WARNING
This drug should be used primarily for treatment of patients with progressive and potentially life-threatening fungal infections; it should not be used to treat noninvasive forms of fungal disease such as oral thrush, vaginal candidiasis and esophageal candidiasis in patients with normal neutrophil counts.
Amphotericin B for Injection should not be given in doses greater than 1.5 mg/kg.
EXERCISE CAUTION to prevent inadvertent overdosage, which may result in potentially fatal cardiac or cardiopulmonary arrest (see WARNINGS, OVERDOSAGE and DOSAGE AND ADMINISTRATION). Verify the product name and dosage pre-administration, especially if dose exceeds 1.5 mg/kg.
DESCRIPTION
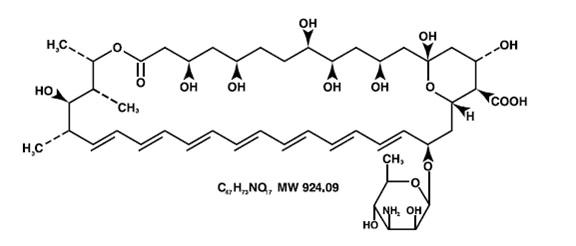
Amphotericin B for Injection USP contains amphotericin B, an antifungal polyene antibiotic obtained from a strain of Streptomyces nodosus. Amphotericin B is designated chemically as [1R- (1R*, 3S*, 5R*, 6R*, 9R*, 11R*, 15S*, 16R*, 17R*, 18S*, 19E, 21E, 23E, 25E, 27E, 29E, 31E, 33R*, 35S*, 36R*, 37S*)] -33-[(3-Amino-3, 6-dideoxy-β-D-mannopyranosyl)-oxy]-1,3,5,6,9,11,17,37-octahydroxy-15,16,18-trimethyl-13-oxo-14,39-dioxabicyclo [33.3.1] nonatriaconta-19,21,23,25,27,29,31-heptaene-36-carboxylic acid. Structural formula:
Each vial contains a sterile, nonpyrogenic, lyophilized cake (which may partially reduce to powder following manufacture) providing 50 mg amphotericin B and 41 mg sodium desoxycholate buffered with 20.2 mg sodium phosphates (consisting of mono and dibasic sodium phosphate, phosphoric acid and sodium hydroxide). Crystalline amphotericin B is insoluble in water; therefore, the antibiotic is solubilized by the addition of sodium desoxycholate to form a mixture which provides a colloidal dispersion for intravenous infusion following reconstitution.
At the time of manufacture the air in the vial is replaced by nitrogen.
CLINICAL PHARMACOLOGY
Microbiology
Amphotericin B shows a high order of in vitro activity against many species of fungi. Histoplasma capsulatum, Coccidioides immitis, Candida species, Blastomyces dermatitidis, Rhodotorula, Cryptococcus neoformans, Sporothrix schenckii, Mucor mucedo, and Aspergillus fumigatus are all inhibited by concentrations of amphotericin B ranging from 0.03 to 1.0 mcg/mL in vitro. While Candida albicans is generally quite susceptible to amphotericin B, non-albicans species may be less susceptible. Pseudallescheria boydii and Fusarium sp. are often resistant to amphotericin B. The antibiotic is without effect on bacteria, rickettsiae, and viruses.
Susceptibility Testing
Standardized techniques for susceptibility testing for antifungal agents have not been established and results of susceptibility studies have not been correlated with clinical outcomes.
Pharmacokinetics
Amphotericin B is fungistatic or fungicidal depending on the concentration obtained in body fluids and the susceptibility of the fungus. The drug acts by binding to sterols in the cell membrane of susceptible fungi with a resultant change in membrane permeability allowing leakage of intracellular components. Mammalian cell membranes also contain sterols and it has been suggested that the damage to human cells and fungal cells may share common mechanisms.
An initial intravenous infusion of 1 to 5 mg of amphotericin B per day, gradually increased to 0.4 to 0.6 mg/kg daily, produces peak plasma concentrations ranging from approximately 0.5 to 2 mcg/mL. Following a rapid initial fall, plasma concentrations plateau at about 0.5 mcg/mL. An elimination half-life of approximately 15 days follows an initial plasma half-life of about 24 hours. Amphotericin B circulating in plasma is highly bound (>90%) to plasma proteins and is poorly dialyzable. Approximately two thirds of concurrent plasma concentrations have been detected in fluids from inflamed pleura, peritoneum, synovium, and aqueous humor. Concentrations in the cerebrospinal fluid seldom exceed 2.5% of those in the plasma. Little amphotericin B penetrates into vitreous humor or normal amniotic fluid. Complete details of tissue distribution are not known.
