FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
1.1 Gout Flares
COLCRYS (colchicine, USP) tablets are indicated for prophylaxis and the treatment of acute gout flares.
- •
-
Prophylaxis of Gout Flares:
COLCRYS is indicated for prophylaxis of gout flares. - •
-
Treatment of Gout Flares:
COLCRYS tablets are indicated for treatment of acute gout flares when taken at the first sign of a flare.
2 DOSAGE AND ADMINISTRATION
The long-term use of colchicine is established for FMF and the prophylaxis of gout flares, but the safety and efficacy of repeat treatment for gout flares has not been evaluated. The dosing regimens for COLCRYS are different for each indication and must be individualized.
The recommended dosage of COLCRYS depends on the patient's age, renal function, hepatic function and use of coadministered drugs [see Dose Modification for Coadministration of Interacting Drugs (2.4)].
COLCRYS tablets are administered orally without regard to meals.
COLCRYS is not an analgesic medication and should not be used to treat pain from other causes.
2.1 Gout Flares
Prophylaxis of Gout Flares
The recommended dosage of COLCRYS for prophylaxis of gout flares for adults and adolescents older than 16 years of age is 0.6 mg once or twice daily. The maximum recommended dose for prophylaxis of gout flares is 1.2 mg/day.
An increase in gout flares may occur after initiation of uric acid-lowering therapy, including pegloticase, febuxostat and allopurinol, due to changing serum uric acid levels resulting in mobilization of urate from tissue deposits. COLCRYS is recommended upon initiation of gout flare prophylaxis with uric acid-lowering therapy. Prophylactic therapy may be beneficial for at least the first six months of uric acid-lowering therapy.
Treatment of Gout Flares
The recommended dose of COLCRYS for treatment of a gout flare is 1.2 mg (two tablets) at the first sign of the flare followed by 0.6 mg (one tablet) one hour later. Higher doses have not been found to be more effective. The maximum recommended dose for treatment of gout flares is 1.8 mg over a one hour period. COLCRYS may be administered for treatment of a gout flare during prophylaxis at doses not to exceed 1.2 mg (two tablets) at the first sign of the flare followed by 0.6 mg (one tablet) one hour later. Wait 12 hours and then resume the prophylactic dose.
2.2 FMF
The recommended dosage of COLCRYS for FMF in adults is 1.2 mg to 2.4 mg daily.
COLCRYS should be increased as needed to control disease and as tolerated in increments of 0.3 mg/day to a maximum recommended daily dose. If intolerable side effects develop, the dose should be decreased in increments of 0.3 mg/day. The total daily COLCRYS dose may be administered in one to two divided doses.
2.3 Recommended Pediatric Dosage
Prophylaxis and Treatment of Gout Flares
COLCRYS is not recommended for pediatric use in prophylaxis or treatment of gout flares.
FMF
The recommended dosage of COLCRYS for FMF in pediatric patients 4 years of age and older is based on age. The following daily doses may be given as a single or divided dose twice daily:
- •
- Children 4 to 6 years: 0.3 mg to 1.8 mg daily
- •
- Children 6 to 12 years: 0.9 mg to 1.8 mg daily
- •
- Adolescents older than 12 years: 1.2 mg to 2.4 mg daily
2.4 Dose Modification for Coadministration of Interacting Drugs
Concomitant Therapy
Coadministration of COLCRYS with drugs known to inhibit CYP3A4 and/or P-glycoprotein (P-gp) increases the risk of colchicine-induced toxic effects (Table 1). If patients are taking or have recently completed treatment with drugs listed in Table 1 within the prior 14 days, the dose adjustments are as shown in the table below [see Drug Interactions (7)].
|
|||||||
|
Strong CYP3A4 Inhibitors2 |
|||||||
|
Drug |
Noted or Anticipated Outcome |
Gout Flares |
FMF |
||||
|
Prophylaxis of Gout Flares |
Treatment of Gout Flares |
Original Intended Dosage |
Adjusted Dose |
||||
|
Original Intended Dosage |
Adjusted Dose |
Original Intended Dosage |
Adjusted Dose | ||||
|
Atazanavir |
Significant increase in colchicine plasma levels*; fatal colchicine toxicity has been reported with clarithromycin, a strong CYP3A4 inhibitor. Similarly, significant increase in colchicine plasma levels is anticipated with other strong CYP3A4 inhibitors. |
0.6 mg twice a day |
0.3 mg once a day |
1.2 mg |
0.6 mg |
Maximum daily dose of 1.2 – 2.4 mg |
Maximum daily dose of 0.6 mg (may be given as 0.3 mg twice a day) |
|
Moderate CYP3A4 Inhibitors |
|||||||
|
Drug |
Noted or Anticipated Outcome |
Gout Flares |
FMF |
||||
|
Prophylaxis of Gout Flares |
Treatment of Gout Flares |
Original Intended Dosage |
Adjusted Dose |
||||
|
Original Intended Dosage |
Adjusted Dose |
Original Intended Dosage |
Adjusted Dose | ||||
|
Amprenavir† Aprepitant |
Significant increase in colchicine plasma concentration is anticipated. Neuromuscular toxicity has been reported with diltiazem and verapamil interactions. |
0.6 mg twice a day |
0.3 mg twice a day or 0.6 mg once a day |
1.2 mg |
1.2 mg |
Maximum daily dose of 1.2 – 2.4 mg. |
Maximum daily dose of 1.2 mg (may be given as 0.6 mg twice a day) |
|
P-gp Inhibitors‡ |
|||||||
|
Drug |
Noted or Anticipated Outcome |
Gout Flares |
FMF |
||||
|
Prophylaxis of Gout Flares |
Treatment of Gout Flares |
Original Intended Dosage |
Adjusted Dose |
||||
|
Original Intended Dosage |
Adjusted Dose |
Original Intended Dosage |
Adjusted Dose | ||||
|
Cyclosporine Ranolazine |
Significant increase in colchicine plasma levels*; fatal colchicine toxicity has been reported with cyclosporine, a P-gp inhibitor. Similarly, significant increase in colchicine plasma levels is anticipated with other P-gp inhibitors. |
0.6 mg twice a day |
0.3 mg once a day |
1.2 mg |
0.6 mg |
Maximum daily dose of 1.2 – 2.4 mg |
Maximum daily dose of 0.6 mg (may be given as 0.3 mg twice a day) |
|
Protease Inhibitor |
Clinical Comment |
w/Colchicine - Prophylaxis of Gout Flares |
w/Colchicine -
|
w/Colchicine - Treatment of FMF |
|
|
Atazanavir sulfate |
Patients with renal or hepatic impairment should not be given colchicine with Reyataz. |
