Label: XADAGO- safinamide mesylate tablet, film coated


-
NDC Code(s):
27505-110-14,
27505-110-30,
27505-110-90,
27505-111-14, view more27505-111-30, 27505-111-90
- Packager: MDD US Operations LLC, a subsidiary of Supernus Pharmaceuticals, Inc.
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: New Drug Application
Drug Label Information
Updated December 20, 2023
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use XADAGO ® safely and effectively. See full prescribing information for XADAGO ®.
XADAGO ®(safinamide) tablets, for oral use.
Initial U.S. Approval: 2017INDICATIONS AND USAGE
XADAGO is a monoamine oxidase type B (MAO-B) inhibitor indicated as adjunctive treatment to levodopa/carbidopa in patients with Parkinson's disease (PD) experiencing "off" episodes ( 1)
DOSAGE AND ADMINISTRATION
- Start with 50 mg administered orally once daily at the same time of day; after two weeks, the dose may be increased to 100 mg once daily, based on individual need and tolerability ( 2.1)
- Hepatic Impairment: Do not exceed 50 mg once daily in patients with moderate hepatic impairment; contraindicated in patients with severe hepatic impairment ( 2.2, 4)
DOSAGE FORMS AND STRENGTHS
Tablets: 50 mg and 100 mg ( 3)
CONTRAINDICATIONS
XADAGO is contraindicated in patients with:
- Concomitant use of the following drugs:
- Other monoamine oxidase inhibitors or other drugs that are potent inhibitors of monoamine oxidase (e.g., linezolid) ( 4, 7.1)
- Opioid drugs (e.g., tramadol, meperidine and related derivatives); serotonin-norepinephrine reuptake inhibitors; tri-or tetra-cyclic or triazolopyridine antidepressants; cyclobenzaprine; methylphenidate, amphetamine, and their derivatives; St. John's wort ( 4, 7.2, 7.3, 7.5)
- Dextromethorphan ( 4, 7.4)
- A history of a hypersensitivity to safinamide ( 4)
- Severe hepatic impairment (Child-Pugh C: 10-15) ( 4)
WARNINGS AND PRECAUTIONS
- May cause or exacerbate hypertension ( 5.1)
- May cause serotonin syndrome when used with MAO inhibitors, antidepressants, or opioid drugs ( 5.2)
- May cause falling asleep during activities of daily living ( 5.3)
- May cause or exacerbate dyskinesia; consider levodopa dose reduction ( 5.4)
- May cause hallucinations and psychotic behavior ( 5.5)
- May cause problems with impulse control/compulsive behaviors ( 5.6)
- May cause withdrawal-emergent hyperpyrexia and confusion ( 5.7)
ADVERSE REACTIONS
Most common adverse reactions (incidence on XADAGO 100 mg/day at least 2% greater than placebo) were dyskinesia, fall, nausea, and insomnia ( 6.1)
To report SUSPECTED ADVERSE REACTIONS, contact MDD US Operations, LLC, at 1-888-492-3246 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 8/2021
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Dosing Information
2.2 Dosing in Patients with Hepatic Impairment
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Hypertension
5.2 Serotonin Syndrome
5.3 Falling Asleep During Activities of Daily Living
5.4 Dyskinesia
5.5 Hallucinations / Psychotic Behavior
5.6 Impulse Control / Compulsive Behaviors
5.7 Withdrawal Emergent Hyperpyrexia and Confusion
5.8 Retinal Pathology
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
7.1 MAO Inhibitors (MAOIs)
7.2 Opioid Drugs
7.3 Serotonergic Drugs
7.4 Dextromethorphan
7.5 Sympathomimetic Medications
7.6 Tyramine
7.7 Dopaminergic Antagonists
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Hepatic Impairment
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
14.1 Adjunctive Treatment in Patients with Parkinson's Disease Experiencing OFF Time on a Stable Dose of Levodopa.
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
16.2 Storage and Handling
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
- 1 INDICATIONS AND USAGE
-
2 DOSAGE AND ADMINISTRATION
2.1 Dosing Information
The recommended starting dosage of XADAGO is 50 mg administered orally once daily (at the same time of day), without regard to meals. After two weeks, the dosage may be increased to 100 mg once daily, based on individual need and tolerability.
Daily dosages of XADAGO above 100 mg have not been shown to provide additional benefit, and higher dosages increase the risk for adverse reactions. XADAGO has been shown to be effective only in combination with levodopa/carbidopa [see Indications and Usage (1)] .
If a dose is missed, the next dose should be taken at the same time the next day.
XADAGO 100 mg should be tapered by decreasing the dose to 50 mg for one week before stopping [see Warnings and Precautions (5.7)] .
2.2 Dosing in Patients with Hepatic Impairment
In patients with moderate hepatic impairment (Child-Pugh B: 7-9), the maximum recommended dosage of XADAGO is 50 mg orally once daily. XADAGO is contraindicated in patients with severe hepatic impairment (Child-Pugh C: 10-15) [see Use in Specific Populations (8.6) and Clinical Pharmacology (12.3)] . If a patient taking 50 mg XADAGO progresses from moderate to severe hepatic impairment, discontinue XADAGO.
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
XADAGO is contraindicated in patients with:
- Concomitant use of other drugs in the monoamine oxidase inhibitor (MAOI) class or other drugs that are potent inhibitors of monoamine oxidase, including linezolid. The combination may result in increased blood pressure, including hypertensive crisis [see Warnings and Precautions (5.1) and Drug Interactions (7.1)] .
- Concomitant use of opioid drugs (e.g., meperidine and its derivatives, methadone, propoxyphene, or tramadol); serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic, tetracyclic, or triazolopyridine antidepressants; cyclobenzaprine; methylphenidate, amphetamine, and their derivatives; or St John's wort. Concomitant use could result in life-threatening serotonin syndrome [see Warnings and Precautions (5.2) and Drug Interactions (7.2, 7.3, 7.5)] .
- Concomitant use of dextromethorphan. The combination of MAOIs and dextromethorphan has been reported to cause episodes of psychosis or abnormal behavior [see Drug Interactions (7.4)] .
- A history of a hypersensitivity to safinamide. Reactions have included swelling of the tongue and oral mucosa, and dyspnea.
- Severe hepatic impairment (Child-Pugh C: 10-15) [see Use in Specific Populations (8.6)] .
-
5 WARNINGS AND PRECAUTIONS
5.1 Hypertension
XADAGO may cause hypertension or exacerbate existing hypertension. In clinical trials, the incidence of hypertension was 7% for XADAGO 50 mg, 5% for XADAGO 100 mg, and 4% for placebo. Monitor patients for new onset hypertension or hypertension that is not adequately controlled after starting XADAGO. Medication adjustment may be necessary if elevation of blood pressure is sustained.
Monitor for hypertension if XADAGO is prescribed concomitantly with sympathomimetic medications, including prescription or nonprescription nasal, oral, and ophthalmic decongestants and cold remedies [see Drug Interactions (7.5)] .
XADAGO is a selective inhibitor of MAO-B at the recommended dosages of 50 mg or 100 mg daily. Selectivity for inhibiting MAO-B decreases above the recommended daily dosages [see Clinical Pharmacology (12.2)] . Therefore, XADAGO should not be used at daily dosages exceeding those recommended because of the risks of hypertension, exacerbation of existing hypertension, or hypertensive crisis.
