Label: XPOVIO- selinexor tablet, film coated




































-
NDC Code(s):
72237-101-01,
72237-101-02,
72237-101-03,
72237-101-04, view more72237-101-05, 72237-101-06, 72237-101-07, 72237-101-11, 72237-101-12, 72237-101-13, 72237-101-14, 72237-101-15, 72237-101-16, 72237-101-17, 72237-102-02, 72237-102-06, 72237-102-07, 72237-102-12, 72237-102-16, 72237-102-17, 72237-103-05, 72237-103-15, 72237-104-01, 72237-104-11
- Packager: Karyopharm Therapeutics Inc.
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: New Drug Application
Drug Label Information
Updated July 25, 2022
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Medication Guide: HTML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use XPOVIO safely and effectively. See full prescribing information for XPOVIO.
XPOVIO® (selinexor) tablets, for oral use
Initial U.S. Approval: 2019INDICATIONS AND USAGE
XPOVIO is a nuclear export inhibitor indicated:
- In combination with bortezomib and dexamethasone for the treatment of adult patients with multiple myeloma who have received at least one prior therapy (1.1).
- In combination with dexamethasone for the treatment of adult patients with relapsed or refractory multiple myeloma who have received at least four prior therapies and whose disease is refractory to at least two proteasome inhibitors, at least two immunomodulatory agents, and an anti-CD38 monoclonal antibody (1.1).
- For the treatment of adult patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL), not otherwise specified, including DLBCL arising from follicular lymphoma, after at least 2 lines of systemic therapy. This indication is approved under accelerated approval based on response rate. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trial(s) (1.2).
DOSAGE AND ADMINISTRATION
- Multiple Myeloma in Combination with Bortezomib and Dexamethasone (XVd): Recommended dosage of XPOVIO is 100 mg taken orally once weekly in combination with bortezomib and dexamethasone (2.1).
- Multiple Myeloma in Combination with Dexamethasone (Xd): Recommended dosage of XPOVIO is 80 mg taken orally on Days 1 and 3 of each week in combination with dexamethasone (2.1).
- DLBCL: Recommended dosage of XPOVIO is 60 mg taken orally on Days 1 and 3 of each week (2.2).
DOSAGE FORMS AND STRENGTHS
Tablets: 20 mg, 40 mg, 50 mg, 60 mg (3).
CONTRAINDICATIONS
None (4).
WARNINGS AND PRECAUTIONS
- Thrombocytopenia: Monitor platelet counts throughout treatment. Manage with dose interruption and/or reduction and supportive care (2.5, 5.1).
- Neutropenia: Monitor neutrophil counts throughout treatment. Manage with dose interruption and/or reduction and granulocyte colony-stimulating factors (2.5, 5.2).
- Gastrointestinal Toxicity: Nausea, vomiting, diarrhea, anorexia, and weight loss may occur. Provide antiemetic prophylaxis. Manage with dose interruption and/or reduction, antiemetics, and supportive care (2.5, 5.3).
- Hyponatremia: Monitor serum sodium levels throughout treatment.
- Correct for concurrent hyperglycemia and high serum paraprotein levels. Manage with dose interruption, reduction, or discontinuation, and supportive care (2.5, 5.4).
- Serious Infection: Monitor for infection and treat promptly (5.2, 5.5).
- Neurological Toxicity: Advise patients to refrain from driving and engaging in hazardous occupations or activities until neurological toxicity resolves. Optimize hydration status and concomitant medications to avoid dizziness or mental status changes (5.6).
- Embryo-Fetal Toxicity: Can cause fetal harm. Advise females of reproductive potential and males with a female partner of reproductive potential, of the potential risk to a fetus and use of effective contraception (5.7, 8.1, 8.3).
- Cataract: Cataracts may develop or progress. Treatment of cataracts usually requires surgical removal of the cataract (5.8).
ADVERSE REACTIONS
- The most common adverse reactions (≥20%) in patients with multiple myeloma who receive XVd are fatigue, nausea, decreased appetite, diarrhea, peripheral neuropathy, upper respiratory tract infection, weight decreased, cataract, and vomiting. Grade 3-4 laboratory abnormalities (≥10%) are thrombocytopenia, lymphopenia, hypophosphatemia, anemia, hyponatremia, and neutropenia (6.1).
- The most common adverse reactions (≥20%) in patients with multiple myeloma who receive Xd are thrombocytopenia, fatigue, nausea, anemia, decreased appetite, weight decreased, diarrhea, vomiting, hyponatremia, neutropenia, leukopenia, constipation, dyspnea, and upper respiratory tract infection (6.1).
- The most common adverse reactions (incidence ≥20%) in patients with DLBCL, excluding laboratory abnormalities, are fatigue, nausea, diarrhea, decreased appetite, weight decreased, constipation, vomiting, and pyrexia. Grade 3-4 laboratory abnormalities (≥15%) are thrombocytopenia, lymphopenia, neutropenia, anemia, and hyponatremia (6.1).
To report SUSPECTED ADVERSE REACTIONS, contact Karyopharm Therapeutics Inc. at 1-888-209-9326 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 7/2022
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
1.1 Multiple Myeloma
1.2 Diffuse Large B-Cell Lymphoma
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage for Multiple Myeloma
2.2 Recommended Dosage for Diffuse Large B-Cell Lymphoma
2.3 Recommended Monitoring for Safety
2.4 Recommended Concomitant Treatments
2.5 Dosage Modification for Adverse Reactions
2.6 Administration
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Thrombocytopenia
5.2 Neutropenia
5.3 Gastrointestinal Toxicity
5.4 Hyponatremia
5.5 Serious Infection
5.6 Neurological Toxicity
5.7 Embryo-Fetal Toxicity
5.8 Cataract
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
14.1 Relapsed or Refractory Multiple Myeloma
14.2 Relapsed or Refractory Diffuse Large B-Cell Lymphoma
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
1.1 Multiple Myeloma
- XPOVIO in combination with bortezomib and dexamethasone is indicated for the treatment of adult patients with multiple myeloma who have received at least one prior therapy.
- XPOVIO in combination with dexamethasone is indicated for the treatment of adult patients with relapsed or refractory multiple myeloma who have received at least four prior therapies and whose disease is refractory to at least two proteasome inhibitors, at least two immunomodulatory agents, and an anti-CD38 monoclonal antibody.
1.2 Diffuse Large B-Cell Lymphoma
XPOVIO is indicated for the treatment of adult patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL), not otherwise specified, including DLBCL arising from follicular lymphoma, after at least 2 lines of systemic therapy.
This indication is approved under accelerated approval based on response rate [see Clinical Studies (14.2)]. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial(s).
-
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage for Multiple Myeloma
In Combination with Bortezomib and Dexamethasone (XVd)
The recommended dosage of XPOVIO is 100 mg taken orally once weekly on Day 1 of each week until disease progression or unacceptable toxicity in combination with:
- Bortezomib 1.3 mg/m2 administered subcutaneously once weekly on Day 1 of each week for 4 weeks followed by 1 week off.
- Dexamethasone 20 mg taken orally twice weekly on Days 1 and 2 of each week.
Refer to Clinical Studies (14.1) and the prescribing information of bortezomib and dexamethasone for additional dosing information.
In Combination with Dexamethasone (Xd)
The recommended dosage of XPOVIO is 80 mg taken orally on Days 1 and 3 of each week until disease progression or unacceptable toxicity in combination with dexamethasone 20 mg taken orally with each dose of XPOVIO on Days 1 and 3 of each week.
For additional information regarding the administration of dexamethasone, refer to its prescribing information.
2.2 Recommended Dosage for Diffuse Large B-Cell Lymphoma
The recommended dosage of XPOVIO is 60 mg taken orally on Days 1 and 3 of each week until disease progression or unacceptable toxicity.
2.3 Recommended Monitoring for Safety
Monitor complete blood count (CBC) with differential, standard blood chemistries, body weight, nutritional status, and volume status at baseline and during treatment as clinically indicated. Monitor more frequently during the first three months of treatment [see Warning and Precautions (5.1, 5.2, 5.3, and 5.4)]. Assess the need for dosage modifications of XPOVIO for adverse reactions [see Dosage and Administration (2.5)].
2.4 Recommended Concomitant Treatments
Advise patients to maintain adequate fluid and caloric intake throughout treatment. Consider intravenous hydration for patients at risk of dehydration [see Warnings and Precautions (5.3, 5.4)].
Provide prophylactic antiemetics. Administer a 5-HT3 receptor antagonist and other anti-nausea agents prior to and during treatment with XPOVIO [see Warnings and Precautions (5.3)].
2.5 Dosage Modification for Adverse Reactions
Recommended XPOVIO dosage reduction steps are presented in Table 1.
Table 1: XPOVIO Dosage Reduction Steps for Adverse Reactions Recommended
Starting DosageMultiple Myeloma
In Combination with
Bortezomib and
Dexamethasone (XVd)Multiple Myeloma
In Combination with
Dexamethasone (Xd)Diffuse Large B-Cell Lymphoma 100 mg once weekly 80 mg Days 1 and 3 of each week
(160 mg total per week)60 mg Days 1 and 3 of each week
(120 mg total per week)First Reduction 80 mg once weekly 100 mg once weekly 40 mg Days 1 and 3 of each week
(80 mg total per week)Second Reduction 60 mg once weekly 80 mg once weekly 60 mg once weekly Third Reduction 40 mg once weekly 60 mg once weekly 40 mg once weekly Fourth Reduction Permanently discontinue Permanently discontinue Permanently discontinue Recommended dosage modifications for hematologic adverse reactions in patients with multiple myeloma and DLBCL are presented in Table 2 and Table 3, respectively. Recommended dosage modifications for nonhematologic adverse reactions are presented in Table 4.
Table 2: XPOVIO Dosage Modification Guidelines for Hematologic Adverse Reactions in Patients with Multiple Myeloma Adverse Reaction Occurrence Action Thrombocytopenia [see Warning and Precautions (5.1)] Platelet count 25,000 to less than 75,000/mcL Any - Reduce XPOVIO by 1 dose level (see Table 1).
Platelet count 25,000 to less than 75,000/mcL with concurrent bleeding Any - Interrupt XPOVIO.
- Restart XPOVIO at 1 dose level lower (see Table 1) after bleeding has resolved.
- Administer platelet transfusions per clinical guidelines.
Platelet count less than 25,000/mcL Any
- Interrupt XPOVIO.
- Monitor until platelet count returns to at least 50,000/mcL.
- Restart XPOVIO at 1 dose level lower (see Table 1).
Adverse Reaction Occurrence Action Neutropenia [see Warning and Precautions (5.2)] Absolute neutrophil count of 0.5 to 1 x 109/L without fever Any - Reduce XPOVIO by 1 dose level (see Table 1).
Absolute neutrophil count less than 0.5 x 109/L OR
febrile neutropeniaAny
- Interrupt XPOVIO.
- Monitor until neutrophil counts return to 1 x 109/L or higher.
- Restart XPOVIO at 1 dose level lower (see Table 1).
Anemia Hemoglobin less than 8 g/dL Any - Reduce XPOVIO by 1 dose level (see Table 1).
- Administer blood transfusions per clinical guidelines.
Life-threatening consequences
Any - Interrupt XPOVIO.
- Monitor hemoglobin until levels return to 8 g/dL or higher.
- Restart XPOVIO at 1 dose level lower (see Table 1).
- Administer blood transfusions per clinical guidelines.
Table 3: XPOVIO Dosage Modification Guidelines for Hematologic Adverse Reactions in Patients with Diffuse Large B-Cell Lymphoma Adverse Reaction Occurrence Action Thrombocytopenia [see Warning and Precautions (5.1)] Platelet count 50,000 to less than 75,000/mcL Any - Interrupt one dose of XPOVIO.
- Restart XPOVIO at the same dose level.
Platelet count 25,000 to less than 50,000/mcL without bleeding 1st - Interrupt XPOVIO.
- Monitor until platelet count returns to at least 50,000/mcL.
- Reduce XPOVIO by 1 dose level (see Table 1).
Platelet count 25,000 to less than 50,000/mcL with concurrent bleeding Any - Interrupt XPOVIO.
- Monitor until platelet count returns to at least 50,000/mcL.
- Restart XPOVIO at 1 dose level lower (see Table 1), after bleeding has resolved.
- Administer platelet transfusions per clinical guidelines.
Platelet count less than 25,000/mcL Any - Interrupt XPOVIO.
- Monitor until platelet count returns to at least 50,000/mcL.
- Restart XPOVIO at 1 dose level lower (see Table 1).
- Administer platelet transfusions per clinical guidelines.
Neutropenia [see Warning and Precautions (5.2)] Absolute neutrophil count of 0.5 to less than 1 x 109/L without fever 1st occurrence - Interrupt XPOVIO.
- Monitor until neutrophil counts return to 1 x 109/L or higher.
- Restart XPOVIO at the same dose level.
Recurrence - Interrupt XPOVIO.
- Monitor until neutrophil counts return to 1 x 109/L or higher.
- Administer growth factors per clinical guidelines.
- Restart XPOVIO at 1 dose level lower (see Table 1).
Absolute neutrophil count less than 0.5 x 109/L
OR
Febrile neutropeniaAny - Interrupt XPOVIO.
- Monitor until neutrophil counts return to 1 x 109/L or higher.
- Administer growth factors per clinical guidelines.
- Restart XPOVIO at 1 dose level lower (see Table 1).
Anemia Hemoglobin less than 8 g/dL Any - Reduce XPOVIO by 1 dose level (see Table 1).
- Administer blood transfusions per clinical guidelines.
Life-threatening consequences Any - Interrupt XPOVIO.
- Monitor hemoglobin until levels return to 8 g/dL or higher.
