DESCRIPTION
Sumatriptan tablets USP contain sumatriptan (as the succinate), a selective 5-hydroxytryptamine1 receptor subtype agonist. Sumatriptan succinate USP is chemically designated as 3-[2- (dimethylamino) ethyl]-N-methyl-indole-5-methanesulfonamide succinate (1:1), and it has the following structure:
The molecular formula is C14H21N3O2S•C4H6O4, representing a molecular weight of 413.5. Sumatriptan succinate USP is a white to off-white powder that is readily soluble in water and in saline. Each sumatriptan tablet USP for oral administration contains 35, 70, or 140 mg of sumatriptan succinate USP equivalent to 25, 50, or 100 mg of sumatriptan, respectively. Each tablet also contains the inactive ingredients croscarmellose sodium, lactose anhydrous, lactose monohydrate, magnesium stearate, mannitol, microcrystalline cellulose, talc, titanium dioxide and triacetin.
CLINICAL PHARMACOLOGY
Mechanism of Action
Sumatriptan is an agonist for a vascular 5-hydroxytryptamine1 receptor subtype (probably a member of the 5-HT1D family) having only a weak affinity for 5-HT1A, 5-HT5A, and 5-HT7 receptors and no significant affinity (as measured using standard radioligand binding assays) or pharmacological activity at 5-HT2, 5-HT3, or 5-HT4 receptor subtypes or at alpha1-, alpha2-, or beta-adrenergic; dopamine1; dopamine2; muscarinic; or benzodiazepine receptors.
The vascular 5-HT1 receptor subtype that sumatriptan activates is present on cranial arteries in both dog and primate, on the human basilar artery, and in the vasculature of human dura mater and mediates vasoconstriction. This action in humans correlates with the relief of migraine headache. In addition to causing vasoconstriction, experimental data from animal studies show that sumatriptan also activates 5-HT1 receptors on peripheral terminals of the trigeminal nerve innervating cranial blood vessels. Such an action may also contribute to the antimigrainous effect of sumatriptan in humans.
In the anesthetized dog, sumatriptan selectively reduces the carotid arterial blood flow with little or no effect on arterial blood pressure or total peripheral resistance. In the cat, sumatriptan selectively constricts the carotid arteriovenous anastomoses while having little effect on blood flow or resistance in cerebral or extracerebral tissues.
Pharmacokinetics
The mean maximum concentration following oral dosing with 25 mg is 18 ng/mL (range: 7 to 47 ng/mL) and 51 ng/mL (range: 28 to 100 ng/mL) following oral dosing with 100 mg of sumatriptan. This compares with a Cmax of 5 and 16 ng/mL following dosing with a 5 and 20 mg intranasal dose, respectively. The mean Cmax following a 6 mg subcutaneous injection is 71 ng/mL (range: 49 to 110 ng/mL). The bioavailability is approximately 15%, primarily due to presystemic metabolism and partly due to incomplete absorption. The Cmax is similar during a migraine attack and during a migraine-free period, but the tmax is slightly later during the attack, approximately 2.5 hours compared to 2.0 hours. When given as a single dose, sumatriptan displays dose proportionality in its extent of absorption (area under the curve [AUC]) over the dose range of 25 to 200 mg, but the Cmax after 100 mg is approximately 25% less than expected (based on the 25 mg dose).
A food effect study involving administration of sumatriptan tablets 100 mg to healthy volunteers under fasting conditions and with a high-fat meal indicated that the Cmax and AUC were increased by 15% and 12 %, respectively, when administered in the fed state.
Plasma protein binding is low (14% to 21%). The effect of sumatriptan on the protein binding of other drugs has not been evaluated, but would be expected to be minor, given the low rate of protein binding. The apparent volume of distribution is 2.4 L/kg.
The elimination half-life of sumatriptan is approximately 2.5 hours. Radiolabeled 14C-sumatriptan administered orally is largely renally excreted (about 60%) with about 40% found in the feces. Most of the radiolabeled compound excreted in the urine is the major metabolite, indole acetic acid (IAA), which is inactive, or the IAA glucuronide. Only 3% of the dose can be recovered as unchanged sumatriptan.
In vitro studies with human microsomes suggest that sumatriptan is metabolized by monoamine oxidase (MAO), predominantly the A isoenzyme, and inhibitors of that enzyme may alter sumatriptan pharmacokinetics to increase systemic exposure. No significant effect was seen with an MAO-B inhibitor (see CONTRAINDICATIONS,WARNINGS, and PRECAUTIONS: Drug Interactions).
Special Populations
Renal Impairment
Renal Impairment:The effect of renal impairment on the pharmacokinetics of sumatriptan has not been examined, but little clinical effect would be expected as sumatriptan is largely metabolized to an inactive substance.
Hepatic Impairment
The liver plays an important role in the presystemic clearance of orally administered sumatriptan. Accordingly, the bioavailability of sumatriptan following oral administration may be markedly increased in patients with liver disease. In 1 small study of hepatically impaired patients (N = 8) matched for sex, age, and weight with healthy subjects, the hepatically impaired patients had an approximately 70% increase in AUC and Cmax and a tmax 40 minutes earlier compared to the healthy subjects (see DOSAGE AND ADMINISTRATION).
Age
The pharmacokinetics of oral sumatriptan in the elderly (mean age, 72 years; 2 males and 4 females) and in patients with migraine (mean age, 38 years; 25 males and 155 females) were similar to that in healthy male subjects (mean age, 30 years) (see PRECAUTIONS: Geriatric Use).
Drug Interactions
Monoamine Oxidase Inhibitors (MAO)
Treatment with MAO-A inhibitors generally leads to an increase of sumatriptan plasma levels (see CONTRAINDICATIONS and PRECAUTIONS).
Due to gut and hepatic metabolic first-pass effects, the increase of systemic exposure after coadministration of an MAO-A inhibitor with oral sumatriptan is greater than after coadministration of the monoamine oxidase inhibitors (MAOI) with subcutaneous sumatriptan. In a study of 14 healthy females, pretreatment with an MAO-A inhibitor decreased the clearance of subcutaneous sumatriptan. Under the conditions of this experiment, the result was a 2-fold increase in the area under the sumatriptan plasma concentration x time curve (AUC), corresponding to a 40% increase in elimination half-life. This interaction was not evident with an MAO-B inhibitor.
A small study evaluating the effect of pretreatment with an MAO-A inhibitor on the bioavailability from a 25 mg oral sumatriptan tablet resulted in an approximately 7-fold increase in systemic exposure.
CLINICAL STUDIES
The efficacy of sumatriptan tablets in the acute treatment of migraine headaches was demonstrated in 3, randomized, double-blind, placebo-controlled studies. Patients enrolled in these 3 studies were predominately female (87%) and Caucasian (97%), with a mean age of 40 years (range, 18 to 65 years). Patients were instructed to treat a moderate to severe headache. Headache response, defined as a reduction in headache severity from moderate or severe pain to mild or no pain, was assessed up to 4 hours after dosing. Associated symptoms such as nausea, photophobia, and phonophobia were also assessed. Maintenance of response was assessed for up to 24 hours postdose. A second dose of sumatriptane tablets or other medication was allowed 4 to 24 hours after the initial treatment for recurrent headache. Acetaminophen was offered to patients in Studies 2 and 3 beginning at 2 hours after initial treatment if the migraine pain had not improved or worsened. Additional medications were allowed 4 to 24 hours after the initial treatment for recurrent headache or as rescue in all 3 studies. The frequency and time to use of these additional treatments were also determined. In all studies, doses of 25, 50, and 100 mg were compared to placebo in the treatment of migraine attacks. In 1 study, doses of 25, 50, and 100 mg were also compared to each other.
