FULL PRESCRIBING INFORMATION
1 INDICATIONS & USAGE
1.1 Acute Coronary Syndrome (ACS)
Eptifibatide injection is indicated to decrease the rate of a combined endpoint of death or new myocardial infarction (MI) in patients with ACS (unstable angina [UA]/non-ST-elevation myocardial infarction [NSTEMI]), including patients who are to be managed medically and those undergoing percutaneous coronary intervention (PCI).
1.2 Percutaneous Coronary Intervention (PCI)
Eptifibatide injection is indicated to decrease the rate of a combined endpoint of death, new MI, or need for urgent intervention in patients undergoing PCI, including those undergoing intracoronary stenting [see Clinical Studies (14.1, 14.2)].
2 DOSAGE & ADMINISTRATION
Before infusion of eptifibatide injection, the following laboratory tests should be performed to identify pre-existing hemostatic abnormalities: hematocrit or hemoglobin, platelet count, serum creatinine, and PT/aPTT. In patients undergoing PCI, the activated clotting time (ACT) should also be measured.
The activated partial thromboplastin time (aPTT) should be maintained between 50 and 70 seconds unless PCI is to be performed. In patients treated with heparin, bleeding can be minimized by close monitoring of the aPTT and ACT.
2.1 Dosage in Acute Coronary Syndrome (ACS)
|
Indication |
Normal Renal Function |
Creatinine Clearance <50 mL/min |
| Patients with ACS | 180 mcg/kg intravenous (IV) bolus as soon as possible after diagnosis, followed by continuous infusion of 2 mcg/kg/min | 180 mcg/kg IV bolus as soon as possible after diagnosis, followed by continuous infusion of 1 mcg/kg/min |
|
||
Eptifibatide injection should be given concomitantly with heparin dosed to achieve the following parameters:
During Medical Management: Target aPTT 50 to 70 seconds
- If weight greater than or equal to 70 kg, 5,000 unit bolus followed by infusion of 1,000 units/h.
- If weight less than 70 kg, 60 units/kg bolus followed by infusion of 12 units/kg/h.
During PCI: Target ACT 200 to 300 seconds
- If heparin is initiated prior to PCI, additional boluses during PCI to maintain an ACT target of 200 to 300 seconds.
- Heparin infusion after the PCI is discouraged.
2.2 Dosage in Percutaneous Coronary Intervention (PCI)
|
Indication |
Normal Renal Function |
Creatinine Clearance <50 mL/min |
| Patients with PCI | 180 mcg/kg IV bolus immediately before PCI followed by continuous infusion of 2 mcg/kg/min and a second bolus of 180 mcg/kg (given 10 minutes after the first bolus) | 180 mcg/kg IV bolus immediately before PCI followed by continuous infusion of 1 mcg/kg/min and a second bolus of 180 mcg/kg (given 10 minutes after the first bolus) |
|
||
- Eptifibatide injection should be given concomitantly with heparin to achieve a target ACT of 200 to 300 seconds. Administer 60 units/kg bolus initially in patients not treated with heparin within 6 hours prior to PCI.
- Additional boluses during PCI to maintain ACT within target.
- Heparin infusion after the PCI is strongly discouraged.
Patients requiring thrombolytic therapy should discontinue eptifibatide injection.
2.3 Important Administration Instructions
- Inspect eptifibatide injection for particulate matter and discoloration prior to administration, whenever solution and container permit.
- May administer eptifibatide injection in the same intravenous line as alteplase, atropine, dobutamine, heparin, lidocaine, meperidine, metoprolol, midazolam, morphine, nitroglycerin, or verapamil. Do not administer eptifibatide injection through the same intravenous line as furosemide.
- May administer eptifibatide injection in the same IV line with 0.9% NaCl or 0.9% NaCl/5% dextrose. With either vehicle, the infusion may also contain up to 60 mEq/L of potassium chloride.
- Withdraw the bolus dose(s) of eptifibatide injection from the 10 mL vial into a syringe. Administer the bolus dose(s) by IV push.
- Immediately following the bolus dose administration, initiate a continuous infusion of eptifibatide injection. When using an intravenous infusion pump, administer eptifibatide injection undiluted directly from the 100 mL vial. Spike the 100 mL vial with a vented infusion set. Center the spike within the circle on the stopper top.
- Discard any unused portion left in the vial.
Administer eptifibatide injection by volume according to patient weight (see Table 1).
Table 1: Eptifibatide Injection Dosing Charts by Weight
|
Patient Weight |
180 mcg/kg Bolus Volume |
2 mcg/kg/min Infusion Volume (CrCl ≥50 mL/min) |
1 mcg/kg/min Infusion Volume (CrCl <50 mL/min) |
|||
|
(kg) |
(lb) |
(from 2 mg/mL vial) |
(from 2 mg/mL 100 mL vial) |
(from 0.75 mg/mL 100 mL vial) |
(from 2 mg/mL 100 mL vial) |
(from 0.75 mg/mL 100 mL vial) |
|
37 to 41 42 to 46 47 to 53 54 to 59 60 to 65 66 to 71 72 to 78 79 to 84 85 to 90 91 to 96 97 to 103 104 to 109 110 to 115 116 to 121 >121 |
81 to 91 92 to 102 103 to 117 118 to 130 131 to 143 144 to 157 158 to 172 173 to 185 186 to 198 199 to 212 213 to 227 228 to 240 241 to 253 254 to 267 >267 |
3.4 mL 4 mL 4.5 mL 5 mL 5.6 mL 6.2 mL 6.8 mL 7.3 mL 7.9 mL 8.5 mL 9 mL 9.5 mL 10.2 mL 10.7 mL 11.3 mL |
2 mL/h 2.5 mL/h 3 mL/h 3.5 mL/h 3.8 mL/h 4 mL/h 4.5 mL/h 5 mL/h 5.3 mL/h 5.6 mL/h 6 mL/h 6.4 mL/h 6.8 mL/h 7 mL/h 7.5 mL/h |
6 mL/h 7 mL/h 8 mL/h 9 mL/h 10 mL/h 11 mL/h 12 mL/h 13 mL/h 14 mL/h 15 mL/h 16 mL/h 17 mL/h 18 mL/h 19 mL/h 20 mL/h |
1 mL/h 1.3 mL/h 1.5 mL/h 1.8 mL/h 1.9 mL/h 2 mL/h 2.3 mL/h 2.5 mL/h 2.7 mL/h 2.8 mL/h 3 mL/h 3.2 mL/h 3.4 mL/h 3.5 mL/h 3.7 mL/h |
3 mL/h 3.5 mL/h 4 mL/h 4.5 mL/h 5 mL/h 5.5 mL/h 6 mL/h 6.5 mL/h 7 mL/h 7.5 mL/h 8 mL/h 8.5 mL/h 9 mL/h 9.5 mL/h 10 mL/h |
3 DOSAGE FORMS & STRENGTHS
- Injection: 20 mg of eptifibatide in 10 mL (2 mg/mL), for intravenous bolus
4 CONTRAINDICATIONS
Treatment with eptifibatide injection is contraindicated in patients with:
- A history of bleeding diathesis, or evidence of active abnormal bleeding within the previous 30 days
- Severe hypertension (systolic blood pressure >200 mm Hg or diastolic blood pressure >110 mm Hg) not adequately controlled on antihypertensive therapy
- Major surgery within the preceding 6 weeks
- History of stroke within 30 days or any history of hemorrhagic stroke
- Current or planned administration of another parenteral GP IIb/IIIa inhibitor
- Dependency on renal dialysis
- Hypersensitivity to eptifibatide injection or any component of the product (hypersensitivity reactions that occurred included anaphylaxis and urticaria).
