline viral isolates ranged from 0.5- to 96-fold the wild-type EC50 value. Fifty-five percent (31/56) of these baseline isolates displayed >4-fold reduced susceptibility to lopinavir. These 31 isolates had a median reduction in lopinavir susceptibility of 18-fold. Response to therapy by baseline lopinavir susceptibility is shown in Table 20.Table 20. HIV-1 RNA Response at Week 48 by Baseline Lopinavir Susceptibility1 Lopinavir susceptibility2 at baseline
HIV-1 RNA <400 copies/mL (%)
HIV-1 RNA <50 copies/mL (%)
< 10 fold
25/27 (93%)
22/27 (81%)
> 10 and < 40 fold
11/15 (73%)
9/15 (60%)
≥ 40 fold
2/8 (25%)
2/8 (25%)
1 Lopinavir susceptibility was determined by recombinant phenotypic technology performed by Virologic. 2 Fold change in susceptibility from wild type.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Lopinavir and ritonavir combination was evaluated for carcinogenic potential by oral gavage administration to mice and rats for up to 104 weeks. Results showed an increase in the incidence of benign hepatocellular adenomas and an increase in the combined incidence of hepatocellular adenomas plus carcinoma in both males and females in mice and males in rats at doses that produced approximately 1.6-2.2 times (mice) and 0.5 times (rats) the human exposure (based on AUC0-24hr measurement) at the recommended dose of 400/100 mg lopinavir and ritonavir twice daily. Administration of lopinavir and ritonavir did not cause a statistically significant increase in the incidence of any other benign or malignant neoplasm in mice or rats.
Carcinogenicity studies in mice and rats have been carried out on ritonavir. In male mice, there was a dose dependent increase in the incidence of both adenomas and combined adenomas and carcinomas in the liver. Based on AUC measurements, the exposure at the high dose was approximately 4-fold for males that of the exposure in humans with the recommended therapeutic dose (400/100 mg lopinavir and ritonavir twice daily). There were no carcinogenic effects seen in females at the dosages tested. The exposure at the high dose was approximately 9-fold for the females that of the exposure in humans. There were no carcinogenic effects in rats. In this study, the exposure at the high dose was approximately 0.7-fold that of the exposure in humans with the 400/100 mg lopinavir and ritonavir twice daily regimen. Based on the exposures achieved in the animal studies, the significance of the observed effects is not known.
Mutagenesis
Neither lopinavir nor ritonavir was found to be mutagenic or clastogenic in a battery of in vitro and in vivo assays including the Ames bacterial reverse mutation assay using S. typhimurium and E. coli, the mouse lymphoma assay, the mouse micronucleus test and chromosomal aberration assays in human lymphocytes.
Impairment of Fertility
Lopinavir in combination with ritonavir at a 2:1 ratio produced no effects on fertility in male and female rats at levels of 10/5, 30/15 or 100/50 mg/kg/day. Based on AUC measurements, the exposures in rats at the high doses were approximately 0.7-fold for lopinavir and 1.8-fold for ritonavir of the exposures in humans at the recommended therapeutic dose (400/100 mg twice daily).
-
14 CLINICAL STUDIES
14.1 Adult Patients without Prior Antiretroviral Therapy
Study 863: Lopinavir and Ritonavir Capsules twice daily + stavudine + lamivudine compared to nelfinavir three times daily + stavudine + lamivudine
Study 863 was a randomized, double-blind, multicenter trial comparing treatment with lopinavir and ritonavir capsules (400/100 mg twice daily) plus stavudine and lamivudine versus nelfinavir (750 mg three times daily) plus stavudine and lamivudine in 653 antiretroviral treatment naïve patients. Patients had a mean age of 38 years (range: 19 to 84), 57% were Caucasian, and 80% were male. Mean baseline CD4+ cell count was 259 cells/mm3 (range: 2 to 949 cells/mm3) and mean baseline plasma HIV-1 RNA was 4.9 log10 copies/mL (range: 2.6 to 6.8 log10 copies/mL).
Treatment response and outcomes of randomized treatment are presented in Table 21.
Table 21. Outcomes of Randomized Treatment Through Week 48 (Study 863) Outcome
Lopinavir and Ritonavir+d4T+3TC
(N = 326)Nelfinavir+d4T+3TC
(N = 327)Responder1
75%
62%
Virologic failure2
Rebound
Never suppressed through Week 48
9%
7%
2%
25%
15%
9%
Death
2%
1%
Discontinued due to adverse events
4%
4%
Discontinued for other reasons3
10%
8%
1 Patients achieved and maintained confirmed HIV-1 RNA < 400 copies/mL through Week 48. 2 Includes confirmed viral rebound and failure to achieve confirmed < 400 copies/mL through Week 48.
3 Includes lost to follow-up, patient's withdrawal, non-compliance, protocol violation and other reasons. Overall discontinuation through Week 48, including patients who discontinued subsequent to virologic failure, was 17% in the lopinavir and ritonavir arm and 24% in the nelfinavir arm.
Through 48 weeks of therapy, there was a statistically significantly higher proportion of patients in the lopinavir and ritonavir arm compared to the nelfinavir arm with HIV-1 RNA < 400 copies/mL (75% vs. 62%, respectively) and HIV-1 RNA < 50 copies/mL (67% vs. 52%, respectively). Treatment response by baseline HIV-1 RNA level subgroups is presented in Table 22.
Table 22. Proportion of Responders Through Week 48 by Baseline Viral Load (Study 863) Baseline Viral Load
(HIV-1 RNA copies/mL)Lopinavir and Ritonavir +d4T+3TC
Nelfinavir +d4T+3TC
<400 copies/mL1
<50 copies/mL2
n
<400 copies/mL1
<50 copies/mL2
n
< 30,000
74%
71%
82
79%
72%
87
≥ 30,000 to < 100,000
81%
73%
79
67%
54%
79
≥ 100,000 to < 250,000
75%
64%
83
60%
47%
72
≥ 250,000
72%
60%
82
44%
33%
89
1 Patients achieved and maintained confirmed HIV-1 RNA < 400 copies/mL through Week 48. 2 Patients achieved HIV-1 RNA < 50 copies/mL at Week 48.
Through 48 weeks of therapy, the mean increase from baseline in CD4+ cell count was 207 cells/mm3 for the lopinavir and ritonavir arm and 195 cells/mm3 for the nelfinavir arm.
