FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Bronchospasm
For treatment of acute episodes of bronchospasm or prevention of symptoms associated with bronchospasm, the usual dosage for adults and children 4 years and older is two inhalations repeated every 4 to 6 hours. More frequent administration or a larger number of inhalations is not recommended. In some patients, one inhalation every 4 hours may be sufficient.
2.2 Exercise-Induced Bronchospasm
The usual dosage for adults and children 4 years of age or older is two inhalations 15 to 30 minutes before exercise.
2.3 Administration Information
Administer albuterol sulfate inhalation aerosol by oral inhalation only. Shake well before each spray. To maintain proper use of this product and to prevent medication build-up and blockage, it is important to follow the cleaning directions carefully.
Priming: Prime the inhaler before using for the first time and in cases where the inhaler has not been used for more than 2 weeks by releasing three sprays into the air, away from the face.
Cleaning: As with all HFA-containing albuterol inhalers, to maintain proper use of this product and to prevent medication build-up and blockage, it is important to clean the plastic mouthpiece regularly. The inhaler may cease to deliver medication if the plastic actuator mouthpiece is not properly cleaned and dried. To clean: Wash the plastic mouthpiece with warm running water for 30 seconds, shake off excess water, and air dry thoroughly at least once a week. If the patient has more than one albuterol sulfate inhalation aerosol inhaler, the patient should wash each one separately to prevent attaching the wrong canister to the wrong plastic actuator. In this way, the patient can be sure to always know the correct number of remaining doses. Never attach a canister of medication from any other inhaler to the albuterol sulfate inhalation aerosol actuator and never attach the albuterol sulfate inhalation aerosol canister to an actuator from any other inhaler. If the mouthpiece becomes blocked, washing the mouthpiece will remove the blockage. If it is necessary to use the inhaler before it is completely dry, shake off excess water, put the cap on the mouthpiece, replace canister, remove the cap from the mouthpiece, spray twice into the air away from face, and take the prescribed dose. After such use, the mouthpiece should be rewashed and allowed to air dry thoroughly. [see FDA-Approved Patient Labeling (17.9)].
Dose Counter: Albuterol sulfate inhalation aerosol has a dose counter attached to the actuator. When the patient receives the inhaler, the number 203 will appear in the viewing window and will count down during each of three priming sprays, at which point the number 200 will be displayed. The dose counter will count down each time a spray is released. When the dose counter reaches 20, the patient should contact their pharmacist for a refill of medication or consult their physician for a prescription refill. When it is time to obtain a new inhaler a red flag will begin to show in the window, getting larger as the number of doses remaining approaches 0. The red flag will remind the patient that a new inhaler is needed. When the dose counter reaches 0, a very large 0 with a solid red background will appear in the window. Albuterol Sulfate Inhalation Aerosol inhaler should be discarded when the dose counter displays 0 or after the expiration date on the product, whichever comes first.
3 DOSAGE FORMS AND STRENGTHS
Albuterol sulfate inhalation aerosol is an inhalation aerosol. Albuterol sulfate inhalation aerosol is supplied as an 8.5 g/200 actuations pressurized aluminum canister with a white plastic actuator with a dose counter and white dust cap each in boxes of one. Each actuation delivers 120 mcg of albuterol sulfate from the canister valve and 108 mcg of albuterol sulfate from the actuator mouthpiece (equivalent to 90 mcg of albuterol base).
4 CONTRAINDICATIONS
Albuterol sulfate inhalation aerosol is contraindicated in patients with a history of hypersensitivity to albuterol and any other albuterol sulfate inhalation aerosol components. Rare cases of hypersensitivity reactions, including urticaria, angioedema, and rash have been reported after the use of albuterol sulfate [see Warnings and Precautions (5.6)].
5 WARNINGS AND PRECAUTIONS
5.1 Paradoxical Bronchospasm
Albuterol sulfate inhalation aerosol can produce paradoxical bronchospasm that may be life threatening. If paradoxical bronchospasm occurs, albuterol sulfate inhalation aerosol should be discontinued immediately and alternative therapy instituted. It should be recognized that paradoxical bronchospasm, when associated with inhaled formulations, frequently occurs with the first use of a new canister.
5.2 Deterioration of Asthma
Asthma may deteriorate acutely over a period of hours or chronically over several days or longer. If the patient needs more doses of albuterol sulfate inhalation aerosol than usual, this may be a marker of destabilization of asthma and requires re-evaluation of the patient and treatment regimen, giving special consideration to the possible need for anti-inflammatory treatment, e.g., corticosteroids.
5.3 Use of Anti-inflammatory Agents
The use of beta-adrenergic-agonist bronchodilators alone may not be adequate to control asthma in many patients. Early consideration should be given to adding anti-inflammatory agents, e.g., corticosteroids, to the therapeutic regimen.
5.4 Cardiovascular Effects
Albuterol sulfate inhalation aerosol, like other beta-adrenergic agonists, can produce clinically significant cardiovascular effects in some patients as measured by pulse rate, blood pressure, and/or symptoms. Although such effects are uncommon after administration of albuterol sulfate inhalation aerosol at recommended doses, if they occur, the drug may need to be discontinued. In addition, beta-agonists have been reported to produce ECG changes, such as flattening of the T wave, prolongation of the QTc interval, and ST segment depression. The clinical significance of these findings is unknown. Therefore, albuterol sulfate inhalation aerosol, like all sympathomimetic amines, should be used with caution in patients with cardiovascular disorders, especially coronary insufficiency, cardiac arrhythmias, and hypertension.
5.5 Do Not Exceed Recommended Dose
Fatalities have been reported in association with excessive use of inhaled sympathomimetic drugs in patients with asthma. The exact cause of death is unknown, but cardiac arrest following an unexpected development of a severe acute asthmatic crisis and subsequent hypoxia is suspected.
5.6 Immediate Hypersensitivity Reactions
Immediate hypersensitivity reactions may occur after administration of albuterol sulfate, as demonstrated by rare cases of urticaria, angioedema, rash, bronchospasm, anaphylaxis, and oropharyngeal edema. The potential for hypersensitivity must be considered in the clinical evaluation of patients who experience immediate hypersensitivity reactions while receiving albuterol sulfate inhalation aerosol.
5.7 Coexisting Conditions
Albuterol sulfate inhalation aerosol, like all sympathomimetic amines, should be used with caution in patients with cardiovascular disorders, especially coronary insufficiency, cardiac arrhythmias, and hypertension; in patients with convulsive disorders, hyperthyroidism, or diabetes mellitus; and in patients who are unusually responsive to sympathomimetic amines. Clinically significant changes in systolic and diastolic blood pressure have been seen in individual patients and could be expected to occur in some patients after use of any beta-adrenergic bronchodilator. Large doses of intravenous albuterol have been reported to aggravate preexisting diabetes mellitus and ketoacidosis.
5.8 Hypokalemia
As with other beta-agonists, albuterol sulfate inhalation aerosol may produce significant hypokalemia in some patients, possibly through intracellular shunting, which has the potential to produce adverse cardiovascular effects. The decrease is usually transient, not requiring supplementation.