Original dose |
Adjusted dose |
0.6 mg (1 tablet) × 1 dose, followed by 0.3 mg (1/2 tablet) 1 hour later. Dose to be repeated no earlier than 3 days. |
Maximum daily dose of 0.6 mg (may be given as 0.3 mg twice a day) |
|
0.6 mg twice a day |
0.3 mg once a day |
||||
|
Darunavir (Prezista) |
Patients with renal or hepatic impairment should not be given colchicine with Prezista/ritonavir. |
Original dose |
Adjusted dose |
0.6 mg (1 tablet) × 1 dose, followed by 0.3 mg (1/2 tablet) 1 hour later. Dose to be repeated no earlier than 3 days. |
Maximum daily dose of 0.6 mg (may be given as 0.3 mg twice a day) |
|
0.6 mg twice a day |
0.3 mg once a day |
||||
|
Fosamprenavir (Lexiva) with Ritonavir |
Patients with renal or hepatic impairment should not be given colchicine with Lexiva/ritonavir. |
Original dose |
Adjusted dose |
0.6 mg (1 tablet) × 1 dose, followed by 0.3 mg (1/2 tablet) 1 hour later. Dose to be repeated no earlier than 3 days. |
Maximum daily dose of 0.6 mg (may be given as 0.3 mg twice a day) |
|
0.6 mg twice a day |
0.3 mg once a day |
||||
|
Fosamprenavir (Lexiva) |
Patients with renal or hepatic impairment should not be given colchicine with Lexiva/ritonavir. |
Original dose |
Adjusted dose |
1.2 mg (2 tablets) × 1 dose. Dose to be repeated no earlier than 3 days. |
Maximum daily dose of 1.2 mg (may be given as 0.6 mg twice a day) |
|
0.6 mg twice a day |
0.3 mg twice a day or 0.6 mg once a day |
||||
|
Indinavir (Crixivan) |
Patients with renal or hepatic impairment should not be given colchicine with Crixivan. |
Original dose |
Adjusted dose |
0.6 mg (1 tablet) × 1 dose, followed by 0.3 mg (1/2 tablet) 1 hour later. Dose to be repeated no earlier than 3 days. |
Maximum daily dose of 0.6 mg (may be given as 0.3 mg twice a day) |
|
0.6 mg twice a day |
0.3 mg once a day |
||||
|
Lopinavir/Ritonavir (Kaletra) |
Patients with renal or hepatic impairment should not be given colchicine with Kaletra. |
Original dose |
Adjusted dose |
0.6 mg (1 tablet) × 1 dose, followed by 0.3 mg (1/2 tablet) 1 hour later. Dose to be repeated no earlier than 3 days. |
Maximum daily dose of 0.6 mg (may be given as 0.3 mg twice a day) |
|
0.6 mg twice a day |
0.3 mg once a day |
||||
|
Nelfinavir mesylate (Viracept) |
Patients with renal or hepatic impairment should not be given colchicine with Viracept. |
Original dose |
Adjusted dose |
0.6 mg (1 tablet) × 1 dose, followed by 0.3 mg (1/2 tablet) 1 hour later. Dose to be repeated no earlier than 3 days. |
Maximum daily dose of 0.6 mg (may be given as 0.3 mg twice a day) |
|
0.6 mg twice a day |
0.3 mg once a day |
||||
|
Ritonavir (Norvir) |
Patients with renal or hepatic impairment should not be given colchicine with Norvir. |
Original dose |
Adjusted dose |
0.6 mg (1 tablet) × 1 dose, followed by 0.3 mg (1/2 tablet) 1 hour later. Dose to be repeated no earlier than 3 days. |
Maximum daily dose of 0.6 mg (may be given as 0.3 mg twice a day) |
|
0.6 mg twice a day |
0.3 mg once a day |
||||
|
Saquinavir mesylate (Invirase) |
Patients with renal or hepatic impairment should not be given colchicine with Invirase/ritonavir. |
Original dose |
Adjusted dose |
0.6 mg (1 tablet) × 1 dose, followed by 0.3 mg (1/2 tablet) 1 hour later. Dose to be repeated no earlier than 3 days. |
Maximum daily dose of 0.6 mg (may be given as 0.3 mg twice a day) |
|
0.6 mg twice a day |
0.3 mg once a day |
||||
|
Tipranavir (Aptivus) |
Patients with renal or hepatic impairment should not be given colchicine with Aptivus/ritonavir. |
Original dose |
Adjusted dose |
0.6 mg (1 tablet) × 1 dose, followed by 0.3 mg (1/2 tablet) 1 hour later. Dose to be repeated no earlier than 3 days. |
Maximum daily dose of 0.6 mg (may be given as 0.3 mg twice a day) |
|
0.6 mg twice a day |
0.3 mg once a day |
||||
Treatment of gout flares with COLCRYS is not recommended in patients receiving prophylactic dose of COLCRYS and CYP3A4 inhibitors.
2.5 Dose Modification in Renal Impairment
Colchicine dosing must be individualized according to the patient's renal function [see Renal Impairment (8.6)].
Clcr in mL/minute may be estimated from serum creatinine (mg/dL) determination using the following formula:
[140-age (years) × weight (kg)]
Clcr = --------------------------------------- × 0.85 for female patients
72 × serum creatinine (mg/dL)
Gout Flares
Prophylaxis of Gout Flares
For prophylaxis of gout flares in patients with mild (estimated creatinine clearance [Clcr] 50 to 80 mL/min) to moderate (Clcr 30 to 50 mL/min) renal function impairment, adjustment of the recommended dose is not required, but patients should be monitored closely for adverse effects of colchicine. However, in patients with severe impairment, the starting dose should be 0.3 mg/day and any increase in dose should be done with close monitoring. For the prophylaxis of gout flares in patients undergoing dialysis, the starting doses should be 0.3 mg given twice a week with close monitoring [see Clinical Pharmacology (12.3) and Renal Impairment (8.6)].
Treatment of Gout Flares
For treatment of gout flares in patients with mild (Clcr 50 to 80 mL/min) to moderate (Clcr 30 to 50 mL/min) renal function impairment, adjustment of the recommended dose is not required, but patients should be monitored closely for adverse effects of colchicine. However, in patients with severe impairment, while the dose does not need to be adjusted for the treatment of gout flares, a treatment course should be repeated no more than once every two weeks. For patients with gout flares requiring repeated courses, consideration should be given to alternate therapy. For patients undergoing dialysis, the total recommended dose for the treatment of gout flares should be reduced to a single dose of 0.6 mg (one tablet). For these patients, the treatment course should not be repeated more than once every two weeks [see Clinical Pharmacology (12.3) and Renal Impairment (8.6)].
Treatment of gout flares with COLCRYS is not recommended in patients with renal impairment who are receiving COLCRYS for prophylaxis.
