WARNING: CIGARETTE SMOKING AND SERIOUS CARDIOVASCULAR EVENTS
Cigarette smoking increases the risk of serious cardiovascular events from combination oral contraceptive (COC) use. This risk increases with age, particularly in women over 35 years of age, and with the number of cigarettes smoked. For this reason, COCs, including norethindrone acetate and ethinyl estradiol tablets, are contraindicated in women who are over 35 years of age and smoke (see CONTRAINDICATIONS and WARNINGS).
DESCRIPTION
Norethindrone Acetate and Ethinyl Estradiol Tablets, USP are a progestogen-estrogen combination.
Each blue tablet contains norethindrone acetate (19-Norpregn-4-en-20-yn-3-one, 17-(acetyloxy)-, (17α)), 1.5 mg; ethinyl estradiol (19-Norpregna-1,3,5(10)-trien-20-yne-3, 17-diol, (17α)-), 0.03 mg. Also contains lactose anhydrous, dl-α-tocopherol, compressible sugar, croscarmellose sodium, FD & C Blue No. 1 Aluminum Lake, lactose monohydrate, magnesium stearate, povidone K-25, sodium lauryl sulphate.
The structural formulas are as follows:
CLINICAL PHARMACOLOGY
Combination oral contraceptives act by suppression of gonadotropins. Although the primary mechanism of this action is inhibition of ovulation, other alterations include changes in the cervical mucus (which increase the difficulty of sperm entry into the uterus) and the endometrium (which reduce the likelihood of implantation).
Pharmacokinetics
The pharmacokinetics of norethindrone acetate and ethinyl estradiol tablets have not been characterized; however, the following pharmacokinetic information regarding norethindrone acetate and ethinyl estradiol is taken from the literature.
Absorption
Norethindrone acetate appears to be completely and rapidly deacetylated to norethindrone after oral administration, since the disposition of norethindrone acetate is indistinguishable from that of orally administered norethindrone (1). Norethindrone acetate and ethinyl estradiol are subject to first-pass metabolism after oral dosing, resulting in an absolute bioavailability of approximately 64% for norethindrone and 43% for ethinyl estradiol (1-3).
Distribution
Volume of distribution of norethindrone and ethinyl estradiol ranges from 2 to 4 L/kg (1-3). Plasma protein binding of both steroids is extensive (greater than 95%); norethindrone binds to both albumin and sex hormone binding globulin, whereas ethinyl estradiol binds only to albumin (4).
Metabolism
Norethindrone undergoes extensive biotransformation, primarily via reduction, followed by sulfate and glucuronide conjugation. The majority of metabolites in the circulation are sulfates, with glucuronides accounting for most of the urinary metabolites (5). A small amount of norethindrone acetate is metabolically converted to ethinyl estradiol. Ethinyl estradiol is also extensively metabolized, both by oxidation and by conjugation with sulfate and glucuronide. Sulfates are the major circulating conjugates of ethinyl estradiol and glucuronides predominate in urine. The primary oxidative metabolite is 2-hydroxy ethinyl estradiol, formed by the CYP3A4 isoform of cytochrome P450. Part of the first-pass metabolism of ethinyl estradiol is believed to occur in gastrointestinal mucosa. Ethinyl estradiol may undergo enterohepatic circulation (6).
Excretion
Norethindrone and ethinyl estradiol are excreted in both urine and feces, primarily as metabolites (5, 6). Plasma clearance values for norethindrone and ethinyl estradiol are similar (approximately 0.4 L/hr/kg) (1-3).
Special Population
Race
The effect of race on the disposition of norethindrone acetate and ethinyl estradiol tablets has not been evaluated.
Renal Insufficiency
The effect of renal disease on the disposition of norethindrone acetate and ethinyl estradiol tablets has not been evaluated. In premenopausal women with chronic renal failure undergoing peritoneal dialysis who received multiple doses of an oral contraceptive containing ethinyl estradiol and norethindrone, plasma ethinyl estradiol concentrations were higher and norethindrone concentrations were unchanged compared to concentrations in premenopausal women with normal renal function.
INDICATIONS AND USAGE
Norethindrone acetate and ethinyl estradiol tablets are indicated for the prevention of pregnancy in women who elect to use oral contraceptives as a method of contraception.
Oral contraceptives are highly effective. Table I lists the typical accidental pregnancy rates for users of combination oral contraceptives and other methods of contraception. The efficacy of these contraceptive methods, except sterilization, depends upon the reliability with which they are used. Correct and consistent use of methods can result in lower failure rates.
TABLE I LOWEST EXPECTED AND TYPICAL FAILURE RATES DURING THE FIRST YEAR OF CONTINUOUS USE OF A METHOD
| Adapted from RA Hatcher et al, Reference 7. | ||
|
||
|
% Of Women Experiencing an Unintended Pregnancy |
||
|
Method |
Lowest Expected* |
Typical† |
|
(No contraception) |
(85) |
(85) |
|
Oral contraceptives |
3 |
|
|
Combined |
0.1 |
N/A ‡ |
|
progestin only |
0.5 |
N/A ‡ |
|
Diaphragm with spermicidal cream or jelly |
6 |
20 |
|
Spermicides alone (foam, creams, gels, vaginal |
6 |
26 |
|
Vaginal Sponge | ||
|
nulliparous |
9 |
20 |
|
parous |
20 |
40 |
|
Implant |
0.05 |
0.05 |
|
Injection: depot medroxyprogesterone acetate |
0.3 |
0.3 |
|
IUD | ||
|
progesterone T |
1.5 |
2.0 |
|
copper T 380A |
0.6 |
0.8 |
|
LNg 20 |
0.1 |
0.1 |
|
Condom without spermicides | ||
|
female |
5 |
21 |
|
male |
3 |
14 |
|
Cervical Cap with spermicidal cream or jelly | ||
|
nulliparous |
9 |
20 |
|
parous |
26 |
40 |
|
Periodic abstinence (all methods) |
1-9 |
25 |
|
Withdrawal |
4 |
19 |
|
Female sterilization |
0.5 |
0.5 |
|
Male sterilization |
0.10 |
0.15 |
CONTRAINDICATIONS
Oral contraceptives are contraindicated in women who currently have the following conditions:
- •
- Thrombophlebitis or thromboembolic disorders
- •
- A past history of deep vein thrombophlebitis or thromboembolic disorders
- •
- Cerebral vascular or coronary artery disease
- •
- Current diagnosis of, or history of, breast cancer, which may be hormone sensitive
- •
- Carcinoma of the endometrium or other known or suspected estrogen-dependent neoplasia
- •
- Undiagnosed abnormal genital bleeding
- •
- Cholestatic jaundice of pregnancy or jaundice with prior pill use
- •
- Hepatic adenomas or carcinomas
- •
- Are receiving Hepatitis C drug combinations containing ombitasvir/paritaprevir/ritonavir, with or without dasabuvir, due to the potential for ALT elevations (see Warnings, RISK OF LIVER ENZYME ELEVATIONS WITH CONCOMITANT HEPATITIS C TREATMENT).
WARNINGS
The use of oral contraceptives is associated with increased risks of several serious conditions including myocardial infarction, thromboembolism, stroke, hepatic neoplasia, and gallbladder disease, although the risk of serious morbidity or mortality is very small in healthy women without underlying risk factors. The risk of morbidity and mortality increases significantly in the presence of other underlying risk factors such as hypertension, hyperlipidemias, obesity, and diabetes.
Practitioners prescribing oral contraceptives should be familiar with the following information relating to these risks.
The information contained in this package insert is principally based on studies carried out in patients who used oral contraceptives with higher formulations of estrogens and progestogens than those in common use today. The effect of long-term use of the oral contraceptives with lower formulations of both estrogens and progestogens remains to be determined.
Throughout this labeling, epidemiological studies reported are of two types: retrospective or case control studies and prospective or cohort studies. Case control studies provide a measure of the relative risk of a disease, namely, a ratio of the incidence of a disease among oral contraceptive users to that among nonusers. The relative risk does not provide information on the actual clinical occurrence of a disease. Cohort studies provide a measure of attributable risk, which is the difference in the incidence of disease between oral contraceptive users and nonusers. The attributable risk does provide information about the actual occurrence of a disease in the population (adapted from References 8 and 9 with the author's permission). For further information, the reader is referred to a text on epidemiological methods.
1. Thromboembolic Disorders and Other Vascular Problems
a. Myocardial Infarction
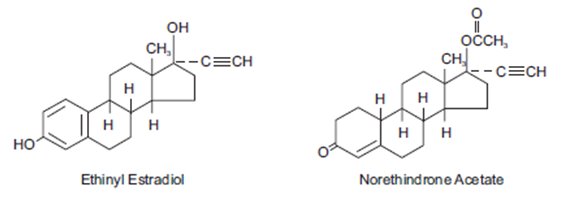
An increased risk of myocardial infarction has been attributed to oral contraceptive use. This risk is primarily in smokers or women with other underlying risk factors for coronary artery disease such as hypertension, hypercholesterolemia, morbid obesity, and diabetes. The relative risk of heart attack for current oral contraceptive users has been estimated to be two to six (10-16). The risk is very low under the age of 30.
Smoking in combination with oral contraceptive use has been shown to contribute substantially to the incidence of myocardial infarctions in women in their mid-thirties or older with smoking accounting for the majority of excess cases (17). Mortality rates associated with circulatory disease have been shown to increase substantially in smokers over the age of 35 and non-smokers over the age of 40 (Table II) among women who use oral contraceptives.
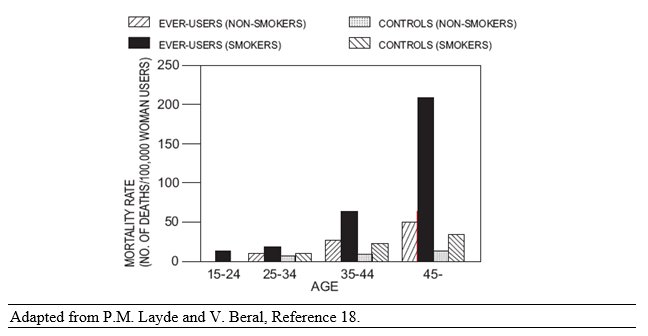
TABLE II CIRCULATORY DISEASE MORTALITY RATES PER 100,000 WOMAN YEARS BY AGE, SMOKING STATUS AND ORAL CONTRACEPTIVE USE
Oral contraceptives may compound the effects of well-known risk factors, such as hypertension, diabetes, hyperlipidemias, age and obesity (19). In particular, some progestogens are known to decrease HDL cholesterol and cause glucose intolerance, while estrogens may create a state of hyperinsulinism (20-24). Oral contraceptives have been shown to increase blood pressure among users (see section 9 in WARNINGS). Similar effects on risk factors have been associated with an increased risk of heart disease. Oral contraceptives must be used with caution in women with cardiovascular disease risk factors.
b. Thromboembolism
An increased risk of thromboembolic and thrombotic disease associated with the use of oral contraceptives is well established. Case control studies have found the relative risk of users compared to non-users to be 3 for the first episode of superficial venous thrombosis, 4 to 11 for deep vein thrombosis or pulmonary embolism, and 1.5 to 6 for women with predisposing conditions for venous thromboembolic disease (9, 10, 25-30). Cohort studies have shown the relative risk to be somewhat lower, about 3 for new cases and about 4.5 for new cases requiring hospitalization (31). The risk of thromboembolic disease due to oral contraceptives is not related to length of use and disappears after pill use is stopped (8).