6 ADVERSE REACTIONS
Use of albuterol sulfate inhalation aerosol may be associated with the following:
- •
- Paradoxical bronchospasm [see Warnings and Precautions (5.1)]
- •
- Cardiovascular Effects [see Warnings and Precautions (5.4)]
- •
- Immediate hypersensitivity reactions [see Warnings and Precautions (5.6)]
- •
- Hypokalemia [see Warnings and Precautions (5.8)]
6.1 Clinical Trials Experience
A total of 1090 subjects were treated with albuterol sulfate inhalation aerosol, or with the same formulation of albuterol as in albuterol sulfate inhalation aerosol, during the worldwide clinical development program.
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Adult and Adolescents 12 Years of Age and Older: The adverse reaction information presented in the table below concerning albuterol sulfate inhalation aerosol is derived from a 6-week, blinded study which compared albuterol sulfate inhalation aerosol (180 mcg four times daily) with a double-blinded matched placebo HFA-inhalation aerosol and an evaluator-blinded marketed active comparator HFA-134a albuterol inhaler in 172 asthmatic patients 12 to 76 years of age. The table lists the incidence of all adverse events (whether considered by the investigator drug related or unrelated to drug) from this study which occurred at a rate of 3% or greater in the albuterol sulfate inhalation aerosol treatment group and more frequently in the albuterol sulfate inhalation aerosol treatment group than in the matched placebo group. Overall, the incidence and nature of the adverse events reported for albuterol sulfate inhalation aerosol and the marketed active comparator HFA-134a albuterol inhaler were comparable.
Adverse Experience Incidences (% of Patients) in a Six-Week Clinical Trial*
|
Body System/Adverse Event (as Preferred Term) |
Albuterol Sulfate Inhalation Aerosol (N = 58) |
Marketed active comparator HFA-134a albuterol inhaler (N = 56) |
Matched Placebo HFA-134a inhalation aerosol (N = 58) |
|
|
Body as a Whole |
Headache |
7 |
5 |
2 |
|
Cardiovascular |
Tachycardia |
3 |
2 |
0 |
|
Musculoskeletal |
Pain |
3 |
0 |
0 |
|
Nervous System |
Dizziness |
3 |
0 |
0 |
|
Respiratory System |
Pharyngitis Rhinitis |
14 5 |
7 4 |
9 2 |
*This table includes all adverse events (whether considered by the investigator drug related or unrelated to drug) which occurred at an incidence rate of at least 3.0% in the albuterol sulfate inhalation aerosol group and more frequently in the albuterol sulfate inhalation aerosol group than in the placebo HFA inhalation aerosol group.
Adverse events reported by less than 3% of the patients receiving albuterol sulfate inhalation aerosol but by a greater proportion of albuterol sulfate inhalation aerosol patients than the matched placebo patients, which have the potential to be related to albuterol sulfate inhalation aerosol, included chest pain, infection, diarrhea, glossitis, accidental injury (nervous system), anxiety, dyspnea, ear disorder, ear pain, and urinary tract infection.
In small cumulative dose studies, tremor, nervousness, and headache were the most frequently occurring adverse events.
Pediatric Patients 4 to 11 Years of Age: Adverse events reported in a 3-week pediatric clinical trial comparing the same formulation of albuterol as in albuterol sulfate inhalation aerosol (180 mcg albuterol four times daily) to a matching placebo HFA inhalation aerosol occurred at a low incidence rate (no greater than 2% in the active treatment group) and were similar to those seen in adult and adolescent trials.
6.2 Postmarketing Experience
The following adverse reactions have been identified during postapproval use of albuterol sulfate inhalation aerosol. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. Reports have included rare cases of aggravated bronchospasm, lack of efficacy, asthma exacerbation (reported fatal in one case), muscle cramps, and various oropharyngeal side-effects such as throat irritation, altered taste, glossitis, tongue ulceration, and gagging.
The following adverse events have been observed in postapproval use of inhaled albuterol: urticaria, angioedema, rash, bronchospasm, hoarseness, oropharyngeal edema, and arrhythmias (including atrial fibrillation, supraventricular tachycardia, extrasystoles). In addition, albuterol, like other sympathomimetic agents, can cause adverse reactions such as: angina, hypertension or hypotension, palpitations, central nervous system stimulation, insomnia, headache, nervousness, tremor, muscle cramps, drying or irritation of the oropharynx, hypokalemia, hyperglycemia, and metabolic acidosis.
7 DRUG INTERACTIONS
Other short-acting sympathomimetic aerosol bronchodilators should not be used concomitantly with albuterol sulfate inhalation aerosol. If additional adrenergic drugs are to be administered by any route, they should be used with caution to avoid deleterious cardiovascular effects.
7.1 Beta-Blockers
Beta-adrenergic-receptor blocking agents not only block the pulmonary effect of beta-agonists, such as albuterol sulfate inhalation aerosol, but may produce severe bronchospasm in asthmatic patients. Therefore, patients with asthma should not normally be treated with beta-blockers. However, under certain circumstances, e.g., as prophylaxis after myocardial infarction, there may be no acceptable alternatives to the use of beta-adrenergic-blocking agents in patients with asthma. In this setting, consider cardioselective beta-blockers, although they should be administered with caution.
7.2 Diuretics
The ECG changes and/or hypokalemia which may result from the administration of non-potassium sparing diuretics (such as loop or thiazide diuretics) can be acutely worsened by beta-agonists, especially when the recommended dose of the beta-agonist is exceeded. Although the clinical significance of these effects is not known, caution is advised in the coadministration of beta-agonists with non-potassium sparing diuretics. Consider monitoring potassium levels.
7.3 Digoxin
Mean decreases of 16% and 22% in serum digoxin levels were demonstrated after single dose intravenous and oral administration of albuterol, respectively, to normal volunteers who had received digoxin for 10 days. The clinical significance of these findings for patients with obstructive airway disease who are receiving albuterol and digoxin on a chronic basis is unclear. Nevertheless, it would be prudent to carefully evaluate the serum digoxin levels in patients who are currently receiving digoxin and albuterol sulfate inhalation aerosol.
7.4 Monoamine Oxidase Inhibitors or Tricyclic Antidepressants
Albuterol sulfate inhalation aerosol should be administered with extreme caution to patients being treated with monoamine oxidase inhibitors or tricyclic antidepressants, or within 2 weeks of discontinuation of such agents, because the action of albuterol on the cardiovascular system may be potentiated. Consider alternative therapy in patients taking MAO inhibitors or tricyclic antidepressants.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to asthma medications during pregnancy. For more information, contact the Mothers To Baby Pregnancy Studies conducted by the Organization of Teratology Information Specialists at 1-877-311-8972 or visit http://mothertobaby.org/pregnancy-studies/.
Risk Summary
There are no randomized clinical studies of use of albuterol during pregnancy. Available data from published epidemiological studies and postmarketing case reports of pregnancy outcomes following inhaled albuterol use do not consistently demonstrate a risk of major birth defects or miscarriage. There are clinical considerations with use of albuterol in pregnant women [see Clinical Considerations]. In animal reproduction studies, when albuterol sulfate was administered subcutaneously to pregnant mice there was evidence of cleft palate at less than and up to 9 times the maximum recommended human daily inhalation dose (MRHDID) [see Data].