- Restart XPOVIO at 1 dose level lower (see Table 1).
- Administer blood transfusions per clinical guidelines.
Table 4: XPOVIO Dosage Modification Guidelines for Non-Hematologic Adverse Reactions Adverse Reaction Occurrence Action Nausea and Vomiting [see Warning and Precautions (5.3)] Grade 1 or 2 nausea (oral intake decreased without significant weight loss,
dehydration or malnutrition)
OR
Grade 1 or 2 vomiting (5 or fewer episodes per day)Any - Maintain XPOVIO and initiate additional anti-nausea medications.
Grade 3 nausea (inadequate oral caloric or fluid intake)
OR
Grade 3 or higher vomiting (6 or more episodes per day)Any - Interrupt XPOVIO.
- Monitor until nausea or vomiting has resolved to Grade 2 or lower or baseline.
- Initiate additional anti-nausea medications.
- Restart XPOVIO at 1 dose level lower (see Table 1).
Diarrhea [see Warning and Precautions (5.3)] Grade 2 (increase of 4 to 6 stools per day over baseline) 1st - Maintain XPOVIO and institute supportive care.
2nd and subsequent - Reduce XPOVIO by 1 dose level (see Table 1).
- Institute supportive care.
Grade 3 or higher (increase of 7 stools or more per day over baseline; hospitalization indicated) Any
- Interrupt XPOVIO and institute supportive care.
- Monitor until diarrhea resolves to Grade 2 or lower.
- Restart XPOVIO at 1 dose level lower (see Table 1).
Weight Loss and Anorexia [see Warning and Precautions (5.3)] Weight loss of 10% to less than 20%
OR
Anorexia associated with significant weight loss or malnutritionAny - Interrupt XPOVIO and institute supportive care.
- Monitor until weight returns to more than 90% of baseline weight.
- Restart XPOVIO at 1 dose level lower (see Table 1).
Hyponatremia [see Warning and Precautions (5.4)] Sodium level 130 mmol/L or less Any - Interrupt XPOVIO, evaluate, and provide supportive care.
- Monitor until sodium levels return to greater than 130 mmol/L.
- Restart XPOVIO at 1 dose level lower (see Table 1).
Fatigue Grade 2 lasting greater than 7 days
OR
Grade 3Any
- Interrupt XPOVIO.
- Monitor until fatigue resolves to Grade 1 or baseline.
- Restart XPOVIO at 1 dose level lower (see Table 1).
Ocular Toxicity [see Warning and Precautions (5.8)] Grade 2, excluding cataract Any - Perform ophthalmologic evaluation.
- Interrupt XPOVIO and provide supportive care.
- Monitor until ocular symptoms resolve to Grade 1 or baseline.
- Restart XPOVIO at 1 dose level lower (see Table 1).
Grade ≥3, excluding cataract Any - Permanently discontinue XPOVIO.
- Perform ophthalmologic evaluation.
Other Non-Hematologic Adverse Reactions [see Warning and Precautions (5.6)] Grade 3 or 4 Any - Interrupt XPOVIO.
- Monitor until resolved to Grade 2 or lower; restart XPOVIO at 1 dose level lower (see Table 1).
2.6 Administration
Each XPOVIO dose should be taken at approximately the same time of day and each tablet should be swallowed whole with water. Do not break, chew, crush, or divide the tablets.
If a dose of XPOVIO is missed or delayed, instruct patients to take their next dose at the next regularly scheduled time.
If a patient vomits a dose of XPOVIO, the patient should not repeat the dose and the patient should take the next dose on the next regularly scheduled day.
-
3 DOSAGE FORMS AND STRENGTHS
Tablets:
20 mg, blue, round, bi-convex, film-coated tablets with “K20” debossed on one side and nothing on the other side.
40 mg tablets, blue, oval, film-coated, debossed on both sides with “X40”.
50 mg tablets, blue, oval, film-coated, debossed on both sides with “X50”.
60 mg tablets, blue, oval, film-coated, debossed on both sides with “X60”.
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Thrombocytopenia
XPOVIO can cause life-threatening thrombocytopenia, potentially leading to hemorrhage. Thrombocytopenia is the leading cause of dosage modifications [see Adverse Reactions (6.1)].
In patients with multiple myeloma who received XPOVIO 100 mg once weekly (BOSTON, n=195), thrombocytopenia was reported in 92% of patients and severe (Grade 3-4) thrombocytopenia was reported in 43% of patients. The median time to first onset was 22 days for any grade thrombocytopenia and 43 days for Grade 3 or 4 thrombocytopenia. Bleeding occurred in 16% of patients with thrombocytopenia, clinically significant bleeding (Grade ≥3 bleeding) occurred in 4% of patients with thrombocytopenia, and fatal hemorrhage occurred in 2% of patients with thrombocytopenia. Permanent discontinuations of XPOVIO due to thrombocytopenia occurred in 2% of patients.
In patients with multiple myeloma who received XPOVIO 80 mg twice weekly (STORM, n=202), thrombocytopenia was reported as an adverse reaction in 74% of patients and severe (Grade 3-4) thrombocytopenia was reported in 61% of patients. The median time to onset of the first event was 22 days. Bleeding occurred in 23% of patients with thrombocytopenia, clinically significant bleeding occurred in 5% of patients with thrombocytopenia, and fatal hemorrhage occurred in <1% of patients.
In patients with DLBCL who received XPOVIO 60 mg twice weekly (SADAL, n=134), thrombocytopenia developed or worsened in 86% of patients, including Grade 3-4 thrombocytopenia in 49% of patients (Grade 4, 18%). The median time to first onset was 28 days for any grade thrombocytopenia and 33 days for Grade 3 or 4 thrombocytopenia.
Monitor platelet counts at baseline and throughout treatment. Monitor more frequently during the first three months of treatment. Institute platelet transfusion and/or other treatments as clinically indicated. Monitor patients for signs and symptoms of bleeding and evaluate promptly. Interrupt, reduce dose, or permanently discontinue based on severity of adverse reaction [see Dosage and Administration (2.5)].
5.2 Neutropenia
XPOVIO can cause life-threatening neutropenia, potentially increasing the risk of infection [see Adverse Reactions (6.1)].
In patients with multiple myeloma who received XPOVIO 100 mg once weekly (BOSTON, n=195), neutropenia was reported in 48% of patients and severe neutropenia (Grade 3-4) was reported in 12% of patients. The median time to onset of the first event was 23 days for any grade neutropenia and 40 days for Grade 3-4 neutropenia. Febrile neutropenia was reported in <1% of patients.
In patients with multiple myeloma who received XPOVIO 80 mg twice weekly (STORM, n=202), neutropenia was reported as an adverse reaction in 34% of patients and severe (Grade 3-4) neutropenia was reported in 21% of patients. The median time to onset of the first event was 25 days. Febrile neutropenia was reported in 3% of patients.
In patients with DLBCL (SADAL, n=134), Grade 3 neutropenia developed in 21% of patients and Grade 4 neutropenia developed in 9% of patients. The median time to first onset of Grade 3 or 4 neutropenia was 32 days. Febrile neutropenia was reported in 3% of patients.
Obtain white blood cell counts with differential at baseline and throughout treatment. Monitor more frequently during the first three months of treatment. Monitor patients for signs and symptoms of concomitant infection and evaluate promptly. Consider supportive measures, including antimicrobials and growth factors (e.g., G-CSF). Interrupt, reduce dose or permanently discontinue based on severity of adverse reaction [see Dosage and Administration (2.5)].
5.3 Gastrointestinal Toxicity
XPOVIO can cause severe gastrointestinal toxicities [see Adverse Reactions (6.1)]. In patients with DLBCL (n=134), gastrointestinal toxicity occurred in 80% of patients with Grade 3 or 4 in 13%.
Nausea/Vomiting
In patients with multiple myeloma who received XPOVIO once weekly (BOSTON, n=195) with use of antiemetic prophylaxis (88% of patients), nausea was reported in 50% of patients and Grade 3 nausea was reported in 8% of patients. The median time to onset of the first event was 6 days. Vomiting was reported in 21% of patients and Grade 3 vomiting was reported in 4.1% of patients. The median time to onset of the first event was 8 days. Permanent discontinuation due to nausea occurred in 3.1% of patients and due to vomiting occurred in 2.1% of patients.
In patients with multiple myeloma receiving XPOVIO 80 mg twice weekly (STORM, n=202) with use of antiemetic prophylaxis, nausea was reported as an adverse reaction in 72% of patients and Grade 3 nausea occurred in 9%. The median time to first onset of nausea was 3 days. Vomiting was reported in 41% of patients and Grade 3 vomiting occurred in 4% of patients. The median time to first onset of vomiting was 5 days.
In patients with DLBCL (SADAL, n=134) with use of antiemetic prophylaxis, nausea occurred in 57% of patients and Grade 3 nausea occurred in 6% of patients. Vomiting occurred in 28% of patients and Grade 3 vomiting occurred in 1.5% of patients. The median time to first onset was 3 days for nausea and 7 days for vomiting.
Provide prophylactic antiemetics. Administer 5-HT3 receptor antagonists and other anti-nausea agents prior to and during treatment with XPOVIO. Interrupt, reduce dose or permanently discontinue based on severity of adverse reaction [see Dosage and Administration (2.5)]. Administer intravenous fluids to prevent dehydration and replace electrolytes as clinically indicated.
Diarrhea
In patients with multiple myeloma who received XPOVIO once weekly (BOSTON, n=195), diarrhea was reported in 32% of patients and Grade 3 diarrhea was reported in 6% of patients. The median time to onset of the first event was 50 days. Permanent discontinuation due to diarrhea occurred in 1% of patients.
In patients with multiple myeloma who received XPOVIO 80 mg twice weekly (STORM, n=202), diarrhea was reported as an adverse reaction in 44% of patients and Grade 3 diarrhea occurred in 6% of patients. The median time to onset of diarrhea was 15 days.
In patients with DLBCL (SADAL, n=134), diarrhea occurred in 37% of patients and Grade 3 diarrhea occurred in 3% of patients treated with XPOVIO. The median time to onset of the first event was 12 days.
Interrupt, reduce dose or permanently discontinue based on severity of adverse reaction [see Dosage and Administration (2.5)]. Provide standard anti-diarrheal agents, administer intravenous fluids to prevent dehydration and replace electrolytes as clinically indicated.
Anorexia/Weight Loss
In patients with multiple myeloma who received XPOVIO 100 mg once weekly (BOSTON, n=195), anorexia was reported in 35% of patients and Grade 3 anorexia was reported in 3.6% of patients. The median time to onset of the first event was 35 days. Permanent discontinuations due to anorexia occurred in 2.1% of patients. Weight loss was reported in 26% of patients and Grade 3 weight loss was reported in 2.1% of patients. The median time to onset of the first event was 58 days. Permanent discontinuation due to weight loss occurred in 1% of patients.
In patients with multiple myeloma who received XPOVIO 80 mg twice weekly (STORM n=202), anorexia was reported as an adverse reaction in 53% of patients and Grade 3 anorexia occurred in 5% of patients. The median time to onset of anorexia was 8 days. Weight loss was reported as an adverse reaction in 47% of patients and Grade 3 weight loss occurred in 1% of patients treated with XPOVIO. The median time to onset of weight loss was 15 days.
In patients with DLBCL (SADAL, n=134), anorexia was reported as an adverse reaction in 37% of patients and Grade 3 anorexia occurred in 3.7% of patients treated with XPOVIO. Weight loss (Grade 1-2) was reported as an adverse reaction in 30% of patients.
Monitor weight, nutritional status, and volume status at baseline and throughout treatment. Monitor more frequently during the first three months of treatment. Interrupt, reduce dose or permanently discontinue based on severity of adverse reaction [see Dosage and Administration (2.5)]. Provide nutritional support, fluids, and electrolyte repletion as clinically indicated.
5.4 Hyponatremia
XPOVIO can cause severe or life-threatening hyponatremia [see Adverse Reactions (6.1)].
In patients with multiple myeloma who received XPOVIO 100 mg once weekly (BOSTON, n=195), hyponatremia was reported in 58% of patients and Grade 3-4 hyponatremia was reported in 14% of patients. The median time to first onset was 21 days for any grade hyponatremia and the median time to first onset for Grade 3 or 4 hyponatremia was 22 days.
In patients with multiple myeloma who received XPOVIO 80 mg twice weekly (STORM, n=202), hyponatremia was reported as an adverse reaction in 39% of patients and Grade 3 or 4 hyponatremia was reported in 22% of patients. The median time to onset of the first event was 8 days.
In patients with DLBCL (SADAL, n=134), hyponatremia developed in 62% of patients and Grade 3 hyponatremia developed in 16% of patients treated with XPOVIO. In approximately 63% of cases, hyponatremia occurred in the context of gastrointestinal toxicity such as nausea, vomiting, diarrhea, dehydration, and anorexia.
Monitor sodium level at baseline and throughout treatment. Monitor more frequently during the first two months of treatment. Correct sodium levels for concurrent hyperglycemia (serum glucose >150 mg/dL) and high serum paraprotein levels. Assess hydration status and manage hyponatremia per clinical guidelines, including intravenous saline and/or salt tablets as appropriate and dietary review. Interrupt, reduce dose or permanently discontinue based on severity of the adverse reaction [see Dosage and Administration (2.5)].
5.5 Serious Infection
XPOVIO can cause serious and fatal infections. Most of these infections were not associated with Grade 3 or higher neutropenia [see Adverse Reactions (6.1)].
In patients with multiple myeloma who received XPOVIO 100 mg once weekly (BOSTON, n=195), 69% of patients experienced any grade of infection. Grade ≥3 infections were reported in 32% of patients, and deaths from infections occurred in 3.1% of patients. The most frequently reported Grade ≥3 infection was pneumonia in 14% of patients, followed by sepsis in 4.1% and upper respiratory tract infection in 3.6% of patients.