In all 3 trials, the percentage of patients achieving headache response 2 and 4 hours after treatment was significantly greater among patients receiving sumatriptan tablets at all doses compared to those who received placebo. In 1 of the 3 studies, there was a statistically significant greater percentage of patients with headache response at 2 and 4 hours in the 50 or 100 mg group when compared to the 25 mg dose groups. There were no statistically significant differences between the 50 and 100 mg dose groups in any study. The results from the 3 controlled clinical trials are summarized in Table 1.
Comparisons of drug performance based upon results obtained in different clinical trials are never reliable. Because studies are conducted at different times, with different samples of patients, by different investigators, employing different criteria and/or different interpretations of the same criteria, under different conditions (dose, dosing regimen, etc.), quantitative estimates of treatment response and the timing of response may be expected to vary considerably from study to study.
|
Placebo 2 hr 4 hr |
Sumatriptan Tablets 25 mg 2 hr 4 hr |
Sumatriptan Tablets 50 mg 2 hr 4 hr |
Sumatriptan Tablets 100 mg 2 hr 4 hr |
|
|
Study 1 |
27% 38% |
52%a 67%a |
61%ab %ab |
62%ab 79%ab |
|
(N = 94) |
(N = 298) |
(N = 296) |
(N = 296) |
|
|
Study 2 |
26% 38% |
52%a 70%a |
50%a 68%a |
56%a 71%a |
|
(N = 65) |
(N = 66) |
(N = 62) |
(N = 66) |
|
|
Study 3 |
17% 19% |
52%a 65%a |
54%a 72%a |
57%a 78%a |
|
(N = 47) |
(N = 48) |
(N = 46) |
(N = 46) |
ap<0.05 in comparison with placebo.
bp<0.05 in comparison with 25 mg.
The estimated probability of achieving an initial headache response over the 4 hours following treatment is depicted in Figure 1.
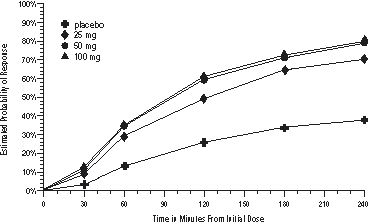
Figure 1. Estimated Probability of Achieving Initial Headache Response Within 240 Minutesa
a The figure shows the probability over time of obtaining headache response (no or mild pain) following treatment with sumatriptan. The averages displayed are based on pooled data from the 3 clinical controlled trials providing evidence of efficacy. Kaplan-Meier plot with patients not achieving response and/or taking rescue within 240 minutes censored to 240 minutes.
For patients with migraine-associated nausea, photophobia, and/or phonophobia at baseline, there was a lower incidence of these symptoms at 2 hours (Study 1) and at 4 hours (Studies 1, 2, and 3) following administration of sumatriptan tablets compared to placebo.
As early as 2 hours in Studies 2 and 3 or 4 hours in Study 1, through 24 hours following the initial dose of study treatment, patients were allowed to use additional treatment for pain relief in the form of a second dose of study treatment or other medication. The estimated probability of patients taking a second dose or other medication for migraine over the 24 hours following the initial dose of study treatment is summarized in Figure 2.
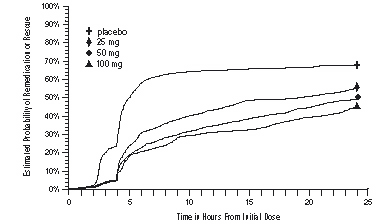
Figure 2. The Estimated Probability of Patients Taking a Second Dose or Other Medication for Migraine Over the 24 Hours Following the Initial Dose of Study Treatmenta
Figure 2. The Estimated Probability of Patients Taking a Second Dose or Other Medication for Migraine Over the 24 Hours Following the Initial Dose of Study Treatmenta
a Kaplan-Meier plot based on data obtained in the 3 clinical controlled trials providing evidence of efficacy with patients not using additional treatments censored to 24 hours. Plot also includes patients who had no response to the initial dose. No remedication was allowed within 2 hours postdose.
There is evidence that doses above 50 mg do not provide a greater effect than 50 mg. There was no evidence to suggest that treatment with sumatriptan was associated with an increase in the severity of recurrent headaches. The efficacy of sumatriptan tablets was unaffected by presence of aura; duration of headache prior to treatment; gender, age, or weight of the patient; relationship to menses; or concomitant use of common migraine prophylactic drugs (e.g., beta-blockers, calcium channel blockers, tricyclic antidepressants). There were insufficient data to assess the impact of race on efficacy.
INDICATIONS AND USAGE
Sumatriptan tablets are indicated for the acute treatment of migraine attacks with or without aura in adults.
Sumatriptan tablets are not intended for the prophylactic therapy of migraine or for use in the management of hemiplegic or basilar migraine (see CONTRAINDICATIONS). Safety and effectiveness of sumatriptan tablets have not been established for cluster headache, which is present in an older, predominantly male population.
CONTRAINDICATIONS
Sumatriptan tablets should not be given to patients with history, symptoms, or signs of ischemic cardiac, cerebrovascular, or peripheral vascular syndromes. In addition, patients with other significant underlying cardiovascular diseases should not receive sumatriptane tablets. Ischemic cardiac syndromes include, but are not limited to, angina pectoris of any type (e.g., stable angina of effort, vasospastic forms of angina such as the Prinzmetal variant), all forms of myocardial infarction, and silent myocardial ischemia.
Cerebrovascular syndromes include, but are not limited to, strokes of any type as well as transient ischemic attacks. Peripheral vascular disease includes, but is not limited to, ischemic bowel disease (see WARNINGS).
Because sumatriptan tablets may increase blood pressure, they should not be given to patients with uncontrolled hypertension.
Concurrent administration of MAO-A inhibitors or use within 2 weeks of discontinuation of MAO-A inhibitor therapy is contraindicated (see CLINICAL PHARMACOLOGY: Drug Interactions and PRECAUTIONS: Drug Interactions).
Sumatriptan tablets should not be administered to patients with hemiplegic or basilar migraine.
Sumatriptan tablets and any ergotamine-containing or ergot-type medication (like dihydroergotamine or methysergide) should not be used within 24 hours of each other, nor should sumatriptan and another 5-HT1 agonist.
Sumatriptan tablets are contraindicated in patients with hypersensitivity to sumatriptan or any of their components.
Sumatriptan tablets are contraindicated in patients with severe hepatic impairment.
WARNINGS
Sumatriptan tablets should only be used where a clear diagnosis of migraine headache has been established.
