DESCRIPTION
Clomiphene Citrate Tablets, USP is an orally administered, nonsteroidal, ovulatory stimulant designated chemically as 2-[p-(2-chloro-1,2-diphenylvinyl)phenoxy] triethylamine citrate (1:1). It has the molecular formula of C26H28CINO • C6H8O7 and a molecular weight of 598.10. It is represented structurally as:
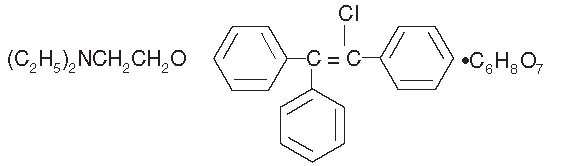
Clomiphene citrate is a white to pale yellow, essentially odorless, crystalline powder. It is freely soluble in methanol; soluble in ethanol; slightly soluble in acetone, water, and chloroform; and insoluble in ether.
Clomiphene citrate is a mixture of two geometric isomers [cis (zuclomiphene) and trans (enclomiphene)] containing between 30% and 50% of the cis-isomer.
Each off-white debossed tablet contains 50 mg clomiphene citrate USP. The tablet also contains the following inactive ingredients: corn starch, lactose monohydrate, magnesium stearate, pregelatinized corn starch, and sucrose.
CLINICAL PHARMACOLOGY
Action
Clomiphene citrate is a drug of considerable pharmacologic potency. With careful selection and proper management of the patient, clomiphene citrate has been demonstrated to be a useful therapy for the anovulatory patient desiring pregnancy.
Clomiphene citrate is capable of interacting with estrogen-receptor-containing tissues, including the hypothalamus, pituitary, ovary, endometrium, vagina, and cervix. It may compete with estrogen for estrogen-receptor-binding sites and may delay replenishment of intracellular estrogen receptors. Clomiphene citrate initiates a series of endocrine events culminating in a preovulatory gonadotropin surge and subsequent follicular rupture. The first endocrine event in response to a course of clomiphene therapy is an increase in the release of pituitary gonadotropins. This initiates steroidogenesis and folliculogenesis, resulting in growth of the ovarian follicle and an increase in the circulating level of estradiol. Following ovulation, plasma progesterone and estradiol rise and fall as they would in a normal ovulatory cycle.
Available data suggest that both the estrogenic and antiestrogenic properties of clomiphene may participate in the initiation of ovulation. The two clomiphene isomers have been found to have mixed estrogenic and antiestrogenic effects, which may vary from one species to another. Some data suggest that zuclomiphene has greater estrogenic activity than enclomiphene.
Clomiphene citrate has no apparent progestational, androgenic, or antiandrogenic effects and does not appear to interfere with pituitary-adrenal or pituitary-thyroid function.
Although there is no evidence of a “carryover effect” of clomiphene citrate, spontaneous ovulatory menses have been noted in some patients after clomiphene citrate therapy.
Pharmacokinetics
Based on early studies with 14C-labeled clomiphene citrate, the drug was shown to be readily absorbed orally in humans and excreted principally in the feces. Cumulative urinary and fecal excretion of the 14C averaged about 50% of the oral dose and 37% of an intravenous dose after 5 days. Mean urinary excretion was approximately 8% with fecal excretion of about 42%.
Some 14C label was still present in the feces 6 weeks after administration. Subsequent single-dose studies in normal volunteers showed that zuclomiphene (cis) has a longer half-life than enclomiphene (trans). Detectable levels of zuclomiphene persisted for longer than a month in these subjects. This may be suggestive of stereo-specific enterohepatic recycling or sequestering of the zuclomiphene. Thus, it is possible that some active drug may remain in the body during early pregnancy in women who conceive in the menstrual cycle during clomiphene citrate therapy.