Amphotericin B is excreted very slowly (over weeks to months) by the kidneys with 2 to 5% of a given dose being excreted in the biologically active form. Details of possible metabolic pathways are not known. After treatment is discontinued, the drug can be detected in the urine for at least 7 weeks due to the slow disappearance of the drug. The cumulative urinary output over a 7 day period amounts to approximately 40% of the amount of drug infused.
INDICATIONS & USAGE
Amphotericin B for Injection USP should be administered primarily to patients with progressive, potentially life-threatening fungal infections. This potent drug should not be used to treat noninvasive fungal infections, such as oral thrush, vaginal candidiasis and esophageal candidiasis in patients with normal neutrophil counts.
Amphotericin B for Injection USP is specifically intended to treat potentially life-threatening fungal infections: aspergillosis, cryptococcosis (torulosis), North American blastomycosis, systemic candidiasis, coccidioido-mycosis, histoplasmosis, zygomycosis including mucormycosis due to susceptible species of the genera Absidia, Mucor and Rhizopus, and infections due to related susceptible species of Conidiobolus and Basidiobolus, and sporotrichosis.
Amphotericin B may be useful in the treatment of American mucocutaneous leishmaniasis, but it is not the drug of choice as primary therapy.
CONTRAINDICATIONS
This product is contraindicated in those patients who have shown hypersensitivity to amphotericin B or any other component in the formulation unless, in the opinion of the physician, the condition requiring treatment is life-threatening and amenable only to amphotericin B therapy.
WARNINGS
Amphotericin B is frequently the only effective treatment available for potentially life-threatening fungal disease. In each case, its possible life-saving benefit must be balanced against its untoward and dangerous side effects.
EXERCISE CAUTION to prevent inadvertent Amphotericin B for Injection overdose, which can result in potentially fatal cardiac or cardiopulmonary arrest. Verify the product name and dosage dosage pre-administration, especially if dose exceeds 1.5 mg/kg. (see OVERDOSAGE and DOSAGE AND ADMINISTRATION)
PRECAUTIONS
General
Amphotericin B should be administered intravenously under close clinical observation by medically trained personnel. It should be reserved for treatment of patients with progressive, potentially life-threatening fungal infections due to susceptible organisms (see INDICATIONS AND USAGE).
Acute reactions including fever, shaking chills, hypotension, anorexia, nausea, vomiting, headache, and tachypnea are common 1 to 3 hours after starting an intravenous infusion. These reactions are usually more severe with the first few doses of amphotericin B and usually diminish with subsequent doses.
Rapid intravenous infusion has been associated with hypotension, hypokalemia, arrhythmias, and shock and should, therefore, be avoided (see DOSAGE AND ADMINISTRATION).
Amphotericin B should be used with care in patients with reduced renal function; frequent monitoring of renal function is recommended (see PRECAUTIONS: Laboratory Tests and ADVERSE REACTIONS). In some patients hydration and sodium repletion prior to amphotericin B administration may reduce the risk of developing nephrotoxicity. Supplemental alkali medication may decrease renal tubular acidosis complications.
Since acute pulmonary reactions have been reported in patients given amphotericin B during or shortly after leukocyte transfusions, it is advisable to temporarily separate these infusions as far as possible and to monitor pulmonary function (see PRECAUTIONS: Drug Interactions).
Leukoencephalopathy has been reported following use of amphotericin B. Literature reports have suggested that total body irradiation may be a predisposition.
Whenever medication is interrupted for a period longer than 7 days, therapy should be resumed by starting with the lowest dosage level, e.g., 0.25 mg/kg of body weight, and increased gradually as outlined under DOSAGE AND ADMINISTRATION.
Laboratory Tests
Renal function should be monitored frequently during amphotericin B therapy (see ADVERSE REACTIONS). It is also advisable to monitor on a regular basis liver function, serum electrolytes (particularly magnesium and potassium), blood counts, and hemoglobin concentrations. Laboratory test results should be used as a guide to subsequent dosage adjustments.