5 WARNINGS AND PRECAUTIONS
5.1 Bleeding
Bleeding is the most common complication encountered during eptifibatide injection therapy. Administration of eptifibatide injection is associated with an increase in major and minor bleeding, as classified by the criteria of the Thrombolysis in Myocardial Infarction Study group (TIMI) [see Adverse Reactions (6.1)]. Most major bleeding associated with eptifibatide injection has been at the arterial access site for cardiac catheterization or from the gastrointestinal or genitourinary tract. Minimize the use of arterial and venous punctures, intramuscular injections, and the use of urinary catheters, nasotracheal intubation, and nasogastric tubes. When obtaining intravenous access, avoid non-compressible sites (e.g., subclavian or jugular veins).
Use of Thrombolytics, Anticoagulants, and Other Antiplatelet Agents
Risk factors for bleeding include older age, a history of bleeding disorders, and concomitant use of drugs that increase the risk of bleeding (thrombolytics, oral anticoagulants, nonsteroidal anti-inflammatory drugs, and P2Y12 inhibitors). Concomitant treatment with other inhibitors of platelet receptor glycoprotein (GP) IIb/IIIa should be avoided. In patients treated with heparin, bleeding can be minimized by close monitoring of the aPTT and ACT [see Dosage and Administration (2)].
Care of the Femoral Artery Access Site in Patients Undergoing Percutaneous Coronary Intervention (PCI)
In patients undergoing PCI, treatment with eptifibatide injection is associated with an increase in major and minor bleeding at the site of arterial sheath placement. After PCI, eptifibatide infusion should be continued until hospital discharge or up to 18 to 24 hours, whichever comes first. Heparin use is discouraged after the PCI procedure. Early sheath removal is encouraged while eptifibatide injection is being infused. Prior to removing the sheath, it is recommended that heparin be discontinued for 3 to 4 hours and an aPTT of <45 seconds or ACT <150 seconds be achieved. In any case, both heparin and eptifibatide injection should be discontinued and sheath hemostasis should be achieved at least 2 to 4 hours before hospital discharge. If bleeding at access site cannot be controlled with pressure, infusion of eptifibatide injection and heparin should be discontinued immediately.
5.2 Thrombocytopenia
There have been reports of acute, profound thrombocytopenia (immune-mediated and non-immune mediated) with eptifibatide injection. In the event of acute profound thrombocytopenia or a confirmed platelet decrease to <100,000/mm3, discontinue eptifibatide injection and heparin (unfractionated or low-molecular weight). Monitor serial platelet counts, assess the presence of drug-dependent antibodies, and treat as appropriate [see Adverse Reactions (6.1)].
There has been no clinical experience with eptifibatide injection initiated in patients with a baseline platelet count <100,000/mm3. If a patient with low platelet counts is receiving eptifibatide injection, their platelet count should be monitored closely.
6 ADVERSE REACTIONS
The following serious adverse reaction is also discussed elsewhere in the labeling:
- Bleeding [see Contraindications (4) and Warnings and Precautions (5.1)]
6.1 Clinical Trials Experience
Because clinical studies are conducted under widely varying conditions, adverse reaction rates observed in the clinical studies of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
A total of 16,782 patients were treated in the Phase III clinical trials (PURSUIT, ESPRIT, and IMPACT II) [see Clinical Studies (14)]. These 16,782 patients had a mean age of 62 years (range: 20 to 94 years). Eighty-nine percent of the patients were Caucasian, with the remainder being predominantly Black (5%) and Hispanic (5%). Sixty-eight percent were men. Because of the different regimens used in PURSUIT, IMPACT II, and ESPRIT, data from the 3 studies were not pooled.
Bleeding and hypotension were the most commonly reported adverse reactions (incidence ≥5% and greater than placebo) in the eptifibatide injection controlled clinical trial database.
Bleeding
The incidence of bleeding and transfusions in the PURSUIT and ESPRIT studies are shown in Table 2. Bleeding was classified as major or minor by the criteria of the TIMI study group. Major bleeding consisted of intracranial hemorrhage and other bleeding that led to decreases in hemoglobin greater than 5 g/dL. Minor bleeding included spontaneous gross hematuria, spontaneous hematemesis, other observed blood loss with a hemoglobin decrease of more than 3 g/dL, and other hemoglobin decreases that were greater than 4 g/dL but less than 5 g/dL. In patients who received transfusions, the corresponding loss in hemoglobin was estimated through an adaptation of the method of Landefeld et al.
