FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
Mupirocin Ointment USP, 2% is indicated for the topical treatment of impetigo due to susceptible isolates of Staphylococcus aureus (S. aureus) and Streptococcus pyogenes (S. pyogenes).
2 DOSAGE AND ADMINISTRATION
- For Topical Use Only.
- Apply a small amount of Mupirocin Ointment USP, 2%, with a cotton swab or gauze pad, to the affected area 3 times daily for up to 10 days.
- Cover the treated area with gauze dressing if desired.
- Re-evaluate patients not showing a clinical response within 3 to 5 days.
- Mupirocin Ointment USP, 2% is not for intranasal, ophthalmic, or other mucosal use [ see Warnings and Precautions (5.2, 5.6)].
- Do not apply Mupirocin Ointment USP, 2% concurrently with any other lotions, creams, or ointments [ see Clinical Pharmacology (12.3)].
3 DOSAGE FORMS AND STRENGTHS
Each gram of Mupirocin Ointment USP, 2% contains 20 mg mupirocin in a water-miscible ointment base supplied in 22-gram tubes.
4 CONTRAINDICATIONS
Mupirocin Ointment USP, 2% is contraindicated in patients with known hypersensitivity to mupirocin or any of the excipients of Mupirocin Ointment USP, 2%.
5 WARNINGS AND PRECAUTIONS
5.1 Severe Allergic Reactions
Systemic allergic reactions, including anaphylaxis, urticaria, angioedema, and generalized rash, have been reported in patients treated with formulations of mupirocin, including Mupirocin Ointment USP, 2% [ see Adverse Reactions (6.2)].
5.2 Eye Irritation
Avoid contact with the eyes. In case of accidental contact, rinse well with water.
5.3 Local Irritation
In the event of a sensitization or severe local irritation from Mupirocin Ointment USP, 2%, usage should be discontinued, and appropriate alternative therapy for the infection instituted.
5.4 Clostridium difficile-Associated Diarrhea
Clostridium difficile-associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile.
C. difficile produces toxins A and B which contribute to the development of CDAD.
Hypertoxin-producing strains of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibacterial drug use.
Careful medical history is necessary since CDAD has been reported to occur over 2 months after the administration of antibacterial agents.
If CDAD is suspected or confirmed, ongoing antibacterial drug use not directed against C. difficile may need to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibacterial treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated.
5.5 Potential for Microbial Overgrowth
As with other antibacterial products, prolonged use of Mupirocin Ointment USP, 2% may result in overgrowth of nonsusceptible microorganisms, including fungi [ see Dosage and Administration (2)].
5.6 Risk Associated with Mucosal Use
Mupirocin Ointment USP, 2% is not formulated for use on mucosal surfaces. Intranasal use has been associated with isolated reports of stinging and drying. A separate formulation, *BACTROBAN® (mupirocin calcium) nasal ointment, is available for intranasal use.
5.7 Risk of Polyethylene Glycol Absorption
Polyethylene glycol can be absorbed from open wounds and damaged skin and is excreted by the kidneys. In common with other polyethylene glycol-based ointments, Mupirocin Ointment USP, 2% should not be used in conditions where absorption of large quantities of polyethylene glycol is possible, especially if there is evidence of moderate or severe renal impairment.
6 ADVERSE REACTIONS
The following adverse reactions are discussed in more detail in other sections of the labeling:
- Severe Allergic Reactions [ see Warnings and Precautions (5.1)]
- Eye Irritation [ see Warnings and Precautions (5.2)]
- Local Irritation [ see Warnings and Precautions (5.3)]
- Clostridium difficile-Associated Diarrhea [ see Warnings and Precautions (5.4)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared with rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The following local adverse reactions were reported by at least 1% of subjects in connection with the use of mupirocin ointment in clinical trials: burning, stinging, or pain in 1.5% of subjects; itching in 1% of subjects. Rash, nausea, erythema, dry skin, tenderness, swelling, contact dermatitis, and increased exudate were reported in less than 1% of subjects.
6.2 Postmarketing Experience
In addition to adverse reactions reported from clinical trials, the following reactions have been identified during postmarketing use of mupirocin ointment. Because they are reported voluntarily from a population of unknown size, estimates of frequency cannot be made. These reactions have been chosen for inclusion due to a combination of their seriousness, frequency of reporting, or potential causal relationship to mupirocin ointment.