Drug Interactions
When administered concurrently, the following drugs may interact with amphotericin B:
Antineoplastic agents: may enhance the potential for renal toxicity, bronchospasm and hypotension. Antineoplastic agents (e.g., nitrogen mustard, etc.) should be given concomitantly only with great caution.
Corticosteroids and Corticotropin (ACTH): may potentiate amphotericin B-induced hypokalemia which may predispose the patient to cardiac dysfunction. Avoid concomitant use unless necessary to control side effects of amphotericin B. If used concomitantly, closely monitor serum electrolytes and cardiac function (see ADVERSE REACTIONS).
Digitalis glycosides: amphotericin B-induced hypokalemia may potentiate digitalis toxicity. Serum potassium levels and cardiac function should be closely monitored and any deficit promptly corrected.
Flucytosine: while a synergistic relationship with amphotericin B has been reported, concomitant use may increase the toxicity of flucytosine by possibly increasing its cellular uptake and/or impairing its renal excretion.
Imidazoles (e.g., ketoconazole, miconazole, clotrimazole, fluconazole, etc.): in vitro and animal studies with the combination of amphotericin B and imidazoles suggest that imidazoles may induce fungal resistance to amphotericin B. Combination therapy should be administered with caution, especially in immunocompromised patients.
Other nephrotoxic medications: agents such as aminoglycosides, cyclosporine, and pentamidine may enhance the potential for drug-induced renal toxicity, and should be used concomitantly only with great caution. Intensive monitoring of renal function is recommended in patients requiring any combination of nephrotoxic medications (see PRECAUTIONS: Laboratory Tests).
Skeletal muscle relaxants: amphotericin B-induced hypokalemia may enhance the curariform effect of skeletal muscle relaxants (e.g., tubocurarine). Serum potassium levels should be monitored and deficiencies corrected.
Leukocyte transfusions: acute pulmonary toxicity has been reported in patients receiving intravenous amphotericin B and leukocyte transfusions (see PRECAUTIONS: General).
Carcinogenesis, Mutagenesis, Impairment of Fertility
No long-term studies in animals have been performed to evaluate carcinogenic potential. There also have been no studies to determine mutagenicity or whether this medication affects fertility in males or females.
Pregnancy
Teratogenic Effects
Pregnancy Category B: Reproduction studies in animals have revealed no evidence of harm to the fetus due to amphotericin B for injection. Systemic fungal infections have been successfully treated in pregnant women with amphotericin B for injection without obvious effects to the fetus, but the number of cases reported has been small. Because animal reproduction studies are not always predictive of human response, and adequate and well-controlled studies have not been conducted in pregnant women, this drug should be used during pregnancy only if clearly indicated.
Nursing Mothers
It is not known whether amphotericin B is excreted in human milk. Because many drugs are excreted in human milk and considering the potential toxicity of amphotericin B, it is prudent to advise a nursing mother to discontinue nursing.
Pediatric Use
Safety and effectiveness in pediatric patients have not been established through adequate and well-controlled studies. Systemic fungal infections have been successfully treated in pediatric patients without reports of unusual side effects. Amphotericin B for Injection when administered to pediatric patients should be limited to the smallest dose compatible with an effective therapeutic regimen.
ADVERSE REACTIONS
Although some patients may tolerate full intravenous doses of amphotericin B without difficulty, most will exhibit some intolerance, often at less than the full therapeutic dose.
Tolerance may be improved by treatment with aspirin, antipyretics (e.g., acetaminophen), antihistamines, or antiemetics. Meperidine (25 to 50 mg IV) has been shown in some patients to decrease the duration of shaking chills and fever that may accompany the infusion of amphotericin B.
Administration of amphotericin B on alternate days may decrease anorexia and phlebitis.
Intravenous administration of small doses of adrenal corticosteroids just prior to or during the amphotericin B infusion may help decrease febrile reactions. Dosage and duration of such corticosteroid therapy should be kept to a minimum (see PRECAUTIONS: Drug Interactions).
Addition of heparin (1000 units per infusion), and the use of a pediatric scalp-vein needle may lessen the incidence of thrombophlebitis. Extravasation may cause chemical irritation.
The adverse reactions most commonly observed are:
General (body as a whole): fever (sometimes accompanied by shaking chills usually occurring within 15 to 20 minutes after initiation of treatment); malaise; weight loss.
Cardiopulmonary: hypotension; tachypnea.
