Label: HEMATOPOIETIC PROGENITOR CELLS, CORD BLOOD- human cord blood hematopoietic progenitor cell solution



- ISBT Code(s): W2263-S1393-02
- Packager: University of Texas MD Anderson Cancer Center
- Category: LICENSED MINIMALLY MANIPULATED CELLS LABEL
Drug Label Information
Updated June 26, 2018
If you are a healthcare professional or from the pharmaceutical industry please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use HPC, Cord Blood safely and effectively. See full prescribing information for HPC, Cord Blood.
HPC, Cord Blood
Injectable Suspension for Intravenous Use
Initial U.S. Approval: 2018WARNING: FATAL INFUSION REACTIONS, GRAFT VERSUS HOST DISEASE, ENGRAFTMENT SYNDROME, AND GRAFT FAILURE
See full prescribing information for complete boxed warning.
- Fatal infusion reactions: Monitor patients during infusion and discontinue for severe reactions. (5.1, 5.2)
- Graft-versus-Host disease (GVHD): GVHD may be fatal. Administration of immunosuppressive therapy may decrease the risk of GVHD. (5.3)
- Engraftment syndrome: Engraftment syndrome may be fatal. Treat engraftment syndrome promptly with corticosteroids. (5.4)
- Graft failure: Graft failure may be fatal. Monitor patients for laboratory evidence of hematopoietic recovery. (5.5)
INDICATIONS AND USAGE
Hematopoietic Progenitor Cell (HPC), Cord Blood, is an allogeneic cord blood hematopoietic progenitor cell therapy indicated for use in unrelated donor hematopoietic progenitor cell transplantation procedures in conjunction with an appropriate preparative regimen for hematopoietic and immunologic reconstitution in patients with disorders affecting the hematopoietic system that are inherited, acquired, or result from myeloablative treatment. (1)
The benefit-risk assessment for an individual patient depends on the patient characteristics, including disease, stage, risk factors, and specific manifestations of the disease, on characteristics of the graft, and on other available treatments or types of hematopoietic progenitor cells. (1)
DOSAGE AND ADMINISTRATION
- For intravenous use only.
- Do not irradiate.
- Unit selection and administration of HPC, Cord Blood should be done under the direction of a physician experienced in hematopoietic progenitor cell transplantation. (2)
- The recommended minimum dose is 2.5 x 107 nucleated cells/kg at cryopreservation. (2.1)
- Do not administer HPC, Cord Blood through the same tubing with other products except for normal saline. (2.3)
DOSAGE FORMS AND STRENGTHS
Each unit contains a minimum of 9 x 108 total nucleated cells with at least 1.25 x 106 viable CD34+ cells at the time of cryopreservation. The exact pre- cryopreservation nucleated cell content of each unit is provided on the container label and accompanying records. (3)
CONTRAINDICATIONS
None. (4)
WARNINGS AND PRECAUTIONS
ADVERSE REACTIONS
Mortality, from all causes, at 100 days post-transplant was 25%. (5, 6.1)
The most common infusion-related adverse reactions (≥5%) are hypertension, vomiting, nausea, bradycardia, and fever. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact the MD Anderson Cord Blood Bank, The University of Texas MD Anderson Cancer Center, at 1-713-563-8000 and FDA at 1-800-FDA-1088 or https://www.fda.gov/Safety/MedWatch.
USE IN SPECIFIC POPULATIONS
- Pregnancy: Based on animal data, may cause fetal harm. Use only if clearly needed. (8.1)
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 8/2018
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: FATAL INFUSION REACTIONS, GRAFT VERSUS HOST DISEASE,
ENGRAFTMENT SYNDROME, AND GRAFT FAILURE
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Dosing
2.2 Preparation for Infusion
2.3 Administration
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity Reactions
5.2 Infusion Reactions
5.3 Graft-versus-Host Disease
5.4 Engraftment Syndrome
5.5 Graft Failure
5.6 Malignancies of Donor Origin
5.7 Transmission of Serious Infections
5.8 Transmission of Rare Genetic Diseases
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Renal Disease
10 OVERDOSAGE
10.1 Human Overdosage Experience
10.2 Management of Overdose
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
14 CLINICAL STUDIES
15 REFERENCES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
INSTRUCTIONS FOR PREPARATION FOR INFUSION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
BOXED WARNING
(What is this?)
WARNING: FATAL INFUSION REACTIONS, GRAFT VERSUS HOST DISEASE,
ENGRAFTMENT SYNDROME, AND GRAFT FAILURE
Fatal infusion reactions: HPC, Cord Blood administration can result in serious, including fatal, infusion reactions. Monitor patients and discontinue HPC, Cord Blood infusion for severe reactions. [See Warnings and Precautions (5.1, 5.2)]
Graft-versus-Host disease (GVHD): GVHD is expected after administration of HPC, Cord Blood, and may be fatal. Administration of immunosuppressive therapy may decrease the risk of GVHD. [See Warnings and Precautions (5.3)]
Engraftment syndrome: Engraftment syndrome may progress to multi-organ failure and death. Treat engraftment syndrome promptly with corticosteroids. [See Warnings and Precautions (5.4)]
Graft failure: Graft failure may be fatal. Monitor patients for laboratory evidence of hematopoietic recovery. Prior to choosing a specific unit of HPC, Cord Blood, consider testing for HLA antibodies to identify patients who are alloimmunized. [See Warnings and Precautions (5.5)]
-
1 INDICATIONS AND USAGE
Hematopoietic Progenitor Cell (HPC), Cord Blood, is an allogeneic cord blood hematopoietic progenitor cell therapy indicated for use in unrelated donor hematopoietic progenitor stem cell transplantation procedures in conjunction with an appropriate preparative regimen for hematopoietic and immunologic reconstitution in patients with disorders affecting the hematopoietic system that are inherited, acquired, or result from myeloablative treatment.
The benefit-risk assessment for an individual patient depends on the patient characteristics, including disease, stage, risk factors, and specific manifestations of the disease, on characteristics of the graft, and on other available treatments or types of hematopoietic progenitor cells.
-
2 DOSAGE AND ADMINISTRATION
For intravenous use only.
Do not irradiate.Unit selection and administration of HPC, Cord Blood should be done under the direction of a physician experienced in hematopoietic progenitor cell transplantation.
2.1 Dosing
The recommended minimum dose is 2.5 x 107 total nucleated cells/kg at cryopreservation. Multiple units may be required in order to achieve the appropriate dose.