Immune System Disorders
Systemic allergic reactions, including anaphylaxis, urticaria, angioedema, and generalized rash [ see Warnings and Precautions (5.1)].
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are insufficient human data to establish whether there is a drug-associated risk with mupirocin ointment in pregnant women. Systemic absorption of mupirocin through intact human skin is minimal following topical administration of mupirocin ointment [ see Clinical Pharmacology (12.3)]. No developmental toxicity was observed in rats or rabbits treated with mupirocin subcutaneously during organogenesis at doses of 160 or 40 mg per kg per day, respectively (22 and 11 times the human topical dose based on calculations of dose divided by the entire body surface area).
The estimated background risk of major birth defects and miscarriages for the indicated population is unknown. The estimated background risk in the U.S. general population of major birth defects is 2% to 4% and of miscarriage is 15% to 20% of clinically recognized pregnancies.
Data
Animal Data: Developmental toxicity studies have been performed with mupirocin administered subcutaneously to rats and rabbits at doses up to 160 mg per kg per day during organogenesis.
This dose is 22 and 43 times, respectively, the human topical dose (approximately 60 mg mupirocin per day) based on calculations of dose divided by the entire body surface area.
Maternal toxicity was observed (body weight loss/decreased body weight gain and reduced feeding) in both species with no evidence of developmental toxicity in rats. In rabbits, excessive maternal toxicity at the high dose precluded the evaluation of fetal outcomes. There was no developmental toxicity in rabbits at 40 mg per kg per day, 11 times the human topical dose based on calculations of dose divided by the entire body surface area.
Mupirocin administered subcutaneously to rats in a pre- and postnatal development study (dosed during late gestation through lactation) was associated with reduced offspring viability in the early postnatal period at a dose of 106.7 mg per kg, in the presence of injection site irritation and/or subcutaneous hemorrhaging. This dose is 14 times the human topical dose based on calculations of dose divided by the entire body surface area. The no-observed adverse effect level in this study was 44.2 mg per kg per day, which is 6 times the human topical dose.
8.2 Lactation
Risk Summary
It is not known whether mupirocin is present in human milk, has effects on the breastfed child, or has effects on milk production. However, breastfeeding is not expected to result in exposure of the child to the drug due to the minimal systemic absorption of mupirocin in humans following topical administration of mupirocin ointment [ see Clinical Pharmacology (12.3)]. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for mupirocin ointment and any potential adverse effects on the breastfed child from mupirocin ointment or from the underlying maternal condition.
Clinical Considerations
To minimize oral exposure of the drug to children, a breast and/or nipple being treated with Mupirocin Ointment USP, 2% should be thoroughly washed prior to breastfeeding.
8.4 Pediatric Use
The safety and effectiveness of mupirocin ointment have been established in the age range of 2 months to 16 years. Use of mupirocin ointment in these age-groups is supported by evidence from adequate and well-controlled trials of mupirocin ointment in impetigo in pediatric subjects studied as a part of the pivotal clinical trials [ see Clinical Studies (14)].
11 DESCRIPTION
Mupirocin Ointment USP, 2% contains the RNA synthetase inhibitor antibacterial, mupirocin.
The chemical name is ( E)-(2 S,3 R,4 R,5 S)-5-[(2 S,3 S,4 S,5 S)-2,3-epoxy-5-hydroxy-4-methylhexyl] tetrahydro-3,4-dihydroxy-β-methyl-2 H-pyran-2-crotonic acid, ester with 9-hydroxynonanoic acid. The molecular formula of mupirocin is C 26H 44O 9, and the molecular weight is 500.6.
The structural formula of mupirocin is:
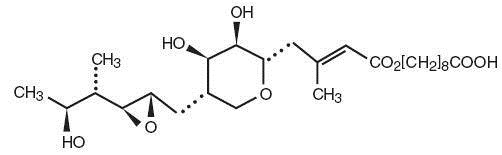
Figure 1. Structure of Murpirocin
Each gram of Mupirocin Ointment USP, 2% contains 20 mg mupirocin in a water-miscible ointment base (polyethylene glycol ointment, NF) consisting of polyethylene glycol 400 and polyethylene glycol 3350.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Mupirocin is an RNA synthetase inhibitor antibacterial [ see Microbiology (12.4)].