FMF
Caution should be taken in dosing patients with moderate and severe renal impairment and in patients undergoing dialysis. For these patients, the dosage should be reduced [see Clinical Pharmacology (12.3)]. Patients with mild (Clcr 50 to 80 mL/min) and moderate (Clcr 30 to 50 mL/min) renal impairment should be monitored closely for adverse effects of COLCRYS. Dose reduction may be necessary. For patients with severe renal failure (Clcr less than 30 mL/min), start with 0.3 mg/day; any increase in dose should be done with adequate monitoring of the patient for adverse effects of colchicine [see Renal Impairment (8.6)]. For patients undergoing dialysis, the total recommended starting dose should be 0.3 mg (half tablet) per day. Dosing can be increased with close monitoring. Any increase in dose should be done with adequate monitoring of the patient for adverse effects of colchicine [see Clinical Pharmacology (12.3) and Renal Impairment (8.6)].
2.6 Dose Modification in Hepatic Impairment
Gout Flares
Prophylaxis of Gout Flares
For prophylaxis of gout flares in patients with mild to moderate hepatic function impairment, adjustment of the recommended dose is not required, but patients should be monitored closely for adverse effects of colchicine. Dose reduction should be considered for the prophylaxis of gout flares in patients with severe hepatic impairment [see Hepatic Impairment (8.7)].
Treatment of Gout Flares
For treatment of gout flares in patients with mild to moderate hepatic function impairment, adjustment of the recommended dose is not required, but patients should be monitored closely for adverse effects of colchicine. However, for the treatment of gout flares in patients with severe impairment, while the dose does not need to be adjusted, a treatment course should be repeated no more than once every two weeks. For these patients, requiring repeated courses for the treatment of gout flares, consideration should be given to alternate therapy [see Hepatic Impairment (8.7)].
Treatment of gout flares with COLCRYS is not recommended in patients with hepatic impairment who are receiving COLCRYS for prophylaxis.
FMF
Patients with mild to moderate hepatic impairment should be monitored closely for adverse effects of colchicine. Dose reduction should be considered in patients with severe hepatic impairment [see Hepatic Impairment (8.7)].
3 DOSAGE FORMS AND STRENGTHS
0.6 mg tablets — purple capsule-shaped, film-coated with “AR 374” debossed on one side and scored on the other side.
4 CONTRAINDICATIONS
Patients with renal or hepatic impairment should not be given COLCRYS in conjunction with P-gp or strong CYP3A4 inhibitors (this includes all protease inhibitors except fosamprenavir). In these patients, life-threatening and fatal colchicine toxicity has been reported with colchicine taken in therapeutic doses.
5 WARNINGS AND PRECAUTIONS
5.1 Fatal Overdose
Fatal overdoses, both accidental and intentional, have been reported in adults and children who have ingested colchicine [see Overdosage (10)]. COLCRYS should be kept out of the reach of children.
5.2 Blood Dyscrasias
Myelosuppression, leukopenia, granulocytopenia, thrombocytopenia, pancytopenia and aplastic anemia have been reported with colchicine used in therapeutic doses.
5.3 Drug Interactions
Colchicine is a P-gp and CYP3A4 substrate. Life-threatening and fatal drug interactions have been reported in patients treated with colchicine given with P-gp and strong CYP3A4 inhibitors. If treatment with a P-gp or strong CYP3A4 inhibitor is required in patients with normal renal and hepatic function, the patient's dose of colchicine may need to be reduced or interrupted [see Drug Interactions (7)]. Use of COLCRYS in conjunction with P-gp or strong CYP3A4 inhibitors (this includes all protease inhibitors except fosamprenavir) is contraindicated in patients with renal or hepatic impairment [see Contraindications (4)].
5.4 Neuromuscular Toxicity
Colchicine-induced neuromuscular toxicity and rhabdomyolysis have been reported with chronic treatment in therapeutic doses. Patients with renal dysfunction and elderly patients, even those with normal renal and hepatic function, are at increased risk. Concomitant use of atorvastatin, simvastatin, pravastatin, fluvastatin, lovastatin, gemfibrozil, fenofibrate, fenofibric acid or benzafibrate (themselves associated with myotoxicity) or cyclosporine with COLCRYS may potentiate the development of myopathy [see Drug Interactions (7)]. Once colchicine is stopped, the symptoms generally resolve within one week to several months.
6 ADVERSE REACTIONS
Prophylaxis of Gout Flares
The most commonly reported adverse reaction in clinical trials of colchicine for the prophylaxis of gout was diarrhea.
Treatment of Gout Flares
The most common adverse reactions reported in the clinical trial with COLCRYS for treatment of gout flares were diarrhea (23%) and pharyngolaryngeal pain (3%).
FMF
Gastrointestinal tract adverse effects are the most frequent side effects in patients initiating COLCRYS, usually presenting within 24 hours, and occurring in up to 20% of patients given therapeutic doses. Typical symptoms include cramping, nausea, diarrhea, abdominal pain and vomiting. These events should be viewed as dose-limiting if severe, as they can herald the onset of more significant toxicity.
6.1 Clinical Trials Experience in Gout
Because clinical studies are conducted under widely varying and controlled conditions, adverse reaction rates observed in clinical studies of a drug cannot be directly compared to rates in the clinical studies of another drug and may not predict the rates observed in a broader patient population in clinical practice.
In a randomized, double-blind, placebo-controlled trial in patients with a gout flare, gastrointestinal adverse reactions occurred in 26% of patients using the recommended dose (1.8 mg over one hour) of COLCRYS compared to 77% of patients taking a nonrecommended high dose (4.8 mg over six hours) of colchicine and 20% of patients taking placebo. Diarrhea was the most commonly reported drug-related gastrointestinal adverse event. As shown in Table 3, diarrhea is associated with COLCRYS treatment. Diarrhea was more likely to occur in patients taking the high-dose regimen than the low-dose regimen. Severe diarrhea occurred in 19% and vomiting occurred in 17% of patients taking the nonrecommended high-dose colchicine regimen but did not occur in the recommended low-dose COLCRYS regimen.
|
MedDRA System Organ Class MedDRA Preferred Term |
COLCRYS Dose |
Placebo
|
|
|
High (N=52)
|
Low (N=74)
|
||
|
Number of Patients with at Least One Drug-Related TEAE |
40 (77) |
27 (37) |
16 (27) |
|
Gastrointestinal Disorders |
40 (77) |
19 (26) |
12 (20) |
|
Diarrhea |
40 (77) |
17 (23) |
8 (14) |
|
Nausea |
9 (17) |
3 (4) |
3 (5) |
|
Vomiting |
9 (17) |
0 |
0 |
|
Abdominal Discomfort |
0 |
0 |
2 (3) |
|
General Disorders and Administration Site Conditions |
4 (8) |
1 (1) |
1 (2) |
|
Fatigue |
2 (4) |
1 (1) |
1 (2) |
|
Metabolic and Nutrition Disorders |
0 |
3 (4) |
2 (3) |
|
Gout |
0 |
3 (4) |
1 (2) |
|
Nervous System Disorders |
1 (2) |
1 (1.4) |
2 (3) |
|
Headache |
1 (2) |
1 (1) |
2 (3) |
|
Respiratory Thoracic Mediastinal Disorders |
1 (2) |
2 (3) |
0 |
|
Pharyngolaryngeal Pain |
1 (2) |
2 (3) |
0 |
6.2 Postmarketing Experience
Serious toxic manifestations associated with colchicine include myelosuppression, disseminated intravascular coagulation and injury to cells in the renal, hepatic, circulatory and central nervous systems.