A two- to four-fold increase in relative risk of postoperative thromboembolic complications has been reported with the use of oral contraceptives (15, 32). The relative risk of venous thrombosis in women who have predisposing conditions is twice that of women without such medical conditions (15, 32). If feasible, oral contraceptives should be discontinued at least four weeks prior to and for two weeks after elective surgery of a type associated with an increase in risk of thromboembolism and during and following prolonged immobilization. Since the immediate postpartum period is also associated with an increased risk of thromboembolism, oral contraceptives should be started no earlier than four to six weeks after delivery in women who elect not to breastfeed.
c. Cerebrovascular Disease
Oral contraceptives have been shown to increase both the relative and attributable risks of cerebrovascular events (thrombotic and hemorrhagic strokes), although, in general, the risk is greatest among older (greater than 35 years), hypertensive women who also smoke. Hypertension was found to be a risk factor for both users and nonusers, for both types of strokes, while smoking interacted to increase the risk for hemorrhagic strokes (33-35).
In a large study, the relative risk of thrombotic strokes has been shown to range from 3 for normotensive users to 14 for users with severe hypertension (36). The relative risk of hemorrhagic stroke is reported to be 1.2 for non-smokers who used oral contraceptives, 2.6 for smokers who did not use oral contraceptives, 7.6 for smokers who used oral contraceptives, 1.8 for normotensive users, and 25.7 for users with severe hypertension (36). The attributable risk is also greater in older women (9).
d. Dose-related Risk of Vascular Disease from Oral Contraceptives
A positive association has been observed between the amount of estrogen and progestogen in oral contraceptives and the risk of vascular disease (37-39). A decline in serum high-density lipoproteins (HDL) has been reported with many progestational agents (20-22). A decline in serum high-density lipoproteins has been associated with an increased incidence of ischemic heart disease. Because estrogens increase HDL cholesterol, the net effect of an oral contraceptive depends on a balance achieved between doses of estrogen and progestin and the nature of the progestin used in the contraceptives. The amount and activity of both hormones should be considered in the choice of an oral contraceptive.
Minimizing exposure to estrogen and progestogen is in keeping with good principles of therapeutics. For any particular oral contraceptive, the dosage regimen prescribed should be one which contains the least amount of estrogen and progestogen that is compatible with the needs of the individual patient. New acceptors of oral contraceptive agents should be started on preparations containing the lowest dose of estrogen which produces satisfactory results for the patient.
e. Persistence of Risk of Vascular Disease
There are two studies which have shown persistence of risk of vascular disease for ever-users of oral contraceptives. In a study in the United States, the risk of developing myocardial infarction after discontinuing oral contraceptives persists for at least 9 years for women 40-49 years who had used oral contraceptives for 5 or more years, but this increased risk was not demonstrated in other age groups (14). In another study in Great Britain, the risk of developing cerebrovascular disease persisted for at least 6 years after discontinuation of oral contraceptives, although excess risk was very small (40). However, both studies were performed with oral contraceptive formulations containing 50 mcg or higher of estrogens.
2. Estimates of Mortality from Contraceptive Use
One study gathered data from a variety of sources which have estimated the mortality rate associated with different methods of contraception at different ages (Table III). These estimates include the combined risk of death associated with contraceptive methods plus the risk attributable to pregnancy in the event of method failure. Each method of contraception has its specific benefits and risks. The study concluded that with the exception of oral contraceptive users 35 and older who smoke and 40 and older who do not smoke, mortality associated with all methods of birth control is low and below that associated with childbirth. The observation of a possible increase in risk of mortality with age for oral contraceptive users is based on data gathered in the 1970's but not reported until 1983 (41). However, current clinical practice involves the use of lower estrogen dose formulations combined with careful restriction of oral contraceptive use to women who do not have the various risk factors listed in this labeling.
Because of these changes in practice and, also, because of some limited new data which suggest that the risk of cardiovascular disease with the use of oral contraceptives may now be less than previously observed (Porter JB, Hunter J, Jick H, et al. Oral contraceptives and nonfatal vascular disease. Obstet Gynecol 1985;66:1-4; and Porter JB, Hershel J, Walker AM. Mortality among oral contraceptive users. Obstet Gynecol 1987;70:29-32), the Fertility and Maternal Health Drugs Advisory Committee was asked to review the topic in 1989. The Committee concluded that although cardiovascular disease risks may be increased with oral contraceptive use after age 40 in healthy non-smoking women (even with the newer low-dose formulations), there are greater potential health risks associated with pregnancy in older women and with the alternative surgical and medical procedures which may be necessary if such women do not have access to effective and acceptable means of contraception.
Therefore, the Committee recommended that the benefits of oral contraceptive use by healthy non-smoking women over 40 may outweigh the possible risks. Of course, older women, as all women who take oral contraceptives, should take the lowest possible dose formulation that is effective.
| Adapted from H.W. Ory, Reference 41. | ||||||
|
Method of control and |
15-19 |
20-24 |
25-29 |
30-34 |
35-39 |
40-44 |
|
No fertility control methods |
7.0 |
7.4 |
9.1 |
14.8 |
25.7 |
28.2 |
|
Oral contraceptives non- |
0.3 |
0.5 |
0.9 |
1.9 |
13.8 |
31.6 |
|
Oral contraceptives |
2.2 |
3.4 |
6.6 |
13.5 |
51.1 |
117.2 |
|
IUD* |
0.8 |
0.8 |
1.0 |
1.0 |
1.4 |
1.4 |
|
Condom† |
1.1 |
1.6 |
0.7 |
0.2 |
0.3 |
0.4 |
|
Diaphragm/ spermicide† |
1.9 |
1.2 |
1.2 |
1.3 |
2.2 |
2.8 |
|
Periodic abstinence† |
2.5 |
1.6 |
1.6 |
1.7 |
2.9 |
3.6 |
3. Malignant Neoplasms
Breast Cancer
Norethindrone acetate and ethinyl estradiol tablets are contraindicated in females who currently have or have had breast cancer because breast cancer may be hormonally sensitive (see CONTRAINDICATIONS).
Epidemiology studies have not found a consistent association between use of combined oral contraceptives (COCs) and breast cancer risk. Studies do not show an association between ever (current or past) use of COCs and risk of breast cancer. However, some studies report a small increase in the risk of breast cancer among current or recent users (<6 months since last use) and current users with longer duration of COC use (see ADVERSE REACTIONS, Postmarketing Experience).
Cervical Cancer
Some studies suggest that oral contraceptive use has been associated with an increase in the risk of cervical intraepithelial neoplasia in some populations of women (42-45). However, there continues to be controversy about the extent to which such findings may be due to differences in sexual behavior and other factors
4. Hepatic Neoplasia
Benign hepatic adenomas are associated with oral contraceptive use, although the incidence of benign tumors is rare in the United States. Indirect calculations have estimated the attributable risk to be in the range of 3.3 cases/100,000 for users, a risk that increases after four or more years of use (46). Rupture of rare, benign, hepatic adenomas may cause death through intra-abdominal hemorrhage (47,48).
Studies from Britain have shown an increased risk of developing hepatocellular carcinoma (49- 51) in long-term (greater than 8 years) oral contraceptive users. However, these cancers are extremely rare in the U.S., and the attributable risk (the excess incidence) of liver cancers in oral contraceptive users approaches less than one per million users.
5. Risk of Liver Enzyme Elevations with Concomitant Hepatitis C Treatment
During clinical trials with the Hepatitis C combination drug regimen that contains ombitasvir/paritaprevir/ritonavir, with or without dasabuvir, ALT elevations greater than 5 times the upper limit of normal (ULN), including some cases greater than 20 times the ULN, were significantly more frequent in women using ethinyl estradiol-containing medications such as COCs. Discontinue norethindrone acetate and ethinyl estradiol tablets prior to starting therapy with the combination drug regimen ombitasvir/paritaprevir/ritonavir, with or without dasabuvir (see Contraindications). Norethindrone acetate and ethinyl estradiol tablets can be restarted approximately 2 weeks following completion of treatment with the combination drug regimen.
6. Ocular Lesions
There have been clinical case reports of retinal thrombosis associated with the use of oral contraceptives. Oral contraceptives should be discontinued if there is unexplained partial or complete loss of vision; onset of proptosis or diplopia; papilledema; or retinal vascular lesions. Appropriate diagnostic and therapeutic measures should be undertaken immediately.
7. Oral Contraceptive Use Before and During Early Pregnancy
Extensive epidemiological studies have revealed no increased risk of birth defects in women who have used oral contraceptives prior to pregnancy (52-54). Studies also do not suggest a teratogenic effect, particularly insofar as cardiac anomalies and limb reduction defects are concerned (52, 53, 55, 56), when taken inadvertently during early pregnancy.
The administration of oral contraceptives to induce withdrawal bleeding should not be used as a test for pregnancy. Oral contraceptives should not be used during pregnancy to treat threatened or habitual abortion.
It is recommended that for any patient who has missed two consecutive periods, pregnancy should be ruled out before continuing oral contraceptive use. If the patient has not adhered to the prescribed schedule, the possibility of pregnancy should be considered at the time of the first missed period. Oral contraceptive use should be discontinued if pregnancy is confirmed.
8. Gallbladder Disease
Earlier studies have reported an increased lifetime relative risk of gallbladder surgery in users of oral contraceptives and estrogens (57, 58). More recent studies, however, have shown that the relative risk of developing gallbladder disease among oral contraceptive users may be minimal (59-61). The recent findings of minimal risk may be related to the use of oral contraceptive formulations containing lower hormonal doses of estrogens and progestogens.
9. Carbohydrate and Lipid Metabolic Effects
Oral contraceptives have been shown to cause glucose intolerance in a significant percentage of users (23). Oral contraceptives containing greater than 75 mcg of estrogens cause hyperinsulinism, while lower doses of estrogen cause less glucose intolerance (62). Progestogens increase insulin secretion and create insulin resistance, this effect varying with different progestational agents (23, 63). However, in the non-diabetic woman, oral contraceptives appear to have no effect on fasting blood glucose (64). Because of these demonstrated effects, prediabetic and diabetic women should be carefully observed while taking oral contraceptives.
A small proportion of women will have persistent hypertriglyceridemia while on the pill. As discussed earlier (see WARNINGS 1a. and 1d.), changes in serum triglycerides and lipoprotein levels have been reported in oral contraceptive users.
10. Elevated Blood Pressure
An increase in blood pressure has been reported in women taking oral contraceptives (65) and this increase is more likely in older oral contraceptive users (66) and with continued use (65). Data from the Royal College of General Practitioners (18) and subsequent randomized trials have shown that the incidence of hypertension increases with increasing concentrations of progestogens.
Women with a history of hypertension or hypertension-related diseases or renal disease (67) should be encouraged to use another method of contraception. If women elect to use oral contraceptives, they should be monitored closely, and if significant elevation of blood pressure occurs, oral contraceptives should be discontinued. For most women, elevated blood pressure will return to normal after stopping oral contraceptives (66), and there is no difference in the occurrence of hypertension among ever and never users (65,67,68).
11. Headache
The onset or exacerbation of migraine or development of headache with a new pattern which is recurrent, persistent, or severe requires discontinuation of oral contraceptives and evaluation of the cause.
12. Bleeding Irregularities
Breakthrough bleeding and spotting are sometimes encountered in patients on oral contraceptives, especially during the first three months of use. Non-hormonal causes should be considered, and adequate diagnostic measures taken to rule out malignancy or pregnancy in the event of breakthrough bleeding, as in the case of any abnormal vaginal bleeding. If pathology has been excluded, time or a change to another formulation may solve the problem. In the event of amenorrhea, pregnancy should be ruled out.
Some women may encounter post-pill amenorrhea or oligomenorrhea, especially when such a condition was preexistent.
PRECAUTIONS
1. Patients should be counseled that this product does not protect against HIV infection (AIDS) and other sexually transmitted infections.
2. Physical Examination and Follow-Up
It is good medical practice for all women to have annual history and physical examinations, including women using oral contraceptives. The physical examination, however, may be deferred until after initiation of oral contraceptives if requested by the woman and judged appropriate by the clinician. The physical examination should include special reference to blood pressure, breasts, abdomen and pelvic organs, including cervical cytology, and relevant laboratory tests. In case of undiagnosed, persistent or recurrent abnormal vaginal bleeding, appropriate measures should be conducted to rule out malignancy. Women with a strong family history of breast cancer or who have breast nodules should be monitored with particular care.
