Label: ESTROPIPATE tablet



-
Contains inactivated NDC Code(s)
NDC Code(s): 54868-3114-0, 54868-3114-1, 54868-4149-0, 54868-4149-1, view more54868-4761-1, 54868-4761-2 - Packager: Physicians Total Care, Inc.
- This is a repackaged label.
- Source NDC Code(s): 52544-414, 52544-415, 52544-416
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: Abbreviated New Drug Application
Drug Label Information
Updated March 14, 2012
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
BOXED WARNING
(What is this?)
WARNINGSESTROGENS INCREASE THE RISK OF ENDOMETRIAL CANCER
Close clinical surveillance of all women taking estrogens is important. Adequate diagnostic measures, including endometrial sampling when indicated, should be undertaken to rule out malignancy in all cases of undiagnosed persistent or recurring abnormal vaginal bleeding. There is no evidence that the use of “natural” estrogens result in a different endometrial risk profile than “synthetic” estrogens at equivalent estrogen doses. (See WARNINGS, Malignant neoplasms, Endometrial cancer.)
CARDIOVASCULAR AND OTHER RISKSEstrogens with and without progestins should not be used for the prevention of cardiovascular disease. (See WARNINGS, Cardiovascular disorders.)
The Women’s Health Initiative (WHI) study reported increased risks of myocardial infarction, stroke, invasive breast cancer, pulmonary emboli, and deep vein thrombosis in postmenopausal women (50 to 79 years of age) during 5 years of treatment with oral conjugated estrogens (CE 0.625 mg) combined with medroxyprogesterone acetate (MPA 2.5 mg) relative to placebo. (see CLINICAL PHARMACOLOGY, Clinical Studies.)
The Women’s Health Initiative Memory Study (WHIMS), a substudy of WHI, reported increased risk of developing probable dementia in postmenopausal women 65 years of age or older during 4 years of treatment with oral conjugated estrogens plus medroxyprogesterone acetate relative to placebo. It is unknown whether this finding applies to younger postmenopausal women or to women taking estrogen alone therapy. (See CLINICAL PHARMACOLOGY, Clinical Studies.)
Other doses of conjugated estrogens with medroxyprogesterone acetate, and other combinations and dosage forms of estrogens and progestins were not studied in the WHI clinical trials and, in the absence of comparable data, these risks should be assumed to be similar. Because of these risks, estrogens with or without progestins should be prescribed at the lowest effective doses and for the shortest duration consistent with treatment goals and risks for the individual woman.
-
DESCRIPTION
Estropipate (formerly piperazine estrone sulfate), is a natural estrogenic substance prepared from purified crystalline estrone, solubilized as the sulfate and stabilized with piperazine. It is appreciably soluble in water and has almost no odor or taste — properties which are ideally suited for oral administration. The amount of piperazine in estropipate is not sufficient to exert a pharmacological action. Its addition ensures solubility, stability, and uniform potency of the estrone sulfate. Chemically estropipate, molecular weight: 436.56, is represented by estra-1,3,5(10)-trien-17-one,3-(sulfooxy)-, compound with piperazine (1:1). The structural formula may be represented as follows:
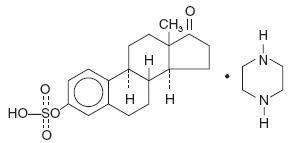
C18H22O5S.C4H10N2 M.W.=436.56
Estropipate is available as tablets for oral administration containing either 0.75 mg, 1.5 mg, 3 mg, or 6 mg estropipate (calculated as sodium estrone sulfate 0.625 mg, 1.25 mg, 2.5 mg and 5 mg, respectively).
Inactive IngredientsEach tablet contains: lactose NF, magnesium stearate NF, piperazine USP, pregelatinized starch NF, talc USP, and coloring agents: 0.75 mg—D&C Yellow #10; 1.5 mg—FD&C Yellow #6; 3 mg—FD&C Blue #2; 6 mg—FD&C Blue #2 and D&C Yellow #10.
-
CLINICAL PHARMACOLOGY
Endogenous estrogens are largely responsible for the development and maintenance of the female reproductive system and secondary sexual characteristics. Although circulating estrogens exist in a dynamic equilibrium of metabolic interconversions, estradiol is the principal intracellular human estrogen and is substantially more potent than its metabolites, estrone and estriol at the receptor level.
The primary source of estrogen in normally cycling adult women is the ovarian follicle, which secretes 70 to 500 mcg of estradiol daily, depending on the phase of the menstrual cycle. After menopause, most endogenous estrogen is produced by conversion of androstenedione, secreted by the adrenal cortex, to estrone by peripheral tissues. Thus, estrone and the sulfate conjugated form, estrone sulfate, are the most abundant circulating estrogens in postmenopausal women.
Estrogens act through binding to nuclear receptors in estrogen-responsive tissues. To date, two estrogen receptors have been identified. These vary in proportion from tissue to tissue.
Circulating estrogens modulate the pituitary secretion of the gonadotropins, luteinizing hormone (LH) and follicle stimulating hormone (FSH), through a negative feedback mechanism. Estrogens act to reduce the elevated levels of these hormones seen in postmenopausal women.
Pharmacokinetics
AbsorptionEstrogens are well absorbed through the skin and gastrointestinal tract. When applied for a local action, absorption is usually sufficient to cause systemic effects.
DistributionThe distribution of exogenous estrogens is similar to that of endogenous estrogens. Estrogens are widely distributed in the body and are generally found in higher concentrations in the sex hormone target organs. Estrogens circulate in the blood largely bound to sex hormone binding globulin (SHBG) and albumin.