These most often occur with excessive accumulation or overdosage [see Overdosage (10)].
The following adverse reactions have been reported with colchicine. These have been generally reversible upon temporarily interrupting treatment or lowering the dose of colchicine.
-
Neurological: sensory motor neuropathy
Dermatological:alopecia, maculopapular rash, purpura, rash
Digestive: abdominal cramping, abdominal pain, diarrhea, lactose intolerance, nausea, vomiting
Hematological: leukopenia, granulocytopenia, thrombocytopenia, pancytopenia, aplastic anemia
Hepatobiliary: elevated AST, elevated ALT
Musculoskeletal: myopathy, elevated CPK, myotonia, muscle weakness, muscle pain, rhabdomyolysis
Reproductive: azoospermia, oligospermia
7 DRUG INTERACTIONS
COLCRYS (colchicine) is a substrate of the efflux transporter P-glycoprotein (P-gp). Of the cytochrome P450 enzymes tested, CYP3A4 was mainly involved in the metabolism of colchicine. If COLCRYS is administered with drugs that inhibit P-gp, most of which also inhibit CYP3A4, increased concentrations of colchicine are likely. Fatal drug interactions have been reported.
Physicians should ensure that patients are suitable candidates for treatment with COLCRYS and remain alert for signs and symptoms of toxicities related to increased colchicine exposure as a result of a drug interaction. Signs and symptoms of COLCRYS toxicity should be evaluated promptly and, if toxicity is suspected, COLCRYS should be discontinued immediately.
Table 4 provides recommendations as a result of other potentially significant drug interactions. Table 1 provides recommendations for strong and moderate CYP3A4 inhibitors and P-gp inhibitors.
|
Concomitant Drug Class or Food |
Noted or Anticipated Outcome |
Clinical Comment |
|
HMG-Co A Reductase Inhibitors:
|
Pharmacokinetic and/or pharmacodynamic interaction: the addition of one drug to a stable long-term regimen of the other has resulted in myopathy and rhabdomyolysis (including a fatality) P-gp substrate; rhabdomyolysis has been reported |
Weigh the potential benefits and risks and carefully monitor patients for any signs or symptoms of muscle pain, tenderness, or weakness, particularly during initial therapy; monitoring CPK (creatine phosphokinase) will not necessarily prevent the occurrence of severe myopathy. |
|
Other Lipid-Lowering Drugs:
|
||
|
Digitalis Glycosides:
|
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Category C.
There are no adequate and well-controlled studies with colchicine in pregnant women. Colchicine crosses the human placenta. While not studied in the treatment of gout flares, data from a limited number of published studies found no evidence of an increased risk of miscarriage, stillbirth or teratogenic effects among pregnant women using colchicine to treat familial Mediterranean fever (FMF). Although animal reproductive and developmental studies were not conducted with COLCRYS, published animal reproduction and development studies indicate that colchicine causes embryofetal toxicity, teratogenicity and altered postnatal development at exposures within or above the clinical therapeutic range. COLCRYS should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
8.3 Nursing Mothers
Colchicine is excreted into human milk. Limited information suggests that exclusively breastfed infants receive less than 10 percent of the maternal weight-adjusted dose. While there are no published reports of adverse effects in breastfeeding infants of mothers taking colchicine, colchicine can affect gastrointestinal cell renewal and permeability. Caution should be exercised, and breastfeeding infants should be observed for adverse effects when COLCRYS is administered to a nursing woman.
8.4 Pediatric Use
The safety and efficacy of colchicine in children of all ages with FMF has been evaluated in uncontrolled studies. There does not appear to be an adverse effect on growth in children with FMF treated long-term with colchicine. Gout is rare in pediatric patients; safety and effectiveness of colchicine in pediatric patients has not been established.
8.5 Geriatric Use
Clinical studies with colchicine for prophylaxis and treatment of gout flares and for treatment of FMF did not include sufficient numbers of patients aged 65 years and older to determine whether they respond differently from younger patients. In general, dose selection for an elderly patient with gout should be cautious, reflecting the greater frequency of decreased renal function, concomitant disease or other drug therapy [see Dose Modification for Coadministration of Interacting Drugs (2.4)and Pharmacokinetics (12.3)].
8.6 Renal Impairment
Colchicine is significantly excreted in urine in healthy subjects. Clearance of colchicine is decreased in patients with impaired renal function. Total body clearance of colchicine was reduced by 75% in patients with end-stage renal disease undergoing dialysis.
Prophylaxis of Gout Flares
For prophylaxis of gout flares in patients with mild (estimated creatinine clearance Clcr 50 to 80 mL/min) to moderate (Clcr 30 to 50 mL/min) renal function impairment, adjustment of the recommended dose is not required, but patients should be monitored closely for adverse effects of colchicine. However, in patients with severe impairment, the starting dose should be 0.3 mg per day and any increase in dose should be done with close monitoring. For the prophylaxis of gout flares in patients undergoing dialysis, the starting doses should be 0.3 mg given twice a week with close monitoring [see Dose Modification in Renal Impairment (2.5)].
Treatment of Gout Flares
For treatment of gout flares in patients with mild (Clcr 50 to 80 mL/min) to moderate (Clcr 30 to 50 mL/min) renal function impairment, adjustment of the recommended dose is not required, but patients should be monitored closely for adverse effects of COLCRYS. However, in patients with severe impairment, while the dose does not need to be adjusted for the treatment of gout flares, a treatment course should be repeated no more than once every two weeks. For patients with gout flares requiring repeated courses, consideration should be given to alternate therapy. For patients undergoing dialysis, the total recommended dose for the treatment of gout flares should be reduced to a single dose of 0.6 mg (one tablet). For these patients, the treatment course should not be repeated more than once every two weeks [see Dose Modification in Renal Impairment (2.5)].
FMF
Although, pharmacokinetics of colchicine in patients with mild (Clcr 50 to 80 mL/min) and moderate (Clcr 30 to 50 mL/min) renal impairment is not known, these patients should be monitored closely for adverse effects of colchicine. Dose reduction may be necessary. In patients with severe renal failure (Clcr less than 30 mL/min) and end-stage renal disease requiring dialysis, COLCRYS may be started at the dose of 0.3 mg/day. Any increase in dose should be done with adequate monitoring of the patient for adverse effects of COLCRYS [see Pharmacokinetics (12.3) and Dose Modification in Renal Impairment (2.5)].
