Label: OPSUMIT- macitentan tablet, film coated

- NDC Code(s): 66215-501-15, 66215-501-30
- Packager: Actelion Pharmaceuticals US, Inc.
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: New Drug Application
Drug Label Information
Updated April 2, 2024
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Medication Guide: HTML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use OPSUMIT safely and effectively. See full prescribing information for OPSUMIT.
OPSUMIT ®(macitentan) tablets, for oral use
Initial U.S. Approval: 2013WARNING: EMBRYO-FETAL TOXICITY
See full prescribing information for complete boxed warning.- Do not administer OPSUMIT to a pregnant female because it may cause fetal harm ( 4.1, 5.1, 8.1).
- Females of reproductive potential: exclude pregnancy before start of treatment, monthly during treatment, and 1 month after stopping treatment. Prevent pregnancy during treatment and for one month after treatment by using acceptable methods of contraception ( 2.2, 8.3).
- For all female patients, OPSUMIT is available only through a restricted program called the Macitentan- Containing Products Risk Evaluation and Mitigation Strategy (REMS) ( 5.2).
INDICATIONS AND USAGE
OPSUMIT is an endothelin receptor antagonist (ERA) indicated for the treatment of pulmonary arterial hypertension (PAH, WHO Group I) to reduce the risks of disease progression and hospitalization for PAH ( 1.1).
DOSAGE AND ADMINISTRATION
- 10 mg once daily .Doses higher than 10 mg once daily have not been studied in patients with PAH and are not recommended ( 2.1).
DOSAGE FORMS AND STRENGTHS
- Tablet: 10 mg ( 3)
WARNINGS AND PRECAUTIONS
- ERAs cause hepatotoxicity and liver failure. Obtain baseline liver enzymes and monitor as clinically indicated ( 5.3).
- Fluid retention may require intervention ( 5.4)
- Decreases in hemoglobin ( 5.5).
- Pulmonary edema in patients with pulmonary veno-occlusive disease. If confirmed, discontinue treatment ( 5.6).
- Decreases in sperm count have been observed in patients taking ERAs ( 5.7).
ADVERSE REACTIONS
Most common adverse reactions (more frequent than placebo by ≥3%) are anemia, nasopharyngitis/pharyngitis, bronchitis, headache, influenza, and urinary tract infection ( 6.1).
To report SUSPECTED ADVERSE REACTIONS, contact Janssen at 1-800-526-7736 (1-800-JANSSEN) or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
- Strong CYP3A4 inducers (rifampin) reduce exposure to macitentan: avoid co-administration with OPSUMIT ( 7.1, 12.3).
- Strong CYP3A4 inhibitors (ketoconazole, ritonavir) increase exposure to macitentan: avoid co-administration with OPSUMIT ( 7.2, 12.3) .
- Moderate dual CYP3A4 and CYP2C9 inhibitors (fluconazole, amiodarone) or use of combined CYP3A4 and CYP2C9 inhibitors may increase exposure to macitentan: avoid co-administration with OPSUMIT ( 7.3, 12.3).
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 3/2024
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: EMBRYO-FETAL TOXICITY
1 INDICATIONS AND USAGE
1.1 Pulmonary Arterial Hypertension
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage
2.2 Pregnancy Testing in Females of Reproductive Potential
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
4.1 Pregnancy
4.2 Hypersensitivity
5 WARNINGS AND PRECAUTIONS
5.1 Embryo-fetal Toxicity
5.2 Macitentan-Containing Products REMS
5.3 Hepatotoxicity
5.4 Fluid Retention
5.5 Hemoglobin Decrease
5.6 Pulmonary Edema with Pulmonary Veno-occlusive Disease (PVOD)
5.7 Decreased Sperm Counts
6 ADVERSE REACTIONS
6.1 Clinical Trial Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
7.1 Strong CYP3A4 Inducers
7.2 Strong CYP3A4 Inhibitors
7.3 Moderate Dual or Combined CYP3A4 and CYP2C9 Inhibitors
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
13.2 Animal Toxicology
14 CLINICAL STUDIES
14.1 Pulmonary Arterial Hypertension
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
BOXED WARNING
(What is this?)
WARNING: EMBRYO-FETAL TOXICITY
- Do not administer OPSUMIT to a pregnant female because it may cause fetal harm [see Contraindications (4.1), Warnings and Precautions (5.1), Use in Specific Populations (8.1)].
- Females of reproductive potential: Exclude pregnancy before the start of treatment, monthly during treatment, and 1 month after stopping treatment. Prevent pregnancy during treatment and for one month after stopping treatment by using acceptable methods of contraception [see Pregnancy Testing in Females of Reproductive Potential (2.2), Use in Specific Populations (8.3)].
- For all female patients, OPSUMIT is available only through a restricted program called the Macitentan-Containing Products Risk Evaluation and Mitigation Strategy (REMS) [see Warnings and Precautions (5.2)] .
-
1 INDICATIONS AND USAGE
1.1 Pulmonary Arterial Hypertension
OPSUMIT is an endothelin receptor antagonist (ERA) indicated for the treatment of pulmonary arterial hypertension (PAH, WHO Group I) to reduce the risks of disease progression and hospitalization for PAH.
Effectiveness was established in a long-term study in PAH patients with predominantly WHO Functional Class II–III symptoms treated for an average of 2 years. Patients had idiopathic and heritable PAH (57%), PAH caused by connective tissue disorders (31%), and PAH caused by congenital heart disease with repaired shunts (8%) [see Clinical Studies (14.1)] .
-
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage
The recommended dosage of OPSUMIT is 10 mg once daily for oral administration. Doses higher than 10 mg once daily have not been studied in patients with PAH and are not recommended.
2.2 Pregnancy Testing in Females of Reproductive Potential
Obtain a pregnancy test in females of reproductive potential prior to OPSUMIT treatment, monthly during treatment and one month after stopping OPSUMIT. Initiate treatment with OPSUMIT in females of reproductive potential only after a negative pregnancy test. [see Boxed Warning, Contraindications (4.1), Warnings and Precautions (5.1), and Use in Specific Populations (8.3)] .