Matching for at least 4 of 6 HLA-A antigens, HLA-B antigens, and HLA-DRB1 alleles is recommended. The HLA typing and nucleated cell content for each individual unit of HPC, Cord Blood are documented on the container label and/or in accompanying records.
2.2 Preparation for Infusion
HPC, Cord Blood should be prepared by a trained healthcare professional.
- Do not irradiate HPC, Cord Blood.
- See the appended detailed instructions for preparation of HPC, Cord Blood for infusion.
- Once prepared for infusion, HPC, Cord Blood may be stored at 4 to 8 °C for up to 30 minutes if product is thawed and DMSO is not removed, or at 4 to 8 °C for up to 4 hours if DMSO is removed in a washing procedure [see Instructions for Preparation for Infusion]. No data are available for the stability of HPC, Cord Blood if DMSO is not removed.
- The recommended limit on DMSO administration is 1 gram per kg body weight per day. [See Warnings and Precautions (5.2) and Overdosage (10)]
2.3 Administration
HPC, Cord Blood should be administered under the supervision of a qualified healthcare professional experienced in hematopoietic progenitor cell transplantation.
- Confirm the identity of the patient for the specified unit of HPC, Cord Blood prior to administration.
- Confirm that emergency medications are available for use in the immediate area.
- Ensure the patient is hydrated adequately.
- Premedicate the patient 30 to 60 minutes before the administration of HPC, Cord Blood. Premedication can include all of the following: antipyretics, histamine antagonists, and corticosteroids.
- Inspect the product for any abnormalities, such as particulates, and for breaches of container integrity prior to administration. Prior to infusion, discuss all such product irregularities with the laboratory issuing the product for infusion.
- Administer HPC, Cord Blood by intravenous infusion. Do not administer in the same tubing concurrently with products other than 0.9% Sodium Chloride, Injection (USP). HPC, Cord Blood may be filtered through a 170 to 260 micron filter designed to remove clots. Do NOT use a filter designed to remove leukocytes.
- For adults, begin infusion of HPC, Cord Blood at 100 milliliters per hour and increase the rate as tolerated.
For children, begin infusion of HPC, Cord Blood at 1 milliliter per kg per hour and increase as tolerated.
Reduce the infusion rate if the fluid load is not tolerated. Discontinue the infusion in the event of an allergic reaction or if the patient develops a moderate to severe infusion reaction. [See Warnings and Precautions (5.2) and Adverse Reactions (6)] - Monitor the patient for adverse reactions during, and for at least six hours after, administration. Because HPC, Cord Blood contains lysed red cells that may cause renal failure, careful monitoring of urine output is also recommended.
NOTE: If product is being prepared for a multi-unit infusion, infuse units independently. Should a reaction occur, appropriately manage the reaction before the second unit is thawed for infusion.
-
3 DOSAGE FORMS AND STRENGTHS
Each unit of HPC, Cord Blood contains a minimum of 9.0 x 108 total nucleated cells with a minimum of 1.25 x 106 viable CD34+ cells, suspended in 10% dimethyl sulfoxide (DMSO) and 1% Dextran 40, at the time of cryopreservation.
The exact pre-cryopreservation nucleated cell content is provided on the container label and in accompanying records.
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity Reactions
Allergic reactions may occur with infusion of HPC, Cord Blood including HPC, Cord Blood manufactured by MD Anderson Cord Blood Bank. Reactions include bronchospasm, wheezing, angioedema, pruritus, and hives [see Adverse Reactions (6.1)]. Serious hypersensitivity reactions, including anaphylaxis, also have been reported. These reactions may be due to dimethyl sulfoxide (DMSO), Dextran 40, hydroxyethyl starch, or a plasma component of HPC, Cord Blood.
HPC, Cord Blood may contain residual antibiotics if the cord blood donor was exposed to antibiotics in utero. Patients with a history of allergic reactions to antibiotics should be monitored for allergic reactions following HPC, Cord Blood administration.
5.2 Infusion Reactions
Infusion reactions are expected to occur and may include nausea, vomiting, fever, rigors or chills, flushing, dyspnea, hypoxemia, chest tightness, hypertension, tachycardia, bradycardia, dysgeusia, hematuria, and mild headache. Premedication with antipyretics, histamine antagonists, and corticosteroids may reduce the incidence and intensity of infusion reactions.
Severe reactions, including respiratory distress, severe bronchospasm, severe bradycardia with heart block or other arrhythmias, cardiac arrest, hypotension, hemolysis, elevated liver enzymes, renal compromise, encephalopathy, loss of consciousness, and seizure also may occur. Many of these reactions are related to the amount of DMSO administered. Minimizing the amount of DMSO administered may reduce the risk of such reactions, although idiosyncratic responses may occur even at DMSO doses thought to be tolerated. The actual amount of DMSO depends on the method of preparation of the product for infusion. Limiting the amount of DMSO infused to no more than 1 gram per kilogram per day is recommended. [See Overdosage (10)]
Infusion reactions may begin within minutes of the start of infusion of HPC, Cord Blood, although symptoms may continue to intensify and not peak for several hours after completion of the infusion. Monitor the patient closely during this period. When a reaction occurs, discontinue the infusion and institute supportive care as needed. If infusing more than one unit of HPC, Cord Blood on the same day, do not administer subsequent units until all signs and symptoms of infusion reactions from the prior unit have resolved.
5.3 Graft-versus-Host Disease
Acute and chronic graft-versus-host disease (GVHD) may occur in patients who have received HPC, Cord Blood. Classic acute GVHD is manifested as fever, rash, elevated bilirubin and liver enzymes, and diarrhea. Patients transplanted with HPC, Cord Blood should receive immunosuppressive drugs to decrease the risk of GVHD. [See Adverse Reactions (6.1)]
5.4 Engraftment Syndrome
Engraftment syndrome is manifested as unexplained fever and rash in the peri-engraftment period. Patients with engraftment syndrome also may have unexplained weight gain, hypoxemia, and pulmonary infiltrates in the absence of fluid overload or cardiac disease. If untreated, engraftment syndrome may progress to multi-organ failure and death. Once engraftment syndrome is recognized, begin treatment with corticosteroids in order to ameliorate the symptoms. [See Adverse Reactions (6.1)]
5.5 Graft Failure
Primary graft failure, which may be fatal, is defined as failure to achieve an absolute neutrophil count greater than 500 cells per microliter of blood by Day 42 after transplantation. Immunologic rejection is the primary cause of graft failure. Patients should be monitored for laboratory evidence of hematopoietic recovery. Consider testing for HLA antibodies in order to identify patients who are alloimmunized prior to transplantation and to assist with choosing a unit with a suitable HLA type for the individual patient. [See Adverse Reactions (6.1)]
5.6 Malignancies of Donor Origin
Patients who have undergone HPC, Cord Blood transplantation may develop post-transplant lymphoproliferative disorder (PTLD), manifested as a lymphoma-like disease favoring non-nodal sites. PTLD is usually fatal if not treated.
