NEGGRAM- nalidixic acid tablet
sanofi-aventis U.S. LLC
----------
To reduce the development of drug-resistant bacteria and maintain the effectiveness of NegGram (nalidixic acid, USP) and other antibacterial drugs, NegGram should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria.
DESCRIPTION
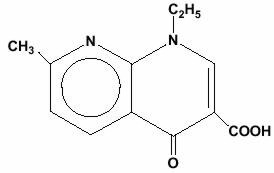
NegGram, brand of nalidixic acid, is a quinolone antibacterial agent for oral administration. Nalidixic acid is 1-ethyl-1,4-dihydro-7-methyl-4-oxo-1,8-naphthyridine-3-carboxylic acid. It is a pale yellow, crystalline substance and a very weak organic acid.
Nalidixic acid has the following structural formula:
Inactive Ingredients - Hydrogenated Vegetable Oil, Methylcellulose, Microcrystalline Cellulose, Sodium Lauryl Sulfate, Yellow Ferric Oxide.
CLINICAL PHARMACOLOGY
Following oral administration, NegGram is rapidly absorbed from the gastrointestinal tract, partially metabolized in the liver, and rapidly excreted through the kidneys. Unchanged nalidixic acid appears in the urine along with an active metabolite, hydroxynalidixic acid, which has antibacterial activity similar to that of nalidixic acid. Other metabolites include glucuronic acid conjugates of nalidixic acid and hydroxy nalidixic acid, and the dicarboxylic acid derivative. The hydroxy metabolite represents 30 percent of the biologically active drug in the blood and 85 percent in the urine. Peak serum levels of active drug average approximately 20 mcg to 40 mcg per mL (90 percent protein bound), one to two hours after administration of a 1 g dose to a fasting normal individual, with a half-life of about 90 minutes. Peak urine levels of active drug average approximately 150 mcg to 200 mcg per mL, three to four hours after administration, with a half-life of about six hours. Approximately four percent of NegGram is excreted in the feces. Traces of nalidixic acid were found in blood and urine of an infant whose mother had received the drug during the last trimester of pregnancy. (See PRECAUTIONS, Drug Interactions)
MICROBIOLOGY
Mechanism of Action
Nalidixic acid blocks DNA replication in susceptible bacteria by inhibiting a subunit of DNA gyrase.
Mechanism of Resistance
Conventional chromosomal resistance to nalidixic acid taken in full dosage has been reported to emerge in approximately 2 to 14 percent of patients during treatment; however, bacterial resistance to nalidixic acid has not been shown to be transferable via R factor. Pseudomonas species are generally resistant to the drug. Nalidixic acid is bactericidal and is effective over the entire urinary pH range.
Nalidixic acid has been shown to be active against most isolates of the following microorganisms, both in vitro and in clinical infections as described in the INDICATIONS AND USAGE section of the package insert for NEGGRAM.
Susceptibility Test
When available, the clinical microbiology laboratory should provide the results of in vitro susceptibility test results for antimicrobial drug products used in resident hospitals to the physician as periodic reports that describe the susceptibility profile of nosocomial and community-acquired pathogens. These reports should aid the physician in selecting an antibacterial drug product for treatment.
Dilution Techniques
Quantitative methods are used to determine antimicrobial minimum inhibitory concentrations (MICs). These MICs provide estimates of the susceptibility of bacteria to antimicrobial compounds. The MICs should be determined using a standardized test method (broth and/or agar).1,3 The MIC values should be interpreted according to criteria provided in Table 1.
