FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
ZYLET® (loteprednol etabonate and tobramycin ophthalmic suspension), 0.5%/0.3% is a topical anti-infective and corticosteroid combination for steroid-responsive inflammatory ocular conditions for which a corticosteroid is indicated and where superficial bacterial ocular infection or a risk of bacterial ocular infection exists.
Ocular steroids are indicated in inflammatory conditions of the palpebral and bulbar conjunctiva, cornea and anterior segment of the globe such as allergic conjunctivitis, acne rosacea, superficial punctate keratitis, herpes zoster keratitis, iritis, cyclitis, and where the inherent risk of steroid use in certain infective conjunctivitides is accepted to obtain a diminution in edema and inflammation. They are also indicated in chronic anterior uveitis and corneal injury from chemical, radiation or thermal burns, or penetration of foreign bodies.
The use of a combination drug with an anti-infective component is indicated where the risk of superficial ocular infection is high or where there is an expectation that potentially dangerous numbers of bacteria will be present in the eye.
The particular anti-infective drug in this product (tobramycin) is active against the following common bacterial eye pathogens:
Staphylococci, including S. aureus and S. epidermidis (coagulase-positive and coagulase-negative), including penicillin-resistant strains. Streptococci, including some of the Group A-beta-hemolytic species, some nonhemolytic species, and some Streptococcus pneumoniae, Pseudomonas aeruginosa, Escherichia coli, Klebsiella pneumoniae, Enterobacter aerogenes, Proteus mirabilis, Morganella morganii, most Proteus vulgaris strains, Haemophilus influenzae, and H. aegyptius, Moraxella lacunata, Acinetobacter calcoaceticus and some Neisseria species.
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosing
Apply one or two drops of ZYLET into the conjunctival sac of the affected eye every four to six hours. During the initial 24 to 48 hours, the dosing may be increased, to every one to two hours. Frequency should be decreased gradually as warranted by improvement in clinical signs. Care should be taken not to discontinue therapy prematurely.
2.2 Prescription Guideline
Not more than 20 mL should be prescribed initially and the prescription should not be refilled without further evaluation [see Warnings and Precautions (5.3)].
3 DOSAGE FORMS AND STRENGTHS
Ophthalmic suspension containing 5 mg/mL (0.5%) loteprednol etabonate and 3 mg/mL (0.3%) tobramycin.
4 CONTRAINDICATIONS
4.1 Nonbacterial Etiology
ZYLET, as with other steroid anti-infective ophthalmic combination drugs, is contraindicated in most viral diseases of the cornea and conjunctiva including epithelial herpes simplex keratitis (dendritic keratitis), vaccinia, and varicella, and also in mycobacterial infection of the eye and fungal diseases of ocular structures.
5 WARNINGS AND PRECAUTIONS
5.1 Intraocular Pressure (IOP) Increase
Prolonged use of corticosteroids may result in glaucoma with damage to the optic nerve, defects in visual acuity and fields of vision. Steroids should be used with caution in the presence of glaucoma.
If this product is used for 10 days or longer, intraocular pressure should be monitored.
5.3 Delayed Healing
The use of steroids after cataract surgery may delay healing and increase the incidence of bleb formation. In those diseases causing thinning of the cornea or sclera, perforations have been known to occur with the use of topical steroids. The initial prescription and renewal of the medication order should be made by a physician only after examination of the patient with the aid of magnification such as a slit lamp biomicroscopy and, where appropriate, fluorescein staining.
5.4 Bacterial Infections
Prolonged use of corticosteroids may suppress the host response and thus increase the hazard of secondary ocular infections. In acute purulent conditions of the eye, steroids may mask infection or enhance existing infection. If signs and symptoms fail to improve after 2 days, the patient should be re-evaluated.
5.5 Viral Infections
Employment of a corticosteroid medication in the treatment of patients with a history of herpes simplex requires great caution. Use of ocular steroids may prolong the course and may exacerbate the severity of many viral infections of the eye (including herpes simplex).
5.6 Fungal Infections
Fungal infections of the cornea are particularly prone to develop coincidentally with long-term local steroid application. Fungus invasion must be considered in any persistent corneal ulceration where a steroid has been used or is in use. Fungal cultures should be taken when appropriate.
5.7 Aminoglycoside Hypersensitivity
Sensitivity to topically applied aminoglycosides may occur in some patients. If hypersensitivity develops with this product, discontinue use and institute appropriate therapy.
6 ADVERSE REACTIONS
Adverse reactions have occurred with steroid/anti-infective combination drugs which can be attributed to the steroid component, the anti-infective component, or the combination.
ZYLET
In a 42-day safety study comparing ZYLET to placebo, ocular adverse reactions included injection (approximately 20%) and superficial punctate keratitis (approximately 15%). Increased intraocular pressure was reported in 10% (ZYLET) and 4% (placebo) of subjects. Nine percent (9%) of ZYLET subjects reported burning and stinging upon instillation.