CLINICAL STUDIES
During clinical investigations, 7578 patients received clomiphene citrate, some of whom had impediments to ovulation other than ovulatory dysfunction (see INDICATIONS AND USAGE). In those clinical trials, successful therapy characterized by pregnancy occurred in approximately 30% of these patients.
There were a total of 2635 pregnancies reported during the clinical trial period. Of those pregnancies, information on outcome was only available for 2369 of the cases. Table 1 summarizes the outcome of these cases.
Of the reported pregnancies, the incidence of multiple pregnancies was 7.98%: 6.9% twin, 0.5% triplet, 0.3% quadruplet, 0.1% quintuplet. Of the 165 twin pregnancies for which sufficient information was available, the ratio of monozygotic to dizygotic twins was about 1:5. Table 1 reports the survival rate of the live multiple births.
A sextuplet birth was reported after completion of original clinical studies; none of the sextuplets survived (each weighed less than 400 g), although each appeared grossly normal.
| * Includes 28 ectopic pregnancies, 4 hydatiform moles, and 1 fetus papyraceous. | ||
| † Indicates percentage of surviving infants from these pregnancies. | ||
|
Outcome |
Total Number of Pregnancies |
Survival Rate |
|
Pregnancy Wastage | ||
|
Spontaneous Abortions |
483* | |
|
Stillbirths |
24 | |
|
Live Births | ||
|
Single Births |
1697 |
98.16%† |
|
Multiple Births |
165 |
83.26%† |
The overall survival of infants from multiple pregnancies including spontaneous abortions, stillbirths, and neonatal deaths is 73%.
Fetal/Neonatal Anomalies and Mortality The following fetal abnormalities have been reported subsequent to pregnancies following ovulation induction therapy with clomiphene citrate during clinical trials. Each of the following fetal abnormalities were reported at a rate of <1% (experiences are listed in order of decreasing frequency): Congenital heart lesions, Down syndrome, club foot, congenital gut lesions, hypospadias, microcephaly, harelip, and cleft palate, congenital hip, hemangioma, undescended testicles, polydactyly, conjoined twins and teratomatous malformation, patent ductus arteriosus, amaurosis, arteriovenous fistula, inguinal hernia, umbilical hernia, syndactyly, pectus excavatum, myopathy, dermoid cyst of scalp, omphalocele, spina bifida occulta, ichthyosis, and persistent lingual frenulum. Neonatal death and fetal death/stillbirth in infants with birth defects have also been reported at a rate of <1%. The overall incidence of reported congenital anomalies from pregnancies associated with maternal clomiphene citrate ingestion during clinical studies was within the range of that reported for the general population.
In addition, reports of congenital anomalies have been received during postmarketing surveillance of clomiphene citrate (see ADVERSE REACTIONS).
INDICATIONS AND USAGE
Clomiphene citrate is indicated for the treatment of ovulatory dysfunction in women desiring pregnancy. Impediments to achieving pregnancy must be excluded or adequately treated before beginning clomiphene citrate therapy. Those patients most likely to achieve success with clomiphene therapy include patients with polycystic ovary syndrome (see WARNINGS: Ovarian Hyperstimulation Syndrome), amenorrhea-galactorrhea syndrome, psychogenic amenorrhea, post-oral-contraceptive amenorrhea, and certain cases of secondary amenorrhea of undetermined etiology.
Properly timed coitus in relationship to ovulation is important. A basal body temperature graph or other appropriate tests may help the patient and her physician determine if ovulation occurred. Once ovulation has been established, each course of clomiphene citrate should be started on or about the 5th day of the cycle. Long-term cyclic therapy is not recommended beyond a total of about six cycles (including three ovulatory cycles). (See DOSAGE AND ADMINISTRATION and PRECAUTIONS.)
Clomiphene citrate is indicated only in patients with demonstrated ovulatory dysfunction who meet the conditions described below:
1. Patients who are not pregnant.
2. Patients without ovarian cysts. Clomiphene citrate should not be used in patients with ovarian enlargement except those with polycystic ovary syndrome. Pelvic examination is necessary prior to the first and each subsequent course of clomiphene citrate treatment.