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
4.1 Pregnancy
OPSUMIT may cause fetal harm when administered to a pregnant woman. OPSUMIT is contraindicated in females who are pregnant. OPSUMIT was consistently shown to have teratogenic effects when administered to animals. If OPSUMIT is used during pregnancy, advise the patient of the potential risk to a fetus [see Warnings and Precautions (5.1) and Use in Specific Populations (8.1)] .
4.2 Hypersensitivity
OPSUMIT is contraindicated in patients with a history of a hypersensitivity reaction to macitentan or any component of the product [see Adverse Reactions (6.2)] .
-
5 WARNINGS AND PRECAUTIONS
5.1 Embryo-fetal Toxicity
OPSUMIT may cause fetal harm when administered during pregnancy and is contraindicated for use in females who are pregnant. In females of reproductive potential, exclude pregnancy prior to initiation of therapy, ensure use of acceptable contraceptive methods and obtain monthly pregnancy tests [see Dosage and Administration (2.2)and Use in Specific Populations (8.1, 8.3)] .
OPSUMIT is available for females through the Macitentan-Containing Products REMS, a restricted distribution program [see Warnings and Precautions (5.2)] .
5.2 Macitentan-Containing Products REMS
For all females, OPSUMIT is available only through a restricted program called the Macitentan-Containing Products REMS, because of the risk of embryo-fetal toxicity [see Contraindications (4.1), Warnings and Precautions (5.1), and Use in Specific Populations (8.1, 8.3)] .
Notable requirements of the Macitentan-Containing Products REMS include the following:
- Prescribers must be certified with the Macitentan-Containing Products REMS by enrolling and completing training.
- All females, regardless of reproductive potential, must enroll in the Macitentan-Containing Products REMS prior to initiating OPSUMIT. Male patients are not enrolled in the REMS.
- Females of reproductive potential must comply with the pregnancy testing and contraception requirements [see Use in Specific Populations (8.3)] .
- Pharmacies must be certified with the Macitentan-Containing Products REMS and must only dispense to patients who are authorized to receive OPSUMIT.
Further information is available at www.MacitentanREMS.com or 1-888-572-2934. Information on Macitentan-Containing Products REMS certified pharmacies or wholesale distributors is available at 1-888-572-2934.
5.3 Hepatotoxicity
ERAs have caused elevations of aminotransferases, hepatotoxicity, and liver failure. The incidence of elevated aminotransferases in the study of OPSUMIT in PAH is shown in Table 1.
Table 1: Incidence of Elevated Aminotransferases in the SERAPHIN Study OPSUMIT 10 mg
(N=242)Placebo
(N=249)>3 × ULN 3.4% 4.5% >8 × ULN 2.1% 0.4% In the placebo-controlled study of OPSUMIT, discontinuations for hepatic adverse events were 3.3% in the OPSUMIT 10 mg group vs. 1.6% for placebo.
Obtain liver enzyme tests prior to initiation of OPSUMIT and repeat during treatment as clinically indicated [see Adverse Reactions (6.2)] .
Advise patients to report symptoms suggesting hepatic injury (nausea, vomiting, right upper quadrant pain, fatigue, anorexia, jaundice, dark urine, fever, or itching). If clinically relevant aminotransferase elevations occur, or if elevations are accompanied by an increase in bilirubin >2 × ULN, or by clinical symptoms of hepatotoxicity, discontinue OPSUMIT. Consider re-initiation of OPSUMIT when hepatic enzyme levels normalize in patients who have not experienced clinical symptoms of hepatotoxicity.
5.4 Fluid Retention
Peripheral edema and fluid retention are known clinical consequences of PAH and known effects of ERAs. In the placebo-controlled study of OPSUMIT in PAH, the incidence of edema was 21.9% in the OPSUMIT 10 mg group and 20.5% in the placebo group.
Patients with underlying left ventricular dysfunction may be at particular risk for developing significant fluid retention after initiation of ERA treatment. In a small study of OPSUMIT in patients with pulmonary hypertension because of left ventricular dysfunction, more patients in the OPSUMIT group developed significant fluid retention and had more hospitalizations because of worsening heart failure compared to those randomized to placebo. Postmarketing cases of edema and fluid retention occurring within weeks of starting OPSUMIT, some requiring intervention with a diuretic or hospitalization for decompensated heart failure, have been reported [see Adverse Reactions (6.2)] .
Monitor for signs of fluid retention after OPSUMIT initiation. If clinically significant fluid retention develops, evaluate the patient to determine the cause, such as OPSUMIT or underlying heart failure, and the possible need to discontinue OPSUMIT.
5.5 Hemoglobin Decrease
Decreases in hemoglobin concentration and hematocrit have occurred following administration of other ERAs and were observed in clinical studies with OPSUMIT. These decreases occurred early and stabilized thereafter. In the placebo-controlled study of OPSUMIT in PAH, OPSUMIT 10 mg caused a mean decrease in hemoglobin from baseline to up to 18 months of about 1.0 g/dL compared to no change in the placebo group. A decrease in hemoglobin to below 10.0 g/dL was reported in 8.7% of the OPSUMIT 10 mg group and in 3.4% of the placebo group. Decreases in hemoglobin seldom require transfusion. Initiation of OPSUMIT is not recommended in patients with severe anemia. Measure hemoglobin prior to initiation of treatment and repeat during treatment as clinically indicated [see Adverse Reactions (6.1)] .
5.6 Pulmonary Edema with Pulmonary Veno-occlusive Disease (PVOD)
Should signs of pulmonary edema occur, consider the possibility of associated PVOD. If confirmed, discontinue OPSUMIT.
5.7 Decreased Sperm Counts
OPSUMIT, like other ERAs, may have an adverse effect on spermatogenesis. Counsel men about potential effects on fertility [see Use in Specific Populations (8.3) and Nonclinical Toxicology (13.1)] .
-
6 ADVERSE REACTIONS
Clinically significant adverse reactions that appear in other sections of the labeling include:
- Embryo-fetal Toxicity [see Warnings and Precautions (5.1)]
- Hepatotoxicity [see Warnings and Precautions (5.3)]
- Fluid Retention [see Warnings and Precautions (5.4)]
- Decrease in Hemoglobin [see Warnings and Precautions (5.5)]
6.1 Clinical Trial Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
Safety data for OPSUMIT were obtained primarily from one placebo-controlled clinical study in 742 patients with PAH (SERAPHIN study) [see Clinical Studies (14)].