Dietary tyramine restriction is not required during treatment with recommended doses of XADAGO. However, use with certain foods that contain very high amounts (i.e., more than 150 mg) of tyramine could cause severe hypertension, resulting from an increased sensitivity to tyramine in patients taking recommended dosages of XADAGO, and patients should be advised to avoid such foods.
Isoniazid has some monoamine oxidase inhibiting activity. Monitor for hypertension and reaction to dietary tyramine in patients treated concomitantly with isoniazid and XADAGO [see Drug Interactions (7.1, 7.6)] .
5.2 Serotonin Syndrome
The development of a potentially life-threatening serotonin syndrome has been reported in patients on concomitant treatment with MAOIs (including selective MAO-B inhibitors), serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants, tetracyclic antidepressants, triazolopyridine antidepressants, cyclobenzaprine, opioid drugs (e.g., meperidine and meperidine derivatives, propoxyphene, tramadol), and methylphenidate, amphetamine, and their derivatives. Concomitant use of XADAGO with these drugs is contraindicated.
In clinical trials, serotonin syndrome was reported in a patient treated with XADAGO and a selective serotonin reuptake inhibitor (SSRI). Use the lowest effective dose of SSRIs in patients treated with concomitant XADAGO.
Serotonin syndrome symptoms may include mental status changes (e.g., agitation, hallucinations, delirium, and coma), autonomic instability (e.g., tachycardia, labile blood pressure, dizziness, diaphoresis, flushing, hyperthermia), neuromuscular symptoms (e.g., tremor, rigidity, myoclonus, hyperreflexia, incoordination), seizures, and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea).
5.3 Falling Asleep During Activities of Daily Living
Patients treated with dopaminergic medications have reported falling asleep while engaged in activities of daily living, including the operation of motor vehicles, which sometimes has resulted in accidents. Patients may not perceive warning signs, such as excessive drowsiness, or they may report feeling alert immediately prior to the event.
In clinical studies, sleep attacks/sudden onset of sleep were reported in patients treated with XADAGO 100 mg/day.
If a patient develops daytime sleepiness or episodes of falling asleep during activities that require full attention (e.g., driving a motor vehicle, conversations, eating), XADAGO should ordinarily be discontinued. If a decision is made to continue these patients on XADAGO, advise them to avoid driving and other potentially dangerous activities.
5.4 Dyskinesia
XADAGO may cause dyskinesia or exacerbate pre-existing dyskinesia.
In clinical trials, the incidence of dyskinesia was 21% for XADAGO 50 mg, 18% for XADAGO 100 mg, and 9% for placebo. There was a greater incidence of dyskinesia causing study discontinuation in patients treated with XADAGO 50 mg or 100 mg (1%), compared to placebo (0%) [see Adverse Reactions (6.1)] .
Reducing the patient's daily levodopa dosage or the dosage of another dopaminergic drug may mitigate dyskinesia.
5.5 Hallucinations / Psychotic Behavior
Patients with a major psychotic disorder should ordinarily not be treated with XADAGO because of the risk of exacerbating the psychosis with an increase in central dopaminergic tone. In addition, treatments for psychosis that antagonize the effects of dopaminergic medications may exacerbate the symptoms of PD [see Drug Interactions (7.7)] .
Consider dosage reduction or stopping the medication if a patient develops hallucinations or psychotic-like behaviors while taking XADAGO.
5.6 Impulse Control / Compulsive Behaviors
Patients can experience intense urges to gamble, increased sexual urges, intense urges to spend money, binge eating, and/or other intense urges, and the inability to control these urges while taking one or more of the medications, including XADAGO, that increase central dopaminergic tone. In some cases, these urges were reported to have stopped when the dose was reduced or the medication was discontinued. Because patients may not recognize these behaviors as abnormal, it is important for prescribers to specifically ask patients or their caregivers about the development of new or increased gambling urges, sexual urges, uncontrolled spending or other urges while being treated with XADAGO. Consider dose reduction or stopping the medication if a patient develops such urges while taking XADAGO.
5.7 Withdrawal Emergent Hyperpyrexia and Confusion
A symptom complex resembling neuroleptic malignant syndrome (characterized by elevated temperature, muscular rigidity, altered consciousness, and autonomic instability), with no other obvious etiology, has been reported in association with rapid dose reduction, withdrawal of, or changes in drugs that increase central dopaminergic tone.
5.8 Retinal Pathology
Retinal degeneration and loss of photoreceptor cells were observed in albino and pigmented rats administered safinamide orally in toxicity studies of up to 6 months duration. In albino rats administered safinamide orally for two years, retinal scarring and cataracts were observed at all doses tested [see Nonclinical Toxicology (13.2)] .
Periodically monitor patients for visual changes in patients with a history of retinal/macular degeneration, uveitis, inherited retinal conditions, family history of hereditary retinal disease, albinism, retinitis pigmentosa, or any active retinopathy (e.g., diabetic retinopathy).
-
6 ADVERSE REACTIONS
The following serious adverse reactions are discussed in greater detail in other sections of labeling:
- Hypertension [see Warnings and Precautions (5.1)]
- Serotonin Syndrome [see Warnings and Precautions (5.2)]
- Falling Asleep During Activities of Daily Living [see Warnings and Precautions (5.3)]
- Dyskinesia [see Warnings and Precautions (5.4)]
- Hallucinations / Psychotic Behavior [see Warnings and Precautions (5.5)]
- Impulse Control / Compulsive Behaviors [see Warnings and Precautions (5.6)]
- Withdrawal-Emergent Hyperpyrexia and Confusion [see Warnings and Precautions (5.7)]
- Retinal Pathology [see Warnings and Precautions (5.8)]
6.1 Clinical Trials Experience
Clinical trials are conducted under widely varying conditions; therefore, adverse reactions observed in the clinical trials of a drug cannot be directly compared to the incidence in the clinical trials of another drug and may not reflect the incidence observed in clinical practice.
Common Adverse Reactions in Placebo-Controlled PD Studies
Table 1 shows the incidence of adverse reactions with an incidence of at least 2% on XADAGO 100 mg/day and greater than placebo in controlled studies in PD (Study 1 and Study 2). The most common adverse reactions associated with XADAGO treatment in which the incidence for XADAGO 100 mg/day was at least 2% greater than the incidence for placebo were dyskinesia, fall, nausea, and insomnia.
Adverse Reactions Reported as Reason for Discontinuation from Study
In pooled placebo-controlled studies (Study 1 and Study 2) in patients with PD taking a stable dose of carbidopa/levodopa with or without other PD medications, there was an increase in the incidence of XADAGO-treated patients who discontinued from the study because of adverse reactions. The incidence of patients discontinuing from Study 1 and Study 2 for any adverse reaction was 5% for XADAGO 50 mg/day, 6% for XADAGO 100 mg/day, and 4% for placebo. The most frequently reported adverse reaction causing study discontinuation was dyskinesia (1% of patients treated with XADAGO 50 mg/day or XADAGO 100 mg/day vs. 0% for placebo).