3. Patients without abnormal vaginal bleeding. If abnormal vaginal bleeding is present, the patient should be carefully evaluated to ensure that neoplastic lesions are not present.
4. Patients with normal liver function.
In addition, patients selected for clomiphene citrate therapy should be evaluated in regard to the following:
1. Estrogen Levels. Patients should have adequate levels of endogenous estrogen (as estimated from vaginal smears, endometrial biopsy, assay of urinary estrogen, or from bleeding in response to progesterone). Reduced estrogen levels, while less favorable, do not preclude successful therapy.
2. Primary Pituitary or Ovarian Failure. Clomiphene citrate therapy cannot be expected to substitute for specific treatment of other causes of ovulatory failure.
3. Endometriosis and Endometrial Carcinoma. The incidence of endometriosis and endometrial carcinoma increases with age as does the incidence of ovulatory disorders. Endometrial biopsy should always be performed prior to clomiphene citrate therapy in this population.
4. Other Impediments to Pregnancy. Impediments to pregnancy can include thyroid disorders, adrenal disorders, hyperprolactinemia, and male factor infertility.
5. Uterine Fibroids. Caution should be exercised when using clomiphene citrate in patients with uterine fibroids due to the potential for further enlargement of the fibroids.
There are no adequate or well-controlled studies that demonstrate the effectiveness of clomiphene citrate in the treatment of male infertility. In addition, testicular tumors and gynecomastia have been reported in males using clomiphene. The cause and effect relationship between reports of testicular tumors and the administration of clomiphene citrate is not known.
Although the medical literature suggests various methods, there is no universally accepted standard regimen for combined therapy (i.e., clomiphene citrate in conjunction with other ovulation-inducing drugs). Similarly, there is no standard clomiphene citrate regimen for ovulation induction in vitro fertilization programs to produce ova for fertilization and reintroduction. Therefore, clomiphene citrate is not recommended for these uses.
CONTRAINDICATIONS
Hypersensitivity
Clomiphene citrate is contraindicated in patients with a known hypersensitivity or allergy to clomiphene citrate or to any of its ingredients.
Pregnancy
Clomiphene citrate use in pregnant women is contraindicated, as clomiphene citrate does not offer benefit in this population.
Available human data do not suggest an increased risk for congenital anomalies above the background population risk when used as indicated. However, animal reproductive toxicology studies showed increased embryo-fetal loss and structural malformations in offspring. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential risks to the fetus. (See PRECAUTIONS: Pregnancy).
Liver Disease. Clomiphene citrate therapy is contraindicated in patients with liver disease or a history of liver dysfunction (see also INDICATIONS AND USAGE and ADVERSE REACTIONS).
Abnormal Uterine Bleeding. Clomiphene citrate is contraindicated in patients with abnormal uterine bleeding of undetermined origin (see INDICATIONS AND USAGE).
Ovarian Cysts. Clomiphene citrate is contraindicated in patients with ovarian cysts or enlargement not due to polycystic ovarian syndrome (see INDICATIONS AND USAGE and WARNINGS).
Other. Clomiphene citrate is contraindicated in patients with uncontrolled thyroid or adrenal dysfunction or in the presence of an organic intracranial lesion such as pituitary tumor (see INDICATIONS AND USAGE).
WARNINGS
Visual Symptoms
Patients should be advised that blurring or other visual symptoms such as spots or flashes (scintillating scotomata) may occasionally occur during therapy with clomiphene citrate. These visual symptoms increase in incidence with increasing total dose or therapy duration. These visual disturbances are usually reversible; however, cases of prolonged visual disturbance have been reported with some occurring after clomiphene citrate discontinuation. The visual disturbances may be irreversible, especially with increased dosage or duration of therapy. Patients should be warned that these visual symptoms may render such activities as driving a car or operating machinery more hazardous than usual, particularly under conditions of variable lighting.