The exposure to OPSUMIT in this trial was up to 3.6 years with a median exposure of about 2 years (N=542 for 1 year; N=429 for 2 years; and N=98 for more than 3 years). The overall incidence of treatment discontinuations because of adverse events was similar across OPSUMIT 10 mg and placebo treatment groups (approximately 11%).
Table 2 presents adverse reactions more frequent on OPSUMIT than on placebo by ≥3%.
Table 2: Adverse Reactions Adverse Reaction OPSUMIT 10 mg
(N=242)
(%)Placebo
(N=249)
(%)Anemia 13 3 Nasopharyngitis/pharyngitis 20 13 Bronchitis 12 6 Headache 14 9 Influenza 6 2 Urinary tract infection 9 6 6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of OPSUMIT. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Immune system disorders:hypersensitivity reactions (angioedema, pruritus and rash)
Vascular disorders: flushing
Respiratory, thoracic and mediastinal disorders: nasal congestion
Gastrointestinal disorders: Elevations of liver aminotransferases (ALT, AST) and liver injury have been reported with OPSUMIT use; in most cases alternative causes could be identified (heart failure, hepatic congestion, autoimmune hepatitis). Endothelin receptor antagonists have been associated with elevations of aminotransferases, hepatotoxicity, and cases of liver failure [see Warnings and Precautions (5.3)] .
General disorders and administration site conditions:edema/fluid retention. Cases of edema and fluid retention occurred within weeks of starting OPSUMIT, some requiring intervention with a diuretic, fluid management or hospitalization for decompensated heart failure. [see Warnings and Precautions (5.4)].
Cardiac disorders: symptomatic hypotension
-
7 DRUG INTERACTIONS
7.1 Strong CYP3A4 Inducers
Strong inducers of CYP3A4 such as rifampin significantly reduce macitentan exposure. Concomitant use of OPSUMIT with strong CYP3A4 inducers should be avoided [see Clinical Pharmacology (12.3)] .
7.2 Strong CYP3A4 Inhibitors
Concomitant use of strong CYP3A4 inhibitors like ketoconazole approximately double macitentan exposure. Many HIV drugs like ritonavir are strong inhibitors of CYP3A4. Avoid concomitant use of OPSUMIT with strong CYP3A4 inhibitors [see Clinical Pharmacology (12.3)] . Use other PAH treatment options when strong CYP3A4 inhibitors are needed as part of HIV treatment [see Clinical Pharmacology (12.3)] .
7.3 Moderate Dual or Combined CYP3A4 and CYP2C9 Inhibitors
Concomitant use of moderate dual inhibitors of CYP3A4 and CYP2C9 such as fluconazole is predicted to increase macitentan exposure approximately 4-fold based on physiologically based pharmacokinetic (PBPK) modelling. Avoid concomitant use of OPSUMIT with moderate dual inhibitors of CYP3A4 and CYP2C9 (such as fluconazole and amiodarone) [see Clinical Pharmacology (12.3)] .
Concomitant treatment of both a moderate CYP3A4 inhibitor and moderate CYP2C9 inhibitor with OPSUMIT should also be avoided [see Clinical Pharmacology (12.3)].
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Based on data from animal reproduction studies, OPSUMIT may cause embryo-fetal toxicity, including birth defects and fetal death, when administered to a pregnant female and is contraindicated during pregnancy. There are risks to the mother and the fetus associated with pulmonary arterial hypertension in pregnancy [see Clinical Considerations] . There are limited data on OPSUMIT use in pregnant women. Macitentan was teratogenic in rabbits and rats at all doses tested. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, advise the patient of the risk to a fetus [see Contraindications (4.1)] .
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2–4% and 15–20%, respectively.
8.3 Females and Males of Reproductive Potential
Pregnancy Testing
Verify the pregnancy status of females of reproductive potential prior to initiating OPSUMIT, monthly during treatment and one month after stopping treatment with OPSUMIT. The patient should contact her physician immediately for pregnancy testing if onset of menses is delayed or pregnancy is suspected. If the pregnancy test is positive, the physician and patient must discuss the risks to her, the pregnancy, and the fetus [see Warnings and Precautions (5.1), and Dosage and Administration (2.2) and Contraindication (4.1)] .
Contraception
Female patients of reproductive potential must use acceptable methods of contraception during treatment with OPSUMIT and for 1 month after treatment with OPSUMIT. Patients may choose one highly effective form of contraception (intrauterine devices (IUD), contraceptive implants or tubal sterilization) or a combination of methods (hormone method with a barrier method or two barrier methods). If a partner's vasectomy is the chosen method of contraception, a hormone or barrier method must be used along with this method. Counsel patients on pregnancy planning and prevention, including emergency contraception, or designate counseling by another healthcare provider trained in contraceptive counseling [see Warnings and Precautions (5.1)] .
Infertility
Based on findings in animals, OPSUMIT may impair fertility in males of reproductive potential. It is not known whether effects on fertility would be reversible [see Warnings and Precautions (5.7), Adverse Reactions (6.1) and Nonclinical Toxicology (13.1)] .
-
10 OVERDOSAGE
OPSUMIT has been administered as a single dose of up to and including 600 mg to healthy subjects (60 times the approved dosage). Adverse reactions of headache, nausea and vomiting were observed. In the event of an overdose, standard supportive measures should be taken, as required. Dialysis is unlikely to be effective because macitentan is highly protein-bound.
-
11 DESCRIPTION
OPSUMIT ® (macitentan) is an endothelin receptor antagonist. The chemical name of macitentan is N-[5-(4-Bromophenyl)-6-[2-[(5-bromo-2-pyrimidinyl)oxy]ethoxy]-4-pyrimidinyl]-N'-propylsulfamide. It has a molecular formula of C 19H 20Br 2N 6O 4S and a molecular weight of 588.27. Macitentan is achiral and has the following structural formula:
Macitentan is a crystalline powder that is insoluble in water. In the solid state macitentan is very stable, is not hygroscopic, and is not light sensitive.