The estimated background risk of major birth defects and miscarriage for the indicated population(s) are unknown. In the U.S. general population, the estimated risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively.
Clinical Considerations
Disease-Associated Maternal and/or Embryo/Fetal Risk
In women with poorly or moderately controlled asthma, there is an increased risk of preeclampsia in the mother and prematurity, low birth weight, and small for gestational age in the neonate. Pregnant women should be closely monitored and medication adjusted as necessary to maintain optimal control.
Labor or Delivery
Because of the potential for beta-agonist interference with uterine contractility, use of albuterol sulfate inhalation aerosol for relief of bronchospasm during labor should be restricted to those patients in whom the benefits clearly outweigh the risk. Albuterol sulfate inhalation aerosol has not been approved for the management of pre-term labor. Serious adverse reactions, including pulmonary edema, have been reported during or following treatment of premature labor with beta2-agonists, including albuterol.
Data
Animal Data
In a mouse reproduction study, subcutaneously administered albuterol sulfate produced cleft palate formation in 5 of 111 (4.5%) fetuses at an exposure nine-tenths of the MRHDID for adults (on a mg/m2 basis at a maternal dose of 0.25 mg/kg) and in 10 of 108 (9.3%) fetuses at approximately 9 times the MRHDID (on a mg/m2 basis at a maternal dose of 2.5 mg/kg). Similar effects were not observed at approximately one-eleventh the MRHDID for adults (on a mg/m2 basis at a maternal dose of 0.025 mg/kg). Cleft palate also occurred in 22 of 72 (30.5%) fetuses from females treated subcutaneously with isoproterenol (positive control).
In a rabbit reproduction study, orally administered albuterol sulfate induced cranioschisis in 7 of 19 fetuses (37%) at approximately 750 times the MRHDID (on a mg/m2 basis at a maternal dose of 50 mg/kg).
In a rat reproduction study, an albuterol sulfate/HFA-134a formulation administered by inhalation did not produce any teratogenic effects at exposures approximately 80 times the MRHDID (on a mg/m2 basis at a maternal dose of 10.5 mg/kg).
A study in which pregnant rats were dosed with radiolabeled albuterol sulfate demonstrated that drug-related material is transferred from the maternal circulation to the fetus.
8.2 Lactation
Risk Summary
There are no available data on the presence of albuterol in human milk, the effects on the breastfed child, or the effects on milk production. However, plasma levels of albuterol after inhaled therapeutic doses are low in humans, and if present in breast milk, albuterol has a low oral bioavailability [see Clinical Pharmacology (12.3)].
The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for albuterol and any potential adverse effects on the breastfed child from albuterol or from the underlying maternal condition.
8.4 Pediatric Use
The safety and effectiveness of albuterol sulfate inhalation aerosol for the treatment or prevention of bronchospasm in children 12 years of age and older with reversible obstructive airway disease is based on one 6-week clinical trial in 116 patients 12 years of age and older with asthma comparing doses of 180 mcg four times daily with placebo, and one single-dose crossover study comparing doses of 90, 180, and 270 mcg with placebo in 58 patients [see Clinical Studies (14.1)]. The safety and effectiveness of albuterol sulfate inhalation aerosol for treatment of exercise-induced bronchospasm in children 12 years of age and older is based on one single-dose crossover study in 24 adults and adolescents with exercise-induced bronchospasm comparing doses of 180 mcg with placebo [see Clinical Studies (14.2)].
The safety of albuterol sulfate inhalation aerosol in children 4 to 11 years of age is based on one 3-week clinical trial in 50 patients 4 to 11 years of age with asthma using the same formulation of albuterol as in albuterol sulfate inhalation aerosol comparing doses of 180 mcg four times daily with placebo. The effectiveness of albuterol sulfate inhalation aerosol in children 4 to 11 years of age is extrapolated from clinical trials in patients 12 years of age and older with asthma and exercise-induced bronchospasm, based on data from a single-dose study comparing the bronchodilatory effect of albuterol sulfate inhalation aerosol 90 mcg and 180 mcg with placebo in 55 patients with asthma and a 3-week clinical trial using the same formulation of albuterol as in albuterol sulfate inhalation aerosol in 95 asthmatic children 4 to 11 years of age comparing a dose of 180 mcg albuterol four times daily with placebo [see Clinical Studies (14.1)]. The safety and effectiveness of albuterol sulfate inhalation aerosol in pediatric patients below the age of 4 years have not been established.
8.5 Geriatric Use
Clinical studies of albuterol sulfate inhalation aerosol did not include sufficient numbers of patients aged 65 and over to determine whether they respond differently from younger patients. Other reported clinical experience has not identified differences in responses between elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy [see Warnings and Precautions (5.4, 5.7)].
All beta2-adrenergic agonists, including albuterol, are known to be substantially excreted by the kidney, and the risk of toxic reactions may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
10 OVERDOSAGE
The expected symptoms with overdosage are those of excessive beta-adrenergic stimulation and/or occurrence or exaggeration of any of the symptoms listed under ADVERSE REACTIONS, e.g., seizures, angina, hypertension or hypotension, tachycardia with rates up to 200 beats per minute, arrhythmias, nervousness, headache, tremor, dry mouth, palpitation, nausea, dizziness, fatigue, malaise, and insomnia.
Hypokalemia may also occur. As with all sympathomimetic medications, cardiac arrest and even death may be associated with abuse of albuterol sulfate inhalation aerosol.
Treatment consists of discontinuation of albuterol sulfate inhalation aerosol together with appropriate symptomatic therapy. The judicious use of a cardioselective beta-receptor blocker may be considered, bearing in mind that such medication can produce bronchospasm. There is insufficient evidence to determine if dialysis is beneficial for overdosage of albuterol sulfate inhalation aerosol.
The oral median lethal dose of albuterol sulfate in mice is greater than 2,000 mg/kg (approximately 6,800 times the maximum recommended daily inhalation dose for adults on a mg/m2 basis and approximately 3,200 times the maximum recommended daily inhalation dose for children on a mg/m2 basis). In mature rats, the subcutaneous median lethal dose of albuterol sulfate is approximately 450 mg/kg (approximately 3,000 times the maximum recommended daily inhalation dose for adults on a mg/m2 basis and approximately 1,400 times the maximum recommended daily inhalation dose for children on a mg/m2 basis). In young rats, the subcutaneous median lethal dose is approximately 2,000 mg/kg (approximately 14,000 times the maximum recommended daily inhalation dose for adults on a mg/m2 basis and approximately 6,400 times the maximum recommended daily inhalation dose for children on a mg/m2 basis). The inhalation median lethal dose has not been determined in animals.