MetabolismExogenous estrogens are metabolized in the same manner as endogenous estrogens. Circulating estrogens exist in a dynamic equilibrium of metabolic interconversions. These transformations take place mainly in the liver. Estradiol is converted reversibly to estrone, and both can be converted to estriol, which is the major urinary metabolite. Estrogens also undergo enterohepatic recirculation via sulfate and glucuronide conjugation in the liver, biliary secretion of conjugates into the intestine, and hydrolysis in the gut followed by reabsorption. In postmenopausal women, a significant proportion of the circulating estrogens exist as sulfate conjugates, especially estrone sulfate, which serves as a circulating reservoir for the formation of more active estrogens.
ExcretionEstradiol, estrone, and estriol are excreted in the urine along with glucuronide and sulfate conjugates.
Drug InteractionsIn vitro and in vivo studies have shown that estrogens are metabolized partially by cytochrome P450 3A4 (CYP3A4). Therefore, inducers or inhibitors of CYP3A4 may affect estrogen drug metabolism. Inducers of CYP3A4 such as St. John’s Wort preparations (Hypericum perforatum), phenobarbital, carbamazepine, and rifampin may reduce plasma concentrations of estrogens, possibly resulting in a decrease in therapeutic effects and/or changes in the uterine bleeding profile. Inhibitors of CYP3A4 such as erythromycin, clarithromycin, ketoconazole
Clinical Studies
Women's Health Initiative StudiesThe Women's Health Initiative (WHI) enrolled a total of 27,000 predominantly healthy postmenopausal women to assess the risks and benefits of either the use of 0.625 mg conjugated estrogens (CE) per day alone or the use of oral 0.625 mg conjugated estrogens plus 2.5 mg medroxyprogesterone acetate (MPA) per day compared to placebo in the prevention of certain chronic diseases. The primary endpoint was the incidence of coronary heart disease (CHD) (nonfatal myocardial infarction and CHD death), with invasive breast cancer as the primary adverse outcome studied. A "global index" included the earliest occurrence of CHD, invasive breast cancer, stroke, pulmonary embolism (PE), endometrial cancer, colorectal cancer, hip fracture, or death due to other cause. The study did not evaluate the effects of CE or CE/MPA on menopausal symptoms.
The CE/MPA substudy was stopped early because, according to the predefined stopping rule, the increased risk of breast cancer and cardiovascular events exceeded the specified benefits included in the "global index." Results of the CE/MPA substudy, which included 16,608 women (average age of 63 years, range 50 to 79; 83.9% White, 6.5% Black, 5.5% Hispanic), after an average follow-up of 5.2 years are presented in Table 1 below:
Table 1: RELATIVE AND ABSOLUTE RISK SEEN IN THE CE/MPA SUBSTUDY OF WHIa Event c Relative Risk Placebo CE/MPA
CE/MPA vs. placebo n=8102 N=8506
at 5.2 Years Absolute Risk per 10,000
(95% CI*) Person-years CHD events 1.29 (1.02-1.63) 30 37 Non -fatal MI 1.32 (1.02-1.72) 23 30 CHD death 1.18 (0.70-1.97) 6 7 Invasive breast cancerb 1.26 (1.00-1.59) 30 38 Stroke 1.41 (1.07-1.85) 21 29 Pulmonary embolism 2.13 (1.39-3.25) 8 16 Colorectal cancer 0.63 (0.43-0.92) 16 10 Endometrial cancer 0.83 (0.47-1.47) 6 5 Hip fracture 0.66 (0.45-0.98) 15 10 Death due to causes 0.92 (0.74-1.14) 40 37 other than the events above
Global indexc 1.15 (1.03-1.28) 151 170 Deep vein thrombosisd 2.07 (1.49-2.87) 13 26 Vertebral fracturesd 0.66 (0.44-0.98) 15 9 Other osteoporotic fracturesd 0.77 (0.69-0.86) 170 131 a adapted from JAMA, 2002; 288:321-333 b includes metastatic and non-metastatic breast cancer with the exception of in situ breast cancer c a subset of the events was combined in a “global index,” defined as the earliest occurrence of CHD events, invasive breast cancer, stroke, pulmonary embolism, endometrial cancer, colorectal cancer, hip fracture, or death due to other causes d not included in Global Index * nominal confidence intervals unadjusted for multiple looks and multiple comparisons For those outcomes included in the "global index," the absolute excess risks per 10,000 person-years in the group treated with CE/MPA were 7 more CHD events, 8 more strokes, 8 more PEs, and 8 more invasive breast cancers, while absolute risk reductions per 10,000 person-years were 6 fewer colorectal cancers and 5 fewer hip fractures. The absolute excess risk of events included in the "global index" was 19 per 10,000 women-years. There was no difference between the groups in terms of all-cause mortality. (See BOXED WARNINGS, WARNINGS and PRECAUTIONS.)
Women’s Health Initiative Memory StudyThe Women’s Health Initiative Memory Study (WHIMS), a substudy of WHI, enrolled 4,532 predominantly healthy postmenopausal women 65 years of age and older (47% were age 65 to 69 years, 35% were 70 to 74 years, and 18% were 75 years of age and older) to evaluate the effects of CE/MPA (0.625mg conjugated estrogens plus 2.5 mg medroxyprogesterone acetate) on the incidence of probable dementia (primary outcome) compared with placebo.