These visual symptoms appear to be due to intensification and prolongation of after-images. Symptoms often first appear or are accentuated with exposure to a brightly lit environment. While measured visual acuity usually has not been affected, a study patient taking 200 mg clomiphene citrate daily developed visual blurring on the 7th day of treatment, which progressed to severe diminution of visual acuity by the 10th day. No other abnormality was found, and the visual acuity returned to normal on the 3rd day after treatment was stopped.
Ophthalmologically definable scotomata and retinal cell function (electroretinographic) changes have also been reported. A patient treated during clinical studies developed phosphenes and scotomata during prolonged clomiphene citrate administration, which disappeared by the 32nd day after stopping therapy.
Postmarketing surveillance of adverse events has also revealed other visual signs and symptoms during clomiphene citrate therapy (see ADVERSE REACTIONS).
While the etiology of these visual symptoms is not yet understood, patients with any visual symptoms should discontinue treatment and have a complete ophthalmological evaluation carried out promptly.
OvarianHyperstimulationSyndrome
The ovarian hyperstimulation syndrome (OHSS) has been reported to occur in patients receiving clomiphene citrate therapy for ovulation induction. OHSS may progress rapidly (within 24 hours to several days) and become a serious medical disorder. In some cases, OHSS occurred following cyclic use of clomiphene citrate therapy or when clomiphene citrate was used in combination with gonadotropins. Transient liver function test abnormalities suggestive of hepatic dysfunction, which may be accompanied by morphologic changes on liver biopsy, have been reported in association with OHSS.
OHSS is a medical event distinct from uncomplicated ovarian enlargement. The clinical signs of this syndrome in severe cases can include gross ovarian enlargement, gastrointestinal symptoms, ascites, dyspnea, oliguria, and pleural effusion. In addition, the following symptoms have been reported in association with this syndrome: pericardial effusion, anasarca, hydrothorax, acute abdomen, hypotension, renal failure, pulmonary edema, intraperitoneal and ovarian hemorrhage, deep venous thrombosis, torsion of the ovary, and acute respiratory distress. The early warning signs of OHSS are abdominal pain and distention, nausea, vomiting, diarrhea, and weight gain. Elevated urinary steroid levels, varying degrees of electrolyte imbalance, hypovolemia, hemoconcentration, and hypoproteinemia may occur. Death due to hypovolemic shock, hemoconcentration, or thromboembolism has occurred. Due to fragility of enlarged ovaries in severe cases, abdominal and pelvic examination should be performed very cautiously. If conception results, rapid progression to the severe form of the syndrome may occur.
To minimize the hazard associated with occasional abnormal ovarian enlargement associated with clomiphene citrate therapy, the lowest dose consistent with expected clinical results should be used. Maximal enlargement of the ovary, whether physiologic or abnormal, may not occur until several days after discontinuation of the recommended dose of clomiphene citrate. Some patients with polycystic ovary syndrome who are unusually sensitive to gonadotropin may have an exaggerated response to usual doses of clomiphene citrate. Therefore, patients with polycystic ovary syndrome should be started on the lowest recommended dose and shortest treatment duration for the first course of therapy (see DOSAGE AND ADMINISTRATION).
If enlargement of the ovary occurs, additional clomiphene citrate therapy should not be given until the ovaries have returned to pretreatment size, and the dosage or duration of the next course should be reduced. Ovarian enlargement and cyst formation associated with clomiphene citrate therapy usually regress spontaneously within a few days or weeks after discontinuing treatment. The potential benefit of subsequent clomiphene citrate therapy in these cases should exceed the risk. Unless surgical indication for laparotomy exists, such cystic enlargement should always be managed conservatively.