Table 2: Bleeding and Transfusions in the PURSUIT and ESPRIT Studies
|
PURSUIT (ACS) |
||
|
|
Placebo n (%) |
Eptifibatide injection 180/2 n (%) |
| Patients |
4,696 |
4,679 |
| Major bleeding* |
425 (9.3%) |
498 (10.8%) |
| Minor bleeding* |
347 (7.6%) |
604 (13.1%) |
| Requiring transfusions† |
490 (10.4%) |
601 (12.8%) |
|
ESPRIT (PCI) |
||
|
Placebo n (%) |
Eptifibatide injection 180/2/180 n (%) |
|
| Patients |
1,024 |
1,040 |
| Major bleeding* |
4 (0.4%) |
13 (1.3%) |
| Minor bleeding* |
18 (2%) |
29 (3%) |
| Requiring transfusions† |
11 (1.1%) |
16 (1.5%) |
| Note: Denominator is based on patients for whom data are available. * For major and minor bleeding, patients are counted only once according to the most severe classification. †Includes transfusions of whole blood, packed red blood cells, fresh frozen plasma, cryoprecipitate, platelets, and autotransfusion during the initial hospitalization. |
||
The majority of major bleeding reactions in the ESPRIT study occurred at the vascular access site (1 and 8 patients, or 0.1% and 0.8% in the placebo and eptifibatide injection groups, respectively). Bleeding at “other” locations occurred in 0.2% and 0.4% of patients, respectively.
In the PURSUIT study, the greatest increase in major bleeding in eptifibatide injection-treated patients compared to placebo-treated patients was also associated with bleeding at the femoral artery access site (2.8% versus 1.3%). Oropharyngeal (primarily gingival), genitourinary, gastrointestinal, and retroperitoneal bleeding were also seen more commonly in eptifibatide injection-treated patients compared to placebo-treated patients.
Among patients experiencing a major bleed in the IMPACT II study, an increase in bleeding on eptifibatide injection versus placebo was observed only for the femoral artery access site (3.2% versus 2.8%).
Table 3 displays the incidence of TIMI major bleeding according to the cardiac procedures carried out in the PURSUIT study. The most common bleeding complications were related to cardiac revascularization (CABG-related or femoral artery access site bleeding). A corresponding table for ESPRIT is not presented, as every patient underwent PCI in the ESPRIT study and only 11 patients underwent CABG.
Table 3: Major Bleeding by Procedures in the PURSUIT Study
|
Placebo n (%) |
Eptifibatide injection 180/2 n (%) |
|
| Patients |
4,577 |
4,604 |
| Overall incidence of major bleeding |
425 (9.3%) |
498 (10.8%) |
| Breakdown by procedure: | ||
| CABG |
375 (8.2%) |
377 (8.2%) |
| Angioplasty without CABG |
27 (0.6%) |
64 (1.4%) |
| Angiography without angioplasty or CABG |
11 (0.2%) |
29 (0.6%) |
| Medical therapy only |
12 (0.3%) |
28 (0.6%) |
| Note: Denominators are based on the total number of patients whose TIMI classification was resolved. | ||
In the PURSUIT and ESPRIT studies, the risk of major bleeding with eptifibatide injection increased as patient weight decreased. This relationship was most apparent for patients weighing less than 70 kg.
Bleeding resulting in discontinuation of the study drug was more frequent among patients receiving eptifibatide injection than placebo (4.6% versus 0.9% in ESPRIT, 8% versus 1% in PURSUIT, 3.5% versus 1.9% in IMPACT II).
Intracranial Hemorrhage and Stroke
Intracranial hemorrhage was rare in the PURSUIT, IMPACT II, and ESPRIT clinical studies. In the PURSUIT study, 3 patients in the placebo group, 1 patient in the group treated with eptifibatide injection 180/1.3, and 5 patients in the group treated with eptifibatide injection 180/2 experienced a hemorrhagic stroke. The overall incidence of stroke was 0.5% in patients receiving eptifibatide injection 180/1.3, 0.7% in patients receiving eptifibatide injection 180/2, and 0.8% in placebo patients.
In the IMPACT II study, intracranial hemorrhage was experienced by 1 patient treated with eptifibatide injection 135/0.5, 2 patients treated with eptifibatide injection 135/0.75, and 2 patients in the placebo group. The overall incidence of stroke was 0.5% in patients receiving 135/0.5 eptifibatide injection, 0.7% in patients receiving eptifibatide injection 135/0.75, and 0.7% in the placebo group.
In the ESPRIT study, there were 3 hemorrhagic strokes, 1 in the placebo group and 2 in the eptifibatide injection group. In addition there was 1 case of cerebral infarction in the eptifibatide injection group.
Immunogenicity/Thrombocytopenia
The potential for development of antibodies to eptifibatide has been studied in 433 subjects. Eptifibatide injection was nonantigenic in 412 patients receiving a single administration of eptifibatide injection (135 mcg/kg bolus followed by a continuous infusion of either 0.5 mcg/kg/min or 0.75 mcg/kg/min), and in 21 subjects to whom eptifibatide injection (135 mcg/kg bolus followed by a continuous infusion of 0.75 mcg/kg/min) was administered twice, 28 days apart. In both cases, plasma for antibody detection was collected approximately 30 days after each dose. The development of antibodies to eptifibatide at higher doses has not been evaluated.
In patients with suspected eptifibatide injection-related immune-mediated thrombocytopenia, IgG antibodies that react with the GP IIb/IIIa complex were identified in the presence of eptifibatide and in eptifibatide injection-naive patients. These findings suggest acute thrombocytopenia after the administration of eptifibatide injection can develop as a result of naturally occurring drug-dependent antibodies or those induced by prior exposure to eptifibatide injection. Similar antibodies were identified with other GP IIb/IIIa ligand-mimetic agents. Immune-mediated thrombocytopenia with eptifibatide injection may be associated with hypotension and/or other signs of hypersensitivity.
In the PURSUIT and IMPACT II studies, the incidence of thrombocytopenia (<100,000/mm3 or ≥50% reduction from baseline) and the incidence of platelet transfusions were similar between patients treated with eptifibatide injection and placebo. In the ESPRIT study, the incidence was 0.6% in the placebo group and 1.2% in the eptifibatide injection group.
