CUTIVATE- fluticasone propionate ointment
PharmaDerm a division of Fougera Pharmaceuticals Inc.
----------
DESCRIPTION
CUTIVATE® (fluticasone propionate ointment) Ointment, 0.005% contains fluticasone propionate [(6α,11β,16α,17α)-6,9,-difluoro-11-hydroxy-16-methyl-3-oxo-17-(1-oxopropoxy)androsta-1,4-diene-17-carbothioic acid, S-fluoromethyl ester], a synthetic fluorinated corticosteroid, for topical dermatologic use. The topical corticosteroids constitute a class of primarily synthetic steroids used as anti-inflammatory and antipruritic agents.
Chemically, fluticasone propionate is C25H31F3O5S. It has the following structural formula:
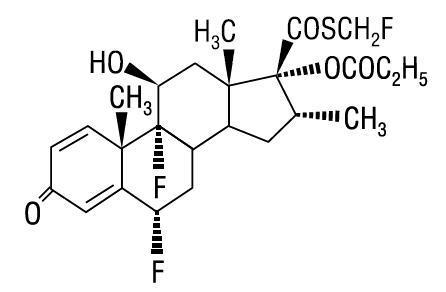
Fluticasone propionate has a molecular weight of 500.6. It is a white to off-white powder and is insoluble in water.
Each gram of CUTIVATE® Ointment contains fluticasone propionate 0.05 mg in a base of liquid paraffin, microcrystalline wax, propylene glycol, and sorbitan sesquioleate.
CLINICAL PHARMACOLOGY
Like other topical corticosteroids, fluticasone propionate has anti-inflammatory, antipruritic, and vasoconstrictive properties. The mechanism of the anti-inflammatory activity of the topical steroids, in general, is unclear. However, corticosteroids are thought to act by the induction of phospholipase A2 inhibitory proteins, collectively called lipocortins. It is postulated that these proteins control the biosynthesis of potent mediators of inflammation such as prostaglandins and leukotrienes by inhibiting the release of their common precursor, arachidonic acid. Arachidonic acid is released from membrane phospholipids by phospholipase A2.
Fluticasone propionate is lipophilic and has a strong affinity for the glucocorticoid receptor. It has weak affinity for the progesterone receptor, and virtually no affinity for the mineralocorticoid, estrogen, or androgen receptors. The therapeutic potency of glucocorticoids is related to the half-life of the glucocorticoid-receptor complex. The half-life of the fluticasone propionate-glucocorticoid receptor complex is approximately 10 hours.
Studies performed with CUTIVATE® Ointment indicate that it is in the medium range of potency as compared with other topical corticosteroids.
Pharmacokinetics:Absorption: The activity of CUTIVATE® is due to the parent drug, fluticasone propionate. The extent of percutaneous absorption of topical corticosteroids is determined by many factors, including the vehicle and the integrity of the epidermal barrier. Occlusive dressing enhances penetration. Topical corticosteroids can be absorbed from normal intact skin. Inflammation and/or other disease processes in the skin increase percutaneous absorption.
In a study of 6 healthy volunteers applying 25 g of fluticasone propionate ointment 0.005% twice daily to the trunk and legs for up to 5 days under occlusion, plasma levels of fluticasone ranged from 0.08 to 0.22 ng/mL.
In an animal study using radiolabeled 0.05% fluticasone propionate cream and ointment preparations, rats received a topical dose of 1 g/kg for a 24-hour period. Total recovery of radioactivity was approximately 80% at the end of 7 days. The majority of the dose (73%) was recovered from the surface of the application site. Less than 1% of the dose was recovered in the skin at the application site. Approximately 5% of the dose was absorbed systemically through the skin. Absorption from the skin continued for the duration of the study (7 days), indicating a long retention time at the application site.
Distribution: Following intravenous administration of 1 mg of fluticasone propionate in healthy volunteers, the initial disposition phase for fluticasone propionate was rapid and consistent with its high lipid solubility and tissue binding. The apparent volume of distribution averaged 4.2 L/kg (range, 2.3 to 16.7 L/kg). The percentage of fluticasone propionate bound to human plasma proteins averaged 91%. Fluticasone propionate is weakly and reversibly bound to erythrocytes. Fluticasone propionate is not significantly bound to human transcortin.