After an average follow-up of 4 years, 40 women in the estrogen/progestin group (45 per 10,000 women-years) and 21 in the placebo group (22 per 10,000 women-years) were diagnosed with probable dementia. The relative risk of probable dementia in the hormone therapy group was 2.05 (95% CI, 1.21 to 3.48) compared to placebo. Differences between groups became apparent in the first year of treatment. It is unknown whether these findings apply to younger postmenopausal women. (See BOXED WARNINGS and WARNINGS, Dementia.)
OsteoporosisThe results of a double-blind, placebo-controlled two-year study have shown that treatment with one tablet of estropipate 0.625 daily for 25 days (of a 31-day cycle per month) prevents vertebral bone mass loss in postmenopausal women. When estrogen therapy is discontinued, bone mass declines at a rate comparable to that of the immediate postmenopausal period. There is no evidence that estrogen replacement therapy restores to premenopausal levels.
-
INDICATIONS AND USAGE
Estropipate tablets are indicated in the:
-
Treatment of moderate to severe vasomotor symptoms associated with the menopause.
-
Treatment of moderate to severe symptoms of vulval and vaginal atrophy associated with the menopause. When prescribing solely for the treatment of symptoms of vulvar and vaginal atrophy, topical vaginal products should be considered.
-
Treatment of hypoestrogenism due to hypogonadism, castration or primary ovarian failure.
-
Prevention of postmenopausal osteoporosis. When prescribing solely for the prevention of postmenopausal osteoporosis, therapy should only be considered for women at significant risk of osteoporosis and for whom non-estrogen medications are not considered to be appropriate.
The mainstays for decreasing the risk of postmenopausal osteoporosis are weight-bearing exercise, adequate calcium and vitamin D intake, and when indicated, pharmacologic therapy. Postmenopausal women require an average of 1500 mg/day of elemental calcium. Therefore, when not contraindicated, calcium supplementation may be helpful for women with suboptimal dietary intake. Vitamin D supplementation of 400-800 IU/day may also be required to ensure adequate daily intake in postmenopausal women.
-
-
CONTRAINDICATIONS
Estropipate tablets should not be used in women with any of the following conditions:
-
Undiagnosed abnormal genital bleeding.
-
Known, suspected, or history of cancer of the breast.
-
Known or suspected estrogen-dependent neoplasia.
-
Active deep vein thrombosis, pulmonary embolism or history of these conditions.
-
Active or recent (e.g., within the past year) arterial thromboembolic disease (e.g., stroke, myocardial infarction).
-
Liver dysfunction or disease.
-
Estropipate tablets should not be used in patients with known hypersensitivity to its ingredients.
-
Known or suspected pregnancy. There is no indication for estropipate tablets in pregnancy.
There appears to be little or no increased risk of birth defects in children born to women who have used estrogens and progestins from oral contraceptives inadvertently during early pregnancy. (See PRECAUTIONS.)
-
-
WARNINGS
See BOXED WARNINGS
1. Cardiovascular disorders
Estrogen and estrogen/progestin therapy have been associated with an increased risk of cardiovascular events such as myocardial infarction and stroke, as well as venous thrombosis and pulmonary embolism (venous thromboembolism or VTE). Should any of these occur or be suspected, estrogens should be discontinued immediately.
Risk factors for arterial vascular disease (e.g., hypertension, diabetes mellitus, tobacco use, hypercholesterolemia, and obesity) and/or venous thromboembolism (e.g., personal history or family history of VTE, obesity, and systemic lupus erythematosus) should be managed appropriately.
a. Coronary heart disease and strokeIn the Women’s Health Initiative (WHI) study, an increase in the number of myocardial infarctions and strokes has been observed in women receiving CE compared to placebo. These observations are preliminary, and the study is continuing. (See CLINICAL PHARMACOLOGY, Clinical Studies.)
In the CE/MPA substudy of WHI, an increased risk of coronary heart disease (CHD) events (defined as nonfatal myocardial infarction and CHD death) was observed in women receiving CE/MPA compared to women receiving placebo (37 vs. 30 per 10,000 women-years). The increase in risk was observed in year one and persisted.
In the same substudy of WHI, an increased risk of stroke was observed in women receiving CE/MPA compared to women receiving placebo (29 vs. 21 per 10,000 women-years). The increase in risk was observed after the first year and persisted.
In postmenopausal women with documented heart disease (n = 2,763, average age 66.7 years) a controlled clinical trial of secondary prevention of cardiovascular disease (Heart and Estrogen/Progestin Replacement Study; HERS) treatment with CE/MPA (0.625 mg/2.5 mg per day) demonstrated no cardiovascular benefit. During an average follow-up of 4.1 years, treatment with CE/MPA did not reduce the overall rate of CHD events in postmenopausal women with established coronary heart disease. There were more CHD events in the CE/MPA-treated group than in the placebo group in year 1, but not during the subsequent years. Two thousand three hundred and twenty one women from the original HERS trial agreed to participate in an open label extension of HERS, HERS II. Average follow-up in HERS II was an additional 2.7 years, for a total of 6.8 years overall. Rates of CHD events were comparable among women in the CE/MPA group and the placebo group in HERS, HERS II, and overall.
Large doses of estrogen (5 mg conjugated estrogens per day), comparable to those used to treat cancer of the prostate and breast, have been shown in a large prospective clinical trial in men to increase the risks of nonfatal myocardial infarction, pulmonary embolism, and thrombophlebitis.
b. Venous thromboembolism (VTE)In the Women’s Health study (WHI) an increase in VTE has been observed in women receiving CE compared to placebo. These observations are preliminary, and the study is continuing.