12.3 Pharmacokinetics
Absorption
Application of 14C-labeled mupirocin ointment to the lower arm of normal male subjects followed by occlusion for 24 hours showed no measurable systemic absorption (less than 1.1 nanogram mupirocin per milliliter of whole blood). Measurable radioactivity was present in the stratum corneum of these subjects 72 hours after application.
The effect of the concurrent application of mupirocin ointment with other topical products has not been studied [ see Dosage and Administration (2)].
Elimination
In a trial conducted in 7 healthy adult male subjects, the elimination half-life after intravenous administration of mupirocin was 20 to 40 minutes for mupirocin and 30 to 80 minutes for monic acid.
Metabolism: Following intravenous or oral administration, mupirocin is rapidly metabolized.
The principal metabolite, monic acid, demonstrates no antibacterial activity.
Excretion: Monic acid is predominantly eliminated by renal excretion.
12.4 Microbiology
Mupirocin is an RNA synthetase inhibitor antibacterial produced by fermentation using the organism Pseudomonas fluorescens.
Mechanism of Action
Mupirocin inhibits bacterial protein synthesis by reversibly and specifically binding to bacterial isoleucyl transfer RNA (tRNA) synthetase.
Mupirocin is bactericidal at concentrations achieved by topical administration. Mupirocin is highly protein bound (greater than 97%) and the effect of wound secretions on the minimum inhibitory concentrations (MICs) of mupirocin has not been determined.
Resistance
When mupirocin resistance occurs, it results from the production of a modified isoleucyl-tRNA synthetase, or the acquisition of, by genetic transfer, a plasmid mediating a new isoleucyl-tRNA synthetase. High-level plasmid-mediated resistance (MIC ≥512 mcg/mL) has been reported in increasing numbers of isolates of S. aureus and with higher frequency in coagulase-negative staphylococci. Mupirocin resistance occurs with greater frequency in methicillin-resistant than methicillin-susceptible staphylococci.
Cross Resistance
Due to its mode of action, mupirocin does not demonstrate cross resistance with other classes of antimicrobial agents.
Antimicrobial Activity
Mupirocin has been shown to be active against susceptible isolates of S. aureus and S. pyogenes, both in vitro and in clinical trials [ see Indications and Usage (1)]. The following in vitro data are available, but their clinical significance is unknown. Mupirocin is active against most isolates of Staphylococcus epidermidis.
Susceptibility Test Methods
High-level mupirocin resistance (≥512 mcg/mL) may be determined using standard disk diffusion or broth microdilution tests. 1,2 Because of the occurrence of mupirocin resistance in methicillin-resistant S. aureus (MRSA), it is appropriate to test MRSA populations for mupirocin susceptibility prior to the use of mupirocin using a standardized method. 3,4,5
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term studies in animals to evaluate carcinogenic potential of mupirocin have not been conducted.
Results of the following studies performed with mupirocin calcium or mupirocin sodium in vitro and in vivo did not indicate a potential for genotoxicity: rat primary hepatocyte unscheduled DNA synthesis, sediment analysis for DNA strand breaks, Salmonella reversion test (Ames), Escherichiacoli mutation assay, metaphase analysis of human lymphocytes, mouse lymphoma assay, and bone marrow micronuclei assay in mice.
In a fertility/reproductive performance study (with dosing through lactation), mupirocin administered subcutaneously to male and female rats at doses up to 100 mg per kg per day which is 14 times the human topical dose (approximately 60 mg mupirocin per day) based on calculations of dose divided by the entire body surface area, did not result in impaired fertility or impaired reproductive performance attributable to mupirocin.
14 CLINICAL STUDIES
The efficacy of topical mupirocin ointment in impetigo was tested in 2 trials. In the first, subjects with impetigo were randomized to receive either mupirocin ointment or vehicle placebo 3 times daily for 8 to 12 days. Clinical efficacy rates at end of therapy in the evaluable populations (adults and pediatric subjects included) were 71% for mupirocin ointment (n = 49) and 35% for vehicle placebo (n = 51). Pathogen eradication rates in the evaluable populations were 94% for mupirocin ointment and 62% for vehicle placebo.
In the second trial, subjects with impetigo were randomized to receive either mupirocin ointment 3 times daily or 30 to 40 mg per kg oral erythromycin ethylsuccinate per day (this was an unblinded trial) for 8 days. There was a follow-up visit 1 week after treatment ended. Clinical efficacy rates at the follow-up visit in the evaluable populations (adults and pediatric subjects included) were 93% for mupirocin ointment (n = 29) and 78.5% for erythromycin (n = 28).
