DEXAMETHASONE SODIUM PHOSPHATE- dexamethasone sodium phosphate injection, solution
REMEDYREPACK INC.
----------
Dexamethasone Sodium Phosphate Injection USP
DESCRIPTION:
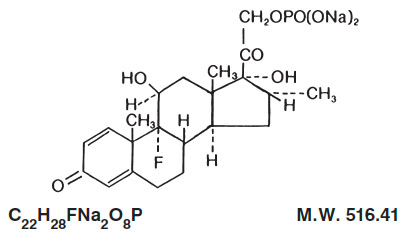
Dexamethasone sodium phosphate is a water-soluble inorganic ester of dexamethasone. It occurs as a white or slightly yellow crystalline powder, is odorless or has a slight odor of alcohol, is exceedingly hygroscopic and is freely soluble in water.
Dexamethasone sodium phosphate is an adrenocortical steroid anti-inflammatory drug.
Chemically, dexamethasone sodium phosphate is 9-Fluoro-11ß,17,21-trihydroxy-16α-methylpregna-1, 4-diene-3,20-dione 21-(dihydrogen phosphate) disodium salt and has the following structural formula:
Dexamethasone Sodium Phosphate Injection, USP is a sterile solution of dexamethasone sodium phosphate in water for injection for intravenous (IV), intramuscular (IM), intra-articular, soft-tissue or intralesional use.
Each mL contains dexamethasone sodium phosphate equivalent to dexamethasone phosphate 4 mg or dexamethasone 3.33 mg; benzyl alcohol 10 mg added as preservative; sodium citrate dihydrate 11 mg; sodium sulfite 1 mg as an antioxidant; Water for Injection q.s. Citric acid and/or sodium hydroxide may have been added for pH adjustment (7.0 to 8.5). Air in the container is displaced by nitrogen.
CLINICAL PHARMACOLOGY:
Dexamethasone sodium phosphate has a rapid onset but short duration of action when compared with less soluble preparations. Because of this, it is suitable for the treatment of acute disorders responsive to adrenocortical steroid therapy.
Naturally occurring glucocorticoids (hydrocortisone and cortisone), which also have salt-retaining properties, are used as replacement therapy in adrenocortical deficiency states. Their synthetic analogs, including dexamethasone, are primarily used for their potent anti-inflammatory effects in disorders of many organ systems.
Glucocorticoids cause profound and varied metabolic effects. In addition, they modify the body’s immune responses to diverse stimuli.
At equipotent anti-inflammatory doses, dexamethasone almost completely lacks the sodium-retaining property of hydrocortisone and closely related derivatives of hydrocortisone.
INDICATIONS AND USAGE:
Intravenous or Intramuscular Injection
When oral therapy is not feasible and the strength, dosage form, and route of administration of the drug reasonably lend the preparation to the treatment of the condition, those products labeled for intravenous or intramuscular use are indicated as follows:
• Endocrine Disorders
Primary or secondary adrenocortical insufficiency(hydrocortisone or cortisone is the drug of choice; synthetic analogs may be used in conjunction with mineralocorticoids where applicable; in infancy, mineralocorticoid supplementation is of particular importance)
Acute adrenocortical insufficiency(hydrocortisone or cortisone is the drug of choice; mineralocorticoid supplementation may be necessary, particularly when syntheticanalogs are used)
Preoperatively, and in the event of serious trauma or illness, in patients with known adrenal insufficiency or when adrenocortical reserve is doubtful
Shock unresponsive to conventional therapy if adrenocortical insufficiency exists or is suspected
Congenital adrenal hyperplasia
Nonsuppurative thyroiditis
Hypercalcemia associated with cancer
• Rheumatic Disorders
As adjunctive therapy for short-term administration(to tide the patient over an acute episode or exacerbation)in:
Post-traumatic osteoarthritis
Synovitis of osteoarthritis