Diffusion Techniques
Quantitative methods that require measurement of zone diameters can also provide reproducible estimates of the susceptibility of bacteria to antimicrobial compounds. The zone size provides an estimate of the susceptibility of bacteria to antimicrobial compounds. The zone size should be determined using a standardized test method.2,3 This procedure uses paper disks impregnated with 30 mcg nalidixic acid to test the susceptibility of bacteria to nalidixic acid. The disc diffusion interpretive criteria are provided in Table 1.
| MIC (mcg/mL) | Zone diameter (mm) | |||||
|---|---|---|---|---|---|---|
| Bacteria | S | I | R | S | I | R |
| S=Susceptible, I=Intermediate, and R=Resistant | ||||||
| Enterobacteriaceae | ≤ 16 | - | ≥ 32 | ≥ 19 | 14–18 | ≤ 13 |
A report of Susceptible indicates that the antimicrobial is likely to inhibit growth of the pathogen if the antimicrobial compound reaches the concentrations at the site of infection necessary to inhibit growth of the pathogen. A report of Intermediate indicates that the result should be considered equivocal, and if the microorganism is not fully susceptible to alternative, clinically feasible drugs, the test should be repeated. This category implies possible clinical applicability in body sites where the drug is physiologically concentrated or in situations where high dosage of drug can be used. This category also provides a buffer zone that prevents small uncontrolled technical factors from causing major discrepancies in interpretation. A report of Resistant indicates that the antimicrobial is not likely to inhibit growth of the pathogen if the antimicrobial compound reaches the concentration usually achievable at the infection site; other therapy should be selected.
Quality Control
Standardized susceptibility test procedures require the use of laboratory controls to monitor and ensure the accuracy and precision of supplies and reagents used in the assay, and the techniques of the individuals performing the test.1,2,3 Standard nalidixic acid powder should provide the following range of MIC values noted in Table 2. For the diffusion technique using the 30 mcg nalidixic acid disk the criteria in Table 2 should be achieved.
| QC Strains | MIC range (mcg/mL) | Zone Diameter (mm) |
|---|---|---|
| Escherichia coli ATCC 25922 | 1–4 | 22–28 |
INDICATIONS AND USAGE
NegGram (nalidixic acid, USP) is indicated for the treatment of urinary tract infections caused by susceptible gram-negative microorganisms, including the majority of E. Coli, Enterobacter species, Klebsiella pneumoniae, Morganella morganii, Proteus mirabilis, Proteus vulgaris, and Providencia rettgeri. Disc susceptibility testing with the 30 mcg disc should be performed prior to administration of the drug, and during treatment if clinical response warrants.
To reduce the development of drug-resistant bacteria and maintain effectiveness of NegGram and other antibacterial drugs, NegGram should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered when selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.
CONTRAINDICATIONS
NegGram is contraindicated in patients with known hypersensitivity to nalidixic acid or to related compounds, infants less than three months of age, and in patients with porphyria or a history of convulsive disorders. NegGram is contraindicated in patients undergoing concomitant therapy with melphalan or other related cancer chemotherapeutic alkylating agents because of serious gastrointestinal toxicity such as hemorrhagic ulcerative colitis or intestinal necrosis.
WARNINGS
Central Nervous System (CNS) effects including convulsions, increased intracranial pressure, and toxic psychosis have been reported with nalidixic acid therapy. Convulsive seizures have been reported with other drugs in this class. Quinolones may also cause CNS stimulation which may lead to tremor, restlessness, lightheadedness, confusion, and hallucinations. Therefore, nalidixic acid should be used with caution in patients with known or suspected CNS disorders, such as, cerebral arteriosclerosis or epilepsy, or other factors which predispose seizures. (See ADVERSE REACTIONS) If these reactions occur in patients receiving nalidixic acid, the drug should be discontinued and appropriate measures instituted.
Serious and occasionally fatal hypersensitivity (anaphylactoid) reactions, some following the first dose, have been reported in patients receiving quinolone therapy. Some reactions were accompanied by cardiovascular collapse, loss of consciousness, tingling, pharyngeal or facial edema, dyspnea, urticaria, and itching. Only a few patients had a history of hypersensitivity reactions. Serious anaphylactoid reactions required immediate emergency treatment with epinephrine. Oxygen, intravenous steroids, and airway management, including intubation, should be administered as indicated.