In the CE/MPA treatment substudy of WHI, a 2-fold greater rate of VTE, including deep venous thrombosis and pulmonary embolism, was observed in women receiving treatment with CE/MPA compared to women receiving placebo. The rate of VTE was 34 per 10,000 woman-years in the CE/MPA group compared to 16 per 10,000 woman-years in the placebo group. The increase in VTE risk was observed during the first year and persisted.
If feasible, estrogens should be discontinued at least 4 to 6 weeks before surgery of the type associated with an increased risk of thromboembolism, or during periods of prolonged immobilization.
2. Malignant neoplasms
a. Endometrial cancerThe use of unopposed estrogens in women with intact uteri has been associated with an increased risk of endometrial cancer. The reported endometrial cancer risk among unopposed estrogen users is about 2–to-12 fold greater than in nonusers, and appears dependent on duration of treatment and on estrogen dose. Most studies show no significant increased risk associated with use of estrogens for less than one year. The greatest risk appears associated with prolonged use, with increased risks of 15–to-24 fold for five to ten years or more and this risk has been shown to persist for at least 8 to 15 years after estrogen therapy is discontinued.
Clinical surveillance of all women taking estrogen/progestin combinations is important. Adequate diagnostic measures, including endometrial sampling when indicated, should be undertaken to rule out malignancy in all cases of undiagnosed persistent or recurring abnormal vaginal bleeding. There is no evidence that the use of natural estrogens results in a different endometrial risk profile than synthetic estrogens of equivalent estrogen dose. Adding a progestin to estrogen therapy has been shown to reduce the risk of endometrial hyperplasia, which may be a precursor to endometrial cancer.
b. Breast cancerThe use of estrogens and progestins by postmenopausal women has been reported to increase the risk of breast cancer. The most important randomized clinical trial providing information about this issue is the Women’s Health Initiative (WHI) substudy of CE/MPA (see CLINICAL PHARMACOLOGY, Clinical Studies). The results from observational studies are generally consistent with those of the WHI clinical trial and report no significant variation in the risk of breast cancer among different estrogens or progestins, doses, or routes of administration.
The CE/MPA substudy of WHI reported an increased risk of breast cancer in women who took CE/MPA for a mean follow-up of 5.6 years. Observational studies have also reported an increased risk for estrogen/progestin combination therapy, and a smaller increased risk for estrogen alone therapy, after several years of use. In the WHI trial and from observational studies, the excess risk increased with duration of use. From observational studies, the risk appeared to return to baseline in about five years after stopping treatment. In addition, observational studies suggest that the risk of breast cancer was greater, and became apparent earlier, with estrogen/progestin combination therapy as compared to estrogen alone therapy.
In the CE/MPA substudy, 26% of the women reported prior use of estrogen alone and/or estrogen/progestin combination hormone therapy. After a mean follow-up of 5.6 years during the clinical trial, the overall relative risk of invasive breast cancer was 1.24 (95% confidence interval 1.01-1.54), and the overall absolute risk was 41 vs. 33 cases per 10,000 women-years, for CE/MPA compared with placebo. Among women who reported prior use of hormone therapy, the relative risk of invasive breast cancer was 1.86, and the absolute risk was 46 vs. 25 cases per 10,000 women-years, for CE/MPA compared with placebo. Among women who reported no prior use of hormone therapy, the relative risk of invasive breast cancer was 1.09, and the absolute risk was 40 vs. 36 cases per 10,000 women-years for CE/MPA compared with placebo. In the same substudy, invasive breast cancers were larger and diagnosed at a more advanced stage in the CE/MPA group compared with the placebo group. Metastatic disease was rare with no apparent difference between the two groups. Other prognostic factors such as histologic subtype, grade and hormone receptor status did not differ between groups.
The use of estrogen plus progestin has been reported to result in an increase in abnormal mammograms requiring further evaluation. All women should receive yearly breast examinations by a health care provider and perform monthly breast self-examinations. In addition, mammography examinations should be scheduled based on patient age, risk factors, and prior mammogram results.
3. Dementia
In the Women’s Health Initiative Memory Study (WHIMS), 4,532 generally healthy postmenopausal women 65 years of age and older were studied, of whom 35% were 70 to 74 years of age and 18% were 75 or older. After an average follow-up of 4 years, 40 women being treated with CE/MPA (1.8%, n= 2,229) and 21 women in the placebo group (0.9%, n= 2,303) received diagnoses of probable dementia. The relative risk for CE/MPA versus placebo was 2.05 (95% confidence interval 1.21 – 3.48), and was similar for women with and without histories of menopausal hormone use before WHIMS. The absolute risk of probable dementia for CE/MPA versus placebo was 45 versus 22 cases per 10,000 women-years. It is unknown whether these findings apply to younger postmenopausal women. (See CLINICAL PHARMACOLOGY, Clinical Studies and PRECAUTIONS, Geriatric Use.)
4. Gallbladder disease
A 2- to 4-fold increase in the risk of gallbladder disease requiring surgery in postmenopausal women receiving estrogens has been reported.
5. Hypercalcemia
Estrogen administration may lead to severe hypercalcemia in patients with breast cancer and bone metastases. If hypercalcemia occurs, use of the drug should be stopped and appropriate measures taken to reduce the serum calcium level.
6. Visual abnormalities
Retinal vascular thrombosis has been reported in patients receiving estrogens. Discontinue medication pending examination if there is sudden partial or complete loss of vision, or a sudden onset of proptosis, diplopia, or migraine. If examination reveals papilledema or retinal vascular lesions, estrogens should be permanently discontinued.