Table 1: Percentage of Patients with Adverse Reactions with an Incidence ≥ 2% in the XADAGO 100 mg/day Group and Greater than Placebo in Studies 1 and 2. XADAGO
50 mg/day
(N = 223)XADAGO
100 mg/day
(N = 498)Placebo
(N = 497)Adverse Reaction % % % Dyskinesia 21 17 9 Fall 4 6 4 Nausea 3 6 4 Insomnia 1 4 2 Orthostatic hypotension 2 2 1 Anxiety 2 2 1 Cough 2 2 1 Dyspepsia 0 2 1 Abnormal Laboratory Changes
In Study 1 and Study 2, the proportion of patients who experienced a shift from normal to above the upper limit of normal for serum alanine aminotransferase (ALT) was 5% for XADAGO 50 mg, 7% for XADAGO 100 mg, and 3% for placebo. No patient treated with XADAGO experienced an increase in ALT that was 3 times the upper limit of normal or higher.
The proportion of patients with a shift from normal to above the upper limit of normal for serum aspartate aminotransferase (AST) was 7% for XADAGO 50 mg, 6% for XADAGO 100 mg, and 3% for placebo. The incidence of patients with an increase in AST to at least 3 times the upper limit of normal was similar for XADAGO and placebo.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of safinamide. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Immune System Disorders: Hypersensitivity: A postmarketing report describes a patient who developed a hypersensitivity reaction consisting of swelling of the tongue and gingiva, dyspnea and skin rash. The symptoms resolved shortly after XADAGO was discontinued, but reappeared following rechallenge a month later.
Nervous System Disorders: Headache
-
7 DRUG INTERACTIONS
7.1 MAO Inhibitors (MAOIs)
XADAGO is contraindicated for use with other drugs in the MAOIs class or other drugs that are potent inhibitors of monoamine oxidase (e.g., linezolid, an oxazolidinone antibacterial, which also has reversible nonselective MAO inhibition activity). Co-administration increases the risk of nonselective MAO inhibition, which may lead to hypertensive crisis [see Contraindications (4) and Warnings and Precautions (5.1)] . At least 14 days should elapse between discontinuation of XADAGO and initiation of treatment with other MAOIs.
Isoniazid has some monoamine oxidase inhibiting activity. Monitor for hypertension and reaction to dietary tyramine in patients treated concomitantly with isoniazid and XADAGO.
7.2 Opioid Drugs
Because serious, sometimes fatal reactions have been precipitated with concomitant use of opioid drugs (e.g., meperidine and its derivatives, methadone, propoxyphene, or tramadol) and MAOIs, including selective MAO-B inhibitors, concomitant use of these drugs is contraindicated [see Warnings and Precautions (5.2)] . At least 14 days should elapse between discontinuation of XADAGO and initiation of treatment with these drugs.
7.3 Serotonergic Drugs
Concomitant use of XADAGO with SNRIs; triazolopyridine, tricyclic or tetracyclic antidepressants; cyclobenzaprine (a skeletal muscle relaxant that is a tricyclic antidepressant derivative); or St. John's wort is contraindicated [see Warnings and Precautions (5.2)] . At least 14 days should elapse between discontinuation of XADAGO and initiation of treatment with these drugs.
Monitor patients for symptoms of serotonin syndrome if SSRIs are used by patients treated with XADAGO [see Warnings and Precautions (5.2)] .
7.4 Dextromethorphan
The combination of MAOIs and dextromethorphan has been reported to cause episodes of psychosis or bizarre behavior. Therefore, in view of XADAGO's MAO inhibitory activity, dextromethorphan is contraindicated for use with XADAGO.
7.5 Sympathomimetic Medications
Severe hypertensive reactions have followed the administration of sympathomimetics and nonselective MAOIs. Hypertensive crisis has been reported in patients taking the recommended doses of selective MAO-B inhibitors and sympathomimetic medications. Concomitant use of XADAGO with methylphenidate, amphetamine, and their derivatives is contraindicated [see Warnings and Precautions (5.1, 5.2)] .
Monitor patients for hypertension if XADAGO is prescribed concomitantly with prescription or nonprescription sympathomimetic medications, including nasal, oral, or ophthalmic decongestants and cold remedies [see Warnings and Precautions (5.1)] .
7.6 Tyramine
MAO in the gastrointestinal tract and liver (primarily type A) provides protection from exogenous amines (e.g., tyramine). If tyramine were absorbed intact, it could lead to severe hypertension, including hypertensive crisis. Aged, fermented, cured, smoked, and pickled foods containing large amounts of exogenous amines (e.g., aged cheese, pickled herring) may cause release of norepinephrine resulting in a rise in blood pressure (Tyramine Reaction). Patients should be advised to avoid foods containing a large amount of tyramine while taking recommended doses of XADAGO [see Warnings and Precautions (5.1)] .
Selectivity for inhibiting MAO-B decreases in a dose-related manner above the highest recommended daily dosage, which may increase the risk for hypertension [see Clinical Pharmacology (12.2)] . In addition, isoniazid has some monoamine oxidase inhibiting activity. Monitor for hypertension and reaction to dietary tyramine in patients treated with isoniazid and XADAGO [see Warnings and Precautions (5.1)] .
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no adequate data on the developmental risk associated with the use of XADAGO in pregnant women. In animals, developmental toxicity, including teratogenic effects, was observed when safinamide was administered during pregnancy at clinically relevant doses. Developmental toxicity was observed at doses lower than those used clinically when safinamide was administered during pregnancy in combination with levodopa/carbidopa.
The background risk of major birth defects and miscarriage for the indicated population is unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Data
Animal Data
In an embryofetal development study in rats, oral administration of safinamide (0, 50, 100, or 150 mg/kg/day) throughout organogenesis resulted in dose-related increases in fetal abnormalities (primarily urogenital malformations) at all doses. A no-effect dose for adverse effects on embryofetal development was not established. The lowest dose tested (50 mg/kg/day) is approximately 5 times the maximum recommended human dose (MRHD) of 100 mg on a body surface area (mg/m 2) basis. In a combination embryofetal development study of safinamide and levodopa (LD)/carbidopa (CD) in rats (80/20 mg/kg/day LD/CD in combination with 0, 25, 50, or 100 mg/kg/day safinamide or 100 mg/kg/day safinamide alone), increased incidences of fetal visceral and skeletal malformations and variations were observed at all doses of safinamide in combination with CD/LD and with safinamide alone. The lowest dose of safinamide tested (25 mg/kg/day) is approximately 2 times the MRHD on a mg/m 2 basis.
In embryofetal development studies in rabbits, no developmental toxicity was observed at up to the highest oral dose of safinamide tested (100 mg/kg/day). However, when safinamide (0, 4, 12, or 40 mg/kg/day) was administered throughout organogenesis in a combination study of safinamide with LD/CD (80/20 mg/kg/day LD/CD), there was an increased incidence of embryofetal death and cardiac and skeletal malformations, compared to LD/CD alone. A no-effect dose for safinamide was not established; the lowest effect dose of safinamide tested (4 mg/kg/day) is less than the MRHD on a mg/m 2 basis.
In a rat pre- and postnatal development study, oral administration of safinamide (0, 4, 12.5, or 37.5 mg/kg/day) throughout pregnancy and lactation resulted in skin discoloration of the offspring, presumed to be due to hepatobiliary toxicity, at the mid and high doses and decreased body weight and increased postnatal mortality in offspring at the highest dose tested. The no-effect dose (4 mg/kg/day) for adverse developmental effects is less than the MRHD on a mg/m 2 basis.
8.2 Lactation
Risk Summary
There is no information regarding the presence of XADAGO or its metabolites in human milk, the effects on the breastfed infant, or the effects on milk production.
The developmental and health benefits of breastfeeding should be considered along with the mothers' clinical need for XADAGO and any potential adverse effects on the breastfed infant from XADAGO or from the underlying maternal condition.