Risk of Myocardial Ischemia and/or Infarction and Other Adverse Cardiac Events
Sumatriptan should not be given to patients with documented ischemic or vasospastic coronary artery disease (CAD) (see CONTRAINDICATIONS). It is strongly recommended that sumatriptan not be given to patients in whom unrecognized CAD is predicted by the presence of risk factors (e.g., hypertension, hypercholesterolemia, smoker, obesity, diabetes, strong family history of CAD, female with surgical or physiological menopause, or male over 40 years of age) unless a cardiovascular evaluation provides satisfactory clinical evidence that the patient is reasonably free of coronary artery and ischemic myocardial disease or other significant underlying cardiovascular disease. The sensitivity of cardiac diagnostic procedures to detect cardiovascular disease or predisposition to coronary artery vasospasm is modest, at best. If, during the cardiovascular evaluation, the patient’s medical history or electrocardiographic investigations reveal findings indicative of, or consistent with, coronary artery vasospasm or myocardial ischemia, sumatriptan should not be administered (see CONTRAINDICATIONS).
For patients with risk factors predictive of CAD, who are determined to have a satisfactory cardiovascular evaluation, it is strongly recommended that administration of the first dose of sumatriptan tablets take place in the setting of a physician’s office or similar medically staffed and equipped facility unless the patient has previously received sumatriptan. Because cardiac ischemia can occur in the absence of clinical symptoms, consideration should be given to obtaining on the first occasion of use an electrocardiogram (ECG) during the interval immediately following sumatriptan tablets, in these patients with risk factors.
It is recommended that patients who are intermittent long-term users of sumatriptan and who have or acquire risk factors predictive of CAD, as described above, undergo periodic interval cardiovascular evaluation as they continue to use sumatriptan.
The systematic approach described above is intended to reduce the likelihood that patients with unrecognized cardiovascular disease will be inadvertently exposed to sumatriptan.
Drug-Associated Cardiac Events and Fatalities
Serious adverse cardiac events, including acute myocardial infarction, life-threatening disturbances of cardiac rhythm, and death have been reported within a few hours following the administration of sumatriptan succinate injection or sumatriptan tablets. Considering the extent of use of sumatriptan in patients with migraine, the incidence of these events is extremely low.
The fact that sumatriptan can cause coronary vasospasm, that some of these events have occurred in patients with no prior cardiac disease history and with documented absence of CAD, and the close proximity of the events to sumatriptan use support the conclusion that some of these cases were caused by the drug. In many cases, however, where there has been known underlying coronary artery disease, the relationship is uncertain.
Premarketing Experience With Sumatriptan
Of 6,348 patients with migraine who participated in premarketing controlled and uncontrolled clinical trials of oral sumatriptan, 2 experienced clinical adverse events shortly after receiving oral sumatriptan that may have reflected coronary vasospasm. Neither of these adverse events was associated with a serious clinical outcome.
Among the more than 1,900 patients with migraine who participated in premarketing controlled clinical trials of subcutaneous sumatriptan, there were 8 patients who sustained clinical events during or shortly after receiving sumatriptan that may have reflected coronary artery vasospasm. Six of these 8 patients had ECG changes consistent with transient ischemia, but without accompanying clinical symptoms or signs. Of these 8 patients, 4 had either findings suggestive of CAD or risk factors predictive of CAD prior to study enrollment.
Among approximately 4,000 patients with migraine who participated in premarketing controlled and uncontrolled clinical trials of sumatriptan nasal spray, 1 patient experienced an asymptomatic subendocardial infarction possibly subsequent to a coronary vasospastic event.
Postmarketing Experience With Sumatriptan
Serious cardiovascular events, some resulting in death, have been reported in association with the use of sumatriptan succinate injection or sumatriptan tablets. The uncontrolled nature of postmarketing surveillance, however, makes it impossible to determine definitively the proportion of the reported cases that were actually caused by sumatriptan or to reliably assess causation in individual cases. On clinical grounds, the longer the latency between the administration of sumatriptan and the onset of the clinical event, the less likely the association is to be causative. Accordingly, interest has focused on events beginning within 1 hour of the administration of sumatriptan.
Cardiac events that have been observed to have onset within 1 hour of sumatriptan administration include: coronary artery vasospasm, transient ischemia, myocardial infarction, ventricular tachycardia and ventricular fibrillation, cardiac arrest, and death.
Some of these events occurred in patients who had no findings of CAD and appear to represent consequences of coronary artery vasospasm. However, among domestic reports of serious cardiac events within 1 hour of sumatriptan administration, almost all of the patients had risk factors predictive of CAD and the presence of significant underlying
Drug-Associated Cerebrovascular Events and Fatalities
Cerebral hemorrhage, subarachnoid hemorrhage, stroke, and other cerebrovascular events have been reported in patients treated with oral or subcutaneous sumatriptan, and some have resulted in fatalities. The relationship of sumatriptan to these events is uncertain. In a number of cases, it appears possible that the cerebrovascular events were primary, sumatriptan having been administered in the incorrect belief that the symptoms experienced were a consequence of migraine when they were not. As with other acute migraine therapies, before treating headaches in patients not previously diagnosed as migraineurs, and in migraineurs who present with atypical symptoms, care should be taken to exclude other potentially serious neurological conditions. It should also be noted that patients with migraine may be at increased risk of certain cerebrovascular events (e.g., cerebrovascular accident, transient ischemic attack).
Other Vasospasm-Related Events
Sumatriptan may cause vasospastic reactions other than coronary artery vasospasm. Both peripheral vascular ischemia and colonic ischemia with abdominal pain and bloody diarrhea have been reported. Very rare reports of transient and permanent blindness and significant partial vision loss have been reported with the use of sumatriptan. Visual disorders may also be part of a migraine attack.
Serotonin Syndrome
Serotonin syndrome may occur with triptans, including Sumatriptan, particularly during combined use with selective serotonin reuptake inhibitors (SSRIs) or serotonin norepinephrine reuptake inhibitors (SNRIs).Serotonin synd rome symptoms may include mental status changes (e.g., agitation, hallucinations, coma), autonomic instability (e.g ., tachycardia, labile blood pressure, hyperthermia), neuromuscular aberrations (e.g., hyperr eflexia, incoordination), and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea). The on set of symptoms can occur within minutes to hours of receiving a new or a greater dose of a serotonergic medication. Treatment with Sumatriptan treatment should be discontinued if serotonin syndrome is suspected.
Increase in Blood Pressure
Significant elevation in blood pressure, including hypertensive crisis, has been reported on rare occasions in patients with and without a history of hypertension. Sumatriptan is contraindicated in patients with uncontrolled hypertension (see CONTRAINDICATIONS). Sumatriptan should be administered with caution to patients with controlled hypertension as transient increases in blood pressure and peripheral vascular resistance have been observed in a small proportion of patients.
Concomitant Drug Use
In patients taking MAO-A inhibitors, sumatriptan plasma levels attained after treatment with recommended doses are 7-fold higher following oral administration than those obtained under other conditions. Accordingly, the coadministration of sumatriptan tablets and an MAO-A inhibitor is contraindicated (see CLINICAL PHARMACOLOGY and CONTRAINDICATIONS).
