Label: LEVOTHYROXINE SODIUM tablet

- NDC Code(s): 82804-168-30
- Packager: Proficient Rx LP
- This is a repackaged label.
- Source NDC Code(s): 16729-447
- Category: HUMAN PRESCRIPTION DRUG LABEL
Drug Label Information
Updated December 1, 2024
If you are a healthcare professional or from the pharmaceutical industry please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use LEVOTHYROXINE SODIUM TABLETS safely and effectively. See full prescribing information for LEVOTHYROXINE SODIUM TABLETS.
LEVOTHYROXINE SODIUM tablets, for oral use
Initial U.S. Approval: 2002WARNING: NOT FOR TREATMENT OF OBESITY OR FOR WEIGHT LOSS
See full prescribing information for complete boxed warning
RECENT MAJOR CHANGES
INDICATIONS AND USAGE
Levothyroxine sodium tablets are a L-thyroxine (T4) indicated in adult and pediatric patients, including neonates, for:
- •
- Hypothyroidism: As replacement therapy in primary (thyroidal), secondary (pituitary), and tertiary (hypothalamic) congenital or acquired hypothyroidism. (1)
- •
- Pituitary Thyrotropin (Thyroid‑Stimulating Hormone, TSH) Suppression: As an adjunct to surgery and radioiodine therapy in the management of thyrotropin-dependent well-differentiated thyroid cancer. (1)
Limitations of Use:
- •
- Not indicated for suppression of benign thyroid nodules and nontoxic diffuse goiter in iodine-sufficient patients
- •
- Not indicated for treatment of hypothyroidism during the recovery phase of subacute thyroiditis
DOSAGE AND ADMINISTRATION
- •
- Administer once daily, preferably on an empty stomach, one-half to one hour before breakfast with a full glass of water. (2.1)
- •
- Administer at least 4 hours before or after drugs that are known to interfere with absorption. (2.1)
- •
- Evaluate the need for dose adjustments when regularly administering within one hour of certain foods that may affect absorption. (2.1)
- •
- Starting dose depends on a variety of factors, including age, body weight, cardiovascular status, and concomitant medications. Peak therapeutic effect may not be attained for 4 to 6 weeks. (2.2)
- •
- See full prescribing information for dosing in specific patient populations. (2.3)
- •
- Adequacy of therapy determined with periodic monitoring of TSH and/or T4 as well as clinical status. (2.4)
DOSAGE FORMS AND STRENGTHS
Tablets (Functional Scoring): 25 mcg (3)
CONTRAINDICATIONS
- •
- Uncorrected adrenal insufficiency. (4)
WARNINGS AND PRECAUTIONS
- •
- Serious risks related to overtreatment or undertreatment with levothyroxine sodium tablets:Titrate the dose of levothyroxine sodium carefully and monitor response to titration. (5.1)
- •
- Cardiac adverse reactions in the elderly and in patients with underlying cardiovascular disease:Initiate levothyroxine sodium at less than the full replacement dose because of the increased risk of cardiac adverse reactions, including atrial fibrillation. (2.3, 5.2, 8.5)
- •
- Myxedema coma:Do not use oral thyroid hormone drug products to treat myxedema coma. (5.3)
- •
- Acute adrenal crisis in patients with concomitant adrenal insufficiency:Treat with replacement glucocorticoids prior to initiation of levothyroxine sodium treatment. (5.4)
- •
- Worsening of diabetic control:Therapy in patients with diabetes mellitus may worsen glycemic control and result in increased antidiabetic agent or insulin requirements. Carefully monitor glycemic control after starting, changing, or discontinuing thyroid hormone therapy. (5.5)
- •
- Decreased bone mineral density associated with thyroid hormone over-replacement:Over-replacement can increase bone resorption and decrease bone mineral density. Give the lowest effective dose. (5.6)
ADVERSE REACTIONS
Adverse reactions associated with levothyroxine sodium therapy are primarily those of hyperthyroidism due to therapeutic overdosage: arrhythmias, myocardial infarction, dyspnea, muscle spasm, headache, nervousness, irritability, insomnia, tremors, muscle weakness, increased appetite, weight loss, diarrhea, heat intolerance, menstrual irregularities, and skin rash. (6)
To report SUSPECTED ADVERSE REACTIONS, contact Accord Healthcare Inc. at 1-866-941-7875 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
See full prescribing information for drugs that affect thyroid hormone pharmacokinetics and metabolism (e.g., absorption, synthesis, secretion, catabolism, protein binding, and target tissue response) and may alter the therapeutic response to levothyroxine sodium. (7)
USE IN SPECIFIC POPULATIONS
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 12/2024
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: NOT FOR TREATMENT OF OBESITY OR FOR WEIGHT LOSS
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Important Administration Instructions
2.2 Important Considerations for Dosing
2.3 Recommended Dosage and Titration
2.4 Monitoring TSH and/or Thyroxine (T4) Levels
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Serious Risks Related to Overtreatment or Undertreatment with Levothyroxine Sodium Tablets
5.2 Cardiac Adverse Reactions in the Elderly and in Patients with Underlying Cardiovascular Disease
5.3 Myxedema Coma
5.4 Acute Adrenal Crisis in Patients with Concomitant Adrenal Insufficiency
5.5 Worsening of Diabetic Control
5.6 Decreased Bone Mineral Density Associated with Thyroid Hormone Over-Replacement
5.7 Risk of Allergic Reactions Due to Tartrazine
6 ADVERSE REACTIONS
7 DRUG INTERACTIONS
7.1 Drugs Known to Affect Thyroid Hormone Pharmacokinetics
7.2 Antidiabetic Therapy
7.3 Oral Anticoagulants
7.4 Digitalis Glycosides
7.5 Antidepressant Therapy
7.6 Ketamine
7.7 Sympathomimetics
7.8 Tyrosine-Kinase Inhibitors
7.9 Drug-Food Interactions
7.10 Drug-Laboratory Test Interactions
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
BOXED WARNING
(What is this?)