A causal relationship between ovarian hyperstimulation and ovarian cancer has not been determined. However, because a correlation between ovarian cancer and nulliparity, infertility, and age has been suggested, if ovarian cysts do not regress spontaneously, a thorough evaluation should be performed to rule out the presence of ovarian neoplasia.
PRECAUTIONS
General
Careful attention should be given to the selection of candidates for clomiphene citrate therapy. Pelvic examination is necessary prior to clomiphene citrate treatment and before each subsequent course (see CONTRAINDICATIONS and WARNINGS).
Information for Patients
The purpose and risks of clomiphene citrate therapy should be presented to the patient before starting treatment. It should be emphasized that the goal of clomiphene citrate therapy is ovulation for subsequent pregnancy. The physician should counsel the patient with special regard to the following potential risks:
Visual Symptoms: Advise that blurring or other visual symptoms occasionally may occur during or shortly after clomiphene citrate therapy. It should be made clear to the patient that, in some instances, visual disturbances may be prolonged, and possibly irreversible, especially with increased dosage or duration of therapy. Warn that visual symptoms may render such activities as driving a car or operating machinery more hazardous than usual, particularly under conditions of variable lighting (see WARNINGS).
The patient should be instructed to inform the physician whenever any unusual visual symptoms occur. If the patient has any visual symptoms, treatment should be discontinued and complete ophthalmologic evaluation performed.
Abdominal/Pelvic Pain or Distention: Ovarian enlargement may occur during or shortly after therapy with clomiphene citrate. To minimize the risks associated with ovarian enlargement, the patient should be instructed to inform the physician of any abdominal or pelvic pain, weight gain, discomfort, or distention after taking clomiphene citrate (see WARNINGS).
Metabolism Disorders: Cases of hypertriglyceridemia have been reported. Preexisting or family history of hyperlipidemia and use of higher than recommended dose and/or longer duration of treatment with clomiphene citrate are associated with a risk of hypertriglyceridemia. Periodic monitoring of plasma triglycerides is recommended in patients with preexisting or family history of hyperlipidemia (see ADVERSE REACTIONS). Pretreatment screening of triglyceride levels is recommended in patients initiating clomiphene citrate therapy.
Gastrointestinal Disorders: Cases of pancreatitis have been reported.
Multiple Pregnancy: Inform the patient that there is an increased chance of multiple pregnancy, including bilateral tubal pregnancy and coexisting tubal and intrauterine pregnancy, when conception occurs in relation to clomiphene citrate therapy. The potential complications and hazards of multiple pregnancy should be explained.
Spontaneous Abortion and Congenital Anomalies: Inform the patient that the available data suggest no increase in the rates of spontaneous abortion (miscarriage) or congenital anomalies with maternal clomiphene citrate use compared to rates in the general population.
During clinical investigation, the experience from patients with known pregnancy outcome (Table 1) shows a spontaneous abortion rate of 20.4% and stillbirth rate of 1.0%. (See CLINICAL STUDIES). Among the birth anomalies spontaneously reported as individual cases since commercial availability of clomiphene citrate, the proportion of neural tube defects has been high among pregnancies associated with ovulation induced by clomiphene citrate, but this has not been supported by data from population-based studies.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term toxicity studies in animals have not been performed to evaluate the carcinogenic or mutagenic potential of clomiphene citrate.
Oral administration of clomiphene citrate to male rats at doses of 0.3 or 1 mg/kg/day caused decreased fertility, while higher doses caused temporary infertility. Oral doses of 0.1 mg/kg/day in female rats temporarily interrupted the normal cyclic vaginal smear pattern and prevented conception. Doses of 0.3 mg/kg/day slightly reduced the number of ovulated ova and corpora lutea, while 3 mg/kg/day inhibited ovulation.
Pregnancy
Fetal Risk Summary
Clomiphene citrate use in pregnant women is contraindicated, as clomiphene citrate treatment does not offer benefit in this population.