Other Adverse Reactions
In the PURSUIT and ESPRIT studies, the incidence of serious nonbleeding adverse reactions was similar in patients receiving placebo or eptifibatide injection (19% and 19%, respectively, in PURSUIT; 6% and 7%, respectively, in ESPRIT). In PURSUIT, the only serious nonbleeding adverse reaction that occurred at a rate of at least 1% and was more common with eptifibatide injection than placebo (7% versus 6%) was hypotension. Most of the serious nonbleeding adverse reactions consisted of cardiovascular reactions typical of a UA population. In the IMPACT II study, serious nonbleeding adverse reactions that occurred in greater than 1% of patients were uncommon and similar in incidence between placebo- and eptifibatide injection-treated patients.
Discontinuation of study drug due to adverse reactions other than bleeding was uncommon in the PURSUIT, IMPACT II, and ESPRIT studies, with no single reaction occurring in >0.5% of the study population (except for “other” in the ESPRIT study).
6.2 Postmarketing Experience
Because the reactions below are reported voluntarily from a population of uncertain size, it is generally not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
The following adverse reactions have been reported in postmarketing experience, primarily with eptifibatide injection in combination with heparin and aspirin: cerebral, GI, and pulmonary hemorrhage. Fatal bleeding reactions have been reported. Acute profound thrombocytopenia, as well as immune-mediated thrombocytopenia, has been reported [see Adverse Reactions (6.1)].
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Category B
Teratology studies have been performed by continuous intravenous infusion of eptifibatide in pregnant rats at total daily doses of up to 72 mg/kg/day (about 4 times the recommended maximum daily human dose on a body surface area basis) and in pregnant rabbits at total daily doses of up to 36 mg/kg/day (also about 4 times the recommended maximum daily human dose on a body surface area basis). These studies revealed no evidence of harm to the fetus due to eptifibatide. There are, however, no adequate and well-controlled studies in pregnant women with eptifibatide injection. Because animal reproduction studies are not always predictive of human response, eptifibatide injection should be used during pregnancy only if clearly needed.
8.3 Nursing Mothers
It is not known whether eptifibatide is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when eptifibatide injection is administered to a nursing mother.
8.4 Pediatric Use
Safety and effectiveness of eptifibatide injection in pediatric patients have not been studied.
8.5 Geriatric Use
The PURSUIT and IMPACT II clinical studies enrolled patients up to the age of 94 years (45% were age 65 and over; 12% were age 75 and older). There was no apparent difference in efficacy between older and younger patients treated with eptifibatide injection. The incidence of bleeding complications was higher in the elderly in both placebo and eptifibatide injection groups, and the incremental risk of eptifibatide injection-associated bleeding was greater in the older patients. No dose adjustment was made for elderly patients, but patients over 75 years of age had to weigh at least 50 kg to be enrolled in the PURSUIT study; no such limitation was stipulated in the ESPRIT study [see Adverse Reactions (6.1)].
8.6 Renal Impairment
Approximately 50% of eptifibatide is cleared by the kidney in patients with normal renal function. Total drug clearance is decreased by approximately 50% and steady-state plasma eptifibatide injection concentrations are doubled in patients with an estimated CrCl <50 mL/min (using the Cockcroft-Gault equation). Therefore, the infusion dose should be reduced to 1 mcg/kg/min in such patients [see Dosage and Administration (2)]. The safety and efficacy of eptifibatide injection in patients dependent on dialysis has not been established.
10 OVERDOSAGE
There has been only limited experience with overdosage of eptifibatide injection. There were 8 patients in the IMPACT II study, 9 patients in the PURSUIT study, and no patients in the ESPRIT study who received bolus doses and/or infusion doses more than double those called for in the protocols. None of these patients experienced an intracranial bleed or other major bleeding.
Eptifibatide was not lethal to rats, rabbits, or monkeys when administered by continuous intravenous infusion for 90 minutes at a total dose of 45 mg/kg (about 2 to 5 times the recommended maximum daily human dose on a body surface area basis). Symptoms of acute toxicity were loss of righting reflex, dyspnea, ptosis, and decreased muscle tone in rabbits and petechial hemorrhages in the femoral and abdominal areas of monkeys.
From in vitro studies, eptifibatide is not extensively bound to plasma proteins and thus may be cleared from plasma by dialysis.
11 DESCRIPTION
Eptifibatide is a cyclic heptapeptide containing 6 amino acids and 1 mercaptopropionyl (des-amino cysteinyl) residue. An interchain disulfide bridge is formed between the cysteine amide and the mercaptopropionyl moieties. Chemically it is N6-(aminoiminomethyl)-N2-(3-mercapto-1-oxopropyl)-L-lysylglycyl-L-α-aspartyl-L-tryptophyl-L-prolyl-L-cysteinamide, cyclic (1→6)-disulfide. Eptifibatide binds to the platelet receptor glycoprotein (GP) IIb/IIIa of human platelets and inhibits platelet aggregation.