Ocular reactions reported with an incidence less than 4% include vision disorders, discharge, itching, lacrimation disorder, photophobia, corneal deposits, ocular discomfort, eyelid disorder, and other unspecified eye disorders.
The incidence of non-ocular reactions reported in approximately 14% of subjects was headache; all other non-ocular reactions had an incidence of less than 5%.
Loteprednol etabonate ophthalmic suspension 0.2% - 0.5%
Reactions associated with ophthalmic steroids include elevated intraocular pressure, which may be associated with infrequent optic nerve damage, visual acuity and field defects, posterior subcapsular cataract formation, delayed wound healing and secondary ocular infection from pathogens including herpes simplex, and perforation of the globe where there is thinning of the cornea or sclera.
In a summation of controlled, randomized studies of individuals treated for 28 days or longer with loteprednol etabonate, the incidence of significant elevation of intraocular pressure (≥10 mm Hg) was 2% (15/901) among patients receiving loteprednol etabonate, 7% (11/164) among patients receiving 1% prednisolone acetate and 0.5% (3/583) among patients receiving placebo.
Tobramycin ophthalmic solution 0.3%
The most frequent adverse reactions to topical tobramycin are hypersensitivity and localized ocular toxicity, including lid itching and swelling and conjunctival erythema. These reactions occur in less than 4% of patients. Similar reactions may occur with the topical use of other aminoglycoside antibiotics.
Secondary Infection
The development of secondary infection has occurred after use of combinations containing steroids and antimicrobials. Fungal infections of the cornea are particularly prone to develop coincidentally with long-term applications of steroids.
The possibility of fungal invasion must be considered in any persistent corneal ulceration where steroid treatment has been used.
Secondary bacterial ocular infection following suppression of host responses also occurs.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no adequate and well-controlled studies with loteprednol etabonate or tobramycin in pregnant women.
Loteprednol etabonate produced teratogenicity at clinically relevant doses in the rabbit and rat when administered orally during pregnancy. Loteprednol etabonate produced malformations when administered orally to pregnant rabbits at doses ≥ 0.54 times the recommended human ophthalmic dose (RHOD) and to pregnant rats at doses ≥ 13 times the RHOD. In pregnant rats receiving oral doses of loteprednol etabonate during the period equivalent to the last trimester of pregnancy through lactation in humans, survival of offspring was reduced at doses ≥ 1.3 times the RHOD. Maternal toxicity was observed in rats at doses ≥ 135 times the RHOD, and a maternal no observed adverse effect level (NOAEL) was established at 13 times the RHOD.
Abortions were observed in pregnant rabbits administered tobramycin via subcutaneous injection at 180 times the RHOD. Tobramycin did not affect fetal development when administered by subcutaneous injection to pregnant rats at doses 450 times the RHOD.
The background risk of major birth defects and miscarriage for the indicated population is unknown. However, the background risk in the U.S. general population of major birth defects is 2 to 4%, and of miscarriage is 15 to 20%, of clinically recognized pregnancies.
Data
Animal Data
Embryofetal studies were conducted in pregnant rabbits administered loteprednol etabonate by oral gavage on gestation days 6 to 18, to target the period of organogenesis. Loteprednol etabonate produced fetal malformations at doses ≥ 0.1 mg/kg/day (0.54 times the recommended human ophthalmic dose (RHOD) based on body surface area, assuming 100% absorption of loteprednol etabonate). Spina bifida (including meningocele) was observed at doses ≥ 0.1 mg/kg/day, and exencephaly and craniofacial malformations were observed at doses ≥ 0.4 mg/kg/day (2.1 times the RHOD). At 3 mg/kg/day (16 times the RHOD), loteprednol etabonate was associated with increased incidences of abnormal left common carotid artery, limb flexures, umbilical hernia, scoliosis, and delayed ossification. Abortion and embryofetal lethality (resorption) occurred at doses ≥ 6 mg/kg/day (32 times the RHOD). A NOAEL for developmental toxicity was not established in this study. The NOAEL for maternal toxicity in rabbits was 3 mg/kg/day.
Embryofetal studies were conducted in pregnant rats administered loteprednol etabonate by oral gavage on gestation days 6 to 15, to target the period of organogenesis. Loteprednol etabonate produced fetal malformations, including absent innominate artery at doses ≥ 5 mg/kg/day (13 times the RHOD); and cleft palate, agnathia, cardiovascular defects, umbilical hernia, decreased fetal body weight and decreased skeletal ossification at doses ≥ 50 mg/kg/day (135 times the RHOD). Embryofetal lethality (resorption) was observed at 100 mg/kg/day (270 times the RHOD). The NOAEL for developmental toxicity in rats was 0.5 mg/kg/day (1.3 times the RHOD). Loteprednol etabonate was maternally toxic (reduced body weight gain) at doses of ≥ 50 mg/kg/day. The NOAEL for maternal toxicity was 5 mg/kg/day.