In patients with multiple myeloma who received XPOVIO 80 mg twice weekly (STORM, n=202), 52% of patients experienced any grade of infection. Grade ≥3 infections were reported in 25% of patients, and deaths from infections occurred in 4% of patients within 30 days of last treatment. Upper respiratory tract infection of any grade occurred in 21%, pneumonia in 13%, and sepsis in 6% of patients. The most frequently reported Grade ≥3 infections were pneumonia in 9% of patients, followed by sepsis in 6%. The median time to onset was 54 days for pneumonia and 42 days for sepsis.
In patients with DLBCL (SADAL, n=134), 25% of patients experienced Grade 3 or higher infection and 21% had an infection-related serious adverse reaction; 49% developed an infection of any grade, most frequently involving the upper or lower respiratory tract. The most frequently reported Grade ≥3 infections were lower respiratory tract infections in 9% of patients (including pneumonia in 6%), followed by sepsis (6%). The median time to onset of Grade ≥3 infection was 42 days.
Atypical infections reported after XPOVIO include, but are not limited to, fungal pneumonia and herpes virus infection.
Monitor for signs and symptoms of infection, evaluate and treat promptly.
5.6 Neurological Toxicity
XPOVIO can cause life-threatening neurological toxicities [see Adverse Reactions (6.1)].
In patients with multiple myeloma who received XPOVIO 100 mg once weekly (BOSTON, n=195), neurological adverse reactions (excluding peripheral neuropathy) including dizziness, syncope, depressed level of consciousness, vertigo, amnesia, and mental status changes (including delirium and confusional state) occurred in 26% of patients and severe events (Grade 3-4) occurred in 3.6% of patients. The median time to the first event was 29 days. Permanent discontinuation due to neurological adverse reactions occurred in 2.1% of patients.
In patients with multiple myeloma who received XPOVIO 80 mg twice weekly (STORM, n=202), neurological adverse reactions, including dizziness, syncope, depressed level of consciousness, and mental status changes (including delirium and confusional state) occurred in 30% of patients and severe events (Grade 3-4) occurred in 9% of patients. The median time to the first event was 15 days.
In patients with DLBCL (SADAL, n=134), neurological adverse reactions occurred in 25% of patients and severe events (Grade 3-4) occurred in 6% of patients treated with XPOVIO. The most frequent manifestations were dizziness (16%) and mental status changes (11%), including confusion, cognitive disorders, somnolence, hallucination, delirium, and depressed level of consciousness. Syncope occurred in 2.2% of patients. The median time to the first event was 28 days. Among patients with such neurological adverse reactions, 68% recovered with a median time to recovery of 14 days.
Coadministration of XPOVIO with other products that cause dizziness or mental status changes may increase the risk of neurological toxicity.
Advise patients to refrain from driving and engaging in hazardous occupations or activities, such as operating heavy or potentially dangerous machinery, until the neurological toxicity fully resolves. Optimize hydration status, hemoglobin level, and concomitant medications to avoid exacerbating dizziness or mental status changes. Institute fall precautions as appropriate.
5.7 Embryo-Fetal Toxicity
Based on data from animal studies and its mechanism of action, XPOVIO can cause fetal harm when administered to a pregnant woman. Selinexor administration to pregnant animals during organogenesis resulted in structural abnormalities and alterations to growth at exposures below those occurring clinically at the recommended dose.
Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential and males with a female partner of reproductive potential to use effective contraception during treatment with XPOVIO and for 1 week after the last dose [see Use in Specific Populations (8.1, 8.3)].
5.8 Cataract
New onset or exacerbation of cataract has occurred during treatment with XPOVIO [see Adverse Reactions (6.1)]. In patients with multiple myeloma who received XPOVIO 100 mg once weekly (BOSTON, n=195), the incidence of new onset or worsening cataracts requiring clinical intervention was reported in 22% of patients. The median time to new onset of cataract was 228 days and was 237 days for worsening of cataract in patients presenting with cataract at start of XPOVIO therapy. Treatment of cataracts usually requires surgical removal of the cataract.
-
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are described in detail in other labeling sections:
- Thrombocytopenia [see Warnings and Precautions (5.1)].
- Neutropenia [see Warnings and Precautions (5.2)].
- Gastrointestinal Toxicity [see Warnings and Precautions (5.3)].
- Hyponatremia [see Warnings and Precautions (5.4)].
- Serious Infection [see Warnings and Precautions (5.5)].
- Neurological Toxicity [see Warnings and Precautions (5.6)].
- Cataract [see Warnings and Precautions (5.8)].
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Multiple Myeloma
XPOVIO in Combination with Bortezomib and Dexamethasone (XVd)
The safety of XPOVIO in combination with bortezomib and dexamethasone was evaluated in BOSTON [see Clinical Studies (14.1)]. Patients were randomized to receive XPOVIO 100 mg orally once weekly in combination with bortezomib and dexamethasone (XVd) (n=195) or bortezomib and dexamethasone (Vd) (n=204). Among patients who received XPOVIO, the median duration of XPOVIO treatment was 29 weeks (range: 1 to 120 weeks) and the median dose was 80 mg (range: 30 to 137 mg) per week.
Serious adverse reactions occurred in 52% of patients who received XPOVIO in combination with bortezomib and dexamethasone. Serious adverse reactions in >3% of patients included pneumonia (14%), sepsis, diarrhea and vomiting (4% each). Fatal adverse reactions occurred in 6% of patients within 30 days of last treatment, including pneumonia (n=3) and sepsis (n=3).
Grade ≥2 peripheral neuropathy, a pre-specified key secondary endpoint, was lower in the XVd arm (21%) compared to the Vd arm (34%); odds ratio 0.50 [95% CI: 0.32, 0.79]. The median treatment duration was 30 weeks (range: 1-120 weeks) in patients who received once weekly XVd as compared to 32 weeks (range: 1-122 weeks) in patients who received twice weekly Vd.
Permanent discontinuation of XPOVIO due to an adverse reaction occurred in 19% of patients. Adverse reactions which resulted in permanent discontinuation of XPOVIO in >2% of patients included fatigue (3.6%), nausea (3.1%), thrombocytopenia, decreased appetite, peripheral neuropathy, and vomiting (2.1% each).
Dosage interruptions of XPOVIO due to an adverse reaction occurred in 83% of patients. Adverse reactions which required dosage interruption in >5% of patients included thrombocytopenia (33%), fatigue (13%), asthenia (12%), pneumonia (11%), upper respiratory tract infection (10%), decreased appetite (9%), neutropenia (8%), pyrexia (8%), nausea (7%), bronchitis (7%), diarrhea (6%), weight decreased (6%), and anemia (5%).
Dose reductions of XPOVIO due to an adverse reaction occurred in 64% of patients. Adverse reactions which required dose reductions in >5% of patients included thrombocytopenia (31%), decreased appetite (8%), nausea, fatigue, weight decreased (7% each), and asthenia (6%).
The most common adverse reactions (≥20% with a difference between arms of >5% compared to Vd) were fatigue, nausea, decreased appetite, diarrhea, peripheral neuropathy, upper respiratory tract infection, weight decreased, cataract, and vomiting. Grade 3-4 laboratory abnormalities (≥10%) were thrombocytopenia, lymphopenia, hypophosphatemia, anemia, hyponatremia, and neutropenia.
Table 5 summarizes the adverse reactions in BOSTON.
Table 5: Adverse Reactions (≥10%) in Patients with Multiple Myeloma Who Received XPOVIO in Combination with Bortezomib and Dexamethasone (XVd) with a Difference Between Arms of >5% Compared to Vd in BOSTON Key: X=XPOVIO, Vd=bortezomib-dexamethasone
a. Fatigue includes fatigue and asthenia.
b. Peripheral neuropathy includes neuropathy peripheral, peripheral sensory neuropathy, polyneuropathy, peripheral sensorimotor neuropathy, toxic neuropathy, and peripheral motor neuropathy.
c. Upper respiratory tract infection includes upper respiratory infection, nasopharyngitis, pharyngitis, respiratory syncytial virus infection, respiratory tract infection, rhinitis, and viral upper respiratory tract infection.
d. Vision blurred includes blurred vision, visual acuity reduced, and visual impairment.
Adverse Reaction Weekly XVd (n=195) Twice Weekly Vd (n=204) All Grades (%) Grade 3 or 4 (%) All Grades (%) Grade 3 or 4 (%) Gastrointestinal
Nausea
50
8
10
0Diarrhea 32 6 25 <1 Vomiting 21 4.1 4.4 0 General Conditions
Fatiguea
59
21
28
5Pyrexia 15 1.5 11 1 Metabolism and Nutrition
Decreased appetite
35
3.6
5
0Weight decreased 26 2.1 12 1 Nervous System
Peripheral neuropathyb
32
4.6
47
9Dizziness 12 <1 3.9 0 Infections
Upper respiratory tract infectionc
29
3.6
22
1.5Eye Disorders
Cataract
22
9
6
1.5Vision blurredd 13 <1 6 0 Clinically relevant adverse reactions in <10% of patients who received XPOVIO in combination with bortezomib and dexamethasone included:
- Neurologic disorders: mental status changes (9%) and syncope (3.6%)
Table 6 summarizes selected laboratory abnormalities in BOSTON.
Table 6: Select Laboratory Abnormalities (≥15%) That Worsened from Baseline in Patients with Multiple Myeloma Who Received XPOVIO in Combination with Bortezomib and Dexamethasone (XVd) in BOSTON The denominator used to calculate the rate varied from 91 to 201 based on the number of patients with at least one post-treatment value.
a. Includes one fatal anemia.
Laboratory Abnormality Weekly XVd Twice Weekly Vd All Grades
(%)Grade 3 or 4
(%)All Grades
(%)Grade 3 or 4
(%)Hematologic
Platelet count decrease
92
43
51
19Lymphocyte count decrease 77 38 70 27 Hemoglobin decrease 71 17 51a 12 Neutrophil count decrease 48 12 19 7 Chemistry
Glucose increase
62
3.8
47
4.1Phosphate decrease 61 23 42 11 Sodium decrease 58 14 25 3 Calcium decrease 55 2.1 47 1 Blood urea nitrogen increase 41 5 40 5 Creatinine increase 28 3.6 24 1.5 Potassium decrease 27 6 22 3.5 Magnesium decrease 27 <1 23 1.5 Potassium increase 18 4.1 21 2.5 Hepatic
ALT increase
33
3.1
30
<1Albumin decrease 27 <1 35 <1 AST increase 24 1.5 19 <1 Bilirubin increase 16 1 13 2 ALP increase 12 0 16 <1 XPOVIO in Combination with Dexamethasone (Xd)
The safety of XPOVIO in combination with dexamethasone was evaluated in STORM [see Clinical Studies (14.1)]. Patients received XPOVIO 80 mg orally with dexamethasone 20 mg on Days 1 and 3 of every week (n=202). The median duration of XPOVIO treatment was 8 weeks (range: 1 to 60 weeks). The median dose was 115 mg (range: 36 to 200 mg) per week.
Fatal adverse reactions occurred in 9% of XPOVIO treated patients. Serious adverse reactions occurred in 58% of patients.
The treatment discontinuation rate due to adverse reactions was 27%; 53% of patients had a reduction in the XPOVIO dose, and 65% had the dose of XPOVIO interrupted. Thrombocytopenia was the leading cause of dose modification, resulting in dose reduction and/or interruption in >25% of patients. The most frequent adverse reactions requiring permanent discontinuation in 4% or greater of patients who received XPOVIO included fatigue, nausea, and thrombocytopenia.
Table 7 summarizes the adverse reactions in STORM.
Table 7: Adverse Reactions (≥10%) in Patients Who Received XPOVIO in STORM a. Thrombocytopenia includes thrombocytopenia and platelet count decreased.
b. Fatigue includes fatigue and asthenia.
c. Anemia includes anemia and hematocrit decreased.
d. Neutropenia includes neutropenia and neutrophil count decreased.
e. Dyspnea includes dyspnea, dyspnea exertional, and dyspnea at rest.
f. Upper respiratory tract infection includes upper respiratory tract infection, respiratory tract infection, pharyngitis, nasopharyngitis, bronchitis, bronchiolitis, respiratory syncytial virus infection, parainfluenza virus infection, rhinitis, rhinovirus infection, and adenovirus infection.
g. Cough includes cough, productive cough, and upper-airway cough syndrome.
h. Mental status changes includes mental status changes, confusional state, and delirium.
i. Hypercreatininemia includes hypercreatininemia and hypercreatinemia.
j. Pneumonia includes pneumonia, atypical pneumonia, lung infection, lower respiratory tract infection, pneumocystis jirovecii pneumonia, pneumonia aspiration, pneumonia influenzal, and pneumonia viral.
k. Includes fatal event.
Adverse Reaction XPOVIO 80 mg twice weekly +
Dexamethasone (n=202)All Grades
(%)Grades ≥3
(%)Thrombocytopeniaa 74 61 Fatigueb 73 22 Nausea 72 9 Anemiac 59 40 Decreased appetite 53 4.5 Weight decreased 47 0.5 Diarrhea 44 6 Vomiting 41 3.5 Hyponatremia 39 22 Neutropeniad 34 21 Leukopenia 28 11 Constipation 25 1.5 Dyspneae 24 3.5k Upper respiratory tract infectionf 21 3 Coughg 16 0 Mental status changesh 16 7 Pyrexia 16 0.5 Hyperglycemia 15 7 Dizziness 15 0 Insomnia 15 2 Lymphopenia 15 10 Dehydration 14 3.5 Hypercreatininemiai 14 2 Pneumoniaj 13 9k Epistaxis 12 0.5 Hypokalemia 12 3.5 Dysgeusia 11 0 Vision blurred 10 0.5 Headache 10 0 Diffuse Large B-Cell Lymphoma
The safety of XPOVIO was evaluated in SADAL [see Clinical Studies (14.2)]. Patients received XPOVIO 60 mg orally on Days 1 and 3 of every week (n=134). The study required an absolute neutrophil count ≥1000/μL, platelet count ≥75,000/μL, hepatic transaminases ≤2.5 times upper limit of normal (ULN) unless abnormal from lymphoma, and bilirubin ≤2 times ULN. The study permitted a maximum of 5 prior systemic regimens for DLBCL. Antiemetic prophylaxis with a 5HT-3 receptor antagonist was required. The median duration of XPOVIO treatment was 2.1 months (range: 1 week to 3.7 years) with 38% receiving at least 3 months and 22% receiving at least 6 months of treatment. The median exposure was 100 mg per week.