The eptifibatide peptide is produced by solution-phase peptide synthesis, and is purified by preparative reverse-phase liquid chromatography and lyophilized. The structural formula is:
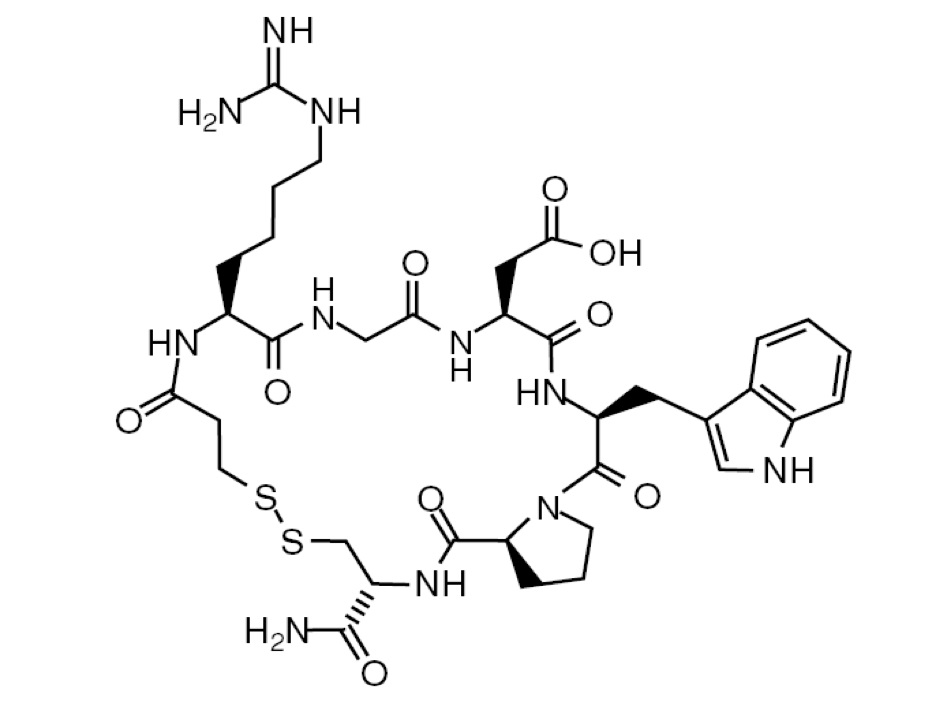
Eptifibatide injection is a clear, colorless, sterile, non-pyrogenic solution for intravenous (IV) use with an empirical formula of C35H49N11O9S2 and a molecular weight of 831.96. Each 10 mL vial contains 2 mg/mL of eptifibatide. Each vial contains 5.25 mg/mL citric acid and sodium hydroxide to adjust the pH to 5.35.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Eptifibatide reversibly inhibits platelet aggregation by preventing the binding of fibrinogen, von Willebrand factor, and other adhesive ligands to GP IIb/IIIa. When administered intravenously, eptifibatide inhibits ex vivo platelet aggregation in a dose- and concentration-dependent manner. Platelet aggregation inhibition is reversible following cessation of the eptifibatide infusion; this is thought to result from dissociation of eptifibatide from the platelet.
12.2 Pharmacodynamics
Infusion of eptifibatide into baboons caused a dose-dependent inhibition of ex vivo platelet aggregation, with complete inhibition of aggregation achieved at infusion rates greater than 5 mcg/kg/min. In a baboon model that is refractory to aspirin and heparin, doses of eptifibatide that inhibit aggregation prevented acute thrombosis with only a modest prolongation (2- to 3-fold) of the bleeding time. Platelet aggregation in dogs was also inhibited by infusions of eptifibatide, with complete inhibition at 2 mcg/kg/min. This infusion dose completely inhibited canine coronary thrombosis induced by coronary artery injury (Folts model).
Human pharmacodynamic data were obtained in healthy subjects and in patients presenting with UA or NSTEMI and/or undergoing percutaneous coronary intervention. Studies in healthy subjects enrolled only males; patient studies enrolled approximately one-third women. In these studies, eptifibatide injection inhibited ex vivo platelet aggregation induced by adenosine diphosphate (ADP) and other agonists in a dose- and concentration-dependent manner. The effect of eptifibatide injection was observed immediately after administration of a 180 mcg/kg intravenous bolus. Table 4 shows the effects of dosing regimens of eptifibatide injection used in the IMPACT II and PURSUIT studies on ex vivo platelet aggregation induced by 20 µM ADP in PPACK-anticoagulated platelet-rich plasma and on bleeding time. The effects of the dosing regimen used in ESPRIT on platelet aggregation have not been studied.
Table 4: Platelet Inhibition and Bleeding Time
|
PURSUIT 180/2* |
|
| Inhibition of platelet aggregation 15 min after bolus |
84% |
| Inhibition of platelet aggregation at steady state |
>90% |
| Bleeding-time prolongation at steady state |
<5x |
| Inhibition of platelet aggregation 4h after infusion discontinuation |
<50% |
| Bleeding-time prolongation 6h after infusion discontinuation |
1.4x |
| *180 mcg/kg bolus followed by a continuous infusion of 2 mcg/kg/min. | |
The eptifibatide injection dosing regimen used in the ESPRIT study included two 180 mcg/kg bolus doses given 10 minutes apart combined with a continuous 2 mcg/kg/min infusion.
When administered alone, eptifibatide injection has no measurable effect on PT or aPTT.
There were no important differences between men and women or between age groups in the pharmacodynamic properties of eptifibatide. Differences among ethnic groups have not been assessed.
12.3 Pharmacokinetics
The pharmacokinetics of eptifibatide are linear and dose-proportional for bolus doses ranging from 90 to 250 mcg/kg and infusion rates from 0.5 to 3 mcg/kg/min. Plasma elimination half-life is approximately 2.5 hours. Administration of a single 180 mcg/kg bolus combined with an infusion produces an early peak level, followed by a small decline prior to attaining steady state (within 4 to 6 hours). This decline can be prevented by administering a second 180 mcg/kg bolus 10 minutes after the first. The extent of eptifibatide binding to human plasma protein is about 25%. Clearance in patients with coronary artery disease is about 55 mL/kg/h. In healthy subjects, renal clearance accounts for approximately 50% of total body clearance, with the majority of the drug excreted in the urine as eptifibatide, deaminated eptifibatide, and other, more polar metabolites. No major metabolites have been detected in human plasma.
Special Populations
Geriatric
Patients in clinical studies were older (range: 20 to 94 years) than those in the clinical pharmacology studies. Elderly patients with coronary artery disease demonstrated higher plasma levels and lower total body clearance of eptifibatide when given the same dose as younger patients. Limited data are available on lighter weight (<50 kg) patients over 75 years of age.
Renal Impairment
In patients with moderate to severe renal insufficiency (CrCl <50 mL/min using the Cockcroft-Gault equation), the clearance of eptifibatide is reduced by approximately 50% and steady-state plasma levels approximately doubled [see Use in Specific Populations (8.6) and Dosage and Administration (2)].
Hepatic Impairment
No studies have been conducted in patients with hepatic impairment.