Gastrointestinal: anorexia; nausea; vomiting; diarrhea; dyspepsia; cramping epigastric pain.
Hematologic: normochromic, normocytic anemia.
Local: pain at the injection site with or without phlebitis or thrombophlebitis.
Musculoskeletal: generalized pain, including muscle and joint pains.
Neurologic: headache.
Renal: decreased renal function and renal function abnormalities including: azotemia, hypokalemia, hyposthenuria, renal tubular acidosis; and nephrocalcinosis. These usually improve with interruption of therapy. However, some permanent impairment often occurs, especially in those patients receiving large amounts (over 5 g) of amphotericin B or receiving other nephrotoxic agents. In some patients hydration and sodium repletion prior to amphotericin B administration may reduce the risk of developing nephrotoxicity. Supplemental alkali medication may decrease renal tubular acidosis.
The following adverse reactions have also been reported:
General (body as a whole): flushing.
Allergic: anaphylactoid and other allergic reactions; bronchospasm; wheezing.
Cardiopulmonary: cardiac arrest; shock; cardiac failure; pulmonary edema; hypersensitivity pneumonitis; arrhythmias, including ventricular fibrillation; dyspnea; hypertension.
Dermatologic: rash, in particular maculopapular; pruritus. Skin exfoliation, toxic epidermal necrolysis, and Stevens-Johnson syndrome have been reported during post-marketing surveillance.
Gastrointestinal: acute liver failure; hepatitis; jaundice; hemorrhagic gastroenteritis; melena.
Hematologic: agranulocytosis; coagulation defects; thrombocytopenia; leukopenia; eosinophilia; leukocytosis.
Neurologic: convulsions; hearing loss; tinnitus; transient vertigo; visual impairment; diplopia; peripheral neuropathy; encephalopathy (see PRECAUTIONS); other neurologic symptoms.
Renal: acute renal failure; anuria; oliguria. Nephrogenic diabetes insipidus has been reported during post-marketing surveillance.
Altered Laboratory Findings
Serum Electrolytes: Hypomagnesemia; hypo- and hyperkalemia; hypocalcemia.
Liver Function Tests: Elevations of AST, ALT, GGT, bilirubin, and alkaline phosphatase.
Renal Function Tests: Elevations of BUN and serum creatinine.
OVERDOSAGE
Amphotericin B overdoses can result in potentially fatal cardiac or cardiopulmonary arrest (see WARNINGS and DOSAGE AND ADMINISTRATION). If an overdose is suspected, discontinue therapy and monitor the patient's clinical status (e.g., cardiorespiratory, renal, and liver function, hematologic status, serum electrolytes) and administer supportive therapy, as required. Amphotericin B is not hemodialyzable.
Prior to reinstituting therapy, the patient's condition should be stabilized (including correction of electrolyte deficiencies, etc.).
DOSAGE & ADMINISTRATION
**VERIFY PRODUCT NAME AND DOSAGE.**
CAUTION: Under no circumstances should a total daily dose of 1.5 mg/kg be exceeded.
Amphotericin B overdoses can result in potentially fatal cardiac or cardiopulmonary arrest (see WARNINGS and OVERDOSAGE).
Amphotericin B for Injection should be administered by slow intravenous infusion. Intravenous infusion should be given over a period of approximately 2 to 6 hours (depending on the dose) observing the usual precautions for intravenous therapy (see PRECAUTIONS: General). The recommended concentration for intravenous infusion is 0.1 mg/mL (1mg/10mL).
Since patient tolerance varies greatly, the dosage of amphotericin B must be individualized and adjusted according to the patient's clinical status (e.g., site and severity of infection, etiologic agent, cardio-renal function, etc.).
A single intravenous test dose (1 mg in 20 mL of 5% dextrose solution) administered over 20 to 30 minutes may be preferred. The patient's temperature, pulse, respiration, and blood pressure should be recorded every 30 minutes for 2 to 4 hours.
In patients with good cardio-renal function and a well tolerated test dose, therapy is usually initiated with a daily dose of 0.25 mg/kg of body weight. However, in those patients having severe and rapidly progressive fungal infection, therapy may be initiated with a daily dose of 0.3 mg/kg of body weight. In patients with impaired cardio-renal function or a severe reaction to the test dose, therapy should be initiated with smaller daily doses (i.e., 5 to 10 mg).