OPSUMIT is available as a 10 mg film-coated tablet for once daily oral administration. The tablets include the following inactive ingredients: lactose monohydrate, magnesium stearate, microcrystalline cellulose, polysorbate 80, povidone, and sodium starch glycolate Type A. The tablets are film-coated with a coating material containing polyvinyl alcohol, soya lecithin, talc, titanium dioxide, and xanthan gum.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Endothelin (ET)-1 and its receptors (ET A and ET B) mediate a variety of deleterious effects, such as vasoconstriction, fibrosis, proliferation, hypertrophy, and inflammation. In disease conditions such as PAH, the local ET system is upregulated and is involved in vascular hypertrophy and in organ damage.
Macitentan is an endothelin receptor antagonist that inhibits the binding of ET-1 to both ET A and ET B receptors. Macitentan displays high affinity and sustained occupancy of the ET receptors in human pulmonary arterial smooth muscle cells. One of the metabolites of macitentan is also pharmacologically active at the ET receptors and is estimated to be about 20% as potent as the parent drug in vitro. The clinical impact of dual endothelin blockage is unknown.
12.2 Pharmacodynamics
Pulmonary Hemodynamics
The clinical efficacy study in patients with pulmonary arterial hypertension assessed hemodynamic parameters in a subset of patients after 6 months of treatment. Patients treated with OPSUMIT 10 mg (N=57) achieved a median reduction of 37% (95% CI 22–49) in pulmonary vascular resistance and an increase of 0.6 L/min/m 2(95% CI 0.3–0.9) in cardiac index compared to placebo (N=67).
12.3 Pharmacokinetics
The pharmacokinetics of macitentan and its active metabolite have been studied primarily in healthy subjects. The pharmacokinetics of macitentan are dose proportional over a range from 1 mg to 30 mg after once daily administration.
A cross study comparison shows that the exposures to macitentan and its active metabolite in patients with PAH are similar to those observed in healthy subjects.
Absorption and Distribution
The maximum plasma concentration of macitentan is achieved about 8 hours after oral administration. The absolute bioavailability after oral administration is not known. In a study in healthy subjects, the exposure to macitentan and its active metabolite were unchanged after a high fat breakfast. Macitentan may therefore be taken with or without food.
Macitentan and its active metabolite are highly bound to plasma proteins (>99%), primarily to albumin and to a lesser extent to alpha-1-acid glycoprotein. The apparent volumes of distribution (Vss/F) of macitentan and its active metabolite were about 50 L and 40 L respectively in healthy subjects.
Metabolism and Elimination
Following oral administration, the apparent elimination half-lives of macitentan and its active metabolite are approximately 16 hours and 48 hours, respectively. Macitentan is metabolized primarily by oxidative depropylation of the sulfamide to form the pharmacologically active metabolite. This reaction is dependent on the cytochrome P450 (CYP) system, mainly CYP3A4 with minor contributions of CYP2C8, CYP2C9, and CYP2C19. At steady state in PAH patients, the systemic exposure to the active metabolite is 3-times the exposure to macitentan and is expected to contribute approximately 40% of the total pharmacologic activity. In a study in healthy subjects with radiolabeled macitentan, approximately 50% of radioactive drug material was eliminated in urine but none was in the form of unchanged drug or the active metabolite. About 24% of the radioactive drug material was recovered from feces.
Special Populations
There are no clinically relevant effects of age, sex, or race on the pharmacokinetics of macitentan and its active metabolite.
Renal Impairment
Exposure to macitentan and its active metabolite in patients with severe renal impairment (CrCl 15–29 mL/min) compared to healthy subjects was increased by 30% and 60%, respectively. This increase is not considered clinically relevant.
Hepatic Impairment
Exposure to macitentan was decreased by 21%, 34%, and 6% and exposure to the active metabolite was decreased by 20%, 25%, and 25% in subjects with mild, moderate, or severe hepatic impairment (Child-Pugh Class A, B, and C), respectively. This decrease is not considered clinically relevant.
Drug Interactions
In Vitro Studies
At plasma levels obtained with dosing at 10 mg once daily, macitentan has no relevant inhibitory or inducing effects on CYP enzymes. Macitentan is not a substrate or inhibitor of multi-drug resistance protein (P-gp, MDR-1). The active metabolite of macitentan also is not an inhibitor of P-gp/MDR-1 at clinically relevant concentrations.
Macitentan and its active metabolite are not expected to have significant interaction with drug transporters such as organic anion transporting polypeptide (OATP1B1, OATP1B3), multidrug and toxin extrusion protein (MATE-1, MATE-2K), bile salt export pump (BSEP), sodium-taurocholate co-transporting polypeptide (NTCP), organic cation transporter (OCT-1, OCT-3), organic anion transporter (OAT-1, OAT-3) or BCRP transporter at clinically relevant plasma concentrations.
In Vivo Studies
Effect of other drugs on macitentan
The effect of other drugs on macitentan and its active metabolite are studied in healthy subjects and are shown in Figure 1 below.
Figure 1
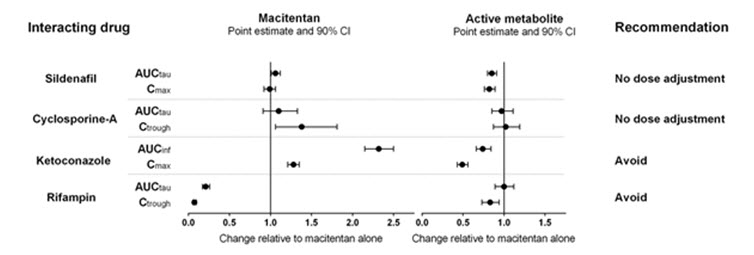
Effects of other strong CYP3A4 inhibitors such as ritonavir on macitentan were not studied, but are likely to result in an increase in macitentan exposure at steady state similar to that seen with ketoconazole [see Drug Interactions (7.2)] .
PBPK modeling and simulations based analysis showed that a moderate dual inhibitor of CYP3A4 and CYP2C9 such as fluconazole (400 mg once daily) is predicted to increase macitentan exposure approximately 4-fold without relevant effect on the exposure to its active metabolite [see Drug Interactions (7.3)] .
Effect of macitentan on other drugs
Warfarin: Macitentan once daily dosing did not alter the exposure to R- and S-warfarin or their effect on international normalized ratio (INR).