Hypersensitivity
Hypersensitivity (anaphylaxis/anaphylactoid) reactions have occurred on rare occasions in patients receiving sumatriptan. Such reactions can be life threatening or fatal. In general, hypersensitivity reactions to drugs are more likely to occur in individuals with a history of sensitivity to multiple allergens (see CONTRAINDICATIONS).
PRECAUTIONS
General
Chest discomfort and jaw or neck tightness have been reported following use of sumatriptan tablets and have also been reported infrequently following administration of sumatriptan succinate Nasal Spray. Chest, jaw, or neck tightness is relatively common after administration of sumatriptan succinate injection. Only rarely have these symptoms been associated with ischemic ECG changes. However, because sumatriptan may cause coronary artery vasospasm, patients who experience signs or symptoms suggestive of angina following sumatriptan should be evaluated for the presence of CAD or a predisposition to Prinzmetal variant angina before receiving additional doses of sumatriptan, and should be monitored electrocardiographically if dosing is resumed and similar symptoms recur. Similarly, patients who experience other symptoms or signs suggestive of decreased arterial flow, such as ischemic bowel syndrome or Raynaud syndrome following sumatriptan should be evaluated for atherosclerosis or predisposition to vasospasm (see WARNINGS).
Sumatriptan should also be administered with caution to patients with diseases that may alter the absorption, metabolism, or excretion of drugs, such as impaired hepatic or renal function.
There have been rare reports of seizure following administration of sumatriptan. Sumatriptan should be used with caution in patients with a history of epilepsy or conditions associated with a lowered seizure threshold.
Care should be taken to exclude other potentially serious neurologic conditions before treating headache in patients not previously diagnosed with migraine headache or who experience a headache that is atypical for them. There have been rare reports where patients received sumatriptan for severe headaches that were subsequently shown to have been secondary to an evolving neurologic lesion (see WARNINGS).
For a given attack, if a patient does not respond to the first dose of sumatriptan, the diagnosis of migraine should be reconsidered before administration of a second dose.
Overuse:
Overuse of acute migraine drugs (e.g., ergotamine, triptans, opioids, or a combination of drugs for 10 or more days per month) may lead to exacerbation of headache (medication overuse headache). Medication overuse headache may present as migraine-like daily headaches, or as a marked increase in frequency of migraine attacks. Detoxification of patients, including withdrawal of the overused drugs, and treatment of withdrawal symptoms (which often includes a transient worsening of headache) may be necessary. Migraine patients should be informed about the risks of medication overuse, and encouraged to record headache frequency and drug use.
Information for Patients
See PATIENTINFORMATION at the end of this labeling for the text of the separate leaflet provided for patients.
Patients should be cautioned about the risk of serotonin syndrome with the use of sumatriptan or other triptans, especially during combined use with SSRIs or SNRIs.
Laboratory Tests
No specific laboratory tests are recommended for monitoring patients prior to and/or after treatment with sumatriptan.
Drug Interactions
Selective Serotonin Reuptake Inhibitors/Serotonin Norepinephrine Reuptake Inhibitors and Serotonin Syndrome:
Cases of life‑threatening serotonin syndrome have been reported during combined use of SSRIs or SNRIs and triptans (see WARNINGS).
Ergot-Containing Drugs
Ergot-containing drugs have been reported to cause prolonged vasospastic reactions. Because there is a theoretical basis that these effects may be additive, use of ergotamine-containing or ergot-type medications (like dihydroergotamine or methysergide) and sumatriptan within 24 hours of each other should be avoided (see CONTRAINDICATIONS).
Monoamine Oxidase-A Inhibitors
MAO-A inhibitors reduce sumatriptan clearance, significantly increasing systemic exposure. Therefore, the use of sumatriptan tablets in patients receiving MAO-A inhibitors is contraindicated (see CLINICALPHARMACOLOGY and CONTRAINDICATIONS).
Drug/Laboratory Test Interactions
Sumatriptan tablets are not known to interfere with commonly employed clinical laboratory tests.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis:
In carcinogenicity studies, rats and mice were given sumatriptan by oral gavage (rats: 104 weeks) or drinking water (mice: 78 weeks). Average exposures achieved in mice receiving the highest dose (target dose of 160 mg/kg/day) were approximately 40 times the exposure attained in humans after the maximum recommended single oral dose of 100 mg. The highest dose administered to rats (160 mg/kg/day, reduced from 360 mg/kg/day during week 21) was approximately 15 times the maximum recommended single human oral dose of 100 mg on a mg/m2 basis. There was no evidence of an increase in tumors in either species related to sumatriptan administration.
Mutagenesis
Sumatriptan was not mutagenic in the presence or absence of metabolic activation when tested in 2 gene mutation assays (the Ames test and the in vitro mammalian Chinese hamster V79/HGPRT assay). In 2 cytogenetics assays (the in vitro human lymphocyte assay and the in vivo rat micronucleus assay) sumatriptan was not associated with clastogenic activity.
Impairment of Fertility
In a study in which male and female rats were dosed daily with oral sumatriptan prior to and throughout the mating period, there was a treatment-related decrease in fertility secondary to a decrease in mating in animals treated with 50 and 500 mg/kg/day. The highest no-effect dose for this finding was 5 mg/kg/day, or approximately one half of the maximum recommended single human oral dose of 100 mg on a mg/m2 basis. It is not clear whether the problem is associated with treatment of the males or females or both combined. In a similar study by the subcutaneous route there was no evidence of impaired fertility at 60 mg/kg/day, the maximum dose tested, which is equivalent to approximately 6 times the maximum recommended single human oral dose of 100 mg on a mg/m2 basis.
Pregnancy
Teratogenic Effects:Pregnancy Category C. In reproductive toxicity studies in rats and rabbits, oral treatment with sumatriptan was associated with embryolethality, fetal abnormalities, and pup mortality. When administered by the intravenous route to rabbits, sumatriptan has been shown to be embryolethal. There are no adequate and well-controlled studies in pregnant women. Therefore, sumatriptan should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. In assessing this information, the following findings should be considered.
Embryolethality
When given orally or intravenously to pregnant rabbits daily throughout the period of organogenesis, sumatriptan caused embryolethality at doses at or close to those producing maternal toxicity. In the oral studies this dose was 100 mg/kg/day, and in the intravenous studies this dose was 2 mg/kg/day. The mechanism of the embryolethality is not known. The highest no-effect dose for embryolethality by the oral route was 50 mg/kg/day, which is approximately 9 times the maximum single recommended human oral dose of 100 mg on a mg/m2 basis. By the intravenous route, the highest no-effect dose was 0.75 mg/kg/day, or approximately one tenth of the maximum single recommended human oral dose of 100 mg on a mg/m2 basis.
The intravenous administration of sumatriptan to pregnant rats throughout organogenesis at 12.5 mg/kg/day, the maximum dose tested, did not cause embryolethality. This dose is equivalent to the maximum single recommended human oral dose of 100 mg on a mg/m2 basis. Additionally, in a study in rats given subcutaneous sumatriptan daily prior to and throughout pregnancy at 60 mg/kg/day, the maximum dose tested, there was no evidence of increased embryo/fetal lethality. This dose is equivalent to approximately 6 times the maximum recommended single human oral dose of 100 mg on a mg/m2 basis.