WARNING: NOT FOR TREATMENT OF OBESITY OR FOR WEIGHT LOSS
- •
- Thyroid hormones, including levothyroxine sodium, either alone or with other therapeutic agents, should not be used for the treatment of obesity or for weight loss.
- •
- In euthyroid patients, doses within the range of daily hormonal requirements are ineffective for weight reduction.
- •
- Larger doses may produce serious or even life-threatening manifestations of toxicity, particularly when given in association with sympathomimetic amines such as those used for their anorectic effects [see Adverse Reactions (6), Drug Interactions (7.7), and Overdosage (10)].
-
1 INDICATIONS AND USAGE
Hypothyroidism
Levothyroxine sodium tablets are indicated in adult and pediatric patients, including neonates, as a replacement therapy in primary (thyroidal), secondary (pituitary), and tertiary (hypothalamic) congenital or acquired hypothyroidism.
Pituitary Thyrotropin (Thyroid‑Stimulating Hormone, TSH) Suppression
Levothyroxine sodium tablets are indicated in adult and pediatric patients, including neonates, as an adjunct to surgery and radioiodine therapy in the management of thyrotropin-dependent well-differentiated thyroid cancer.
Limitations of Use:
- •
- Levothyroxine sodium tablets are not indicated for suppression of benign thyroid nodules and nontoxic diffuse goiter in iodine-sufficient patients as there are no clinical benefits and overtreatment with levothyroxine sodium may induce hyperthyroidism [see Warnings and Precautions(5.1)].
- •
- Levothyroxine sodium tablets are not indicated for treatment of hypothyroidism during the recovery phase of subacute thyroiditis.
-
2 DOSAGE AND ADMINISTRATION
2.1 Important Administration Instructions
Administer levothyroxine sodium tablets as a single daily dose, on an empty stomach, one-half to one hour before breakfast with a full glass of water to avoid choking or gagging [see Adverse Reactions (6)].
Administer levothyroxine sodium tablets at least 4 hours before or after drugs known to interfere with levothyroxine sodium absorption [see Drug Interactions (7.1)].
Evaluate the need for dosage adjustments when regularly administering within one hour of certain foods that may affect levothyroxine sodium tablets absorption [see Dosage and Administration (2.2and 2.3), Drug Interactions (7.9)and Clinical Pharmacology (12.3)].
Administer levothyroxine sodium tablets to pediatric patients who cannot swallow intact tablets by crushing the tablet, suspending the freshly crushed tablet in a small amount (5 to 10 mL) of water and immediately administering the suspension by spoon or dropper. Ensure the patient ingests the full amount of the suspension. Do not store the suspension. Do not administer in foods that decrease absorption of levothyroxine sodium tablets, such as soybean-based infant formula [see Drug Interactions (7.9)].
2.2 Important Considerations for Dosing
The dosage of levothyroxine sodium tablets for hypothyroidism or pituitary TSH suppression depends on a variety of factors including: the patient's age, body weight, cardiovascular status, concomitant medical conditions (including pregnancy), concomitant medications, co-administered food and the specific nature of the condition being treated [see Dosage and Administration (2.3), Warnings and Precautions (5), and Drug Interactions (7)] . Dosing must be individualized to account for these factors and dosage adjustments made based on periodic assessment of the patient's clinical response and laboratory parameters [see Dosage and Administration (2.4)].
For adult patients with primary hypothyroidism, titrate until the patient is clinically euthyroid and the serum TSH returns to normal [see Dosage and Administration (2.3)].
For secondary or tertiary hypothyroidism, serum TSH is not a reliable measure of levothyroxine sodium dosage adequacy and should not be used to monitor therapy. Use the serum free-T4 level to titrate levothyroxine sodium tablets dosing until the patient is clinically euthyroid and the serum free-T4 level is restored to the upper half of the normal range [see Dosage and Administration (2.3)].
The peak therapeutic effect of a given dose of levothyroxine sodium tablets may not be attained for 4 to 6 weeks.
2.3 Recommended Dosage and Titration
Primary, Secondary, and Tertiary Hypothyroidism in Adults
The recommended starting daily dosage of levothyroxine sodium tablets in adults with primary, secondary, or tertiary hypothyroidism is based on age and comorbid cardiac conditions, as described in Table 1. For patients at risk of atrial fibrillation or patients with underlying cardiac disease, start with a lower dosage and titrate the dosage more slowly to avoid exacerbation of cardiac symptoms. Dosage titration is based on serum TSH or free-T4 [see Dosage and Administration (2.2)].
Table 1. Levothyroxine Sodium Tablets Dosing Guidelines for Hypothyroidism in Adults* *Dosages greater than 200 mcg/day are seldom required. An inadequate response to daily dosages greater than 300 mcg/day is rare and may indicate poor compliance, malabsorption, drug interactions, or a combination of these factors [see Dosage and Administration (2.1)and Drug Interactions (7)]. Patient Population
Starting Dosage
Dosage Titration Based on serum TSH or Free-T4
Adults diagnosed with hypothyroidism
Full replacement dose is 1.6 mcg/kg/day.
Some patients require a lower starting dose.Titrate dosage by 12.5 to 25 mcg increments every 4 to 6 weeks, as needed until the patient is euthyroid.
Adults at risk for atrial fibrillation or with underlying cardiac disease
Lower starting dose (less than 1.6 mcg/kg/day)
Titrate dosage every 6 to 8 weeks, as needed until the patient is euthyroid.