Fatal adverse reactions occurred in 3.7% of patients within 30 days and 5% of patients within 60 days of last treatment; the most frequent fatal adverse reaction was infection (4.5% of patients). Serious adverse reactions occurred in 46% of patients who received XPOVIO; the most frequent serious adverse reaction was infection (21% of patients).
Discontinuation due to adverse reactions occurred in 17% of patients who received XPOVIO. Adverse reactions which results in discontinuation in ≥2% of patients included: infection, fatigue, thrombocytopenia, and nausea.
Adverse reactions led to XPOVIO dose interruption in 61% of patients and dose reduction in 49%, with 17% of all patients having 2 or more dose reductions. The median time to first dose modification (reduction or interruption) was 4 weeks, with the leading causes being thrombocytopenia (40% of all patients), neutropenia (16%), fatigue (16%), nausea (10%), and anemia (10%). The median time to first dose reduction was 6 weeks, with 83% of first dose reductions occurring within the first 3 months.
The most common adverse reactions, excluding laboratory abnormalities, in ≥20% of patients were fatigue, nausea, diarrhea, decreased appetite, weight decreased, constipation, vomiting, and pyrexia. Table 8 summarizes selected adverse reactions in SADAL.
Table 8: Adverse Reactions (≥10%), Excluding Laboratory Terms, in Patients with DLBCL Who Received XPOVIO in SADAL a. Fatigue includes fatigue and asthenia.
b. Edema includes edema, swelling, swelling face, edema peripheral, peripheral swelling, acute pulmonary edema.
c. Diarrhea includes diarrhea, post-procedural diarrhea, gastroenteritis.
d. Abdominal pain includes abdominal pain, abdominal pain upper, abdominal discomfort, epigastric discomfort.
e. Decreased appetite includes decreased appetite and hypophagia.
f. Cough includes cough and productive cough.
g. Dyspnea includes dyspnea and dyspnea exertional.
h. Upper respiratory tract infection includes upper respiratory tract infection, sinusitis, nasopharyngitis, pharyngitis, rhinitis, viral upper respiratory infection.
i. Urinary tract infection includes urinary tract infection and specific types of urinary tract infection.
j. Dizziness includes dizziness and vertigo.
k. Taste disorder includes taste disorder, dysgeusia, ageusia.
l. Mental status changes include confusional state, amnesia, cognitive disorder, hallucination, delirium, somnolence, depressed level of consciousness, memory impairment.
m. Peripheral neuropathy includes peripheral neuropathy, peripheral sensory neuropathy, sensory disturbance, paresthesia, neuralgia.
n. Musculoskeletal pain includes musculoskeletal pain, back pain, musculoskeletal chest pain, neck pain, pain in extremity, bone pain.
o. Hemorrhage includes hemorrhage, hematoma, hematuria, epistaxis, rectal hemorrhage, injection site hematoma, subdural hematoma, upper gastrointestinal hemorrhage, corneal bleeding.
p. Vision blurred includes vision blurred, visual acuity reduced, visual impairment.
Adverse Reaction XPOVIO 60 mg twice weekly
(n=134)All Grades
(%)Grade 3 or 4
(%)General Conditions
Fatiguea
63
15Pyrexia 22 4.5 Edemab 17 2.2 Gastrointestinal
Nausea
57
6Diarrheac 37 3.0 Constipation 29 0 Vomiting 28 1.5 Abdominal paind 10 0 Adverse Reaction XPOVIO 60 mg twice weekly
(n=134)All Grades (%) Grade 3 or 4 (%) Metabolism and Nutrition
Decreased appetitee
37
3.7Weight decreased 30 0 Respiratory
Coughf
18
0Dyspneag 10 1.5 Infections
Upper respiratory tract infectionh
17
1.5Pneumonia 10 6 Urinary tract infectioni 10 3 Nervous System
Dizzinessj
16
0.7Taste disorderk 13 0 Mental status changesl 11 3.7 Peripheral neuropathy, sensorym 10 0 Musculoskeletal
Musculoskeletal painn
15
2.2Vascular
Hypotension
13
3.0Hemorrhageo 10 0.7 Eye Disorders
Vision blurredp
11
0.7Clinically relevant adverse reactions in <10% of patients who received XPOVIO included:
- Injury: fall (8%)
- Metabolic and nutrition disorders: dehydration (7%)
- Neurologic disorders: headache (4.5%), syncope (2.2%)
- Infection: sepsis (6%), herpes virus infection (3%)
- Eye disorders: cataract (3.7%)
- Blood and lymphatic disorders: febrile neutropenia (3%)
- Cardiac disorders: cardiac failure (3%)
Table 9 summarizes selected new or worsening laboratory abnormalities in SADAL. Grade 3-4 laboratory abnormalities in ≥15% included thrombocytopenia, lymphopenia, neutropenia, anemia, and hyponatremia. Grade 4 laboratory abnormalities in ≥5% were thrombocytopenia (18%), lymphopenia (5%), and neutropenia (9%).
Table 9: Select Laboratory Abnormalities (≥15%) Worsening from Baseline in Patients with DLBCL Who Received XPOVIO in SADAL The denominator used to calculate the rate varied from 107 to 128 based on the number of patients with at least one post-treatment value.
a. Not fasting.
b. CK increase was not associated with reports of myopathy or myalgia.
Laboratory Abnormality XPOVIO 60 mg twice weekly All Grades
(%)Grade 3 or 4
(%)Hematologic
Platelet count decrease
86
49Hemoglobin decrease 82 25 Lymphocyte count decrease 63 37 Neutrophil count decrease 58 31 Chemistry
Sodium decrease
62
16Glucose increase 57a 5 Creatinine increase 47 3.9 Phosphate decrease 34 11 Magnesium decrease 30 2.6 Calcium decrease 30 0.9 Potassium increase 26 3.9 Potassium decrease 23 7 CK increaseb 21 1.9 Hepatic
ALT increase
29
0.8Albumin decrease 25 0 AST increase 24 3.1 Bilirubin increase 16 1.6 -
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Based on findings in animal studies and its mechanism of action [see Clinical Pharmacology (12.1)], XPOVIO can cause fetal harm when administered to a pregnant woman. There are no available data in pregnant women to inform the drug-associated risk. In animal reproduction studies, administration of selinexor to pregnant rats during organogenesis resulted in structural abnormalities and alterations to growth at exposures that were below those occurring clinically at the recommended dose (see Data). Advise pregnant women of the risks to a fetus.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Data
Animal data
In an embryo-fetal development study in pregnant rats, daily oral administration of selinexor at 0, 0.25, 0.75, or 2 mg/kg throughout organogenesis caused incomplete or delayed ossification, skeletal variations, and reduced fetal weight compared with controls at a dose of 0.75 mg/kg (approximately 0.08-fold of human area under the curve [AUC] at the recommended dose). Malformations were observed at 2 mg/kg, including microphthalmia, fetal edema, malpositioned kidney, and persistent truncus arteriosus.
8.2 Lactation
Risk Summary
There is no information regarding the presence of selinexor or its metabolites in human milk, or their effects on the breastfed child or milk production. Because of the potential for serious adverse reactions in a breastfed child, advise women not to breastfeed during treatment with XPOVIO and for 1 week after the last dose.
8.3 Females and Males of Reproductive Potential
XPOVIO can cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)].
Pregnancy Testing
Verify the pregnancy status of females of reproductive potential prior to initiating XPOVIO [see Use in Specific Populations (8.1)].
Contraception
Infertility
Females and Males
Based on findings in animals, XPOVIO may impair fertility in females and males of reproductive potential [see Nonclinical Toxicology (13.1)].
8.4 Pediatric Use
The safety and effectiveness of XPOVIO have not been established in pediatric patients.
8.5 Geriatric Use
In BOSTON, of the 195 patients with multiple myeloma who received XPOVIO in combination with bortezomib and dexamethasone, 56% were 65 years of age and older, while 17% were 75 years of age and older. No overall differences in effectiveness were observed between these patients and younger patients. When comparing patients 65 years of age and older to younger patients, older patients had a higher incidence of discontinuation due to an adverse reaction (28% vs 13%) and a higher incidence of serious adverse reactions (56% vs 47%).
In STORM, of the 202 patients with multiple myeloma who received XPOVIO, 49% were 65 years of age and older, while 11% were 75 years of age and older. No overall difference in effectiveness was observed in patients over 65 years of age, including patients over 75 years of age, when compared with younger patients. When comparing patients 75 years of age and older to younger patients, older patients had a higher incidence of discontinuation due to an adverse reaction (44% vs 27%), higher incidence of serious adverse reactions (70% vs 58%), and higher incidence of fatal adverse reactions (17% vs 9%).
Among 134 patients with DLBCL who received XPOVIO in SADAL, 61% were 65 years of age and older, while 25% were 75 years of age and older. Clinical studies of XPOVIO in patients with relapsed or refractory DLBCL did not include sufficient numbers of patients aged 65 and over to determine whether they respond differently from younger patients.
-
11 DESCRIPTION
Selinexor is a nuclear export inhibitor. Selinexor is (2Z)-3-{3-[3,5-bis(trifluoromethyl)phenyl]-1H-1,2,4-triazol-1yl}-N'-(pyrazin-2-yl)prop-2-enehydrazide. It is a white to off-white powder and has the molecular formula C17H11F6N7O and a molecular mass of 443.31 g/mol. The molecular structure is shown below:
XPOVIO tablets for oral dosing are supplied in four strengths, with each tablet containing 20 mg, 40 mg, 50 mg, or 60 mg of selinexor as the active ingredient. The inactive ingredients are colloidal silicon dioxide, croscarmellose sodium, magnesium stearate, microcrystalline cellulose, Opadry 200 clear, Opadry II blue, povidone K30, and sodium lauryl sulfate.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
In nonclinical studies, selinexor reversibly inhibits nuclear export of tumor suppressor proteins (TSPs), growth regulators, and mRNAs of oncogenic proteins by blocking exportin 1 (XPO1). XPO1 inhibition by selinexor leads to accumulation of TSPs in the nucleus and reductions in several oncoproteins, such as c-myc and cyclin D1, cell cycle arrest, and apoptosis of cancer cells. Selinexor demonstrated pro-apoptotic activity in vitro in multiple myeloma cells and showed anti-tumor activity in murine xenograft models of multiple myeloma and diffuse large B cell lymphoma. The combination of selinexor and dexamethasone or bortezomib demonstrated synergistic cytotoxic effects in multiple myeloma in vitro and increased anti-tumor activity in murine xenograft multiple myeloma models in vivo, including those resistant to proteasome inhibitors.
12.2 Pharmacodynamics
An increase in selinexor exposure was associated with an increase in the probability of dose modification and some adverse reactions.
Cardiac Electrophysiology
The effect of multiple doses of XPOVIO, up to 175 mg per dose (1.75 times the maximum approved recommended dose), on the QTc interval was evaluated in patients with heavily pretreated hematologic malignancies. XPOVIO had no large effect (i.e. no greater than 20 ms) on QTc interval at the therapeutic dose level.
12.3 Pharmacokinetics
Selinexor Cmax and AUC increased proportionally over a dose range from 3 mg/m2 to 85 mg/m2 (0.05 to 1.44) times the maximum approved recommended dose, based on 1.7 m2 body surface area. No clinically relevant accumulation at steady state was observed. Selinexor Cmax and AUC0-INF after administration of a single dose of XPOVIO in patients with hematologic malignancies are presented in Table 10.
Table 10: Selinexor Cmax and AUC After Administration of a Single Dose of XPOVIO Mean (XD) XPOVIO Dose 60 mg 80 mg 100 mg Cmax (ng/mL) 442 (188) 680 (124) 693 (201) AUC0-INF (ng·h/mL) 4,096 (1,185) 5,386 (1,116) 6,998 (818) Effect of Food
Concomitant administration of a high-fat meal (800 to 1,000 calories with approximately 50% of total caloric content of the meal from fat) did not affect the pharmacokinetics of selinexor to a clinically significant extent.
Distribution
The apparent volume of distribution of selinexor is 133 L in patients with cancer. The protein binding of selinexor is 95%.
Elimination
Following a single dose of XPOVIO, the mean half-life is 6 to 8 hours. The apparent total clearance of selinexor is 18.6 L/h in patients with cancer.
Metabolism
Selinexor is metabolized by CYP3A4, multiple UDP-glucuronosyltransferases (UGTs) and glutathione Stransferases (GSTs).
Specific Populations
No clinically significant differences in the pharmacokinetics of selinexor were observed based on age (18 to 94 years old), sex, body weight (36 to 168 kg), ethnicity, mild to severe renal impairment (CLCR: 15 to 89 mL/min, estimated by the Cockcroft-Gault equation), and disease type (hematological non-DLBCL, solid tumor, DLBCL). The effect of end-stage renal disease (CLCR <15 mL/min) or hemodialysis on selinexor pharmacokinetics is unknown. Mild hepatic impairment had no clinically significant effect on the pharmacokinetics of selinexor. The effect of moderate and severe hepatic impairment on selinexor pharmacokinetics is unknown.
