FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
Verkazia ophthalmic emulsion is indicated for the treatment of vernal keratoconjunctivitis (VKC) in children and adults.
2 DOSAGE AND ADMINISTRATION
2.1 General Dosing Information
Gently shake the single-dose vial several times to obtain a uniform, white, opaque emulsion before use.
Contact lenses should be removed before applying Verkazia and may be reinserted
15 minutes after administration.
If a dose is missed, treatment should be continued as normal, at the next scheduled administration.
If more than one topical ophthalmic product is being used, administer the eye drops at least 10 minutes apart to avoid diluting products. Administer Verkazia 10 minutes prior to using any eye ointment, gel or other viscous eye drops.
Discard the vial immediately after use.
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
Since clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In the VEKTIS study, a multicenter, randomized, double-masked, placebo‑controlled trial, a total of 57 patients received Verkazia dosed four times a day (QID) for 4 months. Forty-two (42) patients received Verkazia in an 8 month extension, safety follow-up of the VEKTIS study. In the NOVATIVE study, a multicenter, randomized, double-masked, placebo‑controlled trial, 39 patients received Verkazia 1 mg/mL dosed QID for one month. A total of 53 patients received Verkazia 1 mg/mL QID during a 3-month safety follow‑up. The majority of the treated patients were male (79%). The most common adverse reactions reported in greater than 5% of patients were eye pain (12%) and eye pruritus (8%) which were usually transitory and occurred during instillation (Table 1).
Table 1: Adverse Reactions Reported in ≥ 1% of Patients Receiving Verkazia
|
(N=135) |
|
|
Eye Disorders |
|
|
Eye pain a |
12% |
|
Eye pruritus b |
8% |
|
Ocular discomfort c |
6% |
|
Visual acuity reduced |
5% |
|
Ocular hyperemia |
4% |
|
Systemic |
|
|
Cough |
5% |
|
Headache |
4% |
|
Upper respiratory tract infection |
2% |
|
a Including eye pain and instillation site pain b Including eye pruritus and instillation site pruritus c Including foreign body sensation and ocular discomfort |
|
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no adequate and well-controlled studies of Verkazia administration in pregnant women to inform a drug-associated risk. Oral administration of cyclosporine to pregnant rats or rabbits did not produce teratogenicity at clinically relevant doses [see Data].
Data
Animal Data
Oral administration of cyclosporine oral solution (USP) to pregnant rats or rabbits was teratogenic at maternally toxic doses of 30 mg/kg/day in rats and 100 mg/kg/day in rabbits, as indicated by increased pre- and postnatal mortality, reduced fetal weight and skeletal retardations. These doses (normalized to body weight) were approximately 320 and 2150 times higher than the daily maximum recommended human ophthalmic dose (MRHOD) of 0.015 mg/kg/day, respectively.
No adverse embryofetal effects were observed in rats or rabbits receiving cyclosporine during organogenesis at oral doses up to 17 mg/kg/day or 30 mg/kg/day, respectively (approximately 185 and 650 times higher than the MRHOD, respectively).
An oral dose of 45 mg/kg/day cyclosporine (approximately 485 times higher than MRHOD) administered to rats from Day 15 of pregnancy until Day 21 postpartum produced maternal toxicity and an increase in postnatal mortality in offspring. No adverse effects in mothers or offspring were observed at oral doses of up to
15 mg/kg/day (160 times greater than MRHOD).
8.2 Lactation
Risk Summary
There is no information regarding the presence of cyclosporine in human milk following topical administration or on the effect of Verkazia on the breastfed infants and milk production. Administration of oral cyclosporine to rats during lactation did not produce adverse effects in offspring at clinically relevant doses [see Pregnancy ( 8.1)] . The development and health benefits of breastfeeding should be considered along with the mother’s clinical need for Verkazia and any potential adverse effects on the breast-fed child from cyclosporine.
8.3 Females and Males of Reproductive Potential
Infertility
There are no data on the effects of Verkazia on human fertility. No impairment of fertility has been reported in animals receiving intravenous cyclosporine [see Impairment of Fertility ( 13.1) ].