Geriatric patients
Lower starting dose (less than 1.6 mcg/kg/day)
Primary, Secondary, and Tertiary Hypothyroidism in Pediatric Patients
The recommended starting daily dosage of levothyroxine sodium tablets in pediatric patients with primary, secondary, or tertiary hypothyroidism is based on body weight and changes with age as described in Table 2. Titrate the dosage (every 2 weeks) as needed based on serum TSH or free-T4 until the patient is euthyroid [see Dosage and Administration (2.2)].
Table 2. Levothyroxine Sodium Tablets Dosing Guidelines for Hypothyroidism in Pediatric Patients Age
Starting Daily Dosage Per Kg Body Weight*
0 to 3 months
10 to 15 mcg/kg/day
3 to 6 months
8 to 10 mcg/kg/day
6 to 12 months
6 to 8 mcg/kg/day
1 to 5 years
5 to 6 mcg/kg/day
6 to 12 years
4 to 5 mcg/kg/day
Greater than 12 years but growth and puberty incomplete
2 to 3 mcg/kg/day
Growth and puberty complete
1.6 mcg/kg/day
*Adjust dosage based on clinical response and laboratory parameters [see Dosage and Administration (2.4) and Use in Specific Populations (8.4)] .
Pediatric Patients from Birth to 3 Months of Age at Risk for Cardiac Failure
Start at a lower starting dosage and increase the dosage every 4 to 6 weeks as needed based on clinical and laboratory response.
Pediatric Patients at Risk for Hyperactivity
To minimize the risk of hyperactivity, start at one-fourth the recommended full replacement dosage, and increase on a weekly basis by one-fourth the full recommended replacement dosage until the full recommended replacement dosage is reached.
Hypothyroidism in Pregnant Patients
For pregnant patients with pre-existing hypothyroidism, measure serum TSH and free-T4 as soon as pregnancy is confirmed and, at minimum, during each trimester of pregnancy. In pregnant patients with primary hypothyroidism, maintain serum TSH in the trimester-specific reference range.
The recommended daily dosage of levothyroxine sodium tablets in pregnant patients is described in Table 3.
Table 3. Levothyroxine Sodium Tablet Dosing Guidelines for Hypothyroidism in Pregnant Patients Patient Population
Starting Dosage
Dose Adjustment and Titration
Pre-existing primary hypothyroidism with serum TSH above normal trimester- specific range
Pre-pregnancy dosage may increase during pregnancy
Increase levothyroxine sodium dosage by 12.5 to 25 mcg per day. Monitor TSH every 4 weeks until a stable dose is reached and serum TSH is within normal trimester-specific range. Reduce levothyroxine sodium dosage to pre-pregnancy levels immediately after delivery. Monitor serum TSH 4 to 8 weeks postpartum.
New onset hypothyroidism (TSH ≥10 IU per liter)
1.6 mcg/kg/day
Monitor serum TSH every 4 weeks and adjust levothyroxine sodium dosage until serum TSH is within normal trimester-specific range.
New onset hypothyroidism (TSH < 10 IU per liter)
1.0 mcg/kg/day
TSH Suppression in Well-differentiated Thyroid Cancer in Adult and Pediatric Patients
The levothyroxine sodium dosage is based on the target level of TSH suppression for the stage and clinical status of thyroid cancer.
2.4 Monitoring TSH and/or Thyroxine (T4) Levels
Assess the adequacy of therapy by periodic assessment of laboratory tests and clinical evaluation. Persistent clinical and laboratory evidence of hypothyroidism despite an apparent adequate replacement dose of levothyroxine sodium may be evidence of inadequate absorption, poor compliance, drug interactions, or a combination of these factors.
Adults
In adult patients with primary hypothyroidism, monitor serum TSH levels after an interval of 6 to 8 weeks after any change in dosage. In patients on a stable and appropriate replacement dosage, evaluate clinical and biochemical response every 6 to 12 months and whenever there is a change in the patient’s clinical status.
Pediatric Patients
In patients with hypothyroidism, assess the adequacy of replacement therapy by measuring both serum TSH and total or free-T4. Monitor TSH and total or free-T4 in pediatric patients as follows: 2 and 4 weeks after the initiation of treatment, 2 weeks after any change in dosage, and then every 3 to 12 months thereafter following dosage stabilization until growth is completed. Poor compliance or abnormal values may necessitate more frequent monitoring. Perform routine clinical examination, including assessment of development, mental and physical growth, and bone maturation, at regular intervals.
The general aim of therapy is to normalize the serum TSH level. TSH may not normalize in some patients due to in utero hypothyroidism causing a resetting of pituitary-thyroid feedback. Failure of the serum T4 to increase into the upper half of the normal range within 2 weeks of initiation of levothyroxine sodium therapy and/or of the serum TSH to decrease below 20 IU per litre within 4 weeks may indicate the patient is not receiving adequate therapy. Assess compliance, dose of medication administered, and method of administration prior to increasing the dose of levothyroxine sodium [see Warnings and Precautions (5.1)and Use in Specific Populations (8.4)] .
-
3 DOSAGE FORMS AND STRENGTHS
All tablets having functional scoring
Levothyroxine sodium tablets USP are available as follows (Table 4):
Table 4: Levothyroxine Sodium Tablet Strengths and Identifying Features Tablet Strength
Tablet Description
25 mcg
Round shaped, Orange colored, uncoated tablets, break line on both side and debossed with "P" and "1" on one side and plain on other side.
-
4 CONTRAINDICATIONS
Levothyroxine sodium tablets are contraindicated in patients with uncorrected adrenal insufficiency [see Warnings and Precautions (5.4)].