8.5 Geriatric Use
Of the 1516 subjects exposed to XADAGO in clinical studies, 38% were 65 and over, while 4% were 75 and over. No overall differences in safety or effectiveness were observed between these patients and younger patients, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
8.6 Hepatic Impairment
XADAGO plasma concentrations are increased in patients with hepatic impairment [see Clinical Pharmacology (12.3)] .
In patients with moderate hepatic impairment (Child-Pugh B: 7-9), the maximum recommended dosage of XADAGO is 50 mg once daily [see Dosage and Administration (2.2)] . XADAGO has not been studied in patients with severe hepatic impairment (Child-Pugh C: 10-15), and is contraindicated in these patients. If patients progress from moderate to severe hepatic impairment, treatment with XADAGO should be stopped.
-
10 OVERDOSAGE
There is no human experience with XADAGO overdose.
There is no known antidote to XADAGO nor any specific treatment for XADAGO overdose. If an overdose occurs, XADAGO treatment should be discontinued and supportive treatment should be administered as clinically indicated. In cases of overdose with XADAGO, dietary tyramine restriction should be observed for several weeks.
The Poison Control Center should be called at 1-800-222-1222 for the most current treatment guidelines.
-
11 DESCRIPTION
XADAGO tablets contain safinamide, which is a MAO-B inhibitor, as the mesylate salt. Safinamide mesylate is (S)-2- [[4-[(3-fluorophenyl) methoxy]phenyl]methyl]aminopropanamide methanesulfonate (1:1) and its structural formula is below.
The molecular formula of safinamide mesylate is C 17H 19FN 2O 2∙CH 4O 3S and its molecular weight is 398.45.
Safinamide mesylate is a white to off-white crystalline powder. Safinamide mesylate is freely soluble in water, methanol and dimethyl sulfoxide. Safinamide mesylate is sparingly soluble in ethanol and is practically insoluble in ethyl acetate. In aqueous buffers that span a pH range of 1.2 to 7.5, safinamide mesylate is highly soluble at pH 1.2 and 4.5, but shows low solubility (<0.4 mg/mL) at pH 6.8 and 7.5.
XADAGO is available as 50 mg and 100 mg film-coated tablets for oral administration. Each XADAGO tablet contains 65.88 mg or 131.76 mg of safinamide mesylate, equivalent to 50 mg or 100 mg, respectively, of safinamide free base. The tablets also contain the following inactive ingredients: colloidal silicon dioxide, crospovidone, hypromellose, iron oxide (red), magnesium stearate, microcrystalline cellulose, polyethylene glycol 6000, potassium aluminum silicate, and titanium dioxide.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
The precise mechanism by which XADAGO exerts its therapeutic effects in PD is unknown. XADAGO is an inhibitor of monoamine oxidase B (MAO-B). Inhibition of MAO-B activity, by blocking the catabolism of dopamine, is thought to result in an increase in dopamine levels and a subsequent increase in dopaminergic activity in the brain.
12.2 Pharmacodynamics
XADAGO inhibits monoamine oxidase B (MAO-B), with more than 1000-fold selectivity over MAO-A. In clinical studies, complete inhibition (>90%) of MAO-B was measured at doses > 20 mg.
Tyramine Challenge Test
In an oral tyramine challenge study, XADAGO produced a distinct but relatively small increase in tyramine sensitivity to increase blood pressure. The results suggest that XADAGO at a dose of 50 mg or 100 mg is relatively selective for inhibiting MAO-B and can be used without dietary tyramine restriction. Relative selectivity of XADAGO for inhibiting MAO-B decreases above the highest recommended daily dosage (100 mg) [see Warnings and Precautions (5.1) and Drug Interactions (7.6)] .
Cardiac Electrophysiology
The effect of XADAGO on the QTc interval was evaluated in a randomized placebo and positive controlled double-blind, multiple-dose parallel thorough QTc study in 240 healthy subjects. At a dose of 350 mg (3.5 times the maximum recommended dosage), XADAGO did not prolong the QTc interval.
12.3 Pharmacokinetics
Pharmacokinetics of safinamide is linear over a range of 50 mg to 300 mg (3 times the maximum recommended daily dose). Steady state is reached within 5 to 6 days.
Absorption
After single and multiple oral dosing under fasting conditions, T max of safinamide ranges from 2 to 3 hours. Absolute bioavailability of safinamide is 95% after oral administration, and first pass metabolism is negligible. A slight delay in T max was observed in the fed state relative to the fasted condition, but there was no effect on safinamide AUC 0−∞ and C max [see Dosage and Administration (2.1)] .
Distribution
The volume of distribution (Vss) is approximately 165 L, indicating extensive extravascular distribution. Safinamide is not highly protein bound (unbound fraction is 11 to 12%).
Metabolism and Excretion
In humans, safinamide is almost exclusively eliminated via metabolism (~5% of the drug is eliminated unchanged, mainly in urine), through three main metabolic pathways. One pathway involves hydrolytic oxidation of the amide moiety leading to the primary metabolite 'safinamide acid' (NW-1153). Another pathway is oxidative cleavage of the ether bond forming 'O- debenzylated safinamide' (NW-1199). Finally, the 'N-dealkylated acid' (NW-1689) is formed by oxidative cleavage of the amine bond of either safinamide or the primary safinamide acid metabolite (NW-1153). The 'N-dealkylated acid' (NW-1689) undergoes further conjugation with glucuronic acid yielding its acyl glucuronide. NW-1689 is the main circulating metabolite in human plasma, exceeding the exposure of the parent (161% of parent). NW-1689 AG and NW-1153 account for about 18% and 11% of the parent drug exposure, respectively. None of the metabolites has pharmacological activity.
Safinamide is predominantly metabolized by non-microsomal enzymes (cytosolic amidases/MAO-A); CYP3A4 and other CYP iso-enzymes play only a minor role in its overall biotransformation.
The total clearance of safinamide was determined to be 4.6 L/h. Terminal half-life is 20-26 h. The primary route of excretion is through the kidney (76% of safinamide dose recovered in the urine, primarily in the form of inactive metabolites).
Specific Populations
Age: Geriatric Population: There are limited clinical data on the use of XADAGO in the elderly (>75 years). These data suggest that the pharmacokinetics of safinamide is not affected by age [see Use in Specific Populations (8.5)] .
Hepatic Impairment: The disposition of XADAGO was assessed in subjects with mild and moderate hepatic impairment and compared with subjects with normal hepatic function. A marginal increase in the exposure of safinamide (approximately 30% increase in AUC) was observed in subjects with mild hepatic impairment (Child-Pugh A). In subjects with moderate hepatic impairment (Child-Pugh B), exposure to safinamide was increased by about 80% (CI: 154-215%) [see Dosage and Administration (2.2) and Use in Specific Populations (8.6)] . XADAGO has not been studied in patients with severe hepatic impairment (Child-Pugh C) [see Contraindications (4)] .
Renal Impairment: The effect of renal impairment on safinamide pharmacokinetics was investigated in an open-label, parallel-group, single oral dose study in subjects with moderate renal impairment, severe renal impairment, or normal renal function. The pharmacokinetics of safinamide was not affected by impaired renal function.
Drug Interaction Studies
In Vitro Studies: In vitro metabolism studies indicate no meaningful inhibition or induction of Cytochrome P450 (CYP) based enzymes by safinamide and its major metabolites at concentrations that are relevant for dosing. Safinamide or its major metabolites at clinically relevant concentrations are not inhibitors of MAO-A, levodopa decarboxylase or aldehyde dehydrogenase enzymes.
