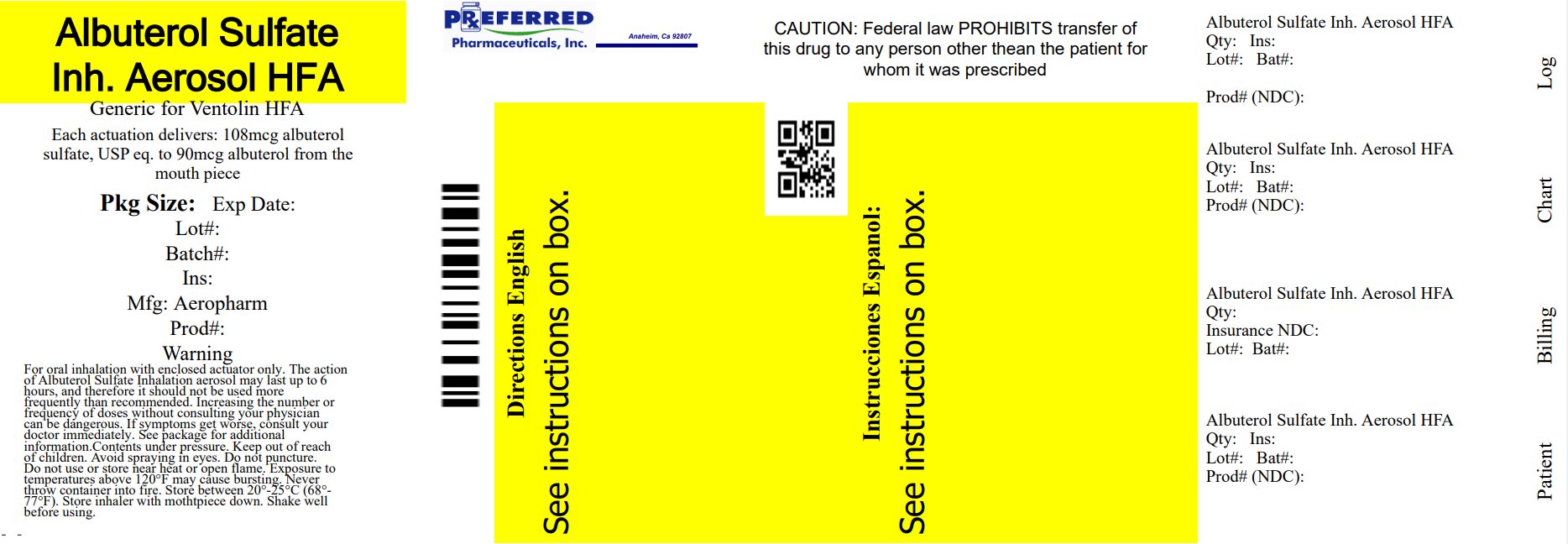
Label: ALBUTEROL SULFATE aerosol, metered

- NDC Code(s): 68788-8787-2
- Packager: Preferred Pharmaceuticals Inc.
- This is a repackaged label.
- Source NDC Code(s): 0054-0742
- Category: HUMAN PRESCRIPTION DRUG LABEL
Drug Label Information
Updated December 16, 2024
If you are a healthcare professional or from the pharmaceutical industry please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
- SPL UNCLASSIFIED SECTION
-
DESCRIPTION
The active component of albuterol sulfate inhalation aerosol is albuterol sulfate, USP racemic α1 [(tert-Butylamino)methyl]-4-hydroxy-m-xylene-α,α'-diol sulfate (2:1)(salt), a relatively selective beta2-adrenergic bronchodilator having the following chemical structure:
Albuterol sulfate is the official generic name in the United States. The World Health Organization recommended name for the drug is salbutamol sulfate. The molecular weight of albuterol sulfate is 576.7, and the molecular formula is (C13H21 NO3)2•H2SO4. Albuterol sulfate is a white to off-white crystalline solid. It is soluble in water and slightly soluble in ethanol. Albuterol sulfate inhalation aerosol is a pressurized metered-dose aerosol unit for oral inhalation. It contains a microcrystalline suspension of albuterol sulfate in propellant HFA-134a (1,1,1,2-tetrafluoroethane), ethanol, and oleic acid.
Each actuation delivers 120 mcg albuterol sulfate, USP from the valve and 108 mcg albuterol sulfate, USP from the mouthpiece (equivalent to 90 mcg of albuterol base from the mouthpiece). Each canister provides 200 inhalations. It is recommended to prime the inhaler before using for the first time and in cases where the inhaler has not been used for more than 2 weeks by releasing four “test sprays” into the air, away from the face.
This product does not contain chlorofluorocarbons (CFCs) as the propellant.
-
CLINICAL PHARMACOLOGY
Mechanism of Action
In vitro studies and in vivo pharmacologic studies have demonstrated that albuterol has a preferential effect on beta2-adrenergic receptors compared with isoproterenol. While it is recognized that beta2-adrenergic receptors are the predominant receptors on bronchial smooth muscle, data indicate that there is a population of beta2-receptors in the human heart existing in a concentration between 10% and 50% of cardiac beta-adrenergic receptors. The precise function of these receptors has not been established. (See WARNINGS, Cardiovascular Effects section.)