Nalidixic acid and other members of the quinolone drug class have been shown to cause arthropathy in juvenile animals. (See PRECAUTIONS and ANIMAL PHARMACOLOGY)
Clostridium difficile associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including NegGram, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile.
C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin producing strains of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibiotic use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents.
If CDAD is suspected or confirmed, ongoing antibiotic use not directed against C. difficile may need to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibiotic treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated.
Peripheral Neuropathy
Rare cases of sensory or sensorimotor axonal polyneuropathy affecting small and/or large axons resulting in paresthesias, hypoesthesias, dysesthesias and weakness have been reported in patients receiving quinolones, including nalidixic acid. Nalidixic acid should be discontinued if the patient experiences symptoms of neuropathy including pain, burning, tingling, numbness, and/or weakness, or is found to have deficits in light touch, pain, temperature, position sense, vibratory sensation, and/or motor strength in order to prevent the development of an irreversible condition.
Tendon Effects
Ruptures of the shoulder, hand, Achilles tendon or other tendons that required surgical repair or resulted in prolonged disability have been reported in patients receiving quinolones, including nalidixic acid. Post-marketing surveillance reports indicate that this risk may be increased in patients receiving concomitant corticosteroids, especially in the elderly. Nalidixic acid should be discontinued if the patient experiences pain, inflammation, or rupture of a tendon. Patients should rest and refrain from exercise until the diagnosis of tendonitis or tendon rupture has been excluded. Tendon rupture can occur during or after therapy with quinolones, including nalidixic acid. (See ADVERSE REACTIONS, Other)
PRECAUTIONS
General
Blood counts and renal and liver function tests should be performed periodically if treatment is continued for more than two weeks. NegGram should be used with caution in patients with liver disease, epilepsy, or severe cerebral arteriosclerosis. (See WARNINGS) Caution should be used in patients with renal insufficiency. (See DOSAGE AND ADMINISTRATION)
Moderate to severe phototoxicity reactions have been observed in patients who are exposed to direct sunlight while receiving NegGram or other members of this drug class. Excessive sunlight should be avoided. Therapy should be discontinued if phototoxicity occurs.
If bacterial resistance to NegGram emerges during treatment, it usually does so within 48 hours, permitting rapid change to another antimicrobial. Therefore, if the clinical response is unsatisfactory or if relapse occurs, cultures and sensitivity tests should be repeated. Underdosage with NegGram during initial treatment (with less than 4 g per day for adults) may predispose to emergence of bacterial resistance. (See DOSAGE AND ADMINISTRATION)
Cross-resistance between nalidixic acid and other quinolone derivatives such as oxolinic acid and cinoxacin has been observed.
Caution should be observed in patients with glucose-6-phosphate dehydrogenase deficiency. (See ADVERSE REACTIONS)
Prescribing NegGram in the absence of a proven or strongly suspected bacterial infection or a prophylactic indication is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria.
Information for Patients
Patients should be advised NegGram may be taken with or without meals. Patients should be advised to drink fluids liberally and not take antacids.
Patients should be advised that quinolones may be associated with hypersensitivity reactions, even following a single dose, and to discontinue the drug at the first sign of a skin rash or other allergic reactions.
Quinolones may cause dizziness and light-headedness, therefore, patients should know how they react to NegGram before they operate an automobile or machinery or engage in activities requiring mental alertness or coordination.
Patients should be advised that quinolones may increase the effects of theophylline and caffeine. There is a possibility of caffeine accumulation when products containing caffeine are consumed while taking quinolones. Patients should be advised to avoid excessive sunlight or artificial ultraviolet light while receiving nalidixic acid and to discontinue therapy if phototoxicity occurs.