-
5 WARNINGS AND PRECAUTIONS
5.1 Serious Risks Related to Overtreatment or Undertreatment with Levothyroxine Sodium Tablets
Levothyroxine sodium tablets has a narrow therapeutic index. Overtreatment or undertreatment with levothyroxine sodium tablets may have negative effects on growth and development, cardiovascular function, bone metabolism, reproductive function, cognitive function, gastrointestinal function, and glucose and lipid metabolism in adult or pediatric patients.
In pediatric patients with congenital and acquired hypothyroidism, undertreatment may adversely affect cognitive development and linear growth, and overtreatment is associated with craniosynostosis and acceleration of bone age [Use in Specific Populations (8.4)].
Titrate the dose of levothyroxine sodium tablets carefully and monitor response to titration to avoid these effects [see Dosage and Administration (2.4)]. Consider the potential for food or drug interactions and adjust the administration or dosage of levothyroxine sodium tablets as needed [see Dosage and Administration (2.1), Drug Interactions (7.1), and Clinical Pharmacology (12.3)].
5.2 Cardiac Adverse Reactions in the Elderly and in Patients with Underlying Cardiovascular Disease
Over-treatment with levothyroxine may cause an increase in heart rate, cardiac wall thickness, and cardiac contractility and may precipitate angina or arrhythmias, particularly in patients with cardiovascular disease and in elderly patients. Initiate levothyroxine sodium therapy in this population at lower doses than those recommended in younger individuals or in patients without cardiac disease [see Dosage and Administration (2.3), Use in Specific Populations (8.5)] .
Monitor for cardiac arrhythmias during surgical procedures in patients with coronary artery disease receiving suppressive levothyroxine sodium therapy. Monitor patients receiving concomitant levothyroxine sodium and sympathomimetic agents for signs and symptoms of coronary insufficiency.
If cardiac symptoms develop or worsen, reduce the levothyroxine sodium tablets dose or withhold for one week and restart at a lower dose.
5.3 Myxedema Coma
Myxedema coma is a life-threatening emergency characterized by poor circulation and hypometabolism and may result in unpredictable absorption of levothyroxine sodium from the gastrointestinal tract. Use of oral thyroid hormone drug products is not recommended to treat myxedema coma. Administer thyroid hormone products formulated for intravenous administration to treat myxedema coma.
5.4 Acute Adrenal Crisis in Patients with Concomitant Adrenal Insufficiency
Thyroid hormone increases metabolic clearance of glucocorticoids. Initiation of thyroid hormone therapy prior to initiating glucocorticoid therapy may precipitate an acute adrenal crisis in patients with adrenal insufficiency. Treat patients with adrenal insufficiency with replacement glucocorticoids prior to initiating treatment with levothyroxine sodium [see Contraindications (4)] .
5.5 Worsening of Diabetic Control
Addition of levothyroxine therapy in patients with diabetes mellitus may worsen glycemic control and result in increased antidiabetic agent or insulin requirements. Carefully monitor glycemic control after starting, changing, or discontinuing levothyroxine sodium [see Drug Interactions (7.2)] .
5.6 Decreased Bone Mineral Density Associated with Thyroid Hormone Over-Replacement
Increased bone resorption and decreased bone mineral density may occur as a result of levothyroxine over-replacement, particularly in post-menopausal women. The increased bone resorption may be associated with increased serum levels and urinary excretion of calcium and phosphorous, elevations in bone alkaline phosphatase, and suppressed serum parathyroid hormone levels. Administer the minimum dose of levothyroxine sodium that achieves the desired clinical and biochemical response to mitigate this risk.
5.7 Risk of Allergic Reactions Due to Tartrazine
This product contains FD&C Yellow No. 5 (tartrazine) which may cause allergic-type reactions (including bronchial asthma) in certain susceptible persons. Although the overall incidence of FD&C Yellow No. 5 (tartrazine) sensitivity in the general population is low, it is frequently seen in patients who also have aspirin hypersensitivity.
-
6 ADVERSE REACTIONS
Adverse reactions associated with levothyroxine sodium therapy are primarily those of hyperthyroidism due to therapeutic overdosage [see Warnings and Precautions (5), Overdosage (10)] . They include the following:
- •
- General:fatigue, increased appetite, weight loss, heat intolerance, fever, excessive sweating
- •
- Central nervous system:headache, hyperactivity, nervousness, anxiety, irritability, emotional lability, insomnia
- •
- Musculoskeletal:tremors, muscle weakness, muscle spasm
- •
- Cardiovascular:palpitations, tachycardia, arrhythmias, increased pulse and blood pressure, heart failure, angina, myocardial infarction, cardiac arrest
- •
- Respiratory:dyspnea
- •
- Gastrointestinal:diarrhea, vomiting, abdominal cramps, elevations in liver function tests
- •
- Dermatologic:hair loss, flushing, rash
- •
- Endocrine:decreased bone mineral density
- •
- Reproductive:menstrual irregularities, impaired fertility
Seizures have been reported rarely with the institution of levothyroxine therapy.
Adverse Reactions in Pediatric Patients
Pseudotumor cerebri and slipped capital femoral epiphysis have been reported in pediatric patients receiving levothyroxine therapy. Overtreatment may result in craniosynostosis in infants who have not undergone complete closure of the fontanelles, and in premature closure of the epiphyses in pediatric patients still experiencing growth with resultant compromised adult height.
Hypersensitivity Reactions
Hypersensitivity reactions to inactive ingredients have occurred in patients treated with thyroid hormone products. These include urticaria, pruritus, skin rash, flushing, angioedema, various gastrointestinal symptoms (abdominal pain, nausea, vomiting and diarrhea), fever, arthralgia, serum sickness, and wheezing. Hypersensitivity to levothyroxine itself is not known to occur.
-
7 DRUG INTERACTIONS
7.1 Drugs Known to Affect Thyroid Hormone Pharmacokinetics
Many drugs can exert effects on thyroid hormone pharmacokinetics and metabolism (e.g., absorption, synthesis, secretion, catabolism, protein binding, and target tissue response) and may alter the therapeutic response to levothyroxine sodium (Tables 5 to 8).