Activation of beta2-adrenergic receptors on airway smooth muscle leads to the activation of adenylcyclase and to an increase in the intracellular concentration of cyclic-3',5'-adenosine monophosphate (cyclic AMP). This increase of cyclic AMP leads to the activation of protein kinase A, which inhibits the phosphorylation of myosin and lowers intracellular ionic calcium concentrations, resulting in relaxation. Albuterol relaxes the smooth muscles of all airways, from the trachea to the terminal bronchioles. Albuterol acts as a functional antagonist to relax the airway irrespective of the spasmogen involved, thus protecting against all bronchoconstrictor challenges. Increased cyclic AMP concentrations are also associated with the inhibition of release of mediators from mast cells in the airway.
Albuterol has been shown in most clinical trials to have more effect on the respiratory tract, in the form of bronchial smooth muscle relaxation, than isoproterenol at comparable doses while producing fewer cardiovascular effects. Controlled clinical studies and other clinical experience have shown that inhaled albuterol, like other beta-adrenergic agonist drugs, can produce a significant cardiovascular effect in some patients, as measured by pulse rate, blood pressure, symptoms, and/or electrocardiographic changes.
Preclinical
Intravenous studies in rats with albuterol sulfate have demonstrated that albuterol crosses the blood-brain barrier and reaches brain concentrations amounting to approximately 5% of the plasma concentrations. In structures outside the blood-brain barrier (pineal and pituitary glands), albuterol concentrations were found to be 100 times those in the whole brain.
Studies in laboratory animals (minipigs, rodents, and dogs) have demonstrated the occurrence of cardiac arrhythmias and sudden death (with histologic evidence of myocardial necrosis) when beta2-agonist and methylxanthines were administered concurrently. The clinical significance of these findings is unknown.
Propellant HFA-134a is devoid of pharmacological activity except at very high doses in animals (380 to 1300 times the maximum human exposure based on comparisons of AUC values), primarily producing ataxia, tremors, dyspnea, or salivation. These are similar to effects produced by the structurally related chlorofluorocarbons (CFCs), which have been used extensively in metered dose inhalers.
In animals and humans, propellant HFA-134a was found to be rapidly absorbed and rapidly eliminated, with an elimination half-life of 3 to 27 minutes in animals and 5 to 7 minutes in humans. Time to maximum plasma concentration (Tmax) and mean residence time are both extremely short, leading to a transient appearance of HFA-134a in the blood with no evidence of accumulation.
Pharmacokinetics
In a single-dose bioavailability study which enrolled six healthy, male volunteers, transient low albuterol levels (close to the lower limit of quantitation) were observed after administration of two puffs from both albuterol sulfate inhalation aerosol and a CFC 11/12 propelled albuterol inhaler. No formal pharmacokinetic analyses were possible for either treatment, but systemic albuterol levels appeared similar.
Clinical Trials
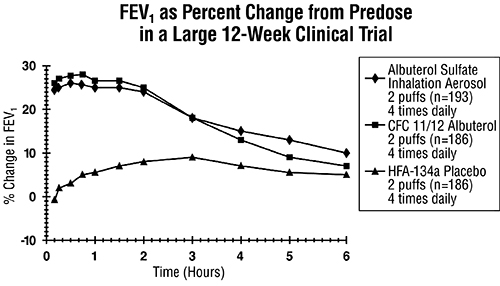
In a 12-week, randomized, double-blind, double-dummy, active- and placebo-controlled trial, 565 patients with asthma were evaluated for the bronchodilator efficacy of albuterol sulfate inhalation aerosol (193 patients) in comparison to a CFC 11/12 propelled albuterol inhaler (186 patients) and an HFA-134a placebo inhaler (186 patients).
Serial FEV1 measurements (shown below as percent change from test-day baseline) demonstrated that two inhalations of albuterol sulfate inhalation aerosol produced significantly greater improvement in pulmonary function than placebo and produced outcomes which were clinically comparable to a CFC 11/12 propelled albuterol inhaler.
The mean time to onset of a 15% increase in FEV1 was 6 minutes and the mean time to peak effect was 50 to 55 minutes. The mean duration of effect as measured by a 15% increase in FEV1 was 3 hours. In some patients, duration of effect was as long as 6 hours.
In another clinical study in adults, two inhalations of albuterol sulfate inhalation aerosol taken 30 minutes before exercise prevented exercise-induced bronchospasm as demonstrated by the maintenance of FEV1 within 80% of baseline values in the majority of patients.
In a 4-week, randomized, open-label trial, 63 children, 4 to 11 years of age, with asthma were evaluated for the bronchodilator efficacy of albuterol sulfate inhalation aerosol (33 pediatric patients) in comparison to a CFC 11/12 propelled albuterol inhaler (30 pediatric patients).