Available human data do not suggest an increased risk for congenital anomalies above the background population risk. However, animal reproductive toxicology studies showed increased embryo-fetal loss and structural malformations in offspring. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential risks to the fetus.
Clinical Considerations
To avoid inadvertent clomiphene citrate administration during early pregnancy, appropriate tests should be utilized during each treatment cycle to determine whether ovulation and/or pregnancy occurs. Patients should be evaluated carefully to exclude ovarian enlargement or ovarian cyst formation between each treatment cycle. The next course of clomiphene citrate therapy should be delayed until these conditions have been excluded.
Human Data
The available human data from epidemiologic studies do not show any apparent cause and effect relationship between clomiphene citrate periconceptual exposure and an increased risk of overall birth defects, or any specific anomaly. However, due to the small number of cases of congenital anomalies occurring in clomiphene citrate treated women, these epidemiologic studies were only able to rule out large differences in risk. The studies did not consider factors associated with female subfertility and were unable to adjust for other important confounders.
In addition, available data do not support an increase rate of spontaneous abortion among subfertile women treated with clomiphene for ovulation induction.
Animal Data
Oral administration of clomiphene citrate to pregnant rats during organogenesis at doses of 1 to 2 mg/kg/day resulted in hydramnion and weak, edematous fetuses with wavy ribs and other temporary bone changes. Doses of 8 mg/kg/day or more also caused increased resorptions and dead fetuses, dystocia, and delayed parturition, and 40 mg/kg/day resulted in increased maternal mortality. Single doses of 50 mg/kg caused fetal cataracts, while 200 mg/kg caused cleft palate.
Following injection of clomiphene citrate 2 mg/kg to mice and rats during pregnancy, the offspring exhibited metaplastic changes of the reproductive tract. Newborn mice and rats injected during the first few days of life also developed metaplastic changes in uterine and vaginal mucosa, as well as premature vaginal opening and anovulatory ovaries. These findings are similar to the abnormal reproductive behavior and sterility described with other estrogens and antiestrogens.
In rabbits, some temporary bone alterations were seen in fetuses from dams given oral doses of 20 or 40 mg/kg/day during pregnancy, but not following 8 mg/kg/day. No permanent malformations were observed in those studies. Also, rhesus monkeys given oral doses of 1.5 to 4.5 mg/kg/day for various periods during pregnancy did not have any abnormal offspring.
Nursing Mothers
It is not known whether clomiphene citrate is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised if clomiphene citrate is administered to a nursing woman. In some patients, clomiphene citrate may reduce lactation.
Ovarian Cancer
Prolonged use of clomiphene citrate tablets USP may increase the risk of a borderline or invasive ovarian tumor (see ADVERSE REACTIONS).
ADVERSE REACTIONS
Clinical Trial Adverse Events. Clomiphene citrate, at recommended dosages, is generally well tolerated. Adverse reactions usually have been mild and transient and most have disappeared promptly after treatment has been discontinued. Adverse experiences reported in patients treated with clomiphene citrate during clinical studies are shown in Table 2.
| *Includes 498 patients whose reports may have been duplicated in the event totals and could not be distinguished as such. Also, excludes 47 patients who did not report symptom data. | |
|
Adverse Event |
% |
|
Ovarian Enlargement |
13.6 |
|
Vasomotor Flushes |
10.4 |
|
Abdominal-Pelvic Discomfort/Distention/Bloating |
5.5 |
|
Nausea and Vomiting |
2.2 |
|
Breast Discomfort |
2.1 |
|
Visual Symptoms |
1.5 |
|
Blurred vision, lights, floaters, waves, unspecified visual | |
|
complaints, photophobia, diplopia, scotomata, phosphenes | |
|
Headache |
1.3 |
|
Abnormal Uterine Bleeding |
1.3 |
|
Intermenstrual spotting, menorrhagia | |
The following adverse events have been reported in fewer than 1% of patients in clinical trials: Acute abdomen, appetite increase, constipation, dermatitis or rash, depression, diarrhea, dizziness, fatigue, hair loss/dry hair, increased urinary frequency/volume, insomnia, light-headedness, nervous tension, vaginal dryness, vertigo, weight gain/loss.
