Label: CEFACLOR capsule

- NDC Code(s): 50090-1602-0, 50090-1602-2
- Packager: A-S Medication Solutions
- This is a repackaged label.
- Source NDC Code(s): 61442-172
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: Abbreviated New Drug Application
Drug Label Information
Updated January 31, 2024
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
- SPL UNCLASSIFIED SECTION
-
DESCRIPTION
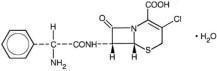
Cefaclor, USP is a semisynthetic cephalosporin antibiotic for oral administration. It is chemically designated as 3-chloro-7-D-(2-phenylglycinamido)-3-cephem-4-carboxylic acid monohydrate. The chemical formula for cefaclor is C15H14ClN3O4S•H2O and the molecular weight is 385.82.
Each 250-mg capsule contains cefaclor monohydrate equivalent to 250 mg (0.68 mmol) of anhydrous cefaclor and inactive ingredients: magnesium stearate, sodium starch glycolate, lactose monohydrate, talc. The 250 mg capsule shell contains gelatin, titanium dioxide, FD & C Blue No. 1, FD & C Red No. 3, and imprinting ink components: shellac, strong ammonia solution, potassium hydroxide, black iron oxide, .dehydrated alcohol, isopropyl alcohol, butyl alcohol and propylene glycol.
Each 500-mg capsule contains cefaclor monohydrate equivalent to 500 mg (1.36 mmol) of anhydrous cefaclor and inactive ingredients: magnesium stearate, sodium starch glycolate, lactose monohydrate, talc. The 500 mg capsule shell contains gelatin, titanium dioxide, FD & C Blue No. 1, FD & C Red No. 3, FD & C Yellow No. 6, FD & C Red No. 40, and imprinting ink components: shellac, strong ammonia solution, titanium dioxide, FD & C Blue No. 1 aluminum lake, dehydrated alcohol, isopropyl alcohol, butyl alcohol and propylene glycol.
-
CLINICAL PHARMACOLOGY
Cefaclor is well absorbed after oral administration to fasting subjects. Total absorption is the same whether the drug is given with or without food; however, when it is taken with food, the peak concentration achieved is 50% to 75% of that observed when the drug is administered to fasting subjects and generally appears from three fourths to 1 hour later. Following administration of 250-mg, 500-mg, and 1-g doses to fasting subjects, average peak serum levels of approximately 7, 13, and 23 mcg/mL respectively were obtained within 30 to 60 minutes. Approximately 60% to 85% of the drug is excreted unchanged in the urine within 8 hours, the greater portion being excreted within the first 2 hours. During this 8-hour period, peak urine concentrations following the 250-mg, 500-mg and 1-g doses were approximately 600, 900 and 1,900 mcg/mL, respectively. The serum half-life in normal subjects is 0.6 to 0.9 hour. In patients with reduced renal function, the serum half-life of cefaclor is slightly prolonged. In those with complete absence of renal function, the plasma half-life of the intact molecule is 2.3 to 2.8 hours. Excretion pathways in patients with markedly impaired renal function have not been determined. Hemodialysis shortens the half-life by 25% to 30%.
Microbiology
Mechanism of Action
As with other cephalosporins, the bactericidal action of cefaclor results from inhibition of cell-wall synthesis.Mechanism of Resistance
Resistance to cefaclor is primarily through hydrolysis of beta-lactamases, alteration of penicillin-binding proteins (PBPs) and decreased permeability. Pseudomonas spp., Acinetobacter calcoaceticus and most strains of Enterococi (Enterococcus faecalis, group D streptococci), Enterobacter spp., indole-positive Proteus, Morganella morganii (formerly Proteus morganii), Providencia rettgeri (formerly Proteus rettgeri) and Serratia spp. are resistant to cefaclor. Cefaclor is inactive against methicillin-resistant staphylococci. -lactamase-negative, ampicillin-resistant strains of H. influenzae should be considered resistant to cefaclor despite apparent in vitro susceptibility to this agent.
Antibacterial Activity
Cefaclor has been shown to be active against most strains of the following microorganisms both in vitro and in clinical infections as described in the INDICATIONS AND USAGE section.