The incidence of PTLD appears to be higher in patients who have received antithymocyte globulin. The etiology is thought to be donor lymphoid cells transformed by Epstein-Barr virus (EBV). Serial monitoring of blood for EBV DNA may be warranted in high-risk groups.
Leukemia of donor origin also has been reported in HPC, Cord Blood recipients. The natural history is presumed to be the same as that for de novo leukemia.
5.7 Transmission of Serious Infections
Transmission of infectious disease may occur because HPC, Cord Blood is derived from human blood. Disease may be caused by known or unknown infectious agents. Donors are screened for increased risk of infection with human immunodeficiency virus (HIV), human T-cell lymphotropic virus (HTLV), hepatitis B virus (HBV), hepatitis C virus (HCV), T. pallidum, T. cruzi, West Nile virus (WNV), transmissible spongiform encephalopathy (TSE) agents, vaccinia and Zika virus. Donors are also screened for clinical evidence of sepsis, and communicable disease risks associated with xenotransplantation. Maternal blood samples are tested for HIV types 1, 2 and O, HTLV types I and II, HBV, HCV, T. pallidum, WNV, and T. cruzi. HPC, Cord Blood is tested for sterility. These measures do not completely eliminate the risk of transmitting these or other transmissible infectious diseases and disease agents. Report the occurrence of a transmitted infection to MD Anderson Cord Blood Bank, The University of Texas MD Anderson Cancer Center at 1-713-563-8000.
Testing of maternal blood is also performed for evidence of donor infection due to cytomegalovirus (CMV).
Test results may be found on the container label and/or in accompanying records.
5.8 Transmission of Rare Genetic Diseases
HPC, Cord Blood may transmit rare genetic diseases involving the hematopoietic system for which donor screening and/or testing has not been performed [see Adverse Reactions (6.1)]. Cord blood donors have been screened by family history to exclude inherited disorders of the blood and marrow. HPC, Cord Blood has been tested to exclude donors with sickle cell anemia, and anemias due to abnormalities in hemoglobins C, D, and E. Because of the age of the donor at the time HPC, Cord Blood collection takes place, the ability to exclude rare genetic diseases is severely limited.
-
6 ADVERSE REACTIONS
Day-100 mortality from all causes was 25%.
The most common infusion-related adverse reactions (≥ 5%) are hypertension, vomiting, nausea, bradycardia, and fever.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety assessment of HPC, Cord Blood is based primarily on review of the data submitted to the FDA dockets from various sources, the dataset for the COBLT1 Study, and published literature.
Infusion Reactions
The Cord Blood Transplantation study group conducted a prospective study (COBLT1) of unrelated cord blood transplantation (CBT) to better define the role of this stem cell source for subjects requiring unrelated allogeneic transplantation. The primary end point of the study was survival at 180 days. Secondary end points included engraftment, graft-versus-host disease, relapse, and long-term survival. Eligibility criteria for malignant and nonmalignant diseases were specified.
The data described in Table 1 reflect exposure to 442 infusions of HPC, Cord Blood (from multiple cord blood banks) in patients treated using a total nucleated cell dose ≥ 2.5 x 107/kg on a single-arm trial or expanded access use (The COBLT1 Study). The population was 60% male, the median age was 5 years (range 0.05-68 years), and included patients treated for hematologic malignancies, inherited metabolic disorders, primary immunodeficiencies, and bone marrow failure. Preparative regimens and GVHD prophylaxis were not standardized. The most common infusion reactions were hypertension, vomiting, nausea, and sinus bradycardia. Hypertension and grades 3-4 infusion-related reactions occurred more frequently in patients receiving HPC, Cord Blood in volumes greater than 150 milliliters and in pediatric patients. The rate of serious adverse cardiopulmonary reactions was 0.8%.
Table 1. Incidence of Infusion-Related Adverse Reactions Occurring in ≥1% of Infusions (The COBLT1 Study) Any grade
Grade 3-4
Any reaction
65.4%
27.6%
Hypertension
48.0%
21.3%
Vomiting
14.5%
0.2%
Nausea
12.7%
5.7%
Sinus bradycardia
10.4%
0
Fever
5.2%
0.2%
Sinus tachycardia
4.5%
0.2%
Allergy
3.4%
0.2%
Hypotension
2.5%
0
Hemogloburia
2.1%
0
Hypoxia
2.0%
2.0%
Information on infusion reactions was available from voluntary reports for 846 patients who received cord blood units manufactured at MD Anderson Cord Blood Bank with a TNC dose ≥ 2.5 x 107/kg and HLA match grade ≥ 4/6. The population included 59% males and 41% females with median age of 25 years (range 0.1-73 years). Preparative regimens and GVHD prophylaxis were not standardized. The reactions, as reported to the MD Anderson Cord Blood Bank by the Stem Cell Outcomes Database (SCTOD) of the Center for International Blood and Marrow Transplant Research (CIBMTR), were not graded. Twenty-two percent of infusions (n=187) were associated with an infusion reaction. The most common infusion reactions, occurring in >1% of infusions, were hypertension (17.1%), nausea (4.3%), vomiting (3.9%), and headache (1.2%).
Other Adverse Reactions
For other adverse reactions, the raw clinical data from the docket were pooled for 1299 (120 adult and 1179 pediatric) patients transplanted with HPC, Cord Blood (from multiple cord blood banks) with total nucleated cell dose ≥2.5 x 107/kg. Sixty-six percent (n=862) underwent transplantation as treatment for hematologic malignancy. The preparative regimens and GVHD prophylaxis varied. The median total nucleated cell dose was 6.4 x 107/kg (range 2.5-73.8 107/kg). For these patients, Day-100 mortality from all causes was 25%. Primary graft failure occurred in 16%; 42% developed grades 2-4 acute GVHD and 19% developed grades 3-4 acute GVHD.
Data from published literature and from observational registries, institutional databases, and cord blood bank reviews reported to the docket for HPC, Cord Blood (from multiple cord blood banks) revealed nine cases of donor cell leukemia, one case of transmission of infection, and one report of transplantation from a donor with an inheritable genetic disorder. The data are not sufficient to support reliable estimates of the incidences of these events.