Gender
Males and females have not demonstrated any clinically significant differences in the pharmacokinetics of eptifibatide.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis & Mutagenesis & Impairment Of Fertility
No long-term studies in animals have been performed to evaluate the carcinogenic potential of eptifibatide. Eptifibatide was not genotoxic in the Ames test, the mouse lymphoma cell (L 5178Y, TK+/-) forward mutation test, the human lymphocyte chromosome aberration test, or the mouse micronucleus test. Administered by continuous intravenous infusion at total daily doses up to 72 mg/kg/day (about 4 times the recommended maximum daily human dose on a body surface area basis), eptifibatide had no effect on fertility and reproductive performance of male and female rats.
14 CLINICAL STUDIES
Eptifibatide injection was studied in 3 placebo-controlled, randomized studies. PURSUIT evaluated patients with acute coronary syndromes: UA or NSTEMI. Two other studies, ESPRIT and IMPACT II, evaluated patients about to undergo a PCI. Patients underwent primarily balloon angioplasty in IMPACT II and intracoronary stent placement, with or without angioplasty, in ESPRIT.
14.1 Non-ST-Segment Elevation Acute Coronary Syndrome
Non-ST-segment elevation acute coronary syndrome is defined as prolonged (≥10 minutes) symptoms of cardiac ischemia within the previous 24 hours associated with either ST-segment changes (elevations between 0.6 mm and 1 mm or depression >0.5 mm), T-wave inversion (>1 mm), or positive CK-MB. This definition includes “unstable angina” and “NSTEMI” but excludes MI that is associated with Q waves or greater degrees of ST-segment elevation.
PURSUIT (Platelet Glycoprotein IIb/IIIa in Unstable Angina: Receptor Suppression Using Eptifibatide Injection Therapy)
PURSUIT was a 726-center, 27-country, double-blind, randomized, placebo-controlled study in 10,948 patients presenting with UA or NSTEMI. Patients could be enrolled only if they had experienced cardiac ischemia at rest (≥10 minutes) within the previous 24 hours and had either ST-segment changes (elevations between 0.6 mm and 1 mm or depression >0.5 mm), T-wave inversion (>1 mm), or increased CK-MB. Important exclusion criteria included a history of bleeding diathesis, evidence of abnormal bleeding within the previous 30 days, uncontrolled hypertension, major surgery within the previous 6 weeks, stroke within the previous 30 days, any history of hemorrhagic stroke, serum creatinine >2 mg/dL, dependency on renal dialysis, or platelet count <100,000/mm3.
Patients were randomized to placebo, to eptifibatide injection 180 mcg/kg bolus followed by a 2 mcg/kg/min infusion (180/2), or to eptifibatide injection 180 mcg/kg bolus followed by a 1.3 mcg/kg/min infusion (180/1.3). The infusion was continued for 72 hours, until hospital discharge, or until the time of CABG, whichever occurred first, except that if PCI was performed, the eptifibatide infusion was continued for 24 hours after the procedure, allowing for a duration of infusion up to 96 hours.
The lower-infusion-rate arm was stopped after the first interim analysis when the 2 active-treatment arms appeared to have the same incidence of bleeding.
Patient age ranged from 20 to 94 (mean 63) years, and 65% were male. The patients were 89% Caucasian, 6% Hispanic, and 5% Black, recruited in the United States and Canada (40%), Western Europe (39%), Eastern Europe (16%), and Latin America (5%).
This was a "real world" study; each patient was managed according to the usual standards of the investigational site; frequencies of angiography, PCI, and CABG therefore differed widely from site to site and from country to country. Of the patients in PURSUIT, 13% were managed with PCI during drug infusion, of whom 50% received intracoronary stents; 87% were managed medically (without PCI during drug infusion).
The majority of patients received aspirin (75 to 325 mg once daily). Heparin was administered intravenously or subcutaneously, at the physician's discretion, most commonly as an intravenous bolus of 5,000 units followed by a continuous infusion of 1,000 units/h. For patients weighing less than 70 kg, the recommended heparin bolus dose was 60 units/kg followed by a continuous infusion of 12 units/kg/h. A target aPTT of 50 to 70 seconds was recommended. A total of 1,250 patients underwent PCI within 72 hours after randomization, in which case they received intravenous heparin to maintain an ACT of 300 to 350 seconds.
The primary endpoint of the study was the occurrence of death from any cause or new MI (evaluated by a blinded Clinical Endpoints Committee) within 30 days of randomization.
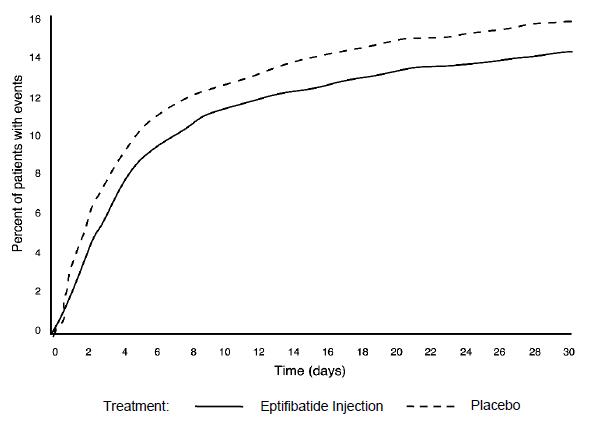
Compared to placebo, eptifibatide injection administered as a 180 mcg/kg bolus followed by a 2 mcg/kg/min infusion significantly (p=0.042) reduced the incidence of endpoint events (see Table 6). The reduction in the incidence of endpoint events in patients receiving eptifibatide injection was evident early during treatment, and this reduction was maintained through at least 30 days (see Figure 1). Table 5 also shows the incidence of the components of the primary endpoint, death (whether or not preceded by an MI) and new MI in surviving patients at 30 days.
Table 5: Clinical Events in the PURSUIT Study
|
Death or MI |
Placebo (n = 4,739) n (%) |
Eptifibatide injection (180 mcg/kg bolus then 2 mcg/kg/min infusion) (n=4,722) n (%) |
p-value |
| 3 days |
359 (7.6%) |
279 (5.9%) |
0.001 |
| 7 days |
552 (11.6%) |
477 (10.1%) |
0.016 |
| 30 days | |||
| Death or MI (primary endpoint) |
745 (15.7%) |
672 (14.2%) |
0.042 |
| Death |
177 (3.7%) |
165 (3.5%) | |
| Nonfatal MI |
568 (12%) |
507 (10.7%) |
Figure 1: Kaplan-Meier Plot of Time to Death or Myocardial Infarction Within 30 Days of Randomization in the PURSUIT Study
Treatment with eptifibatide injection prior to determination of patient management strategy reduced clinical events regardless of whether patients ultimately underwent diagnostic catheterization, revascularization (i.e., PCI or CABG surgery) or continued to receive medical management alone. Table 6 shows the incidence of death or MI within 72 hours.