3. Lipid Disorders
Women who are being treated for hyperlipidemia should be followed closely if they elect to use oral contraceptives. Some progestogens may elevate LDL levels and may render the control of hyperlipidemias more difficult.
4. Liver Function
If jaundice develops in any woman receiving such drugs, the medication should be discontinued. Steroid hormones may be poorly metabolized in patients with impaired liver function.
5. Fluid Retention
Oral contraceptives may cause some degree of fluid retention. They should be prescribed with caution, and only with careful monitoring, in patients with conditions which might be aggravated by fluid retention.
6. Contact Lenses
Contact lens wearers who develop visual changes or changes in lens tolerance should be assessed by an ophthalmologist.
7. Drug Interactions
Effects of Other Drugs on Oral Contraceptives (69)
Rifampin
Metabolism of both norethindrone and ethinyl estradiol is increased by rifampin. A reduction in contraceptive effectiveness and increased incidence of breakthrough bleeding and menstrual irregularities have been associated with concomitant use of rifampin.
Anticonvulsants
Anticonvulsants such as phenobarbital, phenytoin, and carbamazepine, have been shown to increase the metabolism of ethinyl estradiol and/or norethindrone, which could result in a reduction in contraceptive effectiveness.
Troglitazone
Administration of troglitazone with an oral contraceptive containing ethinyl estradiol and norethindrone reduced the plasma concentrations of both by approximately 30%, which could result in a reduction in contraceptive effectiveness.
Antibiotics
Pregnancy while taking oral contraceptives has been reported when the oral contraceptives were administered with antimicrobials such as ampicillin, tetracycline, and griseofulvin. However, clinical pharmacokinetic studies have not demonstrated any consistent effect of antibiotics (other than rifampin) on plasma concentrations of synthetic steroids.
Concomitant Use with HCV Combination Therapy - Liver Enzyme Elevation
Co-administration of norethindrone acetate and ethinyl estradiol tablets with HCV drug combinations containing ombitasvir/paritaprevir/ritonavir, with or without dasabuvir is contraindicated due to potential for ALT elevations (see Warnings, RISK OF LIVER ENZYME ELEVATIONS WITH CONCOMITANT HEPATITIS C TREATMENT). Co-administration of norethindrone acetate and ethinyl estradiol tablets and glecaprevir/pibrentasvir is not recommended due to potential for ALT elevations.
Effects of Oral Contraceptives on Other Drugs
Oral contraceptive combinations containing ethinyl estradiol may inhibit the metabolism of other compounds. Increased plasma concentrations of cyclosporine, prednisolone, and theophylline have been reported with concomitant administration of oral contraceptives. In addition, oral contraceptives may induce the conjugation of other compounds. Decreased plasma concentrations of acetaminophen and increased clearance of temazepam, salicylic acid, morphine, and clofibric acid have been noted when these drugs were administered with oral contraceptives.
8. Interactions with Laboratory Tests
Certain endocrine and liver function tests and blood components may be affected by oral contraceptives:
- a.
- Increased prothrombin and factors VII, VIII, IX, and X; decreased antithrombin 3; increased norepinephrine-induced platelet aggregability.
- b.
- Increased thyroid binding globulin (TBG) leading to increased circulating total thyroid hormone, as measured by protein-bound iodine (PBI), T4 by column or by radioimmunoassay. Free T3 resin uptake is decreased, reflecting the elevated TBG; free T4 concentration is unaltered.
- c.
- Other binding proteins may be elevated in serum.
- d.
- Sex-binding globulins are increased and result in elevated levels of total circulating sex steroids and corticoids; however, free or biologically active levels remain unchanged.
- e.
- Triglycerides may be increased.
- f.
- Glucose tolerance may be decreased.
- g.
- Serum folate levels may be depressed by oral contraceptive therapy. This may be of clinical significance if a woman becomes pregnant shortly after discontinuing oral contraceptives.
10. Pregnancy
Discontinue norethindrone acetate and ethinyl estradiol tablets if pregnancy occurs because there is no reason to use COCs in pregnancy. See WARNINGS section.
11. Lactation
Small amounts of oral contraceptive steroids have been identified in human milk, and a few adverse effects on the child have been reported, including jaundice and breast enlargement. In addition, oral contraceptives given in the postpartum period may interfere with lactation by decreasing the quantity and quality of breast milk. If possible, the nursing mother should be advised not to use oral contraceptives but to use other forms of contraception until she has completely weaned her child.
12. Pediatric Use
Safety and efficacy of norethindrone acetate and ethinyl estradiol tablets have been established in women of reproductive age. Safety and efficacy are expected to be the same for postpubertal adolescents under the age of 16 and for users 16 years and older. Use of this product before menarche is not indicated.
PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (PATIENT PACKAGE INSERT BRIEF SUMMARY and DETAILED PATIENT PACKAGE INSERT).
- •
- Counsel patients that cigarette smoking increases the risk of serious cardiovascular events from COC use, and that women who are over 35 years old and smoke should not use COCs (see BOXED WARNING and CONTRAINDICATIONS).
- •
- Counsel patients that the increased risk of venous thromboembolism compared to non-users of CHCs is greatest after initially starting a CHC or restarting (following a 4-week or greater interruption in intake) the same or a different CHC (see WARNINGS).
- •
- Counsel patients that this product does not protect against HIV-infection (AIDS) and other sexually transmitted infections.
- •
- Counsel patients to take one tablet daily by mouth at the same time every day. Instruct patients what to do in the event pills are missed (see DOSAGE AND ADMINISTRATION).
- •
- Counsel patients to use a back-up or alternative method of contraception when enzyme inducers are used with COCs (see PRECAUTIONS).
- •
- Counsel patients who are breastfeeding or who desire to breastfeed that COCs may reduce breast milk production. This is less likely to occur if breastfeeding is well established (see PRECAUTIONS).
- •
- Counsel any patient who starts norethindrone acetate and ethinyl estradiol tablets postpartum, and who has not yet had a period, to use an additional method of contraception until she has taken a blue tablet for 7 consecutive days (see DOSAGE AND ADMINISTRATION).
- •
- Counsel patients that amenorrhea may occur. Pregnancy should be considered in the event of amenorrhea, and should be ruled out if amenorrhea is associated with symptoms of pregnancy, such as morning sickness or unusual breast tenderness (see WARNINGS).
- •
- Counsel patients with a history of depression that depression may reoccur. Women should contact their healthcare provider if depression occurs (see WARNINGS).
ADVERSE REACTIONS
An increased risk of the following serious adverse reactions has been associated with the use of oral contraceptives (see WARNINGS section):
- •
- Thrombophlebitis
- •
- Arterial thromboembolism
- •
- Pulmonary embolism
- •
- Myocardial infarction
- •
- Cerebral hemorrhage
- •
- Cerebral thrombosis
- •
- Hypertension
- •
- Gallbladder disease
- •
- Hepatic adenomas or benign liver tumors
Post Marketing Experience
Five studies that compared breast cancer risk between ever-users (current or past use) of COCs and never-users of COCs reported no association between ever use of COCs and breast cancer risk, with effect estimates ranging from 0.90 - 1.12 (Figure 1) (70-74).
Three studies compared breast cancer risk between current or recent COC users (<6 months since last use) and never users of COCs (Figure 1) (70,73,75). One of these studies reported no association between breast cancer risk and COC use. The other two studies found an increased relative risk of 1.19 - 1.33 with current or recent use. Both of these studies found an increased risk of breast cancer with current use of longer duration, with relative risks ranging from 1.03 with less than one year of COC use to approximately 1.4 with more than 8-10 years of COC use.
There is evidence of an association between the following conditions and the use of oral contraceptives, although additional confirmatory studies are needed:
- •
- Mesenteric thrombosis
- •
- Retinal thrombosis
The following adverse reactions have been reported in patients receiving oral contraceptives and are believed to be drug-related:
- •
- Nausea
- •
- Vomiting
- •
- Gastrointestinal symptoms (such as abdominal cramps and bloating)
- •
- Breakthrough bleeding
- •
- Spotting
- •
- Change in menstrual flow
- •
- Amenorrhea
- •
- Temporary infertility after discontinuation of treatment
- •
- Edema
- •
- Melasma which may persist
- •
- Breast changes: tenderness, enlargement, secretion
- •
- Change in weight (increase or decrease)
- •
- Change in cervical erosion and secretion
- •
- Diminution in lactation when given immediately postpartum
- •
- Cholestatic jaundice
- •
- Migraine
- •
- Rash (allergic)
- •
- Depression
- •
- Reduced tolerance to carbohydrates
- •
- Vaginal candidiasis
- •
- Change in corneal curvature (steepening)
- •
- Intolerance to contact lenses
The following adverse reactions have been reported in users of oral contraceptives and the association has been neither confirmed nor refuted:
- •
- Pre-menstrual syndrome
- •
- Cataracts
- •
- Changes in appetite
- •
- Cystitis-like syndrome
- •
- Headache
- •
- Nervousness
- •
- Dizziness
- •
- Hirsutism
- •
- Loss of scalp hair
- •
- Erythema multiforme
- •
- Erythema nodosum
- •
- Hemorrhagic eruption
- •
- Vaginitis
- •
- Porphyria
- •
- Impaired renal function
- •
- Hemolytic uremic syndrome
- •
- Budd-Chiari syndrome
- •
- Acne
- •
- Changes in libido
- •
- Colitis
OVERDOSAGE
Serious ill effects have not been reported following acute ingestion of large doses of oral contraceptives by young children. Overdosage may cause nausea, and withdrawal bleeding may occur in females.
NON-CONTRACEPTIVE HEALTH BENEFITS
The following non-contraceptive health benefits related to the use of oral contraceptives are supported by epidemiological studies which largely utilized oral contraceptive formulations containing estrogen doses exceeding 0.035 mg of ethinyl estradiol or 0.05 mg of mestranol (76-81).
Effects on menses:
- •
- Increased menstrual cycle regularity
- •
- Decreased blood loss and decreased incidence of iron deficiency anemia
- •
- Decreased incidence of dysmenorrhea
Effects related to inhibition of ovulation:
- •
- Decreased incidence of functional ovarian cysts
- •
- Decreased incidence of ectopic pregnancies
Effects from long-term use:
- •
- Decreased incidence of fibroadenomas and fibrocystic disease of the breast
- •
- Decreased incidence of acute pelvic inflammatory disease
- •
- Decreased incidence of endometrial cancer
- •
- Decreased incidence of ovarian cancer
DOSAGE AND ADMINISTRATION
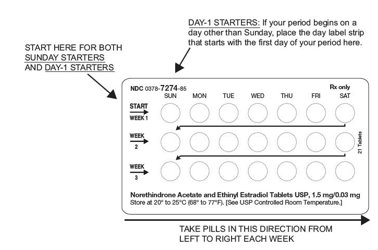
The tablet blister pack has been designed to make oral contraceptive dosing as easy and as convenient as possible. The tablets are arranged in three rows of seven tablets each, with the days of the week appearing on the tablet blister above the first row of tablets.
Note: Each blister card has been preprinted with the days of the week, starting with Sunday, to facilitate a Sunday-Start regimen. Six different day label strips have been provided with the Detailed Patient & Brief Summary Patient Package Insert in order to accommodate a Day-1 Start regimen. If the patient is using the Day-1 Start regimen, she should place the self-adhesive day label strip that corresponds to her starting day over the preprinted days.
Important: The patient should be instructed to use an additional method of protection until after the first week of administration in the initial cycle when utilizing the Sunday-Start regimen.
The possibility of ovulation and conception prior to initiation of use should be considered.
