Label: MAGNESIUM SULFATE IN DEXTROSE- magnesium sulfate heptahydrate injection, solution

- NDC Code(s): 0264-4400-54
- Packager: B. Braun Medical Inc.
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: Abbreviated New Drug Application
Drug Label Information
Updated March 18, 2021
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use MAGNESIUM SULFATE IN 5% DEXTROSE INJECTION safely and effectively. See full prescribing information for MAGNESIUM SULFATE IN 5% DEXTROSE INJECTION.
MAGNESIUM SULFATE IN DEXTROSE injection, for intravenous use
Initial U.S. Approval: 1941INDICATIONS AND USAGE
DOSAGE AND ADMINISTRATION
- Administer via intravenous infusion pump (2.1)
- Recommended loading dosage is 4 to 6 grams over 15 minutes followed by a recommended maintenance dosage of 1 to 2 grams every hour; maximum recommended dosage is 30 to 40 grams over 24 hours (2.2)
- Obtain serum magnesium concentrations and assess clinical status to adjust the dose (2.2)
- Administration beyond 5 to 7 days is not recommended (2.2, 5.1)
- In patients with severe renal impairment and/or urine output less than 0.5 mL/kg/hour, administer a 4 gram loading dose followed by a maintenance dosage of 1 gram every hour; do not exceed the maximum recommended dosage of 20 grams over 48 hours (2.3)
- Do not administer Magnesium Sulfate in 5% Dextrose Injection with incompatible drugs through the same intravenous line, specifically with salicylates and alkali carbonates (2.4)
DOSAGE FORMS AND STRENGTHS
Supplied in premixed single-dose bags: (3)
- 0.01 grams/mL (1%) in 100 mL bag containing 1 gram of magnesium sulfate in 5% dextrose injection
WARNINGS AND PRECAUTIONS
- Fetal-neonatal toxicity with prolonged use: Administration beyond 5 to 7 days is not recommended and can lead to hypocalcemia and bone abnormalities (2.2, 5.1)
- Risk of magnesium toxicity: Monitor magnesium concentrations and clinical signs of magnesium toxicity including respiratory depression, an injectable calcium salt should be immediately available to counteract hazards, for significant toxicity stop Magnesium Sulfate in 5% Dextrose Injection (5.2)
- Risk of elevated blood glucose: Solutions containing dextrose should be used with caution in patients with known prediabetes or diabetes mellitus (5.3)
- Co-administration with unapproved tocolytics: Do not use concomitantly with beta adrenergic agents such as terbutaline and calcium channel blockers such as nifedipine (5.4)
- Aluminum toxicity: Aluminum may reach toxic concentrations with prolonged parenteral administration in patients with renal impairment (5.5)
- Exacerbation of Myasthenia Gravis: Use is contraindicated because use in patients with underlying myasthenia gravis can precipitate a myasthenic crisis (5.6)
ADVERSE REACTIONS
The most common adverse reactions are flushing, sweating, hypotension, depressed reflexes, flaccid paralysis, hypothermia, circulatory collapse, cardiac and central nervous system (CNS) depression proceeding to respiratory paralysis and hypocalcemia. Bradycardia, pulmonary edema, decreased respiratory rate, lethargy, sedation, somnolence, visual disturbances, and hypermagnesemia are also reported (6)
To report SUSPECTED ADVERSE REACTIONS, contact B. Braun Medical Inc. at 1-800-854-6851 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
- Neuromuscular blocking agents: Potentiation and prolongation of neuromuscular blockade is possible with the concomitant use of Magnesium Sulfate in 5% Dextrose Injection (7)
- Narcotics and/or propofol: Potentiation and prolongation of analgesia and CNS depression is possible with the concomitant use of Magnesium Sulfate in 5% Dextrose Injection (7)
- Dihydropyridine calcium channel blockers: An exaggerated hypotensive response is possible with the concomitant use of Magnesium Sulfate in 5% Dextrose Injection (7)
- Drugs that may induce magnesium loss with concomitant use of Magnesium Sulfate in 5% Dextrose Injection: Alcohol, aminoglycosides, amphotericin B, cisplatin, cyclosporine, digitalis, loop diuretics, and thiazide diuretics (7)