11 DESCRIPTION
The active ingredient of albuterol sulfate inhalation aerosol is albuterol sulfate, a racemic salt, of albuterol. Albuterol sulfate has the chemical name α1-[(tert-butylamino) methyl]-4-hydroxy-m-xylene-α,α'-diol sulfate (2:1) (salt), and has the following chemical structure:
The molecular weight of albuterol sulfate is 576.7, and the empirical formula is (C13H21NO3)2•H2SO4. Albuterol sulfate is a white to off-white crystalline powder. It is soluble in water and slightly soluble in ethanol. Albuterol sulfate is the official generic name in the United States, and salbutamol sulfate is the World Health Organization recommended generic name. Albuterol sulfate inhalation aerosol is a pressurized metered-dose aerosol unit with a dose counter. Albuterol sulfate inhalation aerosol is for oral inhalation only. It contains a microcrystalline suspension of albuterol sulfate in propellant HFA-134a (1, 1, 1, 2-tetrafluoroethane) and ethanol.
Prime the inhaler before using for the first time and in cases where the inhaler has not been used for more than 2 weeks by releasing three sprays into the air, away from the face. After priming, each actuation delivers 108 mcg albuterol sulfate, from the actuator mouthpiece (equivalent to 90 mcg of albuterol base). Each canister provides 200 actuations (inhalations).
This product does not contain chlorofluorocarbons (CFCs) as the propellant.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Albuterol sulfate is a beta2-adrenergic agonist. The pharmacologic effects of albuterol sulfate are attributable to activation of beta2-adrenergic receptors on airway smooth muscle. Activation of beta2-adrenergic receptors leads to the activation of adenylcyclase and to an increase in the intracellular concentration of cyclic-3', 5'-adenosine monophosphate (cyclic AMP). This increase of cyclic AMP is associated with the activation of protein kinase A, which in turn inhibits the phosphorylation of myosin and lowers intracellular ionic calcium concentrations, resulting in muscle relaxation. Albuterol relaxes the smooth muscle of all airways, from the trachea to the terminal bronchioles. Albuterol acts as a functional antagonist to relax the airway irrespective of the spasmogen involved, thus protecting against all bronchoconstrictor challenges. Increased cyclic AMP concentrations are also associated with the inhibition of release of mediators from mast cells in the airway. While it is recognized that beta2-adrenergic receptors are the predominant receptors on bronchial smooth muscle, data indicate that there are beta-receptors in the human heart, 10% to 50% of which are cardiac beta2-adrenergic receptors. The precise function of these receptors has not been established [see Warnings and Precautions (5.4)].
Albuterol has been shown in most controlled clinical trials to have more effect on the respiratory tract, in the form of bronchial smooth muscle relaxation, than isoproterenol at comparable doses while producing fewer cardiovascular effects. However, inhaled albuterol, like other beta-adrenergic agonist drugs, can produce a significant cardiovascular effect in some patients, as measured by pulse rate, blood pressure, symptoms, and/or electrocardiographic changes [see Warnings and Precautions (5.4)].
12.2 Pharmacokinetics
The systemic levels of albuterol are low after inhalation of recommended doses. In a crossover study conducted in healthy male and female volunteers, high cumulative doses of albuterol sulfate inhalation aerosol (1,080 mcg of albuterol base administered over one hour) yielded mean peak plasma concentrations (Cmax) and systemic exposure (AUCinf) of approximately 4,100 pg/mL and 28,426 pg/mL*hr, respectively compared to approximately 3,900 pg/mL and 28,395 pg/mL*hr, respectively following the same dose of an active HFA-134a albuterol inhaler comparator. The terminal plasma half-life of albuterol delivered by albuterol sulfate inhalation aerosol was approximately 6 hours. Comparison of the pharmacokinetic parameters demonstrated no differences between the products.
The pharmacokinetic profile of albuterol sulfate inhalation aerosol was evaluated in a two-way cross-over study in 11 healthy pediatric volunteers, 4 to 11 years of age. A single dose administration of albuterol sulfate inhalation aerosol (180 mcg albuterol base) yielded a least square mean (SE) Cmax and AUC0-∞ of 1,100 (1.18) pg/mL and 5,120 (1.15) pg/mL*hr, respectively. The least square mean (SE) terminal plasma half-life of albuterol delivered by albuterol sulfate inhalation aerosol was 166 (7.8) minutes.
Metabolism and Elimination: Information available in the published literature suggests that the primary enzyme responsible for the metabolism of albuterol in humans is SULTIA3 (sulfotransferase). When racemic albuterol was administered either intravenously or via inhalation after oral charcoal administration, there was a 3- to 4-fold difference in the area under the concentration-time curves between the (R)- and (S)-albuterol enantiomers, with (S)-albuterol concentrations being consistently higher. However, without charcoal pretreatment, after either oral or inhalation administration the differences were 8- to 24-fold, suggesting that the (R)-albuterol is preferentially metabolized in the gastrointestinal tract, presumably by SULTIA3.
The primary route of elimination of albuterol is through renal excretion (80% to 100%) of either the parent compound or the primary metabolite. Less than 20% of the drug is detected in the feces. Following intravenous administration of racemic albuterol, between 25% and 46% of the (R)-albuterol fraction of the dose was excreted as unchanged (R)-albuterol in the urine.
Geriatric, Pediatric, Hepatic/Renal Impairment: No pharmacokinetic studies for albuterol sulfate inhalation aerosol have been conducted in neonates or elderly subjects.
The effect of hepatic impairment on the pharmacokinetics of albuterol sulfate inhalation aerosol has not been evaluated.
The effect of renal impairment on the pharmacokinetics of albuterol was evaluated in 5 subjects with creatinine clearance of 7 to 53 mL/min, and the results were compared with those from healthy volunteers. Renal disease had no effect on the half-life, but there was a 67% decline in albuterol clearance. Caution should be used when administering high doses of albuterol sulfate inhalation aerosol to patients with renal impairment [see Use in Specific Populations (8.5)].
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
In a 2-year study in Sprague-Dawley rats, albuterol sulfate caused a dose-related increase in the incidence of benign leiomyomas of the mesovarium at and above dietary doses of 2 mg/kg (approximately 15 times and 6 times the maximum recommended human daily inhalation dose (MRHDID) for adults and children, respectively, on a mg/m2 basis). In another study this effect was blocked by the coadministration of propranolol, a non-selective beta-adrenergic antagonist. In an 18-month study in CD-1 mice, albuterol sulfate showed no evidence of tumorigenicity at dietary doses of up to 500 mg/kg (approximately 1,900 times and 740 times the MRHDID for adults and children, respectively, on a mg/m2 basis). In a 22-month study in Golden Hamsters, albuterol sulfate showed no evidence of tumorigenicity at dietary doses of up to 50 mg/kg (approximately 250 times and 100 times the MRHDID for adults and children, respectively, on a mg/m2 basis).
Albuterol sulfate was not mutagenic in the Ames test or a mutation test in yeast. Albuterol sulfate was not clastogenic in a human peripheral lymphocyte assay or in an AH1 strain mouse micronucleus assay.
Reproduction studies in rats demonstrated no evidence of impaired fertility at oral doses up to 50 mg/kg (approximately 380 times the MRHDID for adults on a mg/m2 basis).
13.2 Animal Toxicology and/or Pharmacology
Preclinical: Intravenous studies in rats with albuterol sulfate have demonstrated that albuterol crosses the blood-brain barrier and reaches brain concentrations amounting to approximately 5% of the plasma concentrations. In structures outside the blood-brain barrier (pineal and pituitary glands), albuterol concentrations were found to be 100 times those in the whole brain.