Dosage and Administration for 21-Day Dosage Regimen
To achieve maximum contraceptive effectiveness, norethindrone acetate and ethinyl estradiol tablets must be taken exactly as directed and at intervals not exceeding 24 hours. Norethindrone acetate and ethinyl estradiol tablets provide the patient with a convenient tablet schedule of “3 weeks on - 1 week off.” Two dosage regimens are described, one of which may be more convenient or suitable than the other for an individual patient. For the initial cycle of therapy, the patient begins her tablets according to the Day-1 Start or Sunday-Start regimen. With either regimen, the patient takes one tablet daily for 21 consecutive days followed by one week of no tablets.
- A.
- Sunday-Start Regimen: The patient begins taking tablets from the top row on the first Sunday after menstrual flow begins. When menstrual flow begins on Sunday, the first tablet is taken on the same day. The last tablet in the blister pack will then be taken on a Saturday, followed by no tablets for a week (7 days). For all subsequent cycles, the patient then begins a new 21-tablet regimen on the eighth day, Sunday, after taking her last tablet. Following this regimen, of 21 days on – 7 days off, the patient will start all subsequent cycles on a Sunday.
- B.
- Day-1 Regimen: The first day of menstrual flow is Day 1. The patient places the self-adhesive day label strip that corresponds to her starting day over the preprinted days on the blister pack. She starts taking one tablet daily, beginning with the first tablet in the top row. The patient completes her 21-tablet regimen when she has taken the last tablet in the tablet blister pack. She will then take no tablets for a week (7 days). For all subsequent cycles, the patient begins a new 21-tablet regimen on the eighth day after taking her last tablet, again starting with the first tablet in the top row after placing the appropriate day label strip over the preprinted days on the tablet blister pack. Following this regimen of 21 days on – 7 days off, the patient will start all subsequent cycles on the same day of the week as the first course. Likewise, the interval of no tablets will always start on the same day of the week.
Tablets should be taken regularly with a meal or at bedtime. It should be stressed that efficacy of medication depends on strict adherence to the dosage schedule.
Special Notes on Administration
Menstruation usually begins two or three days, but may begin as late as the fourth or fifth day, after discontinuing medication. If spotting occurs while on the usual regimen of one tablet daily, the patient should continue medication without interruption.
If the patient forgets to take one or more tablets, the following is suggested:
One tablet is missed
- •
- take tablet as soon as remembered
- •
- take next tablet at the regular time
Two consecutive tablets are missed (week 1 or week 2)
- •
- take two tablets as soon as remembered
- •
- take two tablets the next day
- •
- use another birth control method for seven days following the missed tablets
Two consecutive tablets are missed (week 3)
Sunday-Start Regimen:
- •
- take one tablet daily until Sunday
- •
- discard remaining tablets
- •
- start new pack of tablets immediately (Sunday)
- •
- use another birth control method for seven days following the missed tablets
Day-1 Start Regimen:
- •
- discard remaining tablets
- •
- start new pack of tablets that same day
- •
- use another birth control method for seven days following the missed tablets
Three (or more) consecutive tablets are missed
Sunday-Start Regimen:
- •
- take one tablet daily until Sunday
- •
- discard remaining tablets
- •
- start new pack of tablets immediately (Sunday)
- •
- use another birth control method for seven days following the missed tablets
Day-1 Start Regimen:
- •
- discard remaining tablets
- •
- start new pack of tablets that same day
- •
- use another birth control method for seven days following the missed tablets
The possibility of ovulation occurring increases with each successive day that scheduled tablets are missed. While there is little likelihood of ovulation occurring if only one tablet is missed, the possibility of spotting or bleeding is increased. This is particularly likely to occur if two or more consecutive tablets are missed.
In the rare case of bleeding which resembles menstruation, the patient should be advised to discontinue medication and then begin taking tablets from a new tablet blister pack on the next Sunday or the first day (Day 1), depending on her regimen. Persistent bleeding which is not controlled by this method indicates the need for reexamination of the patient, at which time nonfunctional causes should be considered.
Use of Oral Contraceptives in the Event of a Missed Menstrual Period
- 1.
- If the patient has not adhered to the prescribed dosage regimen, the possibility of pregnancy should be considered after the first missed period and oral contraceptives should be withheld until pregnancy has been ruled out.
- 2.
- If the patient has adhered to the prescribed regimen and misses two consecutive periods, pregnancy should be ruled out before continuing the contraceptive regimen.
After several months on treatment, bleeding may be reduced to a point of virtual absence. This reduced flow may occur as a result of medication, in which event it is not indicative of pregnancy.
HOW SUPPLIED
Norethindrone Acetate and Ethinyl Estradiol Tablets USP, 1.5 mg/0.03 mg are packaged in a carton of three pouches (NDC 0378-7274-53); each pouch contains a blister pack of 21 tablets. Each blister pack contains 21 blue, round, flat-faced, unscored tablet debossed with 237 on one side and plain on the other side.
Store at 20° to 25°C (68° to 77°F). [See USP Controlled Room Temperature.]
REFERENCES
- 1.
- Back DJ, Breckenridge AM, Crawford FE, Mclver M, Orme ML'E, Rowe PH and Smith E: Kinetics of norethindrone in women II. Single-dose kinetics. Clin Pharmacol Ther 1978; 24:448-453.
- 2.
- Humpel M, Nieuweboer B, Wendt H and Speck U: Investigations of pharmacokinetics of ethinyloestradiol to specific consideration of a possible first-pass effect in women. Contraception 1979;19:421-432.
- 3.
- Back DJ, Breckenridge AM, Crawford FE, Maclver M, Orme ML'E, Rowe PH and Watts MJ. An investigation of the pharmacokinetics of ethinyl estradiol in women using radioimmunoassay. Contraception 1979;20:263-273.
- 4.
- Hammond GL, Lahteenmaki PLA, Lahteenmaki P and Luukkainen T. Distribution and percentages of non-protein bound contraceptive steroids in human serum. J Steriod Biochem 1982;17:375-380.
- 5.
- Fotherby K. Pharmacokinetics and metabolism of progestins in humans, in Pharmacology of the contraceptive steroids, Goldzieher JW, Fotherby K (eds), Raven Press, Ltd., New York, 1994;99-126.
- 6.
- Goldzieher JW. Pharmacokinetics and metabolism of ethynyl estrogens, in Pharmacology of the contraceptive steroids, Goldzieher JW, Fotherby K (eds), Raven Press Ltd., New York, 1994;127-151.
- 7.
- Hatcher RA, et al. 1998. Contraceptive Technology, Seventeenth Edition. New York: Irvington Publishers.
- 8.
- Stadel, B.V.: Oral contraceptives and cardiovascular disease. (Pt. 1). New England Journal of Medicine, 305:612-618, 1981.
- 9.
- Stadel, B.V.: Oral contraceptives and cardiovascular disease. (Pt. 2). New England Journal of Medicine, 305:672-677, 1981.
- 10.
- Adam, S.A., and M. Thorogood: Oral contraception and myocardial infarction revisited: The effects of new preparations and prescribing patterns. Brit. J. Obstet. and Gynec., 88:838-845, 1981.
- 11.
- Mann, J.I., and W.H. Inman: Oral contraceptives and death from myocardial infarction. Brit. Med. J., 2(5965): 245-248, 1975.
- 12.
- Mann, J.I., M.P. Vessey, M. Thorogood, and R. Doll: Myocardial infarction in young women with special reference to oral contraceptive practice. Brit. Med. J., 2(5956):241-245, 1975.
- 13.
- Royal College of General Practitioners' Oral Contraception Study: Further analyses of mortality in oral contraceptive users. Lancet, 1:541-546, 1981.
- 14.
- Slone, D., S. Shapiro, D.W. Kaufman, L. Rosenberg, O.S. Miettinen, and P.D. Stolley: Risk of myocardial infarction in relation to current and discontinued use of oral contraceptives. N.E.J.M., 305:420-424, 1981.
- 15.
- Vessey, M.P.: Female hormones and vascular disease: An epidemiological overview. Brit. J. Fam. Plann., 6:1-12, 1980.
- 16.
- Russell-Briefel, R.G., T.M. Ezzati, R. Fulwood, J.A. Perlman, and R.S. Murphy: Cardiovascular risk status and oral contraceptive use, United States, 1976-80. Preventive Medicine, 15:352-362, 1986.
- 17.
- Goldbaum, G.M., J.S. Kendrick, G.C. Hogelin, and E.M. Gentry: The relative impact of smoking and oral contraceptive use on women in the United States. J.A.M.A., 258:1339-1342, 1987.
- 18.
- Layde, P.M., and V. Beral: Further analyses of mortality in oral contraceptive users: Royal College General Practitioners' Oral Contraception Study. (Table 5) Lancet, 1:541-546, 1981.
- 19.
- Knopp, R.H.: Arteriosclerosis risk: The roles of oral contraceptives and postmenopausal estrogens. J. of Reprod. Med., 31(9)(Supplement): 913-921, 1986.
- 20.
- Krauss, R.M., S. Roy, D.R. Mishell, J. Casagrande, and M.C. Pike: Effects of two low-dose oral contraceptives on serum lipids and lipoproteins: Differential changes in high-density lipoproteins subclasses. Am. J. Obstet Gyn., 145:446-452, 1983.
- 21.
- Wahl, P., C. Walden, R. Knopp, J. Hoover, R. Wallace, G. Heiss, and B. Rifkind: Effect of estrogen/progestin potency on lipid/lipoprotein cholesterol. N.E.J.M., 308:862-867, 1983.
- 22.
- Wynn, V., and R. Niththyananthan: The effect of progestin in combined oral contraceptives on serum lipids with special reference to high-density lipoproteins. Am. J. Obstet. and Gyn., 142:766-771, 1982.
- 23.
- Wynn, V., and I. Godsland: Effects of oral contraceptives on carbohydrate metabolism. J. Reprod. Medicine, 31 (9)(Supplement): 892-897, 1986.
- 24.
- LaRosa, J.C.: Atherosclerotic risk factors in cardiovascular disease. J. Reprod. Med., 31(9)(Supplement): 906-912, 1986.
- 25.
- Inman, W.H., and M.P. Vessey: Investigations of death from pulmonary, coronary, and cerebral thrombosis and embolism in women of child-bearing age. Brit. Med. J., 2(5599): 193-199, 1968.
- 26.
- Maguire, M.G., J. Tonascia, P.E. Sartwell, P.D. Stolley, and M.S. Tockman: Increased risk of thrombosis due to oral contraceptives: A further report. Am. J. Epidemiology, 110(2): 188-195, 1979.
- 27.
- Pettiti, D.B., J. Wingerd, F. Pellegrin, and S. Ramacharan: Risk of vascular disease in women: Smoking, oral contraceptives, noncontraceptive estrogens, and other factors. J.A.M.A., 242:1150-1154, 1979.
- 28.
- Vessey, M.P., and R. Doll: Investigation of relation between use of oral contraceptives and thromboembolic disease. Brit. Med. J., 2(5599): 199-205, 1968.
- 29.
- Vessey, M.P., and R. Doll: Investigation of relation between use of oral contraceptives and thromboembolic disease: A further report. Brit. Med. J., 2(5658): 651-657, 1969.
- 30.
- Porter, J.B., J.R. Hunter, D.A. Danielson, H. Jick, and A. Stergachis: Oral contraceptives and non-fatal vascular disease: Recent experience. Obstet. and Gyn., 59(3):299-302, 1982.
- 31.
- Vessey, M., R. Doll, R. Peto, B. Johnson, and P. Wiggins: A long-term follow-up study of women using different methods of contraception: An interim report. J.Biosocial. Sci., 8:375-427, 1976.
- 32.
- Royal College of General Practitioners: Oral contraceptives, venous thrombosis, and varicose veins. J. of Royal College of General Practitioners, 28:393-399, 1978.
- 33.
- Collaborative Group for the study of stroke in young women: Oral contraception and increased risk of cerebral ischemia or thrombosis. N.E.J.M., 288:871-878, 1973.
- 34.
- Petitti, D.B., and J.Wingerd: Use of oral contraceptives, cigarette smoking, and risk of subarachnoid hemorrhage. Lancet, 2:234-236, 1978.