USE IN SPECIFIC POPULATIONS
Patients with severe renal impairment and/or a urine output less than 100 mL every 4 hours are at greater risk for increased magnesium concentrations that may lead to toxicity (8.6)
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 3/2021
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Important Administration Instructions
2.2 Recommended Dosage
2.3 Dosage in Patients with Severe Renal Impairment and/or Oliguria
2.4 Drug Incompatibilities
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Fetal-Neonatal Toxicity with Prolonged Use
5.2 Risk of Magnesium Toxicity
5.3 Risk of Elevated Blood Glucose
5.4 Co-administration with Unapproved Tocolytics
5.5 Aluminum Toxicity
5.6 Exacerbation of Myasthenia Gravis
6 ADVERSE REACTIONS
7 DRUG INTERACTIONS
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.6 Renal Impairment
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
- 1 INDICATIONS AND USAGE
-
2 DOSAGE AND ADMINISTRATION
2.1 Important Administration Instructions
Magnesium Sulfate in 5% Dextrose Injection is:
- A clear solution. Visually inspect Magnesium Sulfate in 5% Dextrose Injection for particulate matter and discoloration prior to administration. Do not administer unless solution is clear and colorless to slightly yellow.
- For intravenous use only
- Administered via intravenous infusion pump
Magnesium Sulfate in 5% Dextrose Injection does not require dilution prior to intravenous administration.
Check for minute leaks by squeezing the container fully. Do not administer Magnesium Sulfate in 5% Dextrose Injection if there is a leak [see Description (11)].
Do not administer Magnesium Sulfate in 5% Dextrose Injection with incompatible drugs through the same intravenous line [see Dosage and Administration (2.4)]. Do not use Magnesium Sulfate in 5% Dextrose Injection in series connections.
2.2 Recommended Dosage
- The recommended loading dosage of Magnesium Sulfate in 5% Dextrose Injection in patients with eclampsia or preeclampsia is 4 to 6 grams over 15 minutes followed by a recommended maintenance dosage of 1 to 2 grams every hour.
- Obtain serum magnesium concentrations and assess clinical status to adjust the dosage.
- In patients with eclampsia, consider targeting the maintenance dosage to achieve serum magnesium concentrations of 3 to 6 mg per 100 mL (2.5 to 5 mEq per liter). For patients with recurrent eclampsia, consider giving an additional 2 gram intravenous bolus.
- For patients with eclampsia, therapy should continue until seizures cease.
- The maximum recommended dosage is 30 to 40 grams of magnesium sulfate over 24 hours.
- Administration of Magnesium Sulfate in 5% Dextrose Injection beyond 5 to 7 days is not recommended [see Warnings and Precautions (5.1)].
2.3 Dosage in Patients with Severe Renal Impairment and/or Oliguria
- In patients with severe renal impairment and/or a urine output less than 0.5 mL/kg/hour, initiate Magnesium Sulfate in 5% Dextrose Injection with a 4 gram loading dose followed by a maintenance dosage of 1 gram every hour.
- Titrate the magnesium sulfate maintenance dosage to maintain concentrations in the target range through frequent monitoring of magnesium concentrations and observation for clinical signs of magnesium toxicity (e.g., facial edema, diminished strength of deep tendon reflexes, respiratory depression). A lower maintenance dosage requirement is likely in these patients.
- Do not exceed the maximum recommended dosage of 20 grams of Magnesium Sulfate in 5% Dextrose Injection over 48 hours.
2.4 Drug Incompatibilities
Magnesium Sulfate in 5% Dextrose Injection is not compatible with administration of a variety of solutions and forms precipitates of magnesium salts. Before using Magnesium Sulfate in 5% Dextrose Injection with another parenteral product, investigate potential incompatibilities. Incompatible products that should not be coadministered include salicylates and alkali carbonates.