Metabolism: No metabolites of fluticasone propionate were detected in an in vitro study of radiolabeled fluticasone propionate incubated in a human skin homogenate. The total blood clearance of systemically absorbed fluticasone propionate averages 1,093 mL/min (range, 618 to 1,702 mL/min) after a 1-mg intravenous dose, with renal clearance accounting for less than 0.02% of the total. Fluticasone propionate is metabolized in the liver by cytochrome P450 3A4-mediated hydrolysis of the 5-fluoromethyl carbothioate grouping. This transformation occurs in 1 metabolic step to produce the inactive 17-β-carboxylic acid metabolite, the only known metabolite detected in man. This metabolite has approximately 2,000 times less affinity than the parent drug for the glucocorticoid receptor of human lung cytosol in vitro and negligible pharmacological activity in animal studies. Other metabolites detected in vitro using cultured human hepatoma cells have not been detected in man.
INDICATIONS AND USAGE
CUTIVATE® Ointment is a medium potency corticosteroid indicated for the relief of the inflammatory and pruritic manifestations of corticosteroid-responsive dermatoses in adult patients.
CONTRAINDICATIONS
CUTIVATE® Ointment is contraindicated in those patients with a history of hypersensitivity to any of the components in the preparation.
PRECAUTIONS
General: Systemic absorption of topical corticosteroids can produce reversible hypothalamic-pituitary-adrenal (HPA) axis suppression with the potential for glucocorticosteroid insufficiency after withdrawal from treatment. Manifestations of Cushing syndrome, hyperglycemia, and glucosuria can also be produced in some patients by systemic absorption of topical corticosteroids while on treatment.
Patients applying a topical steroid to a large surface area or to areas under occlusion should be evaluated periodically for evidence of HPA axis suppression. This may be done by using the ACTH stimulation, A.M. plasma cortisol, and urinary free cortisol tests.
If HPA axis suppression is noted, an attempt should be made to withdraw the drug, to reduce the frequency of application, or to substitute a less potent corticosteroid. Recovery of HPA axis function is generally prompt upon discontinuation of topical corticosteroids. Infrequently, signs and symptoms of glucocorticosteroid insufficiency may occur, requiring supplemental systemic corticosteroids. For information on systemic supplementation, see prescribing information for those products.
Pediatric patients may be more susceptible to systemic toxicity from equivalent doses due to their larger skin surface to body mass ratios (see PRECAUTIONS: Pediatric Use).
Fluticasone propionate ointment, 0.005% may cause local cutaneous adverse reactions (see ADVERSE REACTIONS).
If irritation develops, CUTIVATE® Ointment should be discontinued and appropriate therapy instituted. Allergic contact dermatitis with corticosteroids is usually diagnosed by observing failure to heal rather than noting a clinical exacerbation as with most topical products not containing corticosteroids. Such an observation should be corroborated with appropriate diagnostic patch testing.
If concomitant skin infections are present or develop, an appropriate antifungal or antibacterial agent should be used. If a favorable response does not occur promptly, use of CUTIVATE® Ointment should be discontinued until the infection has been adequately controlled.
CUTIVATE® Ointment should not be used in the treatment of preexisting skin atrophy and should not be used where infection is present at the treatment site. CUTIVATE® Ointment should not be used in the treatment of rosacea and perioral dermatitis.
Information for Patients: Patients using topical corticosteroids should receive the following information and instructions:
- This medication is to be used as directed by the physician. It is for external use only. Avoid contact with the eyes.
- This medication should not be used for any disorder other than that for which it was prescribed.
- The treated skin area should not be bandaged or otherwise covered or wrapped so as to be occlusive unless directed by the physician.
- Patients should report to their physician any signs of local adverse reactions.
- This medication should not be used on the face, underarms, or groin areas unless directed by a physician.
- As with other corticosteroids, therapy should be discontinued when control is achieved. If no improvement is seen within 2 weeks, contact the physician.