Depending on the patient's cardio-renal status (see PRECAUTIONS: Laboratory Tests), doses may gradually be increased by 5 to 10 mg per day to final daily dosage of 0.5 to 0.7 mg/kg.
There are insufficient data presently available to define total dosage requirements and duration of treatment necessary for eradication of specific mycoses. The optimal dose is unknown. Total daily dosage may range up to 1.0 mg/kg per day or up to 1.5 mg/kg when given on alternate days.
Sporotrichosis: Therapy with intravenous amphotericin B for sporotrichosis has ranged up to nine months with a total dose up to 2.5 g.
Aspergillosis: Aspergillosis has been treated with amphotericin B intravenously for a period up to 11 months with a total dose up to 3.6 g.
Rhinocerebral phycomycosis: This fulminating disease generally occurs in association with diabetic ketoacidosis. It is, therefore, imperative that diabetic control be restored in order for treatment with Amphotericin B for Injection to be successful. In contradistinction, pulmonary phycomycosis, which is more common in association with hematologic malignancies, is often an incidental finding at autopsy. A cumulative dose of at least 3 g of amphotericin B is recommended to treat rhinocerebral phycomycosis. Although a total dose of 3 to 4 g will infrequently cause lasting renal impairment, this would seem a reasonable minimum where there is clinical evidence of invasion of deep tissue. Since rhinocerebral phycomycosis usually follows a rapidly fatal course, the therapeutic approach must necessarily be more aggressive than that used in more indolent mycoses.
Preparation of Solutions
Reconstitute as follows: An initial concentrate of 5 mg amphotericin B per mL is first prepared by rapidly expressing 10 mL Sterile Water for Injection USP without a bacteriostatic agent directly into the lyophilized cake, using a sterile needle (minimum diameter: 20 gauge) and syringe. Shake the vial immediately until the colloidal solution is clear. The infusion solution, providing 0.1 mg amphotericin B per mL, is then obtained by further dilution (1:50) with 5% Dextrose Injection USP of pH above 4.2. The pH of each container of Dextrose Injection should be ascertained before use. Commercial Dextrose Injection usually has a pH above 4.2; however, if it is below 4.2, then 1 or 2 mL of buffer should be added to the Dextrose Injection before it is used to dilute the concentrated solution of amphotericin B. The recommended buffer has the following composition:
| Dibasic sodium phosphate (anhydrous) | 1.59 g |
| Monobasic sodium phosphate (anhydrous) | 0.96 g |
| Water for Injection USP | qs 100.0 mL |
The buffer should be sterilized before it is added to the Dextrose Injection, either by filtration through a bacterial retentive stone, mat, or membrane, or by autoclaving for 30 minutes at 15 lb pressure (121˚C).
CAUTION: Aseptic technique must be strictly observed in all handling, since no preservative or bacteriostatic agent is present in the antibiotic or in the materials used to prepare it for administration. All entries into the vial or into the diluents must be made with a sterile needle. Do not reconstitute with saline solutions. The use of any diluent other than the ones recommended or the presence of a bacteriostatic agent (e.g., benzyl alcohol) in the diluent may cause precipitation of the antibiotic. Do not use the initial concentrate or the infusion solution if there is any evidence of precipitation or foreign matter in either one.
An in-line membrane filter may be used for intravenous infusion of amphotericin B; however, the mean pore diameter of the filter should not be less than 1.0 micron in order to assure passage of the antibiotic dispersion.
HOW SUPPLIED
Amphotericin B for Injection USP
Available as single vials providing 50 mg amphotericin B as a yellow to orange lyophilized cake (which may partially reduce to powder following manufacture). NDC 39822-1055-5. Retain in carton until time of use.
Storage
Prior to reconstitution Amphotericin B for Injection USP should be stored under refrigeration, 2˚ to 8˚C (36˚to 46˚F), protected against exposure to light. The concentrate (5 mg amphotericin B per mL after reconstitution with 10 mL Sterile Water for Injection USP) may be stored in the dark, at room temperature for 24 hours, or at refrigerator temperatures for one week with minimal loss of potency and clarity. Any unused material should then be discarded. Solutions prepared for intravenous infusion (0.1 mg or less amphotericin B per mL) should be used promptly after preparation and should be protected from light during administration.
Manufactured for:

XGen Pharmaceuticals DJB, Inc.
Big Flats, NY 14814

Revised October 2020
AM-PI-05
Printed in the USA