-
3 DOSAGE FORMS AND STRENGTHS
Magnesium Sulfate in 5% Dextrose Injection, USP is a clear and colorless to slightly yellow solution supplied in single-dose bags:
- 0.01 grams per mL (1%):
- 100 mL bag containing 1 gram of magnesium sulfate in 5% dextrose injection
Each 100 mL contains 5 grams of hydrous dextrose in Water for Injection.
- 0.01 grams per mL (1%):
-
4 CONTRAINDICATIONS
Magnesium Sulfate in 5% Dextrose Injection is contraindicated in patients:
- with heart block or myocardial damage
- in diabetic coma
- with myasthenia gravis [see Warnings and Precautions (5.6)]
-
5 WARNINGS AND PRECAUTIONS
5.1 Fetal-Neonatal Toxicity with Prolonged Use
Continuous administration of magnesium sulfate beyond 5 to 7 days in pregnant women can lead to hypocalcemia and bone abnormalities in the developing fetus, including skeletal demineralization and osteopenia. In addition, cases of neonatal fracture have been reported.
Neonates of women receiving Magnesium Sulfate in 5% Dextrose Injection (especially with prolonged maternal use) are at risk for magnesium toxicity including hyporeflexia, hypotonia, and respiratory depression. There is one reported case of neonatal death as the result of magnesium toxicity after transplacental exposure.
The shortest duration of magnesium sulfate treatment that can lead to fetal harm is not known. Administration of Magnesium Sulfate in 5% Dextrose Injection beyond 5 to 7 days is not recommended.
5.2 Risk of Magnesium Toxicity
Patients receiving Magnesium Sulfate in 5% Dextrose Injection are at risk for magnesium toxicity including respiratory depression, acute renal failure and rarely, pulmonary edema.
Monitor clinical signs of magnesium toxicity (for example, facial edema, diminished strength of deep tendon reflexes, respiratory depression) and magnesium concentrations during infusions of Magnesium Sulfate in 5% Dextrose Injection. Clinical indications of a safe dosage regimen include the presence of the patellar reflex (knee jerk) and absence of respiratory depression (approximately 16 breaths or more per minute). Serum magnesium concentrations usually sufficient to control convulsions range from 3 to 6 mg per 100 mL (2.5 to 5 mEq per liter). The strength of the deep tendon reflexes begins to diminish when serum magnesium concentrations exceed 4 mEq per liter. Reflexes may be absent at concentration of 10 mEq per liter, at which point respiratory paralysis is a potential hazard. An injectable calcium salt should be immediately available to counteract the potential hazards of magnesium toxicity in patients with preeclampsia and eclampsia. If there is significant magnesium toxicity, stop the Magnesium Sulfate in 5% Dextrose Injection infusion and recheck serum magnesium concentration.
Patients with renal impairment are at greater risk of magnesium toxicity because magnesium is excreted by the body solely by the kidneys [see Use in Specific Populations (8.6)]. Urine output should be maintained at a level of 100 mL per 4 hours. Monitoring serum magnesium levels and the patient's clinical status is essential to avoid the consequences of overdosage in patients with preeclampsia. Discontinuation of the magnesium infusion is recommended when urine output is less than 100 mL every 4 hours to avoid magnesium toxicity, especially if serum creatinine is increasing progressively.
5.3 Risk of Elevated Blood Glucose
Solutions containing dextrose should be used with caution in patients with known prediabetes or diabetes mellitus given the risk of elevated blood glucose.
5.4 Co-administration with Unapproved Tocolytics
Do not use Magnesium Sulfate in 5% Dextrose Injection with unapproved tocolytics (e.g., beta adrenergic agents such as terbutaline, or with calcium channel blockers such as nifedipine). Serious adverse events including pulmonary edema and hypotension have occurred [see Drug Interactions (7)].