Teratogenicity
Oral treatment of pregnant rats with sumatriptan during the period of organogenesis resulted in an increased incidence of blood vessel abnormalities (cervicothoracic and umbilical) at doses of approximately 250 mg/kg/day or higher. The highest no-effect dose was approximately 60 mg/kg/day, which is approximately 6 times the maximum single recommended human oral dose of 100 mg on a mg/m2 basis. Oral treatment of pregnant rabbits with sumatriptan during the period of organogenesis resulted in an increased incidence of cervicothoracic vascular and skeletal abnormalities. The highest no-effect dose for these effects was 15 mg/kg/day, or approximately 3 times the maximum single recommended human oral dose of 100 mg on a mg/m2 basis.
A study in which rats were dosed daily with oral sumatriptan prior to and throughout gestation demonstrated embryo/fetal toxicity (decreased body weight, decreased ossification, increased incidence of rib variations) and an increased incidence of a syndrome of malformations (short tail/short body and vertebral disorganization) at 500 mg/kg/day. The highest no-effect dose was 50 mg/kg/day, or approximately 5 times the maximum single recommended human oral dose of 100 mg on a mg/m2 basis. In a study in rats dosed daily with subcutaneous sumatriptan prior to and throughout pregnancy, at a dose of 60 mg/kg/day, the maximum dose tested, there was no evidence of teratogenicity. This dose is equivalent to approximately 6 times the maximum recommended single human oral dose of 100 mg on a mg/m2 basis.
Pup Deaths
Oral treatment of pregnant rats with sumatriptan during the period of organogenesis resulted in a decrease in pup survival between birth and postnatal day 4 at doses of approximately 250 mg/kg/day or higher. The highest no-effect dose for this effect was approximately 60 mg/kg/day, or 6 times the maximum single recommended human oral dose of 100 mg on a mg/m2 basis.
Oral treatment of pregnant rats with sumatriptan from gestational day 17 through postnatal day 21 demonstrated a decrease in pup survival measured at postnatal days 2, 4, and 20 at the dose of 1,000 mg/kg/day. The highest no-effect dose for this finding was 100 mg/kg/day, approximately 10 times the maximum single recommended human oral dose of 100 mg on a mg/m2 basis. In a similar study in rats by the subcutaneous route there was no increase in pup death at 81 mg/kg/day, the highest dose tested, which is equivalent to 8 times the maximum single recommended human oral dose of 100 mg on a mg/m2 basis.
Nursing Mothers
Sumatriptan is excreted in human breast milk following subcutaneous administration. Infant exposure to sumatriptan can be minimized by avoiding breastfeeding for 12 hours after treatment with sumatriptan tablets.
Pediatric Use
Safety and effectiveness of sumatriptan tablets in pediatric patients have not been established.
Completed placebo-controlled clinical trials evaluating oral sumatriptan (25 to 100 mg) in pediatric patients aged 12 to 17 years enrolled a total of 701 adolescent migraineurs. These studies did not establish the efficacy of oral sumatriptan compared to placebo in the treatment of migraine in adolescents. Adverse events observed in these clinical trials were similar in nature to those reported in clinical trials in adults. The frequency of all adverse events in theses patients appeared to be both dose- and age-dependent, with younger patients reporting events more commonly than older adolescents. Post-marketing experience includes a limited number of reports that describe pediatric patients who have experienced adverse events, some clinically serious, after use of subcutaneous sumatriptan and/or oral sumatriptan. These reports include events similar in nature to those reported rarely in adults. A myocardial infarct has been reported in a 14-year-old male following the use of oral sumatriptan; clinical signs occurred within 1 day of drug administration. Since clinical data to determine the frequency of serious adverse events in pediatric patients who might receive injectable, oral, or intranasal sumatriptan are not presently available, the use of sumatriptan in patients aged younger than 18 years is not recommended.
Geriatric Use
The use of sumatriptan in elderly patients is not recommended because elderly patients are more likely to have decreased hepatic function, they are at higher risk for CAD, and blood pressure increases may be more pronounced in the elderly (see WARNINGS).
ADVERSE REACTIONS
Serious cardiac events, including some that have been fatal, have occurred following the use of sumatriptan succinate injection or tablets. These events are extremely rare and most have been reported in patients with risk factors predictive of CAD. Events reported have included coronary artery vasospasm, transient myocardial ischemia, myocardial infarction, ventricular tachycardia, and ventricular fibrillation (see CONTRAINDICATIONS, WARNINGS, and PRECAUTIONS).
Significant hypertensive episodes, including hypertensive crises, have been reported on rare occasions in patients with or without a history of hypertension (see WARNINGS).
Incidence in Controlled Clinical Trials
Table 2 lists adverse events that occurred in placebo-controlled clinical trials in patients who took at least 1 dose of study drug. Only events that occurred at a frequency of 2% or more in any group treated with sumatriptan tablets and were more frequent in that group than in the placebo group are included in Table 2. The events cited reflect experience gained under closely monitored conditions of clinical trials in a highly selected patient population. In actual clinical practice or in other clinical trials, these frequency estimates may not apply, as the conditions of use, reporting behavior, and the kinds of patients treated may differ.
|
Adverse Event Type |
Percent of Patients Reporting |
|||
|
Placebo (N = 309) |
Sumatriptan 25 mg (N = 417) |
Sumatriptan 50 mg (N = 771) |
Sumatriptan 100 mg (N = 437) |
|
|
Atypical sensations |
4% |
5% |
6% |
6% |
|
Paresthesia (all types) |
2% |
3% |
5% |
3% |
|
Sensation warm/cold |
2% |
3% |
2% |
3% |
|
Pain and other pressure sensations |
4% |
6% |
6% |
8% |
|
Chest - pain/tightness/pressure and/or heaviness |
1% |
1% |
2% |
2% |
|
Neck/throat/jaw - pain/ tightness/pressure |
<1% |
<1% |
2% |
3% |
|
Pain - location specified |
1% |
2% |
1% |
1% |
|
Other - pressure/tightness/ heaviness |
2% |
1% |
1% |
3% |
|
Neurological | ||||
|
Vertigo |
<1% |
<1% |
<1% |
2% |
|
Other | ||||
|
Malaise/fatigue |
<1% |
2% |
2% |
3% |
aEvents that occurred at a frequency of 2% or more in the group treated with sumatriptan tablets and that occurred more frequently in that group than the placebo group.
Other events that occurred in more than 1% of patients receiving sumatriptan tablets and at least as often on placebo included nausea and/or vomiting, migraine, headache, hyposalivation, dizziness, and drowsiness/sleepiness.
Sumatriptan tablets are generally well tolerated. Across all doses, most adverse reactions were mild and transient and did not lead to long-lasting effects. The incidence of adverse events in controlled clinical trials was not affected by gender or age of the patients. There were insufficient data to assess the impact of race on the incidence of adverse events.