- 35.
- Inman, W.H.: Oral contraceptives and fatal subarachnoid hemorrhage. Brit. Med. J., 2(6203): 1468-70, 1979.
- 36.
- Collaborative Group for the study of stroke in young women: Oral contraceptives and stroke in young women: Associated risk factors. J.A.M.A., 231:718-722, 1975.
- 37.
- Inman, W.H., M.P. Vessey, B. Westerholm, and A. Engelund: Thromboembolic disease and the steroidal content of oral contraceptives. A report to the Committee on Safety of Drugs. Brit. Med. J., 2:203-209, 1970.
- 38.
- Meade, T.W., G. Greenberg, and S.G. Thompson: Progestogens and cardiovascular reactions associated with oral contraceptives and a comparison of the safety of 50- and 35-mcg oestrogen preparations. Brit. Med. J., 280(6224): 1157-1161, 1980.
- 39.
- Kay, C.R.: Progestogens and arterial disease: Evidence from the Royal College of General Practitioners' study. Amer. J. Obstet. Gyn., 142:762-765, 1982.
- 40.
- Royal College of General Practitioners: Incidence of arterial disease among oral contraceptive users. J. Coll. Gen. Pract., 33:75-82, 1983.
- 41.
- Ory, H.W: Mortality associated with fertility and fertility control: 1983. Family Planning Perspectives, 15:50-56, 1983.
- 42.
- Ory, H., Z. Naib, S.B. Conger, R.A. Hatcher, and C.W. Tyler: Contraceptive choice and prevalence of cervical dysplasia and carcinoma in situ. Am. J. Obstet. Gynec., 124:573-577, 1976.
- 43.
- Vessey, M.P., M. Lawless, K. McPherson, D. Yeates: Neoplasia of the cervix uteri and contraception: A possible adverse effect of the pill. Lancet, 2:930, 1983.
- 44.
- Brinton, L.A., G.R. Huggins, H.F. Lehman, K. Malli, D.A. Savitz, E. Trapido, J. Rosenthal, and R. Hoover: Long-term use of oral contraceptives and risk of invasive cervical cancer. Int. J. Cancer, 38:339-344, 1986.
- 45.
- WHO Collaborative Study of Neoplasia and Steroid Contraceptives: Invasive cervical cancer and combined oral contraceptives. Brit. Med. J., 290:961-965, 1985.
- 46.
- Rooks, J.B., H.W. Ory, K.G. Ishak, L.T. Strauss, J.R. Greenspan, A.P. Hill, and C.W. Tyler: Epidemiology of hepatocellular adenoma: The role of oral contraceptive use. J.A.M.A., 242:644-648, 1979.
- 47.
- Bein, N.N., and H.S. Goldsmith: Recurrent massive hemorrhage from benign hepatic tumors secondary to oral contraceptives. Brit. J. Surg., 64:433-435, 1977.
- 48.
- Klatskin, G.: Hepatic tumors: Possible relationship to use of oral contraceptives. Gastroenterology, 73:386-394, 1977.
- 49.
- Henderson, B.E., S. Preston-Martin, H.A. Edmondson, R.L. Peters, and M.C. Pike: Hepatocellular carcinoma and oral contraceptives. Brit. J. Cancer, 48:437-440, 1983.
- 50.
- Neuberger, J., D. Forman, R. Doll, and R. Williams: Oral contraceptives and hepatocellular carcinoma. Brit. Med. J., 292:1355-1357, 1986.
- 51.
- Forman, D., T.J. Vincent, and R. Doll: Cancer of the liver and oral contraceptives. Brit. Med. J., 292:1357-1361, 1986.
- 52.
- Harlap, S., and J. Eldor: Births following oral contraceptive failures. Obstet. Gynec., 55:447-452, 1980.
- 53.
- Savolainen, E., E. Saksela, and L. Saxen: Teratogenic hazards of oral contraceptives analyzed in a national malformation register. Amer. J. Obstet. Gynec., 140:521-524, 1981.
- 54.
- Janerich, D.T., J.M. Piper, and D.M. Glebatis: Oral contraceptives and birth defects. Am. J. Epidemiology, 112:73-79, 1980.
- 55.
- Ferencz, C., G.M. Matanoski, P.D. Wilson, J.D. Rubin, C.A. Neill, and R. Gutberlet: Maternal hormone therapy and congenital heart disease. Teratology, 21:225-239, 1980.
- 56.
- Rothman, K.J., D.C. Fyler, A. Goldbatt, and M.B. Kreidberg: Exogenous hormones and other drug exposures of children with congenital heart disease. Am. J. Epidemiology, 109:433-439, 1979.
- 57.
- Boston Collaborative Drug Surveillance Program: Oral contraceptives and venous thromboembolic disease, surgically confirmed gallbladder disease, and breast tumors. Lancet, 1:1399-1404, 1973.
- 58.
- Royal College of General Practitioners: Oral Contraceptives and Health. New York, Pittman, 1974, 100p.
- 59.
- Layde, P.M., M.P. Vessey, and D. Yeates: Risk of gallbladder disease: A cohort study of young women attending family planning clinics. J. of Epidemiol. and Comm. Health, 36:274-278, 1982.
- 60.
- Rome Group for the Epidemiology and Prevention of Cholelithiasis (GREPCO): Prevalence of gallstone disease in an Italian adult female population. Am. J. Epidemiol., 119:796-805, 1984.
- 61.
- Strom, B.L., R.T. Tamragouri, M.L. Morse, E.L. Lazar, S.L. West, P.D. Stolley, and J.K. Jones: Oral contraceptives and other risk factors for gallbladder disease. Clin. Pharmacol. Ther., 39:335-341, 1986.
- 62.
- Wynn, V., P.W. Adams, I.F. Godsland, J. Melrose, R. Niththyananthan, N.W. Oakley, and A. Seedj: Comparison of effects of different combined oral-contraceptive formulations on carbohydrate and lipid metabolism. Lancet, 1:1045-1049, 1979.
- 63.
- Wynn, V.: Effect of progesterone and progestins on carbohydrate metabolism. In Progesterone and Progestin. Edited by C.W. Bardin, E. Milgrom, P. Mauvis-Jarvis. New York, Raven Press, pp. 395-410, 1983.
- 64.
- Perlman, J.A., R. G. Roussell-Briefel, T.M. Ezzati, and G. Lieberknecht: Oral glucose tolerance and the potency of oral contraceptive progestogens. J. Chronic Dis., 38:857-864, 1985.
- 65.
- Royal College of General Practitioners' Oral Contraception Study: Effect on hypertension and benign breast disease of progestogen component in combined oral contraceptives. Lancet, 1:624, 1977.
- 66.
- Fisch, I.R., and J. Frank: Oral contraceptives and blood pressure. J.A.M.A., 237:2499-2503, 1977.
- 67.
- Laragh, A.J.: Oral contraceptive induced hypertension: Nine years later. Amer. J. Obstet. Gynecol., 126:141-147, 1976.
- 68.
- Ramcharan, S., E. Peritz, F.A. Pellegrin, and W.T. Williams: Incidence of hypertension in the Walnut Creek Contraceptive Drug Study cohort. In Pharmacology of Steroid Contraceptive Drugs. Edited by S. Garattini and H.W. Berendes. New York, Raven Press, pp. 277-288, 1977. (Monographs of the Mario Negri Institute for Pharmacological Research, Milan.)
- 69.
- Back DJ, Orme ML'E. Drug interactions, in Pharmacology of the contraceptive steroids. Goldzieher JW, Fotherby K (eds), Raven Press, Ltd., New York, 1994, 407-425.
- 70.
- Marchbanks PA, McDonald JA, Wilson HG, et al. Oral contraceptives and the risk of breast cancer. N Engl J Med. 2002;346(26):2025-2032.
- 71.
- Dumeaux V, Fournier A, Lund E, Clavel-Chapelon F. Previous oral contraceptive use and breast cancer risk according to hormone replacement therapy use among postmenopausal women. Cancer Causes Control. 2005;16(5):537-544.
- 72.
- Dorjgochoo T, Shu XO, Li HL, et al. Use of oral contraceptives, intrauterine devices and tubal sterilization and cancer risk in a large prospective study, from 1996 to 2006. Int J Cancer. 2009;124(10):2442-2449.
- 73.
- Hunter DJ, Colditz GA, Hankinson SE, et al. Oral contraceptive use and breast cancer: a prospective study of young women. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology.
2010;19(10):2496-2502. - 74.
- Vessey M, Yeates D. Oral contraceptive use and cancer. Final report from the Oxford-Family Planning Association contraceptive study. Contraception. 2013; 88(6): 678-683.
- 75.
- Morch LS, Skovlund CW, Hannaford PC, Iversen L, Fielding S, Lidegaard O. Contemporary Hormonal Contraception and the Risk of Breast Cancer. N Engl J Med. 2017;377(23):2228-2239.
- 76.
- The Cancer and Steroid Hormone Study of the Centers for Disease Control and the National Institute of Child Health and Human Development: Oral contraceptive use and the risk of ovarian cancer. J.A.M.A., 249:1596-1599, 1983.
- 77.
- The Cancer and Steroid Hormone Study of the Centers for Disease Control and the National Institute of Child Health and Human Development: Combination oral contraceptive use and the risk of endometrial cancer. J.A.M.A., 257:796-800, 1987.
- 78.
- Ory, H.W.: Functional ovarian cysts and oral contraceptives: Negative association confirmed surgically. J.A.M.A., 228:68-69, 1974.
- 79.
- Ory, H.W., P. Cole, B. Macmahon, and R. Hoover: Oral contraceptives and reduced risk of benign breast disease. N.E.J.M., 294:41-422, 1976.
- 80.
- Ory, H.W.: The noncontraceptive health benefits from oral contraceptive use. Fam. Plann. Perspectives, 14:182-184, 1982.
- 81.
- Ory, H.W., J.D. Forrest, and R. Lincoln: Making Choices: Evaluating the health risks and benefits of birth control methods. New York, The Alan Guttmacher Institute, p.1, 1983.
Patient Package Insert
BRIEF SUMMARY PATIENT PACKAGE INSERT
This product (like all oral contraceptives) is intended to prevent pregnancy. It does not protect against HIV infection (AIDS) and other sexually transmitted infections.
|
Cigarette smoking increases the risk of serious cardiovascular side effects from oral contraceptive use. This risk increases with age and with heavy smoking (15 or more cigarettes per day) and is quite marked in women over 35 years of age. Women who use oral contraceptives are strongly advised not to smoke. |
Oral contraceptives, also known as “birth control pills” or “the pill”, are taken to prevent pregnancy and, when taken correctly, have a failure rate of about 1% per year when used without missing any pills. The typical failure rate of large numbers of pill users is less than 3% per year when women who miss pills are included. For most women oral contraceptives are also free of serious or unpleasant side effects. However, forgetting to take pills considerably increases the chances of pregnancy.
For the majority of women, oral contraceptives can be taken safely. But there are some women who are at high risk of developing certain serious diseases that can be life-threatening or may cause temporary or permanent disability. The risks associated with taking oral contraceptives increase significantly if you:
- •
- Smoke
- •
- Have high blood pressure, diabetes, high cholesterol
- •
- Have or have had clotting disorders, heart attack, stroke, angina pectoris, cancer of the breast, jaundice, or malignant or benign liver tumors.
You should not take the pill if you suspect you are pregnant or have unexplained vaginal bleeding.
Most side effects of the pill are not serious. The most common side effects are nausea, vomiting, bleeding between menstrual periods, weight gain, breast tenderness, and difficulty wearing contact lenses. These side effects, especially nausea, vomiting, and breakthrough bleeding may subside within the first three months of use.
The serious side effects of the pill occur very infrequently, especially if you are in good health and are young. However, you should know that the following medical conditions have been associated with or made worse by the pill:
- 1.