Clinical Studies
Acetaminophen: No clinically significant differences in selinexor pharmacokinetics were observed when coadministered with acetaminophen (up to 1,000 mg daily dose of acetaminophen).
Clarithromycin (a strong CYP3A4 inhibitor): No clinically significant differences in selinexor pharmacokinetics were observed when co-administered with clarithromycin (up to 1,000 mg daily dose of clarithromycin).
In vitro Studies
CYP Enzymes: Selinexor does not inhibit CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, or CYP3A4/5. Selinexor is not a CYP3A4, CYP1A2, or CYP2B6 inducer.
Non-CYP Enzyme Systems: Selinexor is a substrate of UGTs and GSTs.
Transporter Systems: Selinexor inhibits OATP1B3 but does not inhibit other solute carrier (SLC) transporters.
Selinexor is not a substrate of P-gp, BCRP, OATP1B1, OATP1B3, OAT1, OAT3, OCT1, OCT2, MATE1, or MATE2-K.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been conducted with selinexor.
Selinexor was not mutagenic in vitro in a bacterial reverse mutation (Ames) assay and was not clastogenic in either the in vitro cytogenetic assay in human lymphocytes or in the in vivo rat micronucleus assay.
Fertility studies in animals have not been conducted with selinexor. In repeat-dose oral toxicity studies, selinexor was administered for up to 13 weeks in rats and monkeys. Reduced sperm, spermatids, and germ cells in epididymides and testes were observed in rats at ≥1 mg/kg, decreased ovarian follicles were observed in rats at ≥2 mg/kg, and single cell necrosis of testes was observed in monkeys at ≥1.5 mg/kg. These dose levels resulted in systemic exposures approximately 0.11, 0.28, and 0.53 times, respectively, the exposure (AUClast) in humans at the recommended human dose of 80 mg.
-
14 CLINICAL STUDIES
14.1 Relapsed or Refractory Multiple Myeloma
XPOVIO Combination with Bortezomib and Dexamethasone (XVd)
The efficacy of XPOVIO in combination with bortezomib and dexamethasone was evaluated in BOSTON (NCT03110562). BOSTON was a global, randomized, open label, active-controlled trial in adult patients who had received 1 to 3 prior anti-MM regimens. Prior treatment with bortezomib or other PI was allowed.
Patients with Grade 2 or higher peripheral neuropathy at study entry were excluded.
Patients were randomized to receive one of the following:
- XPOVIO 100 mg orally once weekly on Days 1, 8, 15, 22, 29 in combination with bortezomib 1.3 mg/m2 administered subcutaneously once weekly on Days 1, 8, 15, 22 and dexamethasone 20 mg taken orally twice weekly on Days 1, 2, 8, 9, 15, 16, 22, 23, 29, and 30 of each 35-day cycle [XVd arm] or
- Bortezomib 1.3 mg/m2 administered subcutaneously twice weekly on Days 1, 4, 8, 11 and dexamethasone 20 mg taken orally four times weekly on Days 1, 2, 4, 5, 8, 9, 11, 12 of each 21-day cycle for the first 8 cycles, followed by bortezomib 1.3 mg/m2 administered subcutaneously once weekly on Days 1, 8, 15, 22 and dexamethasone 20 mg taken orally twice weekly on Days 1, 2, 8, 9, 15, 16, 22, 23, 29, and 30 of each 35-day cycle (Cycle ≥9) [Vd arm].
Treatment continued in both arms until disease progression or unacceptable toxicity. Randomization was stratified based on prior proteasome inhibitor therapies exposure (yes versus no), number of prior regimens (1 versus >1), Stage (III versus I or II) according to the Revised-International Staging System (RISS) and region. Upon confirmed progressive disease (PD), patients in the Vd arm could receive XPOVIO in combination with bortezomib and dexamethasone (XVd) or XPOVIO 100 mg taken orally on Days 1, 8, 15, 22, 29 with dexamethasone 20 mg taken orally on Days 1, 2, 8, 9, 15, 16, 22, 23, 29, and 30 of each 35-day cycle.
A total of 402 patients were randomized: 195 to XVd arm and 207 to Vd arm. Baseline patient demographics and disease characteristics are summarized in Table 11 and Table 12, respectively.
Table 11: Baseline Demographics (BOSTON) Characteristic XVd
(n=195)Vd
(n=207)Median age, years (range) 66 (40, 87) 67 (38, 90) Age distribution, n (%)
<65 years
86 (44)
75 (36)65 – 74 years 75 (38) 85 (41) ≥75 years 34 (17) 47 (23) Sex, n (%)
Male
115 (59)
115 (56)Female 80 (41) 92 (44) Race, n (%)
White
161 (83)
165 (80)Black or African American 4 (2) 7 (3) Asian 25 (13) 25 (12) Other 0 1 (0.5) Missing 5 (3) 9 (4) Table 12: Disease Characteristics (BOSTON) a. Includes any of del (17p)/p53, t (14;16), t (4;14), 1q21.
Parameter XVd (n=195) Vd (n=207) Median years from diagnosis to randomization (range) 3.81 (0.4,23.0) 3.59 (0.4, 22.0) ECOG performance status score, n (%)
0-1
175 (90)
191 (92)≥2 20 (10) 16 (8) Creatinine Clearance, n (%), mL per minute
<30
3 (1.5)
10 (5)30 to 59 53 (27) 60 (29) ≥60 139 (71) 137 (66) Revised International Staging System at Baseline, n (%)
I
56 (29)
52 (25)II 117 (60) 125 (60) III 12 (6) 16 (8) Unknown 10 (5) 14 (7) Number of Prior Therapies, n (%)
1
2
3
99 (51)
65 (33) 31 (16)
99 (48)
64 (31) 44 (21)Type of known prior therapy, n (%) Stem
Cell transplantation
76 (39)
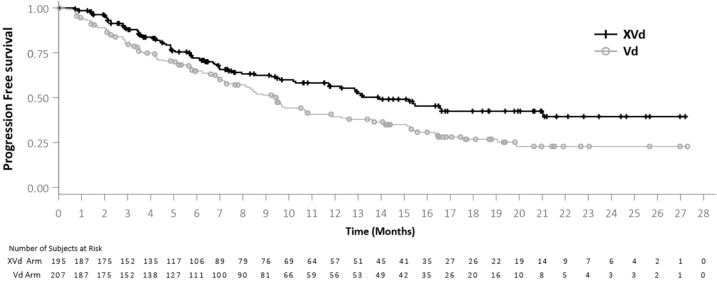
63 (30)Lenalidomide 77 (39) 77 (37) Pomalidomide 11 (6) 7 (3) Bortezomib 134 (69) 145 (70) Carfilzomib 20 (10) 21 (10) Daratumumab 11 (6) 6 (3) Median weeks since end of last prior therapy, (range) 48 (1, 1088) 42 (2, 405) Known high-risk cytogeneticsa, n (%) 97 (50) 95 (46) Efficacy was based on progression free survival (PFS) according to the International Myeloma Working Group (IMWG) Uniform Response Criteria for Multiple Myeloma, as assessed by an Independent Review Committee (IRC). Efficacy results based on a preplanned PFS interim analysis, are shown in Table 13 and Figure 1.
Table 13: Efficacy Results per IRC in Multiple Myeloma (BOSTON) a. Hazard ratio is based on stratified Cox's proportional hazard regression modeling, p-value based on stratified log-rank test.
Median follow up of 15.1 months at the time of the analysis.
b. The pre-planned PFS interim analysis boundary of statistical significance was defined as a p-value <0.0103.
c. Includes sCR + CR + VGPR + PR, p value based on Cochran-Mantel-Haenszel test.
d. Includes sCR + CR + VGPR, p value based on Cochran-Mantel-Haenszel test.
XVd
(n=195)Vd
(n=207)Progression Free Survival (PFS)a
Hazard Ratio [95% CI]
0.70 [0.53, 0.93]One-sided p-valueb 0.0075
Median PFS in months [95% CI]13.9 (11.7, Not Reached) 9.5 (7.6, 10.8) Overall Response Rate (ORR)c, n (%) 149 (76.4) 129 (62.3) 95% CI (69.8, 82.2) (55.3, 68.9) One-sided p-value 0.0012
Stringent Complete Response (sCR)19 (10) 13 (6) Complete Response (CR) 14 (7) 9 (4) Very Good Partial Response (VGPR) 54 (28) 45 (22) Partial Response (PR) 62 (32) 62 (30) ≥ VGPR Response Rated, n (%) 87 (44.6) 67 (32.4) 95% CI (37.5, 51.9) (26.0, 39.2) One-sided p-value 0.0082 Figure 1: Kaplan-Meier Curve of PFS (BOSTON)
The median time to response was 1.4 months in the XVd arm and 1.6 months in the Vd arm. The median duration of response, among responding patients, was 20.3 months and 12.9 months in the XVd and Vd arms, respectively.
XPOVIO Combination with Dexamethasone (Xd)
The efficacy of XPOVIO plus dexamethasone was evaluated in STORM (KCP-330-012; NCT02336815). STORM was a multicenter, single-arm, open-label study of adults with relapsed or refractory multiple myeloma (RRMM). STORM Part 2 included 122 patients with RRMM who had previously received three or more antimyeloma treatment regimens including an alkylating agent, glucocorticoids, bortezomib, carfilzomib, lenalidomide, pomalidomide, and an anti-CD38 monoclonal antibody; and whose myeloma was documented to be refractory to glucocorticoids, a proteasome inhibitor, an immunomodulatory agent, an anti-CD38 monoclonal antibody, and to the last line of therapy.
In STORM Part 2, a total of 122 patients received XPOVIO 80 mg orally in combination with dexamethasone 20 mg orally on Days 1 and 3 of every week. Treatment continued until disease progression or unacceptable toxicity. Eighty-three patients had RRMM that was refractory to bortezomib, carfilzomib, lenalidomide, pomalidomide, and daratumumab. Baseline patient demographics and disease characteristics of these 83 patients are summarized in Table 14 and Table 15, respectively.
Efficacy was based on overall response rate (ORR), as assessed by an Independent Review Committee (IRC) based on the International Myeloma Working Group (IMWG) Uniform Response Criteria for Multiple
Myeloma. The approval of XPOVIO was based upon the efficacy and safety in a prespecified subgroup analysis of the 83 patients whose disease was refractory to bortezomib, carfilzomib, lenalidomide, pomalidomide, and daratumumab, as the benefit-risk ratio appeared to be greater in this more heavily pretreated population than in the overall trial population. Overall response rate results are presented in Table 16. The median time to first response was 4 weeks (range: 1 to 10 weeks). The median duration of response was 3.8 months (95% CI: 2.3, not estimable).
Table 14: Baseline Demographics (STORM) Demographic STORM
(n=83)Median age, years (range) 65 (40, 86) Age category, n (%) <65 years 40 (48) 65 – 74 years 31 (37) ≥75 years 12 (15) Sex, n (%) Male 51 (61) Female 32 (39) Race, n (%) White 58 (70) Black or African American 13 (16) Asian 2 (2) Native Hawaiian or other Pacific Islander 1 (1) Other 6 (7) Missing 3 (4) Table 15: Disease Characteristics (STORM) a. Includes any of del(17p)/p53, t(14; 16), t(4; 14), 1q21.
Parameter STORM
(n=83)Median years from diagnosis to start of study treatment (range) 7 (1, 23) Prior treatment regimens, median (range) 8 (4, 18) Documented refractory status, n (%)
Lenalidomide
83 (100)Pomalidomide 83 (100) Bortezomib 83 (100) Carfilzomib 83 (100) Daratumumab 83 (100) Documented refractory status to specific combinations, n (%)
Bortezomib, carfilzomib, lenalidomide, pomalidomide, and daratumumab
83 (100)Daratumumab in any combination 57 (69) Daratumumab as single agent (+/- dexamethasone) 26 (31) Previous stem cell transplant, n (%) 67 (81) Revised International Staging System at Baseline, n (%)
I
10 (12)II 56 (68) III 17 (21) Unknown 0 High-risk cytogeneticsa, n (%) 47 (57) Table 16: Efficacy Results per IRC in Relapsed or Refractory Multiple Myeloma (STORM) a. Includes sCR + CR + VGPR + PR.
Response STORM
(n=83)Overall Response Rate (ORR)a, n (%) 21 (25.3) 95% CI 16.4, 36 Stringent Complete Response (sCR) 1 (1) Complete Response (CR) 0 Very Good Partial Response (VGPR) 4 (5) Partial Response (PR) 16 (19) 14.2 Relapsed or Refractory Diffuse Large B-Cell Lymphoma
The efficacy of XPOVIO monotherapy was evaluated in SADAL (KCP-330-009; NCT02227251). SADAL was a multicenter, single-arm, open-label study of adults with relapsed or refractory DLBCL, not otherwise specified (NOS), after 2 to 5 systemic regimens. Eligible patients were not candidates for autologous hematopoietic stem cell transplantation (HSCT). The study required a minimum of 60 days since last systemic therapy, with a minimum of 98 days in patients with refractory disease (defined as less than partial response) to last systemic therapy.
Patients received XPOVIO 60 mg orally on Days 1 and 3 of each week. Treatment continued until disease progression or unacceptable toxicity.
Of 134 patients evaluated, the median age was 67 years (range: 35-91), 59% were male, 79% were White, and
7% were Asian. Most patients (88%) had an ECOG performance status of 0 or 1. The diagnosis was de novo
DLBCL not otherwise specified (NOS) in 75% and transformed DLBCL in 23%. The median number of prior systemic therapies was 2 (range: 1-5), with 63% of patients receiving 2 prior systemic therapies, 24% receiving 3 prior therapies, and 10% receiving 4 or 5 prior therapies. Twenty-eight percent had documented refractory disease to the most recent therapy; 30% had prior autologous HSCT. The median time from last systemic therapy to the start of XPOVIO was 5.4 months overall and 3.6 months in the patients with refractory disease.