Serial FEV1 measurements as percent change from test-day baseline demonstrated that two inhalations of albuterol sulfate inhalation aerosol produced outcomes which were clinically comparable to a CFC 11/12 propelled albuterol inhaler.
The mean time to onset of a 12% increase in FEV1 for albuterol sulfate inhalation aerosol was 7 minutes and the mean time to peak effect was approximately 50 minutes. The mean duration of effect as measured by a 12% increase in FEV1 was 2.3 hours. In some pediatric patients, duration of effect was as long as 6 hours.
In another clinical study in pediatric patients, two inhalations of albuterol sulfate inhalation aerosol taken 30 minutes before exercise provided comparable protection against exercise-induced bronchospasm as a CFC 11/12 propelled albuterol inhaler.
- INDICATIONS AND USAGE
- CONTRAINDICATIONS
-
WARNINGS
- 1.
- Paradoxical Bronchospasm
- Inhaled albuterol sulfate can produce paradoxical bronchospasm that may be life threatening. If paradoxical bronchospasm occurs, albuterol sulfate inhalation aerosol should be discontinued immediately and alternative therapy instituted. It should be recognized that paradoxical bronchospasm, when associated with inhaled formulations, frequently occurs with the first use of a new canister.
- 2.
- Deterioration of Asthma
- Asthma may deteriorate acutely over a period of hours or chronically over several days or longer. If the patient needs more doses of albuterol sulfate inhalation aerosol than usual, this may be a marker of destabilization of asthma and requires re-evaluation of the patient and treatment regimen, giving special consideration to the possible need for anti-inflammatory treatment, e.g., corticosteroids.
- 3.
- Use of Anti-inflammatory Agents
- The use of beta-adrenergic-agonist bronchodilators alone may not be adequate to control asthma in many patients. Early consideration should be given to adding anti-inflammatory agents, e.g., corticosteroids, to the therapeutic regimen.
- 4.
- Cardiovascular Effects
- Albuterol sulfate inhalation aerosol, like other beta-adrenergic agonists, can produce clinically significant cardiovascular effects in some patients as measured by pulse rate, blood pressure, and/or symptoms. Although such effects are uncommon after administration of albuterol sulfate inhalation aerosol at recommended doses, if they occur, the drug may need to be discontinued. In addition, beta-agonists have been reported to produce ECG changes, such as flattening of the T wave, prolongation of the QTc interval, and ST segment depression. The clinical significance of these findings is unknown. Therefore, albuterol sulfate inhalation aerosol, like all sympathomimetic amines, should be used with caution in patients with cardiovascular disorders, especially coronary insufficiency, cardiac arrhythmias, and hypertension.
- 5.
- Do Not Exceed Recommended Dose:
- Fatalities have been reported in association with excessive use of inhaled sympathomimetic drugs in patients with asthma. The exact cause of death is unknown, but cardiac arrest following an unexpected development of a severe acute asthmatic crisis and subsequent hypoxia is suspected.
- 6.
- Immediate Hypersensitivity Reactions:
- Immediate hypersensitivity reactions may occur after administration of albuterol sulfate, as demonstrated by rare cases of urticaria, angioedema, rash, bronchospasm, anaphylaxis, and oropharyngeal edema.
-
PRECAUTIONS
General
Albuterol sulfate, as with all sympathomimetic amines, should be used with caution in patients with cardiovascular disorders, especially coronary insufficiency, cardiac arrhythmias, and hypertension; in patients with convulsive disorders, hyperthyroidism, or diabetes mellitus; and in patients who are unusually responsive to sympathomimetic amines. Clinically significant changes in systolic and diastolic blood pressure have been seen in individual patients and could be expected to occur in some patients after use of any beta-adrenergic bronchodilator.
Large doses of intravenous albuterol have been reported to aggravate preexisting diabetes mellitus and ketoacidosis. As with other beta-agonists, albuterol may produce significant hypokalemia in some patients, possibly through intracellular shunting, which has the potential to produce adverse cardiovascular effects. The decrease is usually transient, not requiring supplementation
Information for Patients
See illustrated Patient's Instructions for Use. SHAKE WELL BEFORE USING. Patients should be given the following information:
It is recommended to prime the inhaler before using for the first time and in cases where the inhaler has not been used for more than 2 weeks by releasing four “test sprays” into the air, away from the face.
KEEPING THE PLASTIC MOUTHPIECE CLEAN IS VERY IMPORTANT TO PREVENT MEDICATION BUILDUP AND BLOCKAGE. THE MOUTHPIECE SHOULD BE WASHED, SHAKEN TO REMOVE EXCESS WATER, AND AIR DRIED THOROUGHLY AT LEAST ONCE A WEEK. INHALER MAY CEASE TO DELIVER MEDICATION IF NOT PROPERLY CLEANED.
The mouthpiece should be cleaned (with the canister removed) by running warm water through the top and bottom for 30 seconds at least once a week. The mouthpiece must be shaken to remove excess water, then air dried thoroughly (such as overnight). Blockage from medication buildup or improper medication delivery may result from failure to thoroughly air dry the mouthpiece.