11 DESCRIPTION
Verkazia (cyclosporine ophthalmic emulsion) 0.1% contains a topical calcineurin inhibitor immunosuppressant. Cyclosporine is a white or almost white powder. Cyclosporine’s chemical name is Cyclo[[( E)-(2 S,3 R,4 R)-3-hydroxy-4-methyl-2-(methylamino)-6-octenoyl]-L-2-aminobutyryl- N-methylglycyl- N-methyl-L-leucyl-L-valyl- N-methyl-L-leucyl-L-alanyl-D-alanyl- N-methyl-L-leucyl- N-methyl-L-leucyl- N-methyl-L-valyl] and it has the following structure:
Structural Formula
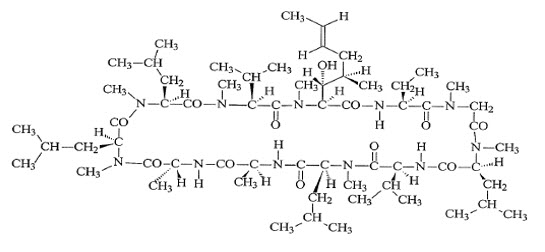
Formula: C 62H 111N 11O 12 Mol. Wt.: 1202.61
Verkazia ophthalmic emulsion is a sterile, unpreserved topical emulsion. It appears as a milky-white homogeneous emulsion. It has an osmolality of approximately 265 mOsmol/kg and a pH of 5-7. Each mL of Verkazia ophthalmic emulsion contains: Active: Cyclosporine 1 mg/mL. Inactives: Cetalkonium chloride, Glycerol, Medium-chain triglycerides, Poloxamer 188, Sodium Hydroxide to adjust pH, Tyloxapol and Water for Injection.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Cyclosporine is a calcineurin inhibitor immunosuppressant agent when administered systemically. Following ocular administration, cyclosporine is thought to act by blocking the release of pro-inflammatory cytokines such as IL-2. The exact mechanism of action in the treatment of VKC is not known.
12.3 Pharmacokinetics
Blood concentrations of cyclosporine were measured in 55 patients administered 1 drop of Verkazia 4 times daily in the VEKTIS Study. Blood samples were collected before administration and after 2, 4, and 12 months of administration of Verkazia. Among those patients that had quantifiable levels of cyclosporine during the study, the maximum blood level of cyclosporine was 0.67 ng/mL.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Systemic carcinogenicity studies were carried out in male and female mice and rats. In the 78-week oral (diet) mouse study, at doses of 1, 4, and 16 mg/kg/day, evidence of a statistically significant trend was found for lymphocytic lymphomas in females, and the incidence of hepatocellular carcinomas in mid-dose males significantly exceeded the control value. The low dose in mice is approximately 5 times greater than MRHOD.
In the 24-month oral (diet) rat study, conducted at 0.5, 2, and 8 mg/kg/day, pancreatic islet cell adenomas significantly exceeded the control rate in the low dose level. The hepatocellular carcinomas and pancreatic islet cell adenomas were not dose related. The low dose in rats is approximately 5 times greater than MRHOD.
Mutagenesis
In genetic toxicity tests, cyclosporine has not been found to be mutagenic/genotoxic in the Ames Test, the V79-HGPRT Test, the micronucleus test in mice and Chinese hamsters, the chromosome-aberration tests in Chinese hamster bone-marrow, the mouse dominant lethal assay, and the DNA-repair test in sperm from treated mice. Cyclosporine was positive in an in vitro sister chromatid exchange (SCE) assay using human lymphocytes.
Impairment of Fertility
Oral administration of cyclosporine to rats for 12 weeks (male) and 2 weeks (female) prior to mating produced no adverse effects on fertility at doses up to 15 mg/kg/day
(160 times higher than MRHOD).
14 CLINICAL STUDIES
The safety and efficacy of Verkazia for the treatment of VKC was evaluated in two randomized, multi-center, double-masked, vehicle-controlled, clinical trials (VEKTIS Study NCT01751126 and NOVATIVE Study NCT00328653).
In the VEKTIS study, patients with severe VKC were randomized to four times daily of Verkazia 1 mg/mL or two times daily (BID) of Verkazia 1 mg/mL and vehicle group for the first 4 months (Period 1). Similarly, in the NOVATIVE study, patients with moderate to severe VKC were randomized to QID of Verkazia 1 mg/mL or QID of cyclosporine ophthalmic emulsion 0.5 mg/mL and vehicle group for the first 1 month (Period 1). In both studies, patients randomized to the vehicle group were switched to Verkazia (QID or BID) from Month 4 to Month 12 in VEKTIS Study and to cyclosporine ophthalmic emulsion 0.5 mg/mL QID or 1 mg/mL from Month 1 to Month 4 in NOVATIVE Study (Period 2).