5.5 Aluminum Toxicity
Magnesium Sulfate in 5% Dextrose Injection contains aluminum that may be toxic (Magnesium Sulfate in 5% Dextrose Injection contains less than 25 mcg/L of aluminum). Aluminum may reach toxic concentrations with prolonged parenteral administration in patients with renal impairment.
Patients with renal impairment who receive parenteral concentrations of aluminum at greater than 4 to 5 mcg/kg/day, accumulate aluminum at concentrations associated with central nervous system and bone toxicity. Tissue loading may occur at even lower rates of administration.
5.6 Exacerbation of Myasthenia Gravis
Magnesium Sulfate in 5% Dextrose Injection is contraindicated in patients with known myasthenia gravis.
Use of magnesium sulfate in patients with underlying myasthenia gravis can precipitate a myasthenic crisis. Myasthenic crisis is a life-threatening condition characterized by neuromuscular respiratory failure. Symptoms of myasthenic crisis may include difficulty swallowing, ptosis, facial droop, weakness and/or difficulty breathing that may require intubation.
If myasthenic crisis is suspected, discontinue use of Magnesium Sulfate in 5% Dextrose Injection immediately. Secure the patient's airway. Consider intensive care unit admission and elective intubation, if respiratory failure is anticipated. Once the airway is secure, confirm the diagnosis. Therapies include plasmapheresis and plasma exchange or intravenous immunoglobulin (IVIG) and immunomodulating therapy in addition to high-dose glucocorticoids.
-
6 ADVERSE REACTIONS
The following adverse reactions have been identified in clinical studies or postmarketing reports. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Cardiovascular:
hypotension, circulatory collapse, cardiac depression including bradycardia Central Nervous System:
central nervous system depression leading to respiratory paralysis, visual disturbances, flushing, sweating, hypothermia Metabolic: hypocalcemia with signs of tetany, hypermagnesemia Neurologic:
lethargy, sedation, somnolence, myasthenic crisis Neuromuscular:
depressed deep tendon reflexes, flaccid paralysis Pulmonary:
decreased respiratory rate, pulmonary edema -
7 DRUG INTERACTIONS
Table 1 presents the potential clinical impact of medications that may be commonly administered concomitantly with Magnesium Sulfate in 5% Dextrose Injection in the clinical setting.
Table 1: Potential Clinically Significant Drug Interactions with Magnesium Sulfate in 5% Dextrose Injection* - *
- For drug incompatibility information [see Dosage and Administration (2.4)].
Neuromuscular Blocking Agents Clinical Impact: - Potentiation and prolongation of neuromuscular blockade is possible with the concomitant use of magnesium sulfate and neuromuscular blocking agents [see Clinical Pharmacology (12.2)].
- The underlying mechanism of this interaction may involve suppression of peripheral neuromuscular function by decreasing acetylcholine release, reduction of endplate sensitivity, and decreased muscle fiber excitability with magnesium sulfate therapy.
Intervention: - Monitor respiration and the depth of neuromuscular blockade frequently (e.g., train-of-four monitoring) when a neuromuscular blocking agent is used concomitantly with Magnesium Sulfate in 5% Dextrose Injection.
- Adjust the dosage of the neuromuscular blocking agent accordingly to maintain the desired level of musculoskeletal activity. The amount of reversal agent(s) required to achieve adequate reversal of the neuromuscular blocking agent(s) may also be increased.
Examples: - Depolarizing neuromuscular blockers: succinylcholine
- Non-depolarizing neuromuscular blockers: atracurium, cisatracurium, pancuronium, rocuronium, vecuronium
Narcotics and/or Propofol Clinical Impact: - Potentiation and prolongation of analgesia and CNS depression is possible with the concomitant use of Magnesium Sulfate in 5% Dextrose Injection with narcotics and/or propofol. The potential for magnesium sulfate to affect other CNS depressants is unknown [see Clinical Pharmacology (12.2)].