Rheumatoid arthritis, including juvenile rheumatoid arthritis(selected cases may require low-dose maintenance therapy)
Acute and subacute bursitis
Epicondylitis
Acute nonspecific tenosynovitis
Acute gouty arthritis
Psoriatic arthritis
Ankylosing spondylitis
• Collagen Diseases
During an exacerbation or as maintenance therapy in selected cases of:
Systemic lupus erythematosus
Acute rheumatic carditis
Dermatologic Diseases
Pemphigus
Severe erythema multiforme (Stevens-Johnson syndrome)
Exfoliative dermatitis
Bullous dermatitis herpetiformis
Severe seborrheic dermatitis
Severe psoriasis
Mycosis fungoides
• Allergic States
Control of severe or incapacitating allergic conditions intractable to adequate trials of conventional treatment in:
Bronchial asthma
Contact dermatitis
Atopic dermatitis
Serum sickness
Seasonal or perennial allergic rhinitis
Drug hypersensitivity reactions
Urticarial transfusion reactions
Acute noninfectious laryngeal edema (epinephrine is the drug of first choice)
• Ophthalmic Diseases
Severe acute and chronic allergic and inflammatory processes involving the eye, such as:
Herpes zoster ophthalmicus
Iritis, iridocyclitis
Chorioretinitis
Diffuse posterior uveitis and choroiditis
Optic neuritis
Sympathetic ophthalmia
Anterior segment inflammation
Allergic conjunctivitis
Keratitis
Allergic corneal marginal ulcers
• Gastrointestinal Diseases
To tide the patient over a critical period of the disease in:
Ulcerative colitis(Systemic therapy)
Regional enteritis(Systemic therapy)
• Respiratory Diseases
Symptomatic sarcoidosis
Berylliosis
Fulminating or disseminated pulmonary tuberculosis when used concurrently with appropriate antituberculous chemotherapy Loeffler’s syndrome not manageable by other means
Aspiration pneumonitis
• Hematologic Disorders
Acquired(autoimmune hemolytic anemia Idiopathic thrombocytopenic purpura in adults(IV only; IM administration is contraindicated)
Secondary thrombocytopenia in adults
Erythroblastopenia(RBC anemia)
Congenital(erythroid hypoplastic anemia
• Neoplastic Diseases
For palliative management of:
Leukemias and lymphomas in adults
Acute leukemia of childhood
• Edematous States
To induce diuresis or remission of proteinuria in the nephrotic syndrome, without uremia, of the idiopathic type, or that due to lupus erythematosus
• Miscellaneous
Tuberculous meningitis with subarachnoid block or impending block when used concurrently with appropriate antituberculous chemotherapy richinosis with neurologic or myocardial involvement
• Diagnostic testing of adrenocortical hyperfunction
• Cerebral Edema associated with primary or metastatic brain tumor, craniotomy, or head injury.
Use in cerebral edema is not a substitute for careful neurosurgical evaluation and definitive management such as neurosurgery or other specific therapy.
By Intra-articular or Soft Tissue Injection
As adjunctive therapy for short-term administration (to tide the patient over an acute episode or exacerbation) in:
Synovitis of osteoarthritis
Rheumatoid arthritis
Acute and subacute bursitis
Acute gouty arthritis
Epicondylitis
Acute nonspecific tenosynovitis
Post-traumatic osteoarthritis
By Intralesional Injection
Keloids
Localized hypertrophic, infiltrated, inflammatory lesions of: lichen planus, psoriatic plaques, granuloma annulare and lichen simplex chronicus (neurodermatitis)
Discoid lupus erythematosus
Necrobiosis lipoidica diabeticorum
Alopecia areata
May also be useful in cystic tumors of an aponeurosis or tendon (ganglia)
CONTRAINDICATIONS:
Systemic fungal infections (see WARNINGS regarding amphotericin B). Hypersensitivity to any component of this product, including sulfites (see WARNINGS).