-
PRECAUTIONS
Enter section text here
A. GENERAL
1. Addition of a progestin when a woman has not had a hysterectomyStudies of the addition of a progestin for 10 or more days of a cycle of estrogen administration, or daily with estrogen in a continuous regimen, have reported a lowered incidence of endometrial hyperplasia than would be induced by estrogen treatment alone. Endometrial hyperplasia may be a precursor to endometrial cancer.
There are, however, possible risks that may be associated with the use of progestins with estrogens compared to estrogen-alone regimens. These include a possible increased risk of breast cancer, adverse effects on lipoprotein metabolism (e.g., lowering HDL, raising LDL) and impairment of glucose tolerance.
2. Elevated blood pressureIn a small number of case reports, substantial increases in blood pressure have been attributed to idiosyncratic reactions to estrogens. In a large, randomized, placebo-controlled clinical trial, a generalized effect of estrogens on blood pressure was not seen. Blood pressure should be monitored at regular intervals with estrogen use.
3. HypertriglyceridemiaIn patients with pre-existing hypertriglyceridemia, estrogen therapy may be associated with elevations of plasma triglycerides leading to pancreatitis and other complications.
4. Impaired liver function and past history of cholestatic jaundiceEstrogens may be poorly metabolized in patients with impaired liver function. For patients with a history of cholestatic jaundice associated with past estrogen use or with pregnancy, caution should be exercised and in the case of recurrence, medication should be discontinued.
5. HypothyroidismEstrogen administration leads to increased thyroid-binding globulin (TBG) levels. Patients with normal thyroid function can compensate for the increased TBG by making more thyroid hormone, thus maintaining free T4 and T3 serum concentrations in the normal range. Patients dependent on thyroid hormone replacement therapy who are also receiving estrogens may require increased doses of their thyroid replacement therapy. These patients should have their thyroid function monitored in order to maintain their free thyroid hormone levels in an acceptable range.
6. Fluid retentionBecause estrogens may cause some degree of fluid retention, patients with conditions that might be influenced by this factor, such as a cardiac or renal dysfunction, warrant careful observation when estrogens are prescribed.
7. HypocalcemiaEstrogens should be used with caution in individuals with severe hypocalcemia.
8. Ovarian cancerThe CE/MPA substudy of WHI reported that estrogen plus progestin increased the risk of ovarian cancer. After an average follow-up of 5.6 years, the relative risk for ovarian cancer for CE/MPA versus placebo was 1.58 (95% confidence interval 0.77 – 3.24) but was not statistically significant. The absolute risk for CE/MPA versus placebo was 4.2 versus 2.7 cases per 10,000 women-years. In some epidemiologic studies, the use of estrogen alone, in particular for ten or more years, has been associated with an increased risk of ovarian cancer. Other epidemiologic studies have not found these associations.
9. Exacerbation of endometriosisEndometriosis may be exacerbated with administration of estrogens. A few cases of malignant transformation of residual endometrial implants have been reported in women treated post-hysterectomy with estrogen alone therapy. For patients known to have residual endometriosis post-hysterectomy, the addition of progestin should be considered.
10. Exacerbation of other conditionsEstrogens may cause an exacerbation of asthma, diabetes mellitus, epilepsy, migraine or porphyria, systemic lupus erythematosus, and hepatic hemangiomas and should be used with caution in women with these conditions.
B. PATIENT INFORMATION
Physicians are advised to discuss the PATIENT INFORMATION leaflet with patients for whom they prescribe estropipate tablets.
C. LABORATORY TESTS
Estrogen administration should be initiated at the lowest dose approved for the indication and then guided by clinical response rather than by serum hormone levels (e.g., estradiol, FSH).
D. DRUG/ LABORATORY TEST INTERACTIONS
-
Accelerated prothrombin time, partial thromboplastin time, and platelet aggregation time; increased platelet count; increased factors II, VII antigen, VIII antigen, VIII coagulant activity, IX, X, XII, VII— X complex, II—VII—X complex, and beta-thromboglobulin; decreased levels of anti-factor Xa and antithrombin III, decreased antithrombin III activity; increased levels of fibrinogen and fibrinogen activity; increased plasminogen antigen and activity.
-
Increased thyroid-binding globulin (TBG) levels leading to increased circulating total thyroid hormone, levels as measured by protein-bound iodine (PBI), T4 levels (by column or by radioimmunoassay) or T3 levels by radioimmunoassay. T3 resin uptake is decreased, reflecting the elevated TBG. Free T4 and free T3 concentrations are unaltered. Patients on thyroid replacement therapy may require higher doses of thyroid hormone.
-
Other binding proteins may be elevated in serum, (i.e., corticosteroid binding globulin (CBG), sex hormone-binding globulin (SHBG), leading to increased circulating corticosteroids and sex steroids, respectively. Free or biologically active hormone concentrations are unchanged. Other plasma proteins may be increased (angiotensinogen/renin substrate, alpha-1-antitrypsin, ceruloplasmin).
-
Increased plasma HDL and HDL2 subfraction concentrations, reduced LDL cholesterol concentration, increased triglycerides levels.
-
Impaired glucose tolerance.
-
Reduced response to metyrapone test.
-
Reduced serum folate concentration.
E. CARCINOGENESIS, MUTAGENESIS, IMPAIRMENT OF FERTILITY
Long-term continuous administration of estrogen, with and without progestin, in women with and without a uterus, has shown an increased risk of endometrial cancer, breast cancer, and ovarian cancer. (See BOXED WARNINGS, WARNINGS, and PRECAUTIONS.)
Long-term continuous administration of natural and synthetic estrogens in certain animal species increases the frequency of carcinomas of the breast, uterus, cervix, vagina, testis, and liver.