Sildenafil: At steady-state, the exposure to sildenafil 20 mg t.i.d. increased by 15% during concomitant administration of macitentan 10 mg once daily. This change is not considered clinically relevant.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Carcinogenicity studies of 2 years' duration did not reveal any carcinogenic potential at exposures 75-fold and 140-fold the human exposure (based on AUC) in male and female mice, respectively, and 8.3- and 42-fold in male and female rats, respectively.
Mutagenesis
Macitentan was not genotoxic in a standard battery of in vitro and in vivo assays that included a bacterial reverse mutation assay, an assay for gene mutations in mouse lymphoma cells, a chromosome aberration test in human lymphocytes, and an in vivo micronucleus test in rats.
Impairment of Fertility
Treatment of juvenile rats from postnatal Day 4 to Day 114 led to reduced body weight gain and testicular tubular atrophy at exposures 7-fold the human exposure. Fertility was not affected.
Reversible testicular tubular dilatation was observed in chronic toxicity studies at exposures greater than 7-fold and 23-fold the human exposure in rats and dogs, respectively. After 2 years of treatment, tubular atrophy was seen in rats at 4-fold the human exposure. Macitentan did not affect male or female fertility at exposures ranging from 19- to 44-fold the human exposure, respectively, and had no effect on sperm count, motility, and morphology in male rats. No testicular findings were noted in mice after treatment up to 2 years.
13.2 Animal Toxicology
In dogs, macitentan decreased blood pressure at exposures similar to the therapeutic human exposure. Intimal thickening of coronary arteries was observed at 17-fold the human exposure after 4 to 39 weeks of treatment. Due to the species-specific sensitivity and the safety margin, this finding is considered not relevant for humans.
There were no adverse liver findings in long-term studies conducted in mice, rats, and dogs at exposures of 12- to 116-fold the human exposure.
-
14 CLINICAL STUDIES
14.1 Pulmonary Arterial Hypertension
The effect of macitentan on progression of PAH was demonstrated in a multi-center, long-term (average duration of exposure approximately 2 years), placebo-controlled study in 742 patients with symptomatic [WHO functional class (FC) II–IV] PAH who were randomized to placebo (n=250), 3 mg macitentan (n=250), or 10 mg macitentan (n=242) once daily. Patients were treated with OPSUMIT monotherapy or in combination with phosphodiesterase-5 inhibitors or inhaled prostanoids.
The primary study endpoint was time to the first occurrence of death, a significant morbidity event, defined as atrial septostomy, lung transplantation, initiation of IV or subcutaneous (SC) prostanoids, or "other worsening of PAH" during double-blind treatment plus 7 days. Other worsening was defined as all of the following: 1) a sustained ≥15% decrease from baseline in 6 minute walk distance (6MWD), 2) worsening of PAH symptoms (worsening of WHO FC), and 3) need for additional treatment for PAH. All of these other worsening events were confirmed by an independent adjudication committee, blinded to treatment allocation. A critical secondary endpoint was time to PAH death or PAH hospitalization.
The mean patient age was 46 years (14% were age 65 or above). Most patients were white (55%) or Asian (29%) and female (77%). Approximately 52%, 46%, and 2% of patients were in WHO FC II, III, and IV, respectively.
Idiopathic or heritable PAH was the most common etiology in the study population (57%) followed by PAH caused by connective tissue disorders (31%), PAH caused by congenital heart disease with repaired shunts (8%), and PAH caused by other etiologies [drugs and toxins (3%) and HIV (1%)].
At baseline, the majority of enrolled patients (64%) were being treated with a stable dose of specific therapy for PAH, either oral phosphodiesterase inhibitors (61%) and/or inhaled/oral prostanoids (6%).
Study results are described for the placebo and OPSUMIT 10 mg groups. The median treatment durations were 101 and 118 weeks in the placebo and OPSUMIT 10 mg groups, respectively, up to a maximum of 188 weeks.
Treatment with OPSUMIT 10 mg resulted in a 45% reduction (HR 0.55, 97.5% CI 0.39–0.76; logrank p<0.0001) in the occurrence of the primary endpoint up to end of double-blind treatment compared to placebo (Table 3 and Figure 2). The beneficial effect of OPSUMIT 10 mg was primarily attributable to a reduction in clinical worsening events (deterioration in 6MWD and worsening of PAH symptoms and need for additional PAH treatment).
Figure 2 Kaplan-Meier Estimates of the Occurrence of the Primary Endpoint Event in the SERAPHIN Study
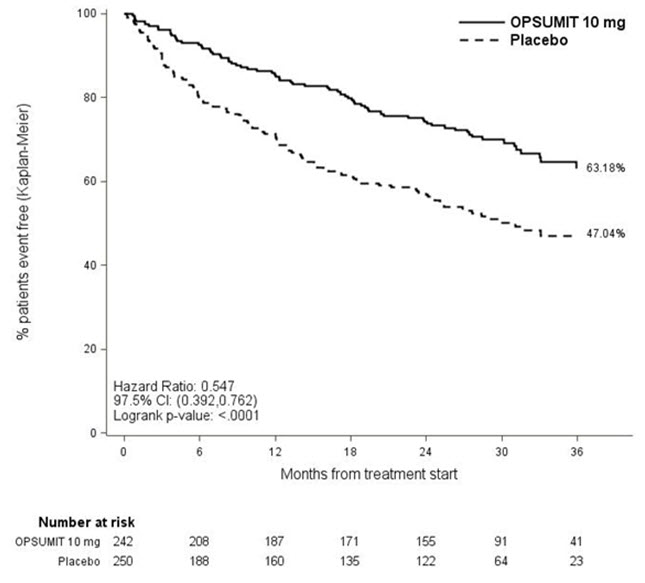
Table 3: Summary of Primary Endpoint Events Placebo
N=250
n (%)OPSUMIT 10 mg
N=242
n (%)- *
- No patients experienced an event of lung transplantation or atrial septostomy in the placebo or OPSUMIT 10 mg treatment groups.