Study 730: Lopinavir and Ritonavir Tablets once daily + tenofovir DF + emtricitabine compared to Lopinavir and Ritonavir Tablets twice daily + tenofovir DF + emtricitabine
Study 730 was a randomized, open-label, multicenter trial comparing treatment with lopinavir and ritonavir 800/200 mg once daily plus tenofovir DF and emtricitabine versus lopinavir and ritonavir 400/100 mg twice daily plus tenofovir DF and emtricitabine in 664 antiretroviral treatment-naïve patients. Patients were randomized in a 1:1 ratio to receive either lopinavir and ritonavir 800/200 mg once daily (n = 333) or lopinavir and ritonavir 400/100 mg twice daily (n = 331). Further stratification within each group was 1:1 (tablet vs. capsule). Patients administered the capsule were switched to the tablet formulation at Week 8 and maintained on their randomized dosing schedule. Patients were administered emtricitabine 200 mg once daily and tenofovir DF 300 mg once daily. Mean age of patients enrolled was 39 years (range: 19 to 71); 75% were Caucasian, and 78% were male. Mean baseline CD4+ cell count was 216 cells/mm3 (range: 20 to 775 cells/mm3) and mean baseline plasma HIV-1 RNA was 5.0 log10 copies/mL (range: 1.7 to 7.0 log10 copies/mL).
Treatment response and outcomes of randomized treatment through Week 48 are presented in Table 23.
Table 23. Outcomes of Randomized Treatment Through Week 48 (Study 730) Outcome
Lopinavir and Ritonavir Once Daily + TDF + FTC
(n = 333)Lopinavir and Ritonavir Twice Daily + TDF + FTC
(n = 331)Responder1
78%
77%
Virologic failure2
Rebound
Never suppressed through Week 48
10%
5%
5%
8%
5%
3%
Death
1%
<1%
Discontinued due to adverse events
4%
3%
Discontinued for other reasons3
8%
11%
1 Patients achieved and maintained confirmed HIV-1 RNA < 50 copies/mL through Week 48. 2 Includes confirmed viral rebound and failure to achieve confirmed < 50 copies/mL through Week 48.
3 Includes lost to follow-up, patient's withdrawal, non-compliance, protocol violation and other reasons.
Through 48 weeks of therapy, 78% in the lopinavir and ritonavir once daily arm and 77% in the lopinavir and ritonavir twice daily arm achieved and maintained HIV-1 RNA < 50 copies/mL (95% confidence interval for the difference, -5.9% to 6.8%). Mean CD4+ cell count increases at Week 48 were 186 cells/mm3 for the lopinavir and ritonavir once daily arm and 198 cells/mm3 for the lopinavir and ritonavir twice daily arm.
14.2 Adult Patients with Prior Antiretroviral Therapy
Study 888: Lopinavir and Ritonavir Capsules twice daily + nevirapine + NRTIs compared to investigator-selected protease inhibitor(s) + nevirapine + NRTIs
Study 888 was a randomized, open-label, multicenter trial comparing treatment with lopinavir and ritonavir capsules (400/100 mg twice daily) plus nevirapine and nucleoside reverse transcriptase inhibitors versus investigator-selected protease inhibitor(s) plus nevirapine and nucleoside reverse transcriptase inhibitors in 288 single protease inhibitor-experienced, non-nucleoside reverse transcriptase inhibitor (NNRTI)-naïve patients. Patients had a mean age of 40 years (range: 18 to 74), 68% were Caucasian, and 86% were male. Mean baseline CD4+ cell count was 322 cells/mm3 (range: 10 to 1059 cells/mm3) and mean baseline plasma HIV-1 RNA was 4.1 log10 copies/mL (range: 2.6 to 6.0 log10 copies/mL).
Treatment response and outcomes of randomized treatment through Week 48 are presented in Table 24.
Table 24. Outcomes of Randomized Treatment Through Week 48 (Study 888) Outcome
Lopinavir and Ritonavir + nevirapine + NRTIs
(n = 148)Investigator-Selected Protease Inhibitor(s) + nevirapine + NRTIs
(n = 140)Responder1
57%
33%
Virologic failure2
Rebound
Never suppressed through Week 48
24%
11%
13%
41%
19%
23%
Death
1%
2%
Discontinued due to adverse events
5%
11%
Discontinued for other reasons3
14%
13%
1 Patients achieved and maintained confirmed HIV-1 RNA < 400 copies/mL through Week 48. 2 Includes confirmed viral rebound and failure to achieve confirmed < 400 copies/mL through Week 48.
3 Includes lost to follow-up, patient's withdrawal, non-compliance, protocol violation and other reasons.
Through 48 weeks of therapy, there was a statistically significantly higher proportion of patients in the lopinavir and ritonavir arm compared to the investigator-selected protease inhibitor(s) arm with HIV-1 RNA < 400 copies/mL (57% vs. 33%, respectively).
Through 48 weeks of therapy, the mean increase from baseline in CD4+ cell count was 111 cells/mm3 for the lopinavir and ritonavir arm and 112 cells/mm3 for the investigator-selected protease inhibitor(s) arm.
Study 802: Lopinavir and Ritonavir Tablets 800/200 mg Once Daily Versus 400/100 mg Twice Daily when Co-administered with Nucleoside/Nucleotide Reverse Transcriptase Inhibitors in Antiretroviral-Experienced, HIV-1 Infected Subjects
M06-802 was a randomized open-label study comparing the safety, tolerability, and antiviral activity of once daily and twice daily dosing of lopinavir and ritonavir tablets in 599 subjects with detectable viral loads while receiving their current antiviral therapy. Of the enrolled subjects, 55% on both treatment arms had not been previously treated with a protease inhibitor and 81 – 88% had received prior NNRTIs as part of their anti-HIV treatment regimen. Patients were randomized in a 1:1 ratio to receive either lopinavir and ritonavir 800/200 mg once daily (n = 300) or lopinavir and ritonavir 400/100 mg twice daily (n = 299). Patients were administered at least two nucleoside/nucleotide reverse transcriptase inhibitors selected by the investigator. Mean age of patients enrolled was 41 years (range: 21 to 73); 51% were Caucasian, and 66% were male. Mean baseline CD4+ cell count was 254 cells/mm3 (range: 4 to 952 cells/mm3) and mean baseline plasma HIV-1 RNA was 4.3 log10 copies/mL (range: 1.7 to 6.6 log10 copies/mL).
Treatment response and outcomes of randomized treatment through Week 48 are presented in Table 25.