Gram-positive Bacteria
Staphylococcus aureus (methicillin susceptible only)
Coagulase negative staphylococci (methicillin susceptible only)
Streptococcus pneumoniae
Streptococcus pyogenes (group A -hemolytic streptococci)Gram-negative Bacteria
Escherichia coli
Haemophilus influenzae (excluding -lactamase-negative, ampicillin-resistant strains)
Klebsiella spp.
Proteus mirabilisThe following in vitro data are available, but their clinical significance is unknown. At least 90 percent of the following bacteria exhibit an in vitro minimum inhibitory concentrations (MICs) less than or equal to the susceptible breakpoint of cefaclor. However, the safety and effectiveness of cefaclor in treating clinical infections due to these bacteria has not been established in adequate and well-controlled trials.
Gram-negative Bacteria
Citrobacter diversus
Moraxella catarrhalis
Neisseria gonorrhoeaeAnaerobic Bacteria
Bacteroides spp.
Peptococcus spp.
Peptostreptococcus spp.
Propionibacterium acnesSusceptibility Test Methods
When available, the clinical microbiology laboratory should provide the result of in vitro susceptibility test results for antimicrobial drugs used in resident hospitals to the physician as periodic reports that describe the susceptibility profile of nosocomial and community-acquired pathogens. These reports should aid the physician in selecting an antibacterial drug for treatment.
Dilution Techniques
Quantitative methods are used to determine antimicrobial minimum inhibitory concentrations (MICs). These MICs provide estimates of the susceptibility of bacteria to antimicrobial compounds. The MICs should be determined using a standardized method (broth, agar, or microdilution)1,3. The MIC values should be interpreted according to criteria provided in Table 1.Diffusion Techniques
Quantitative methods that require measurement of zone diameters also provide reproducible estimates of the susceptibility of bacteria to antimicrobial compounds. The zone size provides an estimate of the susceptibility of bacteria to antimicrobial compounds. The zone size should be determined using a standardized test method2,3. This procedure uses paper disks impregnated with 30-mcg cefaclor to test the susceptibility of microorganisms to cefaclor. The disc diffusion interpretive criteria are provided in Table 1.Table 1: Susceptibility Test Interpretive Criteria for Cefaclor
Table 1: Susceptibility Test Interpretive Criteria for Cefaclor Microorganisms1,2 Minimal Inhibitory
Concentration
(mcg/mL)Zone
Diameter
(mm)S I R S I R Streptococcus pneumoniae ≤1 2 ≥4 -- -- -- 1 Susceptibility of staphylococci to cefaclor may be deduced from testing only penicillin and either cefoxitin or oxacillin
2 Susceptibility of Streptococcus pyogenes to cefaclor may also be deduced from testing penicillinA report of Susceptible indicates that antimicrobial is likely to inhibit growth of the pathogen if the antimicrobial compound reaches the concentrations at the site of infection necessary to inhibit growth of the pathogen. A report of Intermediate indicates that the result should be considered equivocal, and, if the microorganism is not fully susceptible to alternative, clinically feasible drugs, the test should be repeated. This category implies possible clinical applicability in body sites where the drug is physiologically concentrated or in situations where a high dosage of drug can be used. This category also provides a buffer zone that prevents small uncontrolled technical factors from causing major discrepancies in interpretation. A report of Resistant indicates that the antimicrobial is not likely to inhibit growth of the pathogen if the antimicrobial compound reaches the concentrations usually achievable at the infection site; other therapy should be selected.