A peri-/postnatal study was conducted in rats administered loteprednol etabonate by oral gavage from gestation day 15 (start of fetal period) to postnatal day 21 (the end of lactation period). At doses ≥ 0.5 mg/kg/day (1.3 times the RHOD), reduced survival was observed in live-born offspring. Doses ≥ 5 mg/kg/day (13 times the RHOD) caused umbilical hernia/incomplete gastrointestinal tract. Doses ≥ 50 mg/kg/day (135 times the RHOD) produced maternal toxicity (reduced body weight gain, death), decreased number of live-born offspring, decreased birth weight, and delays in postnatal development. A developmental NOAEL was not established in this study. The NOAEL for maternal toxicity was 5 mg/kg/day.
An embryofetal study was conducted in pregnant rabbits administered 20 or 40 mg/kg/day tobramycin by subcutaneous injection on gestational days 6 to 18, to target the period of organogenesis. Abortions and maternal toxicity (renal nephrosis and cortical tubular necrosis) were observed at both dose levels. The developmental and maternal lowest observed adverse effect level (LOAEL) is 20 mg/kg/day (180 times the RHOD based on body surface area, assuming 100% absorption of tobramycin). An embryofetal study was conducted in pregnant rats administered 50 or 100 mg/kg/day tobramycin by subcutaneous injection on gestational days 6 to 15, to target the period of organogenesis. No effects on development, reproduction, or maternal toxicity were reported. The developmental and maternal NOAEL is 100 mg/kg/day (450 times the RHOD).
8.2 Lactation
There are no data on the presence of loteprednol etabonate or tobramycin in human milk, the effects on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered, along with the mother’s clinical need for ZYLET and any potential adverse effects on the breastfed infant from ZYLET.
8.4 Pediatric Use
Two trials were conducted to evaluate the safety and efficacy of ZYLET (loteprednol etabonate and tobramycin ophthalmic suspension) in pediatric subjects age zero to six years; one was in subjects with lid inflammation and the other was in subjects with blepharoconjunctivitis.
In the lid inflammation trial, ZYLET with warm compresses did not demonstrate efficacy compared to vehicle with warm compresses. Patients received warm compress lid treatment plus ZYLET or vehicle for 14 days. The majority of patients in both treatment groups showed reduced lid inflammation.
In the blepharoconjunctivitis trial, ZYLET did not demonstrate efficacy compared to vehicle, loteprednol etabonate ophthalmic suspension, or tobramycin ophthalmic solution. There was no difference between treatment groups in mean change from baseline blepharoconjunctivitis score at Day 15.
There were no differences in safety assessments between the treatment groups in either trial.
11 DESCRIPTION
ZYLET (loteprednol etabonate and tobramycin ophthalmic suspension) is a sterile, multiple dose topical anti-inflammatory corticosteroid and anti-infective combination for ophthalmic use. Both loteprednol etabonate and tobramycin are white to off-white powders. The chemical structures of loteprednol etabonate and tobramycin are shown below.
Loteprednol etabonate:
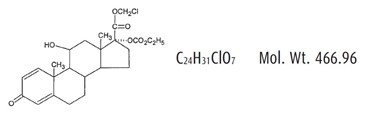
Chemical name: chloromethyl 17α-[(ethoxycarbonyl)oxy]-11β-hydroxy-3-oxoandrosta-1,4-diene-17β-carboxylate
Tobramycin:
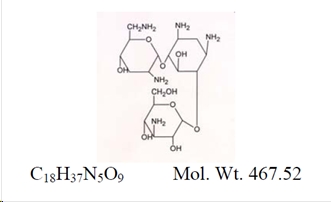
Chemical name:
O-3-Amino-3-deoxy-α-D-glucopyranosyl-(1→4)-O-[2,6-diamino-2,3,6-trideoxy-α-D-ribo-hexopyranosyl-(1→6)]-2-deoxystreptamine
Each mL contains: Actives: Loteprednol Etabonate 5 mg (0.5%) and Tobramycin 3 mg (0.3%). Inactives: Edetate Disodium, Glycerin, Povidone, Purified Water, Tyloxapol, and Benzalkonium Chloride 0.01% (preservative). Sulfuric Acid and/or Sodium Hydroxide may be added to adjust the pH to 5.5 to 6.2. The suspension is essentially isotonic with a tonicity of 260 to 320 mOsm/kg.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Corticosteroids inhibit the inflammatory response to a variety of inciting agents and probably delay or slow healing. They inhibit the edema, fibrin deposition, capillary dilation, leukocyte migration, capillary proliferation, fibroblast proliferation, deposition of collagen, and scar formation associated with inflammation. There is no generally accepted explanation for the mechanism of action of ocular corticosteroids. However, corticosteroids are thought to act by the induction of phospholipase A2 inhibitory proteins, collectively called lipocortins. It is postulated that these proteins control the biosynthesis of potent mediators of inflammation such as prostaglandins and leukotrienes by inhibiting the release of their common precursor arachidonic acid.