G. NURSING MOTHERS
Estrogen administration to nursing mothers has been shown to decrease the quantity and quality of the milk. Detectable amounts of estrogens have been identified in the milk of mothers receiving this drug. Caution should be exercised when estropipate is administered to a nursing woman.
H. GERIATRIC USE
In the Women’s Health Initiative Memory Study, including 4,532 women 65 years of age and older, followed for an average of 4 years, 82% (n= 3,729) were 65 to 74 while 18% (n= 803) were 75 and over. Most women (80%) had no prior hormone therapy use. Women treated with conjugated estrogens plus medroxyprogesterone acetate were reported to have a two-fold increase in the risk of developing probable dementia. Alzheimer’s disease was the most common classification of probable dementia in both the conjugated estrogens plus medroxyprogesterone acetate group and the placebo group. Ninety percent of the cases of probable dementia occurred in the 54% of women that were older than 70. (See WARNINGS, Dementia.)
-
-
ADVERSE REACTIONS
See BOXED WARNINGS, WARNINGS and PRECAUTIONS.
The following additional adverse reactions have been reported with estrogens and/or progestin therapy.
1. Genitourinary system
Changes in vaginal bleeding pattern and abnormal withdrawal bleeding or flow; breakthrough bleeding; spotting; dysmenorrhea; increase in size of uterine leiomyomata; vaginitis; including vaginal candidiasis; change in amount of cervical secretion; changes in cervical ectropion; ovarian cancer; endometrial hyperplasia; endometrial cancer.
2. Breasts
Tenderness, enlargement, pain, nipple discharge, galactorrhea; fibrocystic breast changes; breast cancer.
3. Cardiovascular
Deep and superficial venous thrombosis; pulmonary embolism; thrombophlebitis; myocardial infarction; stroke; increase in blood pressure.
4. Gastrointestinal
Nausea, vomiting; abdominal cramps, bloating; cholestatic jaundice; increased incidence of gallbladder disease; pancreatitis; enlargement of hepatic hemangiomas.
5. Skin
Chloasma or melasma that may persist when drug is discontinued; erythema multiforme; erythema nodosum; hemorrhagic eruption; loss of scalp hair; hirsutism; pruritus, rash.
6. Eyes
Retinal vascular thrombosis; steepening of corneal curvature; intolerance to contact lenses.
- OVERDOSAGE
-
DOSAGE AND ADMINISTRATION
When estrogen is prescribed for a woman with a uterus, progestin should also be initiated to reduce the risk of endometrial cancer. A woman without a uterus does not need progestin. Use of estrogen, alone or in combination with a progestin, should be with the lowest effective dose and for the shortest duration consistent with treatment goals and risks for the individual woman. Patients should be reevaluated periodically as clinically appropriate (e.g., 3-month to 6-month intervals) to determine if treatment is still necessary (See BOXED WARNINGS and WARNINGS.) For women who have a uterus, adequate diagnostic measures, such as endometrial sampling, when indicated, should be undertaken to rule out malignancy in cases of undiagnosed persistent or recurring abnormal vaginal bleeding.
-
For treatment of moderate to severe vasomotor symptoms, vulval and vaginal atrophy associated with the menopause, the lowest dose and regimen that will control symptoms should be chosen and medication should be discontinued as promptly as possible. Attempts to discontinue or taper medication should be made at 3month to 6-month intervals. Usual dosage ranges:
Vasomotor symptoms—One estropipate 0.75 mg tablet to two estropipate 3 mg tablets per day. The lowest dose that will control symptoms should be chosen. If the patient has not menstruated within the last two months or more, cyclic administration is started arbitrarily. If the patient is menstruating, cyclic administration is started on day 5 of bleeding.
Vulval and vaginal atrophy—One estropipate 0.75 mg tablet to two estropipate 3 mg tablets daily, depending upon the tissue response of the individual patient. The lowest dose that will control symptoms should be chosen. Administer cyclically.
-
For treatment of female hypoestrogenism due to hypogonadism, castration, or primary ovarian failure. Usual dosage ranges:
Female hypogonadism—A daily dose of one estropipate 1.5 mg tablet to three estropipate 3 mg tablets may be given for the first three weeks of a theoretical cycle, followed by a rest period of eight to ten days. The lowest dose that will control symptoms should be chosen. If bleeding does not occur by the end of this period, the same dosage schedule is repeated. The number of courses of estrogen therapy necessary to produce bleeding may vary depending on the responsiveness of the endometrium. If satisfactory withdrawal bleeding does not occur, an oral progestogen may be given in addition to estrogen during the third week of the cycle.
Female castration or primary ovarian failure—A daily dose of one estropipate 1.5 mg tablet to three estropipate 3 mg tablets may be given for the first three weeks of a theoretical cycle, followed by a rest period of eight to ten days. Adjust dosage upward or downward according to severity of symptoms and response of the patient. For maintenance, adjust dosage to lowest level that will provide effective control.
Treated patients with an intact uterus should be monitored closely for signs of endometrial cancer and appropriate diagnostic measures should be taken to rule out malignancy in the event of persistent or recurring abnormal vaginal bleeding.
-
For prevention of osteoporosis. A daily dose of one estropipate 0.75 mg tablet for 25 days of a 31-day cycle per month.