Table 25. Outcomes of Randomized Treatment Through Week 48 (Study 802) Outcome
Lopinavir and Ritonavir Once Daily + NRTIs
(n = 300)Lopinavir and Ritonavir Twice Daily + NRTIs
(n = 299)Virologic Success
(HIV-1 RNA <50 copies/mL)57%
54%
Virologic failure1
22%
24%
No virologic data in Week 48 window
Discontinued study due to adverse event or death2
5%
7%
Discontinued study for other reasons3
13%
12%
Missing data during window but on study
3%
3%
1 Includes patients who discontinued prior to Week 48 for lack or loss of efficacy and patients with HIV-1 RNA ≥ 50 copies/mL at Week 48. 2 Includes patients who discontinued due to adverse events or death at any time from Day 1 through Week 48 if this resulted in no virologic data on treatment at Week 48.
3 Includes withdrawal of consent, loss to follow-up, non-compliance, protocol violation and other reasons.
Through 48 weeks of treatment, the mean change from baseline for CD4 + cell count was 135 cells/mm3 for the once daily group and 122 cells/mm3 for the twice daily group.
14.3 Other Studies Supporting Approval in Adult Patients
Study 720: Lopinavir and Ritonavir twice daily + stavudine + lamivudine
Study 765: Lopinavir and Ritonavir twice daily + nevirapine + NRTIs
Study 720 (patients without prior antiretroviral therapy) and study 765 (patients with prior protease inhibitor therapy) were randomized, blinded, multi-center trials evaluating treatment with lopinavir and ritonavir at up to three dose levels (200/100 mg twice daily [720 only], 400/100 mg twice daily, and 400/200 mg twice daily). In Study 720, all patients switched to 400/100 mg twice daily between Weeks 48-72. Patients in study 720 had a mean age of 35 years, 70% were Caucasian, and 96% were male, while patients in study 765 had a mean age of 40 years, 73% were Caucasian, and 90% were male. Mean (range) baseline CD4+ cell counts for patients in study 720 and study 765 were 338 (3-918) and 372 (72-807) cells/mm3, respectively. Mean (range) baseline plasma HIV-1 RNA levels for patients in study 720 and study 765 were 4.9 (3.3 to 6.3) and 4.0 (2.9 to 5.8) log10 copies/mL, respectively.
Through 360 weeks of treatment in study 720, the proportion of patients with HIV-1 RNA < 400 (< 50) copies/mL was 61% (59%) [n = 100]. Among patients completing 360 weeks of treatment with CD4+ cell count measurements [n=60], the mean (median) increase in CD4+ cell count was 501 (457) cells/mm3. Thirty-nine patients (39%) discontinued the study, including 13 (13%) discontinuations due to adverse reactions and 1 (1%) death.
Through 144 weeks of treatment in study 765, the proportion of patients with HIV-1 RNA < 400 (< 50) copies/mL was 54% (50%) [n = 70], and the corresponding mean increase in CD4+ cell count was 212 cells/mm3. Twenty-seven patients (39%) discontinued the study, including 5 (7%) discontinuations secondary to adverse reactions and 2 (3%) deaths.
14.4 Pediatric Studies
Study 1030 was an open-label, multicenter, dose-finding trial evaluating the pharmacokinetic profile, tolerability, safety and efficacy of lopinavir and ritonavir oral solution containing lopinavir 80 mg/mL and ritonavir 20 mg/mL at a dose of 300/75 mg/m2 twice daily plus 2 NRTIs in HIV-1 infected infants ≥14 days and <6 months of age.
Ten infants, ≥14 days and <6 wks of age, were enrolled at a median (range) age of 5.7 (3.6-6.0) weeks and all completed 24 weeks. At entry, median (range) HIV-1 RNA was 6.0 (4.7-7.2) log10 copies/mL. Seven of 10 infants had HIV-1 RNA <400 copies/mL at Week 24. At entry, median (range) CD4+ percentage was 41 (16-59) with a median decrease of 1% (95% CI: -10, 18) from baseline to week 24 in 6 infants with available data.
Twenty-one infants, between 6 weeks and 6 months of age, were enrolled at a median (range) age of 14.7 (6.9-25.7) weeks and 19 of 21 infants completed 24 weeks. At entry, median (range) HIV RNA level was 5.8 (3.7-6.9) log10 copies/mL. Ten of 21 infants had HIV RNA <400 copies/mL at Week 24. At entry, the median (range) CD4+ percentage was 32 (11-54) with a median increase of 4% (95% CI: -1, 9) from baseline to week 24 in 19 infants with available data [see Clinical Pharmacology (12.3) for pharmacokinetic results].
Study 940 was an open-label, multicenter trial evaluating the pharmacokinetic profile, tolerability, safety and efficacy of lopinavir and ritonavir oral solution containing lopinavir 80 mg/mL and ritonavir 20 mg/mL in 100 antiretroviral naïve (44%) and experienced (56%) pediatric patients. All patients were non-nucleoside reverse transcriptase inhibitor naïve. Patients were randomized to either 230 mg lopinavir/57.5 mg ritonavir per m2 or 300 mg lopinavir/75 mg ritonavir per m2. Naïve patients also received lamivudine and stavudine. Experienced patients received nevirapine plus up to two nucleoside reverse transcriptase inhibitors.
Safety, efficacy and pharmacokinetic profiles of the two dose regimens were assessed after three weeks of therapy in each patient. After analysis of these data, all patients were continued on the 300 mg lopinavir/75 mg ritonavir per m2 dose. Patients had a mean age of 5 years (range 6 months to 12 years) with 14% less than 2 years. Mean baseline CD4+ cell count was 838 cells/mm3 and mean baseline plasma HIV-1 RNA was 4.7 log10 copies/mL.
Through 48 weeks of therapy, the proportion of patients who achieved and sustained an HIV-1 RNA < 400 copies/mL was 80% for antiretroviral naïve patients and 71% for antiretroviral experienced patients. The mean increase from baseline in CD4+ cell count was 404 cells/mm3 for antiretroviral naïve and 284 cells/mm3 for antiretroviral experienced patients treated through 48 weeks. At 48 weeks, two patients (2%) had prematurely discontinued the study. One antiretroviral naïve patient prematurely discontinued secondary to an adverse reaction, while one antiretroviral experienced patient prematurely discontinued secondary to an HIV-1 related event.
Dose selection in pediatric patients was based on the following:
- Among patients 14 days to 6 months of age receiving 300/75 mg/m2 twice daily without nevirapine, plasma concentrations were lower than those observed in adults or in older children. This dose resulted in HIV-1 RNA < 400 copies/mL in 55% of patients (70% in those initiating treatment at <6 weeks of age).