In the COBLT1 study, 15% of the patients developed engraftment syndrome.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no data with HPC, Cord Blood use in pregnant women to inform a product-associated risk. Animal reproduction studies have not been conducted with HPC, Cord Blood. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
8.2 Lactation
Risk Summary
There is no information regarding the presence of HPC, Cord Blood in human milk, the effects on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for HPC, Cord Blood and any potential adverse effects on the breastfed infant from HPC, Cord Blood or from the underlying maternal condition.
8.4 Pediatric Use
HPC, Cord Blood has been used in pediatric patients with disorders affecting the hematopoietic system that are inherited, acquired, or resulted from myeloablative treatment. [See Dosage and Administration (2), Adverse Reactions (6), and Clinical Studies (14)]
8.5 Geriatric Use
Clinical studies of HPC, Cord Blood (from multiple cord blood banks) did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently than younger subjects. In general, administration of HPC, Cord Blood to patients over age 65 should be cautious, reflecting their greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
-
10 OVERDOSAGE
10.1 Human Overdosage Experience
There has been no experience with overdose of HPC, Cord Blood in human clinical trials. Single doses of HPC, Cord Blood up to 5.0 x 108 TNC/kg have been administered. HPC, Cord Blood prepared for infusion may contain dimethyl sulfoxide (DMSO). The maximum tolerated dose of DMSO has not been established, but it is customary not to exceed a DMSO dose of 1 gm/kg/day when given intravenously. Several cases of altered mental status and coma have been reported with higher doses of DMSO.
-
11 DESCRIPTION
HPC, Cord Blood consists of hematopoietic progenitor cells, monocytes, lymphocytes, and granulocytes from human cord blood for intravenous infusion. Blood recovered from the umbilical cord and placenta is volume reduced and partially depleted of red blood cells and plasma.
The active ingredient is hematopoietic progenitor cells, which express the cell surface marker CD34. The potency of cord blood is determined by measuring the numbers of total nucleated cells (TNC) and CD34+ cells, and cell viability. Each unit of HPC, Cord Blood contains a minimum of 9.0 x 108 total nucleated cells with at least 1.25 x 106 viable CD34+ cells at the time of cryopreservation. The cellular composition of HPC, Cord Blood depends on the composition of cells in the blood recovered from the umbilical cord and placenta of the donor. The actual nucleated cell count, the CD34+ cell count, the ABO group, and the human leukocyte antigen (HLA) typing are listed on the container label and/or accompanying records sent with each individual unit.
HPC, Cord Blood has the following inactive ingredients: dimethyl sulfoxide (DMSO), citrate phosphate dextrose (CPD), hydroxyethyl starch, and Dextran 40. When prepared for infusion according to instructions, the infusate contains the following inactive ingredients: Dextran 40, human serum albumin, residual DMSO, residual hydroxyethyl starch and residual CPD.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Hematopoietic stem/progenitor cells from HPC, Cord Blood migrate to the bone marrow where they divide and mature. The mature cells are released into the bloodstream, where some circulate and others migrate to tissue sites, partially or fully restoring peripheral blood counts and function, including immune function, of blood-borne cells of marrow origin. [See Clinical Studies (14)]
In patients with enzymatic abnormalities due to certain severe types of storage disorders, mature leukocytes resulting from HPC, Cord Blood transplantation may synthesize enzymes that may be able to circulate and improve cellular functions of some native tissues. However, the precise mechanism of action is unknown.
-
14 CLINICAL STUDIES
The effectiveness of HPC, Cord Blood, as defined by hematopoietic reconstitution, was demonstrated in the single-arm prospective COBLT1 study, and in retrospective review of data from an observational database for MD Anderson Cord Blood Bank, using data from the Center for International Blood and Marrow Transplant Research (CIBMTR), the National Marrow Donor Program (NMDP), and data in the FDA dockets and public information. The total nucleated cell dose and degree of HLA match were inversely associated with the time to neutrophil recovery in the docket data. Sixty-six percent (n=862) of the 1299 patients in the docket and public data underwent transplantation as treatment for hematologic malignancy. In the MD Anderson Cord Blood Bank database, 84% of patients (708 of 846) underwent transplantation for a hematologic malignancy.
Table 2 describes the recipient characteristics and hematopoietic recovery of 846 patients who received a total nucleated cell dose of ≥ 2.5 x 107/kg from at least a single cord blood unit manufactured at MD Anderson Cord Blood Bank, alone or in combination with another unit of HPC, Cord Blood and who had an HLA match ≥ 4/6, as well as the outcomes from the COBLT1 study and the docket data.
Neutrophil recovery is defined as the time from transplantation to an absolute neutrophil count greater than 500 cells/μL. Platelet recovery is the time to a platelet count greater than 20,000 cells/μL without a platelet transfusion for the preceding seven days. Erythrocyte recovery is the time to a reticulocyte count greater than 30,000 cells/μL.
Table 2: Hematopoietic Recovery in Patients Transplanted with HPC, Cord Blood units supplied by the MD Anderson Cord Blood Bank compared to the COBLT1 study and Docket Data Data Source The COBLT1 Study Docket and Public Data MD Anderson Cord Blood Bank Data* *Data from patients who received a suitable allograft (TNC ≥ 2.5 x 107/kg and ≥ 4/6 HLA match). Note that evaluable data for outcomes were not available for all patients and there are various amounts of missing data. NA: Not Available Design Single-arm prospective Retrospective Retrospective Number of patients 324 1299 846 Median age (range) years 4.6 (0.07 - 52.2) 7.0 (<1 - 65.7) 24.8 (0.1 – 73.3) Sex 59% male 57% male 58% male 41% female 43% female 42% female Median Weight (range) at transplant (kg) NA NA 59
(2.6-146.0)Median TNC Dose (range) (x 107/kg) 6.7
(2.6 -38.8)6.4
(2.5- 73.8)5.4
(2.5-76.9)Neutrophil Recovery at Day 42
(ANC > 500/µL) (95% Cl)76%
(71% - 81%)77%
(75% - 79%)88.2%
(85.9% - 90.2%)Platelet Recovery at Day 100 (20,000/µL) (95% CI) 57%
(51% - 63%)NA 73.6%
(70%-77%)Platelet Recovery at Day 100 (50,000/µL) (95% Cl) 46%
(39% - 51%)45%
(42% - 48%)43%
(39%, 46%)Erythrocyte Recovery at Day 100 (95% CI) 65%
(58%-7 1%)NA NA Median Time to Neutrophil Recovery 27 days 25 days 19 days Median Time to Platelet Recovery (20,000/µL) 90 days NA 47 days Median Time to Platelet Recovery (20,000/µL) 113 days 122 days 65 days Median Days to Erythrocyte Recovery 64 days NA NA - 15 REFERENCES
-
16 HOW SUPPLIED/STORAGE AND HANDLING
HPC, Cord Blood is supplied as a cryopreserved cell suspension in a sealed bag containing a minimum of 9.0 x 108 total nucleated cells with a minimum of 1.25 x 106 viable CD34+ cells in a volume of 25 milliliters (ISBT 128 Product Code S1393, ISBT 128 Facility Identifier Number W2263). The exact pre-cryopreservation nucleated cell content is provided on the container label and accompanying records.