Table 6: Clinical Events (Death or MI) in the PURSUIT Study Within 72 Hours of Randomization
|
Placebo |
Eptifibatide injection (180 mcg/kg bolus then 2 mcg/kg/min infusion) |
|
| Overall patient population |
n=4,739 |
n=4,722 |
| – At 72 hours |
7.6% |
5.9% |
| Patients undergoing early PCI |
n=631 |
n=619 |
| – Pre-procedure (nonfatal MI only) |
5.5% |
1.8% |
| – At 72 hours |
14.4% |
9% |
| Patients not undergoing early PCI |
n=4,108 |
n=4,103 |
| – At 72 hours |
6.5% |
5.4% |
All of the effect of eptifibatide injection was established within 72 hours (during the period of drug infusion), regardless of management strategy. Moreover, for patients undergoing early PCI, a reduction in events was evident prior to the procedure.
An analysis of the results by sex suggests that women who would not routinely be expected to undergo PCI receive less benefit from eptifibatide injection (95% confidence limits for relative risk of 0.94 to 1.28) than do men (0.72 to 0.9). This difference may be a true treatment difference, the effect of other differences in these subgroups, or a statistical anomaly. No differential outcomes were seen between male and female patients undergoing PCI (see results for ESPRIT).
Follow-up data were available through 165 days for 10,611 patients enrolled in the PURSUIT trial (96.9% of the initial enrollment). This follow-up included 4,566 patients who received eptifibatide injection at the 180/2 dose. As reported by the investigators, the occurrence of death from any cause or new MI for patients followed for at least 165 days was reduced from 13.6% with placebo to 12.1% with eptifibatide injection 180/2.
14.2 Percutaneous Coronary Intervention (PCI)
IMPACT II (Eptifibatide Injection to MinimizePlatelet Aggregation and Prevent Coronary Thrombosis II)
IMPACT II was a multicenter, double-blind,randomized, placebo-controlled study conducted in the United States in 4,010patients undergoing PCI. Major exclusion criteria included a history ofbleeding diathesis, major surgery within 6 weeks of treatment, gastrointestinalbleeding within 30 days, any stroke or structural CNS abnormality, uncontrolledhypertension, PT >1.2 times control, hematocrit <30%, platelet count<100,000/mm3, and pregnancy. Patient age ranged from 24 to 89 (mean 60)years, and 75% were male.
The patients were 92% Caucasian, 5% Black, and 3%Hispanic. Forty-one percent of the patients underwent PCI for ongoing ACS.Patients were randomly assigned to 1 of 3 treatment regimens, eachincorporating a bolus dose initiated immediately prior to PCI followed by acontinuous infusion lasting 20 to 24 hours:
- 135 mcg/kg bolus followed by a continuous infusion of 0.5 mcg/kg/min of eptifibatide injection (135/0.5);
- 135 mcg/kg bolus followed by a continuous infusion of 0.75 mcg/kg/min of eptifibatide injection (135/0.75); or
- a matching placebo bolus followed by a matching placebo continuous infusion.
Each patient received aspirin and an intravenous heparin bolus of100 units/kg, with additional bolus infusions of up to 2,000 additional unitsof heparin every 15 minutes to maintain an ACT of 300 to 350 seconds.
The primary endpoint was the composite of death, MI, or urgentrevascularization, analyzed at 30 days after randomization in all patients whoreceived at least 1 dose of study drug.
As shown in Table 7, each eptifibatide injection regimen reduced the rate ofdeath, MI, or urgent intervention, although at 30 days, this finding wasstatistically significant only in the lower-dose eptifibatide injection group.As in the PURSUIT study, the effects of eptifibatide injection were seen earlyand persisted throughout the 30-day period.
Table 7: ClinicalEvents in the IMPACT II Study
|
|
Placebo n(%) |
Eptifibatide injection (135 mcg/kg bolus then 0.5 mcg/kg/min infusion) n (%) |
Eptifibatide injection (135 mcg/kg bolus then 0.75 mcg/kg/min infusion) n (%) |
| Patients |
1,285 |
1,300 |
1,286 |
| Abrupt Closure |
65 (5.1%) |
36 (2.8%) |
43 (3.3%) |
|
p-value versus placebo |
0.003 |
0.003 |
|
| Death, MI, or Urgent Intervention |
|
|
|
|
24 hours |
123 (9.6%) |
86 (6.6%) |
89 (6.9%) |
|
p-value versus placebo |
0.006 |
0.014 |
|
|
48 hours |
131 (10.2%) |
99 (7.6%) |
102 (7.9%) |
|
p-value versus placebo |
0.021 |
0.045 |
|
|
30 days (primary endpoint) |
149 (11.6%) |
118 (9.1%) |
128 (10%) |
|
p-value versus placebo |
0.035 |
0.179 |
|
| Death or MI |
|
|
|
|
30 days |
110 (8.6%) |
89 (6.8%) |
95 (7.4%) |
|
p-value versus placebo |
0.102 |
0.272 |
|
|
6 months |
151 (11.9%)* |
136 (10.6%)* |
130 (10.3%)* |
|
p-value versus placebo |
0.297 |
0.182 |
|
| * Kaplan-Meier estimate of event rate. | |||
ESPRIT (Enhanced Suppression of the Platelet IIb/IIIa Receptor with Eptifibatide Injection Therapy)
The ESPRIT study was a multicenter, double-blind, randomized, placebo-controlled study conducted in the United States and Canada that enrolled 2,064 patients undergoing elective or urgent PCI with intended intracoronary stent placement. Exclusion criteria included MI within the previous 24 hours, ongoing chest pain, administration of any oral antiplatelet or oral anticoagulant other than aspirin within 30 days of PCI (although loading doses of thienopyridine on the day of PCI were encouraged), planned PCI of a saphenous vein graft or subsequent “staged” PCI, prior stent placement in the target lesion, PCI within the previous 90 days, a history of bleeding diathesis, major surgery within 6 weeks of treatment, gastrointestinal bleeding within 30 days, any stroke or structural CNS abnormality, uncontrolled hypertension, PT >1.2 times control, hematocrit <30%, platelet count <100,000/mm3, and pregnancy.