8.7 Hepatic Impairment
The clearance of colchicine may be significantly reduced and plasma half-life prolonged in patients with chronic hepatic impairment compared to healthy subjects [see Pharmacokinetics (12.3)].
Prophylaxis of Gout Flares
For prophylaxis of gout flares in patients with mild to moderate hepatic function impairment, adjustment of the recommended dose is not required, but patients should be monitored closely for adverse effects of colchicine. Dose reduction should be considered for the prophylaxis of gout flares in patients with severe hepatic impairment [see Dose Modification in Hepatic Impairment (2.6)].
Treatment of Gout Flares
For treatment of gout flares in patients with mild to moderate hepatic function impairment, adjustment of the recommended COLCRYS dose is not required, but patients should be monitored closely for adverse effects of COLCRYS. However, for the treatment of gout flares in patients with severe impairment, while the dose does not need to be adjusted, the treatment course should be repeated no more than once every two weeks. For these patients, requiring repeated courses for the treatment of gout flares, consideration should be given to alternate therapy [see Dose Modification in Hepatic Impairment (2.6)].
FMF
In patients with severe hepatic disease, dose reduction should be considered with careful monitoring [see Pharmacokinetics (12.3) and Dose Modification in Hepatic Impairment (2.6)].
10 OVERDOSAGE
The exact dose of colchicine that produces significant toxicity is unknown. Fatalities have occurred after ingestion of a dose as low as 7 mg over a four-day period, while other patients have survived after ingesting more than 60 mg. A review of 150 patients who overdosed on colchicine found that those who ingested less than 0.5 mg/kg survived and tended to have milder toxicities such as gastrointestinal symptoms, whereas those who took 0.5 to 0.8 mg/kg had more severe reactions such as myelosuppression. There was 100% mortality in those who ingested more than 0.8 mg/kg.
The first stage of acute colchicine toxicity typically begins within 24 hours of ingestion and includes gastrointestinal symptoms such as abdominal pain, nausea, vomiting, diarrhea and significant fluid loss, leading to volume depletion. Peripheral leukocytosis may also be seen. Life-threatening complications occur during the second stage, which occurs 24 to 72 hours after drug administration, attributed to multiorgan failure and its consequences. Death is usually a result of respiratory depression and cardiovascular collapse. If the patient survives, recovery of multiorgan injury may be accompanied by rebound leukocytosis and alopecia starting about one week after the initial ingestion.
Treatment of colchicine poisoning should begin with gastric lavage and measures to prevent shock. Otherwise, treatment is symptomatic and supportive. No specific antidote is known. Colchicine is not effectively removed by dialysis [see Pharmacokinetics (12.3)].
11 DESCRIPTION
Colchicine is an alkaloid chemically described as (S)N- (5,6,7,9-tetrahydro- 1,2,3, 10-tetramethoxy-9-oxobenzo [alpha] heptalen-7-yl) acetamide with a molecular formula of C22H25NO6 and a molecular weight of 399.4. The structural formula of colchicine is given below.
Colchicine occurs as a pale yellow powder that is soluble in water.
COLCRYS (colchicine, USP) tablets are supplied for oral administration as purple, film-coated, capsule-shaped tablets (0.1575" × 0.3030"), debossed with “AR 374” on one side and scored on the other, containing 0.6 mg of the active ingredient colchicine USP. Inactive ingredients: carnauba wax, FD&C blue #2, FD&C red #40, hypromellose, lactose monohydrate, magnesium stearate, microcrystalline cellulose, polydextrose, polyethylene glycol, pregelatinized starch, sodium starch glycolate, titanium dioxide and triacetin.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
The mechanism by which COLCRYS exerts its beneficial effect in patients with FMF has not been fully elucidated; however, evidence suggests that colchicine may interfere with the intracellular assembly of the inflammasome complex present in neutrophils and monocytes that mediates activation of interleukin-1β. Additionally, colchicine disrupts cytoskeletal functions through inhibition of β-tubulin polymerization into microtubules and consequently prevents the activation, degranulation and migration of neutrophils thought to mediate some gout symptoms.
12.3 Pharmacokinetics
Absorption
In healthy adults, COLCRYS is absorbed when given orally, reaching a mean Cmax of 2.5 ng/mL (range 1.1 to 4.4 ng/mL) in one to two hours (range 0.5 to three hours) after a single dose administered under fasting conditions.
Following oral administration of COLCRYS given as 1.8 mg colchicine over one hour to healthy, young adults under fasting conditions, colchicine appears to be readily absorbed, reaching mean maximum plasma concentrations of 6.2 ng/mL at a median 1.81 hours (range: 1.0 to 2.5 hours). Following administration of the nonrecommended high-dose regimen (4.8 mg over six hours), mean maximal plasma concentrations were 6.8 ng/mL, at a median 4.47 hours (range: 3.1 to 7.5 hours).
After 10 days on a regimen of 0.6 mg twice daily, peak concentrations are 3.1 to 3.6 ng/mL (range 1.6 to 6.0 ng/mL), occurring 1.3 to 1.4 hours postdose (range 0.5 to 3.0 hours). Mean pharmacokinetic parameter values in healthy adults are shown in Table 5.
|
Cmax (Colchicine ng/mL) |
Tmax* (h) |
Vd/F (L) |
CL/F (L/hr) |
t1/2 (h) |
|
COLCRYS 0.6 mg Single Dose (N=13) |
||||
|
2.5 (28.7) |
1.5 (1.0 – 3.0) |
341.5 (54.4) |
54.1 (31.0) |
-- |
|
COLCRYS 0.6 mg Twice Daily × 10 Days (N=13) |
||||
|
3.6 (23.7) |
1.3 (0.5 – 3.0) |
1150 (18.7) |
30.3 (19.0) |
26.6 (16.3) |
|
*Tmax mean (range) |
||||
In some subjects, secondary colchicine peaks are seen, occurring between three and 36 hours postdose and ranging from 39% to 155% of the height of the initial peak. These observations are attributed to intestinal secretion and reabsorption and/or biliary recirculation.
Absolute bioavailability is reported to be approximately 45%.
Administration of COLCRYS with food has no effect on the rate of colchicine absorption but does decrease the extent of colchicine by approximately 15%. This is without clinical significance.
Distribution
The mean apparent volume of distribution in healthy young volunteers is approximately 5 to 8 L/kg.
Colchicine binding to serum protein is low, 39 ± 5%, primarily to albumin regardless of concentration.
Colchicine crosses the placenta (plasma levels in the fetus are reported to be approximately 15% of the maternal concentration). Colchicine also distributes into breast milk at concentrations similar to those found in the maternal serum [see Pregnancy (8.1) and Nursing Mothers (8.3)].