Safinamide is not a substrate of P-gp. Safinamide and its metabolites did not inhibit P-gp or other transporters OCT2, OATP1B1, OATP1B3, BSEP, OAT1/3/4.
In Vivo Studies: Dedicated drug-drug interactions studies conducted with ketoconazole, levodopa (LD), BCRP substrate (rosuvastatin), and CYP1A2 and CYP3A4 substrates (caffeine and midazolam, respectively) did not demonstrate any clinically significant effects on the pharmacokinetic profile of XADAGO, or on the pharmacokinetic profile of co-administered levodopa, rosuvastatin, or CYP1A2 and CYP3A4 substrates.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
In carcinogenicity studies in mice and rats, safinamide was administered at oral doses of 0, 50, 100 and 200 mg/kg/day, and 0, 25, 50 and 100 mg/kg/day, respectively, for 2 years. The highest doses tested in both species were approximately 10 times the maximum recommended human dose (MRHD) of 100 mg/day on a body surface area (mg/m 2) basis. No evidence of tumorigenic potential was observed in either species.
Mutagenesis
Safinamide was negative for genotoxicity in in vitro (Ames, mouse lymphoma) and in vivo (mouse micronucleus) assays.
Impairment of Fertility
In a rat fertility study in which males and females were orally administered safinamide (0, 50, 100, 150 mg/kg/day) prior to and during mating and continuing through early pregnancy in females, adverse effects on reproductive function were observed in both males (sperm abnormalities) and females (decreased corpora lutea, increased pre-implantation loss). The no-effect dose for reproductive toxicity (50 mg/kg/day) is approximately 5 times the MRHD on a mg/m 2 basis.
13.2 Animal Toxicology and/or Pharmacology
Retinal Pathology in Rats
Degeneration and loss of photoreceptor cells were observed in the retina of both albino and pigmented rats at plasma exposures lower than that in humans at the maximum recommended human dose of 100 mg/kg/day. The findings were dose- and time-dependent and progressed from minimal loss to severe outer nuclear cell layer loss after one year of oral dosing with safinamide. In a two year study, total retinal atrophy and scarring and lens opacities (cataracts) were seen at all oral doses tested (0, 25, 50, and 100 mg/kg/day).
In a study in rats dosed orally with safinamide alone or in combination with pramipexole, pramipexole, at a dose (25 mg/kg/day) that did not cause retinal changes, exacerbated the retinal pathology caused by safinamide alone (50 mg/kg/day) in both pigmented and albino rats.
Investigative studies were not able to identify a mechanism underlying the retinal toxicity; the relevance to humans is unknown.
-
14 CLINICAL STUDIES
14.1 Adjunctive Treatment in Patients with Parkinson's Disease Experiencing OFF Time on a Stable Dose of Levodopa.
Two double-blind, placebo-controlled, multi-national, 24-week studies (Study 1 and Study 2) were conducted in PD patients experiencing "OFF" Time during treatment with carbidopa/levodopa and other PD medications, e.g., dopamine agonists, catechol-O-methyl transferase (COMT) inhibitors, anticholinergics, and/or amantadine. In both studies, the primary measure of effectiveness was the change from baseline in total daily "ON" Time without troublesome dyskinesia (i.e., "ON" Time without dyskinesia plus "ON" Time with non-troublesome dyskinesia), based on 18-hour diaries completed by patients for at least 3 days before each of the scheduled visits. Secondary endpoints included "OFF" Time during the diary period and reduction in Unified PD Rating Scale (UPDRS) Part III (motor examination).
In Study 1, patients (n=645) were randomized equally to treatment with XADAGO 50 mg/day (n=217 patients), XADAGO 100 mg/day (n=216 patients), or placebo (n=212 patients), and had at least one post-baseline assessment of "ON" Time.
The percentages of patients taking stable doses of other classes of PD medications, in addition to levodopa/decarboxylase inhibitor, were: dopamine agonists (61%), COMT inhibitors (24%), anticholinergics (37%), and amantadine (14%). Use of MAOIs was prohibited. The average daily dosage of levodopa was 630 mg. The mean duration of PD was approximately 8 years.
In Study 1, XADAGO 50 mg/day and 100 mg/day significantly increased "ON" Time compared to placebo (Table 2). The increase in "ON" Time without troublesome dyskinesia was accompanied by a similar significant reduction in "OFF" Time and a reduction in Unified PD Rating Scale Part III (UPDRS III) scores assessed during "ON" Time (Table 3). Improvement in "ON" Time occurred without an increase in troublesome dyskinesia.
Table 2: Change in Mean Total Daily "ON" Time * in Study 1 N Baseline (hours)
(mean ± SD)Change from Baseline to Endpoint
(LSD † vs. placebo)
(95% CI) ‡
p-valuePlacebo 212 9.3 ± 2.2 -- XADAGO 50 mg once daily 217 9.4 ± 2.2 0.50 (0.03, 0.96)
p=0.0356XADAGO 100 mg once daily 216 9.6 ± 2.5 0.53 (0.07, 1.00)
p=0.0238Table 3: Secondary Measures of Effectiveness in Study 1 N Baseline (hours) (mean ± SD) Change from Baseline to Endpoint (LSD * vs. placebo) (95% CI) †p-value Change in mean daily "OFF" time Placebo 212 5.3 ± 2.1 -- XADAGO 50 mg once daily 217 5.2 ± 2.0 -0.55 (-0.93, -0.17) p=0.0049 XADAGO 100 mg once daily 216 5.2 ± 2.2 -0.57 (-0.95, -0.19) p=0.0037 Change in UPDRS Part III (Motor subscale) Placebo 212 28.6 ± 12.0 -- XADAGO 50 mg once daily 217 27.3 ± 12.8 -1.75 (-3.24, -0.36) p=0.0212 XADAGO 100 mg once daily 216 28.4 ± 13.5 -2.48 (-3.97, -1.00) p=0.0011 The effect of XADAGO 100 mg on "ON" Time was only slightly numerically greater than the effect of XADAGO 50 mg. In addition, the time course of improvement in total daily "ON" Time was similar between both doses (Figure 1). The time course of improvement in total daily "ON" Time showed numerically greater improvement with both XADAGO 50 mg and 100 mg compared to placebo, at all post-baseline timepoints (Figure 1).
