Reye’s Syndrome may develop in individuals who have chicken pox, influenza, or flu symptoms. Some studies suggest possible association between the development of Reye’s Syndrome and the use of ...
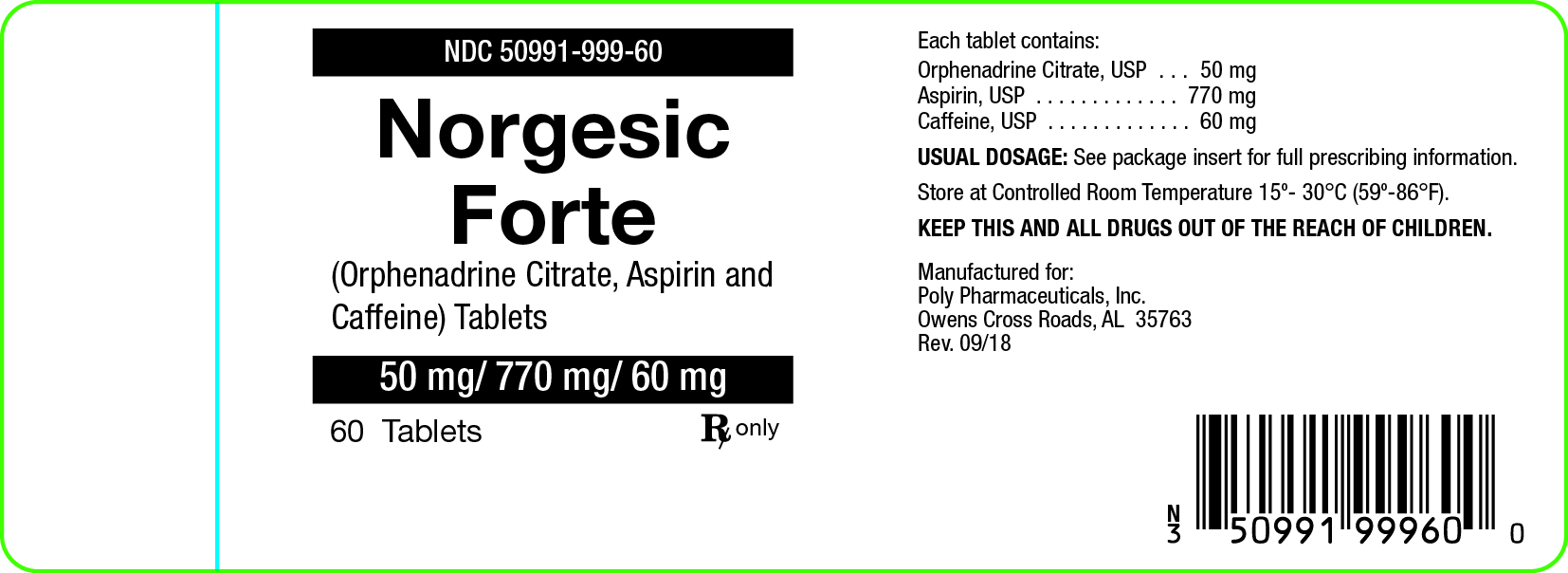
Reye’s Syndrome may develop in individuals who have chicken pox, influenza, or flu symptoms. Some studies suggest possible association between the development of Reye’s Syndrome and the use of medicines containing salicylate or aspirin. Norgesic Forte Tablets 50mg/770mg/60mg contain aspirin and therefore are not recommended for use in patients with chicken pox, influenza, or flu symptoms.
Norgesic Forte Tablets may impair the ability of the patient to engage in potentially hazardous activities such as operating machinery or driving a motor vehicle: ambulatory patients should therefore be cautioned accordingly.
Aspirin should be used with extreme caution in the presence of peptic ulcers and coagulation abnormalities.
Usage in Pregnancy
Risk Summary
Use of NSAIDs, including aspirin, can cause premature closure of the fetal ductus arteriosus and
fetal renal dysfunction leading to oligohydramnios and, in some cases, neonatal renal
impairment. Because of these risks, limit dose and duration of Orphengesic Forte Tablets use
between about 20 and 30 weeks of gestation, and avoid Orphengesic Forte Tablets use at about
30 weeks of gestation and later in pregnancy [see WARNINGS; Fetal Toxicity].
Premature Closure of Fetal Ductus Arteriosus
Use of NSAIDs, including aspirin, at about 30 weeks gestation or later in pregnancy
increases the risk of premature closure of the fetal ductus arteriosus.
Oligohydramnios/Neonatal Renal Impairment
Use of NSAIDs at about 20 weeks gestation or later in pregnancy has been associated with
cases of fetal renal dysfunction leading to oligohydramnios, and in some cases, neonatal
renal impairment.
Data from observational studies regarding other potential embryofetal risks of NSAID use in
women in the first or second trimesters of pregnancy are inconclusive.