Metabolism
Colchicine is demethylated to two primary metabolites, 2-O-demethylcolchicine and 3-O-demethylcolchicine (2- and 3-DMC, respectively) and one minor metabolite, 10-O-demethylcolchicine (also known as colchiceine). In vitro studies using human liver microsomes have shown that CYP3A4 is involved in the metabolism of colchicine to 2- and 3-DMC. Plasma levels of these metabolites are minimal (less than 5% of parent drug).
Elimination/Excretion
In healthy volunteers (n=12), 40% to 65% of 1 mg orally administered colchicine was recovered unchanged in urine. Enterohepatic recirculation and biliary excretion are also postulated to play a role in colchicine elimination. Following multiple oral doses (0.6 mg twice daily), the mean elimination half-lives in young healthy volunteers (mean age 25 to 28 years of age) is 26.6 to 31.2 hours. Colchicine is a substrate of P-gp.
Special Populations
There is no difference between men and women in the pharmacokinetic disposition of colchicine.
Elderly: A published report described the pharmacokinetics of 1 mg oral colchicine tablet in four elderly women compared to six young healthy males. The mean age of the four elderly women was 83 years (range 75 to 93), mean weight was 47 kg (38 to 61 kg) and mean creatinine clearance was 46 mL/min (range 25 to 75 mL/min). Mean peak plasma levels and AUC of colchicine were two times higher in elderly subjects compared to young healthy males.
A pharmacokinetic study using a single oral dose of one 0.6 mg colchicine tablet was conducted in young healthy subjects (n=20) between the ages of 18 and 30 years and elderly subjects (n=18) between the ages of 60 and 70 years. Elderly subjects in this study had a median age of 62 years and a mean (±SD) age of 62.83 ± 2.83 years. A statistically significant difference in creatinine clearance (mean ± SD) was found between the two age groups (132.56 ± 23.16 mL/min for young vs. 87.02 ± 17.92 mL/min for elderly subjects, respectively). The following pharmacokinetic parameter values (mean ± SD) were observed for colchicine in the young and elderly subjects, respectively: AUC0-inf (ng/hr/mL) 22.39 ± 6.95 and 25.01 ± 6.92; Cmax (ng/mL) 2.61 ± 0.71 and 2.56 ± 0.97; Tmax (hr) 1.38 ± 0.42 and 1.25 ± 0.43; apparent elimination half-life (hr) 24.92 ± 5.34 and 30.06 ± 10.78; and clearance (mL/min) 0.0321 ± 0.0091 and 0.0292 ± 0.0071.
Clinical studies with colchicine for prophylaxis and treatment of gout flares and for treatment of FMF did not include sufficient numbers of patients aged 65 years and older to determine whether they respond differently than younger patients. In general, dose selection for an elderly patient with gout should be cautious, reflecting the greater frequency of decreased renal function, concomitant disease or other drug therapy [see Dose Modification for Coadministration of Interacting Drugs (2.4) and Geriatric Use (8.5)].
Renal Impairment: Pharmacokinetics of colchicine in patients with mild and moderate renal impairment is not known. A published report described the disposition of colchicine (1 mg) in young adult men and women with FMF who had normal renal function or end-stage renal disease requiring dialysis. Patients with end-stage renal disease had 75% lower colchicine clearance (0.17 vs. 0.73 L/hr/kg) and prolonged plasma elimination half-life (18.8 hours vs. 4.4 hours) as compared to subjects with FMF and normal renal function [see Dose Modification in Renal Impairment (2.5) and Renal Impairment (8.6)].
Hepatic Impairment: Published reports on the pharmacokinetics of IV colchicine in patients with severe chronic liver disease, as well as those with alcoholic or primary biliary cirrhosis and normal renal function suggest wide interpatient variability. In some subjects with mild to moderate cirrhosis, the clearance of colchicine is significantly reduced and plasma half-life prolonged compared to healthy subjects. In subjects with primary biliary cirrhosis, no consistent trends were noted [see Dose Modification in Hepatic Impairment (2.6) and Hepatic Impairment (8.7)]. No pharmacokinetic data are available for patients with severe hepatic impairment (Child-Pugh C).
Drug Interactions
In Vitro Drug Interactions:In vitro studies in human liver microsomes have shown that colchicine is not an inhibitor or inducer of CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP2E1 or CYP3A4 activity.
In Vivo Drug Interactions: The effects of coadministration of other drugs with COLCRYS on Cmax, AUC and Cmin are summarized in Table 6 (effect of other drugs on colchicine) and Table 7 (effect of colchicine on other drugs). For information regarding clinical recommendations, see Table 1 in Dose Modification for Coadministration of Interacting Drugs [see Dose Modification for Coadministration of Interacting Drugs (2.4)].
|
Coadministered Drug |
Dose of Coadministered Drug (mg) |
Dose of COLCRYS (mg) |
N |
% Change in Colchicine Concentrations from Baseline
|
|
|
Cmax |
AUC0-t |
||||
|
Cyclosporine |
100 mg |
0.6 mg |
23 |
270.0 |
259.0 |
|
Clarithromycin |
250 mg twice daily, |
0.6 mg |
23 |
227.2 |
281.5 |
|
Ketoconazole |
200 mg twice daily, |
0.6 mg |
24 |
101.7 |
212.2 |
|
Ritonavir |
100 mg twice daily, |
0.6 mg |
18 |
184.4 |
296.0 |
|
Verapamil |
240 mg daily, |
0.6 mg |
24 |
40.1 |
103.3 |
|
Diltiazem |
240 mg daily, |
0.6 mg |
20 |
44.2 |
93.4 |
|
Azithromycin |
500 mg × 1 day, then |
0.6 mg |
21 |
21.6 |
57.1 |
|
Grapefruit juice |
240 mL twice daily, |
0.6 mg |
21 |
-2.55 |
-2.36 |
Estrogen-containing oral contraceptives: In healthy female volunteers given ethinyl estradiol and norethindrone (Ortho-Novum 1/35) coadministered with COLCRYS (0.6 mg twice daily × 14 days), hormone concentrations are not affected.
In healthy volunteers given theophylline coadministered with COLCRYS (0.6 mg twice daily × 14 days), theophylline concentrations were not affected.
|
Coadministered Drug |
Dose of Coadministered Drug (mg) |
Dose of COLCRYS (mg) |
N |
% Change in Coadministered Drug Concentrations from Baseline
|
|
|
Cmax |
AUC0-t |
||||
|
Theophylline |
300 mg (elixir) single dose |
0.6 mg twice daily × 14 days |
27 |
1.6 |
1.6 |
|
Ethinyl Estradiol (Ortho-Novum 1/35) |
21-day cycle (active treatment) + 7-day placebo |
0.6 mg twice daily × 14 days |
27* |
-6.7 |
-3.0†
|
|
Norethindrone (Ortho-Novum 1/35) |
0.94 |
-1.6†
|
|||
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Carcinogenicity studies of colchicine have not been conducted. Due to the potential for colchicine to produce aneuploid cells (cells with an unequal number of chromosomes), there is theoretically an increased risk of malignancy.