If the mouthpiece should become blocked (little or no medication coming out of the mouthpiece), the blockage may be removed by washing as described above.
If it is necessary to use the inhaler before it is completely dry, shake off excess water, replace canister, test spray twice away from face, and take the prescribed dose. After such use, the mouthpiece should be rewashed and allowed to air dry thoroughly.
The action of albuterol sulfate inhalation aerosol should last up to 4 to 6 hours. Albuterol sulfate inhalation aerosol should not be used more frequently than recommended. Do not increase the dose or frequency of doses of albuterol sulfate inhalation aerosol without consulting your physician. If you find that treatment with albuterol sulfate inhalation aerosol becomes less effective for symptomatic relief, your symptoms become worse, and/or you need to use the product more frequently than usual, medical attention should be sought immediately. While you are taking albuterol sulfate inhalation aerosol, other inhaled drugs and asthma medications should be taken only as directed by your physician.
Common adverse effects of treatment with inhaled albuterol include palpitations, chest pain, rapid heart rate, tremor, or nervousness. If you are pregnant or nursing, contact your physician about use of albuterol sulfate inhalation aerosol. Effective and safe use of albuterol sulfate inhalation aerosol includes an understanding of the way that it should be administered. Use albuterol sulfate inhalation aerosol only with the actuator supplied with the product. Discard the canister after 200 sprays have been used.
In general, the technique for administering albuterol sulfate inhalation aerosolto children is similar to that for adults. Children should use albuterol sulfate inhalation aerosolunder adult supervision, as instructed by the patient's physician. (See Patient's Instructions for Use.)
Drug Interactions
- 1.
- Beta-Blockers Beta-adrenergic-receptor blocking agents not only block the pulmonary effect of beta-agonists, such as albuterol sulfate inhalation aerosol, but may produce severe bronchospasm in asthmatic patients. Therefore, patients with asthma should not normally be treated with beta-blockers. However, under certain circumstances, e.g., as prophylaxis after myocardial infarction, there may be no acceptable alternatives to the use of beta-adrenergic blocking agents in patients with asthma. In this setting, cardioselective beta-blockers should be considered, although they should be administered with caution.
- 2.
- Diuretics The ECG changes and/or hypokalemia which may result from the administration of nonpotassium-sparing diuretics (such as loop or thiazide diuretics) can be acutely worsened by beta-agonists, especially when the recommended dose of the beta-agonist is exceeded. Although the clinical significance of these effects is not known, caution is advised in the coadministration of beta-agonists with nonpotassium-sparing diuretics.
- 3.
- Albuterol-Digoxin Mean decreases of 16% and 22% in serum digoxin levels were demonstrated after single-dose intravenous and oral administration of albuterol, respectively, to normal volunteers who had received digoxin for 10 days. The clinical significance of these findings for patients with obstructive airway disease who are receiving albuterol and digoxin on a chronic basis is unclear; nevertheless, it would be prudent to carefully evaluate the serum digoxin levels in patients who are currently receiving digoxin and albuterol.
- 4.
- Monoamine Oxidase Inhibitors or Tricyclic Antidepressants Albuterol sulfate inhalation aerosol should be administered with extreme caution to patients being treated with monoamine oxidase inhibitors or tricyclic antidepressants, or within 2 weeks of discontinuation of such agents, because the action of albuterol on the cardiovascular system may be potentiated
Carcinogenesis, Mutagenesis, and Impairment of Fertility
In a 2-year study in SPRAGUE-DAWLEY® rats, albuterol sulfate caused a dose-related increase in the incidence of benign leiomyomas of the mesovarium at the above dietary doses of 2 mg/kg (approximately 15 times the maximum recommended daily inhalation dose for adults on a mg/m2 basis and approximately 6 times the maximum recommended daily inhalation dose for children on a mg/m2 basis). In another study this effect was blocked by the coadministration of propranolol, a nonselective beta-adrenergic antagonist. In an 18-month study in CD-1 mice, albuterol sulfate showed no evidence of tumorigenicity at dietary doses of up to 500 mg/kg (approximately 1700 times the maximum recommended daily inhalation dose for adults on a mg/m2 basis and approximately 800 times the maximum recommended daily inhalation dose for children on a mg/m2 basis). In a 22-month study in Golden Hamsters, albuterol sulfate showed no evidence of tumorigenicity at dietary doses of up to 50 mg/kg (approximately 225 times the maximum recommended daily inhalation dose for adults on a mg/m2 basis and approximately 110 times the maximum recommended daily inhalation dose for children on a mg/m2 basis).
Albuterol sulfate was not mutagenic in the Ames test or a mutation test in yeast. Albuterol sulfate was not clastogenic in a human peripheral lymphocyte assay or in an AH1 strain mouse micronucleus assay.
Reproduction studies in rats demonstrated no evidence of impaired fertility at oral doses up to 50 mg/kg (approximately 340 times the maximum recommended daily inhalation dose for adults on a mg/m2 basis).