-
-
HOW SUPPLIED
Estropipate tablets USP are supplied as follows:
Store at 20° - 25°C (68° - 77°F). [See USP controlled room temperature.]- 0.75 mg Estropipate (calculated as sodium estrone sulfate 0.625 mg) as round, scored, yellow tablets, in:
bottles of 100 NDC 54868-3114-1
- 1.5 mg Estropipate (calculated as sodium estrone sulfate 1.25 mg) as round, scored, peach tablets, in:
bottles of 100 NDC 54868-4149-1
- 3 mg Estropipate (calculated as sodium estrone sulfate 2.5 mg) as round, scored, blue tablets, in:
bottles of 60 NDC 54868-4761-2
-
SUPPLEMENTAL PATIENT MATERIAL
PATIENT INFORMATION
Estropipate Tablets USP
Read this PATIENT INFORMATION before you start taking estropipate tablets and read what you get each time you refill estropipate tablets. There may be new information. This information does not take the place of talking to your health care provider about your medical condition or your treatment.
WHAT IS THE MOST IMPORTANT INFORMATION I SHOULD KNOW ABOUT ESTROPIPATE (AN ESTROGEN HORMONE)? • Estrogens increase the chances of getting cancer of the uterus.
Report any unusual vaginal bleeding right away while you are taking estrogens. Vaginal bleeding after menopause may be a warning sign of cancer of the uterine (womb). Your health care provider should check any unusual vaginal bleeding to find out the cause.
• Do not use estrogens with or without progestins to prevent heart disease, heart attacks or strokes.
Using estrogens with or without progestins may increase your chances of getting heart attacks, strokes, breast cancer and blood clots. You and your health care provider should talk regularly about whether you still need treatment with estropipate tablets.
What is estropipate?
Estropipate is a medicine that contains estrogen hormones.
What is estropipate used for?
Estropipate is used during and after menopause to:
-
reduce moderate or severe hot flashes.
Estrogens are hormones made by a woman’s ovaries. The ovaries normally stop making estrogens when a woman is between 45 to 55 years old. This drop in body estrogen levels causes the “change of life” or menopause (the end of monthly menstrual periods). Sometimes, both ovaries are removed during an operation before natural menopause takes place. The sudden drop in estrogen levels causes “surgical menopause”.
When the estrogen levels begin dropping, some women develop very uncomfortable symptoms, such as feelings of warmth in the face, neck, and chest, or sudden strong feelings of heat and sweating (“hot flashes” or “hot flushes”). In some women, the symptoms are mild, and they do not need to use estrogens. In other women, symptoms can be more severe. You and your health care provider should talk regularly about whether you still need treatment with estropipate tablets.
-
treat moderate to severe dryness, itching, and burning in and around the vagina.
You and your health care provider should talk regularly about whether you still need treatment with estropipate tablets to control these problems. If you use estropipate tablets only to treat your dryness, itching, and burning in and around your vagina, talk with your health care provider about whether a topical vaginal product would be better for you.
-
help reduce your chances of getting osteoporosis (thin weak bones).
Osteoporosis from menopause is a thinning of the bones that makes them weaker and easier to break. If you use estropipate tablets only to prevent osteoporosis from menopause, talk with your health care provider about whether a different treatment or medicine without estrogens might be better for you. You and your health care provider should talk regularly about whether you should continue with estropipate tablets.
Weight-bearing exercise, like walking or running, and taking calcium and vitamin D supplements may also lower your chances of getting postmenopausal osteoporosis. It is important to talk about exercise and supplements with your health care provider before starting them.
Estropipate is also used to:
treat certain conditions in women before menopause if their ovaries do not make enough estrogen naturally.
Who should not take estropipate tablets?
Do not start taking estropipate tablets if you:
-
have unusual vaginal bleeding.
-
currently have or have had certain cancers.
Estrogens may increase the chances of getting certain types of cancers, including cancer of the breast or uterus. If you have or had cancer, talk with your health care provider about whether you should take estropipate tablets.
-
had a stroke or heart attack in the past year.
-
currently have or have had blood clots.
-
currently have or have had liver problems.
-
are allergic to estropipate tablets or any of its ingredients.
See the end of this leaflet for a list of ingredients in estropipate tablets.
-
think you may be pregnant.
Tell your health care provider:
-
if you are breastfeeding.
The hormone in estropipate tablets can pass into your milk.
-
about all of your medical problems.
Your health care provider may need to check you more carefully if you have certain conditions, such as asthma (wheezing), epilepsy (seizures), migraine, endometriosis, or problems with your heart, liver, thyroid, kidneys, or have high calcium levels in your blood.
-
about all the medicines you take.
This includes prescription and nonprescription medicines, vitamins, and herbal supplements. Some medicines may affect how estropipate works. Estropipate may also affect how your other medicines work.
-
if you are going to have surgery or will be on bed rest.
You may need to stop taking estrogens.
How should I take estropipate tablets?
Take estropipate tablets as directed by your health care provider. Estropipate comes in four strengths. Check with your health care provider periodically to make sure you are using the appropriate dose.
Estropipate Tablets USP
Revised April 2006
Rx only
1. Start at the lowest dose and talk to your health care provider about how well that dose is working for you.
2. Estrogens should be used at the lowest dose possible for your treatment only as long as needed. The lowest effective dose of estropipate has not been determined. You and your health care provider should talk regularly (for example, every 3 to 6 months) about whether you still need treatment with estropipate tablets.
What are the possible side effects of estrogens?
Less common but serious side effects include:
-
Breast cancer
-
Cancer of the uterus
-
Stroke
-
Heart attack
-
Blood clots
-
Gallbladder disease
-
Ovarian cancer
These are some of the warning signs of serious side effects:
-
Breast lumps
-
Unusual vaginal bleeding
-
Dizziness and faintness
-
Changes in speech
-
Severe headaches
-
Chest pain
-
Shortness of breath
-
Pains in your legs
-
Changes in vision
-
Vomiting
Call your health care provider right away if you get any of these warning signs, or any other unusual symptom that concerns you.