- Blood clots in the legs (thrombophlebitis), lungs (pulmonary embolism), stoppage or rupture of a blood vessel in the brain (stroke), blockage of blood vessels in the heart (heart attack or angina pectoris) or other organs of the body. As mentioned above, smoking increases the risk of heart attacks and strokes and subsequent serious medical consequences.
- 2.
- Liver tumors, which may rupture and cause severe bleeding. A possible but not definite association has been found with the pill and liver cancer. However, liver cancers are extremely rare. The chance of developing liver cancer from using the pill is thus even rarer.
- 3.
- High blood pressure, although blood pressure usually returns to normal when the pill is stopped.
The symptoms associated with these serious side effects are discussed in the detailed leaflet given to you with your supply of pills. Notify your doctor or healthcare provider if you notice any unusual physical disturbances while taking the pill. In addition, drugs such as rifampin, as well as some anticonvulsants and some antibiotics, may decrease oral contraceptive effectiveness.
There may be slight increases in the risk of breast cancer among current users of hormonal birth control pills with longer duration of use of 8 years or more. Some studies have found an increase in the risk of developing cancer of the cervix in women taking the pill, but this finding may be related to differences in sexual behavior or other factors not related to use of the pill.
Taking the pill provides some important non-contraceptive benefits. These include less painful menstruation, less menstrual blood loss and anemia, fewer pelvic infections, and fewer cancers of the ovary and the lining of the uterus.
Be sure to discuss any medical condition you may have with your healthcare provider. Your healthcare provider will take a medical and family history and examine you before prescribing oral contraceptives. The physical examination may be delayed to another time if you request it and your healthcare provider believes that it is a good medical practice to postpone it. You should be reexamined at least once a year while taking oral contraceptives. The detailed patient information leaflet gives you further information which you should read and discuss with your healthcare provider.
This product (like all oral contraceptives) is intended to prevent pregnancy. It does not protect against transmission of HIV (AIDS) and other sexually transmitted infections such as Chlamydia, genital herpes, genital warts, gonorrhea, hepatitis B and syphilis.
INSTRUCTIONS TO PATIENT
TABLET BLISTER PACK
The norethindrone acetate and ethinyl estradiol tablet blister pack has been designed to make oral contraceptive dosing as easy and as convenient as possible. The tablets are arranged in three rows of seven tablets each, with the days of the week appearing on the tablet blister pack above the first row of tablets.
|
If your TABLET BLISTER PACK contains: |
You are taking: |
|
21 blue tablets |
Norethindrone Acetate and Ethinyl |
Each blue tablet contains 1.5 mg norethindrone acetate and 0.03 mg ethinyl estradiol.
DIRECTIONS
To remove a tablet, press down on it with your thumb or finger. The tablet will drop through the back of the tablet blister. Do not press with your thumbnail, fingernail, or any other sharp object.
HOW TO TAKE THE PILL
|
IMPORTANT POINTS TO REMEMBER
|
BEFORE YOU START TAKING YOUR PILLS:
- 1.
- BE SURE TO READ THESE DIRECTIONS:
Before you start taking your pills.
Anytime you are not sure what to do.
- 2.
- THE RIGHT WAY TO TAKE THE PILL IS TO TAKE ONE PILL EVERY DAY AT THE SAME TIME. If you miss pills you could get pregnant. This includes starting the pack late. The more pills you miss, the more likely you are to get pregnant.
- 3.
- MANY WOMEN HAVE SPOTTING OR LIGHT BLEEDING, OR MAY FEEL SICK TO THEIR STOMACH, DURING THE FIRST 1-3 PACKS OF PILLS. If you do have spotting or light bleeding or feel sick to your stomach, do not stop taking the pill. The problem will usually go away. If it doesn't go away, check with your doctor or clinic.
- 4.
- MISSING PILLS CAN ALSO CAUSE SPOTTING OR LIGHT BLEEDING, even when you make up these missed pills. On the days you take 2 pills to make up for missed pills, you could also feel a little sick to your stomach.
- 5.
- IF YOU HAVE VOMITING OR DIARRHEA, for any reason, or IF YOU TAKE SOME MEDICINES, including some antibiotics, your birth control pills may not work as well. Use a back-up birth control method (such as condoms or foam) until you check with your doctor or clinic.
- 6.
- IF YOU HAVE TROUBLE REMEMBERING TO TAKE THE PILL, talk to your doctor or clinic about how to make pill-taking easier or about using another method of birth control.
- 7.
- IF YOU HAVE ANY QUESTIONS OR ARE UNSURE ABOUT THE INFORMATION IN THIS LEAFLET, call your doctor or clinic.
|
BEFORE YOU START TAKING YOUR PILLS
|
- 1.
- DECIDE WHAT TIME OF DAY YOU WANT TO TAKE YOUR PILL. It is important to take it at about the same time every day.
- 2.
- LOOK AT YOUR PILL PACK TO SEE IF IT HAS 21 PILLS:
The 21-Day pill pack has 21 “active” blue pills (with hormones) to take for 3 weeks, followed by 1 week without pills.
- 3.
- ALSO FIND:
- 1)
- where on the pack to start taking pills,
- 2)
- in what order to take the pills (follow the arrows), and
- 3)
- the week numbers as shown in the following picture:
Norethindrone Acetate and Ethinyl Estradiol Tablets, 1.5 mg/0.03 mg will contain: ALL BLUE PILLS.
- 4.
- BE SURE YOU HAVE READY AT ALL TIMES:
ANOTHER KIND OF BIRTH CONTROL (such as condoms or foam) to use as a back-up in case you miss pills.
An EXTRA, FULL PILL PACK.
|
WHEN TO START THE FIRST PACK OF PILLS
|
You have a choice of which day to start taking your first pack of pills. Decide with your doctor or clinic which is the best day for you. Pick a time of day which will be easy to remember.
DAY-1 START:
- 1.
- Pick the day label strip that starts with the first day of your period. (This is the day you start bleeding or spotting, even if it is almost midnight when the bleeding begins.)
- 2.
- Place this day label strip on the tablet blister card over the area that has the days of the week (starting with Sunday) printed on the blister card.

- 3.
- Take the first “active” blue pill of the first pack during the first 24 hours of your period.
- 4.
- You will not need to use a back-up method of birth control, since you are starting the pill at the beginning of your period.
SUNDAY START:
- 1.
- Take the first “active” blue pill of the first pack on the Sunday after your period starts, even if you are still bleeding. If your period begins on Sunday, start the pack that same day.
- 2.
- Use another method of birth control as a back-up method if you have sex anytime from the Sunday you start your first pack until the next Sunday (7 days). Condoms or foam are good back-up methods of birth control.
|
WHAT TO DO DURING THE MONTH
|
- 1.
- TAKE ONE PILL AT THE SAME TIME EVERY DAY UNTIL THE PACK IS EMPTY.
Do not skip pills even if you are spotting or bleeding between monthly periods or feel sick to your stomach (nausea).
Do not skip pills even if you do not have sex very often.
- 2.
- WHEN YOU FINISH A PACK OR SWITCH YOUR BRAND OF PILLS:
Wait 7 days to start the next pack. You will probably have your period during that week. Be sure that no more than 7 days pass between 21-day packs.
|
WHAT TO DO IF YOU MISS PILLS
|
If you MISS 1 blue “active” pill:
- 1.
- Take it as soon as you remember. Take the next pill at your regular time. This means you may take 2 pills in 1 day.
- 2.
- You do not need to use a back-up birth control method if you have sex.
If you MISS 2 blue “active” pills in a row in WEEK 1 OR WEEK 2 of your pack:
- 1.
- Take 2 pills on the day you remember and 2 pills the next day.
- 2.
- Then take 1 pill a day until you finish the pack.
- 3.
- You COULD GET PREGNANT if you have sex in the 7 days after you miss pills. You MUST use another birth control method (such as condoms or foam) as a back-up method of birth control until you have taken a blue “active” pill every day for 7 days.
If you MISS 2 blue “active” pills in a row in THE 3rd WEEK:
- 1.
- If you are a Day-1 Starter:
THROW OUT the rest of the pill pack and start a new pack that same day.
If you are a Sunday Starter:
Keep taking 1 pill every day until Sunday. On Sunday, THROW OUT the rest of the pack and start a new pack of pills that same day.
- 2.
- You may not have your period this month, but this is expected. However, if you miss your period 2 months in a row, call your doctor or clinic because you might be pregnant.
- 3.
- You COULD GET PREGNANT if you have sex in the 7 days after you miss pills. You MUST use another birth control method (such as condoms or foam) as a back-up method of birth control until you have taken a blue “active” pill every day for 7 days.
If you MISS 3 OR MORE blue “active” pills in a row (during the first 3 weeks):
- 1.
- If you are a Day-1 Starter:
THROW OUT the rest of the pill pack and start a new pack that same day.
If you are a Sunday Starter:
Keep taking 1 pill every day until Sunday. On Sunday, THROW OUT the rest of the pack and start a new pack of pills that same day.
- 2.
- You may not have your period this month, but this is expected. However, if you miss your period 2 months in a row, call your doctor or clinic because you might be pregnant.
- 3.
- You COULD GET PREGNANT if you have sex in the 7 days after you miss pills. You MUST use another birth control method (such as condoms or foam) as a back-up method of birth control until you have taken a blue “active” pill every day for 7 days.
|
FINALLY, IF YOU ARE STILL NOT SURE WHAT TO DO ABOUT THE PILLS YOU HAVE MISSED:
|
|
Based on his or her assessment of your medical needs, your doctor or healthcare provider has prescribed this drug for you. Do not give this drug to anyone else. |
Keep this and all drugs out of the reach of children.
Store at 20° to 25°C (68° to 77°F). [See USP Controlled Room Temperature.]
DETAILED PATIENT PACKAGE INSERT
|
Cigarette smoking increases the risk of serious cardiovascular side effects from oral contraceptive use. This risk increases with age and with heavy smoking (15 or more cigarettes per day) and is quite marked in women over 35 years of age. Women who use oral contraceptives are strongly advised not to smoke. |
This product (like all oral contraceptives) is intended to prevent pregnancy. It does not protect against HIV infection (AIDS) and other sexually transmitted infections.
What You Should Know About Oral Contraceptives
Any woman who considers using oral contraceptives (the “birth control pill” or “the pill”) should understand the benefits and risks of using this form of birth control. This leaflet will give you much of the information you will need to make this decision and will also help you determine if you are at risk of developing any of the serious side effects of the pill. It will tell you how to use the pill properly so that it will be as effective as possible. However, this leaflet is not a replacement for a careful discussion between you and your healthcare provider. You should discuss the information provided in this leaflet with him or her, both when you first start taking the pill and during your revisits. You should also follow your healthcare provider's advice with regard to regular check-ups while you are on the pill.
EFFECTIVENESS OF ORAL CONTRACEPTIVES
Oral contraceptives or “birth control pills” or “the pill” are used to prevent pregnancy and are more effective than other non-surgical methods of birth control. When they are taken correctly, the chance of becoming pregnant is less than 1% (1 pregnancy per 100 women per year of use) when used perfectly, without missing any pills. Typical failure rates are actually 3% per year. The chance of becoming pregnant increases with each missed pill during a menstrual cycle.
In comparison, typical failure rates for other methods of birth control during the first year of use are as follows:
|
Implant: < 1% |
Male sterilization: < 1% |
|
Injection: < 1% |
Cervical Cap: 20 to 40% |
|
IUD: < 1 to 2% |
Condom alone (male): 14% |
|
Diaphragm with spermicides: 20% |
Condom alone (female): 21% |
|
Spermicides alone: 26% |
Periodic abstinence: 25% |
|
Vaginal Sponge: 20 to 40% |
Withdrawal: 19% |
|
Female sterilization: < 1% |
No method: 85% |
WHO SHOULD NOT TAKE ORAL CONTRACEPTIVES
|
Cigarette smoking increases the risk of serious cardiovascular side effects from oral contraceptive use. This risk increases with age and with heavy smoking (15 or more cigarettes per day) and is quite marked in women over 35 years of age. Women who use oral contraceptives are strongly advised not to smoke. |
Some women should not use the pill. For example, you should not take the pill if you are pregnant or think you may be pregnant.