Pregnancy
Teratogenic Effects
Albuterol sulfate has been shown to be teratogenic in mice. A study in CD-1 mice given albuterol sulfate subcutaneously showed cleft palate formation in 5 of 111 (4.5%) fetuses at 0.25 mg/kg (less than the maximum recommended daily inhalation dose for adults on a mg/m2 basis) and in 10 of 108 (9.3%) fetuses at 2.5 mg/kg (approximately 8 times the maximum recommended daily inhalation dose for adults on a mg/m2 basis). The drug did not induce cleft palate formation at a dose of 0.025 mg/kg (less than the maximum recommended daily inhalation dose for adults on a mg/m2 basis). Cleft palate also occurred in 22 of 72 (30.5%) fetuses from females treated subcutaneously with 2.5 mg/kg of isoproterenol (positive control).
A reproduction study in Stride Dutch rabbits revealed cranioschisis in 7 of 19 (37%) fetuses when albuterol sulfate was administered orally at 50 mg/kg dose (approximately 680 times the maximum recommended daily inhalation dose for adults on a mg/m2 basis).
In an inhalation reproduction study in SPRAGUE-DAWLEY rats, the albuterol sulfate/HFA-134a formulation did not exhibit any teratogenic effects at 10.5 mg/kg (approximately 70 times the maximum recommended daily inhalation dose for adults on a mg/m2 basis).
A study in which pregnant rats were dosed with radiolabeled albuterol sulfate demonstrated that drug-related material is transferred from the maternal circulation to the fetus.
There are no adequate and well-controlled studies of albuterol sulfate inhalation aerosol or albuterol sulfate in pregnant women. Albuterol sulfate inhalation aerosol should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
During worldwide marketing experience, various congenital anomalies, including cleft palate and limb defects, have been reported in the offspring of patients being treated with albuterol. Some of the mothers were taking multiple medications during their pregnancies. Because no consistent pattern of defects can be discerned, a relationship between albuterol use and congenital anomalies has not been established.
Use in Labor and Delivery
Because of the potential for beta-agonist interference with uterine contractility, use of albuterol sulfate inhalation aerosol for relief of bronchospasm during labor should be restricted to those patients in whom the benefits clearly outweigh the risk.
Tocolysis
Albuterol has not been approved for the management of preterm labor. The benefit:risk ratio when albuterol is administered for tocolysis has not been established. Serious adverse reactions, including pulmonary edema, have been reported during or following treatment of premature labor with beta2-agonists, including albuterol.
Nursing Mothers
Plasma levels of albuterol sulfate and HFA-134a after inhaled therapeutic doses are very low in humans, but it is not known whether the components of albuterol sulfate inhalation aerosol are excreted in human milk.
Because of the potential for tumorigenicity shown for albuterol in animal studies and lack of experience with the use of albuterol sulfate inhalation aerosol by nursing mothers, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother. Caution should be exercised when albuterol sulfate is administered to a nursing woman.
Pediatrics
The safety and effectiveness of albuterol sulfate inhalation aerosol in pediatric patients below the age of 4 years have not been established.
Geriatrics
Albuterol sulfate inhalation aerosol has not been studied in a geriatric population. As with other beta2-agonists, special caution should be observed when using albuterol sulfate inhalation aerosol in elderly patients who have concomitant cardiovascular disease that could be adversely affected by this class of drug.
-
ADVERSE REACTIONS
Adverse reaction information concerning albuterol sulfate inhalation aerosol is derived from a 12-week, double-blind, double-dummy study which compared albuterol sulfate inhalation aerosol, a CFC 11/12 propelled albuterol inhaler, and an HFA-134a placebo inhaler in 565 asthmatic patients. The following table lists the incidence of all adverse events (whether considered by the investigator drug related or unrelated to drug) from this study which occurred at a rate of 3% or greater in the albuterol sulfate inhalation aerosol treatment group and more frequently in the albuterol sulfate inhalation aerosol treatment group than in the placebo group. Overall, the incidence and nature of the adverse reactions reported for albuterol sulfate inhalation aerosol and a CFC 11/12 propelled albuterol inhaler were comparable.