- Among patients 6 months to 12 years of age, the 230/57.5 mg/m2 oral solution twice daily regimen without nevirapine and the 300/75 mg/m2 oral solution twice daily regimen with nevirapine provided lopinavir plasma concentrations similar to those obtained in adult patients receiving the 400/100 mg twice daily regimen (without nevirapine). These doses resulted in treatment benefit (proportion of patients with HIV-1 RNA < 400 copies/mL) similar to that seen in the adult clinical trials.
- Among patients 12 to 18 years of age receiving 400/100 mg/m2 or 480/120 mg/m2 (with efavirenz) twice daily, plasma concentrations were 60-100% higher than among 6 to 12 year old patients receiving 230/57.5 mg/m2. Mean apparent clearance was similar to that observed in adult patients receiving standard dose and in patients 6 to 12 years of age. Although changes in HIV-1 RNA in patients with prior treatment failure were less than anticipated, the pharmacokinetic data supports use of similar dosing as in patients 6 to 12 years of age, not to exceed the recommended adult dose.
- For all age groups, the body surface area dosing was converted to body weight dosing using the patient’s prescribed lopinavir dose.
-
16 HOW SUPPLIED/STORAGE AND HANDLING
Lopinavir and Ritonavir Oral Solution USP is a colorless to yellow colored liquid supplied in amber-colored multiple-dose bottles containing 400 mg lopinavir and 100 mg ritonavir per 5 mL (80 mg lopinavir and 20 mg ritonavir per mL) packaged with a marked syringe and bottle adapter in the following size:
160 mL bottle …………………………………(NDC 0527-1947-48)
Recommended Storage:
Store lopinavir and ritonavir oral solution at 2°-8°C (36°-46°F) until dispensed. Avoid exposure to excessive heat. For patient use: refrigerated lopinavir and ritonavir oral solution remains stable until the expiration date printed on the label. If stored at room temperature up to 25°C (77°F), oral solution should be used within 2 months.
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide)
General Administration Information [see Dosage and Administration (2)]:
- Advise patients to pay special attention to accurate administration of their dose to minimize the risk of accidental overdose or underdose of lopinavir and ritonavir.
- Advise patients and caregivers that the oral solution should be administered using the calibrated dosing cup (supplied) or oral dosing syringe.
- Advise caregivers to inform their healthcare provider if the child’s weight changes in order to make sure that the child’s lopinavir and ritonavir dose is adjusted as needed.
- Inform patients and caregivers that lopinavir and ritonavir oral solution should be taken with food to enhance absorption.
- Advise patients to remain under the care of a healthcare provider while using lopinavir and ritonavir and to take lopinavir and ritonavir in combination with other antiretroviral drugs as prescribed.
- Advise patients not to alter the dose or discontinue therapy without consulting with their healthcare provider. If a dose of lopinavir and ritonavir is missed patients should take the dose as soon as possible and then return to their normal schedule. However, if a dose is skipped the patient should not double the next dose.
- Inform patients that it is important to take lopinavir and ritonavir on a regular dosing schedule as directed and to avoid missing doses as that can result in development of resistance.
- Inform patients that there may be a greater chance of developing diarrhea with the once daily regimen as compared with the twice daily regimen.
- Inform patients that lopinavir and ritonavir is not a cure for HIV-1 infection and that they may continue to experience illnesses associated with HIV-1 infection, including opportunistic infections.
Drug Interactions
Inform patients that lopinavir and ritonavir may interact with some drugs; therefore, patients should be advised to report to their healthcare provider the use of any prescription, non-prescription medication or herbal products such as St. John’s Wort [see Contraindications (4), Warnings and Precautions (5.1) and Drug Interactions (7)].
Pancreatitis
Advise patients that pancreatitis has been observed in patients receiving lopinavir and ritonavir and to alert their healthcare provider if they experience symptoms such as nausea, vomiting or abdominal pain [see Warnings and Precautions (5.3)].
Skin Rash
Inform patients that skin rash ranging in severity from mild to toxic epidermal necrolysis (TEN), Stevens-Johnson syndrome, erythema multiforme, urticaria, and angioedema have been reported in patients receiving lopinavir and ritonavir or its components lopinavir and/or ritonavir. Advise patients to contact their healthcare provider if they develop a rash while taking lopinavir and ritonavir [see Adverse Reactions (6.1)].
Hepatotoxicity
Pre-existing liver disease including Hepatitis B or C can worsen with use of lopinavir and ritonavir. This can be seen as worsening of transaminase elevations or hepatic decompensation. Advise patients that their liver function tests will need to be monitored closely especially during the first several months of lopinavir and ritonavir treatment and that they should notify their healthcare provider if they develop the signs and symptoms of worsening liver disease including loss of appetite, abdominal pain, jaundice, and itchy skin [see Warnings and Precautions (5.4)].
QT and PR Interval Prolongation
Advise patients that lopinavir and ritonavir may produce changes in the electrocardiogram (e.g., PR and/or QT prolongation) and to consult their healthcare provider if they experience symptoms such as dizziness, lightheadedness, abnormal heart rhythm or loss of consciousness [see Warnings and Precautions (5.5, 5.6)].
Diabetes Mellitus/Hyperglycemia
Advise patients that new onset of diabetes or exacerbation of pre-existing diabetes mellitus, and hyperglycemia have been reported during lopinavir and ritonavir use. Advise patients to notify their healthcare provider if they develop the signs and symptoms of diabetes mellitus including frequent urination, excessive thirst, extreme hunger or unusual weight loss and/or an increased blood sugar while on lopinavir and ritonavir as they may require a change in their diabetes treatment or new treatment [see Warnings and Precautions (5.7)].
Immune Reconstitution Syndrome
Advise patients that immune reconstitution syndrome has been reported in HIV-infected patients treated with combination antiretroviral therapy, including lopinavir and ritonavir [see Warnings and Precautions (5.8)].
Lipid Disorders
Advise patients that treatment with lopinavir and ritonavir therapy can result in substantial increases in the concentration of total cholesterol and triglycerides [see Warnings and Precautions (5.9)].
Fat Redistribution
Advise patients that redistribution or accumulation of body fat may occur in patients receiving antiretroviral therapy and that the cause and long term health effects of these conditions are not known at this time [see Warnings and Precautions (5.10)].
Patients with Hemophilia
Advise patients with hemophilia that they may experience increased bleeding when treated with protease inhibitors such as lopinavir and ritonavir [see Warnings and Precautions (5.11)].