Mutagenesis
Colchicine was negative for mutagenicity in the bacterial reverse mutation assay. In a chromosomal aberration assay in cultured human white blood cells, colchicine treatment resulted in the formation of micronuclei. Since published studies demonstrated that colchicine induces aneuploidy from the process of mitotic nondisjunction without structural DNA changes, colchicine is not considered clastogenic, although micronuclei are formed.
Impairment of Fertility
No studies of colchicine effects on fertility were conducted with COLCRYS. However, published nonclinical studies demonstrated that colchicine-induced disruption of microtubule formation affects meiosis and mitosis. Reproductive studies also reported abnormal sperm morphology and reduced sperm counts in males, and interference with sperm penetration, second meiotic division and normal cleavage in females when exposed to colchicine. Colchicine administered to pregnant animals resulted in fetal death and teratogenicity. These effects were dose-dependent, with the timing of exposure critical for the effects on embryofetal development. The nonclinical doses evaluated were generally higher than an equivalent human therapeutic dose, but safety margins for reproductive and developmental toxicity could not be determined.
Case reports and epidemiology studies in human male subjects on colchicine therapy indicated that infertility from colchicine is rare. A case report indicated that azoospermia was reversed when therapy was stopped. Case reports and epidemiology studies in female subjects on colchicine therapy have not established a clear relationship between colchicine use and female infertility. However, since the progression of FMF without treatment may result in infertility, the use of colchicine needs to be weighed against the potential risks.
14 CLINICAL STUDIES
The evidence for the efficacy of colchicine in patients with chronic gout is derived from the published literature. Two randomized clinical trials assessed the efficacy of colchicine 0.6 mg twice a day for the prophylaxis of gout flares in patients with gout initiating treatment with urate-lowering therapy. In both trials, treatment with colchicine decreased the frequency of gout flares.
The efficacy of a low-dosage regimen of oral colchicine (COLCRYS total dose 1.8 mg over one hour) for treatment of gout flares was assessed in a multicenter, randomized, double-blind, placebo-controlled, parallel group, one week, dose-comparison study. Patients meeting American College of Rheumatology criteria for gout were randomly assigned to three groups: high-dose colchicine (1.2 mg, then 0.6 mg hourly × 6 hours [4.8 mg total]); low-dose colchicine (1.2 mg, then 0.6 mg in 1 hour [1.8 mg total] followed by five placebo doses hourly); or placebo (two capsules, then one capsule hourly × 6 hours). Patients took the first dose within 12 hours of the onset of the flare and recorded pain intensity (11-point Likert scale) and adverse events over 72 hours. The efficacy of colchicine was measured based on response to treatment in the target joint, using patient self-assessment of pain at 24 hours following the time of first dose as recorded in the diary. A responder was one who achieved at least a 50% reduction in pain score at the 24-hour postdose assessment relative to the pretreatment score and did not use rescue medication prior to the actual time of 24-hour postdose assessment.
Rates of response were similar for the recommended low-dose treatment group (38%) and the nonrecommended high-dose group (33%) but were higher as compared to the placebo group (16%) as shown in Table 8.
|
COLCRYS Dose Responders n (%) |
Placebo
|
% Differences in Proportion |
||
|
Low-Dose
|
High-Dose
|
Low-Dose vs Placebo
|
High-Dose vs Placebo
|
|
|
28 (38%) |
17 (33%) |
9 (16%) |
22 (8, 37) |
17 (1, 33) |
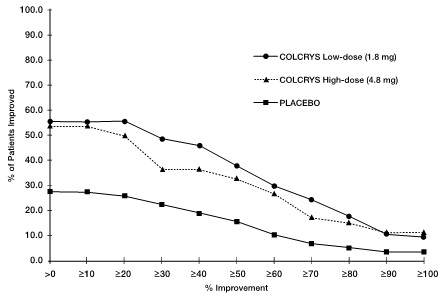
Figure 1 shows the percentage of patients achieving varying degrees of improvement in pain from baseline at 24 hours.
Figure 1
Pain Relief on Low and High Doses of COLCRYS and Placebo (Cumulative)
The evidence for the efficacy of colchicine in patients with FMF is derived from the published literature. Three randomized, placebo-controlled studies were identified. The three placebo-controlled studies randomized a total of 48 adult patients diagnosed with FMF and reported similar efficacy endpoints as well as inclusion and exclusion criteria.
One of the studies randomized 15 patients with FMF to a six-month crossover study during which five patients discontinued due to study noncompliance. The 10 patients completing the study experienced five attacks over the course of 90 days while treated with colchicine compared to 59 attacks over the course of 90 days while treated with placebo. Similarly, the second study randomized 22 patients with FMF to a four-month crossover study during which nine patients discontinued due to lack of efficacy while receiving placebo or study noncompliance. The 13 patients completing the study experienced 18 attacks over the course of 60 days while treated with colchicine compared to 68 attacks over the course of 60 days while treated with placebo. The third study was discontinued after an interim analysis of six of the 11 patients enrolled had completed the study; results could not be confirmed.
Open-label experience with colchicine in adults and children with FMF is consistent with the randomized, controlled trial experience and was utilized to support information on the safety profile of colchicine and for dosing recommendations.
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
See FDA-approved Medication Guide.
17.1 Dosing Instructions
Patients should be advised to take COLCRYS as prescribed, even if they are feeling better. Patients should not alter the dose or discontinue treatment without consulting with their doctor. If a dose of COLCRYS is missed:
- •
- For treatment of a gout flare when the patient is not being dosed for prophylaxis, take the missed dose as soon as possible.
- •
- For treatment of a gout flare during prophylaxis, take the missed dose immediately, wait 12 hours, then resume the previous dosing schedule.
- •
- For prophylaxis without treatment for a gout flare, or FMF, take the dose as soon as possible and then return to the normal dosing schedule. However, if a dose is skipped the patient should not double the next dose.
17.2 Fatal Overdose
Instruct patient that fatal overdoses, both accidental and intentional, have been reported in adults and children who have ingested colchicine. COLCRYS should be kept out of the reach of children.
17.3 Blood Dyscrasias
Patients should be informed that bone marrow depression with agranulocytosis, aplastic anemia and thrombocytopenia may occur with COLCRYS.
17.4 Drug and Food Interactions
Patients should be advised that many drugs or other substances may interact with COLCRYS and some interactions could be fatal. Therefore, patients should report to their healthcare provider all of the current medications they are taking and check with their healthcare provider before starting any new medications, particularly antibiotics. Patients should also be advised to report the use of nonprescription medication or herbal products. Grapefruit and grapefruit juice may also interact and should not be consumed during COLCRYS treatment.