Figure 1: Mean Change from Baseline in Total Daily "ON" Time by Week and Treatment in Study 1
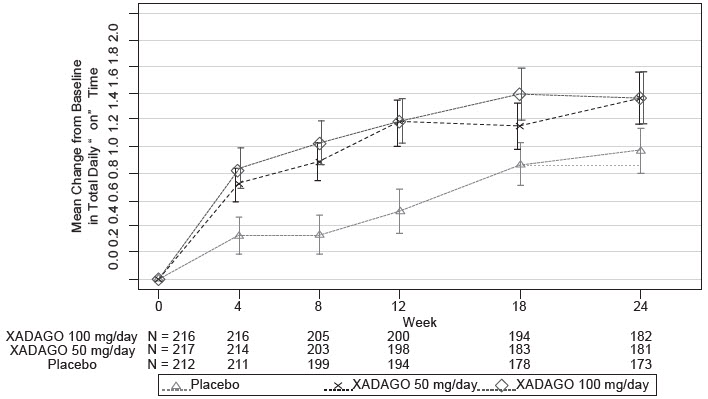
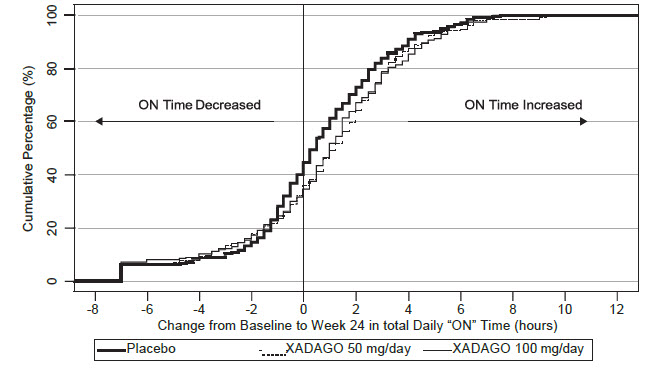
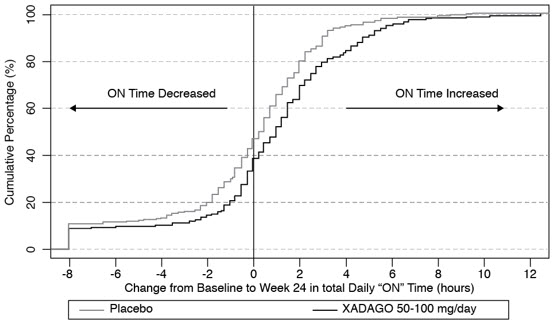
Figure 2 shows the empirical cumulative distribution functions (CDF) for the change from baseline to Week 24 in total daily "ON" Time in Study 1. The cumulative percentage of patients with a change in "ON" Time was similar for the XADAGO 50 mg and 100 mg groups. The cumulative percentage of patients with an increase in "ON" Time is higher for both XADAGO 50 mg and 100 mg treated patients than for placebo patients.
Figure 2: Study 1 Empirical Cumulative Distribution Functions (CDF) for the Change from Baseline to Week 24 in Total Daily "ON" Time
Patients who dropped out of the study because of an adverse reaction, lack of efficacy, non-compliance, or withdrawal of consent were treated as treatment failures and assumed to have the smallest change from baseline among all patients. The failure rates are 6.1%, 5.6%, and 6.9% for the placebo group, XADAGO 50 mg/day group, and XADAGO 100 mg/day group, respectively.
In Study 2, patients (n=549) were randomized to treatment with XADAGO 100 mg daily (n=274 patients) or placebo (n=275 patients) for up to 24 weeks. The percentages of patients taking stable doses of other classes of PD medication, in addition to levodopa/decarboxylase inhibitor, were: dopamine agonists (74%), COMT inhibitors (18%), anticholinergics (17%), and amantadine (30%). Use of MAOIs was prohibited. The average daily dosage of levodopa was 777 mg. The mean duration of PD was approximately 9 years.
In Study 2, XADAGO was significantly better than placebo for increasing "ON"Time (Table 4). The observed increase in "ON" Time without troublesome dyskinesia was accompanied by a reduction in "OFF" Time of similar magnitude and a reduction in UPDRS III score (assessed during "ON" Time). The time course of effect was similar to that showed in the above figure for Study 1. As in Study 1, the increase in "ON" Time without troublesome dyskinesia was accompanied by a similar significant reduction in "OFF" Time and a reduction in Unified PD Rating Scale Part III (UPDRS III) scores assessed during "ON" Time (Table 5).
Table 4: Change in Mean Total Daily "ON" Time * in Study 2 N Baseline (hours)
(mean ± SD)Change from Baseline to Endpoint
(LSD † vs. placebo) (95% CI) ‡p-value Placebo 273 9.1 ± 2.5 -- -- XADAGO
100 mg once daily270 9.3 ± 2.4 0.99 (0.58, 1.39) < 0.001 Table 5: Secondary Measures of Effectiveness in Study 2 N Baseline (hours)
(mean ± SD)Change from Baseline to Endpoint (LSD * vs. placebo) (95% CI) †p-value Change in mean daily "OFF" time Placebo 273 5.36 ± 2.00 -- XADAGO 100 mg once daily 270 5.35 ± 1.98 -1.06 (-1.43, -0.69)
<0.001Change in UPDRS Part III (Motor subscale) Placebo 273 23.03 ± 12.75 -- XADAGO 100 mg once daily 270 22.33 ± 11.79 -1.70 (-2.89, -0.50)
0.005The time course of improvement in total daily "ON" Time showed numerically greater improvement with XADAGO 100 mg compared to placebo at all post-baseline timepoints (Figure 3).
Figure 3: Mean Change from Baseline in Total Daily "ON" Time by Week and Treatment in Study 2
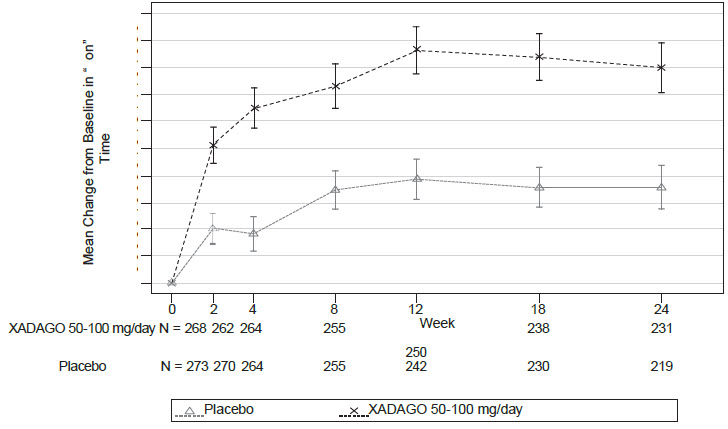
Figure 4 shows the empirical cumulative distribution functions (CDF) for the change from baseline to Week 24 in total daily "ON" Time in Study 2. The cumulative percentage of patients with an increase in "ON" Time treated with XADAGO 50 mg to 100 mg is higher than for placebo patients.
Figure 4: Study 2 Empirical Cumulative Distribution Functions (CDF) for the Change from Baseline to Week 24 in Total Daily "ON" Time
-
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
50 mg (orange to copper colored with metallic gloss, round film-coated, biconcave shaped tablet embossed with "50" on one side; approximately 7 mm in diameter).
Bottles of 30 tablets NDC 27505-110-30 Bottles of 90 tablets NDC 27505-110-90 100 mg (orange to copper colored with metallic gloss, round film-coated, biconcave shaped tablet embossed with "100" on one side; approximately 9 mm in diameter).
Bottles of 30 tablets NDC 27505-111-30 Bottles of 90 tablets NDC 27505-111-90 -
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Hypertension
Advise patients that treatment with recommended doses of XADAGO may be associated with elevations of blood pressure or onset of hypertension. Tell patients who experience elevation of blood pressure while taking XADAGO to contact their healthcare provider.
Explain the risk of using higher than recommended daily doses of XADAGO, and provide a brief description of the tyramine associated hypertensive reaction.
Advise patients to avoid certain foods (e.g., aged cheese) containing a very large amount of tyramine while taking recommended doses of XADAGO because of the potential for large increases in blood pressure. If patients eat foods very rich in tyramine and do not feel well soon after eating, they should contact their healthcare provider [see Warnings and Precautions (5.1)] .