Patients should be advised that convulsions have been reported in patients taking quinolones, including nalidixic acid, and to notify their physician before taking this drug if there is a history of this condition. Patients should be advised that mineral supplements, vitamins with iron or minerals, calcium-, aluminum-, magnesium-based antacids, sucralfate or Videx®, (didanosine), chewable/buffered tablets of the pediatric powder for oral solution should not be taken within the two-hour period before or within the two-hour period after taking nalidixic acid. (See Drug Interactions)
Patients should be advised:
- -
- that nalidixic acid may cause changes in the electrocardiogram (QTc interval prolongation)
- -
- that nalidixic acid should be avoided in patients receiving class IA (e.g. quinidine, Procainamide) or class III (e.g. amiodarone, sotalol) antiarrhythmic agents
- -
- that nalidixic acid should be used with caution in subjects receiving drugs that affect the QTc interval such as cisapride, erythromycin, antipsychotics, and tricyclic antidepressants
- -
- to inform their physicians of any personal or family history of QTc prolongation or proarrhythmic conditions such as hypokalemia, bradycardia or recent myocardial ischemia
- -
- that peripheral neuropathies have been associated with nalidixic acid use. If symptoms of peripheral neuropathy including pain, burning, tingling, numbness, and/or weakness develop, they should discontinue treatment and contact their physicians
- -
- that diarrhea is a common problem caused by antibiotics which usually ends when the antibiotic is discontinued. Sometimes after starting treatment with antibiotics, patients can develop watery and bloody stools (with or without stomach cramps and fever) even as late as two or more months after having taken the last dose of the antibiotic. If this occurs, patients should contact their physician as soon as possible.
Patients should be counseled that antibacterial drugs including NegGram should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). When NegGram is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by NegGram or other antibacterial drugs in the future.
Drug Interactions
Elevated plasma levels of theophylline have been reported with concomitant quinolone use. There have been reports of theophylline-related side effects in patients on concomitant therapy with quinolones and theophylline. Therefore, monitoring of theophylline plasma levels should be considered and dosage of theophylline adjusted, as required.
Quinolones have been shown to interfere with the metabolism of caffeine. This may lead to reduced clearance of caffeine and the prolongation of its plasma half-life.
Quinolones, including nalidixic acid, may enhance the effects of the oral anticoagulant warfarin or its derivatives. When these products are administered concomitantly, prothrombin time or other suitable coagulation test should be closely monitored.
Since active proliferation of organisms is a necessary condition for its antibacterial activity, the action of nalidixic acid may be inhibited by the presence of other antibacterial substances, especially bacteriostatic agents such as tetracycline, chloramphenicol, or nitrofurantoin, which is antagonistic to nalidixic acid in vitro.
Probenecid inhibits the tubular secretion of nalidixic acid and may reduce its efficacy in the treatment of urinary tract infections while increasing the risk of systemic side effects.
Serious gastrointestinal toxicity has been associated with the concomitant use of nalidixic acid and the anti-cancer drug melphalan. (See CONTRAINDICATIONS)
Antacids containing magnesium, aluminum, or calcium; sucralfate or divalent or trivalent cations such as iron; multivitamins containing zinc; and Videx®, (Didanosine), chewable/buffered tablets or the pediatric powder for oral solution may substantially interfere with the absorption of quinolones, resulting in systemic levels considerably lower than desired. These agents should not be taken within the two-hour period before or within the two-hour period after nalidixic acid administration.
Elevated serum levels of cyclosporine have been reported with the concomitant use of some quinolones and cyclosporine. Therefore, cyclosporine serum levels should be monitored and appropriate cyclosporine dosage adjustments made when these drugs are used concomitantly.
Drug Laboratory Test Interactions
When Benedict's or Fehling's solution or Clinitest® Reagent Tablets are used to test the urine of patients taking NegGram, a false-positive reaction for glucose may be obtained, due to the liberation of glucuronic acid from the metabolites excreted. However, a colorimetric test for glucose based on an enzyme reaction (e.g., with Clinistix® Reagent Strips or Tes-Tape®) does not give a false-positive reaction to the liberated glucuronic acid.