Patients on prolonged clomiphene citrate therapy may show elevated serum levels of desmosterol. This is most likely due to a direct interference with cholesterol synthesis. However, the serum sterols in patients receiving the recommended dose of clomiphene citrate are not significantly altered. Ovarian cancer has been infrequently reported in patients who have received fertility drugs. Infertility is a primary risk factor for ovarian cancer; however, epidemiology data suggest that prolonged use of clomiphene may increase the risk of a borderline or invasive ovarian tumor.
Postmarketing Adverse Events
The following adverse reactions have been identified during the post approval use of clomiphene citrate. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Body as a Whole: Fever, tinnitus, weakness
Cardiovascular: Arrhythmia, chest pain, edema, hypertension, palpitation, phlebitis, pulmonary embolism, shortness of breath, tachycardia, thrombophlebitis
Central Nervous System: Migraine headache, paresthesia, seizure, stroke, syncope
Dermatologic: Acne, allergic reaction, erythema, erythema multiforme, erythema nodosum, hypertrichosis, pruritus, urticaria
Fetal/Neonatal Anomalies:
- Abnormal bone development: skeletal malformations of the skull, face, nasal passages, jaw, hand, limb (ectromelia including amelia, hemimelia, and phocomelia),foot (clubfoot), spine and joints
- Cardiac abnormalities: septal heart defects, muscular ventricular septal defect, patent ductus arteriosus, tetralogy of Fallot, and coarctation of the aorta
- Chromosomal disorders: Downs syndrome
- Ear abnormalities and deafness
- Gastrointestinal tract abnormalities: cleft lip and palate, imperforate anus, tracheoesophageal fistula, diaphragmatic hernia, omphalocele
- Genitalia abnormalities: hypospadias, cloacal exstrophy
- Lung tissue malformations
- Malformations of the eye and lens (cataract)
- Neoplasms: neuroectodermal tumor, thyroid tumor, hepatoblastoma, lymphocytic, leukemia
- Nervous system abnormalities: neural tube defects (anencephaly, meningomyelocele),microcephaly, and hydrocephalus
- Renal abnormalities: renal agenesis and renal dysgenesis
- Others: dwarfism, mental retardation
Gastrointestinal: Pancreatitis
Genitourinary: Endometriosis, ovarian cyst (ovarian enlargement or cysts could, as such, be complicated by adnexal torsion), ovarian hemorrhage, tubal pregnancy, uterine hemorrhage, reduced endometrial thickness
Hepatic: Transaminases increased, hepatitis.
Metabolism Disorders: Hypertriglyceridemia, in some cases with pancreatitis
Musculoskeletal: Arthralgia, back pain, myalgia.
Neoplasms: Liver (hepatic hemangiosarcoma, liver cell adenoma, hepatocellular carcinoma); breast (fibrocystic disease, breast carcinoma); endometrium (endometrial carcinoma); nervous system (astrocytoma, pituitary tumor, prolactinoma, neurofibromatosis, glioblastoma multiforme, brain abcess); ovary (luteoma of pregnancy, dermoid cyst of the ovary, ovarian carcinoma); trophoblastic (hydatiform mole, choriocarcinoma); miscellaneous (melanoma, myeloma, perianal cysts, renal cell carcinoma, Hodgkin’s lymphoma, tongue carcinoma, bladder carcinoma);
Psychiatric: Anxiety, irritability, mood changes, psychosis.
Visual Disorders: Abnormal accommodation, cataract, eye pain, macular edema, optic neuritis, photopsia, posterior vitreous detachment, retinal hemorrhage, retinal thrombosis, retinal vascular spasm, temporary or prolonged loss of vision, possibly irreversible.