Quality Control
Standardized susceptibility test procedures require the use of laboratory controls to monitor and ensure the accuracy and precision of supplies and reagents used in the assay, and the techniques of the individuals performing the test.1,2,3 Standard cefaclor powder should provide the following range of MIC values noted in Table 2. For the diffusion technique using the 30 mcg disk the criteria in Table 2 should be achieved.Table 2: Acceptable Quality Control Ranges for Cefaclor
Table 2: Acceptable Quality Control Ranges for Cefaclor QC Strain Minimal Inhibitory
Concentration
(mcg/mL)Zone
Diameter
(mm)Escherichia coli ATCC 25922 1 – 4 23 – 27 Haemophilus influenzae ATCC 49766 1 – 4 25 – 31 Staphylococcus aureus ATCC 25923 -- 27 - 31 Staphylococcus aureus ATCC 29213 1 – 4 -- Streptococcus pneumoniae ATCC 49619 1 – 4 24 – 32 -
INDICATIONS AND USAGE
Cefaclor is indicated in the treatment of the following infections when caused by susceptible strains of the designated microorganisms:
Otitis media caused by Streptococcus pneumoniae, Haemophilus influenzae, staphylococci, and Streptococcus pyogenes
Note: β-lactamase-negative, ampicillin-resistant (BLNAR) strains of Haemophilus influenzae should be considered resistant to cefaclor despite apparent in vitro susceptibility of some BLNAR strains.
Lower respiratory tract infections, including pneumonia, caused by Streptococcus pneumoniae, Haemophilus influenzae, and Streptococcus pyogenes
Note: β-lactamase-negative, ampicillin-resistant (BLNAR) strains of Haemophilus influenzae should be considered resistant to cefaclor despite apparent in vitro susceptibility of some BLNAR strains.
Pharyngitis and Tonsillitis, caused by Streptococcus pyogenes
Note: Penicillin is the usual drug of choice in the treatment and prevention of streptococcal infections, including the prophylaxis of rheumatic fever. Cefaclor is generally effective in the eradication of streptococci from the nasopharynx; however, substantial data establishing the efficacy of cefaclor in the subsequent prevention of rheumatic fever are not available at present.
Urinary tract infections, including pyelonephritis and cystitis, caused by Escherichia coli, Proteus mirabilis, Klebsiella spp., and coagulase-negative staphylococci
Skin and skin structure infections caused by Staphylococcus aureus and Streptococcus pyogenes
Appropriate culture and susceptibility studies should be performed to determine susceptibility of the causative organism to cefaclor.
To reduce the development of drug-resistant bacteria and maintain the effectiveness of Cefaclor Capsule and other antibacterial drugs, Cefaclor Capsule should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.
- CONTRAINDICATION
-
WARNINGS
BEFORE THERAPY WITH CEFACLOR IS INSTITUTED, CAREFUL INQUIRY SHOULD BE MADE TO DETERMINE WHETHER THE PATIENT HAS HAD PREVIOUS HYPERSENSITIVITY REACTIONS TO CEFACLOR, CEPHALOSPORINS, PENICILLINS, OR OTHER DRUGS. IF THIS PRODUCT IS TO BE GIVEN TO PENICILLINSENSITIVE PATIENTS, CAUTION SHOULD BE EXERCISED BECAUSE CROSS-HYPERSENSITIVITY AMONG β-LACTAM ANTIBIOTICS HAS BEEN CLEARLY DOCUMENTED AND MAY OCCUR IN UP TO 10% OF PATIENTS WITH A HISTORY OF PENICILLIN ALLERGY.
IF AN ALLERGIC REACTION TO CEFACLOR OCCURS, DISCONTINUE THE DRUG. SERIOUS ACUTE HYPERSENSITIVITY REACTIONS MAY REQUIRE TREATMENT WITH EPINEPHRINE AND OTHER EMERGENCY MEASURES, INCLUDING OXYGEN, INTRAVENOUS FLUIDS, INTRAVENOUS ANTIHISTAMINES, CORTICOSTEROIDS, PRESSOR AMINES, AND AIRWAY MANAGEMENT, AS CLINICALLY INDICATED.
Antibiotics, including cefaclor, should be administered cautiously to any patient who has demonstrated some form of allergy, particularly to drugs.
Pseudomembranous colitis has been reported with nearly all antibacterial agents, including cefaclor, and has ranged in severity from mild to life-threatening. Therefore, it is important to consider this diagnosis in patients who present with diarrhea subsequent to the administration of antibacterial agents.
Treatment with antibacterial agents alters the normal flora of the colon and may permit overgrowth of clostridia. Studies indicate that a toxin produced by Clostridium difficile is one primary cause of antibiotic-associated colitis.