A total of 168 and 118 patients were enrolled in the VEKTIS and NOVATIVE studies for the efficacy analyses, respectively. Patients’ age ranged from 4 through 17 years (mean age 9 years) in VEKTIS and 4 through 21 years (mean age 9 years) in NOVATIVE, with most patients being between 4 and 11 years of age (76% in VEKTIS and 80% in NOVATIVE) and male (79% in VEKTIS and 81% in NOVATIVE). Most of the patients had both limbal and tarsal forms of VKC (65% in VEKTIS and 74% in NOVATIVE). In both studies, patients had experienced VKC for a mean of 3 years prior to enrollment and all patients had a history of at least one recurrence of VKC in the year prior to study entry.
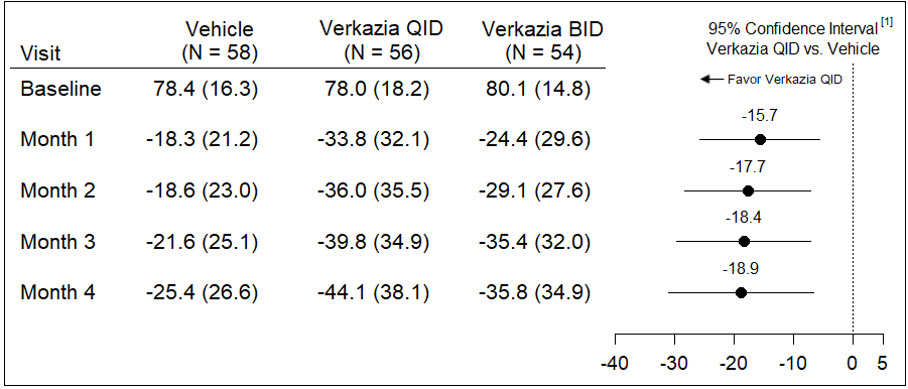
In the VEKTIS study, key efficacy evaluation was based on the change in corneal fluorescein staining (CFS) score and in itching score over 4 months. The results at each month are presented in Table 2 for the CFS score and in Table 3 for the Itching score.
Table 2: Efficacy Results of the Mean Change in Keratitis Score from Baseline at Each Visit (Full Analysis Set)
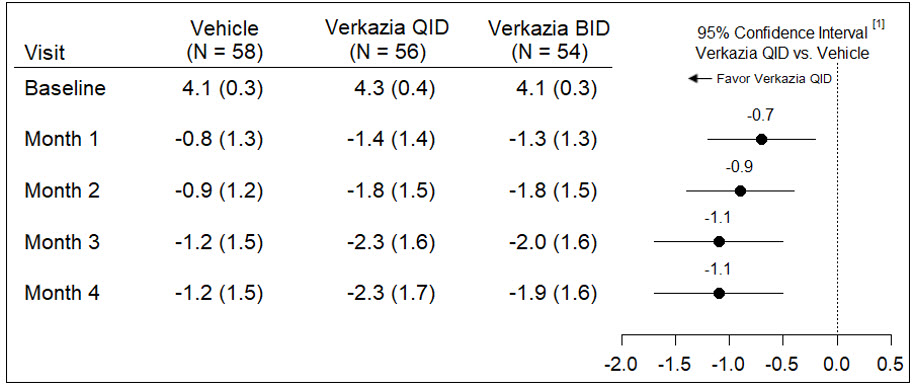
[1] Treatment differences (numbers in the middle of the horizontal lines) and 95% confidence intervals (horizontal lines) are based on ANCOVA model including baseline CFS score and the proportion of time potentially spent in taking study medication during the VKC season as covariate. For subjects that received rescue therapy during the study, all post-rescue data were imputed by the last available data observed prior to rescue initiation.
Note 1: CFS score was measured at each month using a 5-point scale (0 = no stain, and 5 = more stain).
Note 2: The Full Analysis Set included all randomized subjects that received at least one drop of study medication.
Table 3: Efficacy Results of the Mean Change in Itching Score from Baseline at Each Visit (Full Analysis Set)
[1] Treatment differences (numbers in the middle of the horizontal lines) and 95% confidence intervals (horizontal lines) are based on ANCOVA model including baseline Itching score and the proportion of time potentially spent in taking study medication as covariate. For subjects that received rescue therapy during the study, all post-rescue data were imputed by the last available data observed prior to rescue initiation.
Note 1: Itching score at each visit was measured using a Visual Analogue Scale (0 = no itch to 100 = maximal itch).
Analyses of the CFS score and Itching score at Month 1 of the efficacy evaluation period in the NOVATIVE Study also provided supporting evidence.
16 HOW SUPPLIED/STORAGE AND HANDLING
Verkazia (cyclosporine ophthalmic emulsion) 0.1% is packaged in low-density polyethylene single-dose vials. Each vial contains 0.3 mL fill; 5 vials are packaged in an aluminum pouch; 24 pouches are packaged in a box of 120 vials.