Pregnancy Exposure Registry
Inform patients that there is an antiretroviral pregnancy registry that monitors fetal outcomes of pregnant women exposed to lopinavir and ritonavir [see Use in Specific Populations (8.1)].
Lactation
Instruct women with HIV-1 infection not to breastfeed because HIV-1 can be passed to the baby in breast milk [see Use in Specific Populations (8.2)].
Distributed by:
Lannett Company, Inc.Philadelphia, PA 19136
10-1133
Rev. 11/2020
MG #38379
-
MEDICATION GUIDE
Lopinavir and Ritonavir
(loe pin' a vir) (ri ton' na vir)
Oral Solution USP
What is the most important information I should know about lopinavir and ritonavir? Lopinavir and ritonavir may cause serious side effects, including:
- Interactions with other medicines. It is important to know the medicines that should not be taken with lopinavir and ritonavir. For more information, see "Who should not take lopinavir and ritonavir?”
- Side Effects in babies taking lopinavir and ritonavir oral solution. Lopinavir and ritonavir oral solution contains alcohol (ethanol) and propylene glycol. Call your healthcare provider right away if your baby appears too sleepy or their breathing changes.
- Inflammation of your pancreas (pancreatitis). Lopinavir and ritonavir can cause pancreatitis which may be serious and may lead to death. People who have high levels of a certain fat (triglycerides) have a risk for developing pancreatitis. If you have advanced HIV-1 disease, you may have an increased risk of high triglyceride levels in your blood, and pancreatitis. If you have a history of pancreatitis, you may have an increased risk of it coming back again during treatment with lopinavir and ritonavir. Tell your healthcare provider if you have any signs or symptoms of pancreatitis including:
° nausea
° vomiting
° stomach-area (abdominal) pain
- Liver problems. Liver problems, including death, can happen in people who take lopinavir and ritonavir. Your healthcare provider should do blood tests before and during your treatment with lopinavir and ritonavir to check your liver function. If you have Hepatitis B or Hepatitis C, or other liver problems, you may have an increased risk for developing new or worsening of liver problems during treatment with lopinavir and ritonavir. Tell your healthcare provider right away if you have any signs and symptoms of liver problems including:
° loss of appetite
° yellow skin and whites of eyes (jaundice)
° dark-colored urine
° pale colored stools
° itchy skin
° stomach area (abdominal) pain
- Changes in your heart rhythm and the electrical activity of your heart. These changes may be seen on an EKG (electrocardiogram) and can lead to serious heart problems. Your risk for these problems may be higher if you:
° have a history of abnormal heart rhythm or certain types of heart problems.
° take other medicines that can affect your heart rhythm during treatment with lopinavir and ritonavir.
Tell your healthcare provider right away if you have any of these symptoms:
° dizziness
° lightheadedness
° fainting
° sensation of abnormal heartbeats
See “What are the possible side effects of lopinavir and ritonavir?” for more information about serious side effects.
What is lopinavir and ritonavir? Lopinavir and ritonavir is a prescription medicine that is used with other antiretroviral medicines to treat Human Immunodeficiency Virus-1 (HIV-1) infection in adults and children 14 days of age and older. HIV is the virus that causes AIDS (Acquired Immune Deficiency Syndrome).
It is not known if lopinavir and ritonavir is safe and effective in children under 14 days old.
Who should not take lopinavir and ritonavir? Do not take lopinavir and ritonavir if you:
- are allergic to lopinavir, ritonavir, or any of the ingredients in lopinavir and ritonavir. See the end of this Medication Guide for a complete list of ingredients in lopinavir and ritonavir.
- if you take any of the following medicines:
° alfuzosin
° apalutamide
° ranolazine
° dronedarone
° colchicine, if you have kidney or liver problems.
° rifampin
° lurasidone
° pimozide
° ergot containing medicines including:
- dihydroergotamine mesylate
- ergotamine tartrate
- methylergonovine
° cisapride
° elbasvir/grazoprevir
° lovastatin
° simvastatin
° lomitapide
° sildenafil (Revatio®), when used for the treatment of pulmonary arterial hypertension
° triazolam
° midazolam when taken by mouth
° St. John’s Wort (Hypericum perforatum®)
Serious problems can happen if you or your child takes any of the medicines listed above with lopinavir and ritonavir.
Before taking lopinavir and ritonavir, tell your healthcare provider about all of your medical conditions, including if you: - have ever had a serious skin rash or an allergic reaction to medicines that contain lopinavir or ritonavir.
- have or had pancreas problems.
- have liver problems, including Hepatitis B or Hepatitis C.
- have any heart problems, including if you have a condition called Congenital Long QT Syndrome.
- have low potassium in your blood.
- have diabetes.
- have high cholesterol in your blood.
- have hemophilia. Lopinavir and ritonavir may cause increased bleeding.
- are pregnant or plan to become pregnant. It is not known if lopinavir and ritonavir will harm your unborn baby.
° Lopinavir and ritonavir oral solution contains alcohol (ethanol) and propylene glycol. You should not take lopinavir and ritonavir oral solution during pregnancy because there is no safe level of alcohol exposure during pregnancy. Tell your healthcare provider if you become pregnant during treatment with lopinavir and ritonavir.
° Lopinavir and ritonavir may reduce how well hormonal birth control works. Females who may become pregnant should use another effective form of birth control or an additional barrier method of birth control during treatment with lopinavir and ritonavir.
° Pregnancy Registry: There is a pregnancy registry for women who take antiretroviral medicines during pregnancy. The purpose of the pregnancy registry is to collect information about the health of you and your baby. Talk to your healthcare provider about how you can take part in this registry.
- are breastfeeding or plan to breastfeed. Do not breastfeed if you take lopinavir and ritonavir.
° You should not breastfeed if you have HIV-1 because of the risk of passing HIV-1 to your baby.
° Talk to your healthcare provider about the best way to feed your baby.
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. Many medicines interact with lopinavir and ritonavir. Keep a list of your medicines to show your healthcare provider and pharmacist.
You can ask your healthcare provider or pharmacist for a list of medicines that interact with lopinavir and ritonavir.
Do not start taking a new medicine without telling your healthcare provider. Your healthcare provider can tell you if it is safe to take lopinavir and ritonavir with other medicines. Your healthcare provider may need to change the dose of other medicines during treatment with lopinavir and ritonavir.
How should I take lopinavir and ritonavir? - Take lopinavir and ritonavir every day exactly as prescribed by your healthcare provider.