Store HPC, Cord Blood at or below -150°C until ready for thawing and preparation.
-
17 PATIENT COUNSELING INFORMATION
Discuss the following with patients receiving HPC, Cord Blood:
- Report immediately any signs and symptoms of acute infusion reactions, such as fever, chills, fatigue, breathing problems, dizziness, nausea, vomiting, headache, or muscle aches.
- Report immediately any signs or symptoms suggestive of graft-vs-host disease, including rash, diarrhea, or yellowing of the eyes.
INSTRUCTIONS FOR PREPARATION FOR INFUSION
MD Anderson Cord Blood Bank recommends washing of the HPC, Cord Blood unit prior to infusion. Once the wash procedure is complete, the product must be infused within four hours. Included below are instructions for washing HPC, Cord Blood. Prior to thawing of the unit, read the thaw and wash instructions and emergency product recovery procedure below. Prepare all required reagents, supplies, equipment, and forms listed, and ensure they are readily available.
1 Reagents
- Human serum albumin, 5%, USP
- Dextran 40 in Sodium Chloride Injection, USP (10% Low Molecular Weight Dextran in 0.9% Sodium Chloride Injection)
- Sterile water
- 70% Isopropyl Alcohol (for cleaning)
2 Supplies
- Bacterial culture bottles, aerobic and anaerobic [or other supplies for performing sterility testing]
- Bag spike with tubing (2)
- 300 ml transfer pack (2)
- 60 ml sterile disposable syringe with tubing (4)
- 10 ml sterile disposable syringe (2)
- 3 ml sterile disposable syringe with tubing (1)
- 16-gauge needles
- Blunt end needle (Emergency Product Recovery)
- 2 ml cryogenic vial
- Tubes for cell counts, progenitor assays (optional)
- Alcohol prep pads
- Sterile plastic zip-lock bags
- Product labels
- Refrigerated gel/ice pack
- Hemostat or Hoffman clamp
- Absorbent wipes
- Canister opening tool
- Scissors
- Personal protective equipment: gloves
protective cryogloves
safety goggles or face shield
3 Equipment
- Biosafety Cabinet
- Liquid nitrogen freezer
- Refrigerated centrifuge
- Water bath
- Sterile tubing connecting device
- Tube sealer, compatible with polyvinyl chloride (PVC)
- Automated cell counter
4 Forms
- Cell Product Shipment Integrity Form
- National Marrow Donor Program (NMDP) Receipt of Cord Blood Unit Form
II PRODUCT RECEIPT AND IDENTITY VERIFICATION
HPC, Cord Blood is shipped frozen at or below -150°C using a liquid nitrogen (LN2) dry shipper. The unit is packed for transport in a stainless steel canister contained within an insulated transport sleeve. Keep HPC, Cord Blood at or below -150°C, either inside the dry shipper container used for shipping or in a liquid nitrogen (LN2) cooled device at the transplant center (recommended). If the HPC, Cord Blood will be stored inside the dry shipper, add liquid nitrogen to the vessel to ensure the unit will be kept at or below -150°C.
Upon receipt of the shipment perform the following steps:
- Using scissors, cut the zip ties used to secure the outer lid of the liquid nitrogen dry shipper.
- Open the outer lid of the liquid nitrogen dry shipper and remove shipment documentation packet from inside of lid.
- Remove the Cell Product Shipment Integrity form from the shipment documentation packet and complete the following information:
3.1 Record date and time of receipt
3.2 Inspect shipper for damage or tampering, verify shipper inner lid is secured with tie tag
3.3 Record temperature from the temperature data logger attached to the inner lid on the
Cell Product Shipment Integrity form. Check for alarms.
NOTE: Do not stop the logging process or download data when recording temperature from data logger.
- Cut the tie tag securing the inner lid assembly and remove inner lid.
NOTE: The lid assembly should be held by another person or placed, black side down, on a stable surface to protect the temperature probe (see Figure 1).
- Wearing cryogloves, remove the HPC, Cord Blood product and accompanying samples from the shipper and transfer to vapor phase of liquid nitrogen and maintain temperature at or below -150°C for label and product integrity verification.
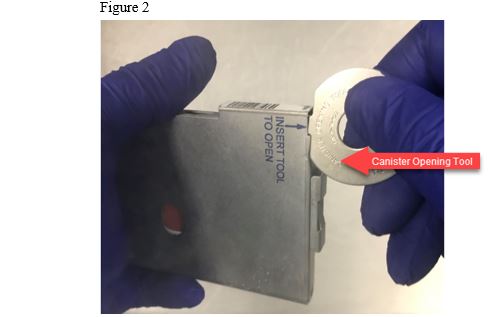
5.1 Remove the canister from the insulated transport sleeve.
5.2 Remove the canister opening tool from the shipment documentation packet.
5.3 Using the canister opening tool, carefully pry open the canister at the top and bottom,
working carefully to avoid damage to the frozen plastic product bag (See Figure 2).
NOTE: Use of other methods for opening the canister could result in damage to the cryopreserved HPC, Cord Blood product.
- Verify that the product and any accompanying samples have remained frozen and document
on the Cell Product Shipment Integrity form.
- Verify the physical integrity of the cryobag for visible cracks, holes or leaks; document
cryobag integrity or any damage on the Cell Product Shipment Integrity form. - Verify patient/donor name, medical record number and unit number information match the
information on the bag’s label(s), shipment documentation and your records. Document match
on the Cell Product Shipment Integrity form.
NOTE: If there is any error or ambiguity with the HPC, Cord Blood product, accompanying
samples, or product documentation, keep the product in the canister and store at or
below -150°C. Report the discrepancy immediately to the MD Anderson Cord Blood
Bank at 1-713-563-8000. Do not proceed until the problem is resolved.