Patients with a primary endpoint event * 116 (46.4) 76 (31.4) Component as first event Worsening PAH 93 (37.2) 59 (24.4) Death 17 (6.8) 16 (6.6) IV/SC prostanoid 6 (2.4) 1 (0.4) Subgroup analyses were performed to examine their influence on outcome as shown in Figure 3. Consistent efficacy of OPSUMIT 10 mg on the primary endpoint was seen across subgroups of age, sex, race, etiology, by monotherapy or in combination with another PAH therapy, baseline 6MWD, and baseline WHO FC.
Figure 3 Subgroup Analysis of the SERAPHIN Study
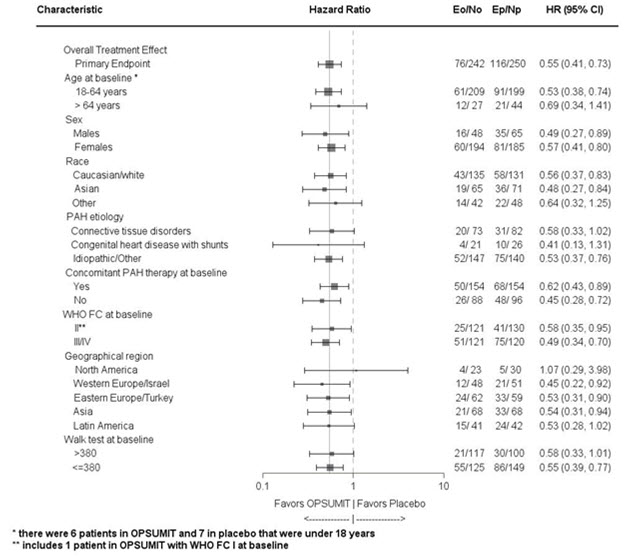
Eo = Number of events OPSUMIT 10 mg; No = Number of patients randomized to OPSUMIT 10 mg
Ep = Number of events placebo; Np = Number of patients randomized to placeboPAH related death or hospitalization for PAH was assessed as a secondary endpoint. The risk of PAH related death or hospitalization for PAH was reduced by 50% in patients receiving OPSUMIT 10 mg compared to placebo (HR 0.50, 97.5% CI 0.34–0.75; logrank p<0.0001) (Table 4 and Figure 4).
Figure 4 Kaplan-Meier Estimates of the Occurrence of Death due to PAH or Hospitalization for PAH in SERAPHIN
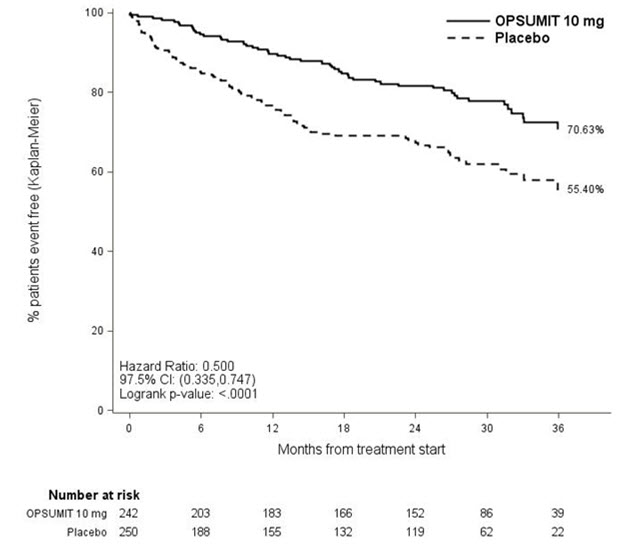
Table 4: Summary of Death due to PAH and Hospitalization due to PAH Placebo
(N=250)
n (%)OPSUMIT 10 mg
(N=242)
n (%)Death due to PAH or hospitalization for PAH 84 (33.6) 50 (20.7) Component as first event Death due to PAH 5 (2.0) 5 (2.1) Hospitalization for PAH 79 (31.6) 45 (18.6) Treatment with OPSUMIT 10 mg resulted in a placebo-corrected mean increase in 6MWD of 22 meters at Month 6 (97.5% CI 3–41; p=0.0078), with significant improvement in 6MWD by Month 3. 6MWD increased more in patients with worse baseline WHO Functional Class (37 meters and 12 meters placebo-corrected mean increase in WHO FC III/IV and FC I/II, respectively). The increase in 6MWD achieved with OPSUMIT was maintained for the duration of the study.
Treatment with OPSUMIT 10 mg led to an improvement of at least one WHO Functional Class at Month 6 in 22% of patients compared to 13% of patients treated with placebo.
Long-Term Treatment of PAH
In long-term follow-up of patients who were treated with OPSUMIT 10 mg in the placebo-controlled study (N=242) and the open-label extension study, Kaplan-Meier estimates of survival at 1, 2, 5, and 7 years were 95%, 89%, 73%, and 63% respectively. The median exposure to OPSUMIT was 4.6 years. These uncontrolled observations do not allow comparison with a group not given OPSUMIT and cannot be used to determine the long term-effect of OPSUMIT on mortality.
- 16 HOW SUPPLIED/STORAGE AND HANDLING
-
17 PATIENT COUNSELING INFORMATION
Advise patient to read FDA-approved patient labeling (Medication Guide).
Embryo-Fetal Toxicity
Counsel female patients of reproductive potential about the need to use reliable methods of contraception during treatment with OPSUMIT and for one month after treatment discontinuation. Females of reproductive potential must have monthly pregnancy tests and must use reliable methods of contraception while taking OPSUMIT and for one month after discontinuing OPSUMIT [see Use in Specific Populations (8.1)] .
Macitentan-Containing Products REMS
For female patients, OPSUMIT is available only through a restricted program called the Macitentan-Containing Products REMS [see Warnings and Precautions (5.2)] . Male patients are not enrolled in the Macitentan-Containing Products REMS.
Patients may choose one highly effective form of contraception (intrauterine devices (IUD), contraceptive implants or tubal sterilization) or a combination of methods (hormone method with a barrier method or two barrier methods).
Patients should be instructed to contact their physician if they suspect they may be pregnant. Patients should seek additional contraceptive advice from a gynecologist or similar expert as needed.
Inform female patients (and their guardians, if applicable) of the following notable requirements.
- Female patients must sign an enrollment form.
- Female patients of reproductive potential must comply with the pregnancy testing and contraception requirements [see Use in Specific Populations (8.3)] .