Other Events Observed in Association With the Administration of Sumatriptan Tablets
In the paragraphs that follow, the frequencies of less commonly reported adverse clinical events are presented. Because the reports include events observed in open and uncontrolled studies, the role of sumatriptan tablets in their causation cannot be reliably determined. Furthermore, variability associated with adverse event reporting, the terminology used to describe adverse events, etc., limit the value of quantitative frequency estimates provided. Event frequencies are calculated as the number of patients who used sumatriptane tablets (25, 50, or 100 mg) and reported an event divided by the total number of patients (N = 6,348) exposed to sumatriptan tablets. All reported events are included except those already listed in the previous table, those too general to be informative, and those not reasonably associated with the use of the drug. Events are further classified within body system categories and enumerated in order of decreasing frequency using the following definitions: frequent adverse events are defined as those occurring in at least 1/100 patients, infrequent adverse events are those occurring in 1/100 to 1/1,000 patients, and rare adverse events are those occurring in fewer than 1/1,000 patients.
Atypical Sensations
Frequent were burning sensation and numbness. Infrequent was tight feeling in head. Rare were dysesthesia.
Cardiovascular
Frequent were palpitations, syncope, decreased blood pressure, and increased blood pressure. Infrequent were arrhythmia, changes in ECG, hypertension, hypotension, pallor, pulsating sensations, and tachycardia. Rare were angina, atherosclerosis, bradycardia, cerebral ischemia, cerebrovascular lesion, heart block, peripheral cyanosis, thrombosis, transient myocardial ischemia, and vasodilation.
Ear, Nose, and Throat
Frequent were sinusitis, tinnitus; allergic rhinitis; upper respiratory inflammation; ear, nose, and throat hemorrhage; external otitis; hearing loss; nasal inflammation; and sensitivity to noise. Infrequent were hearing disturbances and otalgia. Rare was feeling of fullness in the ear(s).
Endocrine and Metabolic
Infrequent was thirst. Rare were elevated thyrotropin stimulating hormone (TSH) levels; galactorrhea; hyperglycemia; hypoglycemia; hypothyroidism; polydipsia; weight gain; weight loss; endocrine cysts, lumps, and masses; and fluid disturbances.
Eye
Rare were disorders of sclera, mydriasis, blindness and low vision, visual disturbances, eye edema and swelling, eye irritation and itching, accommodation disorders, external ocular muscle disorders, eye hemorrhage, eye pain, and keratitis and conjunctivitis.
Gastrointestinal
Frequent were diarrhea and gastric symptoms. Infrequent were constipation, dysphagia, and gastroesophageal reflux. Rare were gastrointestinal bleeding, hematemesis, melena, peptic ulcer, gastrointestinal pain, dyspeptic symptoms, dental pain, feelings of gastrointestinal pressure, gastritis, gastroenteritis, hypersalivation, abdominal distention, oral itching and irritation, salivary gland swelling, and swallowing disorders.
Musculoskeletal
Frequent was myalgia. Infrequent was muscle cramps. Rare were tetany; muscle atrophy, weakness, and tiredness; arthralgia and articular rheumatitis; acquired musculoskeletal deformity; muscle stiffness, tightness, and rigidity; and musculoskeletal inflammation.
Neurological
Frequent were phonophobia and photophobia. Infrequent were confusion, depression, difficulty concentrating, disturbance of smell, dysarthria, euphoria, facial pain, heat sensitivity, incoordination, lacrimation, monoplegia, sleep disturbance, shivering, syncope, and tremor. Rare were aggressiveness, apathy, bradylogia, cluster headache, convulsions, decreased appetite, drug abuse, dystonic reaction, facial paralysis, hallucinations, hunger, hyperesthesia, hysteria, increased alertness, memory disturbance, neuralgia, paralysis, personality change, phobia, radiculopathy, rigidity, suicide, twitching, agitation, anxiety, depressive disorders, detachment, motor dysfunction, neurotic disorders, psychomotor disorders, taste disturbances, and raised intracranial pressure.
Respiratory
Frequent was dyspnea. Infrequent was asthma. Rare were hiccoughs, breathing disorders, cough, and bronchitis.
Skin
Frequent was sweating. Infrequent were erythema, pruritus, rash, and skin tenderness. Rare were dry/scaly skin, tightness of skin, wrinkling of skin, eczema, seborrheic dermatitis, and skin nodules.
Breasts
Infrequent was tenderness. Rare were nipple discharge; breast swelling; cysts, lumps, and masses of breasts; and primary malignant breast neoplasm.
Urogenital
Infrequent were dysmenorrhea, increased urination, and intermenstrual bleeding. Rare were abortion and hematuria, urinary frequency, bladder inflammation, micturition disorders, urethritis, urinary infections, menstruation symptoms, abnormal menstrual cycle, inflammation of fallopian tubes, and menstrual cycle symptoms.
Other Events Observed in the Clinical Development of Sumatriptan
The following adverse events occurred in clinical trials with sumatriptan succinate injection and sumatriptan succinate nasal spray. Because the reports include events observed in open and uncontrolled studies, the role of sumatriptan in their causation cannot be reliably determined. All reported events are included except those already listed, those too general to be informative, and those not reasonably associated with the use of the drug.
Cardiovascular
Abdominal aortic aneurysm, abnormal pulse, flushing, phlebitis, Raynaud syndrome, and various transient ECG changes (nonspecific ST or T wave changes, prolongation of PR or QTc intervals, sinus arrhythmia, nonsustained ventricular premature beats, isolated junctional ectopic beats, atrial ectopic beats, delayed activation of the right ventricle).
Ear, Nose, and Throat
Disorder/discomfort nasal cavity and sinuses, ear infection, Meniere disease, and throat discomfort.
Gastrointestinal
Abdominal discomfort, colitis, disturbance of liver function tests, flatulence/eructation, gallstones, intestinal obstruction, pancreatitis, and retching.
Miscellaneous
Difficulty in walking, hypersensitivity to various agents, jaw discomfort, miscellaneous laboratory abnormalities, “serotonin agonist effect,” swelling of the extremities, and swelling of the face.
Mouth and Teeth
Disorder of mouth and tongue (e.g., burning of tongue, numbness of tongue, dry mouth).
Musculoskeletal
Arthritis, backache, intervertebral disc disorder, neck pain/stiffness, need to flex calf muscles, and various joint disturbances (pain, stiffness, swelling, ache).
Neurological
Bad/unusual taste, chills, diplegia, disturbance of emotions, sedation, globus hystericus, intoxication, myoclonia, neoplasm of pituitary, relaxation, sensation of lightness, simultaneous hot and cold sensations, stinging sensations, stress, tickling sensations, transient hemiplegia, and yawning.
Postmarketing Experience (Reports for Subcutaneous or Oral Sumatriptan)
The following section enumerates potentially important adverse events that have occurred in clinical practice and that have been reported spontaneously to various surveillance systems. The events enumerated represent reports arising from both domestic and nondomestic use of oral or subcutaneous dosage forms of sumatriptan. The events enumerated include all except those already listed in the ADVERSE REACTIONS section above or those too general to be informative. Because the reports cite events reported spontaneously from worldwide postmarketing experience, frequency of events and the role of sumatriptan in their causation cannot be reliably determined. It is assumed, however, that systemic reactions following sumatriptan use are likely to be similar regardless of route of administration.
Cardiovascular
Atrial fibrillation, cardiomyopathy, colonic ischemia (see WARNINGS), Prinzmetal variant angina, pulmonary embolism, shock, thrombophlebitis.