- Stay under the care of your healthcare provider during treatment with lopinavir and ritonavir.
- It is important to set up a dosing schedule and follow it every day.
- Do not change your treatment or stop treatment without first talking with your healthcare provider.
- Lopinavir and ritonavir oral solution must be taken with food.
- If you are taking both didanosine and lopinavir and ritonavir:
◦ Take didanosine either 1 hour before or 2 hours after taking lopinavir and ritonavir oral solution.
- If you are pregnant:
◦ Avoid use of lopinavir and ritonavir oral solution.
- If your child is prescribed lopinavir and ritonavir:
◦ Tell your healthcare provider if your child’s weight changes.
- Lopinavir and ritonavir should not be given to children on a 1 time each day dose schedule. When giving lopinavir and ritonavir to your child, give lopinavir and ritonavir exactly as prescribed.
° Use the dosing cup (supplied) or an oral syringe with mL (milliliter) markings to give the prescribed dose of lopinavir and ritonavir oral solution to your child. Your pharmacist should provide an oral syringe to you.
° Lopinavir and ritonavir oral solution contains propylene glycol and a large amount of alcohol (ethanol). Lopinavir and ritonavir oral solution should not be given to babies younger than 14 days of age unless your healthcare provider thinks it is right for your baby.
- Talk with your healthcare provider if you plan to take or give lopinavir and ritonavir oral solution through a feeding tube. Lopinavir and ritonavir oral solution contains propylene glycol and alcohol (ethanol), and should not be used with certain feeding tubes.
- You may have a greater chance of getting diarrhea if you take lopinavir and ritonavir 1 time each day than if you take it 2 times each day.
- Do not miss a dose of lopinavir and ritonavir. This could make the virus harder to treat. If you forget to take lopinavir and ritonavir, take the missed dose right away. If it is almost time for your next dose, do not take the missed dose. Instead, follow your regular dosing schedule by taking your next dose at its regular time. Do not take more than one dose of lopinavir and ritonavir at one time.
- If you or your child take more than the prescribed dose of lopinavir and ritonavir, call your healthcare provider or go to the nearest emergency room right away.
What are the possible side effects of lopinavir and ritonavir? Lopinavir and ritonavir can cause serious side effects, including:
- See “What is the most important information I should know about lopinavir and ritonavir?”
-
Diabetes and high blood sugar (hyperglycemia). You may develop new or worsening diabetes or high blood sugar during treatment with lopinavir and ritonavir. Tell your healthcare provider if you get any of the following signs or symptoms:
° urinate more often than usual
° increased hunger or thirst
° unusual weight loss
° increase in your blood sugar levels
Your healthcare provider may need to start you on medicine to treat high blood sugar or change your diabetes medicines.
- Changes in your immune system (Immune Reconstitution Syndrome) can happen when you start taking HIV-1 medicines. Your immune system may get stronger and begin to fight infections that have been hidden in your body for a long time. Call your healthcare provider right away if you start having new symptoms after starting your HIV-1 medicine.
- Increases in certain fat (triglycerides and cholesterol) levels in your blood. Large increases of triglycerides and cholesterol can be seen in blood test results of some people who take lopinavir and ritonavir. Your healthcare provider should do blood tests to check your cholesterol and triglyceride levels before you start taking lopinavir and ritonavir and during your treatment.
- Changes in body fat can happen in some people who take antiretroviral therapy. These changes may include increased amount of fat in the upper back and neck ("buffalo hump"), breast, and around the middle of your body (trunk). Loss of fat from the legs, arms and face may also happen. The exact cause and long-term health effects of these conditions are not known at this time.
- Increased bleeding in people with hemophilia. Some people with hemophilia have increased bleeding with lopinavir and ritonavir or similar medicines.
- Skin rash, which can be severe, can happen in people who take lopinavir and ritonavir. Tell your healthcare provider if you have a history of skin rash with other medicine used to treat your HIV-1 infection or if you get any skin rash during treatment with lopinavir and ritonavir.
-
Kidney stones
Common side effects of lopinavir and ritonavir include:
- diarrhea ● vomiting
- nausea ● increased fats in blood (triglycerides or cholesterol)
These are not all of the possible side effects of lopinavir and ritonavir. For more information, ask your healthcare provider or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store lopinavir and ritonavir? Lopinavir and ritonavir oral solution:
- Store lopinavir and ritonavir oral solution in a refrigerator, between 36°F to 46°F (2°C to 8°C). Lopinavir and ritonavir oral solution that is kept refrigerated may be used until the expiration date printed on the label.
- Lopinavir and ritonavir oral solution that is stored at room temperature (less than 77°F or 25°C) should be used within 2 months.
- Keep lopinavir and ritonavir away from high heat.
- Throw away any medicine that is out of date or that you no longer need.
Keep lopinavir and ritonavir and all medicines out of the reach of children.
General information about the safe and effective use of lopinavir and ritonavir. Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use lopinavir and ritonavir for a condition for which it was not prescribed. Do not give lopinavir and ritonavir to other people, even if they have the same condition you have. It may harm them.
You can ask your pharmacist or healthcare provider for information about lopinavir and ritonavir that is written for health professionals.
What are the ingredients in lopinavir and ritonavir? Active ingredients: lopinavir and ritonavir
Inactive ingredients:
Lopinavir and ritonavir oral solution: bubble gum flavor, ethanol, glycerin, high fructose corn syrup, malic acid, polyoxyl 40 hydrogenated castor oil, povidone, propylene glycol, sodium hydroxide, sucralose, and water.
Lopinavir and ritonavir oral solution contains approximately 42% ethanol (a type of alcohol) and approximately 15% propylene glycol. See “How should I take lopinavir and ritonavir?”
For more information about lopinavir and ritonavir call 1-844-834-0530.
The brands listed are trademarks of their respective owners and are not trademarks of Lannett Company, Inc. The makers of these brands are not affiliated with and do not endorse Lannett Company, Inc. or its products.
Distributed by:
Lannett Company, Inc.
Philadelphia, PA 19136
This Medication Guide has been approved by the U.S. Food and Drug Administration.
10-1146
Rev. 11/2020
MG #38380
-
INSTRUCTIONS FOR USE
Lopinavir and Ritonavir (loe pin' a vir) (ri ton' na vir)
Oral Solution USPRead this Instructions for Use before you start taking lopinavir and ritonavir oral solution and each time you get a refill. There may be new information. This leaflet does not take the place of talking to your doctor about your medical condition or treatment.