Educate and counsel females of reproductive potential on the use of emergency contraception in the event of unprotected sex or contraceptive failure.
Advise pre-pubertal females to report any changes in their reproductive status immediately to her prescriber.
Review the Medication Guide and REMS educational materials with female patients.
Lactation
Advise women not to breastfeed during treatment with OPSUMIT [see Use in Specific Population (8.2)] .
Hepatotoxicity
Some members of this pharmacological class are hepatotoxic. Educate patients on signs of hepatotoxicity. Advise patients that they should contact their doctor if they have unexplained nausea, vomiting, right upper quadrant pain, fatigue, anorexia, jaundice, dark urine, fever, or itching.
- SPL UNCLASSIFIED SECTION
-
MEDICATION GUIDE
MEDICATION GUIDE
OPSUMIT ® (OP-sum-it)
(macitentan)
tabletsThis Medication Guide has been approved by the U.S. Food and Drug Administration. Revised: 03/2024 Read this Medication Guide for OPSUMIT before you start taking OPSUMIT and each time you get a refill. There may be new information. This Medication Guide does not take the place of talking with your healthcare provider about your medical condition or your treatment. What is the most important information I should know about OPSUMIT?
- Serious birth defects.
OPSUMIT can cause serious birth defects if taken during pregnancy. - Females must not be pregnant when they start taking OPSUMIT or become pregnant during treatment with OPSUMIT.
- Females who are able to get pregnant must have a negative pregnancy test before beginning treatment with OPSUMIT, each month during treatment with OPSUMIT and 1 month after stopping OPSUMIT. Talk to your healthcare provider about your menstrual cycle. Your healthcare provider will decide when to do the pregnancy test, and will order a pregnancy test for you depending on your menstrual cycle.
- Females who
are able to get pregnant are females who:
- have entered puberty, even if they have not started their menstrual period, and
- have a uterus, and
- have not gone through menopause. Menopause means that you have not had a menstrual period for at least 12 months for natural reasons, or that you have had your ovaries removed.
- Females who
are not able to get pregnant are females who:
- have not yet entered puberty, or
- do not have a uterus, or
- have gone through menopause. Menopause means that you have not had a menstrual period for at least 12 months for natural reasons, or that you have had your ovaries removed, or
- are infertile for other medical reasons and this infertility is permanent and cannot be reversed.
- Females who
are able to get pregnant are females who:
Females who are able to get pregnant must use two acceptable forms of birth control during treatment with OPSUMIT, and for one month after stopping OPSUMIT because the medicine may still be in the body. - If you have had a tubal sterilization, have a progesterone implant, or have an IUD (intrauterine device), these methods can be used alone and no other form of birth control is needed.
- Talk with your healthcare provider or gynecologist (a doctor who specializes in female reproduction) to find out about options for acceptable birth control that you may use to prevent pregnancy during treatment with OPSUMIT.
- If you decide that you want to change the form of birth control that you use, talk with your healthcare provider or gynecologist to be sure that you choose another acceptable form of birth control.
See the chart below for Acceptable Birth Control Options during treatment with OPSUMIT. 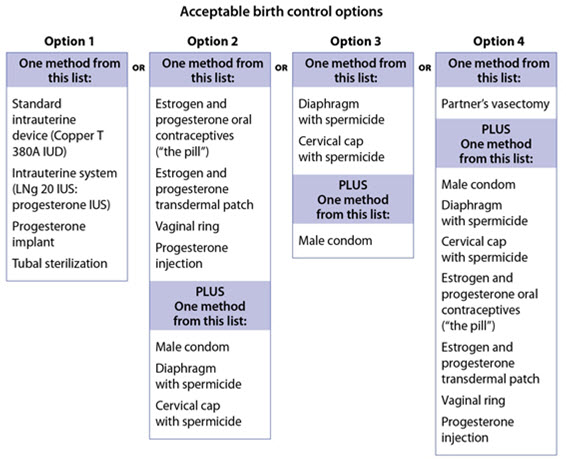
- Do not have unprotected sex. Talk to your healthcare provider or pharmacist right away if you have unprotected sex or if you think your birth control has failed. Your healthcare provider may talk with you about using emergency birth control.
- Tell your healthcare provider right away if you miss a menstrual period or think you may be pregnant.
If you are the parent or caregiver of a female child who started taking OPSUMIT before reaching puberty, you should check your child regularly to see if she is developing signs of puberty. Tell your healthcare provider right away if you notice that she is developing breast buds or any pubic hair. Your healthcare provider should decide if your child has reached puberty. Your child may reach puberty before having her first menstrual period. Females can only receive OPSUMIT through a restricted program called the Macitentan-Containing Products Risk Evaluation and Mitigation Strategy (REMS). If you are a female who can get pregnant, you must talk to your healthcare provider, understand the benefits and risks of OPSUMIT, and agree to all of the instructions in the Macitentan-Containing Products REMS. Males can receive OPSUMIT without taking part in the Macitentan-Containing Products REMS. What is OPSUMIT? - OPSUMIT is a prescription medicine used to treat pulmonary arterial hypertension (PAH), which is high blood pressure in the arteries of your lungs.
- OPSUMIT can improve your ability to exercise, improve some of your symptoms, and help slow down the progression of your disease. OPSUMIT can also lower your chance of being hospitalized for PAH.
- It is not known if OPSUMIT is safe and effective in children.
Who should not take OPSUMIT? Do not take OPSUMIT if you are pregnant, plan to become pregnant, or become pregnant during treatment with OPSUMIT. OPSUMIT can cause serious birth defects (see the Medication Guide section above called " What is the most important information I should know about OPSUMIT?").
Do not take OPSUMIT if you are allergic to macitentan or any of the ingredients in OPSUMIT. See the end of this Medication Guide for a complete list of ingredients in OPSUMIT.Tell your healthcare provider about all your medical conditions and all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. OPSUMIT and other medicines may affect each other causing side effects. Do not start any new medicine until you check with your healthcare provider. Especially tell your healthcare provider if you take an HIV medicine. How should I take OPSUMIT? OPSUMIT will be mailed to you by a specialty pharmacy. Your healthcare provider will give you complete details. - Take OPSUMIT exactly as your healthcare provider tells you to take it. Do not stop taking OPSUMIT unless your healthcare provider tells you.