WARNINGS:
Because rare instances of anaphylactoid reactions have occurred in patients receiving parenteral corticosteroid therapy, appropriate precautionary measures should be taken prior to administration, especially when the patient has a history of allergy to any drug. Anaphylactoid and hypersensitivity reactions have been reported for dexamethasone sodium phosphate (see ADVERSE REACTIONS).
Dexamethasone sodium phosphate injection contains sodium bisulfite, a sulfite that may cause allergic-type reactions including anaphylactic symptoms and life-threatening or less severe asthmatic episodes in certain susceptible people. The overall prevalence of sulfite sensitivity in the general population is unknown and probably low. Sulfite sensitivity is seen more frequently in asthmatic than in non-asthmatic people.
Corticosteroids may exacerbate systemic fungal infections and therefore, should not be used in the presence of such infections unless they are needed to control drug reactions due to amphotericin B. Moreover, there have been cases reported in which concomitant use of amphotericin B and hydrocortisone was followed by cardiac enlargement and congestive failure.
In patients on corticosteroid therapy subjected to any unusual stress, increased dosage of rapidly acting corticosteroids before, during, and after the stressful situation is indicated.
Drug-induced secondary adrenocortical insufficiency may result from too rapid withdrawal of corticosteroids and may be minimized by gradual reduction of dosage. This type of relative insufficiency may persist for months after discontinuation of therapy; therefore, in any situation of stress occurring during that period, hormone therapy should be reinstituted. If the patient is receiving steroids already, dosage may have to be increased. Since mineralocorticoid secretion may be impaired, salt and/or a mineralocorticoid should be administered concurrently.
Corticosteroids may mask some signs of infection, and new infections may appear during their use. There may be decreased resistance and inability to localize infection when corticosteroids are used. Moreover, corticosteroids may affect the nitroblue-tetrazolium test for bacterial infection and produce false negative results.
In cerebral malaria, a double-blind trial has shown that the use of corticosteroids is associated with prolongation of coma and a higher incidence of pneumonia and gastrointestinal bleeding.
Corticosteroids may activate latent amebiasis. Therefore, it is recommended that latent or active amebiasis be ruled out before initiating corticosteroid therapy in any patient who has spent time in the tropics or any patient with unexplained diarrhea.
Prolonged use of corticosteroids may produce posterior subcapsular cataracts, glaucoma with possible damage to the optic nerves, and may enhance the establishment of secondary ocular infections due to fungi or viruses.
Average and large doses of cortisone or hydrocortisone can cause elevation of blood pressure, salt and water retention, and increased excretion of potassium. These effects are less likely to occur with the synthetic derivatives except when used in large doses. Dietary salt restriction and potassium supplementation may be necessary. All corticosteroids increase calcium excretion.
Administration of live virus vaccines, including smallpox, is contraindicated in individuals receiving immunosuppressive doses of corticosteroids. If inactivated viral or bacterial vaccines are administered to individuals receiving immunosuppressive doses of corticosteroids, the expected serum antibody response may not be obtained. However, immunization procedures may be undertaken in patients who are receiving corticosteroids as replacement therapy, e.g., for Addison’s disease.
Persons who are on drugs which suppress the immune system are more susceptible to infections than healthy individuals. Chickenpox and measles, for example, can have a more serious or even fatal course in non-immune children or adults on corticosteroids. In such children or adults who have not had these diseases, particular care should be taken to avoid exposure. How the dose, route and duration of corticosteroid administration affects the risk of developing a disseminated infection is not known. The contribution of the underlying disease and/or prior corticosteroid treatment to the risk is also not known. If exposed to chickenpox, prophylaxis with varicella zoster immune globulin (VZIG) may be indicated. If exposed to measles, prophylaxis with pooled intramuscular immunoglobulin (IG) may be indicated. (See the respective package inserts for complete VZIG and IG prescribing information). If chickenpox develops, treatment with antiviral agents may be considered.
The use of dexamethasone sodium phosphate in active tuberculosis should be restricted to those cases of fulminating or disseminated tuberculosis in which the corticosteroid is used for the management of the disease in conjunction with an appropriate antituberculous regimen.