- Close the canister and transfer the HPC, Cord Blood cryobag and accompanying samples to
storage vessels capable of maintaining HPC, Cord Blood at or below -150°C and
accompanying samples at or below -70°C.
9.1 If the HPC, Cord Blood cryobag and accompanying samples are to be stored in the dry
shipper until time of thaw, add additional liquid nitrogen to the dry shipper to ensure the
product will be maintained at or below -150°C.
NOTE: Aside from the segment, ancillary samples are not intended to represent the cell
count or potency of the cryopreserved HPC, Cord Blood product.
- Fax the completed Cell Product Shipment Integrity form to the MD Anderson Cord Blood
Bank at 1-713-563-3468. - Once use of the dry shipper is complete, prepare for shipment and return to MD Anderson
Cord Blood bank per instructions provided in the shipment documentation packet.
III PREPARATION
-
General Preparation Information
1.1. Every attempt should be made to ensure HPC, Cord Blood is thawed rapidly, kept cool after thawing, and
immediately washed as detailed below in order to limit exposure of thawed cells to DMSO.
1.2. Use aseptic techniques in a biological safety cabinet (BSC) for processing steps,
including spiking of the product bag ports and post-wash product sampling.
1.3 Use only sterile, single use supplies and reagents.
1.4 Record the manufacturer information, lot number and expiration date (if applicable) of all reagents and
supplies.
1.5 Review Section 9: Emergency Product Recovery in the Event of Primary Container
Failure prior to thawing product. Always thaw the cryobag inside a sterile zip-lock bag
so product can be recovered if leakage occurs. If product leaks from the cryobag into the
sterile zip-lock bag, follow the Emergency Product Recovery procedure described below
in Section 9.
-
Prepare 200 ml Dextran 40/Albumin Wash Solution
2.1. Aseptically withdraw 100 ml of Human Serum Albumin and 100ml of Dextran 40 and
combine in a single 300 ml transfer pack (Dextran/Albumin wash solution) labelled with the
HPC, Cord Blood identifier.
2.2. Mix contents of the transfer pack.
NOTE: The transfer bag now contains a total of 200 ml of solution containing both
Dextran 40 and human serum albumin and will be referred to as the wash solution
2.3. Using a sterile tubing connecting device, sterile connect a 60ml syringe with tubing to the
transfer pack containing the Dextran/Albumin wash solution. Withdraw 20 ml of the wash
solution for diluting the thawed HPC, Cord Blood product.
2.4. Using a heat sealer, remove the 60ml syringe containing the 20ml aliquot of wash solution
from the bag of wash solution ensuring to leave enough of the transfer line for additional
connections.
2.5. Repeat steps 2.3 through 2.4 to create a second 20ml aliquot of wash solution for rinsing
the HPC, Cord Blood bag.
2.6. Using a sterile tubing connecting device, sterile connect a 60ml syringe with tubing to the
transfer pack containing the Dextran/Albumin wash solution. Withdraw 50 ml of the wash
solution for resuspending the washed HPC, Cord Blood product/cells.
2.7 Using a heat sealer, remove the 60ml syringe containing the 50ml aliquot of wash
solution from the bag of wash solution, ensuring to leave enough of the transfer line for
connection to the cryobag.
2.8 Place the transfer pack containing the remaining wash solution and the 60ml syringes into
a zip-lock bag and store at 2 - 8°C until ready to use.
-
Thawing
3.1. Fill an empty, clean water bath with sterile water. Verify the set point of water bath is 37±1°C
3.2. Prior to removal of HPC, Cord Blood from storage, confirm water bath temperature is
37± 1°C. If the water bath temperature is not within range, wait and/or adjust it such that
it reaches the desired range.
3.3. Retrieve canister containing HPC, Cord Blood from storage and place into vapor phase of
the LN2 freezer or other vessel capable of maintaining temperatures at or below -150°C.
NOTE: Handle HPC, Cord Blood with extreme caution when removing it from the liquid
nitrogen, metal cassette and the protective overwrap. Cryobags are very fragile.
3.4. Working in the vapor phase LN2, remove HPC, Cord Blood cryobag from the metal
canister.
3.4.1 Verify label information with a second technologist against transport
documentation and confirm unit identity and intended recipient.
NOTE: Labels on HPC, Cord Blood cryobag should match the labels on the
metal cassette, the tie tag, and on the accompanying paperwork.
3.4.2 Visually inspect the physical integrity of the cryobag for visible cracks, holes or
leaks.
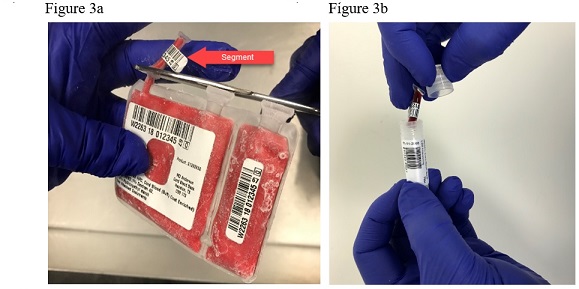
3.5. Using scissors, remove and place the remaining segment in a labeled 2ml cryovial (See
Figures 3a and 3b). Store the segment in liquid or vapor phase of liquid nitrogen at or
below -150°C.
3.6. Gently, wipe the external surface of the cryobag with an absorbent wipe soaked with
70% isopropyl alcohol.
3.7. Place the cryobag inside a sterile zip-lock bag, let out the air, and seal the zip-lock bag.
NOTE: Use of the sterile zip-lock bag allows for recovery of product in the case of an
unexpected leak or container failure during thawing or centrifugation
3.8. Place zip-lock bag into 37±1°C water bath.
3.9. Gently massage the cryobag to promote uniform thawing (See Figure 4). Observe
cryobag for any sign of leakage.
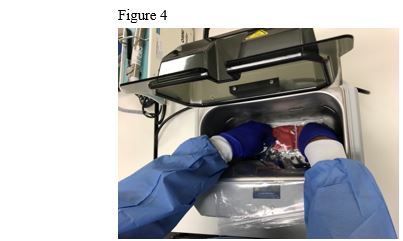
3.10. Continue to massage the cryobag until the HPC, Cord Blood reaches a slushy
consistency. This generally takes about 1-2 minutes.
3.11. Carefully remove the thawed HPC, Cord Blood cryobag from the zip-lock bag and dry
off moisture using an absorbent wipe(s).