Serotonin Syndrome
Tell patients to inform their physician if they are taking, or plan to take, any prescription or over-the-counter drugs, especially antidepressants and over-the-counter cold medications, because there is a potential for interaction with XADAGO. Because patients should not use meperidine or certain other analgesics with XADAGO, they should contact their healthcare provider before taking new medications including antidepressants, analgesics, and prescription or nonprescription decongestants [see Contraindications (4) and Warnings and Precautions (5.2)] .
Falling Asleep During Activities of Daily Living and Somnolence
Inform patients about the potential for sedating effects associated with XADAGO and other dopaminergic medications, including somnolence and particularly to the possibility of falling asleep while engaged in activities of daily living. Because somnolence can be a frequent adverse reaction with potentially serious consequences, patients should not operate a motor vehicle or engage in other potentially dangerous activities until they have gained sufficient experience with XADAGO.
Advise patients that if increased somnolence or new episodes of falling asleep during activities of daily living (e.g., watching television, passenger in a car, etc.) are experienced at any time during treatment, they should not drive or participate in potentially dangerous activities until they have contacted their physician. Patients should not drive, operate machinery, or work at heights during treatment if they have previously experienced somnolence and/or have fallen asleep without warning prior to use of XADAGO.
Because of possible additive effects, advise patients about the potential for increased somnolence when patients are taking other sedating medications, alcohol, or other central nervous system depressants (e.g., benzodiazepines, antipsychotics, antidepressants) in combination with XADAGO [see Warnings and Precautions (5.3)] .
Dyskinesia
Advise patients taking XADAGO as adjunct to levodopa that there is a possibility of dyskinesia or increased dyskinesia [see Warnings and Precautions (5.4)] .
Hallucinations / Psychotic Behavior
Inform patients that hallucinations or other manifestations of psychotic behavior can occur when taking XADAGO. Advise patients that, if they have a major psychotic disorder, that XADAGO should not ordinarily be used because of the risk of exacerbating the psychosis. Patients with a major psychotic disorder should also be aware that many treatments for psychosis may decrease the effectiveness of XADAGO [see Warnings and Precautions (5.5) and Drug Interactions (7.7)] .
Impulse Control/Compulsive Behaviors
Advise patients that they may experience intense urges to gamble, increased sexual urges, other intense urges, and the inability to control these urges while taking XADAGO. Although it is not proven that the medications caused these events, these urges were reported to have stopped in some cases when the dose was reduced or the medication was stopped. Prescribers should ask patients about the development of new or increased gambling urges, sexual urges, or other urges while being treated with XADAGO. Patients should inform their physician if they experience these urges while taking XADAGO [see Warnings and Precautions 5.6] .
Withdrawal-Emergent Hyperpyrexia and Confusion
Tell patients to contact their healthcare provider if they wish to discontinue XADAGO and seek guidance for tapering XADAGO instead of abruptly discontinuing XADAGO [see Warnings and Precautions (5.7)] .
Missing Dose
Instruct patients to take XADAGO as prescribed. If a dose is missed, instruct patients to take the next dose at the usual time on the following day.
Concomitant Medications
Advise patients to inform their physicians if they are taking, or plan to take, any prescription or over-the-counter medications because of a potential for interactions [see Contraindications (4), and Drug Interactions (7.3, 7.4, and 7.5)] .
-
SPL UNCLASSIFIED SECTION
Distributed by:
MDD US Operations, LLC
9715 Key West Ave
Rockville, MD 20850Under License from Newron Pharmaceuticals SpA.
MDD US Operations, LLC is the exclusive licensee and distributor of XADAGO in the United States and Its territories.
©20xx. Zambon SpA. XADAGO is a registered trademark of Zambon SpA.
298558
A_HQ_2019000185-1
-
PATIENT PACKAGE INSERT
This Patient Information has been approved by the U.S. Food and Drug Administration Revised: 8/2021 PATIENT INFORMATION
XADAGO ® (ZA-da-go)
(safinamide) TabletsWhat is XADAGO? XADAGO is a type of prescription medicine known as a monoamine oxidase type B (MAO-B) inhibitor used with levodopa and carbidopa to treat adults with Parkinson's disease (PD) who are having "off" episodes. It is not known if XADAGO is safe and effective in children. Do not take XADAGO if you: - take another medicine called a Monoamine Oxidase Inhibitor (MAOI) because it may cause a sudden severe increase in your blood pressure (hypertensive crisis).
- Do not take an MAOI within 14 days after you stop taking XADAGO.
- Do not start XADAGO if you stopped taking an MAOI in the last 14 days.
- take an opioid drug, St. John's wort, serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants, tetracyclic antidepressants, triazolopyridine antidepressants, cyclobenzaprine, methylphenidate (or similar drugs), or amphetamine (or similar drugs) because it could be life-threatening. Ask your healthcare provider if you are not sure if you are taking any of these medicines.
- Do not take XADAGO within 14 days after you stop taking any of these medicines.
- Do not start taking XADAGO if you stopped taking any of these medicines in the last 14 days.
- take a medicine used to treat a cough or cold called dextromethorphan because it may cause psychosis or abnormal behavior.
- have a history of an allergic reaction to safinamide. Signs of an allergic reaction to safinamide could include swelling of your tongue, mouth or trouble breathing. Ask your healthcare provider if you are not sure if you have had an allergic reaction to safinamide in the past.
- have severe liver problems.
Before taking XADAGO, tell your healthcare provider about all of your medical conditions, including if you: - have high or low blood pressure
- have a sleep disorder, have unexpected or unpredictable daytime sleepiness or take a medicine to help you sleep
- drink alcoholic beverages. This may increase your chances of becoming drowsy or sleepy while taking XADAGO
- have a history of abnormal movement (dyskinesia)
- have or have had a mental health problem such as schizophrenia, bipolar disorder or psychosis
- have or have had unusual urges
- have or have had problems with the retina in your eye or have a family history of problems with the retina
- are pregnant or plan to become pregnant. It is not known if XADAGO will harm your unborn baby.
- are breastfeeding or plan to breastfeed. It is not known if XADAGO passes into breast milk or if it can cause side effects in a breastfed baby. Talk to your healthcare provider about the best way to feed your baby if you take XADAGO.
Tell your healthcare provider about all the medicines that you take or plan to take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. XADAGO and other medicines may affect each other causing side effects. XADAGO may affect the way other medicines work, and other medicines may affect how XADAGO works. Especially tell your healthcare provider if you take: - selective serotonin reuptake inhibitors (SSRIs)
- meperidine, methadone, propoxyphene, tramadol
- metoclopramide
Ask your healthcare provider if you are not sure if you are taking any of these medicines. Know the medicines you take. Keep a list of them to show your healthcare provider and pharmacist when you get a new medicine. How should I take XADAGO? - Take XADAGO exactly as your healthcare provider tells you to take it.
- Take XADAGO at the same time each day.
- Take XADAGO with or without food.
- If you miss a dose, take your next dose of XADAGO at the same time the next day.
- Your healthcare provider may need to change the dose of XADAGO until the dose is right for you.
- Do not start or stop taking XADAGO without talking to your healthcare provider first.
- If you take too much XADAGO, call the Poison Control Center at 1-800-222-1222 or go to the nearest hospital emergency room right away.
What should I avoid while taking XADAGO? - Avoid certain foods and beverages that are high in tyramine such as aged, fermented, cured, smoked and pickled foods.