If corticosteroids are indicated in patients with latent tuberculosis or tuberculin reactivity, close observation is necessary as reactivation of the disease may occur. During prolonged corticosteroid therapy, these patients should receive chemoprophylaxis.
Literature reports suggest an apparent association between use of corticosteroids and left ventricular free wall rupture after a recent myocardial infarction; therefore, therapy with corticosteroids should be used with great caution in these patients.
Serious Neurologic Adverse Reactions with Epidural Administration
Serious neurologic events, some resulting in death, have been reported with epidural injection of corticosteroids. Specific events reported include, but are not limited to, spinal cord infarction, paraplegia, quadriplegia, cortical blindness, and stroke. These serious neurologic events have been reported with and without use of fluoroscopy. The safety and effectiveness of epidural administration of corticosteroids has not been established, and corticosteroids are not approved for this use.
Pregnancy
Teratogenic Effects: Pregnancy Category C–
Since adequate human reproduction studies have not been done with corticosteroids, use of these drugs in pregnancy or in women of childbearing potential requires that the anticipated benefits be weighed against the possible hazards to the mother and embryo or fetus. Infants born of mothers who have received substantial doses of corticosteroids during pregnancy should be carefully observed for signs of hypoadrenalism.
Corticosteroids appear in breast milk and could suppress growth, interfere with endogenous corticosteroid production, or cause other unwanted effects. Mothers taking pharmacologic doses of corticosteroids should be advised not to nurse.
PRECAUTIONS:
This product, like many other steroid formulations, is sensitive to heat. Therefore, it should not be autoclaved when it is desirable to sterilize the exterior of the vial.
Following prolonged therapy, withdrawal of corticosteroids may result in symptoms of the corticosteroid withdrawal syndrome including fever, myalgia, arthralgia, and malaise. This may occur in patients even without evidence of adrenal insufficiency.
There is an enhanced effect of corticosteroids in patients with hypothyroidism and in those with cirrhosis.
Corticosteroids should be used cautiously in patients with ocular herpes simplex for fear of corneal perforation.
The lowest possible dose of corticosteroid should be used to control the condition under treatment, and when reduction in dosage is possible, the reduction must be gradual.
Psychic derangements may appear when corticosteroids are used, ranging from euphoria, insomnia, mood swings, personality changes, and severe depression to frank psychotic manifestations. Also, existing emotional instability or psychotic tendencies may be aggravated by corticosteroids.
Aspirin should be used cautiously in conjunction with corticosteroids in hypoprothrombinemia.
Steroids should be used with caution in nonspecific ulcerative colitis, if there is a probability of impending perforation, abscess, or other pyogenic infection, also in diverticulitis, fresh intestinal anastomoses, active or latent peptic ulcer, renal insufficiency, hypertension, osteoporosis, and myasthenia gravis. Signs of peritoneal irritation following gastrointestinal perforation in patients receiving large doses of corticosteroids may be minimal or absent. Fat embolism has been reported as a possible complication of hypercortisonism.
When large doses are given, some authorities advise that antacids be administered between meals to help to prevent peptic ulcer.
Growth and development of infants and children on prolonged corticosteroid therapy should be carefully followed.
Steroids may increase or decrease motility and number of spermatozoa in some patients.
Phenytoin, phenobarbital, ephedrine, and rifampin may enhance the metabolic clearance of corticosteroids resulting in decreased blood levels and lessened physiologic activity, thus requiring adjustment in corticosteroid dosage. These interactions may interfere with dexamethasone suppression tests which should be interpreted with caution during administration of these drugs.
False negative results in the dexamethasone suppression test (DST) in patients being treated with indomethacin have been reported. Thus, results of the DST should be interpreted with caution in these patients.
The prothrombin time should be checked frequently in patients who are receiving corticosteroids and coumarin anticoagulants at the same time because of reports that corticosteroids have altered the response to these anticoagulants. Studies have shown that the usual effect produced by adding corticosteroids is inhibition of response to coumarins, although there have been some conflicting reports of potentiation not substantiated by studies.