Laboratory Tests: The following tests may be helpful in evaluating patients for HPA axis suppression:
- ACTH stimulation test
- A.M. plasma cortisol test
- Urinary free cortisol test
A concentrated fluticasone propionate ointment, 0.05% (10 times that of the marketed fluticasone propionate ointment, 0.005%) suppressed 24-hour urinary free cortisol levels in 2 of 6 patients when used at a dose of 30 g/day for a week in patients with psoriasis or atopic eczema. No suppression of A.M. plasma cortisol was observed. In a second study of the same concentrated formulation of fluticasone propionate ointment, 0.05%, depression of A.M. plasma cortisol levels was noted in 2 of 8 normal volunteers when applied at doses of 50 g/day for 21 days. Morning plasma levels returned to normal levels within 4 days upon discontinuation of fluticasone propionate. In this study there was no corresponding decrease in 24-hour urinary free cortisol levels.
In a study of 35 pediatric patients treated with fluticasone propionate ointment, 0.005% for atopic dermatitis over at least 35% of body surface area, subnormal adrenal function was observed with cosyntropin stimulation testing at the end of 3 to 4 weeks of treatment in 4 patients who had normal testing prior to treatment. It is not known if these patients had recovery of adrenal function because follow-up testing was not performed (see PRECAUTIONS: Pediatric Use and ADVERSE REACTIONS). Adrenal suppression was indicated by either a 5 mcg/dL prestimulation cortisol, or a cosyntropin poststimulation cortisol ≤18 mcg/dL, and/or an increase of <7 mcg/dL from the baseline cortisol level.
Carcinogenesis, Mutagenesis, and Impairment of Fertility: Two 18-month studies were performed in mice to evaluate the carcinogenic potential of fluticasone propionate when given topically (as a 0.05% ointment) and orally. No evidence of carcinogenicity was found in either study.
Fluticasone propionate was not mutagenic in the standard Ames test, E. coli fluctuation test, S. cerevisiae gene conversion test, or Chinese Hamster ovarian cell assay. It was not clastogenic in mouse micronucleus or cultured human lymphocyte tests.
In a fertility and general reproductive performance study in rats, fluticasone propionate administered subcutaneously to females at up to 50 mcg/kg/day and to males at up to 100 mcg/kg/day (later reduced to 50 mcg/kg/day) had no effect upon mating performance or fertility. These doses are approximately 150 and 300 times, respectively, the human systemic exposure following use of the recommended human topical dose of fluticasone propionate ointment, 0.005%, assuming human percutaneous absorption of approximately 3% and the use in a 70-kg person of 15 g/day.
Pregnancy:Teratogenic Effects: Pregnancy Category C. Corticosteroids have been shown to be teratogenic in laboratory animals when administered systemically at relatively low dosage levels. Some corticosteroids have been shown to be teratogenic after dermal application in laboratory animals. Teratology studies in the mouse demonstrated fluticasone propionate to be teratogenic (cleft palate) when administered subcutaneously in doses of 45 mcg/kg/day and 150 mcg/kg/day. This dose is approximately 140 and 450 times, respectively, the human topical dose of fluticasone propionate ointment, 0.005%. There are no adequate and well-controlled studies in pregnant women. CUTIVATE® Ointment should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Nursing Mothers: Systemically administered corticosteroids appear in human milk and could suppress growth, interfere with endogenous corticosteroid production, or cause other untoward effects. It is not known whether topical administration of corticosteroids could result in sufficient systemic absorption to produce detectable quantities in human milk. Because many drugs are excreted in human milk, caution should be exercised when CUTIVATE® Ointment is administered to a nursing woman.
Pediatric Use: Use of CUTIVATE® Ointment in pediatric patients is not recommended.