Table 5. Drugs That May Decrease T4 Absorption (Hypothyroidism) Potential impact: Concurrent use may reduce the efficacy of levothyroxine sodium by binding and delaying or preventing absorption, potentially resulting in hypothyroidism.
Drug or Drug Class
Effect
Phosphate Binders
(e.g., calcium carbonate, ferrous sulfate, sevelamer, lanthanum)Phosphate binders may bind to levothyroxine. Administer levothyroxine sodium tablets at least 4 hours apart from these agents.
Orlistat
Monitor patients treated concomitantly with orlistat and levothyroxine sodium for changes in thyroid function.
Bile Acid Sequestrants
(e.g., colesevelam, cholestyramine, colestipol)
Ion Exchange Resins
(e.g., Kayexalate)Bile acid sequestrants and ion exchange resins are known to decrease levothyroxine absorption. Administer levothyroxine sodium tablets at least 4 hours prior to these drugs or monitor TSH levels.
Proton Pump Inhibitors
Sucralfate
Antacids
(e.g., aluminum & magnesium hydroxides, simethicone)Gastric acidity is an essential requirement for adequate absorption of levothyroxine. Sucralfate, antacids and proton pump inhibitors may cause hypochlorhydria, affect intragastric pH, and reduce levothyroxine absorption. Monitor patients appropriately.
Table 6. Drugs That May Alter T4 and Triiodothyronine (T3) Serum Transport Without Affecting Free Thyroxine (FT4) Concentration (Euthyroidism) Drug or Drug Class
Effect
Clofibrate
Estrogen-containing oral contraceptives
Estrogens (oral)
Heroin / Methadone
5-Fluorouracil
Mitotane
TamoxifenThese drugs may increase serum thyroxine-binding globulin (TBG) concentration.
Androgens / Anabolic Steroids
Asparaginase
Glucocorticoids
Slow-Release Nicotinic AcidThese drugs may decrease serum TBG concentration.
Potential impact (below): Administration of these agents with levothyroxine sodium results in an initial transient increase in FT4. Continued administration results in a decrease in serum T4 and normal FT4 and TSH concentrations.
Salicylates (> 2 g/day)
Salicylates inhibit binding of T4 and T3 to TBG and transthyretin. An initial increase in serum FT4 is followed by return of FT4 to normal levels with sustained therapeutic serum salicylate concentrations, although total T4 levels may decrease by as much as 30%.
Other drugs:
Carbamazepine
Furosemide (> 80 mg IV)
Heparin
Hydantoins
Non-Steroidal Anti-inflammatory Drugs
- FenamatesThese drugs may cause protein-binding site displacement. Furosemide has been shown to inhibit the protein binding of T4 to TBG and albumin, causing an increase free T4 fraction in serum. Furosemide competes for T4-binding sites on TBG, prealbumin, and albumin, so that a single high dose can acutely lower the total T4 level. Phenytoin and carbamazepine reduce serum protein binding of levothyroxine, and total and free T4 may be reduced by 20% to 40%, but most patients have normal serum TSH levels and are clinically euthyroid. Closely monitor thyroid hormone parameters.
Table 7. Drugs That May Alter Hepatic Metabolism of T4 (Hypothyroidism) Potential impact: Stimulation of hepatic microsomal drug-metabolizing enzyme activity may cause increased hepatic degradation of levothyroxine, resulting in increased levothyroxine sodium requirements.
Drug or Drug Class
Effect
Phenobarbital
RifampinPhenobarbital has been shown to reduce the response to thyroxine. Phenobarbital increases L-thyroxine metabolism by inducing uridine 5’-diphospho-glucuronosyltransferase (UGT) and leads to a lower T4 serum levels. Changes in thyroid status may occur if barbiturates are added or withdrawn from patients being treated for hypothyroidism. Rifampin has been shown to accelerate the metabolism of levothyroxine.
Table 8. Drugs That May Decrease Conversion of T4 to T3 Potential impact: Administration of these enzyme inhibitors decreases the peripheral conversion of T4 to T3, leading to decreased T3 levels. However, serum T4 levels are usually normal but may occasionally be slightly increased.
Drug or Drug Class
Effect
Beta-adrenergic antagonists
(e.g., Propranolol > 160 mg/day)In patients treated with large doses of propranolol (> 160 mg/day), T3 and T4 levels change, TSH levels remain normal, and patients are clinically euthyroid. Actions of particular beta-adrenergic antagonists may be impaired when a hypothyroid patient is converted to the euthyroid state.
Glucocorticoids
(e.g., Dexamethasone ≥4 mg/day)Short-term administration of large doses of glucocorticoids may decrease serum T3 concentrations by 30% with minimal change in serum T4 levels. However, long-term glucocorticoid therapy may result in slightly decreased T3 and T4 levels due to decreased TBG production (See above).
Other drugs:
AmiodaroneAmiodarone inhibits peripheral conversion of levothyroxine (T4) to triiodothyronine (T3) and may cause isolated biochemical changes (increase in serum free-T4, and decreased or normal free-T3) in clinically euthyroid patients.
7.2 Antidiabetic Therapy
Addition of levothyroxine sodium therapy in patients with diabetes mellitus may worsen glycemic control and result in increased antidiabetic agent or insulin requirements. Carefully monitor glycemic control, especially when thyroid therapy is started, changed, or discontinued [see Warnings and Precautions (5.5)] .
7.3 Oral Anticoagulants
Levothyroxine sodium increases the response to oral anticoagulant therapy. Therefore, a decrease in the dose of anticoagulant may be warranted with correction of the hypothyroid state or when the levothyroxine sodium dose is increased. Closely monitor coagulation tests to permit appropriate and timely dosage adjustments.