When corticosteroids are administered concomitantly with potassium-depleting diuretics, patients should be observed closely for development of hypokalemia.
Intra-articular injection of a corticosteroid may produce systemic as well as local effects.
Appropriate examination of any joint fluid present is necessary to exclude a septic process.
A marked increase in pain accompanied by local swelling, further restriction of joint motion, fever, and malaise is suggestive of septic arthritis. If this complication occurs and the diagnosis of sepsis is confirmed, appropriate antimicrobial therapy should be instituted.
Injection of a steroid into an infected site is to be avoided.
Corticosteroids should not be injected into unstable joints.
Patients should be impressed strongly with the importance of not overusing joints in which symptomatic benefit has been obtained as long as the inflammatory process remains active.
Frequent intra-articular injection may result in damage to joint tissues.
The slower rate of absorption by intramuscular administration should be recognized.
ADVERSE REACTIONS:
Fluid and electrolyte disturbances:
Sodium retention
Fluid retention
Congestive heart failure in susceptible patients
Potassium loss
Hypokalemic alkalosis
Hypertension
Musculoskeletal:
Muscle weakness
Steroid myopathy
Loss of muscle mass
Osteoporosis
Pathologic fracture of long bones
Vertebral compression fractures
Aseptic necrosis of femoral and humeral heads
Tendon rupture
Gastrointestinal:
Peptic ulcer with possible subsequent perforation and hemorrhage
Perforation of the small and large bowel, particularly in patients with inflammatory bowel disease
Pancreatitis
Abdominal distention
Ulcerative esophagitis
Dermatologic:
Impaired wound healing
Thin fragile skin
Petechiae and ecchymoses
Erythema
Increased sweating
May suppress reactions to skin tests
Burning or tingling, especially in the perineal area (after IV injection)
Other cutaneous reactions, such as allergic dermatitis, urticaria, angioneurotic edema
Neurologic:
Convulsions
Increased intracranial pressure with papilledema (pseudotumor cerebri) usually after treatment
Vertigo
Headache
Psychic disturbances
Endocrine:
Menstrual irregularities
Development of cushingoid state
Suppression of growth in children
Secondary adrenocortical and pituitary unresponsiveness, particularly in times of stress, as in trauma, surgery, or illness
Decreased carbohydrate tolerance
Manifestations of latent diabetes mellitus
Increased requirements for insulin or oral hypoglycemic agents in diabetics
Hirsutism
Ophthalmic:
Posterior subcapsular cataracts
Increased intraocular pressure
Glaucoma
Exophthalmos
Metabolic:
Negative nitrogen balance due to protein catabolism
Cardiovascular:
Myocardial rupture following recent myocardial infarction (see WARNINGS)
Other:
Anaphylactoid or hypersensitivity reactions
Thromboembolism
Weight gain
Increased appetite
Nausea
Malaise
Hiccups
The following additional adverse reactions are related to parenteral corticosteroid therapy:
Rare instances of blindness associated with intralesional therapy around the face and head
Hyperpigmentation or hypopigmentation
Subcutaneous and cutaneous atrophy
Sterile abscess
Post-injection flare (following intra-articular use)
Charcot-like arthropathy
OVERDOSAGE:
Reports of acute toxicity and/or death following overdosage of glucocorticoids are rare. In the event of overdosage, no specific antidote is available; treatment is supportive and symptomatic.
The oral LD 50 of dexamethasone in female mice was 6.5 g/kg. The intravenous LD 50 of dexamethasone sodium phosphate in female mice was 794 mg/kg.
DOSAGE AND ADMINISTRATION:
Dexamethasone sodium phosphate injection, 4 mg/mL– For intravenous, intramuscular, intra-articular, intralesional, and soft tissue injection.
Dexamethasone sodium phosphate injection can be given directly from the vial, or it can be added to Sodium Chloride Injection or Dextrose Injection and administered by intravenous drip.