Neurological
Central nervous system vasculitis, cerebrovascular accident, dysphasia, serotonin syndrome, subarachnoid hemorrhage.
Skin
Exacerbation of sunburn, hypersensitivity reactions (allergic vasculitis, erythema, pruritus, rash, shortness of breath, urticaria; in addition, severe anaphylaxis/anaphylactoid reactions have been reported [see WARNINGS]), photosensitivity.
DRUG ABUSE AND DEPENDENCE
One clinical study with sumatriptan succinate injection enrolling 12 patients with a history of substance abuse failed to induce subjective behavior and/or physiologic response ordinarily associated with drugs that have an established potential for abuse.
OVERDOSAGE
Patients (N = 670) have received single oral doses of 140 to 300 mg without significant adverse effects. Volunteers (N = 174) have received single oral doses of 140 to 400 mg without serious adverse events.
Overdose in animals has been fatal and has been heralded by convulsions, tremor, paralysis, inactivity, ptosis, erythema of the extremities, abnormal respiration, cyanosis, ataxia, mydriasis, salivation, and lacrimation. The elimination half-life of sumatriptan is approximately 2.5 hours (see CLINICALPHARMACOLOGY), and therefore monitoring of patients after overdose with sumatriptan tablets should continue for at least 12 hours or while symptoms or signs persist.
It is unknown what effect hemodialysis or peritoneal dialysis has on the serum concentrations of sumatriptan.
DOSAGE AND ADMINISTRATION
In controlled clinical trials, single doses of 25, 50, or 100 mg of sumatriptan tablets were effective for the acute treatment of migraine in adults. There is evidence that doses of 50 and 100 mg may provide a greater effect than 25 mg (see CLINICALTRIALS). There is also evidence that doses of 100 mg do not provide a greater effect than 50 mg. Individuals may vary in response to doses of sumatriptan tablets. The choice of dose should therefore be made on an individual basis, weighing the possible benefit of a higher dose with the potential for a greater risk of adverse events.
If the headache returns or the patient has a partial response to the initial dose, the dose may be repeated after 2 hours, not to exceed a total daily dose of 200 mg. If a headache returns following an initial treatment with sumatriptan succinate injection, additional single sumatriptan tablets (up to 100 mg/day) may be given with an interval of at least 2 hours between tablet doses. The safety of treating an average of more than 4 headaches in a 30-day period has not been established.
Because of the potential of MAO-A inhibitors to cause unpredictable elevations in the bioavailability of oral sumatriptan, their combined use is contraindicated (see CONTRAINDICATIONS).
Hepatic disease/functional impairment may also cause unpredictable elevations in the bioavailability of orally administered sumatriptan. Consequently, if treatment is deemed advisable in the presence of liver disease, the maximum single dose should in general not exceed 50 mg (see CLINICALPHARMACOLOGYfor the basis of this recommendation).
HOW SUPPLIED
Sumatriptan tablets USP, 50 mg of sumatriptan (base) as the succinate.
Sumatriptan tablets USP, 50 mg are white, round, biconvex film-coated tablets debossed with “RDY” on one side and “292” on the other side. The tablets are supplied in bottles of 30, 36, 90 100, 500, unit of use blister pack of 9's and unit dose package of 100's.
Bottles of 9 NDC 63187-049-09
Store at 20to 25°C (68 – 77°F) [See USP Controlled Room Temperature].
Dispense in a tight, light-resistant container as defined in the USP, with a child-resistant closure (as required).
ANIMAL TOXICOLOGY
Corneal Opacities
Dogs receiving oral sumatriptan developed corneal opacities and defects in the corneal epithelium. Corneal opacities were seen at the lowest dosage tested, 2 mg/kg/day, and were present after 1 month of treatment. Defects in the corneal epithelium were noted in a 60-week study. Earlier examinations for these toxicities were not conducted and no-effect doses were not established; however, the relative exposure at the lowest dose tested was approximately 5 times the human exposure after a 100 mg oral dose. There is evidence of alterations in corneal appearance on the first day of intranasal dosing to dogs. Changes were noted at the lowest dose tested, which was approximately one half the maximum single human oral dose of 100 mg on a mg/m2 basis.
RX Only
Manufactured by:
Dr. Reddy’s Laboratories Limited
Bachepalli – 502 325 INDIA
Revised: 0312
Relabeled by:
Proficient Rx LP
Thousand Oaks, CA 91320
PATIENT PACKAGE INSERT
Patient Information
Sumatriptan Tablets USP
Read this Patient Information before you start taking sumatriptan tablets and each time you get a refill. There may be new information. This information does not take the place of talking with your healthcare provider about your medical condition or treatment.
What is the most important information I should know about sumatriptan tablets?
Sumatriptan tablets can cause serious side effects, including: Heart attack and other heart problems. Heart problems may lead to death.
Stop taking sumatriptan tablets and get emergency medical help right away if you have any of the following symptoms of a heart attack:
- •
- discomfort in the center of your chest that lasts for more than a few minutes, or that goes away and comes back
- •
- chest pain or chest discomfort that feels like uncomfortable heavy pressure, squeezing, or fullness, or pain
- •
- pain or discomfort in your arms, back, neck, jaw, or stomach
- •
- shortness of breath with or without chest discomfort
- •
- breaking out in a cold sweat
- •
- nausea or vomiting
- •
- feeling lightheaded
Sumatriptan tablets are not for people with risk factors for heart disease unless a heart exam is done and shows no problem. You have a higher risk for heart disease if you:
- •
- have high blood pressure
- •
- have high cholesterol levels
- •
- smoke
- •
- are overweight
- •
- have diabetes
- •
- have a family history of heart disease
- •
- are a female who has gone through menopause
- •
- are a male over age 40
Serotonin syndrome. Serotonin syndrome is a serious and life-threatening problem that can happen in people taking sumatriptan tablets, especially if sumatriptan tablets are used with antidepressant medicines called selective serotonin reuptake inhibitors (SSRIs) or selective norepinephrine reuptake inhibitors (SNRIs).
Ask your healthcare provider or pharmacist for a list of these medicines if you are not sure.
Call your healthcare provider right away if you have any of the following symptoms of serotonin syndrome:
- •
- mental changes such as seeing things that are not there (hallucinations), agitation, or coma
- •
- fast heartbeat
- •
- changes in blood pressure
- •
- high body temperature
- •
- tight muscles
- •
- trouble walking
- •
- nausea, vomiting, or diarrhea
What are sumatriptan tablets?
Sumatriptan tablets are a prescription medicine used to treat acute migraine headaches with or without aura in adults.
Sumatriptan tablets are not used to prevent or decrease the number of migraine headaches you have.
Sumatriptan tablets are not used to treat other types of headaches such as hemiplegic (that make you unable to move on one side of your body) or basilar migraines (rare form of migraine with aura).
It is not known if sumatriptan tablets are safe and effective to treat cluster headaches.
It is not known if sumatriptan tablets are safe and effective in children under 18 years of age.
Who should not take sumatriptan tablets?