Studies in laboratory animals (minipigs, rodents, and dogs) have demonstrated the occurrence of cardiac arrhythmias and sudden death (with histologic evidence of myocardial necrosis) when β-agonists and methylxanthines were administered concurrently. The clinical significance of these findings is unknown.
Propellant HFA-134a is devoid of pharmacological activity except at very high doses in animals (380 – 1300 times the maximum human exposure based on comparisons of AUC values), primarily producing ataxia, tremors, dyspnea, or salivation. These are similar to effects produced by the structurally related chlorofluorocarbons (CFCs), which have been used extensively in metered-dose inhalers.
In animals and humans, propellant HFA-134a was found to be rapidly absorbed and rapidly eliminated, with an elimination half-life of 3 - 27 minutes in animals and 5 - 7 minutes in humans. Time to maximum plasma concentration (Tmax) and mean residence time are both extremely short leading to a transient appearance of HFA-134a in the blood with no evidence of accumulation.
14 CLINICAL STUDIES
14.1 Bronchospasm Associated with Asthma
Adult and Adolescent Patients 12 Years of Age and Older: In a 6-week, randomized, double-blind, placebo-controlled trial, albuterol sulfate inhalation aerosol (58 patients) was compared to a matched placebo HFA inhalation aerosol (58 patients) in asthmatic patients 12 to 76 years of age at a dose of 180 mcg albuterol four times daily. An evaluator-blind marketed active comparator HFA-134a albuterol inhaler arm (56 patients) was included.
Serial FEV1 measurements, shown below as percent change from test-day baseline at Day 1 and at Day 43, demonstrated that two inhalations of albuterol sulfate inhalation aerosol produced significantly greater improvement in FEV1 over the pre-treatment value than the matched placebo, as well as a comparable bronchodilator effect to the marketed active comparator HFA-134a albuterol inhaler.
FEV1 as Mean Percent Change from Test-Day Pre-Dose in a 6-Week Clinical Trial
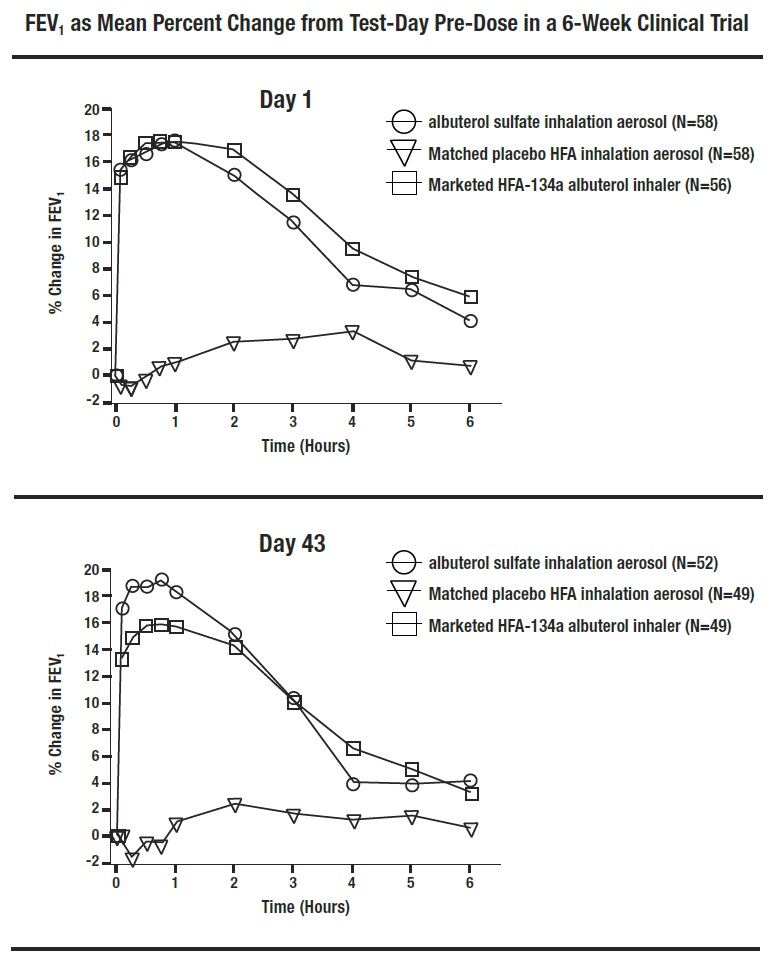
In this study, 31 of 58 patients treated with albuterol sulfate inhalation aerosol achieved a 15% increase in FEV1 within 30 minutes post-dose on Day 1. In these patients, the median time to onset, median time to peak effect, and median duration of effect were 8.2 minutes, 47 minutes, and approximately 3 hours, respectively. In some patients, the duration of effect was as long as 6 hours.
In a placebo-controlled, single-dose, crossover study, albuterol sulfate inhalation aerosol, administered at albuterol doses of 90, 180 and 270 mcg, produced bronchodilator responses significantly greater than those observed with a matched placebo HFA inhalation aerosol and comparable to a marketed active comparator HFA-134a albuterol inhaler.
Pediatric Patients 4 to 11 Years of Age: In a 3-week, randomized, double-blind, placebo-controlled trial, the same formulation of albuterol as in albuterol sulfate inhalation aerosol (50 patients) was compared to a matched placebo HFA inhalation aerosol (45 patients) in asthmatic children 4 to 11 years of age at a dose of 180 mcg albuterol four times daily. Serial FEV1 measurements, expressed as the maximum percent change from test-day baseline in percent predicted FEV1 at Day 1 and at Day 22 observed within two hours post-dose, demonstrated that two inhalations of HFA albuterol sulfate produced significantly greater improvement in FEV1 over the pre-treatment value than the matched placebo.
In this study, 21 of 50 pediatric patients treated with the same formulation of albuterol as in albuterol sulfate inhalation aerosol achieved a 15% increase in FEV1 within 30 minutes post-dose on Day 1. In these patients, the median time to onset, median time to peak effect and median duration of effect were 10 minutes, 31 minutes, and approximately 4 hours, respectively. In some pediatric patients, the duration of effect was as long as 6 hours.
In a placebo-controlled, single-dose, crossover study in 55 pediatric patients 4 to 11 years of age, albuterol sulfate inhalation aerosol, administered at albuterol doses of 90 and 180 mcg, was compared with a matched placebo HFA inhalation aerosol. Serial FEV1 measurements, expressed as the baseline-adjusted percent predicted FEV1 observed over 6 hours post-dose, demonstrated that one and two inhalations of albuterol sulfate inhalation aerosol produced significantly greater bronchodilator responses than the matched placebo.
14.2 Exercise-Induced Bronchospasm
In a randomized, single-dose, crossover study in 24 adults and adolescents with exercise-induced bronchospasm (EIB), two inhalations of albuterol sulfate inhalation aerosol taken 30 minutes before exercise prevented EIB for the hour following exercise (defined as maintenance of FEV1 within 80% of post-dose, pre-exercise baseline values) in 83% (20 of 24) of patients as compared to 25% (6 of 24) of patients when they received placebo.
Some patients who participated in these clinical trials were using concomitant steroid therapy.