Efficacy was based on overall response rate (ORR) and duration of response as assessed by an Independent Review Committee (IRC) using Lugano 2014 criteria (Table 17). The median time to first response was 8.1 weeks (range: 6.7-16.4 weeks).
Table 17: Efficacy Results per IRC in Relapsed or Refractory DLBCL (SADAL)
ParameterXPOVIO 60 mg twice weekly
(n=134)ORR per Lugano criteria, n (%)
95% CI, %39 (29)
22, 38Complete Response 18 (13) Partial Response 21 (16) Duration of Response
Patients maintaining response at 3 months, n/N (%)
22/39 (56)Patients maintaining response at 6 months, n/N (%) 15/39 (38) Patients maintaining response at 12 months, n/N (%) 6/39 (15) -
16 HOW SUPPLIED/STORAGE AND HANDLING
XPOVIO 20 mg tablets are blue, round, bi-convex, film-coated debossed with “K20” on one side and nothing on the other side.
XPOVIO 40 mg tablets are blue, oval, film-coated, debossed on both sides with “X40”.
XPOVIO 50 mg tablets are blue, oval, film-coated, debossed on both sides with “X50”.
XPOVIO 60 mg tablets are blue, oval, film-coated, debossed on both sides with “X60”.
Tablets are packaged in a child-resistant blister pack. Four blister packs are supplied per carton. The following twelve dose presentations are available:
Weekly dose Strength per tablet Carton (28 day supply) Blister Pack NDC 80 mg twice weekly 20 mg 4 blister packs
(32 tablets total in the
carton)Each blister has eight 20 mg tablets Outer carton NDC
72237-101-04
Blister pack NDC
72237-101-1460 mg twice weekly 20 mg 4 blister packs
(24 tablets total in the
carton)Each blister has six 20 mg tablets Outer carton NDC
72237-101-03
Blister pack NDC
72237-101-13100 mg once weekly 20 mg 4 blister packs
(20 tablets total in the
carton)Each blister has five 20 mg tablets Outer carton NDC
72237-101-05
Blister pack NDC
72237-101-1580 mg once weekly 20 mg 4 blister packs
(16 tablets total in the
carton)Each blister has four 20 mg tablets Outer carton NDC
72237-101-02
Blister pack NDC
72237-101-1240 mg twice weekly 20 mg 4 blister packs
(16 tablets total in the
carton)Each blister has four 20 mg tablets Outer carton NDC
72237-101-06
Blister pack NDC
72237-101-1660 mg once weekly 20 mg 4 blister packs
(12 tablets total in the
carton)Each blister has three 20 mg tablets Outer carton NDC
72237-101-01
Blister pack NDC
72237-101-1140 mg once weekly 20 mg 4 blister packs
(8 tablets total in the carton)Each blister has two 20 mg tablets Outer carton NDC
72237-101-07
Blister pack NDC
72237-101-17100 mg once weekly 50 mg 4 blister packs
(8 tablets total in the carton)Each blister has two 50 mg tablets Outer carton NDC 72237-103-05
Blister pack NDC
72237-103-1580 mg once weekly 40 mg 4 blister packs
(8 tablets total in the carton)Each blister has two 40 mg tablets Outer carton NDC 72237-102-02
Blister pack NDC
72237-102-1240 mg twice weekly 40 mg 4 blister packs
(8 tablets total in the carton)Each blister has two 40 mg tablets Outer carton NDC 72237-102-06
Blister pack NDC
72237-102-1660 mg once weekly 60 mg 4 blister packs
(4 tablets total in the carton)Each blister has one 60 mg tablet Outer carton NDC 72237-104-01
Blister pack NDC
72237-104-1140 mg once weekly 40 mg 4 blister packs
(4 tablets total in the carton)Each blister has one 40 mg tablet Outer carton NDC 72237-102-07
Blister pack NDC
72237-102-17Store at or below 30°C (86°F).
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Dosing Instructions [see Dosage and Administration (2)]:
- Instruct patients to take XPOVIO exactly as prescribed.
- Advise patients to swallow the tablet whole with water. The tablet should not be broken, chewed, crushed, or divided.
- If a patient misses a dose, advise them to take their next dose at its regularly scheduled time. If a patient vomits or misses a dose of XPOVIO, advise them to take the next dose on the next regularly scheduled day.
- Advise patients that XPOVIO comes in a child-resistant blister pack.
- Advise patients to take their prescribed dexamethasone (if applicable) and prophylactic anti-nausea medications as directed [see Dosage and Administration (2.1, 2.3)].
- Advise patients that blood tests and body weight will be monitored at baseline and during treatment as clinically indicated, with more frequent monitoring during the first three months of treatment [see Dosage and Administration (2.3)].
- Advise patients to maintain appropriate fluid and caloric intake throughout their treatment [see Dosage and Administration (2.4)].
Hematologic Adverse Reactions
Thrombocytopenia
Advise patients that they may develop low platelet counts (thrombocytopenia). Symptoms of thrombocytopenia may include bleeding and easy bruising. Advise patients that platelet counts will be monitored at baseline, during treatment, and as clinically indicated, with more frequent monitoring during the first 3 months of treatment. Advise patients to report signs of bleeding right away [see Warnings and Precautions (5.1)].
Anemia
Advise patients that they may develop anemia. Symptoms of anemia may include fatigue and shortness of breath. Advise patients to report signs or symptoms of anemia [see Adverse Reactions (6.1)].
Neutropenia
Advise patients that they may develop low neutrophil counts which may increase their susceptibility to infection [see Warnings and Precautions (5.2)]. Advise patients that neutrophil counts will be monitored at baseline, during treatment, and as clinically indicated, with more frequent monitoring during the first 3 months of treatment.
Gastrointestinal Adverse Reactions
Advise patients they may experience nausea/vomiting or diarrhea and to contact their physician if these adverse reactions occur or persist [see Warnings and Precautions (5.3)].
Advise patients that they may experience weight loss or decreased appetite. Advise patients to report decreased appetite and weight loss [see Warnings and Precautions (5.3)].
Hyponatremia
Advise patients that they may develop low sodium levels (hyponatremia). Most cases of hyponatremia were not associated with specific symptoms. Advise patients that levels of sodium will be monitored at baseline and during treatment as clinically indicated, with more frequent monitoring during the first two months of treatment [see Warnings and Precautions (5.4)].
Serious Infection
Advise patients of the possibility of serious infections. Instruct patients to immediately report infection-related signs or symptoms (e.g., chills, fever) [see Warnings and Precautions (5.5)].
Neurotoxicity
Advise patients that they may experience confusion and dizziness. Advise patients to report symptoms of neurological toxicity right away. Advise patients not to drive or operate hazardous machinery until the neurological toxicity fully resolves. Advise patients to use fall prevention measures as warranted [see Warnings and Precautions (5.6)].
Embryo-Fetal Toxicity
Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to contact their healthcare provider of a known or suspected pregnancy [see Warnings and Precautions (5.7) and Use in Specific Populations (8.1)].
Advise females of reproductive potential and males with a female partner of reproductive potential to use effective contraception during treatment with XPOVIO and for 1 week after the final dose [see Use in Specific Populations (8.3)].
Cataract
Advise patients of the potential risk of worsening or new onset of cataract, that may require surgery. Advise patients to readily inform their healthcare professionals of changes in vision (i.e. blurred vision) and that ophthalmologic evaluation may be performed as clinically indicated [see Warnings and Precautions (5.8)].
Lactation
Advise women not to breastfeed during treatment with XPOVIO and for 1 week after the last dose [see Use in Specific Populations (8.2)].
Concomitant Medications
Advise patients to take 5-HT3 antagonist prophylactic treatment and other anti-nausea agents prior to and during treatment with XPOVIO [see Dosage and Administration (2.4)].
Advise patients to speak with their physician about other medications they are currently taking and before starting any new medication.
Manufactured for and marketed by: Karyopharm Therapeutics Inc., 85 Wells Avenue, Newton, MA, 02459.
XPOVIO is a registered trademark of Karyopharm Therapeutics Inc.
©2022 Karyopharm Therapeutics Inc.
For more information, call 1-888-209-9326 or go to www.XPOVIO.com. -
MEDICATION GUIDE
This Medication Guide has been approved by the U.S. Food and Drug Administration.
Revised: 3/2022
MEDICATION GUIDE
XPOVIO® (x-PO-Vee-O)
(selinexor) tabletsWhat is the most important information I should know about XPOVIO?
XPOVIO can cause serious side effects, including:
-
Low platelet counts. Low platelet counts are common with XPOVIO and can lead to bleeding which can be severe and can sometimes cause death. Your healthcare provider may prescribe platelet transfusions or other treatments for your low platelet counts.
Tell your healthcare provider right away if you have any bleeding or easy bruising during treatment with XPOVIO. - Low white blood cell counts. Low white blood cell counts are common with XPOVIO and can sometimes be severe. You may have an increased risk of getting bacterial infections during treatment with XPOVIO. Your healthcare provider may prescribe antibiotics if you have signs or symptoms of infection, or certain medicines to help increase your white blood cell count, if needed.
Your healthcare provider will do blood tests before you start taking XPOVIO and often during the first 3 months of treatment and then as needed during treatment to monitor you for side effects.
Your healthcare provider may change your dose of XPOVIO, stop your treatment for a period of time, or completely stop your treatment if you have certain side effects during treatment with XPOVIO.
See “What are the possible side effects of XPOVIO?” for more information about side effects.What is XPOVIO?
XPOVIO is a prescription medicine used:
- in combination with the medicines VELCADE® (bortezomib) and dexamethasone to treat adults with multiple myeloma (MM) who have received at least one prior treatment for their disease.
- in combination with dexamethasone to treat adults with multiple myeloma (MM) that has come back (relapsed) or that did not respond to previous treatment (refractory), and
- who have received at least 4 prior therapies, and
- whose disease did not respond to (refractory) to at least 2 proteasome inhibitor medicines, at least 2 immunomodulatory agents, and an anti-CD38 monoclonal antibody medicine.
- to treat adults with certain types of diffuse large B-cell lymphoma (DLBCL) that has come back (relapsed) or that did not respond to previous treatment (refractory) and who have received at least 2 prior therapies
It is not known if XPOVIO is safe and effective in children less than 18 years of age. What should I tell my healthcare provider before taking XPOVIO?
Before taking XPOVIO, tell your healthcare provider about all of your medical conditions, including if you:
- have or have had a recent or active infection
- have or have had bleeding problems
- are pregnant or plan to become pregnant. XPOVIO can harm your unborn baby.
Females who are able to become pregnant:- Your healthcare provider will check to see if you are pregnant before you start taking XPOVIO.
- You should use effective birth control (contraception) during treatment with XPOVIO and for 1 week after your last dose.
- Tell your healthcare provider right away if you become pregnant or think you might be pregnant during treatment with XPOVIO.
Males with female partners who are able to become pregnant:
- You should use effective birth control during treatment with XPOVIO and for 1 week after your last dose.
- are breastfeeding or plan to breastfeed. It is not known if XPOVIO passes into your breast milk.
- Do not breastfeed during treatment with XPOVIO and for 1 week after your last dose of XPOVIO.
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. Talk with your healthcare provider before taking any new medicines. - Take XPOVIO exactly as prescribed by your healthcare provider.
- If you have multiple myeloma, your healthcare provider will prescribe dexamethasone with your XPOVIO treatment. Take dexamethasone exactly as prescribed.
- Your healthcare provider will tell you how much XPOVIO to take and when to take it. Do not change your dose or stop taking XPOVIO without talking to your healthcare provider first.
- Swallow XPOVIO tablets whole with water. Do not break, chew, crush, or divide the tablets.
- Be sure to take any medicines prescribed by your healthcare provider before and during treatment with XPOVIO to help prevent nausea and vomiting. Tell your healthcare provider if the prescribed medicine does not control your nausea and vomiting.
- It is important for you to drink enough fluids to help prevent dehydration and to eat enough calories to help prevent weight loss during treatment with XPOVIO. Talk to your healthcare provider if this is a problem for you. See “What are the possible side effects of XPOVIO?”
- If you miss a dose of XPOVIO, take your next dose at your next regularly scheduled day and time.
- If you vomit after taking a dose of XPOVIO, do not take an extra dose. Take your next dose at your next regularly scheduled day and time.
- If you take too much XPOVIO, call your healthcare provider right away.
What should I avoid while taking XPOVIO?
XPOVIO can cause neurologic side effects.
- See “What are the possible side effects of XPOVIO?” below.
- If you have any neurologic side effects with XPOVIO, do not drive or operate heavy or dangerous machinery until your neurologic side effects go away.
- Avoid falling. Use care as needed to avoid falling due to neurologic side effects.
What are the possible side effects of XPOVIO?
XPOVIO can cause serious side effects, including:
- See “What is the most important information I should know about XPOVIO?”
- Nausea and vomiting. Nausea and vomiting are common with XPOVIO and can sometimes be severe. Nausea and vomiting may affect your ability to eat and drink well. You can lose too much body fluid and body salts (electrolytes) and may be at risk for becoming dehydrated. You may need to receive intravenous (IV) fluids or other treatments to help prevent dehydration. Your healthcare provider will prescribe anti-nausea medicines for you to take before you start and during treatment with XPOVIO. See “How should I take XPOVIO?”
- Diarrhea. Diarrhea is common with XPOVIO and can sometimes be severe. You can lose too much body fluid and body salts (electrolytes) and may be at risk for becoming dehydrated. You may need to receive IV fluids or other treatments to help prevent dehydration. Your healthcare provider will prescribe anti-diarrhea medicine for you as needed.