7.4 Digitalis Glycosides
Levothyroxine sodium may reduce the therapeutic effects of digitalis glycosides. Serum digitalis glycoside levels may decrease when a hypothyroid patient becomes euthyroid, necessitating an increase in the dose of digitalis glycosides.
7.5 Antidepressant Therapy
Concurrent use of tricyclic (e.g., amitriptyline) or tetracyclic (e.g., maprotiline) antidepressants and levothyroxine sodium may increase the therapeutic and toxic effects of both drugs, possibly due to increased receptor sensitivity to catecholamines. Toxic effects may include increased risk of cardiac arrhythmias and central nervous system stimulation. Levothyroxine sodium may accelerate the onset of action of tricyclics. Administration of sertraline in patients stabilized on levothyroxine sodium may result in increased levothyroxine sodium requirements.
7.6 Ketamine
Concurrent use of ketamine and levothyroxine sodium may produce marked hypertension and tachycardia. Closely monitor blood pressure and heart rate in these patients.
7.7 Sympathomimetics
Concurrent use of sympathomimetics and levothyroxine sodium may increase the effects of sympathomimetics or thyroid hormone. Thyroid hormones may increase the risk of coronary insufficiency when sympathomimetic agents are administered to patients with coronary artery disease.
7.8 Tyrosine-Kinase Inhibitors
Concurrent use of tyrosine-kinase inhibitors such as imatinib may cause hypothyroidism. Closely monitor TSH levels in such patients.
7.9 Drug-Food Interactions
Consumption of certain foods may affect levothyroxine sodium absorption thereby necessitating adjustments in dosing [see Dosage and Administration (2.1)] . Soybean flour, cottonseed meal, walnuts, and dietary fiber may bind and decrease the absorption of levothyroxine sodium from the gastrointestinal tract. Grapefruit juice may delay the absorption of levothyroxine and reduce its bioavailability.
7.10 Drug-Laboratory Test Interactions
Consider changes in TBG concentration when interpreting T4 and T3 values. Measure and evaluate unbound (free) hormone and/or determine the free-T4 index (FT4I) in this circumstance. Pregnancy, infectious hepatitis, estrogens, estrogen-containing oral contraceptives, and acute intermittent porphyria increase TBG concentration. Nephrosis, severe hypoproteinemia, severe liver disease, acromegaly, androgens, and corticosteroids decrease TBG concentration. Familial hyper- or hypo-thyroxine binding globulinemias have been described, with the incidence of TBG deficiency approximating 1 in 9000.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
The clinical experience, including data from postmarketing studies, in pregnant women treated with oral levothyroxine to maintain euthyroid state have not reported increased rates of major birth defects, miscarriages, or other adverse maternal or fetal outcomes. There are risks to the mother and fetus associated with untreated hypothyroidism in pregnancy. Since TSH levels may increase during pregnancy, TSH should be monitored and levothyroxine sodium dosage adjusted during pregnancy (see Clinical Considerations). Animal reproductive studies have not been conducted with levothyroxine sodium. Levothyroxine sodium should not be discontinued during pregnancy and hypothyroidism diagnosed during pregnancy should be promptly treated.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Disease-Associated Maternal and/or Embryo/Fetal Risk
Maternal hypothyroidism during pregnancy is associated with a higher rate of complications, including spontaneous abortion, gestational hypertension, pre‑eclampsia, stillbirth, and premature delivery. Untreated maternal hypothyroidism may have an adverse effect on fetal neurocognitive development.
Dose Adjustments During Pregnancy and the Postpartum Period
Pregnancy may increase levothyroxine sodium requirements. Serum TSH levels should be monitored and the levothyroxine sodium dosage adjusted during pregnancy. Since postpartum TSH levels are similar to preconception values, the levothyroxine sodium dosage should return to the pre-pregnancy dose immediately after delivery [see Dosage and Administration Error! Hyperlink reference not valid.].
8.2 Lactation
Risk Summary
Published studies report that levothyroxine is present in human milk following the administration of oral levothyroxine. No adverse effects on the breastfed infant have been reported there is no information on the effects of levothyroxine on milk production. Adequate levothyroxine treatment during lactation may normalize milk production in hypothyroid lactating mothers with low milk supply. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for levothyroxine sodium and any potential adverse effects on the breastfed infant from levothyroxine sodium or from the underlying maternal condition
8.4 Pediatric Use
Levothyroxine sodium is indicated in patients from birth to less than 17 years of age:
- •
- As a replacement therapy in primary (thyroidal), secondary (pituitary), and tertiary (hypothalamic) congenital or acquired hypothyroidism.
- •
- As an adjunct to surgery and radioiodine therapy in the management of thyrotropin-dependent well-differentiated thyroid cancer.
Rapid restoration of normal serum T4 concentrations is essential for preventing the adverse effects of congenital hypothyroidism on cognitive development as well as on overall physical growth and maturation. Therefore, initiate levothyroxine sodium therapy immediately upon diagnosis. Levothyroxine is generally continued for life in these patients [see Warnings and Precautions Error! Hyperlink reference not valid.].
Closely monitor infants during the first 2 weeks of levothyroxine sodium therapy for cardiac overload, arrhythmias.
8.5 Geriatric Use
Because of the increased prevalence of cardiovascular disease among the elderly, initiate levothyroxine sodium at less than the full replacement dose [see Dosage and Administration (2.3)and Warnings and Precautions (5.2)] . Atrial arrhythmias can occur in elderly patients. Atrial fibrillation is the most common of the arrhythmias observed with levothyroxine overtreatment in the elderly.