Do not take sumatriptan tablets if you have:
- •
- heart problems or a history of heart problems
- •
- narrowing of blood vessels to your legs, arms, stomach, or kidney (peripheral vascular disease)
- •
- uncontrolled high blood pressure
- •
- severe liver problems
- •
- hemiplegic migraines or basilar migraines. If you are not sure if you have these types of migraines, ask your healthcare provider.
- •
- had a stroke, transient ischemic attacks (TIAs), or problems with your blood circulation
- •
- taken any of the following medicines in the last 24 hours:
- •
- almotriptan (AXERT®)
- •
- eletriptan (RELPAX®)
- •
- frovatriptan (FROVA®)
- •
- naratriptan (AMERGE®)
- •
- rizatriptan (MAXALT®, MAXALT-MLT®)
- •
- sumatriptan and naproxen (TREXIMET®)
- •
- ergotamines (CAFERGOT®, ERGOMAR®, MIGERGOT®)
- •
- dihydroergotamine (D.H.E. 45®, MIGRANAL®)
Ask your doctor if you are not sure if your medicine is listed above.
- •
- an allergy to sumatriptan or any of the ingredients in sumatriptan tablets. See the end of this leaflet for a complete list of ingredients in sumatriptan tablets.
What should I tell my healthcare provider before taking sumatriptan tablets?
Before you take sumatriptan tablets, tell your healthcare provider about all of your medical conditions, including if you:
- •
- have high blood pressure
- •
- have high cholesterol
- •
- have diabetes
- •
- smoke
- •
- are overweight
- •
- are a female who has gone through menopause
- •
- have heart disease or a family history of heart disease or stroke
- •
- have kidney problems
- •
- have liver problems
- •
- have had epilepsy or seizures
- •
- are not using effective birth control
- •
- are pregnant or plan to become pregnant. It is not known if sumatriptan tablets will harm your unborn baby.
- •
- are breastfeeding or plan to breastfeed. Sumatriptan tablets passes into your breast milk and may harm your baby. Talk with your healthcare provider about the best way to feed your baby if you take sumatriptan tablets.
Tell your healthcare provider about all the medicines you take, including prescription and nonprescription medicines, vitamins, and herbal supplements.
Sumatriptan tablets and other medicines may affect each other, causing side effects.
Especially tell your healthcare provider if you take anti-depressant medicines called:
- •
- selective serotonin reuptake inhibitors (SSRIs)
- •
- serotonin norepinephrine reuptake inhibitors (SNRIs)
- •
- monoamine oxidase inhibitors (MAOIs)
Ask your healthcare provider or pharmacist for a list of these medicines if you are not sure.
Know the medicines you take. Keep a list of them to show your healthcare provider or pharmacist when you get a new medicine.
How should I take sumatriptan tablets?
- •
- Certain people should take their first dose of sumatriptan tablets in their healthcare provider’s office or in another medical setting. Ask your healthcare provider if you should take your first dose in a medical setting.
- •
- Take sumatriptan tablets exactly as your healthcare provider tells you to take it.
- •
- Your healthcare provider may change your dose. Do not change your dose without first talking to your healthcare provider.
- •
- Take sumatriptan tablets with water or other liquids.
- •
- If you do not get any relief after your first sumatriptan tablet, do not take a second tablet without first talking with your healthcare provider.
- •
- If your headache comes back or you only get some relief from your headache, you can take a second tablet 2 hours after the first tablet
- •
- Do not take more than a total of 200 mg of sumatriptan tablets in a 24-hour period.
- •
- Some people who take too many sumatriptan tablets may have worse headaches (medication overuse headache). If your headaches get worse, your healthcare provider may decide to stop your treatment with sumatriptan tablets.
- •
- If you take too much sumatriptan tablets, call your healthcare provider or go to the nearest hospital emergency room right away.
- •
- You should write down when you have headaches and when you take sumatriptan tablets so you can talk with your healthcare provider about how sumatriptan tablets are working for you.
What should I avoid while taking sumatriptan tablets?
Sumatriptan tablets can cause dizziness, weakness, or drowsiness. If you have these symptoms, do not drive a car, use machinery, or do anything where you need to be alert.
What are the possible side effects of sumatriptan tablets? Sumatriptan tablets may cause serious side effects. See “What is the most important information I should know about sumatriptan tablets?”
These serious side effects include:
- •
- changes in color or sensation in your fingers and toes (Raynaud’s syndrome)
- •
- stomach and intestinal problems (gastrointestinal and colonic ischemic events). Symptoms of gastrointestinal and colonic ischemic events include:
- •
- sudden or severe stomach pain
- •
- stomach pain after meals
- •
- weight loss
- •
- nausea or vomiting
- •
- constipation or diarrhea
- •
- bloody diarrhea
- •
- fever
- •
- problems with blood circulation to your legs and feet (peripheral vascular ischemia). Symptoms of peripheral vascular ischemia include:
- •
- cramping and pain in your legs or hips
- •
- feeling of heaviness or tightness in your leg muscles
- •
- burning or aching pain in your feet or toes while resting
- •
- numbness, tingling, or weakness in your legs
- •
- cold feeling or color changes in 1 or both legs or feet
- •
- shortness of breath or wheezing
- •
- hives (itchy bumps); swelling of your tongue, mouth, or throat
The most common side effects of sumatriptan tablets include:
- •
- tingling or numbness in your fingers or toes
- •
- dizziness
- •
- warm, hot, burning feeling to your face (flushing)
- •
- feeling weak, drowsy, or tired
Tell your healthcare provider if you have any side effect that bothers you or that does not go away.
These are not all the possible side effects of sumatriptan tablets. For more information, ask your healthcare provider or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store Sumatriptan Tablets?
Store at 20to 25°C (68 – 77°F) [See USP Controlled Room Temperature].
Dispense in a tight, light-resistant container as defined in the USP, with a child-resistant closure (as required).
Keep sumatriptan tablets and all medicines out of the reach of children.
General information about the safe and effective use of sumatriptan tablets.
Medicines are sometimes prescribed for purposes other than those listed in Patient Information leaflets. Do not use sumatriptan tablets for a condition for which it was not prescribed. Do not give sumatriptan tablets to other people, even if they have the same symptoms you have. It may harm them.
This Patient Information leaflet summarizes the most important information about sumatriptan tablets. If you would like more information, talk with your healthcare provider. You can ask your healthcare provider or pharmacist for information about sumatriptan tablets that is written for healthcare professionals.
For more information, call 1-888-375-3784.
What are the ingredients in Sumatriptan Tablets?
Active ingredients: Sumatriptan succinate
Inactive ingredients: croscarmellose sodium, lactose anhydrous, lactose monohydrate, magnesium stearate, mannitol, microcrystalline cellulose, talc, titanium dioxide and triacetin.
To reorder additional Patient Information Leaflets, please contact Dr. Reddy’s Customer Service at 1-866-733-3952.
IMITREX, AMERGE, and TREXIMET are registered trademarks of GlaxoSmithKline. The other brands listed are trademarks of their respective owners.
This Patient Information has been approved by the U.S. Food and Drug Administration.
RX Only
Manufactured by:
Dr. Reddy’s Laboratories Limited
Bachepalli – 502 325 INDIA
Revised : 0312
Repackaged by:
Proficient Rx LP
Thousand Oaks, CA 91320