Patient age ranged from 24 to 93 (mean 62) years, and 73% of patients were male. The study enrolled 90% Caucasian, 5% African American, 2% Hispanic, and 1% Asian patients. Patients received a wide variety of stents. Patients were randomized either to placebo or eptifibatide injection administered as an intravenous bolus of 180 mcg/kg followed immediately by a continuous infusion of 2 mcg/kg/min, and a second bolus of 180 mcg/kg administered 10 minutes later (180/2/180). Eptifibatide infusion was continued for 18 to 24 hours after PCI or until hospital discharge, whichever came first. Each patient received at least 1 dose of aspirin (162 to 325 mg) and 60 units/kg of heparin as a bolus (not to exceed 6,000 units) if not already receiving a heparin infusion. Additional boluses of heparin (10 to 40 units/kg) could be administered in order to reach a target ACT between 200 and 300 seconds.
The primary endpoint of the ESPRIT study was the composite of death, MI, urgent target vessel revascularization (UTVR), and “bailout” to open-label eptifibatide injection due to a thrombotic complication of PCI (TBO) (e.g., visible thrombus, “no reflow,” or abrupt closure) at 48 hours. MI, UTVR, and TBO were evaluated by a blinded Clinical Events Committee.
As shown in Table 8, the incidence of the primary endpoint and selected secondary endpoints was significantly reduced in patients who received eptifibatide injection. A treatment benefit in patients who received eptifibatide injection was seen by 48 hours and at the end of the 30-day observation period.
Table 8: Clinical Events in the ESPRIT Study
|
Placebo (n=1,024) |
Eptifibatide injection* (n=1,040) |
Relative Risk (95% CI) | p-value | |
| Death, MI, UTVR, or Thrombotic “Bailout” | ||||
| 48 hours (primary endpoint) |
108 (10.5%) |
69 (6.6%) |
0.629 (0.471, 0.84) |
0.0015 |
| 30 days |
120 (11.7%) |
78 (7.5%) |
0.64 (0.488, 0.84) | 0.0011 |
| Death, MI, or UTVR | ||||
| 48 hours |
95 (9.3%) |
62 (6%) | 0.643 (0.472, 0.875) |
0.0045 |
| 30 days (key secondary endpoint) |
107 (10.4%) |
71 (6.8%) |
0.653 (0.49, 0.871) |
0.0034 |
| Death or MI | ||||
| 48 hours |
94 (9.2%) |
57 (5.5%) |
0.597 (0.435, 0.82) |
0.0013 |
| 30 days |
104 (10.2%) |
66 (6.3%) |
0.625 (0.465, 0.84) | 0.0016 |
| *Eptifibatide injection was administered as 180 mcg/kg boluses at times 0 and 10 minutes and an infusion at 2 mcg/kg/min. | ||||
The need for thrombotic “bailout” was significantly reduced with eptifibatide injection at 48 hours (2.1% for placebo, 1% for eptifibatide injection; p=0.029). Consistent with previous studies of GP IIb/IIIa inhibitors, most of the benefit achieved acutely with eptifibatide injection was in the reduction of MI. Eptifibatide injection reduced the occurrence of MI at 48 hours from 9% for placebo to 5.4% (p=0.0015) and maintained that effect with significance at 30 days.
There was no treatment difference with respect to sex in ESPRIT. Eptifibatide injection reduced the incidence of the primary endpoint in both men (95% confidence limits for relative risk: 0.54, 1.07) and women (0.24, 0.72) at 48 hours.
Follow-up (12-month) mortality data were available for 2,024 patients (1,017 on eptifibatide injection) enrolled in the ESPRIT trial (98.1% of the initial enrollment). Twelve-month clinical event data were available for 1,964 patients (988 on eptifibatide injection), representing 95.2% of the initial enrollment. As shown in Table 9, the treatment effect of eptifibatide injection seen at 48 hours and 30 days appeared preserved at 6 months and 1 year. Most of the benefit was in reduction of MI.
Table 9: Clinical Events at 6 Months and 1 Year in the ESPRIT Study
|
|
Placebo (n=1,024) |
Eptifibatide injection (n=1,040) |
Hazard Ratio (95% CI) |
| Death, MI, or Target Vessel Revascularization | |||
|
6 Months | 187 (18.5%) |
146 (14.3%) | 0.744 (0.599, 0.924) |
|
1 Year | 222 (22.1%) |
178 (17.5%) | 0.762 (0.626, 0.929) |
| Death, MI | |||
|
6 Months | 117 (11.5%) |
77 (7.4%) | 0.631 (0.473, 0.841) |
|
1 Year | 126 (12.4%) |
83 (8%) | 0.63 (0.478, 0.832) |
| Percentages are Kaplan-Meier event rates. | |||
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
Eptifibatide injection is supplied as a sterile solution in 10 mL vials containing 20 mg of eptifibatide.
| NDC No. | Strength | Vial Pack |
| 62147-0600-1 | 20 mg per 10 mL (2 mg per mL) | 10 mL vial packaged individually. |
This container closure is not made with natural rubber latex.
16.2 Storage
Vials should be stored refrigerated at 2º to 8°C (36º to 46°F). Vials may be transferred to room temperature storage* for a period not to exceed 2 months. Upon transfer, vial cartons must be marked by the dispensing pharmacist with a “DISCARD BY” date (2 months from the transfer date or the labeled expiration date, whichever comes first).
* Store at 25°C (77°F); excursions permitted to 15º to 30°C (59º to 86°F) [see USP Controlled Room Temperature].
Manufactured for:
USV Private Limited
B.S.D. Marg, Govandi,
Mumbai - 400 088
Made in India.
Issued: March 2019