- You can take OPSUMIT with or without food.
- If you take too much OPSUMIT, call your healthcare provider or go to the nearest hospital emergency room right away.
- If you miss a dose of OPSUMIT, take it as soon as you remember that day. Take the next dose at your regular time. Do not take 2 doses at the same time to make up for a missed dose.
What should I avoid while taking OPSUMIT? - Do not get pregnant while taking OPSUMIT. See the serious birth defects section of the Medication Guide above called " What is the most important information I should know about OPSUMIT?" If you miss a menstrual period, or think you might be pregnant, call your healthcare provider right away.
- It is not known if OPSUMIT passes into your breastmilk. You should not breastfeed if you take OPSUMIT. Talk to your healthcare provider about the best way to feed your baby if you take OPSUMIT.
What are the possible side effects of OPSUMIT? OPSUMIT can cause serious side effects, including: - Serious birth defects. See " What is the most important information I should know about OPSUMIT?"
- Some medicines that are like OPSUMIT can cause liver problems. Your healthcare provider should do blood tests to check your liver before you start taking OPSUMIT. Tell your healthcare provider if you have any of the following symptoms of liver problems while taking OPSUMIT.
- nausea or vomiting
- pain in the upper right stomach
- tiredness
- loss of appetite
- yellowing of your skin or whites of your eyes
- dark urine
- fever
- itching
- Fluid retention can happen within weeks after starting OPSUMIT. Tell your healthcare provider right away if you have any unusual weight gain or swelling of your ankles or legs. Your healthcare provider will look for the cause of any fluid retention.
- Low red blood cell levels (anemia) can occur with OPSUMIT treatment, usually during the first weeks after starting therapy. In some cases a blood transfusion may be needed, but this is not common. Your healthcare provider will do blood tests to check your red blood cells before starting OPSUMIT. Your healthcare provider may also need to do these tests during treatment with OPSUMIT.
- Decreased sperm count. OPSUMIT, and other medicines like OPSUMIT, may cause decreased sperm counts in men who take these medicines. A decreased sperm count may affect the ability to father a child. Tell your healthcare provider if being able to have children is important to you.
The most common side effects of OPSUMIT are: - Stuffy nose or sore throat
- Irritation of the airways (bronchitis)
- Headache
- Flu
- Urinary tract infection
Tell your healthcare provider if you have any side effect that bothers you or that does not go away. These are not all the possible side effects of OPSUMIT. For more information, ask your healthcare provider or pharmacist. Call your healthcare provider for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. How should I store OPSUMIT? - Store OPSUMIT tablets at room temperature between 68°F and 77°F (20°C and 25°C).
- Keep OPSUMIT and all medicines out of the reach of children.
General information about OPSUMIT Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use OPSUMIT for a condition for which it was not prescribed. Do not give OPSUMIT to other people, even if they have the same symptoms that you have. It may harm them. This Medication Guide summarizes the most important information about OPSUMIT. If you would like more information, talk with your healthcare provider. You can ask your pharmacist or healthcare provider for information about OPSUMIT that is written for health professionals. For more information, call 1-800-526-7736 (1-800-JANSSEN), or visit www.OPSUMIT.com. What are the ingredients in OPSUMIT? Active ingredient: macitentan Inactive ingredients: lactose monohydrate, magnesium stearate, microcrystalline cellulose, polysorbate 80, povidone, and sodium starch glycolate Type A. The tablets are film-coated with a coating material containing polyvinyl alcohol, soya lecithin, talc, titanium dioxide, and xanthan gum. Manufactured for:
Actelion Pharmaceuticals US, Inc.,
a Janssen Pharmaceutical Company
Titusville, NJ 08560, USA
For patent information: www.janssenpatents.com
© 2013 – 2019 Actelion Pharmaceuticals US, Inc. All rights reserved. - PRINCIPAL DISPLAY PANEL - 10 mg Tablet Bottle Carton
-
INGREDIENTS AND APPEARANCE
OPSUMIT
macitentan tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:66215-501 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength MACITENTAN (UNII: Z9K9Y9WMVL) (MACITENTAN - UNII:Z9K9Y9WMVL) MACITENTAN 10 mg Inactive Ingredients Ingredient Name Strength LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) SODIUM STARCH GLYCOLATE TYPE A POTATO (UNII: 5856J3G2A2) POVIDONE, UNSPECIFIED (UNII: FZ989GH94E) MAGNESIUM STEARATE (UNII: 70097M6I30) POLYSORBATE 80 (UNII: 6OZP39ZG8H) POLYVINYL ALCOHOL, UNSPECIFIED (UNII: 532B59J990) LECITHIN, SOYBEAN (UNII: 1DI56QDM62) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) XANTHAN GUM (UNII: TTV12P4NEE) Product Characteristics Color white Score no score Shape ROUND Size 6mm Flavor Imprint Code 10 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:66215-501-30 1 in 1 CARTON 11/04/2013 1 30 in 1 BOTTLE; Type 0: Not a Combination Product 2 NDC:66215-501-15 1 in 1 CARTON 11/04/2013 2 15 in 1 BLISTER PACK; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA204410 11/04/2013 Labeler - Actelion Pharmaceuticals US, Inc. (002641228) Establishment Name Address ID/FEI Business Operations Allpack Group AG 484572565 pack(66215-501) , label(66215-501) Establishment Name Address ID/FEI Business Operations Lonza AG 480007517 api manufacture(66215-501) , analysis(66215-501) Establishment Name Address ID/FEI Business Operations JETPHARMA SA 481885861 particle size reduction(66215-501) Establishment Name Address ID/FEI Business Operations Patheon France S.A.S. 543127229 pack(66215-501) , label(66215-501) , manufacture(66215-501) , analysis(66215-501) Establishment Name Address ID/FEI Business Operations Excella GmbH & Co. KG 329809800 manufacture(66215-501) , analysis(66215-501) Establishment Name Address ID/FEI Business Operations MICRO-MACINAZIONE SA 480918515 analysis(66215-501) , particle size reduction(66215-501) Establishment Name Address ID/FEI Business Operations Johnson & Johnson Private Ltd. 677603030 analysis(66215-501)