- Do not drive, operate heavy machinery, work in high places or do other dangerous activities until you know how XADAGO affects you.
What are the possible side effects of XADAGO? XADAGO may cause serious side effects, including: - high blood pressure (hypertension). XADAGO may raise your blood pressure or make your high blood pressure worse. Your healthcare provider will check your blood pressure while you take XADAGO.
- serotonin syndrome. A potentially life-threatening problem called serotonin syndrome can happen when medicines such as XADAGO are taken with certain other medicines. Symptoms of serotonin syndrome may include:
- agitation, hallucinations, coma, or other changes in mental status
- high or low blood pressure
- seizures
- problems controlling your movements or muscle twitching
- sweating or fever
- nausea or vomiting
- fast heartbeat
- muscle stiffness or tightness
- diarrhea
-
falling asleep during normal activities. You may fall asleep while doing normal activities such as driving a car, doing physical tasks, or using hazardous machinery while taking XADAGO. You may suddenly fall asleep without being drowsy or without warning. This may result in having accidents. Your chances of falling asleep while doing normal activities while taking XADAGO are greater if you take other medicines that cause drowsiness. Tell your healthcare provider right away if this happens. Before starting XADAGO, be sure to tell your healthcare provider if you take any medicines that make you drowsy.
- Do not drive or operate machinery until you know how XADAGO affects you.
- uncontrolled, sudden movements (dyskinesia). XADAGO may cause uncontrolled sudden movements or make such movements you already have worse or more frequent. Tell your healthcare provider if this happens. The doses of your anti-Parkinson's medicine may need to be changed.
- hallucinations and other psychosis. XADAGO can cause or worsen psychotic symptoms including hallucinations (seeing or hearing things that are not real), confusion, agitation, delusional beliefs (believing things that are not real), and disorganized thinking. If you have hallucinations or any of these other psychotic-like changes, talk with your healthcare provider.
- unusual urges. Some patients taking XADAGO get urges to behave in a way unusual for them. Examples of this are unusual urge to gamble, increased sexual urges, strong urges to spend money, binge eating and the inability to control these urges. If you notice or your family notices that you are developing any unusual behaviors, talk to your healthcare provider.
- problems with the retina in your eye (retinal changes). Tell your healthcare provider if your eyesight changes.
The most common side effects of XADAGO include uncontrolled, sudden movements (dyskinesia), falls, nausea, trouble sleeping or falling asleep (insomnia). These are not all the possible side effects of XADAGO. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. How should I store XADAGO? Store XADAGO at room temperature, about 68°F to 77°F (20°C to 25°C). Keep XADAGO and all medicines out of the reach of children. General information about the safe and effective use of XADAGO. Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use XADAGO for a condition for which it was not prescribed. Do not give XADAGO to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about XADAGO that is written for health professionals. What are the ingredients in XADAGO? Active ingredient: safinamide mesylate Inactive ingredients: microcrystalline cellulose, crospovidone, colloidal silicon dioxide, magnesium stearate, hypromellose, polyethylene glycol 6000, iron oxide (red), potassium aluminum silicate, and titanium dioxide Distributed by:
MDD US Operations, LLC
9715 Key West Avenue
Rockville MD 20852
Under License from Newron Pharmaceuticals SpA.
MDD US Operations, LLC is the exclusive licensee and distributor of XADAGO in the United States and Its territories.
©2019. Zambon SpA. XADAGO is a registered trademark of Zambon SpA.
For more information, call 1-888-492-3246. - take another medicine called a Monoamine Oxidase Inhibitor (MAOI) because it may cause a sudden severe increase in your blood pressure (hypertensive crisis).
- PRINCIPAL DISPLAY PANEL - 50 mg Tablet Bottle Carton
- PRINCIPAL DISPLAY PANEL - 100 mg Tablet Bottle Carton
-
INGREDIENTS AND APPEARANCE
XADAGO
safinamide mesylate tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:27505-110 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SAFINAMIDE MESYLATE (UNII: YS90V3DTX0) (SAFINAMIDE - UNII:90ENL74SIG) SAFINAMIDE 50 mg Inactive Ingredients Ingredient Name Strength CROSPOVIDONE (120 .MU.M) (UNII: 68401960MK) MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) MAGNESIUM STEARATE (UNII: 70097M6I30) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) HYPROMELLOSE, UNSPECIFIED (UNII: 3NXW29V3WO) POLYETHYLENE GLYCOL 6000 (UNII: 30IQX730WE) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FERRIC OXIDE RED (UNII: 1K09F3G675) MICA (UNII: V8A1AW0880) Product Characteristics Color orange Score no score Shape ROUND Size 7mm Flavor Imprint Code 50 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:27505-110-30 1 in 1 CARTON 05/08/2017 1 30 in 1 BOTTLE; Type 0: Not a Combination Product 2 NDC:27505-110-90 1 in 1 CARTON 05/08/2017 2 90 in 1 BOTTLE; Type 0: Not a Combination Product 3 NDC:27505-110-14 1 in 1 CARTON 05/08/2017 3 14 in 1 BLISTER PACK; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA207145 05/08/2017 XADAGO
safinamide mesylate tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:27505-111 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SAFINAMIDE MESYLATE (UNII: YS90V3DTX0) (SAFINAMIDE - UNII:90ENL74SIG) SAFINAMIDE 100 mg Inactive Ingredients Ingredient Name Strength MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) CROSPOVIDONE (120 .MU.M) (UNII: 68401960MK) MAGNESIUM STEARATE (UNII: 70097M6I30) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) HYPROMELLOSE, UNSPECIFIED (UNII: 3NXW29V3WO) POLYETHYLENE GLYCOL 6000 (UNII: 30IQX730WE) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FERRIC OXIDE RED (UNII: 1K09F3G675) MICA (UNII: V8A1AW0880) Product Characteristics Color orange Score no score Shape ROUND Size 9mm Flavor Imprint Code 100 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:27505-111-30 1 in 1 CARTON 05/08/2017 1 30 in 1 BOTTLE; Type 0: Not a Combination Product 2 NDC:27505-111-90 1 in 1 CARTON 05/08/2017 2 90 in 1 BOTTLE; Type 0: Not a Combination Product 3 NDC:27505-111-14 1 in 1 CARTON 05/08/2017 3 14 in 1 BLISTER PACK; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA207145 05/08/2017 Labeler - MDD US Operations LLC, a subsidiary of Supernus Pharmaceuticals, Inc. (087875626) Establishment Name Address ID/FEI Business Operations Catalent Germany Schorndorf GmbH 315732628 manufacture(27505-110, 27505-111) , pack(27505-110, 27505-111) , analysis(27505-110, 27505-111) , label(27505-110, 27505-111) Establishment Name Address ID/FEI Business Operations BioChem Labor fur biologische und chemische Analytik GmbH 318354230 analysis(27505-110, 27505-111) Establishment Name Address ID/FEI Business Operations PHAST Gesellschaft fuer Pharmazeutische Qualitatsstandards mbH 331156161 analysis(27505-110, 27505-111) Establishment Name Address ID/FEI Business Operations Merck KGaA 342249299 analysis(27505-110, 27505-111) , api manufacture(27505-110, 27505-111) Establishment Name Address ID/FEI Business Operations PRC Ticinum Lab s.r.l 437339604 analysis(27505-110, 27505-111) Establishment Name Address ID/FEI Business Operations Solvias AG 480739627 analysis(27505-110, 27505-111)