Adverse Experience Incidences (% of patients) in a Large 12-week Clinical Trial* Body System/
Adverse Event (Preferred Term)Albuterol SulfateInhalation Aerosol (N=193) CFC 11/12 Propelled Albuterol Inhaler (N=186) HFA-134a Placebo Inhaler (N=186) *This table includes all adverse events (whether considered by the investigator drug related or unrelated to drug) which occurred at an incidence rate of at least 3.0% in the albuterol sulfate inhalation aerosol group and more frequently in the albuterol sulfate inhalation aerosol group than in the HFA-134a placebo inhaler group. Application Site Disorders
Inhalation Site Sensation
6
9
2
Inhalation Taste Sensation
4
3
3
Body as a Whole
Allergic Reaction/Symptoms
6
4
<1
Back Pain
4
2
3
Fever
6
2
5
Central and Peripheral Nervous System
Tremor
7
8
2
Gastrointestinal System
Nausea
10
9
5
Vomiting
7
2
3
Heart Rate and Rhythm Disorder
Tachycardia
7
2
<1
Psychiatric Disorders
Nervousness
7
9
3
Respiratory System Disorders
Respiratory Disorder
(unspecified)
6
4
5
Rhinitis
16
22
14
Upper Resp Tract Infection
21
20
18
Urinary System Disorder
Urinary Tract Infection
3
4
2
Adverse events reported by less than 3% of the patients receiving albuterol sulfate inhalation aerosol, and by a greater proportion of albuterol sulfate inhalation aerosol patients than placebo patients, which have the potential to be related to albuterol sulfate inhalation aerosol include: dysphonia, increased sweating, dry mouth, chest pain, edema, rigors, ataxia, leg cramps, hyperkinesia, eructation, flatulence, tinnitus, diabetes mellitus, anxiety, depression, somnolence, rash. Palpitation and dizziness have also been observed with albuterol sulfate inhalation aerosol.
Adverse events reported in a 4-week pediatric clinical trial comparing albuterol sulfate inhalation aerosol and a CFC 11/12 propelled albuterol inhaler occurred at a low incidence rate and were similar to those seen in the adult trials.
In small, cumulative dose studies, tremor, nervousness, and headache appeared to be dose related.
Rare cases of urticaria, angioedema, rash, bronchospasm, and oropharyngeal edema have been reported after the use of inhaled albuterol. In addition, albuterol, like other sympathomimetic agents, can cause adverse reactions such as hypertension, angina, vertigo, central nervous system stimulation, insomnia, headache, metabolic acidosis, and drying or irritation of the oropharynx.
To report SUSPECTED ADVERSE REACTIONS, contact Sandoz Inc. at 1-800-525-8747 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
-
OVERDOSAGE
The expected symptoms with overdosage are those of excessive beta-adrenergic stimulation and/or occurrence or exaggeration of any of the symptoms listed under ADVERSE REACTIONS, e.g., seizures, angina, hypertension or hypotension, tachycardia with rates up to 200 beats per minute, arrhythmias, nervousness, headache, tremor, dry mouth, palpitation, nausea, dizziness, fatigue, malaise, and insomnia.
Hypokalemia may also occur. As with all sympathomimetic medications, cardiac arrest and even death may be associated with abuse of albuterol sulfate inhalation aerosol. Treatment consists of discontinuation of albuterol sulfate inhalation aerosol together with appropriate symptomatic therapy. The judicious use of a cardioselective beta-receptor blocker may be considered, bearing in mind that such medication can produce bronchospasm. There is insufficient evidence to determine if dialysis is beneficial for overdosage of albuterol sulfate inhalation aerosol.
The oral median lethal dose of albuterol sulfate in mice is greater than 2000 mg/kg (approximately 6800 times the maximum recommended daily inhalation dose for adults on a mg/m2 basis and approximately 3200 times the maximum recommended daily inhalation dose for children on a mg/m2 basis). In mature rats, the subcutaneous median lethal dose of albuterol sulfate is approximately 450 mg/kg (approximately 3000 times the maximum recommended daily inhalation dose for adults on a mg/m2 basis and approximately 1400 times the maximum recommended daily inhalation dose for children on a mg/m2 basis). In young rats, the subcutaneous median lethal dose is approximately 2000 mg/kg (approximately 14,000 times the maximum recommended daily inhalation dose for adults on a mg/m2 basis and approximately 6400 times the maximum recommended daily inhalation dose for children on a mg/m2 basis). The inhalation median lethal dose has not been determined in animals.
-
DOSAGE AND ADMINISTRATION
For treatment of acute episodes of bronchospasm or prevention of asthmatic symptoms, the usual dosage for adults and children 4 years of age and older is two inhalations repeated every 4 to 6 hours. More frequent administration or a larger number of inhalations is not recommended. In some patients, one inhalation every 4 hours may be sufficient. Each actuation of albuterol sulfate inhalation aerosol delivers 108 mcg of albuterol sulfate (equivalent to 90 mcg of albuterol base) from the mouthpiece. It is recommended to prime the inhaler before using for the first time and in cases where the inhaler has not been used for more than 2 weeks by releasing four “test sprays” into the air, away from the face.
Albuterol sulfate Inhalation Aerosol contains 200 inhalations per canister. The canister has an attached dose indicator, which indicates how many inhalations remain. The dose indicator display will move after every tenth actuation. When nearing the end of the usable inhalations, the background behind the number in the dose indicator display window changes to red at 20 actuations or lower. Albuterol sulfate Inhalation Aerosol should be discarded when the dose indicator display window shows zero.
Exercise Induced Bronchospasm Prevention
The usual dosage for adults and children 4 years of age and older is two inhalations 15 to 30 minutes before exercise.