Based on animal data, prostaglandins have been shown to have an important role in endometrial
vascular permeability, blastocyst implantation, and decidualization. In animal studies,
administration of prostaglandin synthesis inhibitors such as aspirin, resulted in increased pre- and
post-implantation loss. Prostaglandins also have been shown to have an important role in fetal
kidney development. In published animal studies, prostaglandin synthesis inhibitors have been
reported to impair kidney development when administered at clinically relevant doses.
The estimated background risk of major birth defects and miscarriage for the indicated
population(s) is unknown. All pregnancies have a background risk of birth defect, loss, or other
adverse outcomes. In the U.S. general population, the estimated background risk of major birth
defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
Clinical Considerations
Fetal/Neonatal Adverse Reactions
Premature Closure of Fetal Ductus Arteriosus: Avoid use of NSAIDs in women at about 30
weeks gestation and later in pregnancy, because NSAIDs, including Orphengesic Forte Tablets,
can cause premature closure of the fetal ductus arteriosus (see WARNINGS; Fetal Toxicity).
Oligohydramnios/Neonatal Renal Impairment
If an NSAID is necessary at about 20 weeks gestation or later in pregnancy, limit the use to the
lowest effective dose and shortest duration possible. If Orphengesic Forte Tablets treatment
extends beyond 48 hours, consider monitoring with ultrasound for oligohydramnios. If
oligohydramnios occurs, discontinue Orphengesic Forte Tablets and follow up according to
clinical practice (see WARNINGS; Fetal Toxicity).
Data
Human Data
Premature Closure of Fetal Ductus Arteriosus
:
Published literature reports that the use of NSAIDs at about 30 weeks of gestation and later in
pregnancy may cause premature closure of the fetal ductus arteriosus.
Oligohydramnios/Neonatal Renal Impairment:
Published studies and postmarketing reports describe maternal NSAID use at about 20 weeks
gestation or later in pregnancy associated with fetal renal dysfunction leading to
oligohydramnios, and in some cases, neonatal renal impairment. These adverse outcomes are
seen, on average, after days to weeks of treatment, although oligohydramnios has been
infrequently reported as soon as 48 hours after NSAID initiation. In many cases, but not all, the
decrease in amniotic fluid was transient and reversible with cessation of the drug. There have
been a limited number of case reports of maternal NSAID use and neonatal renal dysfunction
without oligohydramnios, some of which were irreversible. Some cases of neonatal renal
dysfunction required treatment with invasive procedures, such as exchange transfusion or
dialysis.
Methodological limitations of these postmarketing studies and reports include lack of a control
group; limited information regarding dose, duration, and timing of drug exposure; and
concomitant use of other medications. These limitations preclude establishing a reliable estimate
of the risk of adverse fetal and neonatal outcomes with maternal NSAID use. Because the
published safety data on neonatal outcomes involved mostly preterm infants, the generalizability
of certain reported risks to the full-term infant exposed to NSAIDs through maternal use is
uncertain.
Usage in Children
The safe and effective use of this drug in children has not been established. Usage of this drug in children under 12 years of age is not recommended.
Fetal Toxicity
Premature Closure of Fetal Ductus Arteriosus:
Avoid use of NSAIDs, including Norgesic Forte Tablets, in pregnant women at about 30
weeks gestation and later. NSAIDs including Orphengesic Forte Tablets, increase the risk of
premature closure of the fetal ductus arteriosus at approximately this gestational age.
Oligohydramnios/Neonatal Renal Impairment:
Use of NSAIDs, including Norgesic Forte Tablets, at about 20 weeks gestation or later in
pregnancy may cause fetal renal dysfunction leading to oligohydramnios and, in some cases,
neonatal renal impairment. These adverse outcomes are seen, on average, after days to weeks of
treatment, although oligohydramnios has been infrequently reported as soon as 48 hours after
NSAID initiation. Oligohydramnios is often, but not always, reversible with treatment
discontinuation. Complications of prolonged oligohydramnios may, for example, include limb
contractures and delayed lung maturation. In some postmarketing cases of impaired neonatal
renal function, invasive procedures such as exchange transfusion or dialysis were required.
If NSAID treatment is necessary between about 20 weeks and 30 weeks gestation, limit
Orphengesic Forte Tablets use to the lowest effective dose and shortest duration possible.
Consider ultrasound monitoring of amniotic fluid if Norgesic Forte Tablets treatment extends
beyond 48 hours. Discontinue if oligohydramnios occurs and follow
up according to clinical practice [see PRECAUTIONS; Pregnancy].
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS)
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) has been reported in
patients taking NSAIDs such as Orphengesic Forte Tablets. Some of these events have been fatal
or life-threatening. DRESS typically, although not exclusively, presents with fever, rash,
lymphadenopathy, and/or facial swelling. Other clinical manifestations may include hepatitis,
nephritis, hematological abnormalities, myocarditis, or myositis. Sometimes symptoms of
DRESS may resemble an acute viral infection. Eosinophilia is often present. Because this
disorder is variable in its presentation, other organ systems not noted here may be involved. It is
important to note that early manifestations of hypersensitivity, such as fever or
lymphadenopathy, may be present even though rash is not evident. If such signs or symptoms are
present, discontinue and evaluate the patient immediately.
Close