The entire contents of each box of 120 vials must be dispensed intact.
120 Single-Dose Vials 0.3 mL each — NDC 65086-001-12
Storage: Do not freeze Verkazia. Store at 20°C to 25°C (68°F to 77°F). After opening the aluminum pouch, the single-dose vial should be kept in the pouch to protect from light and avoid evaporation. Any opened individual single-dose vial with any remaining emulsion should be discarded immediately after use.
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Instructions for Use).
Handling the Vial
Advise patients to not allow the tip of the vial to touch the eye or any surface, as this may contaminate the emulsion. Advise patients to not touch the vial tip to their eye to avoid the potential for injury to the eye [see Warnings and Precautions ( 5.1)].
Use with Contact Lenses
Advise patients that contact lenses should be removed before administering Verkazia and to wait at least 15 minutes after instillation of the dose before reinserting the contact lenses [see Dosage and Administration ( 2.1)] .
Administration
Advise patients that the emulsion from one individual single-dose vial is to be used immediately after opening for administration to one or both eyes, and the remaining contents should be discarded immediately after administration [see Dosage and Administration ( 2) ].
Missed Dose
If a dose is missed, Verkazia should be continued as normal at the next dose as planned. [see Dosage and Administration ( 2.1)] .
Manufactured for: Santen Inc.
Manufactured by: ExcelVision
Distributed by:
Santen Inc.
6401 Hollis Street, Suite 125
Emeryville, CA 94608
United States
INSTRUCTIONS FOR USE
INSTRUCTIONS FOR USE
Verkazia® [ver ka' zee ah]
(cyclosporine ophthalmic emulsion, 0.1%)
for topical ophthalmic use
Read this Instructions for Use before you start using Verkazia and each time you get a refill. There may be new information. This leaflet does not take the place of talking to your healthcare provider about your medical condition or your treatment.
Important Information You Need to Know Before Using Verkazia
- Verkazia is for use in the eye.
- Verkazia is supplied as 5 single-dose vials packaged in a foil pouch.
- If you are using any other eye drops, use each eye drop at least 10 minutes apart from each other, including Verkazia.
- If you are using any eye ointment, gel or other thicker in consistency (viscous) eye drops, use Verkazia 10 minutes before using them.
- Do not let the tip of the Verkazia vial touch your eye or any other surfaces to avoid contamination or injury to your eye.
- Adults should help children when starting treatment. Adults should continue to help until the child is able to properly use Verkazia alone. Use 1 drop of Verkazia in the affected eye or eyes, 4 times a day (morning, noon, afternoon and evening). There is enough medicine in one vial to use in both eyes. Throw away (discard) the vial immediately after use.
- If you forget to use Verkazia, skip that dose and continue with the next dose as planned.
- Contact lenses should be taken out before using Verkazia and wait at least 15 minutes after giving the dose before putting the contact lenses back into your eyes.
- Do not use Verkazia after the expiration date (EXP) appearing on the outer carton, pouch and single-dose vial. The expiration date is the last day of that month.
Using Verkazia
Follow the instructions ( Step 1 to Step 12) each time you use Verkazia. If there is anything that you do not understand, ask your healthcare provider.
Step 1. Wash your hands.
Step 2. Open the aluminum pouch, which contains 5 single-dose vials.
Step 3. Take 1 vial from the aluminum pouch. Leave the remaining vials in the pouch.
Step 4. Gently shake the vial.
Step 5. Twist off the cap (see Figure A).

Figure A
Step 6. Pull down your lower eyelid (see Figure B).

Figure B
Step 7. Tilt your head back and look up.
Step 8. Gently squeeze 1 drop of the medicine onto your eye. Make sure that the tip of the vial does not touch your eye. If a drop misses your eye, try again.
Step 9. Blink a few times so that the medicine spreads across your eye.
Step 10. After using Verkazia, press the corner of your eye closest to your nose and gently close the eyelid for 2 minutes (see Figure C).
Figure C
Step 11. If you need to use drops in both eyes, repeat Steps 6 to 10 for your other eye. There is enough medicine in one single-dose vial to use in both eyes.
Step 12. Throw away the vial with any remaining medicine after use.
Storing Verkazia
- Store Verkazia at room temperature between 68°F to 77°F (20°C to 25°C).
- Do not freeze.
- After opening the pouch, keep vials in the pouch to protect from light and evaporation.
Throwing away Verkazia
- Any open vial with any medicine left over should be thrown out right after use.
Talk with your healthcare provider if you want more information about Verkazia.
Distributed by:
Santen Incorporated
6401 Hollis St., Suite 125
Emeryville, CA 94608
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Approved: June 2021