- Loss of appetite and weight loss. Loss of appetite and weight loss are common with XPOVIO and can sometimes be severe. Tell your healthcare provider if you have a decrease or loss of appetite and if you notice that you are losing weight at any time during treatment. Your healthcare provider may prescribe medicines that can help increase your appetite or prescribe other kinds of nutritional support. Your healthcare provider will monitor your appetite and weight before you start XPOVIO and often during the first 3 months, then as needed during treatment.
- Decreased sodium levels in your blood. Decreased sodium levels in your blood is common with XPOVIO but can also sometimes be severe. Low sodium levels in your blood can happen if you have nausea, vomiting, or diarrhea, you become dehydrated, or if you have loss of appetite with XPOVIO. You may not have any symptoms of a low sodium level. Your healthcare provider may talk with you about your diet and prescribe IV fluids for you based on the sodium levels in your blood. Your healthcare provider will do blood tests before you start taking XPOVIO, and often during the first 2 months of treatment, and then as needed during treatment to monitor the sodium levels in your blood.
- Serious infections. Infections are common with XPOVIO and can be serious and can sometimes cause death. XPOVIO can cause infections including upper or lower respiratory tract infections, such as pneumonia, and an infection throughout your body (sepsis). Tell your healthcare provider right away if you have any signs or symptoms of an infection such as cough, chills or fever, during treatment with XPOVIO.
-
Neurologic side effects. XPOVIO can cause neurologic side effects that can sometimes be severe and life- threatening.
- XPOVIO can cause dizziness, fainting, decreased alertness, and changes in your mental status including confusion and decreased awareness of things around you (delirium).
- In some people, XPOVIO may also cause problems with thinking (cognitive problems), seeing or hearing things that are not really there (hallucinations), and may become very sleepy or drowsy.
- Taking other medicines that can cause dizziness or mental status changes during treatment with XPOVIO may increase your risk of neurologic side effects.
Tell your healthcare provider right away if you get any of these signs or symptoms.
- New or worsening cataract, a cloudy or loss of transparency of the lens in the eye. New or worsening cataract are common with XPOVIO. If a cataract forms, your vision may decrease, and you may need eye surgery to remove the cataract and restore your vision. Tell your healthcare provider right away if you have symptoms of a cataract such as double vision, blurred vision, sensitivity to light or glare.
Your healthcare provider may change your dose of XPOVIO, stop your treatment for a period of time, or completely stop your treatment if you have certain side effects during treatment with XPOVIO. Common side effects of XPOVIO include:
- tiredness
- low red blood cell count (anemia). Symptoms may include tiredness and shortness of breath.
- constipation
- shortness of breath
- increased blood sugar
- changes in body salt and mineral levels in your blood
- changes in kidney and liver function blood tests
XPOVIO may cause fertility problems in males and females, which may affect your ability to have children. Talk to your healthcare provider if you have concerns about fertility.
These are not all the possible side effects of XPOVIO.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.How should I store XPOVIO?
- Store XPOVIO at or below 86°F (30°C).
- XPOVIO comes in a child-resistant blister pack.
Keep XPOVIO and all medicines out of the reach of children. General information about the safe and effective use of XPOVIO.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use XPOVIO for a condition for which it was not prescribed. Do not give XPOVIO to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about XPOVIO that is written for health professionals.What are the ingredients in XPOVIO?
Active ingredient: selinexor
Inactive ingredients: colloidal silicon dioxide, croscarmellose sodium, magnesium stearate, microcrystalline cellulose, Opadry 200 clear, Opadry II blue, povidone K30, and sodium lauryl sulfate.
Manufactured for and marketed by: Karyopharm Therapeutics Inc., 85 Wells Avenue, Newton, MA, 02459
XPOVIO is a registered trademark of Karyopharm Therapeutics Inc. All other trademarks are the property of their respective owners.
©2022 Karyopharm Therapeutics Inc.
For more information, call 1-888-209-9326 or go to www.XPOVIO.com -
Low platelet counts. Low platelet counts are common with XPOVIO and can lead to bleeding which can be severe and can sometimes cause death. Your healthcare provider may prescribe platelet transfusions or other treatments for your low platelet counts.
-
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 60 mg (Once Weekly) Carton Label
NDC 72237-101-01
Rx ONLY
60 mg
Once
Weekly
Blister PacksXPOVIO®
(selinexor) tablets
Contents: 4 individual weekly
blister packs. Each blister pack
contains 3 tablets (20 mg per tablet).12 film-coated tablets
Dispense enclosed Medication Guide
to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 60 mg (Once Weekly) Blister Sleeve Label
NDC 72237-101-11
Rx ONLY
1 PRESS
& HOLD
HERE60 mg
Once
Weekly
Blister Pack1. PRESS 2. PULL
XPOVIO®
(selinexor) tablets
TO OPEN
Step 1: Press and
hold button gently.Step 2: Pull out
medication card.Blister pack contains
3 tablets (20 mg per tablet).Refer to Prescribing
Information for dosing
instructions.Do not break, chew, crush,
or divide the tablets.Dispense enclosed Medication
Guide to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 60 mg (Once Weekly) Blister Pack Label
XPOVIO®(selinexor tablets)
60 mg
Dose
(entire pack)Push tablets through foil.
Swallow whole with water.
IMPORTANT: Take each dose as prescribed by your physician.
Take only one 60 mg dose in a single day per week.
Refer to Prescribing Information for dosing instructions.
-
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 80 mg (Once Weekly) Carton Label
NDC 72237-101-02
Rx ONLY
80 mg
Once
Weekly
Blister PacksXPOVIO®
(selinexor) tablets
Contents: 4 individual weekly
blister packs. Each blister pack
contains 4 tablets (20 mg per tablet).16 film-coated tablets
Dispense enclosed Medication Guide
to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 80 mg (Once Weekly) Blister Sleeve Label
NDC 72237-101-12
Rx ONLY
1 PRESS
& HOLD
HERE80 mg
Once
Weekly
Blister Pack1. PRESS 2. PULL
XPOVIO®
(selinexor) tablets
TO OPEN
Step 1: Press and
hold button gently.Step 2: Pull out
medication card.Blister pack contains
4 tablets (20 mg per tablet).Refer to Prescribing
Information for dosing
instructions.Do not break, chew, crush,
or divide the tablets.Dispense enclosed Medication
Guide to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 80 mg (Once Weekly) Blister Pack Label
XPOVIO®(selinexor tablets)
80 mg
Dose
(entire pack)Push tablets
through foil.Swallow
whole with
water.IMPORTANT: Take each dose as prescribed by your physician.
Take only one 80 mg dose in a single day per week.
Refer to Prescribing Information for dosing instructions.
-
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 60 mg (Twice Weekly) Carton Label
NDC 72237-101-03
Rx ONLY
60 mg
Twice
Weekly
Blister Packs(120 mg total weekly dose)
XPOVIO®
(selinexor) tablets
Contents: 4 individual weekly
blister packs. Each blister pack
contains 6 tablets (20 mg per tablet).24 film-coated tablets
Dispense enclosed Medication Guide
to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 60 mg (Twice Weekly) Blister Sleeve Label
NDC 72237-101-13
Rx ONLY
1 PRESS
& HOLD
HERE60 mg
Twice
Weekly
Blister Pack(120 mg total weekly dose)
1. PRESS 2. PULL
XPOVIO®
(selinexor) tablets
TO OPEN
Step 1: Press and
hold button gently.Step 2: Pull out
medication card.Blister pack contains
6 tablets (20 mg per tablet).Refer to Prescribing
Information for dosing
instructions.Do not break, chew, crush,
or divide the tablets.
Dispense enclosed Medication
Guide to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 60 mg (Twice Weekly) Blister Pack Label
XPOVIO®(selinexor tablets)
60 mg
Dose
(entire pack)Push tablets
through foil.Swallow
whole with
water.IMPORTANT: Take each dose as prescribed by your physician.
Take only one 60 mg dose in a single day. Take one 60 mg dose on Day 1 and one 60 mg dose on Day 3 of the week.
Refer to Prescribing Information for dosing instructions.
-
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 80 mg (Twice Weekly) Carton Label
NDC 72237-101-04
Rx ONLY
80 mg
Twice
Weekly
Blister Packs(160 mg total weekly dose)
XPOVIO®
(selinexor) tablets
Contents: 4 individual weekly
blister packs. Each blister pack
contains 8 tablets (20 mg per tablet).32 film-coated tablets
Dispense enclosed Medication Guide
to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 80 mg (Twice Weekly) Blister Sleeve Label
NDC 72237-101-14
Rx ONLY
1 PRESS
& HOLD
HERE80 mg
Twice
Weekly
Blister Pack(160 mg total weekly dose)
1.PRESS 2. PULL
XPOVIO®
(selinexor) tablets
TO OPEN
Step 1: Press and
hold button gently.Step 2: Pull out
medication card.Blister pack contains
8 tablets (20 mg per tablet).Refer to Prescribing
Information for dosing
instructions.Do not break, chew, crush,
or divide the tablets.Dispense enclosed Medication
Guide to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 80 mg (twice Weekly) Blister Pack Label
XPOVIO®(selinexor tablets)
80 mg
Dose
(entire pack)Push tablets
through foil.Swallow
whole with
water.IMPORTANT: Take each dose as prescribed by your physician.
Take only one 80 mg dose in a single day. Take one 80 mg dose on Day 1 and one 80 mg dose on Day 3 of the week.
Refer to Prescribing Information for dosing instructions.
-
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 100 mg (Once Weekly) Carton Label
NDC 72237-101-05
Rx ONLY
100 mg
Once
Weekly
Blister PacksXPOVIO®
(selinexor) tablets
Contents: 4 individual weekly
blister packs. Each blister pack
contains 5 tablets (20 mg per tablet).20 film-coated tablets
Dispense enclosed Medication Guide
to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 100 mg (Once Weekly) Blister Sleeve Label
NDC 72237-101-15
Rx ONLY
1 PRESS
& HOLD
HERE100 mg
Once
Weekly
Blister Pack1.PRESS 2. PULL
XPOVIO®
(selinexor) tablets
TO OPEN
Step 1: Press and
hold button gently.Step 2: Pull out
medication card.Blister pack contains
5 tablets (20 mg per tablet).Refer to Prescribing
Information for dosing
instructions.Do not break, chew, crush,
or divide the tablets.
Dispense enclosed Medication
Guide to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 100 mg (Once Weekly) Blister Pack Label
XPOVIO®(selinexor tablets)
100 mg
Dose
(entire pack)Push tablets
through foil.Swallow
whole with
water.IMPORTANT: Take each dose as prescribed by your physician.
Take only one 100 mg dose in a single day per week.
Refer to Prescribing Information for dosing instructions.
-
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 40 mg (Twice Weekly) Carton Label
NDC 72237-101-06
Rx ONLY
40 mg
Twice
Weekly
Blister Packs(80 mg total weekly dose)
XPOVIO®
(selinexor) tablets
Contents: 4 individual weekly
blister packs. Each blister pack
contains 4 tablets (20 mg per tablet).16 film-coated tablets
Dispense enclosed Medication Guide
to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 40 mg (Twice Weekly) Blister Sleeve Label
NDC 72237-101-16
Rx ONLY
1 PRESS
& HOLD
HERE40 mg
Twice
Weekly
Blister Pack(80 mg total weekly dose)
1. PRESS 2. PULL
XPOVIO®
(selinexor) tablets
TO OPEN
Step 1: Press and
hold button gently.Step 2: Pull out
medication card.Blister pack contains
4 tablets (20 mg per tablet).Refer to Prescribing
Information for dosing
instructions.Do not break, chew, crush,
or divide the tablets.Dispense enclosed Medication
Guide to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 40 mg (Twice Weekly) Blister Pack Label
XPOVIO®(selinexor tablets)
40 mg
DosePush tablets
through foil.Swallow
whole with
water.IMPORTANT: Take each dose as prescribed by your physician.
Take only one 40 mg dose in a single day. Take one 40 mg dose on Day 1 and one 40 mg dose on Day 3 of the week.
Refer to Prescribing Information for dosing instructions.
-
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 40 mg (Once Weekly) Carton Label
NDC 72237-101-07
Rx ONLY
40 mg
Once
Weekly
Blister PacksXPOVIO®
(selinexor) tablets
Contents: 4 individual weekly
blister packs. Each blister pack
contains 2 tablets (20 mg per tablet).8 film-coated tablets
Dispense enclosed Medication Guide
to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 40 mg (Once Weekly) Blister Sleeve Label
NDC 72237-101-17
Rx ONLY
1 PRESS
& HOLD
HERE40 mg
Once
Weekly
Blister Pack1. PRESS 2. PULL
XPOVIO®
(selinexor) tablets
TO OPEN
Step 1: Press and
hold button gently.Step 2: Pull out
medication card.Blister pack contains
2 tablets (20 mg per tablet).Refer to Prescribing
Information for dosing
instructions.Do not break, chew, crush,
or divide the tablets.Dispense enclosed Medication
Guide to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 40 mg (Once Weekly) Blister Pack Label
XPOVIO®(selinexor tablets)
40 mg
Dose
(entire pack)Push tablets through foil.
Swallow whole with water.
IMPORTANT: Take each dose as prescribed by your physician.
Take only one 40 mg dose in a single day per week.
Refer to Prescribing Information for dosing instructions.
-
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 40 mg (Once Weekly) Carton Label
NDC 72237-102-07
Rx ONLY
40 mg
Once
Weekly
Blister PacksXPOVIO®
(selinexor) tablets
Contents: 4 individual weekly blister packs. Each blister pack contains 1 tablet (40 mg per tablet).