Common side effects include:
-
Headache
-
Breast pain
-
Irregular vaginal bleeding or spotting
-
Stomach/abdominal cramps, bloating
-
Nausea and vomiting
Other side effects include:
-
High blood pressure
-
Liver problems
-
High blood sugar
-
Fluid retention
-
Enlargement of benign tumors of the uterus (“fibroids”)
-
Vaginal yeast infections
-
Hair loss
These are not all the possible side effects of estropipate tablets. For more information, ask your health care provider or pharmacist.
What can I do to lower my chances of getting a serious side effect with estropipate tablets?
Talk with your health care provider regularly about whether you should continue taking estropipate tablets. If you have a uterus, talk to your health care provider about whether the addition of a progestin is right for you. See your health care provider right away if you get vaginal bleeding while taking estropipate tablets. Have a breast exam and mammogram (breast X-ray) every year unless your health care provider tells you something else. If members of your family have had breast cancer or if you have ever had breast lumps or an abnormal mammogram, you may need to have breast examinations more often. If you have high blood pressure, high cholesterol (fat in the blood), diabetes, are overweight, or if you use tobacco, you may have higher chances for getting heart disease. Ask your health care provider for ways to lower your chances for getting heart disease.
General information about safe and effective use of estropipate
Medicines are sometimes prescribed for conditions that are not mentioned in patient information leaflets. Do not take estropipate for conditions for which it was not prescribed. Do not give estropipate tablets to other people, even if they have the same symptoms you have. It may harm them. Keep estropipate tablets out of the reach of children.
This leaflet provides a summary of the most important information about estropipate tablets. If you would like more information, talk with your health care provider or pharmacist. You can ask for information about estropipate tablets that is written for health professionals. You can get more information by calling the toll free number 1-800-272-5525.
What are the ingredients in estropipate tablets?
Estropipate tablets contain estropipate as the active ingredient. Estropipate tablets also contain: lactose NF, magnesium stearate NF, piperazine USP, pregelatinized starch NF, talc USP, and coloring agents: 0.75 mg—D&C Yellow #10; 1.5 mg—FD&C Yellow #6; 3 mg— FD&C Blue #2; 6 mg—FD&C Blue #2 and D&C Yellow #10.
Watson Laboratories, Inc.
Corona, CA 92880 USA
12270-4
Revised April 2006
Relabeling and Repackaging by:
Physicians Total Care, Inc.
Tulsa, OK 74146
-
- PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
ESTROPIPATE
estropipate tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:54868-3114(NDC:52544-414) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength ESTROPIPATE (UNII: SVI38UY019) (ESTROPIPATE - UNII:SVI38UY019) ESTROPIPATE 0.75 mg Inactive Ingredients Ingredient Name Strength MAGNESIUM STEARATE (UNII: 70097M6I30) LACTOSE (UNII: J2B2A4N98G) PIPERAZINE (UNII: 1RTM4PAL0V) STARCH, CORN (UNII: O8232NY3SJ) TALC (UNII: 7SEV7J4R1U) D&C YELLOW NO. 10 (UNII: 35SW5USQ3G) Product Characteristics Color yellow Score 2 pieces Shape ROUND Size 3mm Flavor Imprint Code Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:54868-3114-0 30 in 1 BOTTLE 2 NDC:54868-3114-1 100 in 1 BOTTLE Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA081213 03/21/2003 ESTROPIPATE
estropipate tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:54868-4149(NDC:52544-415) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength ESTROPIPATE (UNII: SVI38UY019) (ESTROPIPATE - UNII:SVI38UY019) ESTROPIPATE 1.5 mg Inactive Ingredients Ingredient Name Strength MAGNESIUM STEARATE (UNII: 70097M6I30) LACTOSE (UNII: J2B2A4N98G) PIPERAZINE (UNII: 1RTM4PAL0V) STARCH, CORN (UNII: O8232NY3SJ) TALC (UNII: 7SEV7J4R1U) FD&C YELLOW NO. 6 (UNII: H77VEI93A8) Product Characteristics Color brown Score 2 pieces Shape ROUND Size 5mm Flavor Imprint Code Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:54868-4149-0 30 in 1 BOTTLE 2 NDC:54868-4149-1 100 in 1 BOTTLE Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA081214 03/21/2003 ESTROPIPATE
estropipate tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:54868-4761(NDC:52544-416) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength ESTROPIPATE (UNII: SVI38UY019) (ESTROPIPATE - UNII:SVI38UY019) ESTROPIPATE 3 mg Inactive Ingredients Ingredient Name Strength MAGNESIUM STEARATE (UNII: 70097M6I30) LACTOSE (UNII: J2B2A4N98G) PIPERAZINE (UNII: 1RTM4PAL0V) STARCH, CORN (UNII: O8232NY3SJ) TALC (UNII: 7SEV7J4R1U) FD&C BLUE NO. 2 (UNII: L06K8R7DQK) Product Characteristics Color blue Score 2 pieces Shape ROUND Size 5mm Flavor Imprint Code Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:54868-4761-1 30 in 1 BOTTLE 2 NDC:54868-4761-2 60 in 1 BOTTLE Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA081215 03/26/2003 Labeler - Physicians Total Care, Inc. (194123980) Establishment Name Address ID/FEI Business Operations Physicians Total Care, Inc. 194123980 relabel, repack