Incorrect values may be obtained for urinary 17-keto and ketogenic steroids in patients receiving NegGram, because of an interaction between the drug and the m-dinitrobenzene used in the usual assay method. In such cases, the Porter-Silber test for 17-hydroxycorticoids may be used.
Carcinogenesis, Mutagenesis, Impairment of Fertility
In lifetime studies in the rat given nalidixic acid in the diet, there was an increased incidence of preputial gland neoplasms in the treated males and clitoral gland neoplasms in the treated females. Studies in mice in which nalidixic acid was administered in the feed for two years, or was given in the feed for 76 weeks followed by no treatment for 9 weeks, gave equivocal evidence of carcinogenic activity.
Nalidixic acid was tested in the Ames bacterial mutagenicity test (maximum dose 33 mcg/plate) and the mouse lymphoma assay (L5178Y/TK; maximum dose 100 mcg/mL) with and without metabolic activation, and results were negative.
Pregnancy
Teratogenic Effects
Pregnancy Category C
NegGram has been shown to be teratogenic and embryocidal in rats when given in oral doses six times the human dose. NegGram also prolonged the duration of pregnancy especially at four times the clinical dose. There are no adequate and well-controlled studies in pregnant women. Since nalidixic acid, like other drugs in this class, causes arthropathy in immature animals, NegGram should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. (See WARNINGS and ANIMAL PHARMACOLOGY)
Nursing Mothers
Since nalidixic acid is excreted in breast milk, it is contraindicated during lactation.
Pediatric Use
Safety and effectiveness in infants below the age of three months have not been established.
Usage in Patients Under 18 Years of Age
Toxicological studies have shown that nalidixic acid and related drugs can produce erosions of the cartilage in weight-bearing joints and other signs of arthropathy in immature animals of most species tested. No such joint lesions have been reported in humans to date. Nevertheless, until the significance of this finding is clarified, this drug should only be used in patients under 18 years of age when the potential benefit justifies the potential risk. If arthralgia occurs, treatment with nalidixic acid should be stopped. (See WARNINGS and ANIMAL PHARMACOLOGY)
Geriatric Use
Clinical studies of NegGram did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. Caution should therefore be observed in using nalidixic acid in elderly patients. This drug is known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function. (See PRECAUTIONS, General)
ADVERSE REACTIONS
Reactions reported after oral administration of NegGram include the following:
CNS effects
Drowsiness, weakness, headache, dizziness and vertigo. Reversible subjective visual disturbances without objective findings have occurred infrequently (generally with each dose during the first few days of treatment). These reactions include overbrightness of lights, change in color perception, difficulty in focusing, decrease in visual acuity, and double vision. They usually disappeared promptly when dosage was reduced or therapy was discontinued. Toxic psychosis or brief convulsions have been reported rarely, usually following excessive doses. In general, the convulsions have occurred in patients with predisposing factors such as epilepsy or cerebral arteriosclerosis. In infants and children receiving therapeutic doses of NegGram, increased intracranial pressure with bulging anterior fontanel, papilledema, and headache has occasionally been observed. A few cases of 6th cranial nerve palsy have been reported. Although the mechanisms of these reactions are unknown, the signs and symptoms usually disappeared rapidly with no sequelae when treatment was discontinued.
Gastrointestinal
Abdominal pain, nausea, vomiting, and diarrhea.
Allergic
Rash, pruritus, urticaria, angioedema, eosinophilia, arthralgia with joint stiffness and swelling, and anaphylactoid reaction, including anaphylactic shock. Erythema Multiforme and Stevens-Johnson syndrome have been reported with nalidixic acid and other drugs in this class. Rash was the most frequently reported adverse reaction. Photosensitivity reactions consisting of erythema and bullae on exposed skin surfaces usually resolve completely in 2 weeks to 2 months after NegGram is discontinued; however, bullae may continue to appear with successive exposures to sunlight or with mild skin trauma for up to 3 months after discontinuation of drug. (See PRECAUTIONS)
Other
Tendon disorders including tendon rupture, cholestasis, paresthesia, metabolic acidosis, thrombocytopenia, leukopenia, or hemolytic anemia, sometimes associated with glucose 6-phosphate dehydrogenase deficiency and peripheral neuropathy. (See WARNINGS)
OVERDOSAGE
Manifestations
Toxic psychosis, convulsions, increased intracranial pressure, or metabolic acidosis may occur in patients taking more than the recommended dosage. Vomiting, nausea, and lethargy may also occur following overdosage.