- The underlying mechanism of this interaction may involve antagonism of N-methyl-D-aspartate (NMDA) by magnesium sulfate therapy.
Intervention: - Monitor the depth of CNS depression frequently using a reliable instrument.
- Adjust the narcotic and/or propofol dosage accordingly to maintain the desired level of analgesia and sedation.
Examples: - Narcotics and propofol
Dihydropyridine Calcium Channel Blockers Clinical Impact: - An exaggerated hypotensive response is possible with the concomitant use of Magnesium Sulfate in 5% Dextrose Injection with dihydropyridine calcium channel blockers. The potential for magnesium sulfate to affect other calcium channel blockers (e.g., diltiazem and verapamil) is unknown [see Clinical Pharmacology (12.2)].
Intervention: - Monitor vital signs (heart rate, blood pressure, respiration) frequently.
- Supportive care and/or discontinuation of the calcium channel blocker may be required.
Examples: - Amlodipine, clevidipine, felodipine, isradipine, nicardipine, nifedipine, nimodipine, and nisoldipine
Drugs that May Induce Magnesium Loss Clinical Impact: - Reduced magnesium concentrations may impact efficacy
Intervention: - Monitor magnesium concentrations frequently and adjust the Magnesium Sulfate in 5% Dextrose Injection dosage to maintain concentrations in the target range [see Dosage and Administration (2)].
Examples: - Alcohol, aminoglycosides, amphotericin B, cisplatin, cyclosporine, digitalis, loop diuretics, thiazide diuretics
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Magnesium Sulfate in 5% Dextrose Injection is indicated in pregnant women for the prevention of eclampsia in women with preeclampsia and the treatment of seizures and prevention of recurrent seizures in women with eclampsia. Fetal, neonatal, and maternal risks are discussed throughout the labeling.
Clinical Considerations
Labor or Delivery:
Magnesium Sulfate in 5% Dextrose Injection is not approved for the treatment of pre-term labor.
Administration of Magnesium Sulfate in 5% Dextrose Injection to pregnant women longer than 5 to 7 days may lead to hypocalcemia and bone abnormalities in the developing fetus, including skeletal demineralization and osteopenia [see Warnings and Precautions (5.1)].
8.2 Lactation
The use of intravenous magnesium in pregnant women increases human milk magnesium concentrations only slightly and oral absorption of magnesium by the infant is poor. The effect of intravenous magnesium on milk production is unknown. The developmental and health benefits to the neonate of breastfeeding should be considered along with the mother's clinical need for Magnesium Sulfate in 5% Dextrose Injection and any potential adverse effects on the breastfed infant from Magnesium Sulfate in 5% Dextrose Injection or from the underlying maternal condition.
8.4 Pediatric Use
The safety and effectiveness of Magnesium Sulfate in 5% Dextrose Injection have been established for the prevention of eclampsia in adolescents with preeclampsia and the treatment of seizures and prevention of recurrent seizures in adolescents with eclampsia. Dosing recommendation in pregnant adolescent patients are the same as for pregnant adult patients [see Dosage and Administration (2.2)].
8.6 Renal Impairment
Magnesium is excreted solely by the kidneys. Patients with severe renal impairment (urine output less than 100 mL per 4 hours) are at greater risk for increased magnesium concentrations that may lead to magnesium toxicity [see Warnings and Precautions (5.2) and Clinical Pharmacology (12.3)]. In patients with severe renal impairment, dosage reduction is recommended and the maximum recommended dosage is lower than patients with normal renal function [see Dosage and Administration (2.3)].