Solutions used for intravenous administration or further dilution of this product should be preservative free when used in the neonate, especially the premature infant.
When it is mixed with an infusion solution, sterile precautions should be observed. Since infusion solutions generally do not contain preservatives, mixtures should be used within 24 hours.
DOSAGE REQUIREMENTS ARE VARIABLE AND MUST BE INDIVIDUALIZED ON THE BASIS OF THE DISEASE AND THE RESPONSE OF THE PATIENT.
Intravenous and Intramuscular Injection:
The initial dosage of dexamethasone sodium phosphate injection varies from 0.5 to 9 mg a day depending on the disease being treated. In less severe diseases doses lower than 0.5 mg may suffice, while in severe diseases doses higher than 9 mg may be required.
The initial dosage should be maintained or adjusted until the patient’s response is satisfactory. If a satisfactory clinical response does not occur after a reasonable period of time, discontinue dexamethasone sodium phosphate injection and transfer the patient to other therapy.
After a favorable initial response, the proper maintenance dosage should be determined by decreasing the initial dosage in small amounts to the lowest dosage that maintains an adequate clinical response.
Patients should be observed closely for signs that might require dosage adjustment, including changes in clinical status resulting from remissions or exacerbations of the disease, individual drug responsiveness, and the effect of stress (e.g., surgery, infection, trauma). During stress it may be necessary to increase dosage temporarily.
If the drug is to be stopped after more than a few days of treatment, it usually should be withdrawn gradually.
When the intravenous route of administration is used, dosage usually should be the same as the oral dosage. In certain overwhelming, acute, life-threatening situations, however, administration in dosages exceeding the usual dosages may be justified and may be in multiples of the oral dosages. The slower rate of absorption by intramuscular administration should be recognized.
Shock
There is a tendency in current medical practice to use high (pharmacologic) doses of corticosteroids for the treatment of unresponsive shock. The following dosages of dexamethasone sodium phosphate injection have been suggested by various authors:
| Author
| Dosage
|
| Cavanagh
1
| 3 mg/kg of body weight per 24 hours by constant intravenous infusion after an initial intravenous injection of 20 mg
|
| Dietzman
2
| 2 to 6 mg/kg of body weight as a single intravenous injection
|
| Frank
3
| 40 mg initially followed by repeat
intravenous injection every 4 to 6 hours while shock persists |
| Oaks
4
| 40 mg initially followed by repeat
intravenous injection every 2 to 6 hours while shock persists |
| Schumer
5
| 1 mg/kg of body weight as a single intravenous injection
|
Administration of high dose corticosteroid therapy should be continued only until the patient’s condition has stabilized and usually not longer than 48 to 72 hours.
Although adverse reactions associated with high dose, short term corticosteroid therapy are uncommon, peptic ulceration may occur.
Cerebral Edema
Dexamethasone sodium phosphate injection is generally administered initially in a dosage of 10 mg intravenously followed by four mg every six hours intramuscularly until the symptoms of cerebral edema subside. Response is usually noted within 12 to 24 hours and dosage may be reduced after two to four days and gradually discontinued over a period of five to seven days. For palliative management of patients with recurrent or inoperable brain tumors, maintenance therapy with two mg two or three times a day may be effective.
Acute Allergic Disorders
In acute, self-limited allergic disorders or acute exacerbations of chronic allergic disorders, the following dosage schedule combining parenteral and oral therapy is suggested:
Dexamethasone sodium phosphate injection, 4 mg/mL: first day, 1 or 2 mL (4 or 8 mg), intramuscularly.
Dexamethasone tablets, 0.75 mg: second and third days, 4 tablets in two divided doses each day; fourth day, 2 tablets in two divided doses; fifth and sixth days, 1 tablet each day; seventh day, no treatment; eighth day, follow-up visit.
This schedule is designed to ensure adequate therapy during acute episodes, while minimizing the risk of overdosage in chronic cases.