Treatment
Reactions are short-lived (two to three hours) because the drug is rapidly excreted. If absorption has occurred, increased fluid administration is advisable and supportive measures such as oxygen and means of artificial respiration should be available. Although anticonvulsant therapy has not been used in the few instances of overdosage reported, it may be indicated in a severe case.
DOSAGE AND ADMINISTRATION
Antacids containing calcium, magnesium, or aluminum; sucralfate; divalent or trivalent cations such as iron; multivitamins containing zinc; or Videx® (Didanosine), chewable/buffered tablets of the pediatric powder for oral solution should not be taken within the two-hour period before or within the two-hour period after taking nalidixic acid.
Adults
The recommended dosage for initial therapy in adults is 1 g administered four times daily for one or two weeks (total daily dose, 4 g). For prolonged therapy, the total daily dose may be reduced to 2 g after the initial treatment period. Underdosage during initial treatment may predispose to emergence of bacterial resistance.
Renal Insufficiency
The normal dosage of nalidixic acid may be employed in patients with plasma creatinine of less than 300 µmol/L (creatinine clearance more than 20 mL/minute). Dosage should be halved in patients with plasma creatinine of more than 300 µmol/L (creatinine clearance 20 mL/minute or less).
Pediatric Patients
Until further experience is gained, NegGram should not be administered to infants younger than three months. Dosage in pediatric patients 12 years of age and under should be calculated on the basis of body weight. The recommended total daily dosage for initial therapy is 25 mg/lb/day (55 mg/kg/day), administered in four equally divided doses. For prolonged therapy, the total daily dose may be reduced to 15 mg/lb/day (33 mg/kg/day). NegGram Caplets of 250 mg may be used.
HOW SUPPLIED
NegGram (nalidixic acid, USP) is supplied as:
Caplets of 500 mg, light buff-colored capsule-shaped tablets, bottles of 56 (NDC 0024-1322-03).
ANIMAL PHARMACOLOGY
NegGram (nalidixic acid) and related drugs have been shown to cause arthropathy in juvenile animals of most species tested. (See WARNINGS)
Long-term administration of nalidixic acid to rats resulted in retinal degeneration and cataracts.
Hydroxynalidixic acid, the principal metabolite of NegGram, did not produce any oculotoxic effects at any dosage level in seven species of animals including three primate species. However, oral administration of this metabolite in high doses has been shown to have oculotoxic potential, namely in dogs and cats where it produced retinal degeneration upon prolonged administration leading, in some cases, to blindness.
In experiments with NegGram itself, little if any such activity could be elicited in either dogs or cats. Sensitivity to CNS side effects in these species limited the doses of NegGram that could be used; this factor, together with a low conversion rate to the hydroxy metabolite in these species, may explain the absence of these effects.
REFERENCES
- Clinical and Laboratory Standards Institute, Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically; Approved Standard – 9th Edition. CLSI Document M7- A9, Vol. 29, No. 2, CLSI, 950 West Valley Rd., Suite 2500, Wayne, PA, January, 2012.
- CLSI, Performance Standards for Antimicrobial Disk Susceptibility Tests; Approved Standard –11th Edition. CLSI Document M2- A11Vol. 29, No. 1, CLSI, Wayne, PA, January, 2012.
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing; 22nd Informational Supplement. CLSI Document M100-S22, January 2012.
| NEGGRAM
nalidixic acid tablet |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Labeler - sanofi-aventis U.S. LLC (824676584) |