16 HOW SUPPLIED/STORAGE & HANDLING
Product: 53002-1552
NDC: 53002-1552-1 200 AEROSOL, METERED in a INHALER / 1 in a CARTON
17 PATIENT COUNSELING INFORMATION
See FDA-Approved Patient Labeling (17.9)
Patients should be given the following information:
17.1 Frequency of Use
The action of albuterol sulfate inhalation aerosol should last for 4 to 6 hours. Do not use albuterol sulfate inhalation aerosol more frequently than recommended. Instruct patients to not increase the dose or frequency of doses of albuterol sulfate inhalation aerosol without consulting the physician. If patients find that treatment with albuterol sulfate inhalation aerosol becomes less effective for symptomatic relief, symptoms become worse, and/or they need to use the product more frequently than usual, they should seek medical attention immediately.
17.2 Priming and Cleaning
Priming: Priming is essential to ensure appropriate albuterol content in each actuation. Instruct patients to prime the inhaler before using for the first time and in cases where the inhaler has not been used for more than 2 weeks by releasing three sprays into the air, away from the face.
Cleaning: To ensure proper dosing and prevent actuator orifice blockage, instruct patients to wash the white plastic actuator mouthpiece and dry thoroughly at least once a week. Instruct patients that if they have more than one albuterol sulfate inhalation aerosol inhaler, they should wash each one at separate times to prevent attaching the wrong canister to the wrong plastic actuator. In this way, they can be sure they will always know the correct number of remaining doses. Patients should be instructed to never attach a canister of medicine from any other inhaler to the albuterol sulfate inhalation aerosol actuator and never attach the albuterol sulfate inhalation aerosol canister to an actuator from any other inhaler. Patients should not remove the canister from the actuator except during cleaning because reattachment may release a dose into the air and the dose counter will count down each time a spray is released. Detailed cleaning instructions are included in the illustrated Information for the Patient leaflet.
17.3 Dose Counter
Patients should be informed that albuterol sulfate inhalation aerosol has a dose counter attached to the actuator. When the patient receives the inhaler, the number 203 will appear in the viewing window and will count down during each of three priming sprays, at which point the number 200 will be displayed. The dose counter will count down each time a spray is released. The dose-counter window displays the number of sprays left in the inhaler. When the counter displays 20, the patient should contact their pharmacist for a refill of medication or consult their physician for a prescription refill. When it is time to obtain a new inhaler a red flag will begin to show in the window, getting larger as the number of doses remaining approaches 0. The red flag will remind the patient that a new inhaler is needed. When the dose counter reaches 0, a very large 0 with a solid red background will appear in the window. Patients should be informed to discard albuterol sulfate inhalation aerosol inhaler when the dose counter displays 0 or after the expiration date on the product, whichever comes first.
17.4 Paradoxical Bronchospasm
Inform patients that albuterol sulfate inhalation aerosol can produce paradoxical bronchospasm. Instruct patients to discontinue albuterol sulfate inhalation aerosol if paradoxical bronchospasm occurs.
17.5 Concomitant Drug Use
While patients are taking albuterol sulfate inhalation aerosol, other inhaled drugs and asthma medications should be taken only as directed by a physician.
17.6 Common Adverse Events
Common adverse effects of treatment with inhaled albuterol include palpitations, chest pain, rapid heart rate, tremor, or nervousness.
17.7 Pregnancy
Patients who are pregnant or nursing should contact their physician about the use of albuterol sulfate inhalation aerosol.
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to asthma medications during pregnancy [see Use in Specific Populations (8.1)].
17.8 General Information on Use
Effective and safe use of albuterol sulfate inhalation aerosol includes an understanding of the way that it should be administered.
Shake well before each spray.
Use albuterol sulfate inhalation aerosol only with the actuator supplied with the product. Discard the albuterol sulfate inhalation aerosol inhaler when the dose counter displays a solid red background with a large 0 or after expiration date on the product, whichever comes first. Never immerse the canister in water to determine how full the canister is ("float test").
In general, the technique for administering albuterol sulfate inhalation aerosol to children is similar to that for adults. Children should use albuterol sulfate inhalation aerosol under adult supervision, as instructed by the patient's physician.
Distributed By Perrigo, Allegan, MI 49010 • www.perrigorx.com
Rev 09/2020
4K000 RC J9
Attention Pharmacist: Detach Patient’s Instructions for use from package insert and dispense with the product.
Patient Information
Albuterol Sulfate (al bue׳ ter ol sul׳ fate) Inhalation Aerosol
Read this Patient Information before you start using Albuterol Sulfate Inhalation Aerosol and each time you get a refill. There may be new information.
This information does not take the place of talking to your doctor about your medical condition or your treatment.
What is Albuterol Sulfate Inhalation Aerosol?
Albuterol Sulfate Inhalation Aerosol is a prescription medicine used in people 4 years of age and older to:
- •
- treat or prevent bronchospasm in people who have reversible obstructive airway disease
- •
- prevent exercise induced bronchospasm
It is not known if Albuterol Sulfate Inhalation Aerosol is safe and effective in children under 4 years of age.
Who should not use Albuterol Sulfate Inhalation Aerosol?
Do not use Albuterol Sulfate Inhalation Aerosol if you are allergic to albuterol sulfate or any of the ingredients in Albuterol Sulfate Inhalation Aerosol. See the end of this leaflet for a complete list of ingredients in Albuterol Sulfate Inhalation Aerosol.
What should I tell my doctor before I use Albuterol Sulfate Inhalation Aerosol?
Before you use Albuterol Sulfate Inhalation Aerosol, tell your doctor if you:
- •
- have heart problems
- •
- have high blood pressure (hypertension)
- •
- have convulsions (seizures)
- •
- have thyroid problems
- •
- have diabetes
- •
- have low potassium levels in your blood
- •
- are pregnant or plan to become pregnant. It is not known if Albuterol Sulfate Inhalation Aerosol will harm your unborn baby. Talk to your doctor if you are pregnant or plan to become pregnant.
- •
- are breastfeeding or plan to breastfeed. It is not known if Albuterol Sulfate Inhalation Aerosol passes into your breast milk. Talk to your doctor about the best way to feed your baby if you are using Albuterol Sulfate Inhalation Aerosol.
Tell your doctor about all the medicines you take, including prescription and non-prescription medicines, vitamins, and herbal supplements.
Albuterol Sulfate Inhalation Aerosol and other medicines may affect each other and cause side effects. Albuterol Sulfate Inhalation Aerosol may affect the way other medicines work, and other medicines may affect the way Albuterol Sulfate Inhalation Aerosol works.
Especially tell your doctor if you take:
- •
- other inhaled medicines or asthma medicines
- •
- beta blocker medicines
- •
- diuretics
- •
- digoxin
- •
- monoamine oxidase inhibitors
- •
- tricyclic antidepressants
Ask your doctor or pharmacist for a list of these medicines if you are not sure. Know the medicines you take. Keep a list of them to show your doctor and pharmacist when you get a new medicine.
How should I use Albuterol Sulfate Inhalation Aerosol?
- •
- For detailed instructions, see “Instructions for Use” at the end of this Patient Information.