To maintain proper use of this product, it is important that the mouthpiece be washed and dried thoroughly at least once a week. The inhaler may cease to deliver medication if not properly cleaned and dried thoroughly (see PRECAUTIONS, Information for Patients section). Keeping the plastic mouthpiece clean is very important to prevent medication buildup and blockage. The inhaler may cease to deliver medication if not properly cleaned and air dried thoroughly. If the mouthpiece becomes blocked, washing the mouthpiece will remove the blockage.
If a previously effective dose regimen fails to provide the usual response, this may be a marker of destabilization of asthma and requires reevaluation of the patient and the treatment regimen, giving special consideration to the possible need for anti-inflammatory treatment, e.g., corticosteroids.
-
HOW SUPPLIED
Albuterol sulfate inhalation aerosol is supplied as a pressurized aluminum canister with an attached dose indicator, a light blue plastic actuator and dark blue dust cap each in boxes of one. Each actuation delivers 120 mcg of albuterol sulfate from the valve and 108 mcg of albuterol sulfate from the mouthpiece (equivalent to 90 mcg of albuterol base). Canisters with a labeled net weight of 6.7 g contain 200 inhalations NDC 68788-8787-2
Rx only. Store at 20° to 25°C (68° to 77°F) [See USP Controlled Room Temperature]. Store the inhaler with the mouthpiece down. For best results, canister should be at room temperature before use.
SHAKE WELL BEFORE USING.
The light blue actuator supplied with albuterol sulfate inhalation aerosolshould not be used with any other product canisters, and actuator from other products should not be used with albuterol sulfate inhalation aerosolcanister. The correct amount of medication in each canister cannot be assured after 200 actuations, and when the dose indicator display window shows zero, even though the canister is not completely empty. The canister should be discarded when the labeled number of actuations have been used.
WARNING: Avoid spraying in eyes. Contents under pressure. Do not puncture or incinerate. Exposure to temperatures above 120°F may cause bursting. Keep out of reach of children.
Albuterol sulfate inhalation aerosol does not contain chlorofluorocarbons (CFCs) as the propellant.
Manufactured by Aeropharm GmbH
D-07407 Rudolstadt, GermanyDistributed by: Hikma
Pharmaceuticals USA Inc.Berkeley Heights, NJ 07922
The brands listed are the registered trademarks of their respective owners and are not trademarks of Sandoz Inc.
Rev. July 2021
46293491
Relabeled By: Preferred Pharmaceuticals Inc.
-
INSTRUCTIONS FOR USEAlbuterol Sulfate Inhalation AerosolWith Dose Indicator(al bue’ter ol sul’fate)
Read this Instructions for Use before you start using albuterol sulfate inhalation aerosol and each time you get a refill. There may be new information. This information does not take the place of talking to your doctor about your medical condition or treatment. Your doctor should show you how your child should use albuterol sulfate inhalation aerosol.
Important Information:
- •
- Albuterol sulfate inhalation aerosol is for oral inhalation use only.
- •
- Take albuterol sulfate inhalation aerosol exactly as your doctor tells you to.
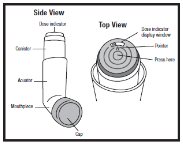
Albuterol sulfate inhalation aerosol comes as a canister with a dose indicator. The dose indicator is located on the top of the canister that fits into an actuator (See Figure A). The dose indicator display window will show you how many puffs of medicine you have left. A puff of medicine is released each time you press the center of the dose indicator.
- •
- Do not use the Albuterol Sulfate Inhalation Aerosol actuator with a canister of medicine from any other inhaler.
- •
- Do not use the Albuterol Sulfate Inhalation Aerosol canister with an actuator from any other inhaler.
Figure A
Before you use albuterol sulfate inhalation aerosol for the first time make sure that the pointer on the dose indicator is pointing to the right of the “200” inhalation mark in the dose indicator display window (See Figure A).
Each canister of albuterol sulfate inhalation aerosol contains 200 puffs of medicine. This does not include the sprays of medicine used for priming your inhaler.
- •
- The dose indicator display window will continue to move after every 10 puffs.
- •
- The number in the dose indicator display window will continue to change after every 20 puffs.
- •
- The color in the dose indicator display window will change to red, as shown in the shaded area, when there are only 20 puffs of medicine left in your inhaler (See Figure B). This is when you need to refill your prescription or ask your doctor if you need another prescription for albuterol sulfate inhalation aerosol.
Figure B
Priming your albuterol sulfate inhalation aerosol inhaler: Before you use albuterol sulfate inhalation aerosol for the first time, you should prime your inhaler. If you do not use your albuterol sulfate inhalation aerosol for more than 2 weeks, you should re-prime it before use.
- •
- Remove the cap from the mouthpiece (See Figure C). Check inside the mouthpiece for objects before use.
- •
- Make sure the canister is fully inserted into the actuator.
- •
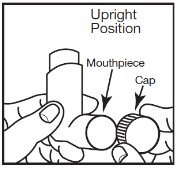
- Hold the inhaler in an upright position away from your face and shake the inhaler well.
- •
- Press down fully on the center of the dose indicator to release a spray of medicine. You may hear a soft click from the dose indicator as it counts down during use.