Pathogen eradication rates in the evaluable populations were 100% for both test groups.
Pediatrics
There were 91 pediatric subjects aged 2 months to 15 years in the first trial described above. Clinical efficacy rates at end of therapy in the evaluable populations were 78% for mupirocin ointment (n = 42) and 36% for vehicle placebo (n = 49). In the second trial described above, all subjects were pediatric except 2 adults in the group receiving mupirocin ointment. The age range of the pediatric subjects was 7 months to 13 years. The clinical efficacy rate for mupirocin ointment (n = 27) was 96%, and for erythromycin it was unchanged (78.5%).
15 REFERENCES
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing; Twenty-sixth Informational Supplement. CLSI document M100-S26. Clinical and Laboratory Standards Institute, 950 West Valley Rd., Suite 2500, Wayne, PA 19087, USA, 2016.
- Patel J, Gorwitz RJ, et al. Mupirocin Resistance. Clinical Infectious Diseases. 2009; 49(6): 935-41.
- Clinical and Laboratory Standards Institute (CLSI). Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria that Grow Aerobically; Approved Standard – Tenth Edition. CLSI document M07-A10. Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087, USA, 2015.
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Disk Diffusion Susceptibility Tests; Approved Standard – Twelfth Edition. CLSI document M02-A12. Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087, USA, 2015.
- Finlay JE, Miller LA, Poupard JA. Interpretive criteria for testing susceptibility of staphylococci to mupirocin. Antimicrob Agents Chemother. 1997;41(5):1137-1139.
16 HOW SUPPLIED/STORAGE AND HANDLING
Each gram of Mupirocin Ointment USP, 2% contains 20 mg mupirocin in a water-miscible ointment base.
Mupirocin Ointment USP, 2% is supplied in 22-gram tubes.
NDC 76420-128-22 (22-gram tube) (relabeled from NDC 45802-112-22)
Store at 20-25°C (68-77°F) [see USP Controlled Room Temperature].
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Advise the patient to administer Mupirocin Ointment USP, 2% as follows:
- Use Mupirocin Ointment USP, 2% only as directed by the healthcare provider. It is for external use only. Avoid contact of Mupirocin Ointment USP, 2% with the eyes. If Mupirocin Ointment USP, 2% gets in the eyes, rinse thoroughly with water.
- Do not use Mupirocin Ointment USP, 2% in the nose.
- Wash your hands before and after applying Mupirocin Ointment USP, 2%.
- Use a gauze pad or cotton swab to apply a small amount of Mupirocin Ointment USP, 2% to the affected area. The treated area may be covered by gauze dressing if desired.
- Report to the healthcare provider any signs of local adverse reactions. Mupirocin Ointment USP, 2% should be stopped and the healthcare provider contacted if irritation, severe itching, or rash occurs.
- Report to the healthcare provider or go to the nearest emergency room if severe allergic reactions, such as swelling of the lips, face, or tongue, or wheezing occur [ see Warnings and Precautions (5.1)].
- If impetigo has not improved in 3 to 5 days, contact the healthcare provider.
*BACTROBAN is a registered trademark of the GSK group of companies.
PATIENT INFORMATION
Mupirocin Ointment USP, 2%
What is Mupirocin Ointment USP, 2%?
Mupirocin Ointment USP, 2% is a prescription medicine used on the skin (topical use) to treat a skin infection called impetigo that is caused by bacteria called Staphylococcus aureus and Streptococcus pyogenes.
It is not known if Mupirocin Ointment USP, 2% is safe and effective in children under 2 months of age.
Who should not use Mupirocin Ointment USP, 2%?
Do not use Mupirocin Ointment USP, 2% if:
- you are allergic to mupirocin or any of the ingredients in Mupirocin Ointment USP, 2%. See the end of this Patient Information leaflet for a complete list of the ingredients in Mupirocin Ointment USP, 2%.
What should I tell my healthcare provider before using Mupirocin Ointment USP, 2%?
Before using Mupirocin Ointment USP, 2%, tell your healthcare provider about all of your medical conditions including if you:
- have kidney problems
- are pregnant or plan to become pregnant. It is not known if Mupirocin Ointment USP, 2% will harm your unborn baby.