- •
- Use Albuterol Sulfate Inhalation Aerosol exactly as your doctor tells you to use it.
- •
- If your child needs to use Albuterol Sulfate Inhalation Aerosol, watch your child closely to make sure your child uses the inhaler correctly. Your doctor will show you how your child should use Albuterol Sulfate Inhalation Aerosol.
- •
- Each dose of Albuterol Sulfate Inhalation Aerosol should last up to 4 hours to 6 hours.
- •
- Do not increase your dose or take extra doses of Albuterol Sulfate Inhalation Aerosol without first talking to your doctor.
- •
- Get medical help right away if Albuterol Sulfate Inhalation Aerosol no longer helps your symptoms.
- •
- Get medical help right away if your symptoms get worse or if you need to use your inhaler more often.
- •
- While you are using Albuterol Sulfate Inhalation Aerosol, do not use other inhaled rescue medicines and asthma medicines unless your doctor tells you to do so.
- •
- Call your doctor if your asthma symptoms like wheezing and trouble breathing become worse over a few hours or days. Your doctor may need to give you another medicine (for example, corticosteroids) to treat your symptoms.
What are the possible side effects of Albuterol Sulfate Inhalation Aerosol?
Albuterol Sulfate Inhalation Aerosol may cause serious side effects, including:
- •
- worsening trouble breathing, coughing and wheezing (paradoxical bronchospasm).
If this happens stop using Albuterol Sulfate Inhalation Aerosol and call your doctor or get emergency help right away. Paradoxical bronchospasm is more likely to happen with your first use of a new canister of medicine.
- •
- heart problems including faster heart rate and higher blood pressure
- •
- possible death in people with asthma who use too much Albuterol Sulfate Inhalation Aerosol
- •
-
allergic reactions. Call your doctor right away if you have the following symptoms of an allergic reaction:
- o
- itchy skin
- o
- swelling beneath your skin or in your throat
- o
- rash
- o
- worsening trouble breathing
- •
- low potassium levels in your blood
- •
- worsening of other medical problems in people who also use Albuterol Sulfate Inhalation Aerosol including increases in blood sugar
The most common side effects of Albuterol Sulfate Inhalation Aerosol include:
- •
- your heart feels like it is pounding or racing (palpitations)
- •
- chest pain
- •
- fast heart rate
- •
- shakiness
- •
- nervousness
- •
- headache
- •
- dizziness
- •
- sore throat
- •
- runny nose
Tell your doctor if you have any side effect that bothers you or that does not go away.
These are not all of the possible side effects of Albuterol Sulfate Inhalation Aerosol.
For more information, ask your doctor or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store Albuterol Sulfate Inhalation Aerosol?
- •
- Store Albuterol Sulfate Inhalation Aerosol at room temperature between 68° F and 77° F (20° C and 25° C).
- •
- Avoid exposure to extreme heat and cold.
- •
- Shake the Albuterol Sulfate Inhalation Aerosol canister well before use.
- •
- Do not puncture the Albuterol Sulfate Inhalation Aerosol canister.
- •
- Do not store the Albuterol Sulfate Inhalation Aerosol canister near heat or a flame. Temperatures above 120° F may cause the canister to burst.
- •
- Do not throw the Albuterol Sulfate Inhalation Aerosol canister into a fire or an incinerator.
- •
- Avoid spraying Albuterol Sulfate Inhalation Aerosol in your eyes.
Keep Albuterol Sulfate Inhalation Aerosol and all medicines out of the reach of children.
General Information about the safe and effective use of Albuterol Sulfate Inhalation Aerosol
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use Albuterol Sulfate Inhalation Aerosol for a condition for which it was not prescribed. Do not give Albuterol Sulfate Inhalation Aerosol to other people, even if they have the same symptoms that you have. It may harm them.
This Patient Information summarizes the most important information about Albuterol Sulfate Inhalation Aerosol. If you would like more information, talk with your doctor. You can ask your pharmacist or doctor for information about Albuterol Sulfate Inhalation Aerosol that is written for health professionals.
For more information, call 1-866-634-9120.
What are the ingredients in Albuterol Sulfate Inhalation Aerosol?
Active ingredient: albuterol sulfate
Inactive ingredients: propellant HFA-134a and ethanol.
Instructions for Use
Albuterol Sulfate (al bue׳ ter ol sul׳ fate) Inhalation Aerosol
Read this Instructions for Use before you start using Albuterol Sulfate Inhalation Aerosol and each time you get a refill. There may be new information. This information does not take the place of talking to your doctor about your medical condition or your treatment.
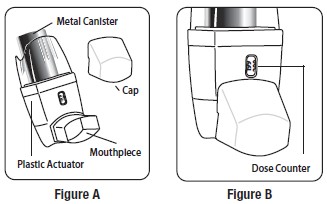
The Parts of Your Albuterol Sulfate Inhalation Aerosol Inhaler Device:
There are 2 main parts of your Albuterol Sulfate Inhalation Aerosol inhaler device including a:
- •
- white plastic actuator that sprays the medicine from the canister. See Figure A.
- •
- white protective dust cap that covers the mouthpiece of the actuator. See Figure A.
There is also a metal canister that holds the medicine. See Figure A.
There is also a dose counter attached to the actuator with a viewing window that shows you how many sprays of medicine you have left. See Figure B.
You will see the number 203 in the viewing window which will count down during each of 3 priming shots. See Figure B and “Priming Your Albuterol Sulfate Inhalation Aerosol Device” below.
- •
- Do not use the Albuterol Sulfate Inhalation Aerosol actuator with a canister of medicine from any other inhaler.
- •
- Do not use a Albuterol Sulfate Inhalation Aerosol canister with an actuator from any other inhaler, including another Albuterol Sulfate Inhalation Aerosol inhaler.
Priming Your Albuterol Sulfate Inhalation Aerosol Device:
Your Albuterol Sulfate Inhalation Aerosol device must be primed before you use it for the first time or if your device has not been used for more than 14 days in a row. Do not prime your Albuterol Sulfate Inhalation Aerosol device every day.
- •
- Remove your Albuterol Sulfate Inhalation Aerosol device from its package.
- •
- Remove the protective dust cap from the mouthpiece.
- •
- Shake the inhaler well, and spray it into the air away from your face. See Figure C.
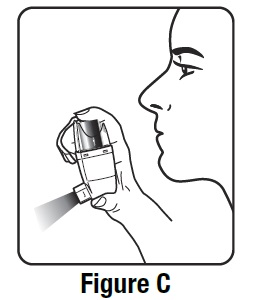
- •
- Shake and spray the inhaler like this 2 more times to finish priming it. The dose counter on the actuator should display the number 200 after you finish priming the inhaler for the first time. See Figure D.
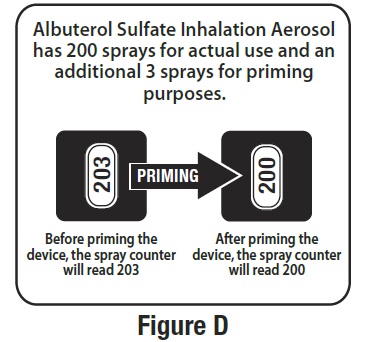
- •
- Priming is necessary to make sure the correct dose of albuterol is contained in each actuation (spray). Your inhaler has 200 sprays for actual use and an extra 3 sprays for priming purposes. When the dose counter reads 203, 202, or 201, spray it into the air away from your face to prime it until the dose counter reads 200. Only begin using the new inhaler after priming, by actuating (spraying) 3 times, and when the dose counter reads 200 in the window.