- •
- Repeat the priming step 3 more times to release a total of 4 sprays of medicine. Shake the inhaler well before each priming spray.
- •
- After the 4 priming sprays, the dose indicator should be pointing to 200. There are now 200 puffs of medicine left in the canister.
- •
- Your inhaler is now ready to use.
Using your albuterol sulfate inhalation aerosol inhaler:
Step 1: Shake the inhaler well before each use. Remove the cap from the mouthpiece (see Figure C). Check inside the mouthpiece for objects before use. Make sure the canister is fully inserted into the actuator.
Figure C
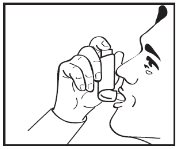
Step 2: Breathe out as fully as you comfortably can through your mouth. Hold the inhaler in the upright position with the mouthpiece pointing towards you and place the mouthpiece fully into the mouth (SeeFigure D). Close your lips around the mouthpiece.
Figure D
Step 3: While breathing in deeply and slowly, press down on the center of the dose indicator with your index finger until the canister stops moving in the actuator and a puff of medicine has been released (SeeFigure D). Then stop pressing the dose indicator.
Step 4: Hold your breath as long as you comfortably can, up to 10 seconds. Remove the inhaler from your mouth, and then breathe out.
Step 5:If your doctor has prescribed additional puffs of albuterol sulfate inhalation aerosol, wait 1 minute, then shake the inhaler well. Repeat steps 3 through 5 in the section “Using your albuterol sulfate inhalation aerosol inhaler”.
Step 6: Replace the cap right away after use.
Cleaning your albuterol sulfate inhalation aerosol inhaler:
It is very important that you keep the mouthpiece clean so that medicine will not build up and block the spray through the mouthpiece. Clean the mouthpiece 1 time each week or if your mouthpiece becomes blocked (See Figure F).
Step 1: Remove the canister from the actuator and take the cap off the mouthpiece. Do not clean the metal canister or let it get wet.
Step 2: Wash the mouthpiece through the top and bottom with warm running water for 30 seconds (See Figure E).
Figure E
Step 3: Shake off as much water from the mouthpiece as you can.
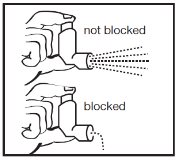
Step 4: Look in the mouthpiece to make sure any medicine buildup has been completely washed away. If the mouthpiece is blocked with buildup, little to no medicine will come out of the mouthpiece (See FigureF). If there is any buildup, repeat Steps 2 through 4 in the section “Cleaning your albuterol sulfate inhalation aerosol inhaler”.
Figure F
Step 5: Let the mouthpiece air-dry such as overnight (See Figure G). Do not put the canister back into the actuator if it is still wet.
Figure G
Step 6: When the mouthpiece is dry, put the canister back in the actuator and put the cap on the mouthpiece.
Note: If you need to use your albuterol sulfate inhalation aerosol inhaler before it is completely dry, put the canister back in the actuator and shake the inhaler well. Press down on the center of the dose indicator 2 times to release a total of 2 sprays into the air, away from your face. Take your dose as prescribed then clean and air-dry your inhaler as described in the section “Cleaning your albuterol sulfate inhalation aerosol inhaler”.
How should I store albuterol sulfate inhalation aerosol?
- •
- Store albuterol sulfate inhalation aerosol at room temperature between 20° to 25°C (68° to 77°F).
- •
- Store with the mouthpiece down.
- •
- Avoid exposing albuterol sulfate inhalation aerosol to extreme heat and cold.
- •
- Do not puncture or burn the canister.
- •
- Keep your albuterol sulfate inhalation aerosol inhaler and all medicines out of the reach of children.
Manufactured by
Aeropharm GmbH
D-07407 Rudolstadt, Germany
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Distributed by: Hikma
Pharmaceuticals USA Inc.
Berkeley Heights, NJ 07922
Rev. July 2021
46293491
Relabeled By: Preferred Pharmaceuticals Inc.
- Principal Display Panel
-
INGREDIENTS AND APPEARANCE
ALBUTEROL SULFATE
albuterol sulfate aerosol, meteredProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:68788-8787(NDC:0054-0742) Route of Administration RESPIRATORY (INHALATION) Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength ALBUTEROL SULFATE (UNII: 021SEF3731) (ALBUTEROL - UNII:QF8SVZ843E) ALBUTEROL 90 ug Inactive Ingredients Ingredient Name Strength ALCOHOL (UNII: 3K9958V90M) NORFLURANE (UNII: DH9E53K1Y8) OLEIC ACID (UNII: 2UMI9U37CP) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:68788-8787-2 1 in 1 CARTON 12/16/2024 1 200 in 1 CANISTER; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA207085 12/16/2024 Labeler - Preferred Pharmaceuticals Inc. (791119022) Registrant - Preferred Pharmaceuticals Inc. (791119022) Establishment Name Address ID/FEI Business Operations Preferred Pharmaceuticals Inc. 791119022 RELABEL(68788-8787)