-
10 OVERDOSAGE
Manifestations of magnesium toxicity include a drop in blood pressure, difficulty breathing, and disappearance of the patellar reflex. As serum magnesium rises above 4 mEq per liter, the deep tendon reflexes decrease. As the serum magnesium level approaches 10 mEq per liter, the tendon reflexes disappear and respiratory paralysis may occur [see Warnings and Precautions (5.2)]. Other signs and symptoms of magnesium overdosage include flushing, sweating, hypotension, weakness, hypothermia, circulatory collapse, cardiac and central nervous system depression proceeding to respiratory paralysis, cardiac arrest, and prolongation of PR and QRS intervals. Patients with renal impairment and underlying neuromuscular diseases such as myasthenia gravis may experience magnesium intoxication at lower magnesium concentrations (Magnesium Sulfate in 5% Dextrose Injection is contraindicated in patients with myasthenia gravis).
If patient is experiencing magnesium toxicity, immediately discontinue Magnesium Sulfate in 5% Dextrose Injection. Artificial respiration may be required. Administer an injectable calcium salt to counteract the potential hazards of magnesium toxicity [see Warnings and Precautions (5.2)].
Hypermagnesemia in the newborn (after administration of Magnesium Sulfate in 5% Dextrose Injection to the mother) may require resuscitation and assisted ventilation via endotracheal intubation or intermittent positive pressure ventilation as well as intravenous calcium.
-
11 DESCRIPTION
Magnesium Sulfate in 5% Dextrose Injection, USP is a sterile, nonpyrogenic solution of magnesium sulfate heptahydrate and dextrose in water for injection for intravenous use. Each 100 mL contains 1 gram of magnesium sulfate heptahydrate and dextrose, hydrous 5 grams in water for injection [see How Supplied/Storage and Handling (16)]. Magnesium Sulfate in 5% Dextrose Injection, USP may contain sulfuric acid and/or sodium hydroxide for pH adjustment. The pH is 4.5 (3.5 to 6.5).
Magnesium Sulfate, USP heptahydrate is chemically known as sulfuric acid magnesium salt (1:1), heptahydrate and chemically designated MgSO4 ∙ 7H2O, with a molecular weight of 246.47. It occurs as colorless crystals or white powder freely soluble in water.
Dextrose, USP is chemically designated D-glucose, monohydrate, a hexose sugar freely soluble in water. The molecular formula is C6H12O6 ∙ H2O and the molecular weight is 198.17. It has the following structural formula:
Water for Injection, USP is chemically designated H2O.
Not made with natural rubber latex, DEHP or PVC.
The plastic container is a copolymer of ethylene and propylene formulated and developed for parenteral drugs. The copolymer contains no plasticizers. The safety of the plastic container has been confirmed by biological evaluation procedures. The material passes Class Vl testing as specified in the U.S. Pharmacopeia for Biological Tests — Plastic Containers.
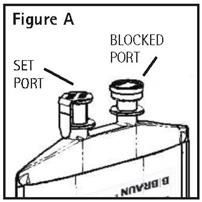
The container/solution unit is a closed system and is not dependent upon entry of external air during administration. The container has two ports, one is for the intravenous administration set covered by a tamper proof barrier and the other is a blocked port. Refer to the directions for use of the container to properly identify the ports [see How Supplied/Storage and handling (16)].
No vapor barrier is necessary.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Magnesium prevents seizures in patients with preeclampsia and controls seizures in patients with eclampsia by blocking neuromuscular transmission and decreasing the amount of acetylcholine liberated at the end plate by the motor nerve impulse. Magnesium has a depressant effect on the central nervous system [see Drug Interactions (7)]. Magnesium acts peripherally to produce vasodilation.
12.2 Pharmacodynamics
With intravenous administration of magnesium sulfate the onset of anticonvulsant action is immediate and lasts about 30 minutes. The estimated magnesium concentration (above baseline) required to elicit half-maximum effect (EC50) on systolic and diastolic blood pressure in pregnant women with preeclampsia that received intravenous magnesium sulfate therapy was reported to be 1.5 and 1.8 mEq per liter (1.9 and 2.2 mg per dL), respectively, in a published study. Effective anticonvulsant serum concentrations range from 2.5 to 7.5 mEq per liter.