Intra-articular, Intralesional and Soft Tissue Injection:
Intra-articular, intralesional, and soft tissue injections are generally employed when the affected joints or areas are limited to one or two sites. Dosage and frequency of injection varies depending on the condition and the site of injection. The usual dose is from 0.2 to 6 mg. The frequency usually ranges from once every three to five days to once every two to three weeks. Frequent intra-articular injection may result in damage to joint tissues.
Some of the usual single doses are:
|
Site of Injection | Amount of
Dexamethasone Phosphate (mg) |
| Large Joints
(e.g., Knee) | 2 to 4
|
| Small Joints
(e.g., Interphalangeal, Temporomandibular) | 0.8 to 1
|
| Bursae
| 2 to 3
|
| Tendon Sheaths
| 0.4 to 1
|
| Soft Tissue Infiltration
| 2 to 6
|
| Ganglia
| 1 to 2
|
Dexamethasone sodium phosphate injection is particularly recommended for use in conjunction with one of the less soluble, longer-acting steroids for intra-articular and soft tissue injection.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever the solution and container permit.
HOW SUPPLIED:
| Product
No. | NDC
No. |
|
| PRX16501
| 63323-165-16
| Dexamethasone Sodium Phosphate Injection, USP (equivalent to 4 mg per mL dexamethasone phosphate) 1 mL fill, in a 2 mL flip-top vial, packaged in 25.
|
| PRX16505
| 63323-165-26
| Dexamethasone Sodium Phosphate Injection, USP (equivalent to 20 mg per 5 mL [4 mg per mL] dexamethasone phosphate) 5 mL fill, in a 5 mL flip-top vial, packaged in 25.
|
Store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature]. Protect from freezing. Sensitive to heat. Do not autoclave.
Protect from light. Store container in carton until contents have been used.
Do not use if precipitate is present.
REFERENCES:
- Cavanagh, D.; Singh, K.B.: Endotoxin shock in pregnancy and abortion, in: “Corticosteroids in the Treatment of Shock”, Schumer, W.; Nyhus, L.M., Editors, Urbana, University of Illinois Press, 1970, pp. 86-96.
- Dietzman, R.H.; Ersek, R.A.; Bloch, J.M.; Lillehei, R.C.: High-output, low-resistance gram-negative septic shock in man, Angiology 20: 691-700, Dec. 1969.
- Frank, E.: Clinical observations in shock and management (In: Shields, T.F., ed.: Symposium on current concepts and management of shock), J. Maine Med. Ass. 59: 195-200, Oct. 1968.
- Oaks, W. W.; Cohen, H.E.: Endotoxin shock in the geriatric patient, Geriat. 22: 120-130, Mar. 1967.
- Schumer, W.; Nyhus, L.M.: Corticosteroid effect on biochemical parameters of human oligemic shock, Arch. Surg. 100: 405-408, Apr. 1970.
PremierProRx ® is a registered trademark of Premier, Inc., used under license.
Manufactured by:
Fresenius Kabi
Lake Zurich, IL 60047
451449
www.fresenius-kabi.us
Issued: August 2015

DRUG: Dexamethasone Sodium Phosphate
GENERIC: DEXAMETHASONE SODIUM PHOSPHATE
DOSAGE: INJECTION, SOLUTION
ADMINSTRATION: INTRAMUSCULAR
NDC: 70518-0872-0
PACKAGING: 1 mL in 1 VIAL
ACTIVE INGREDIENT(S):
- DEXAMETHASONE SODIUM PHOSPHATE 4mg in 1mL
INACTIVE INGREDIENT(S):
- BENZYL ALCOHOL
- SODIUM HYDROXIDE
- CITRIC ACID MONOHYDRATE
- SODIUM CITRATE
- SODIUM SULFITE
| DEXAMETHASONE SODIUM PHOSPHATE
dexamethasone sodium phosphate injection, solution |
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
| Labeler - REMEDYREPACK INC. (829572556) |