3.12 Place the thawed cryobag on ice or cool pack in the BSC.
-
Cell Extraction
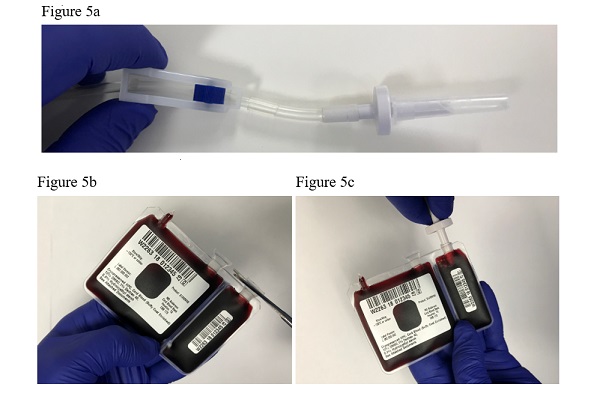
4.1. Using scissors cleaned with an alcohol prep pad, aseptically cut open the port protector
of the 20% fraction and insert the bag spike with tubing (See Figures 5a, 5b, and 5c).
NOTE: Ensure clamp on bag spike with tubing is closed prior to spiking bag ports.
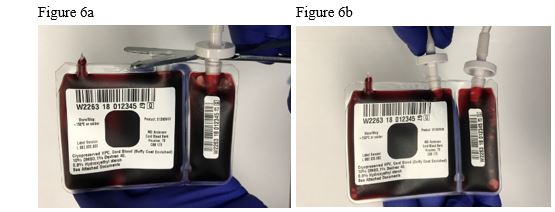
4.2. Using scissors cleaned with alcohol, repeat the process in 4.1 above and aseptically open
the port protector of the 80% fraction and insert bag spike with tubing (See Figures 6a
and 6b).
4.3. With the cryobag on the ice or cool pack, aseptically connect one of the 60ml
syringes with tubing containing 20 ml of wash solution onto the tubing from the 80% fraction of
the unit using a sterile connection device.
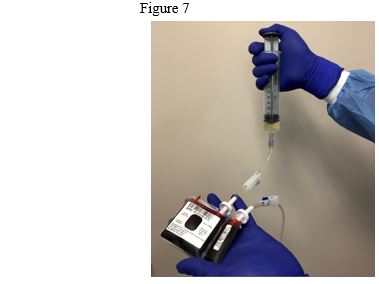
4.4. Slowly inject half of the wash media (approx. 10 ml) from the 60ml syringe into the
HPC, Cord Blood cryobag; gently mix, and then remove the same amount of solution
added (See Figure 7).
4.5. Repeat once more by adding half the contents of the 60ml syringe into the HPC, Cord
Blood cryobag gently mix, and then empty the cryobag compartment by drawing the
entire contents into the syringe.
4.6. Using a heat sealer, seal the line attached to the bag spike, ensuring enough tubing is left
for connection of the second 20ml aliquot of wash solution.
4.7. Using a sterile tubing connecting device, sterile connect the syringe removed from the
80% fraction to the 20% fraction and repeat steps 4.5 through 4.8. Seal the line and
sterile connect the 60ml syringe containing the cells and wash solution to the
Dextran/Albumin wash transfer pack and add the entire contents of the syringe to the
300ml transfer pack containing the remainder wash solution; this is now the product
bag. Mix well.
-
Cryobag Rinse
5.1. Using a sterile tubing connecting device, sterile connect the second 60ml syringe
containing 20 ml of wash solution onto the tubing from the 80% fraction of the cryobag.
5.2. Rinse the 80% compartment with wash solution and collect the contents.
5.3 Seal the line and remove the syringe.
5.4 Repeat steps 5.1 through 5.3 for the 20% fraction.
5.5 Using a sterile tubing connecting device, sterile connect the 60ml syringe containing the
rinse solution to Dextran/Albumin wash transfer pack and add the entire contents of the
syringe. Mix well.
5.6 Clamp the tubing between the syringe and 300ml transfer pack now containing the
product using a hemostat.
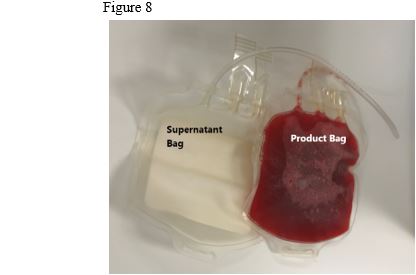
5.7 Using a sterile tubing connecting device, sterile connect a second 300ml transfer pack to
the product bag. Do not open weld. This bag will be used to collect the wash
supernatant (See Figure 8).
-
Centrifugation and Supernatant Removal
6.1. Place the 300ml transfer pack containing the HPC, Cord Blood product into a sterile zip-lock
bag supported to sit in the middle of the centrifuge bucket.
6.2. Balance and centrifuge at 800g for 15 minutes at 4°C.
6.3. After centrifugation, carefully remove bags from centrifuge bucket ensuring not to
disturb the cell pellet.
6.4. Place the bag containing the washed HPC, Cord Blood upright in the plasma expresser.
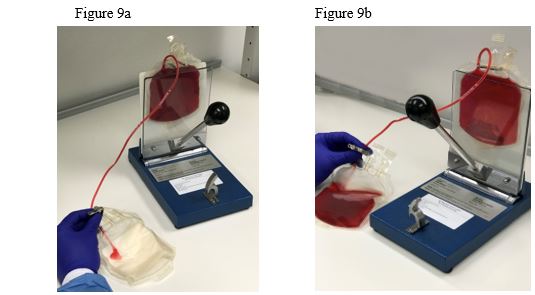
6.5. Open the sterile weld to supernatant bag and using a hemostat or Hoffman clamp to
control flow rate, and carefully express supernatant into the empty transfer pack using
the plasma expressor until approximately 50 ml remains in the product bag. Carefully
avoid passage of cells into supernatant (See Figures 9a and 9b).
6.6. Seal line and remove transfer pack containing supernatant.
6.7. Resuspend cell pellet in remaining supernatant.
6.8. Using a sterile tubing connecting device, sterile connect a 60ml syringe with tubing onto
HPC, Cord Blood product bag and measure the volume.
6.9. Push the resuspended cells back into the transfer pack.
6.10. Using a sterile tubing connecting device, sterile connect the 60ml syringe containing 50 ml
of wash solution to the transfer pack and adjust the volume of the cell suspension in
the transfer pack to a maximum volume of 100 ml.