You should also not use the pill if you have any of the following conditions:
- •
- A history of heart attack or stroke
- •
- Blood clots in the legs (thrombophlebitis), lungs (pulmonary embolism), or eyes
- •
- A history of blood clots in the deep veins of your legs
- •
- Chest pain (angina pectoris)
- •
- Known or suspected breast cancer or cancer
- •
- Unexplained vaginal bleeding (until a diagnosis is reached by your doctor)
- •
- Yellowing of the whites of the eyes or of the skin (jaundice) during pregnancy or during previous use of the pill
- •
- Liver tumor (benign or cancerous)
- •
- Take any Hepatitis C drug combination containing ombitasvir/paritaprevir/ritonavir, with or without dasabuvir. This may increase levels of the liver enzyme “alanine aminotransferase” (ALT) in the blood.
Tell your healthcare provider if you have ever had any of these conditions. Your healthcare provider can recommend a safer method of birth control.
OTHER CONSIDERATIONS BEFORE TAKING ORAL CONTRACEPTIVES
Tell your healthcare provider if you have:
- •
- Breast nodules, fibrocystic disease of the breast, an abnormal breast x-ray or mammogram
- •
- Diabetes
- •
- Elevated cholesterol or triglycerides
- •
- High blood pressure
- •
- Migraine or other headaches or epilepsy
- •
- Depression
- •
- Gallbladder, heart, or kidney disease
- •
- History of scanty or irregular menstrual periods
Women with any of these conditions should be checked often by their healthcare provider if they choose to use oral contraceptives.
Also, be sure to inform your doctor or healthcare provider if you smoke or are on any medications.
RISKS OF TAKING ORAL CONTRACEPTIVES
- 1.
- Risk of Developing Blood Clots
Blood clots and blockage of blood vessels are the most serious side effects of taking oral contraceptives; in particular, a clot in the legs can cause thrombophlebitis, and a clot that travels to the lungs can cause a sudden blocking of the vessel carrying blood to the lungs. Rarely, clots occur in the blood vessels of the eye and may cause blindness, double vision, or impaired vision.
If you take oral contraceptives and need elective surgery, need to stay in bed for a prolonged illness, or have recently delivered a baby, you may be at risk of developing blood clots. You should consult your doctor about stopping oral contraceptives three to four weeks before surgery and not taking oral contraceptives for two weeks after surgery or during bed rest. You should also not take oral contraceptives soon after delivery of a baby. It is advisable to wait for at least four weeks after delivery if you are not breastfeeding. If you are breastfeeding, you should wait until you have weaned your child before using the pill. (See also the section on Breastfeeding in GENERAL PRECAUTIONS.)
- 2.
- Heart Attacks and Strokes
Oral contraceptives may increase the tendency to develop strokes (stoppage or rupture of blood vessels in the brain) and angina pectoris and heart attacks (blockage of blood vessels in the heart). Any of these conditions can cause death or disability.
Smoking greatly increases the possibility of suffering heart attacks and strokes. Furthermore, smoking and the use of oral contraceptives greatly increase the chances of developing and dying of heart disease.
- 3.
- Gallbladder Disease
Oral contraceptive users probably have a greater risk than nonusers of having gallbladder disease, although this risk may be related to pills containing high doses of estrogens.
- 4.
- Liver Tumors
In rare cases, oral contraceptives can cause benign but dangerous liver tumors. These benign liver tumors can rupture and cause fatal internal bleeding. In addition, a possible but not definite association has been found with the pill and liver cancers in two studies, in which a few women who developed these very rare cancers were found to have used oral contraceptives for long periods. However, liver cancers are extremely rare. The chance of developing liver cancer from using the pill is thus even rarer.
- 5.
- Risk of Cancer
It is not known if hormonal birth control pills cause breast cancer. Some studies, but not all, suggest that there could be a slight increase in the risk of breast cancer among current users with longer duration of use.
If you have breast cancer now, or have had it in the past, do not use hormonal birth control because some breast cancers are sensitive to hormones.
Some studies have found an increase in the incidence of cancer of the cervix in women who use oral contraceptives. However, this finding may be related to factors other than the use of oral contraceptives.
ESTIMATED RISK OF DEATH FROM A BIRTH CONTROL METHOD OR PREGNANCY
All methods of birth control and pregnancy are associated with a risk of developing certain diseases which may lead to disability or death. An estimate of the number of deaths associated with different methods of birth control and pregnancy has been calculated and is shown in the following table.
|
Method of control and |
15-19
|
20-24
|
25-29
|
30-34
|
35-39
|
40-44
|
|
No fertility control methods*
|
7.0 |
7.4 |
9.1 |
14.8 |
25.7 |
28.2 |
|
Oral contraceptives non- |
0.3 |
0.5 |
0.9 |
1.9 |
13.8 |
31.6 |
|
Oral contraceptives smoker†
|
2.2 |
3.4 |
6.6 |
13.5 |
51.1 |
117.2 |
|
IUD†
|
0.8 |
0.8 |
1.0 |
1.0 |
1.4 |
1.4 |
|
Condom*
|
1.1 |
1.6 |
0.7 |
0.2 |
0.3 |
0.4 |
|
Diaphragm/ spermicide*
|
1.9 |
1.2 |
1.2 |
1.3 |
2.2 |
2.8 |
|
Periodic abstinence*
|
2.5 |
1.6 |
1.6 |
1.7 |
2.9 |
3.6 |
In the above table, the risk of death from any birth control method is less than the risk of childbirth, except for oral contraceptive users over the age of 35 who smoke and pill users over the age of 40 even if they do not smoke. It can be seen in the table that for women aged 15 to 39, the risk of death was highest with pregnancy (7-26 deaths per 100,000 women, depending on age). Among pill users who do not smoke, the risk of death was always lower than that associated with pregnancy for any age group, although over the age of 40, the risk increases to 32 deaths per 100,000 women, compared to 28 associated with pregnancy at that age. However, for pill users who smoke and are over the age of 35, the estimated number of deaths exceeds those for other methods of birth control. If a woman is over the age of 40 and smokes, her estimated risk of death is four times higher (117/100,000 women) than the estimated risk associated with pregnancy (28/100,000 women) in that age group.
The suggestion that women over 40 who don't smoke should not take oral contraceptives is based on information from older higher dose pills and on less selective use of pills than is practiced today. An Advisory Committee of the FDA discussed this issue in 1989 and recommended that the benefits of oral contraceptive use by healthy, non-smoking women over 40 years of age may outweigh the possible risks. However, all women, especially older women, are cautioned to use the lowest dose pill that is effective.
WARNING SIGNALS
If any of these adverse effects occur while you are taking oral contraceptives, call your doctor immediately:
- •
- Sharp chest pain, coughing of blood, or sudden shortness of breath (indicating a possible clot in the lung)
- •
- Pain in the calf (indicating a possible clot in the leg)
- •
- Crushing chest pain or heaviness in the chest (indicating a possible heart attack)
- •
- Sudden severe headache or vomiting, dizziness or fainting, disturbances of vision or speech, weakness, or numbness in an arm or leg (indicating a possible stroke)
- •
- Sudden partial or complete loss of vision (indicating a possible clot in the eye)
- •
- Breast lumps (indicating possible breast cancer or fibrocystic disease of the breast; ask your doctor or healthcare provider to show you how to examine your breasts)
- •
- Severe pain or tenderness in the stomach area (indicating a possibly ruptured liver tumor)
- •
- Difficulty in sleeping, weakness, lack of energy, fatigue, or change in mood (possibly indicating severe depression)
- •
- Jaundice or a yellowing of the skin or eyeballs, accompanied frequently by fever, fatigue, loss of appetite, dark colored urine, or light-colored bowel movements (indicating possible liver problems)
SIDE EFFECTS OF ORAL CONTRACEPTIVES
- 1.
- Vaginal Bleeding
Irregular vaginal bleeding or spotting may occur while you are taking the pills. Irregular bleeding may vary from slight staining between menstrual periods to breakthrough bleeding which is a flow much like a regular period. Irregular bleeding occurs most often during the first few months of oral contraceptive use, but may also occur after you have been taking the pill for some time. Such bleeding may be temporary and usually does not indicate serious problems. It is important to continue taking your pills on schedule. If the bleeding occurs in more than one cycle or lasts for more than a few days, talk to your doctor or healthcare provider.
- 2.
- Contact Lenses
If you wear contact lenses and notice a change in vision or an inability to wear your lenses, contact your doctor or healthcare provider.
- 3.
- Fluid Retention
Oral contraceptives may cause edema (fluid retention) with swelling of the fingers or ankles and may raise your blood pressure. If you experience fluid retention, contact your doctor or healthcare provider.
- 4.
- Melasma
A spotty darkening of the skin is possible, particularly of the face.
- 5.
- Other Side Effects
Other side effects may include change in appetite, headache, nervousness, depression, dizziness, loss of scalp hair, rash, and vaginal infections.
If any of these side effects bother you, call your doctor or healthcare provider.
GENERAL PRECAUTIONS
- 1.
- Missed Periods and Use of Oral Contraceptives Before or During Early Pregnancy
There may be times when you may not menstruate regularly after you have completed taking a cycle of pills. If you have taken your pills regularly and miss one menstrual period, continue taking your pills for the next cycle but be sure to inform your healthcare provider before doing so. If you have not taken the pills daily as instructed and missed a menstrual period, or if you missed two consecutive menstrual periods, you may be pregnant. Check with your healthcare provider immediately to determine whether you are pregnant. Do not continue to take oral contraceptives until you are sure you are not pregnant, but continue to use another method of contraception.
There is no conclusive evidence that oral contraceptive use is associated with an increase in birth defects, when taken inadvertently during early pregnancy. Previously, a few studies had reported that oral contraceptives might be associated with birth defects, but these studies have not been confirmed. Nevertheless, oral contraceptives or any other drugs should not be used during pregnancy unless clearly necessary and prescribed by your doctor. You should check with your doctor about risks to your unborn child of any medication taken during pregnancy.
- 2.
- While Breastfeeding
If you are breastfeeding, consult your doctor before starting oral contraceptives. Some of the drug will be passed on to the child in the milk. A few adverse effects on the child have been reported, including yellowing of the skin (jaundice) and breast enlargement. In addition, oral contraceptives may decrease the amount and quality of your milk. If possible, do not use oral contraceptives while breastfeeding. You should use another method of contraception since breastfeeding provides only partial protection from becoming pregnant and this partial protection decreases significantly as you breastfeed for longer periods of time. You should consider starting oral contraceptives only after you have weaned your child completely.
- 3.
- Laboratory Tests
If you are scheduled for any laboratory tests, tell your doctor you are taking birth control pills. Certain blood tests may be affected by birth control pills.
- 4.
- Drug Interactions
Certain drugs may interact with birth control pills to make them less effective in preventing pregnancy or cause an increase in breakthrough bleeding. Such drugs include rifampin; drugs used for epilepsy such as barbiturates (for example, phenobarbital), carbamazepine, and phenytoin (Dilantin® is one brand of this drug); troglitazone; phenylbutazone; and possibly certain antibiotics. You may need to use additional contraception when you take drugs which can make oral contraceptives less effective.
Birth control pills interact with certain drugs. These drugs include acetaminophen, clofibric acid, cyclosporine, morphine, prednisolone, salicylic acid, temazepam, and theophylline. You should tell your doctor if you are taking any of these medications.
- 5.
- This product (like all oral contraceptives) is intended to prevent pregnancy. It does not protect against transmission of HIV (AIDS) and other sexually transmitted infections such as Chlamydia, genital herpes, genital warts, gonorrhea, hepatitis B, and syphilis.