4 film-coated tablets
Dispense enclosed Medication Guide to each patient
Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 40 mg (Once Weekly) Blister Sleeve Label
NDC 72237-102-17
Rx ONLY
1 PRESS
& HOLD
HERE40 mg
Once
Weekly
Blister Pack1. PRESS 2. PULL
XPOVIO®
(selinexor) tablets
TO OPEN
Step 1: Press and
hold button gently.Step 2: Pull out
medication card.Blister pack contains
1 tablet (40 mg per tablet).Refer to Prescribing
Information for dosing
instructions.Do not break, chew, crush,
or divide the tablets.Dispense enclosed Medication
Guide to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 40 mg (Once Weekly) Blister Pack Label
XPOVIO®(selinexor)tablets
40 mg Dose
40
mgIMPORTANT: Take each dose as prescribed by your physician.
Take only one 40 mg dose in a single day per week.
Refer to Prescribing Information for dosing instructions.
Push tablet through foil.
Swallow whole with water.
-
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 40 mg (Twice Weekly) Carton Label
NDC 72237-102-06
Rx ONLY
40 mg
Twice
Weekly
Blister Packs(80 mg total
weekly dose)XPOVIO®
(selinexor) tablets
Contents: 4 individual weekly blister packs. Each blister pack contains 2 tablets (40 mg per tablet).
8 film-coated tablets
Dispense enclosed Medication Guide to each patient
Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 40 mg (Twice Weekly) Blister Sleeve Label
NDC 72237-102-16
Rx ONLY
1 PRESS
& HOLD
HERE40 mg
Twice
Weekly
Blister Pack(80 mg total
weekly dose)1. PRESS 2. PULL
XPOVIO®
(selinexor) tablets
TO OPEN
Step 1: Press and
hold button gently.Step 2: Pull out
medication card.Blister pack contains
2 tablets (40 mg per tablet).Refer to Prescribing
Information for dosing
instructions.Do not break, chew, crush,
or divide the tablets.Dispense enclosed Medication
Guide to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 40 mg (Twice Weekly) Blister Pack Label
XPOVIO®(selinexor) tablets
40
mg40 mg
DoseIMPORTANT: Take each dose as prescribed by your physician.
Take only one 40 mg dose in a single day.
Take one 40 mg dose on Day 1 and one 40 mg dose on Day 3 of the week.
Refer to Prescribing Information for dosing instructions.
Push tablet through foil.
Swallow whole with water.
-
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 60 mg (Once Weekly) Carton Label
NDC 72237-104-01
Rx ONLY
60 mg
Once
Weekly
Blister PacksXPOVIO®
(selinexor) tablets
Contents: 4 individual weekly blister packs. Each blister pack contains 1 tablet (60 mg per tablet).
4 film-coated tablets
Dispense enclosed Medication Guide to each patient
Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 60 mg (Once Weekly) Blister Sleeve Label
NDC 72237-104-11
Rx ONLY
1 PRESS
& HOLD
HERE60 mg
Once
Weekly
Blister Pack1. PRESS 2. PULL
XPOVIO®
(selinexor) tablets
TO OPEN
Step 1: Press and
hold button gently.Step 2: Pull out
medication card.Blister pack contains
1 tablet (60 mg per tablet).Refer to Prescribing
Information for dosing
instructions.Do not break, chew, crush,
or divide the tablets.Dispense enclosed Medication
Guide to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 60 mg (Once Weekly) Blister Pack Label
XPOVIO®(selinexor) tablets
60 mg Dose
60
mgIMPORTANT: Take each dose as prescribed by your physician.
Take only one 60 mg dose in a single day per week.
Refer to Prescribing Information for dosing instructions.
Push tablet through foil.
Swallow whole with water.
-
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 80 mg (Once Weekly) Carton Label
NDC 72237-102-02
Rx ONLY
80 mg
Once
Weekly
Blister PacksXPOVIO®
(selinexor) tablets
Contents: 4 individual weekly blister packs. Each blister pack contains 2 tablets (40 mg per tablet).
8 film-coated tablets
Dispense enclosed Medication Guide to each patient
Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 80 mg (Once Weekly) Blister Sleeve Label
NDC 72237-102-12
Rx ONLY
1 PRESS
& HOLD
HERE80 mg
Once
Weekly
Blister Pack1. PRESS 2. PULL
XPOVIO®
(selinexor) tablets
TO OPEN
Step 1: Press and
hold button gently.Step 2: Pull out
medication card.Blister pack contains
2 tablets (40 mg per tablet).Refer to Prescribing
Information for dosing
instructions.Do not break, chew, crush,
or divide the tablets.Dispense enclosed Medication
Guide to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 80 mg (Once Weekly) Blister Pack Label
XPOVIO®(selinexor) tablets
80 mg Dose
(entire pack)
40
mg40
mgIMPORTANT: Take each dose as prescribed by your physician.
Take only one 80 mg dose in a single day per week.
Refer to Prescribing Information for dosing instructions.
Push tablet through foil.
Swallow whole with water.
-
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 100 mg (Once Weekly) Carton Label
NDC 72237-103-05
Rx ONLY
100 mg
Once
Weekly
Blister PacksXPOVIO®
(selinexor) tablets
Contents: 4 individual weekly blister packs. Each blister pack contains 2 tablets (50 mg per tablet).
8 film-coated tablets
Dispense enclosed Medication Guide to each patient
Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 100 mg (Once Weekly) Blister Sleeve Label
NDC 72237-103-15
Rx ONLY
1 PRESS
& HOLD
HERE100 mg
Once
Weekly
Blister Pack1. PRESS 2. PULL
XPOVIO®
(selinexor) tablets
TO OPEN
Step 1: Press and
hold button gently.Step 2: Pull out
medication card.Blister pack contains
2 tablets (50 mg per tablet).Refer to Prescribing
Information for dosing
instructions.Do not break, chew, crush,
or divide the tablets.Dispense enclosed Medication
Guide to each patient.Karyopharm®
Therapeutics -
PRINCIPAL DISPLAY PANEL
Principal Display Panel – 100 mg (Once Weekly) Blister Pack Label
XPOVIO®(selinexor) tablets
100 mg Dose
(entire pack)
50
mg50
mgIMPORTANT: Take each dose as prescribed by your physician.
Take only one 100 mg dose in a single day per week.
Refer to Prescribing Information for dosing instructions.
Push tablet through foil.
Swallow whole with water.
-
INGREDIENTS AND APPEARANCE
XPOVIO
selinexor tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:72237-101 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength selinexor (UNII: 31TZ62FO8F) (selinexor - UNII:31TZ62FO8F) selinexor 20 mg Inactive Ingredients Ingredient Name Strength Microcrystalline Cellulose 101 (UNII: 7T9FYH5QMK) Microcrystalline Cellulose 102 (UNII: PNR0YF693Y) Croscarmellose Sodium (UNII: M28OL1HH48) Povidone K30 (UNII: U725QWY32X) Sodium Lauryl Sulfate (UNII: 368GB5141J) Silicon Dioxide (UNII: ETJ7Z6XBU4) Magnesium Stearate (UNII: 70097M6I30) TALC (UNII: 7SEV7J4R1U) POLYVINYL ALCOHOL, UNSPECIFIED (UNII: 532B59J990) GLYCERYL MONOSTEARATE (UNII: 230OU9XXE4) POLYSORBATE 80 (UNII: 6OZP39ZG8H) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) POLYETHYLENE GLYCOL 3350 (UNII: G2M7P15E5P) FD&C BLUE NO. 2--ALUMINUM LAKE (UNII: 4AQJ3LG584) FD&C BLUE NO. 1 ALUMINUM LAKE (UNII: J9EQA3S2JM) Product Characteristics Color blue (blue) Score no score Shape ROUND (ROUND) Size 7mm Flavor Imprint Code K20 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:72237-101-07 4 in 1 CARTON 06/22/2020 1 NDC:72237-101-17 2 in 1 BLISTER PACK; Type 0: Not a Combination Product 2 NDC:72237-101-01 4 in 1 CARTON 07/10/2019 2 NDC:72237-101-11 3 in 1 BLISTER PACK; Type 0: Not a Combination Product 3 NDC:72237-101-06 4 in 1 CARTON 06/22/2020 3 NDC:72237-101-16 4 in 1 BLISTER PACK; Type 0: Not a Combination Product 4 NDC:72237-101-02 4 in 1 CARTON 07/10/2019 4 NDC:72237-101-12 4 in 1 BLISTER PACK; Type 0: Not a Combination Product 5 NDC:72237-101-05 4 in 1 CARTON 07/10/2019 5 NDC:72237-101-15 5 in 1 BLISTER PACK; Type 0: Not a Combination Product 6 NDC:72237-101-03 4 in 1 CARTON 06/22/2020 6 NDC:72237-101-13 6 in 1 BLISTER PACK; Type 0: Not a Combination Product 7 NDC:72237-101-04 4 in 1 CARTON 07/10/2019 7 NDC:72237-101-14 8 in 1 BLISTER PACK; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA212306 07/10/2019 XPOVIO
selinexor tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:72237-102 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength selinexor (UNII: 31TZ62FO8F) (selinexor - UNII:31TZ62FO8F) selinexor 40 mg Inactive Ingredients Ingredient Name Strength Microcrystalline Cellulose 101 (UNII: 7T9FYH5QMK) Microcrystalline Cellulose 102 (UNII: PNR0YF693Y) Croscarmellose Sodium (UNII: M28OL1HH48) Povidone K30 (UNII: U725QWY32X) Sodium Lauryl Sulfate (UNII: 368GB5141J) Silicon Dioxide (UNII: ETJ7Z6XBU4) Magnesium Stearate (UNII: 70097M6I30) TALC (UNII: 7SEV7J4R1U) POLYVINYL ALCOHOL, UNSPECIFIED (UNII: 532B59J990) GLYCERYL MONOSTEARATE (UNII: 230OU9XXE4) POLYSORBATE 80 (UNII: 6OZP39ZG8H) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) POLYETHYLENE GLYCOL 3350 (UNII: G2M7P15E5P) FD&C BLUE NO. 2--ALUMINUM LAKE (UNII: 4AQJ3LG584) FD&C BLUE NO. 1 ALUMINUM LAKE (UNII: J9EQA3S2JM) Product Characteristics Color blue (blue) Score no score Shape OVAL (OVAL) Size 12mm Flavor Imprint Code X40 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:72237-102-07 4 in 1 CARTON 05/19/2021 1 NDC:72237-102-17 1 in 1 BLISTER PACK; Type 0: Not a Combination Product 2 NDC:72237-102-06 4 in 1 CARTON 05/19/2021 2 NDC:72237-102-16 2 in 1 BLISTER PACK; Type 0: Not a Combination Product 3 NDC:72237-102-02 4 in 1 CARTON 05/19/2021 3 NDC:72237-102-12 2 in 1 BLISTER PACK; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA212306 05/19/2021 XPOVIO
selinexor tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:72237-103 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength selinexor (UNII: 31TZ62FO8F) (selinexor - UNII:31TZ62FO8F) selinexor 50 mg Inactive Ingredients Ingredient Name Strength Microcrystalline Cellulose 101 (UNII: 7T9FYH5QMK) Microcrystalline Cellulose 102 (UNII: PNR0YF693Y) Croscarmellose Sodium (UNII: M28OL1HH48) Povidone K30 (UNII: U725QWY32X) Sodium Lauryl Sulfate (UNII: 368GB5141J) Silicon Dioxide (UNII: ETJ7Z6XBU4) Magnesium Stearate (UNII: 70097M6I30) TALC (UNII: 7SEV7J4R1U) POLYVINYL ALCOHOL, UNSPECIFIED (UNII: 532B59J990) GLYCERYL MONOSTEARATE (UNII: 230OU9XXE4) POLYSORBATE 80 (UNII: 6OZP39ZG8H) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) POLYETHYLENE GLYCOL 3350 (UNII: G2M7P15E5P) FD&C BLUE NO. 2--ALUMINUM LAKE (UNII: 4AQJ3LG584) FD&C BLUE NO. 1 ALUMINUM LAKE (UNII: J9EQA3S2JM) Product Characteristics Color blue (blue) Score no score Shape OVAL (OVAL) Size 13mm Flavor Imprint Code X50 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:72237-103-05 4 in 1 CARTON 05/19/2021 1 NDC:72237-103-15 2 in 1 BLISTER PACK; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA212306 05/19/2021 XPOVIO
selinexor tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:72237-104 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength selinexor (UNII: 31TZ62FO8F) (selinexor - UNII:31TZ62FO8F) selinexor 60 mg Inactive Ingredients Ingredient Name Strength Microcrystalline Cellulose 101 (UNII: 7T9FYH5QMK) Microcrystalline Cellulose 102 (UNII: PNR0YF693Y) Croscarmellose Sodium (UNII: M28OL1HH48) Povidone K30 (UNII: U725QWY32X) Sodium Lauryl Sulfate (UNII: 368GB5141J) Silicon Dioxide (UNII: ETJ7Z6XBU4) Magnesium Stearate (UNII: 70097M6I30) TALC (UNII: 7SEV7J4R1U) POLYVINYL ALCOHOL, UNSPECIFIED (UNII: 532B59J990) GLYCERYL MONOSTEARATE (UNII: 230OU9XXE4) POLYSORBATE 80 (UNII: 6OZP39ZG8H) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) POLYETHYLENE GLYCOL 3350 (UNII: G2M7P15E5P) FD&C BLUE NO. 2--ALUMINUM LAKE (UNII: 4AQJ3LG584) FD&C BLUE NO. 1 ALUMINUM LAKE (UNII: J9EQA3S2JM) Product Characteristics Color blue (blue) Score no score Shape OVAL (OVAL) Size 14mm Flavor Imprint Code X60 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:72237-104-01 4 in 1 CARTON 05/19/2021 1 NDC:72237-104-11 1 in 1 BLISTER PACK; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA212306 05/19/2021 Labeler - Karyopharm Therapeutics Inc. (061317680)