6.11. Record the date/time of completion of the wash procedure.
6.12. Proceed to Section 7.
-
Preparation of HPC, Cord Blood for Transplantation
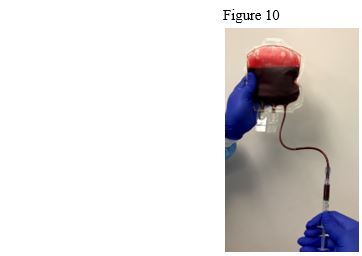
7.1. Using a sterile tubing connecting device, sterile connect a 3ml syringe with tubing to the
transfer line of the transfer pack containing the washed product (See Figure 10).
7.2. Working in a BSC, using aseptic technique, aseptically remove a 1 ml sample from the
washed product using the 3ml syringe with tubing.
NOTE: Use this sample to perform viability analysis, total nucleated cell count and
other testing as recommended in Section 8: Quality Control Testing.
7.3. Using a heat sealer, seal the line between the washed product bag and the 3ml syringe.
Separate the 3ml syringe from the line by cutting through the seal using scissors.
7.4. Working in a BSC, using aseptic technique, use two 10ml syringes to
obtain two separate 8 ml aliquots of wash supernatant from the supernatant transfer pack for
sterility testing.
7.5. Calculate viable cell recovery using the following formula:
(Total Viable Nucleated Cells on the Infusion Ready Product ÷ Total Viable Nucleated
Cells of Cryopreserved Unit Provided on Shipment Report) x 100%
7.6 Label the infusion bag with patient and donor information per institutional standard
operating procedures.
7.7 Label the infusion bag with the washed product expiration date/time. The expiration
date/time of the washed product is four hours from completion of wash procedure
described in Section 6.
7.8 Confirm and document, with a second technologist or designee, the cord blood identifier
is affixed to infusion bag.
7.9 Complete appropriate site-specific laboratory forms to document the thawing process
and final volumes.
7.10 Transport infusion bag to the site of administration to the patient in a transport container
capable of maintaining the unit temperature between 2 - 22°C.
7.11 Infuse within four hours of completion of wash procedure.
7.12 Infuse the product through a 170-260 micron filter at the bedside. Do not use
leukoreduction filters.
-
Quality Control Testing
The following tests are recommended:
8.1. Cell Counts: perform on final product to be infused.
8.2. Cell Viability: perform on final product to be infused (Viable CD45+ determination by
flow cytometric analysis recommended).
8.3. Colony assay for CFU-GM, CFU-GEMM, and BFU-E: perform on final product to be
infused.
8.4. Viable CD34+ determination by flow cytometric analysis: perform on final product to
be infused.
8.5. Sterility test: perform on wash supernatant.
-
Emergency Product Recovery in Event of Primary Container Failure
9.1 If the cryobag is compromised, move further handling into BSC after thawing.
NOTE: It is the transplant physician’s (or designee’s) responsibility to determine
whether the product will be used or discarded if the container is
compromised at any step of the procedure.
9.2 If the transplant physician (or designee) decides that the product should be used,
recovery of the product may be attempted as described below.
9.3 Use a long (3-5 inch) blunt needle (a sterile spinal needle with trochar removed if
available).
9.4 Attach the blunt needle to a sterile 60 mL syringe.
9.5 Aspirate the product from the cryobag and inject into a sterile transfer bag.
9.6 Continue to the wash step for the transferred product.
9.7 Start and complete the wash process for the transferred product.
9.8 Perform sterility test on a sample of the recovered wash product.
NOTE: Alert the clinical team at the transplant center that the product could potentially
be contaminated.
9.9 Contact the MD Anderson Cord Blood Bank at 1-713-563-8000 or 713-794-1908 if
during thawing, any portion of the product container appears to be damaged or
compromised. Save the ruptured cryobag if possible. The Cord Blood Bank will
provide further instructions for return of the container, if required for investigation.
Distributed by:
MD Anderson Cord Blood Bank
1841 Old Spanish Trail
Houston, TX 77054
713-563-8000
U.S. License # 2072 -
PACKAGE LABEL

Store/Ship:
-150C or colder
Product: S1393V00
Label Version:
L 082.033.002
MD Anderson
Cord Blood Bank
Houston, TX
CBB 173
Cryopreserved HPC, Cord Blood (Buffy Coat Enriched)
10% DMSO, 1% Dextran 40,
0.8% Hydroxyethyl starch
See Attached Documents
Collection
Date
0150910316
01 APR 2015 03:16
Properly identify intended Recipient and Product
Rx only.
A
Rh POSITIVE
FOR USE BY INTENDED
RECIPIENT ONLY
INTENDED RECIPIENT
Name: Doe, John
DOB: 12/25/1992
ID: 123-456-7
DO NOT IRRADIATE
DO NOT USE LEUKOREDUCTION FILTER
CRYOPRESERVED
HPC, CORD BLOOD
Buffy Coat Enriched
Approx. 25 ml
10% DMSO, 1% DEXTRAN 40,
0.8% Hydroxyethyl starch
Store at -150°C or colder
See package insert for full prescribing
information and instructions for preparation
Expiration
Date
01 APR 2025 03:0316
ADDITIONAL CBU IDENTIFIERS
NMDP ID: 9876-5432-1
Local ID: 012345
Collected and Processed By
MD Anderson Cord Blood Bank
1841 Old Spanish Trail, Houston, TX
US License: 2072
Label Version: L 082.027.002
-
INGREDIENTS AND APPEARANCE
HEMATOPOIETIC PROGENITOR CELLS, CORD BLOOD
human cord blood hematopoietic progenitor cell solutionProduct Information Product Type LICENSED MINIMALLY MANIPULATED CELLS Item Code (Source) ISBT:W2263-S1393 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Human Cord Blood Hematopoietic Progenitor Cell (UNII: XU53VK93MC) (Human Cord Blood Hematopoietic Progenitor Cell - UNII:XU53VK93MC) Human Cord Blood Hematopoietic Progenitor Cell 900000000 in 25 mL Inactive Ingredients Ingredient Name Strength Dextran 40 (UNII: K3R6ZDH4DU) Dimethyl Sulfoxide (UNII: YOW8V9698H) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 ISBT:W2263-S1393-02 1 in 1 CANISTER 1 25 mL in 1 BAG; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125657 06/22/2018 Labeler - University of Texas MD Anderson Cancer Center (800772139) Establishment Name Address ID/FEI Business Operations University of Texas MD Anderson Cancer Center 117159375 label(W2263-S1393) , manufacture(W2263-S1393)