Each Time You Use Your Albuterol Sulfate Inhalation Aerosol Device:
- •
- Make sure the canister fits firmly in the plastic actuator.
- •
- Look into the mouthpiece to make sure there are no foreign objects there, especially if the cap has not been used to cover the mouthpiece.
Reading the Dose Counter on Your Albuterol Sulfate Inhalation Aerosol Actuator
- •
- The dose counter will count down each time a spray is released. The dose counter window shows the number of sprays left in your inhaler. See Figure D.
- •
- When the dose counter reaches 0 with a solid red background, it will continue to show a large 0 and you should replace your Albuterol Sulfate Inhalation Aerosol device.
- •
- The dose counter cannot be reset and is permanently attached to the actuator. Never change the numbers for the dose counter or touch the parts inside the actuator.
- •
- Do not remove the canister from the plastic actuator except during cleaning, and make sure the cap is on the mouthpiece when reattaching the canister to the plastic actuator. Placing the cap on the mouthpiece before reattaching the canister will prevent accidental release of a dose of Albuterol Sulfate Inhalation Aerosol into the air or increasing of the number of doses on the dose counter. The dose counter will count down each time a spray is released.
Using Your Albuterol Sulfate Inhalation Aerosol Device:
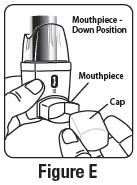
Step 1. Shake the inhaler well before each spray. Take the cap off the mouthpiece of the actuator.
Step 2. Hold the inhaler with the mouthpiece down. See Figure E.
Step 3. Breathe out through your mouth and push as much air from your lungs as you can. Put the mouthpiece in your mouth and close your lips around it. See Figure F.
Step 4. Push the top of the canister all the way down while you breathe in deeply and slowly through your mouth. See Figure F.
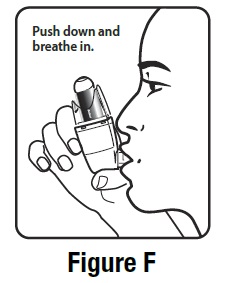
Step 5. Right after the spray comes out, take your finger off the canister. After you have breathed in all the way, take the inhaler out of your mouth and close your mouth.
Step 6. Hold your breath as long as you can, up to 10 seconds, then breathe normally. If your doctor has told you to use more sprays, wait 1 minute and shake the inhaler again. Repeat Steps 2 through Step 6.
Step 7. Put the cap back on the mouthpiece after every time you use the inhaler. Make sure the cap snaps firmly into place.
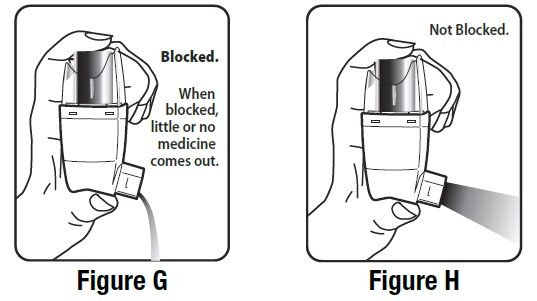
Cleaning Your Albuterol Sulfate Inhalation Aerosol Device:
It is very important to keep the plastic actuator clean so the medicine will not build-up and block the spray. See Figure G and Figure H.
- •
- Do not try to clean the metal canister or let it get wet. The inhaler may stop spraying if it is not cleaned correctly.
- •
- If you have more than 1 Albuterol Sulfate Inhalation Aerosol inhaler, wash each device at separate times to prevent putting the wrong canister together with the wrong plastic actuator. This way you can be sure you will always know the correct number of remaining doses of Albuterol Sulfate Inhalation Aerosol.
- •
-
Wash the actuator at least 1 time each week as follows:
- o
- Take the canister out of the actuator, and take the cap off the mouthpiece.
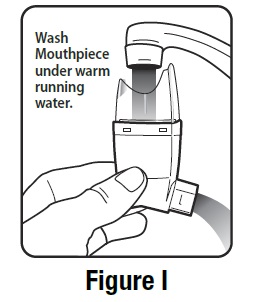
- o
- Hold the actuator under the faucet and run warm water through it for about 30 seconds. See Figure I.
-
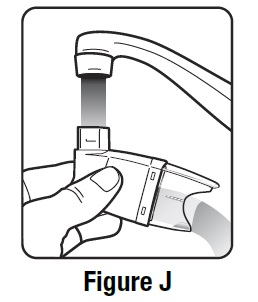
- o
- Turn the actuator upside down and run warm water through the mouthpiece for about 30 seconds. See Figure J.
-
- o
- Shake off as much water from the actuator as you can. Look into the mouthpiece to make sure any medicine build-up has been completely washed away. If there is any build-up, repeat the washing instructions.
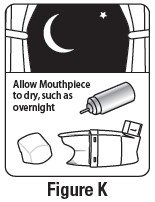
- o
- Let the actuator air-dry completely, such as overnight. See Figure K.
-
- o
- When the actuator is dry, put the cap on the mouthpiece and then put the canister in the actuator and make sure it fits firmly. Remove the cap from the mouthpiece, shake the inhaler well and spray it twice into the air away from your face. Put the cap back on the mouthpiece.
If you need to use your inhaler before the actuator is completely dry:
- •
- Shake as much water off the actuator as you can.
- •
- Place the cap on the mouthpiece and then put the canister in the actuator and make sure it fits firmly.
- •
- Remove the cap from the mouthpiece, shake the inhaler well and spray it twice into the air away from your face.
- •
- Take your Albuterol Sulfate Inhalation Aerosol dose as prescribed.
- •
- Follow the Cleaning Instructions above.
Replacing Your Albuterol Sulfate Inhalation Aerosol Device
- •
- When the dose counter on the actuator says the number 20, contact your pharmacy to refill your prescription or ask your doctor for another prescription for Albuterol Sulfate Inhalation Aerosol. When it is time to obtain a new inhaler a red flag will begin to show in the window, getting larger as the number of doses remaining approaches 0. When the dose counter reaches 0, the background color will change to solid red. The red flag is to remind you to refill your prescription or ask your doctor for another prescription.
- •
- Throw the Albuterol Sulfate Inhalation Aerosol inhaler away as soon as the dose counter says 0 with a solid red background or after the expiration date on the Albuterol Sulfate Inhalation Aerosol packaging, whichever comes first. You should not keep using the inhaler after 200 sprays even though the canister may not be completely empty. You cannot be sure you will receive any medicine after using 200 sprays.
- •
- Do not use the inhaler after the expiration date on the Albuterol Sulfate Inhalation Aerosol packaging.
This Patient Information and Instructions for Use has been approved by the U.S. Food and Drug Administration.
Distributed By Perrigo, Allegan, MI 49010 • www.perrigorx.com
Rev 09/2020