After the diagnosis of pseudomembranous colitis has been established, therapeutic measures should be initiated. Mild cases of pseudomembranous colitis usually respond to drug discontinuation alone. In moderate to severe cases, consideration should be given to management with fluids and electrolytes, protein supplementation and treatment with an antibacterial drug effective against C. difficile.
-
PRECAUTIONS
General
Prescribing cefaclor in the absence of a proven or strongly suspected bacterial infection or a prophylactic indication is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria.
Prolonged use of cefaclor may result in the overgrowth of nonsusceptible organisms. Careful observation of the patient is essential. If superinfection occurs during therapy, appropriate measures should be taken.
Positive direct Coombs' tests have been reported during treatment with the cephalosporin antibiotics. It should be recognized that a positive Coombs' test may be due to the drug, e.g., in hematologic studies or in transfusion cross-matching procedures when antiglobulin tests are performed on the minor side or in Coombs' testing of newborns whose mothers have received cephalosporin antibiotics before parturition.
Cefaclor should be administered with caution in the presence of markedly impaired renal function. Since the half-life of cefaclor in anuria is 2.3 to 2.8 hours, dosage adjustments for patients with moderate or severe renal impairment are usually not required. Clinical experience with cefaclor under such conditions is limited; therefore, careful clinical observation and laboratory studies should be made.
As with other β-lactam antibiotics, the renal excretion of cefaclor is inhibited by probenecid.
Antibiotics, including cephalosporins, should be prescribed with caution in individuals with a history of gastrointestinal disease, particularly colitis.
Information for Patients
Patients should be counseled that antibacterial drugs including cefaclor should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). When cefaclor is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by cefaclor or other antibacterial drugs in the future.
Drug/Laboratory Test Interactions
Patients receiving cefaclor may show a false-positive reaction for glucose in the urine with tests that use Benedict's and Fehling's solutions and also with Clinitest® tablets.
There have been reports of increased anticoagulant effect when cefaclor and oral anticoagulants were administered concomitantly.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Studies have not been performed to determine potential for carcinogenicity, mutagenicity, or impairment of fertility.
Pregnancy ─ Teratogenic Effects ─ Pregnancy Category B
Reproduction studies have been performed in mice and rats at doses up to 12 times the human dose and in ferrets given 3 times the maximum human dose and have revealed no harm to the fetus due to cefaclor. There are, however, no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.
Nursing Mothers
Small amounts of cefaclor have been detected in mother's milk following administration of single 500-mg doses. Average levels were 0.18, 0.20, 0.21, and 0.16 mcg/mL at 2, 3, 4, and 5 hours respectively. Trace amounts were detected at 1 hour. The effect on nursing infants is not known. Caution should be exercised when cefaclor is administered to a nursing woman.
Pediatric Use
Safety and effectiveness of this product for use in infants less than 1 month of age have not been established.
Geriatric Use
Of the 3703 patients in clinical studies of cefaclor, 594 (16.0%) were 65 and older. No overall differences in safety or effectiveness were observed between these subjects and younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
This drug is known to be substantially excreted by the kidney (see CLINICAL PHARMACOLOGY), and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful in monitor renal function (see DOSAGE AND ADMINISTRATION).
-
ADVERSE REACTIONS
Adverse effects considered to be related to therapy with cefaclor are listed below:
Hypersensitivity reactions have been reported in about 1.5% of patients and include morbilliform eruptions (1 in 100). Pruritus, urticaria, and positive Coombs' tests each occur in less than 1 in 200 patients.
Cases of serum-sickness-like reactions have been reported with the use of cefaclor. These are characterized by findings of erythema multiforme, rashes, and other skin manifestations accompanied by arthritis/arthralgia, with or without fever, and differ from classic serum sickness in that there is infrequently associated lymphadenopathy and proteinuria, no circulating immune complexes, and no evidence to date of sequelae of the reaction. Occasionally, solitary symptoms may occur, but do not represent a serum-sickness-like reaction. While further investigation is ongoing, serum-sicknesslike reactions appear to be due to hypersensitivity and more often occur during or following a second (or subsequent) course of therapy with cefaclor. Such reactions have been reported more frequently in pediatric patients than in adults with an overall occurrence ranging from 1 in 200 (0.5%) in one focused trial to 2 in 8,346 (0.024%) in overall clinical trials (with an incidence in pediatric patients in clinical trials of 0.055%) to 1 in 38,000 (0.003%) in spontaneous event reports. Signs and symptoms usually occur a few days after initiation of therapy and subside within a few days after cessation of therapy; occasionally these reactions have resulted in hospitalization, usually of short duration (median hospitalization = 2 to 3 days, based on postmarketing surveillance studies). In those requiring hospitalization, the symptoms have ranged from mild to severe at the time of admission with more of the severe reactions occurring in pediatric patients. Antihistamines and glucocorticoids appear to enhance resolution of the signs and symptoms. No serious sequelae have been reported.