Important information about measuring lopinavir and ritonavir oral solution:
Always use the oral syringe that comes with your lopinavir and ritonavir oral solution to measure your prescribed dose. Ask your doctor or pharmacist to show you how to measure your prescribed dose.
Each lopinavir and ritonavir oral solution carton contains:
-
1 Lopinavir and Ritonavir Oral Solution bottle
-
1 Bottle adapter
-
1 Oral syringe
-
1 Prescribing Information
-
1 Medication Guide and Instructions for Use
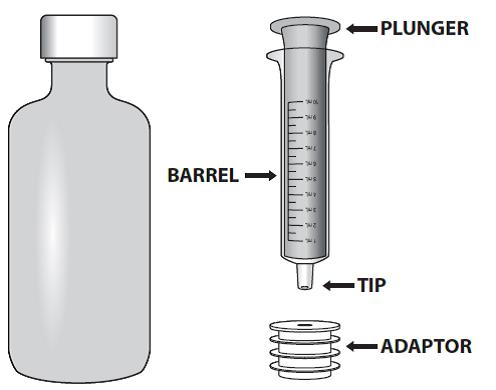
Step 1: Remove the lopinavir and ritonavir oral solution bottle, bottle adapter, and oral syringe from the carton.
Step 2: Open the bottle by pressing downward firmly on the child-resistant cap and twisting it in the direction of the arrow in the figure (counter-clockwise).
Do not throw away the child-resistant cap.
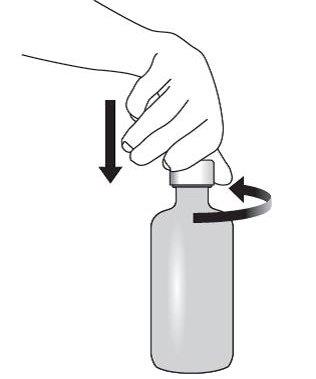
Step 3: Check the dose in milliliters (mL) as prescribed by your doctor. Find this number on the oral syringe.
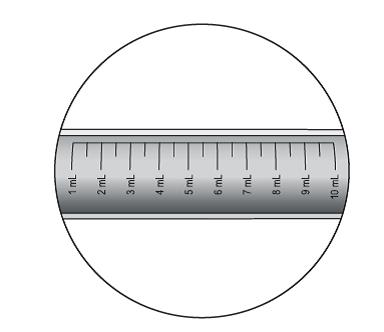
Step 4: Push the oral syringe plunger to the bottom of the barrel of the oral syringe (toward its tip) to remove excess air. 
Step 5: Remove bottle cap and insert bottle adapter into bottle opening.
Insert the oral syringe tip into the upright bottle through the opening of the bottle adapter until it is firmly in place.
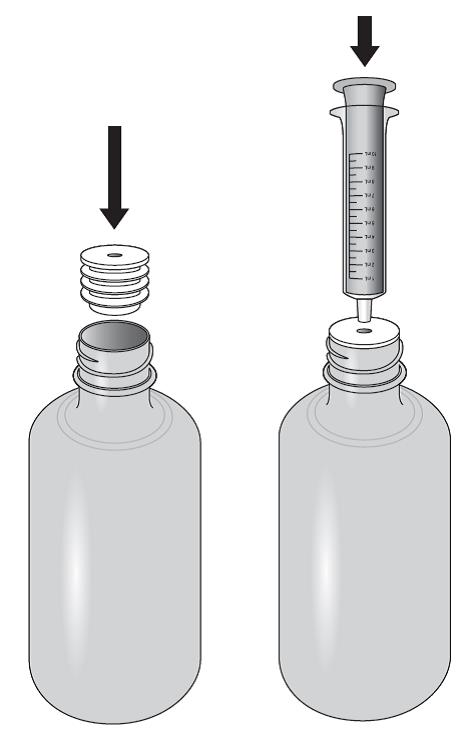
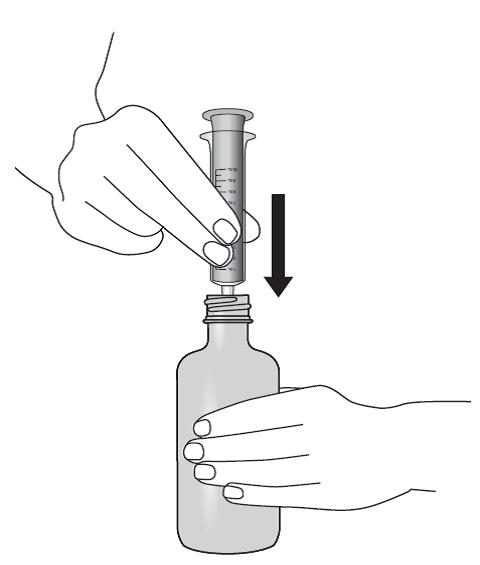
Step 6: With the oral syringe in place, turn the bottle upside down. Pull the plunger to withdraw the dose prescribed by your doctor (the amount of oral solution in Step 3).