- are breastfeeding or plan to breastfeed. It is not known if Mupirocin Ointment USP, 2% passes into your breast milk. You and your healthcare provider should decide if you can use Mupirocin Ointment USP, 2% while breastfeeding.
Tell your healthcare provider about all of the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. Do not mix Mupirocin Ointment USP, 2% with other lotions, creams, or ointments.
How should I use Mupirocin Ointment USP, 2%?
- Mupirocin Ointment USP, 2% is for use on the skin (topical). Do not get Mupirocin Ointment USP, 2% in your eyes, nose, mouth, or vagina (mucosal surfaces).
- Use Mupirocin Ointment USP, 2% exactly as your healthcare provider tells you to use it.
- Apply a small amount of Mupirocin Ointment USP, 2%, with a cotton swab or gauze pad, to the affected area 3 times each day.
- It is important that you take the full course of Mupirocin Ointment USP, 2%. Do not stop early because your symptoms may disappear before the infection is fully cleared.
- Wash your hands before and after applying Mupirocin Ointment USP, 2%.
- After applying Mupirocin Ointment USP, 2%, you may cover the treated area with a clean gauze pad, unless your healthcare provider has told you to leave it uncovered.
- Talk to your healthcare provider if your skin does not improve after 3 to 5 days of treatment with Mupirocin Ointment USP, 2%.
- If you are breastfeeding and use Mupirocin Ointment USP, 2% on your breast or nipple, wash the area well before breastfeeding your child.
What are the possible side effects of Mupirocin Ointment USP, 2%?
Mupirocin Ointment USP, 2% may cause serious side effects, including:
- severe allergic reactions. Stop using Mupirocin Ointment USP, 2% and call your healthcare provider or go to the nearest emergency room right away if you have any of the following signs or symptoms of a severe allergic reaction:
ο hives
ο swelling of your face, lips, mouth, or tongue
ο a rash over your whole body
ο trouble breathing or wheezing
ο dizziness, fast heartbeat or pounding in your chest
- eye irritation. Do not get Mupirocin Ointment USP, 2% in your eyes. If Mupirocin Ointment USP, 2% gets in your eyes, rinse your eyes well with water.
- irritation in the area Mupirocin Ointment USP, 2% is used. Stop using Mupirocin Ointment USP, 2% and call your healthcare provider if you develop an irritation, severe itching, or a rash while using Mupirocin Ointment USP, 2%.
- a type of diarrhea called clostridium difficile-associated diarrhea (CDAD) . CDAD may happen in people who use or have used medicine to treat bacterial infections. The severity of CDAD can range from mild diarrhea to severe diarrhea that may cause death (fatal colitis).
- Call your healthcare provider or go to the nearest emergency room right away if you have diarrhea while using or after you stop using Mupirocin Ointment USP, 2%.
- risk of absorption of polyethylene glycol through the skin. Mupirocin Ointment USP, 2% contains polyethylene glycol, which in large amounts can cause kidney damage. You should not apply Mupirocin Ointment USP, 2% to open skin wounds or damaged skin, especially if you have kidney problems
- increased risk of infection at IV (intravenous) sites. Mupirocin Ointment USP, 2% should not be used on skin that is near an IV (intravenous) site.
The most common side effects of Mupirocin Ointment USP, 2% include:
- burning
- stinging or pain
- itching
These are not all the possible side effects of Mupirocin Ointment USP, 2%. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store Mupirocin Ointment USP, 2%?
- Store Mupirocin Ointment USP, 2% at room temperature between 68°F to 77°F (20°C to 25°C).
- Keep Mupirocin Ointment USP, 2% and all medicines out of the reach of children.
General information about the safe and effective use of Mupirocin Ointment USP, 2%
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet.
Do not use Mupirocin Ointment USP, 2% for a condition for which it was not prescribed. Do not give Mupirocin Ointment USP, 2% to other people, even if they have the same symptoms that you have.
It may harm them. You can ask your pharmacist or healthcare provider for information about Mupirocin Ointment USP, 2% that is written for health professionals.
What are the ingredients in Mupirocin Ointment USP, 2%?
Active Ingredient: mupirocin
Inactive Ingredients: polyethylene glycol 400 and polyethylene glycol 3350
This Patient Information has been approved by the U.S. Food and Drug Administration.