Drug Interaction Studies
The following information is based upon published case reports and clinical studies that could not be confirmed by an adequately controlled study, but still warrant consideration given the potential risks involved [see Drug Interactions (7)].
Neuromuscular Blocking Agents:
Potentiation and prolongation of neuromuscular blockade requiring modification of the neuromuscular blocking agent dosage and/or increased reversal agent requirements were reported in preeclamptic women who received magnesium sulfate treatment who underwent subsequent surgery (for example, caesarian section) with anesthesia that included either a depolarizing (d-tubocurarine, succinylcholine) or nondepolarizing neuromuscular blocking agent (vecuronium, rocuronium).
Narcotics and/or Propofol:
Potentiation and prolongation of analgesic and/or sedative effects as well as a reduced requirement for an intravenous narcotic (fentanyl, sufentanil, tramadol), intrathecal narcotic (fentanyl), and/or intravenous propofol was reported in magnesium sulfate treated patients who required surgery or intensive care that also included narcotic and/or propofol therapy.
Dihydropyridine Calcium Channel Blockers:
An exaggerated hypotensive response (blood pressure 80–93/49–60 mm Hg) was reported in preeclamptic women who received oral nifedipine in addition to magnesium sulfate treatment. Blood pressure returned to previous levels within approximately 30 minutes with supportive care.
12.3 Pharmacokinetics
Distribution
Approximately 1 to 2% of total body magnesium is located in the extracellular fluid space. Magnesium is 30% bound to albumin.
Elimination
The average half-life and systemic clearance of magnesium sulfate in preeclamptic women is approximately 4 to 5 hours and 4 to 5 liters per hour, respectively.
Specific Populations
Patients with Renal Impairment:
Plasma magnesium concentrations of 7 to 12.3 mEq per liter (8.6 to 15.1 mg per dL) were reported in preeclamptic women with a urine output less than 100 mL per 4 hours that received 20 grams of magnesium sulfate intravenously over 2 to 8 hours in a published study [see Dosage and Administration (2.3) and Use in Specific Populations (8.6)].
- 13 NONCLINICAL TOXICOLOGY
-
16 HOW SUPPLIED/STORAGE AND HANDLING
Magnesium Sulfate in 5% Dextrose Injection, USP is a clear solution supplied in single-dose 100 mL fill PAB® containers packaged 24 per case (see Table 2).
PAB is a registered trademark of B. Braun Medical Inc.
Table 2: How Supplied Information Magnesium Sulfate* Concentration NDC Number REF: Container Size† Total Magnesium Sulfate* Total Magnesium Ion Magnesium Ion Concentration Osmolarity‡ 0.01 grams/mL (1%) 0264-4400-54 D4400-54
100 mL 1 gram 8.1 mEq 8.1 mEq/100 mL 333 mOsmol/liter Storage
Store at 20° to 25°C (68° to 77°F); excursions permitted between 15° to 30°C (59° to 86°F). [See USP Controlled Room Temperature.] Protect from freezing.
Handling
Directions For Use of PAB® Container
CAUTION: DO NOT ADD SUPPLEMENTARY MEDICATION. WHENEVER POSSIBLE USE CENTRAL ROUTE.
Aseptic technique is required.
Before use, perform the following checks: Read the label. Ensure solution is the one ordered and is within the expiration date.
Inspect the solution in good light for cloudiness, haze or particulate matter; check the container for leakage or damage. Any container which is suspect should not be used.
Use only if solution is clear and container and seals are intact. Single dose plastic container. Discard unused portion. Consult Package Insert for complete product information.
WARNING: DO NOT USE PLASTIC CONTAINER IN SERIES CONNECTION.
This solution is intended for intravenous administration using sterile equipment. It is recommended that intravenous administration apparatus be replaced at least once every 24 hours.