In a study of 35 pediatric patients treated with fluticasone propionate ointment, 0.005% for atopic dermatitis over at least 35% of body surface area, subnormal adrenal function was observed with cosyntropin stimulation testing at the end of 3 to 4 weeks of treatment in 4 patients who had normal testing prior to treatment. It is not known if these patients had recovery of adrenal function because follow-up testing was not performed (see PRECAUTIONS: Laboratory Tests and ADVERSE REACTIONS). The decreased responsiveness to cosyntropin testing was not correlated to age of patient, amount of fluticasone propionate ointment used, or serum levels of fluticasone propionate. Plasma fluticasone propionate were not performed in a 6-month-old patient who demonstrated an abnormal response to cosyntropin stimulation testing.
Pediatric patients may demonstrate greater susceptibility to topical corticosteroid-induced HPA axis suppression and Cushing syndrome than mature patients because of a larger skin surface to body weight ratio.
HPA axis suppression, Cushing syndrome, linear growth retardation, delayed weight gain, and intracranial hypertension have been reported in pediatric patients receiving topical corticosteroids. Manifestations of adrenal suppression in pediatric patients include low plasma cortisol levels and an absence of response to ACTH stimulation.
Manifestations of intracranial hypertension include bulging fontanelles, headaches, and bilateral papilledema.
Geriatric Use: A limited number of patients above 65 years of age (n = 203) have been treated with CUTIVATE® Ointment in US and non-US clinical trials. While the number of patients is too small to permit separate analysis of efficacy and safety, the adverse reactions reported in this population were similar to those reported by younger patients. Based on available data, no adjustment of dosage of CUTIVATE® in geriatric patients is warranted.
ADVERSE REACTIONS
In controlled clinical trials, the total incidence of adverse reactions associated with the use of CUTIVATE® Ointment was approximately 4%. These adverse reactions were usually mild, self-limiting, and consisted primarily of pruritus, burning, hypertrichosis, increased erythema, hives, irritation, and lightheadedness. Each of these events occurred individually in less than 1% of patients.
In a study of 35 pediatric patients treated with fluticasone propionate ointment, 0.005% for atopic dermatitis over at least 35% of body surface area, subnormal adrenal function was observed with cosyntropin stimulation testing at the end of 3 to 4 weeks of treatment in 4 patients who had normal testing prior to treatment. It is not known if these patients had recovery of adrenal function because follow-up testing was not performed (see PRECAUTIONS: Laboratory Tests and PRECAUTIONS: Pediatric Use). Telangiectasia on the face was noted in 1 patient on the eighth day of a 4-week treatment period. Facial use was discontinued and the telangiectasia resolved.
The following additional local adverse reactions have been reported infrequently with topical corticosteroids, including fluticasone propionate, and they may occur more frequently with the use of occlusive dressings and higher potency corticosteroids. These reactions are listed in an approximately decreasing order of occurrence: dryness, folliculitis, acneiform eruptions, hypopigmentation, perioral dermatitis, allergic contact dermatitis, secondary infection, skin atrophy, striae, and miliaria. Also, there are reports of the development of pustular psoriasis from chronic plaque psoriasis following reduction or discontinuation of potent topical corticosteroid products.
OVERDOSAGE
Topically applied CUTIVATE® Ointment can be absorbed in sufficient amounts to produce systemic effects (see PRECAUTIONS).
DOSAGE AND ADMINISTRATION
Apply a thin film of CUTIVATE® Ointment to the affected skin areas twice daily. Rub in gently.
CUTIVATE® Ointment should not be used with occlusive dressings.
HOW SUPPLIED
CUTIVATE® (fluticasone propionate ointment) Ointment, 0.005% is supplied in:
- 15-g tubes (NDC 0462-0333-15),
- 30-g tubes (NDC 0462-0333-30), and
- 60-g tubes (NDC 0462-0333-60).
Store between 2°and 30°C (36°and 86°F).
PharmaDerm®
A division of Nycomed US Inc.
Melville, NY 11747 USA
www.pharmaderm.com
I8333B
R6/08
#144

| CUTIVATE
fluticasone propionate ointment |
||||||||||||||||
|
||||||||||||||||
|
||||||||||||||||
|
||||||||||||||||
|
||||||||||||||||
|
||||||||||||||||
| Labeler - PharmaDerm a division of Fougera Pharmaceuticals Inc. (043838424) |