Other: Leukocytosis, thyroid disorder.
OVERDOSAGE
Signs and Symptoms
Toxic effects accompanying acute overdosage of clomiphene citrate have not been reported. Signs and symptoms of overdosage as a result of the use of more than the recommended dose during clomiphene citrate therapy include nausea, vomiting, vasomotor flushes, visual blurring, spots or flashes, scotomata, ovarian enlargement with pelvic or abdominal pain. (See CONTRAINDICATIONS: Ovarian Cyst.)
Oral LD50. The acute oral LD50 of clomiphene citrate is 1700 mg/kg in mice and 5750 mg/kg in rats. The toxic dose in humans is not known.
Dialysis. It is not known if clomiphene citrate is dialyzable.
Treatment
In the event of overdose, appropriate supportive measures should be employed in addition to gastrointestinal decontamination.
DOSAGE AND ADMINISTRATION
General Considerations
The workup and treatment of candidates for clomiphene citrate therapy should be supervised by physicians experienced in management of gynecologic or endocrine disorders. Patients should be chosen for therapy with clomiphene citrate only after careful diagnostic evaluation (see INDICATIONS AND USAGE). The plan of therapy should be outlined in advance. Impediments to achieving the goal of therapy must be excluded or adequately treated before beginning clomiphene citrate. The therapeutic objective should be balanced with potential risks and discussed with the patient and others involved in the achievement of a pregnancy.
Ovulation most often occurs from 5 to 10 days after a course of clomiphene citrate. Coitus should be timed to coincide with the expected time of ovulation. Appropriate tests to determine ovulation may be useful during this time.
Recommended Dosage
Treatment of the selected patient should begin with a low dose, 50 mg daily (1 tablet) for 5 days. The dose should be increased only in those patients who do not ovulate in response to cyclic 50 mg clomiphene citrate. A low dosage or duration of treatment course is particularly recommended if unusual sensitivity to pituitary gonadotropin is suspected, such as in patients with polycystic ovary syndrome (see WARNINGS; Ovarian Hyperstimulation Syndrome).
The patient should be evaluated carefully to exclude pregnancy, ovarian enlargement, or ovarian cyst formation between each treatment cycle.
If progestin-induced bleeding is planned, or if spontaneous uterine bleeding occurs prior to therapy, the regimen of 50 mg daily for 5 days should be started on or about the 5th day of the cycle. Therapy may be started at any time in the patient who has had no recent uterine bleeding. When ovulation occurs at this dosage, there is no advantage to increasing the dose in subsequent cycles of treatment.
If ovulation does not appear to occur after the first course of therapy, a second course of 100 mg daily (two 50 mg tablets given as a single daily dose) for 5 days should be given. This course may be started as early as 30 days after the previous one after precautions are taken to exclude the presence of pregnancy. Increasing the dosage or duration of therapy beyond 100 mg/day for 5 days is not recommended.
The majority of patients who are going to ovulate will do so after the first course of therapy. If ovulation does not occur after three courses of therapy, further treatment with clomiphene citrate is not recommended and the patient should be reevaluated. If three ovulatory responses occur, but pregnancy has not been achieved, further treatment is not recommended. If menses does not occur after an ovulatory response, the patient should be reevaluated. Long-term cyclic therapy is not recommended beyond a total of about six cycles (see PRECAUTIONS).
HOW SUPPLIED
Clomiphene Citrate Tablets, USP, 50 mg are round, off-white, debossed “Par 701” with bisect on one side and plain on the other. They are supplied in cartons of 30 (NDC 63629-2165-1).
Store tablets at controlled room temperature 15° to 30°C (59° to 86°F). Protect from heat, light, and excessive humidity, and store in closed containers.
Rx Only
Repackaged/Relabeled by:
Bryant Ranch Prepack, Inc.
Burbank, CA 91504