17.5 Neuromuscular Toxicity
Patients should be informed that muscle pain or weakness, tingling or numbness in fingers or toes may occur with COLCRYS alone or when it is used with certain other drugs. Patients developing any of these signs or symptoms must discontinue COLCRYS and seek medical evaluation immediately.
MEDICATION GUIDE
COLCRYS
(KOL-kris)
(colchicine) tablets
Read the Medication Guide that comes with COLCRYS before you start taking it and each time you get a refill. There may be new information. This Medication Guide does not take the place of talking to your healthcare provider about your medical condition or treatment. You and your healthcare provider should talk about COLCRYS when you start taking it and at regular checkups.
What is the most important information that I should know about COLCRYS?
COLCRYS can cause serious side effects or death if levels of COLCRYS are too high in your body.
- •
- Taking certain medicines with COLCRYS can cause your level of COLCRYS to be too high, especially if you have kidney or liver problems.
- •
- Tell your healthcare provider about all your medical conditions, including if you have kidney or liver problems. Your dose of COLCRYS may need to be changed.
- •
- Tell your healthcare provider about all the medicines you take, including prescription and nonprescription medicines, vitamins and herbal supplements.
- •
- Even medicines that you take for a short period of time, such as antibiotics, can interact with COLCRYS and cause serious side effects or death.
- •
- Talk to your healthcare provider or pharmacist before taking any new medicine.
- •
- Especially tell your healthcare provider if you take:
|
|
|
|
Ask your healthcare provider or pharmacist if you are not sure if you take any of the medicines listed above. This is not a complete list of all the medicines that can interact with COLCRYS.
- •
- Know the medicines you take. Keep a list of them and show it to your healthcare provider and pharmacist when you get a new medicine.
- •
- Keep COLCRYS out of the reach of children.
What is COLCRYS?
COLCRYS is a prescription medicine used to:
- •
- prevent and treat gout flares in adults
- •
- treat familial Mediterranean fever (FMF) in adults and children age 4 or older
COLCRYS is not a pain medicine, and it should not be taken to treat pain related to other conditions unless specifically prescribed for those conditions.
Who should not take COLCRYS?
Do not take COLCRYS if you have liver or kidney problems and you take certain other medicines. Serious side effects, including death, have been reported in these patients even when taken as directed. See "What is the most important information that I should know about COLCRYS?"
What should I tell my healthcare provider before starting COLCRYS?
See "What is the most important information that I should know about COLCRYS?"
Before you take COLCRYS, tell your healthcare provider about all your medical conditions, including if you:
- •
- have liver or kidney problems.
- •
- are pregnant or plan to become pregnant. It is not known if COLCRYS will harm your unborn baby. Talk to your healthcare provider if you are pregnant or plan to become pregnant.
- •
- are breastfeeding or plan to breastfeed. COLCRYS passes into your breast milk. You and your healthcare provider should decide if you will take COLCRYS or breastfeed. If you take COLCRYS and breastfeed, you should talk to your child's healthcare provider about how to watch for side effects in your child.
Tell your healthcare provider about all the medicines you take, including ones that you may only be taking for a short time, such as antibiotics. See "What is the most important information that I should know about COLCRYS?" Do not start a new medicine without talking to your healthcare provider.
Using COLCRYS with certain other medicines, such as cholesterol-lowering medications and digoxin, can affect each other, causing serious side effects. Your healthcare provider may need to change your dose of COLCRYS. Talk to your healthcare provider about whether the medications you are taking might interact with COLCRYS and what side effects to look for.
How should I take COLCRYS?
- •
- Take COLCRYS exactly as your healthcare provider tells you to take it. If you are not sure about your dosing, call your healthcare provider.
- •
- COLCRYS can be taken with or without food.
- •
- If you take too much COLCRYS, go to the nearest hospital emergency room right away.
- •
- Do not stop taking COLCRYS even if you start to feel better, unless your healthcare provider tells you.
- •
- Your healthcare provider may do blood tests while you take COLCRYS.
- •
- If you take COLCRYS daily and you miss a dose, then take it as soon as you remember. If it is almost time for your next dose, just skip the missed dose. Take the next dose at your regular time. Do not take two doses at the same time.
- •
- If you have a gout flare while taking COLCRYS daily, report this to your healthcare provider.
What should I avoid while taking COLCRYS?
- •
- Avoid eating grapefruit or drinking grapefruit juice while taking COLCRYS. It can increase your chances of getting serious side effects.
What are the possible side effects of COLCRYS?
COLCRYS can cause serious side effects or even cause death. See "What is the most important information that I should know about COLCRYS?"
Get medical help right away if you have:
- •
- Muscle weakness or pain
- •
- Numbness or tingling in your fingers or toes
- •
- Unusual bleeding or bruising
- •
- Increased infections
- •
- Feel weak or tired
- •
- Pale or gray color to your lips, tongue or palms of your hands
- •
- Severe diarrhea or vomiting
Gout Flares: The most common side effect of COLCRYS in people who have gout flares is diarrhea.
FMF: The most common side effects of COLCRYS in people who have FMF are abdominal pain, diarrhea, nausea and vomiting.
Tell your healthcare provider if you have any side effect that bothers you or that does not go away.
These are not all of the possible side effects of COLCRYS. For more information, ask your healthcare provider or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store COLCRYS?
- •
- Store COLCRYS at room temperature between 68°F and 77°F (20°C and 25°C).
- •
- Keep COLCRYS in a tightly closed container.
- •
- Keep COLCRYS out of the light.
Keep COLCRYS and all medicines out of the reach of children.
General Information about COLCRYS
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use COLCRYS for a condition for which it was not prescribed. Do not give COLCRYS to other people, even if they have the same symptoms that you have. It may harm them. This Medication Guide summarizes the most important information about COLCRYS. If you would like more information, talk with your healthcare provider. You can ask your healthcare provider or pharmacist for information about COLCRYS that is written for healthcare professionals.
For more information, go to www.COLCRYS.com or call 1-877-825-3327.
What are the ingredients in COLCRYS?
Active Ingredient: colchicine.
Inactive Ingredients: carnauba wax, FD&C blue #2, FD&C red #40, hypromellose, lactose monohydrate, magnesium stearate, microcrystalline cellulose, polydextrose, polyethylene glycol, pregelatinized starch, sodium starch glycolate, titanium dioxide and triacetin.
This Medication Guide has been approved by the U.S. Food and Drug Administration.
Distributed by:
Takeda Pharmaceuticals America, Inc.
Deerfield, IL 60015
Repackaged by:
Proficient Rx LP
Thousand Oaks, CA 91320
Revised: November 2012
COLCRYS is a trademark of Takeda Pharmaceuticals U.S.A., Inc., registered with the U.S. Patent and Trademark Office and used under license by Takeda Pharmaceuticals America, Inc.
All other trademarks are the property of their respective owners.
COL243 R1