1. Identify Two Ports (See Figure A).
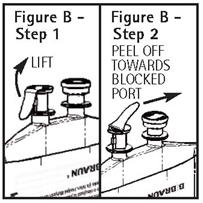
2. To Attach Administration Set
To aseptically remove the set port closure: hold container below the set port and grasp the foil tab between the thumb and forefinger then pull the tab in two steps as shown in Figure B Steps 1 and 2.
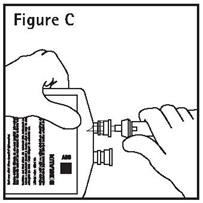
3. Push spike through the diaphragm of the port (See Figure C). Hang container using hole on the lower flap. Prime set in accordance with the Directions for Use provided with the set in use.
PAB® containers can be safely transported in a standard 6-inch carrier through a pneumatic tube system that is well maintained and running properly.
-
17 PATIENT COUNSELING INFORMATION
Magnesium Sulfate in 5% Dextrose Injection is typically administered to pregnancy women in emergent situations. When feasible, advise the patient and family of the following:
Fetal-Neonatal Toxicity Reported With Prolonged Use
Continuous administration of Magnesium Sulfate in 5% Dextrose Injection in pregnant women beyond 5 to 7 days can lead to hypocalcemia and bone abnormalities in the developing fetus, including skeletal demineralization and osteopenia. In addition, cases of neonatal fracture have been reported [see Warnings and Precautions (5.1)].
Risk of Magnesium Toxicity
Pregnant women receiving Magnesium Sulfate in 5% Dextrose Injection are at risk for magnesium toxicity, including facial edema, diminished strength of deep tendon reflexes, and respiratory depression [see Warnings and Precautions (5.2)].
- SPL UNCLASSIFIED SECTION
-
PRINCIPAL DISPLAY PANEL - 100 mL Bag Label
NDC 0264-4400-54
Magnesium Sulfate in
5% Dextrose Injection, USP1 g/100 mL (10 mg/mL)
(0.081 mEq Mg++/mL)
1g
Total100 mL PAB® Container
Each 100 mL contains Magnesium Sulfate Heptahydrate 1 g
(equivalent to 8.1 mEq Magnesium) and Dextrose, Hydrous 5 g in
Water for Injection. May contain Sulfuric Acid and/or Sodium
Hydroxide for pH adjustment.pH 4.5 (3.5 to 6.5); 333 mOsmol/liter (Calc.)
Single dose container. Discard unused portion. For Intravenous
Use Only. Usual dosage: See prescribing information.
Sterile, nonpyrogenic. Use only if solution is clear and container
is undamaged. Must not be used in series connections.CAUTION: DO NOT ADD SUPPLEMENTARY MEDICATION.
WHENEVER POSSIBLE USE CENTRAL ROUTE.Store at 20° to 25°C (68° to 77°F); excursions permitted between
15° to 30°C (59° to 86°F). [See USP Controlled Room Temperature.]
Protect from freezing.REF D4400-54
Not made with natural
rubber latex, DEHP or PVC.Rx only
B. Braun Medical Inc.
Bethlehem, PA 18018-3524 USA
1-800-227-2862Y94-003-431 LD-473-2
LOT
EXP
-
INGREDIENTS AND APPEARANCE
MAGNESIUM SULFATE IN DEXTROSE
magnesium sulfate heptahydrate injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:0264-4400 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength MAGNESIUM SULFATE HEPTAHYDRATE (UNII: SK47B8698T) (MAGNESIUM CATION - UNII:T6V3LHY838) MAGNESIUM SULFATE HEPTAHYDRATE 10 mg in 1 mL Inactive Ingredients Ingredient Name Strength SULFURIC ACID (UNII: O40UQP6WCF) SODIUM HYDROXIDE (UNII: 55X04QC32I) DEXTROSE MONOHYDRATE (UNII: LX22YL083G) WATER (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:0264-4400-54 24 in 1 CASE 10/27/2020 1 100 mL in 1 CONTAINER; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA207966 10/27/2020 Labeler - B. Braun Medical Inc. (002397347)