If you see air bubbles in the oral syringe, fully push the plunger so that the oral solution flows back into the bottle. Then withdraw your prescribed dose of oral solution.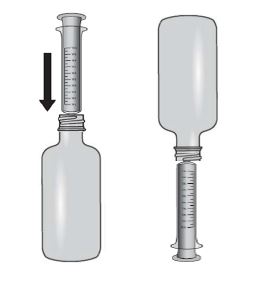
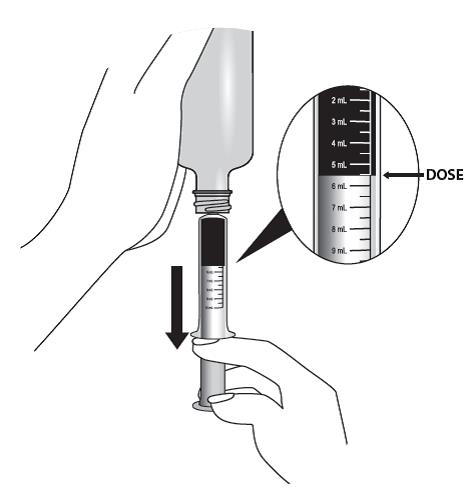
Step 7: Leave the oral syringe in the bottle adapter and turn the bottle to an upright position. 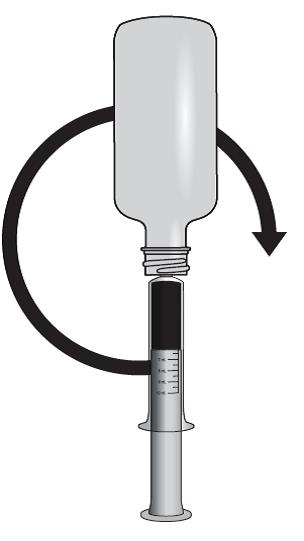
Step 8: Place the bottle on a flat surface. Remove the oral syringe from the bottle adapter and bottle by pulling straight up on the oral syringe. 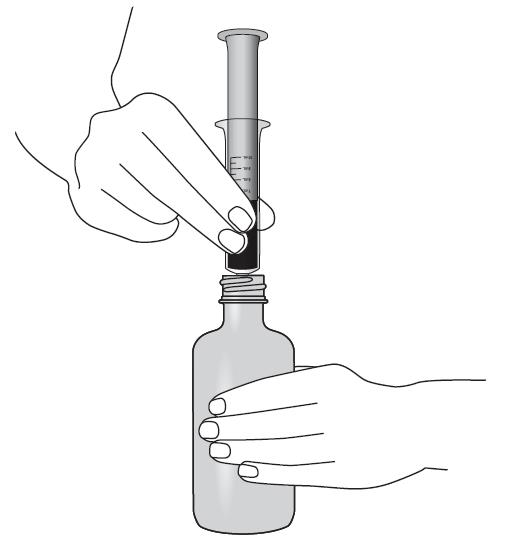
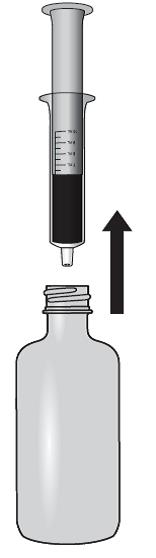
Step 9: Check that the correct dose was drawn up into the oral syringe.
Measure the dosage from the base of the plunger.
If the dose is not correct, insert the oral syringe tip firmly into the bottle adapter. Fully push in the plunger so that the oral solution flows back into the bottle.
Repeat Steps 6 through 8, if required.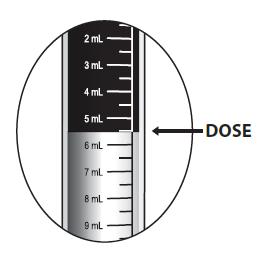
Step 10: Take the dose of lopinavir and ritonavir oral solution.
-
Swallow the lopinavir and ritonavir oral solution directly from the oral syringe.
-
Place the tip of the oral syringe in your mouth, point towards your check. Close your lips around the barrel of the oral syringe.
-
Slowly push down the oral syringe plunger until the oral syringe is empty.
Note: There may be some medicine that remains in the tip of the oral syringe. No additional action is necessary to account for residual medication remaining in the tip.
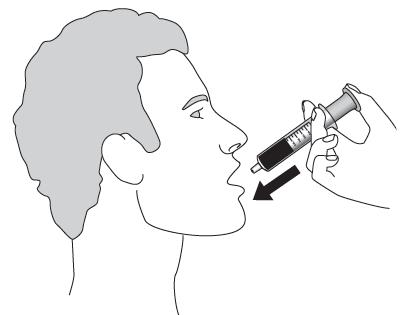
Step 11: Put the child-resistant cap back on the bottle. The cap will fit over the bottle adapter. 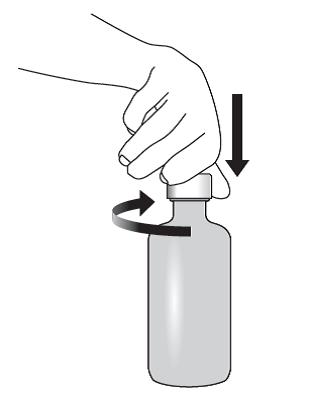
Step 12: Rinse the oral syringe with tap water after each use.
-
Remove the plunger from the oral syringe barrel.
-
Rinse the oral syringe barrel and plunger with water and let them air dry.
-
When the oral syringe barrel and plunger are dry, put the plunger back into the oral syringe barrel for the next use.
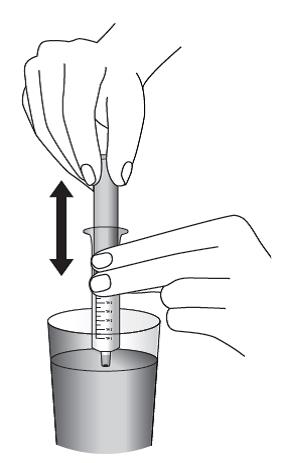
How should I store lopinavir and ritonavir oral solution?
-
Store lopinavir and ritonavir oral solution in a refrigerator, between 36°F to 46°F (2°C to 8°C). Lopinavir and ritonavir oral solution that is kept refrigerated may be used until the expiration date printed on the label.
-
Lopinavir and ritonavir oral solution that is stored at room temperature (less than 77°F or 25°C) should be used within 2 months.
-
Keep lopinavir and ritonavir oral solution away from high heat.
Throw away any medicine that is out of date or that you no longer need.
Keep lopinavir and ritonavir oral solution and all medicines out of the reach of children.
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Distributed by:
Lannett Company, Inc.
Philadelphia, PA 19136
10-1154
Rev. 11/2020
MG #38380
-
- PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
LOPINAVIR-RITONAVIR
lopinavir-ritonavir solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:0527-1947 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength LOPINAVIR (UNII: 2494G1JF75) (LOPINAVIR - UNII:2494G1JF75) LOPINAVIR 80 mg in 1 mL RITONAVIR (UNII: O3J8G9O825) (RITONAVIR - UNII:O3J8G9O825) RITONAVIR 20 mg in 1 mL Inactive Ingredients Ingredient Name Strength POLYOXYL 40 HYDROGENATED CASTOR OIL (UNII: 7YC686GQ8F) HIGH FRUCTOSE CORN SYRUP (UNII: XY6UN3QB6S) ALCOHOL (UNII: 3K9958V90M) GLYCERIN (UNII: PDC6A3C0OX) MALIC ACID (UNII: 817L1N4CKP) POVIDONE K30 (UNII: U725QWY32X) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) SODIUM HYDROXIDE (UNII: 55X04QC32I) SUCRALOSE (UNII: 96K6UQ3ZD4) WATER (UNII: 059QF0KO0R) Product Characteristics Color Score Shape Size Flavor BUBBLE GUM Imprint Code Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:0527-1947-48 1 in 1 CARTON 12/27/2016 1 160 mL in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA207407 12/27/2016 Labeler - Lannett Company, Inc. (002277481)