Arachidonic acid is released from membrane phospholipids by phospholipase A2. Corticosteroids are capable of producing a rise in intraocular pressure.
Loteprednol etabonate is structurally similar to other corticosteroids. However, the number 20 position ketone group is absent.
The anti-infective component in the combination (tobramycin) is included to provide action against susceptible organisms. In vitro studies have demonstrated that tobramycin is active against susceptible strains of the following microorganisms:
Staphylococci, including S. aureus and S. epidermidis (coagulase-positive and coagulase-negative), including penicillin-resistant strains.
Streptococci, including some of the Group A-beta-hemolytic species, some nonhemolytic species, and some Streptococcus pneumoniae. Pseudomonas aeruginosa, Escherichia coli, Klebsiella pneumoniae, Enterobacter aerogenes, Proteus mirabilis, Morganella morganii, most Proteus vulgaris strains, Haemophilus influenzae and H. aegyptius, Moraxella lacunata, Acinetobacter calcoaceticus and some Neisseria species.
12.3 Pharmacokinetics
In a controlled clinical study of ocular penetration, the levels of loteprednol etabonate in the aqueous humor were found to be comparable between LOTEMAX® and ZYLET treatment groups.
Results from a bioavailability study in normal volunteers established that plasma levels of loteprednol etabonate and Δ1 cortienic acid etabonate (PJ 91), its primary, inactive metabolite, were below the limit of quantitation (1 ng/mL) at all sampling times.
The results were obtained following the ocular administration of one drop in each eye of 0.5% loteprednol etabonate ophthalmic suspension 8 times daily for 2 days or 4 times daily for 42 days. This study suggests that limited (<1 ng/mL) systemic absorption occurs with 0.5% loteprednol etabonate.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Long-term animal studies have not been conducted to evaluate the carcinogenic potential of loteprednol etabonate or tobramycin.
Mutagenesis
Loteprednol etabonate was not genotoxic in vitro in the Ames test, the mouse lymphoma TK assay, a chromosome aberration test in human lymphocytes, or in an in vivo mouse micronucleus assay.
Impairment of Fertility
Oral treatment of female and male rats with 25 mg/kg/day of loteprednol etabonate (67 times the RHOD based on body surface area, assuming 100% absorption) prior to and during mating caused preimplantation loss and decreased the number of live fetuses/live births. The NOAEL for fertility in rats was 5 mg/kg/day (13 times the RHOD). Subcutaneous administration of male and female rats with tobramycin did not affect mating behavior or cause impairment of fertility at 100 mg/kg/day (450 times the RHOD based on body surface area, assuming 100% absorption).
16 HOW SUPPLIED/STORAGE AND HANDLING
ZYLET (loteprednol etabonate and tobramycin ophthalmic suspension) 0.5%/0.3% is supplied in a white low density polyethylene plastic bottle with a white controlled drop tip and a white polypropylene cap in the following sizes:
NDC 24208-358-05 5 mL fill in a 7.5 mL bottle
NDC 24208-358-10 10 mL fill in a 10 mL bottle
USE ONLY IF IMPRINTED NECKBAND IS INTACT.
Storage: Store upright at 15ºC to 25ºC (59ºF to 77ºF). PROTECT FROM FREEZING. SHAKE VIGOROUSLY BEFORE USING. After opening, ZYLET can be used until the expiration date on the bottle.
17 PATIENT COUNSELING INFORMATION
Risk of Contamination
This product is sterile when packaged. Advise patients not to allow the dropper tip to touch any surface, as this may contaminate the suspension.
Risk of Secondary Infection
Advise patients to consult a physician if pain develops, redness, itching or inflammation becomes aggravated.
Contact Lens Wear
As with all ophthalmic preparations containing benzalkonium chloride, advise patients not to wear soft contact lenses when using ZYLET.
Distributed by:
Bausch & Lomb Americas Inc.
Bridgewater, NJ 08807 USA
Manufactured by:
Bausch & Lomb Incorporated
Tampa, FL 33637 USA
ZYLET and LOTEMAX are trademarks of Bausch & Lomb Incorporated or its affiliates.
© 2022 Bausch & Lomb Incorporated or its affiliates
9007709 (FOLDED)
9004409 (FLAT)