More severe hypersensitivity reactions, including Stevens-Johnson syndrome, toxic epidermal necrolysis, and anaphylaxis have been reported rarely. Anaphylactoid events may be manifested by solitary symptoms, including angioedema, asthenia, edema (including face and limbs), dyspnea, paresthesias, syncope, hypotension, or vasodilatation. Anaphylaxis may be more common in patients with a history of penicillin allergy.
Rarely, hypersensitivity symptoms may persist for several months.
Gastrointestinal symptoms occur in about 2.5% of patients and include diarrhea (1 in 70).
Onset of pseudomembranous colitis symptoms may occur during or after antibiotic treatment. (see WARNINGS). Nausea and vomiting have been reported rarely. As with some penicillins and some other cephalosporins, transient hepatitis and cholestatic jaundice have been reported rarely.
Other effects considered related to therapy included eosinophilia (1 in 50 patients), genital pruritus, moniliasis or vaginitis (about 1 in 50 patients), and, rarely, thrombocytopenia or reversible interstitial nephritis.
Causal Relationship Uncertain –
CNS ─ Rarely, reversible hyperactivity, agitation, nervousness, insomnia, confusion, hypertonia, dizziness, hallucinations, and somnolence have been reported.
Transitory abnormalities in clinical laboratory test results have been reported. Although they were of uncertain etiology, they are listed below to serve as alerting information for the physician.
Hepatic ─ Slight elevations of AST, ALT, or alkaline phosphatase values (1 in 40).
Hematopoietic ─ As has also been reported with other β-lactam antibiotics, transient lymphocytosis, leukopenia, and, rarely, hemolytic anemia, aplastic anemia, agranulocytosis, and reversible neutropenia of possible clinical significance.
There have been rare reports of increased prothrombin time with or without clinical bleeding in patients receiving cefaclor and Coumadin® concomitantly.
Renal ─ Slight elevations in BUN or serum creatinine (less than 1 in 500) or abnormal urinalysis (less than 1 in 200).
Cephalosporin-class Adverse Reactions
In addition to the adverse reactions listed above that have been observed in patients treated with cefaclor, the following adverse reactions and altered laboratory tests have been reported for cephalosporin-class antibiotics: fever, abdominal pain, superinfection, renal dysfunction, toxic nephropathy, hemorrhage, false positive test for urinary glucose, elevated bilirubin, elevated LDH, and pancytopenia.
Several cephalosporins have been implicated in triggering seizures, particularly in patients with renal impairment when the dosage was not reduced. If seizures associated with drug therapy occur, the drug should be discontinued. Anticonvulsant therapy can be given if clinically indicated (see DOSAGE AND ADMINISTRATION and OVERDOSAGE sections).
-
OVERDOSAGE
Signs and Symptoms ─ The toxic symptoms following an overdose of cefaclor may include nausea, vomiting, epigastric distress, and diarrhea. The severity of the epigastric distress and the diarrhea are dose related. If other symptoms are present, it is probable that they are secondary to an underlying disease state, an allergic reaction, or the effects of other intoxication.
Treatment -- To obtain up-to-date information about the treatment of overdose, a good resource is your certified Regional Poison Control Center. Telephone numbers of certified poison control centers are listed in the Physicians' Desk Reference (PDR). In managing overdosage, consider the possibility of multiple drug overdoses, interaction among drugs, and unusual drug kinetics in your patient. Unless 5 times the normal dose of cefaclor has been ingested, gastrointestinal decontamination will not be necessary.