-
10 OVERDOSAGE
The signs and symptoms of overdosage are those of hyperthyroidism [see Warnings and Precautions (5)and Adverse Reactions (6)] . In addition, confusion and disorientation may occur. Cerebral embolism, shock, coma, and death have been reported. Seizures occurred in a 3-year-old child ingesting 3.6 mg of levothyroxine. Symptoms may not necessarily be evident or may not appear until several days after ingestion of levothyroxine sodium.
Reduce the levothyroxine sodium dosage or discontinue temporarily if signs or symptoms of overdosage occur. Initiate appropriate supportive treatment as dictated by the patient’s medical status.
For current information on the management of poisoning or overdosage, contact the National Poison Control Center at 1-800-222-1222 or www.poison.org.
-
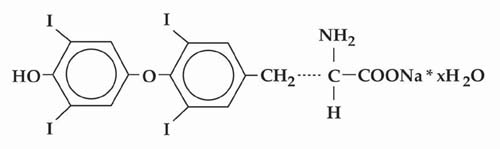
11 DESCRIPTION
Levothyroxine sodium tablets, USP is L-thyroxine (T4) and contains synthetic crystalline L-3,3’,5,5’-tetraiodothyronine sodium salt. Synthetic T4 is chemically identical to that produced in the human thyroid gland. Levothyroxine (T4) sodium has an empirical formula of C 15H 10I 4N NaO 4• H 2O, molecular weight of 798.86 (anhydrous), and structural formula as shown:
Levothyroxine sodium tablets, USP for oral administration are supplied in the following strengths: 25 mcg, 50 mcg, 75 mcg, 88 mcg, 100 mcg, 112 mcg, 125 mcg, 137 mcg, 150 mcg, 175 mcg, 200 mcg, and 300 mcg. Each levothyroxine sodium tablet contains the inactive ingredients microcrystalline sodium, light magnesium oxide, sodium starch glycolate and sodium stearyl fumarate.
Levothyroxine sodium tablets, USP contain no ingredients made from a gluten-containing grain (wheat, barley, or rye). Table 9 provides a listing of the color additives by tablet strength:
Table 9. Levothyroxine Sodium Tablet Color Additives Strength
(mcg)Color additive(s)
25
FD&C Yellow No. 6 Aluminum Lake
50
None
75
FD&C Red No. 40 Aluminum Lake, FD&C Blue No. 2 Aluminum Lake
88
FD&C Blue No. 2 Aluminum Lake, FD&C Yellow No. 5 Aluminum Lake
100
FD&C Yellow No. 5 Aluminum Lake, FD&C Yellow No. 6 Aluminum Lake
112
FD&C Red No. 40 Aluminum Lake, Carmine
125
FD&C Yellow No. 6 Aluminum Lake, FD&C Red No. 40 Aluminum Lake, FD&C Blue No. 1 Aluminum Lake
137
FD&C Blue No. 1 Aluminum Lake
150
FD&C Blue No. 2 Aluminum Lake
175
FD&C Blue No. 1 Aluminum Lake, Carmine
200
FD&C Red No. 40 Aluminum Lake
300
D&C Yellow No. 10 Aluminum Lake, FD&C Yellow No. 6 Aluminum Lake, FD&C Blue No. 1 Aluminum Lake
Levothyroxine sodium tablets, USP meets USP Dissolution Test 7.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Thyroid hormones exert their physiologic actions through control of DNA transcription and protein synthesis. Triiodothyronine (T3) and L-thyroxine (T4) diffuse into the cell nucleus and bind to thyroid receptor proteins attached to DNA. This hormone nuclear receptor complex activates gene transcription and synthesis of messenger RNA and cytoplasmic proteins.
The physiological actions of thyroid hormones are produced predominantly by T3, the majority of which (approximately 80%) is derived from T4 by deiodination in peripheral tissues.
12.2 Pharmacodynamics
Oral levothyroxine sodium is a synthetic T4 hormone that exerts the same physiologic effect as endogenous T4, thereby maintaining normal T4 levels when a deficiency is present.
12.3 Pharmacokinetics
Absorption
Absorption of orally administered T4 from the gastrointestinal tract ranges from 40% to 80%. The majority of the levothyroxine sodium dose is absorbed from the jejunum and upper ileum. The relative bioavailability of levothyroxine sodium tablets, compared to an equal nominal dose of oral levothyroxine sodium solution, is approximately 93%. T4 absorption is increased by fasting, and decreased in malabsorption syndromes and by certain foods such as soybeans. Dietary fiber decreases bioavailability of T4. Absorption may also decrease with age. In addition, many drugs and foods affect T4 absorption [see Drug Interactions (7)] .
Distribution
Circulating thyroid hormones are greater than 99% bound to plasma proteins, including thyroxine-binding globulin (TBG), thyroxine-binding prealbumin (TBPA), and albumin (TBA), whose capacities and affinities vary for each hormone. The higher affinity of both TBG and TBPA for T4 partially explains the higher serum levels, slower metabolic clearance, and longer half-life of T4 compared to T3. Protein-bound thyroid hormones exist in reverse equilibrium with small amounts of free hormone. Only unbound hormone is metabolically active. Many drugs and physiologic conditions affect the binding of thyroid hormones to serum proteins [see Drug Interactions (7)] . Thyroid hormones do not readily cross the placental barrier [see Use in Specific Populations (8.1)] .
Elimination
Metabolism
T4 is slowly eliminated (see Table 10). The major pathway of thyroid hormone metabolism is through sequential deiodination. Approximately 80% of circulating T3 is derived from peripheral T4 by monodeiodination. The liver is the major site of degradation for both T4 and T3, with T4 deiodination also occurring at a number of additional sites, including the kidney and other tissues. Approximately 80% of the daily dose of T4 is deiodinated to yield equal amounts of T3 and reverse T3 (rT3). T3 and rT3 are further deiodinated to diiodothyronine. Thyroid hormones are also metabolized via conjugation with glucuronides and sulfates and excreted directly into the bile and gut where they undergo enterohepatic recirculation.