Protect the patient's airway and support ventilation and perfusion. Meticulously monitor and maintain, within acceptable limits, the patient's vital signs, blood gases, serum electrolytes, etc. Absorption of drugs from the gastrointestinal tract may be decreased by giving activated charcoal, which, in many cases, is more effective than emesis or lavage; consider charcoal instead of or in addition to gastric emptying. Repeated doses of charcoal over time may hasten elimination of some drugs that have been absorbed. Safeguard the patient's airway when employing gastric emptying or charcoal.
Forced diuresis, peritoneal dialysis, hemodialysis, or charcoal hemoperfusion have not been established as beneficial for an overdose of cefaclor.
-
DOSAGE AND ADMINISTRATION
Cefaclor is administered orally.
Adults ─ The usual adult dosage is 250 mg every 8 hours. For more severe infections (such as pneumonia) or those caused by less susceptible organisms, doses may be doubled.
Pediatric Patients ─ The usual recommended daily dosage for pediatric patients is 20 mg/kg/day in divided doses every 8 hours. In more serious infections, otitis media, and infections caused by less susceptible organisms, 40 mg/kg/day are recommended, with a maximum dosage of 1 g/day.
Cefaclor may be administered in the presence of impaired renal function. Under such a condition, the dosage usually is unchanged (see PRECAUTIONS).
In the treatment of β-hemolytic streptococcal infections, a therapeutic dosage of cefaclor should be administered for at least 10 days.
- HOW SUPPLIED
-
REFERENCES
1. Clinical and Laboratory Standards Institute (CLSI). Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria that Grow Aerobically; Approved Standard - Tenth Edition. CLSI document M07-A10, Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087, USA, 2015.
2. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Disk Diffusion Susceptibility Tests; Approved Standard – Twelfth Edition. CLSI document M02-A12, Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087, USA, 2015.
3. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing; Twenty-fifth Informational Supplement. CLSI document M100-S25. Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087, USA, 2015.
Manufactured by:
Yung Shin Pharmaceutical Ind. Co., Ltd.Tachia, Taichung 43769, TAIWANDistributed by:
Carlsbad Technology, Inc.5923 Balfour Ct.
Carlsbad, CA 92008 USARevised: 09/15
- Cefaclor
-
INGREDIENTS AND APPEARANCE
CEFACLOR
cefaclor capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:50090-1602(NDC:61442-172) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength CEFACLOR (UNII: 69K7K19H4L) (CEFACLOR ANHYDROUS - UNII:3Z6FS3IK0K) CEFACLOR ANHYDROUS 500 mg Inactive Ingredients Ingredient Name Strength magnesium stearate (UNII: 70097M6I30) SODIUM STARCH GLYCOLATE TYPE A POTATO (UNII: 5856J3G2A2) lactose monohydrate (UNII: EWQ57Q8I5X) talc (UNII: 7SEV7J4R1U) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) titanium dioxide (UNII: 15FIX9V2JP) FD&C Blue No. 1 (UNII: H3R47K3TBD) FD&C Red No. 3 (UNII: PN2ZH5LOQY) FD&C Yellow No. 6 (UNII: H77VEI93A8) FD&C Red No. 40 (UNII: WZB9127XOA) shellac (UNII: 46N107B71O) ammonia (UNII: 5138Q19F1X) alcohol (UNII: 3K9958V90M) isopropyl alcohol (UNII: ND2M416302) tert-butyl alcohol (UNII: MD83SFE959) propylene glycol (UNII: 6DC9Q167V3) Product Characteristics Color blue (BLUE) , orange (ORANGE) Score no score Shape CAPSULE (CAPSULE) Size 23mm Flavor Imprint Code KRC500 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:50090-1602-0 30 in 1 BOTTLE; Type 0: Not a Combination Product 02/20/2019 2 NDC:50090-1602-2 21 in 1 BOTTLE; Type 0: Not a Combination Product 01/06/2015 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA065146 07/31/2008 Labeler - A-S Medication Solutions (830016429) Establishment Name Address ID/FEI Business Operations A-S Medication Solutions 830016429 RELABEL(50090-1602) , REPACK(50090-1602)