Excretion
Thyroid hormones are primarily eliminated by the kidneys. A portion of the conjugated hormone reaches the colon unchanged and is eliminated in the feces. Approximately 20% of T4 is eliminated in the stool. Urinary excretion of T4 decreases with age.
Table 10. Pharmacokinetic Parameters of Thyroid Hormones in Euthyroid Patients Hormone
Ratio in Thyroglobulin
Biologic Potency
t 1/2(days)
Protein Binding (%) *
Levothyroxine (T4)
10 to 20
1
6 to 7 **
99.96
Liothyronine (T3)
1
4
≤ 2
99.5
*Includes TBG, TBPA, and TBA
** 3 to 4 days in hyperthyroidism, 9 to 10 days in hypothyroidism - 13 NONCLINICAL TOXICOLOGY
-
16 HOW SUPPLIED/STORAGE AND HANDLING
All tablets having functional scoring.
Levothyroxine sodium, USP tablets are supplied as follows (Table 11):
Table 11: Levothyroxine Sodium Tablet Presentations Strength
(mcg)Tablet Description
NDC# for bottles with child-resistant closure of 90
25
Round shaped, Orange colored, uncoated tablets, break line on both side and debossed with "P" and "1" on one side and plain on other side.
82804-168-30
Storage Conditions
Store levothyroxine sodium tablets at 20°C to 25°C (68°F to 77°F); excursions permitted to 15°C to 30°C (59°F to 86°F) (see USP Controlled Room Temperature).
Levothyroxine sodium tablets should be protected from light and moisture.
-
17 PATIENT COUNSELING INFORMATION
Inform the patient of the following information to aid in the safe and effective use of Levothyroxine sodium tablets:
Dosing and Administration
- •
- Instruct patients to take levothyroxine sodium tablets only as directed by their healthcare provider.
- •
- Instruct patients to take levothyroxine sodium tablets as a single dose, preferably on an empty stomach, one-half to one hour before breakfast with a full glass of water to avoid choking or gagging.
- •
- Inform patients that agents such as iron and calcium supplements and antacids can decrease the absorption of levothyroxine. Instruct patients not to take levothyroxine sodium tablets within 4 hours of these agents.
- •
- Instruct patients to notify their healthcare provider if they are pregnant or breastfeeding or are thinking of becoming pregnant while taking levothyroxine sodium tablets.
Important Information
- •
- Inform patients that it may take several weeks before they notice an improvement in symptoms.
- •
- Inform patients that the levothyroxine in levothyroxine sodium tablets is intended to replace a hormone that is normally produced by the thyroid gland. Generally, replacement therapy is to be taken for life.
- •
- Inform patients that levothyroxine sodium tablets should not be used as a primary or adjunctive therapy in a weight control program.
- •
- Instruct patients to notify their healthcare provider if they are taking any other medications, including prescription and over-the-counter preparations.
- •
- Instruct patients to notify their physician of any other medical conditions they may have, particularly heart disease, diabetes, clotting disorders, and adrenal or pituitary gland problems, as the dose of medications used to control these other conditions may need to be adjusted while they are taking levothyroxine sodium tablets. If they have diabetes, instruct patients to monitor their blood and/or urinary glucose levels as directed by their physician and immediately report any changes to their physician. If patients are taking anticoagulants, their clotting status should be checked frequently.
- •
- Instruct patients to notify their physician or dentist that they are taking levothyroxine sodium tablets prior to any surgery.
Adverse Reactions
- •
- Instruct patients to notify their healthcare provider if they experience any of the following symptoms: rapid or irregular heartbeat, chest pain, shortness of breath, leg cramps, headache, nervousness, irritability, sleeplessness, tremors, change in appetite, weight gain or loss, vomiting, diarrhea, excessive sweating, heat intolerance, fever, changes in menstrual periods, hives or skin rash, or any other unusual medical event.
- •
- Inform patients that partial hair loss may occur rarely during the first few months of levothyroxine sodium tablets therapy, but this is usually temporary.
Manufactured For:
Accord Healthcare, Inc.,
8041 Arco Corporate Drive,
Suite 200,
Raleigh, NC 27617,
USA.Manufactured By:
Intas Pharmaceuticals Limited,
Camp Road,
Selaqui, Dehradun,
Uttarakhand 248197,
India (IND)Repackaged by:
Proficient Rx LP
Thousand Oaks, CA 91320
Issued October 2023
- PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
LEVOTHYROXINE SODIUM
levothyroxine sodium tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:82804-168(NDC:16729-447) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength LEVOTHYROXINE SODIUM (UNII: 9J765S329G) (LEVOTHYROXINE - UNII:Q51BO43MG4) LEVOTHYROXINE SODIUM ANHYDROUS 25 ug Inactive Ingredients Ingredient Name Strength MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) MAGNESIUM OXIDE (UNII: 3A3U0GI71G) SODIUM STARCH GLYCOLATE TYPE A POTATO (UNII: 5856J3G2A2) SODIUM STEARYL FUMARATE (UNII: 7CV7WJK4UI) FD&C YELLOW NO. 6 (UNII: H77VEI93A8) Product Characteristics Color orange Score 2 pieces Shape ROUND Size 7mm Flavor Imprint Code P;1 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:82804-168-30 30 in 1 BOTTLE; Type 0: Not a Combination Product 12/09/2024 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA212399 12/10/2020 Labeler - Proficient Rx LP (079196022) Establishment Name Address ID/FEI Business Operations Proficient Rx LP 079196022 REPACK(82804-168) , RELABEL(82804-168)