INSTRUCTIONS TO PATIENT
TABLET BLISTER PACK
The norethindrone acetate and ethinyl estradiol tablet blister pack has been designed to make oral contraceptive dosing as easy and as convenient as possible. The tablets are arranged in three rows of seven tablets each, with the days of the week appearing on the tablet blister pack above the first row of tablets.
|
If your TABLET BLISTER PACK contains: |
You are taking: |
|
21 blue tablets |
Norethindrone Acetate and Ethinyl |
Each blue tablet contains 1.5 mg norethindrone acetate and 0.03 mg ethinyl estradiol.
DIRECTIONS
To remove a tablet, press down on it with your thumb or finger. The tablet will drop through the back of the tablet blister. Do not press with your thumbnail, fingernail, or any other sharp object.
HOW TO TAKE THE PILL
|
IMPORTANT POINTS TO REMEMBER
|
BEFORE YOU START TAKING YOUR PILLS:
- 1.
- BE SURE TO READ THESE DIRECTIONS:
Before you start taking your pills.
Anytime you are not sure what to do.
- 2.
- THE RIGHT WAY TO TAKE THE PILL IS TO TAKE ONE PILL EVERY DAY AT THE SAME TIME. If you miss pills you could get pregnant. This includes starting the pack late. The more pills you miss, the more likely you are to get pregnant.
- 3.
- MANY WOMEN HAVE SPOTTING OR LIGHT BLEEDING, OR MAY FEEL SICK TO THEIR STOMACH DURING THE FIRST 1-3 PACKS OF PILLS. If you do have spotting or light bleeding or feel sick to your stomach, do not stop taking the pill. The problem will usually go away. If it doesn't go away, check with your doctor or clinic.
- 4.
- MISSING PILLS CAN ALSO CAUSE SPOTTING OR LIGHT BLEEDING, even when you make up these missed pills. On the days you take 2 pills to make up for missed pills, you could also feel a little sick to your stomach.
- 5.
- IF YOU HAVE VOMITING OR DIARRHEA, for any reason, or IF YOU TAKE SOME MEDICINES, including some antibiotics, your birth control pills may not work as well. Use a back-up birth control method (such as condoms or foam) until you check with your doctor or clinic.
- 6.
- IF YOU HAVE TROUBLE REMEMBERING TO TAKE THE PILL, talk to your doctor or clinic about how to make pill-taking easier or about using another method of birth control.
- 7.
- IF YOU HAVE ANY QUESTIONS OR ARE UNSURE ABOUT THE INFORMATION IN THIS LEAFLET, call your doctor or clinic.
|
BEFORE YOU START TAKING YOUR PILLS
|
- 1.
- DECIDE WHAT TIME OF DAY YOU WANT TO TAKE YOUR PILL. It is important to take it at about the same time every day.
- 2.
- LOOK AT YOUR PILL PACK TO SEE IF IT HAS 21 PILLS:
The 21-Day pill pack has 21 “active” blue pills (with hormones) to take for 3 weeks, followed by 1 week without pills.
- 3.
- ALSO FIND:
- 1)
- where on the pack to start taking pills,
- 2)
- in what order to take the pills (follow the arrows), and
- 3)
- the week numbers as shown in the following picture:
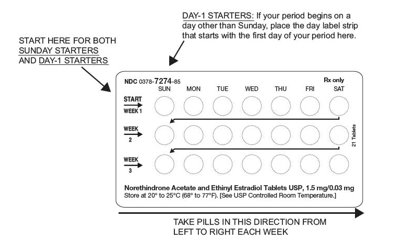
Norethindrone Acetate and Ethinyl Estradiol Tablets, 1.5 mg/0.03 mg will contain: ALL BLUE PILLS.
- 4.
- BE SURE YOU HAVE READY AT ALL TIMES:
ANOTHER KIND OF BIRTH CONTROL (such as condoms or foam) to use as a back-up in case you miss pills.
AN EXTRA, FULL PILL PACK.
|
WHEN TO START THE FIRST PACK OF PILLS
|
You have a choice of which day to start taking your first pack of pills. Decide with your doctor or clinic which is the best day for you. Pick a time of day which will be easy to remember.
DAY-1 START:
- 1.
- Pick the day label strip that starts with the first day of your period. (This is the day you start bleeding or spotting, even if it is almost midnight when the bleeding begins.)
- 2.
- Place this day label strip on the tablet blister card over the area that has the days of the week (starting with Sunday) printed on the blister card.
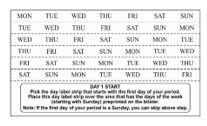
- 3.
- Take the first “active” blue pill of the first pack during the first 24 hours of your period.
- 4.
- You will not need to use a back-up method of birth control, since you are starting the pill at the beginning of your period.
SUNDAY START:
- 1.
- Take the first “active” blue pill of the first pack on the Sunday after your period starts, even if you are still bleeding. If your period begins on Sunday, start the pack that same day.
- 2.
- Use another method of birth control as a back-up method if you have sex anytime from the Sunday you start your first pack until the next Sunday (7 days). Condoms or foam are good back-up methods of birth control.
|
WHAT TO DO DURING THE MONTH
|
- 1.
- TAKE ONE PILL AT THE SAME TIME EVERY DAY UNTIL THE PACK IS EMPTY.
Do not skip pills even if you are spotting or bleeding between monthly periods or feel sick to your stomach (nausea).
Do not skip pills even if you do not have sex very often.
- 2.
- WHEN YOU FINISH A PACK OR SWITCH YOUR BRAND OF PILLS:
Wait 7 days to start the next pack. You will probably have your period during that week. Be sure that no more than 7 days pass between 21-day packs.
|
WHAT TO DO IF YOU MISS PILLS
|
If you MISS 1 blue “active” pill:
- 1.
- Take it as soon as you remember. Take the next pill at your regular time. This means you may take 2 pills in 1 day.
- 2.
- You do not need to use a back-up birth control method if you have sex.
If you MISS 2 blue “active” pills in a row in WEEK 1 OR WEEK 2 of your pack:
- 1.
- Take 2 pills on the day you remember and 2 pills the next day.
- 2.
- Then take 1 pill a day until you finish the pack.
- 3.
- You COULD GET PREGNANT if you have sex in the 7 days after you miss pills. You MUST use another birth control method (such as condoms or foam) as a back-up method of birth control until you have taken a blue “active” pill every day for 7 days.
If you MISS 2 blue “active” pills in a row in THE 3rd WEEK:
- 1.
- If you are a Day-1 Starter:
THROW OUT the rest of the pill pack and start a new pack that same day.
If you are a Sunday Starter:
Keep taking 1 pill every day until Sunday. On Sunday, THROW OUT the rest of the pack and start a new pack of pills that same day.
- 2.
- You may not have your period this month, but this is expected. However, if you miss your period 2 months in a row, call your doctor or clinic because you might be pregnant.
- 3.
- You COULD GET PREGNANT if you have sex in the 7 days after you miss pills. You MUST use another birth control method (such as condoms or foam) as a back-up method of birth control until you have taken a blue “active” pill every day for 7 days.
If you MISS 3 OR MORE blue “active” pills in a row (during the first 3 weeks):
- 1.
- If you are a Day-1 Starter:
THROW OUT the rest of the pill pack and start a new pack that same day.
If you are a Sunday Starter:
Keep taking 1 pill every day until Sunday. On Sunday, THROW OUT the rest of the pack and start a new pack of pills that same day.
- 2.
- You may not have your period this month, but this is expected. However, if you miss your period 2 months in a row, call your doctor or clinic because you might be pregnant.
- 3.
- You COULD GET PREGNANT if you have sex in the 7 days after you miss pills. You MUST use another birth control method (such as condoms or foam) as a back-up method of birth control until you have taken a blue “active” pill every day for 7 days.
|
FINALLY, IF YOU ARE STILL NOT SURE WHAT TO DO ABOUT THE PILLS YOU HAVE MISSED:
|
PREGNANCY DUE TO PILL FAILURE
The incidence of pill failure resulting in pregnancy is approximately 1% (i.e., one pregnancy per 100 women per year) if taken every day as directed, but more typical failure rates are about 3%. If failure does occur, the risk to the fetus is minimal.
PREGNANCY AFTER STOPPING THE PILL
There may be some delay in becoming pregnant after you stop using oral contraceptives, especially if you had irregular menstrual cycles before you used oral contraceptives. It may be advisable to postpone conception until you begin menstruating regularly once you have stopped taking the pill and desire pregnancy.
There does not appear to be any increase in birth defects in newborn babies when pregnancy occurs soon after stopping the pill.
OVERDOSAGE
Serious ill effects have not been reported following ingestion of large doses of oral contraceptives by young children. Overdosage may cause nausea and withdrawal bleeding in females. In case of overdosage, contact your healthcare provider or pharmacist.
OTHER INFORMATION
Your healthcare provider will take a medical and family history and examine you before prescribing oral contraceptives. The physical examination may be delayed to another time if you request it and your healthcare provider believes that it is a good medical practice to postpone it. You should be reexamined at least once a year. Be sure to inform your healthcare provider if there is a family history of any of the conditions listed previously in this leaflet. Be sure to keep all appointments with your healthcare provider, because this is a time to determine if there are early signs of side effects of oral contraceptive use.
Do not use the drug for any condition other than the one for which it was prescribed. This drug has been prescribed specifically for you; do not give it to others who may want birth control pills.
HEALTH BENEFITS FROM ORAL CONTRACEPTIVES
In addition to preventing pregnancy, use of oral contraceptives may provide certain benefits. They are:
- •
- Menstrual cycles may become more regular
- •
- Blood flow during menstruation may be lighter and less iron may be lost. Therefore, anemia due to iron deficiency is less likely to occur
- •
- Pain or other symptoms during menstruation may be encountered less frequently
- •
- Ectopic (tubal) pregnancy may occur less frequently
- •
- Noncancerous cysts or lumps in the breast may occur less frequently
- •
- Acute pelvic inflammatory disease may occur less frequently
- •
- Oral contraceptive use may provide some protection against developing two forms of cancer: cancer of the ovaries and cancer of the lining of the uterus.
If you want more information about birth control pills, ask your doctor or pharmacist. They have a more technical leaflet called the “Physician Insert”, which you may wish to read.
Remembering to take tablets according to schedule is stressed because of its importance in providing you the greatest degree of protection.
MISSED MENSTRUAL PERIODS FOR BOTH DOSAGE REGIMENS
At times there may be no menstrual period after a cycle of pills. Therefore, if you miss one menstrual period but have taken the pills exactly as you were supposed to, continue as usual into the next cycle. If you have not taken the pills correctly and miss a menstrual period, you may be pregnant and should stop taking oral contraceptives until your doctor or healthcare provider determines whether or not you are pregnant. Until you can get to your doctor or healthcare provider, use another form of contraception. If two consecutive menstrual periods are missed, you should stop taking pills until it is determined whether or not you are pregnant. Although there does not appear to be any increase in birth defects in newborn babies if you become pregnant while using oral contraceptives, you should discuss the situation with your doctor or healthcare provider.
Periodic Examination
Your doctor or healthcare provider will take a complete medical and family history before prescribing oral contraceptives. At that time and about once a year thereafter, he or she will generally examine your blood pressure, breasts, abdomen, and pelvic organs (including a Papanicolaou smear, i.e., test for cancer).
Keep this and all drugs out of the reach of children.
Store at 20° to 25°C (68° to 77°F). [See USP Controlled Room Temperature.]
Manufactured for:
Mylan Pharmaceuticals Inc.
Morgantown, WV 26505 U.S.A.
Manufactured by:
Mylan Laboratories Limited, India
Ahmedabad - 382 213, India
Code No.: GUJ-DRUGS/G/28/1297
75101205
Revised: 1/2024
FC:OT:7274:R7
PRINCIPAL DISPLAY PANEL - 1.5 mg/0.03 mg
NDC 0378-7274-53
Rx only
Norethindrone Acetate and
Ethinyl Estradiol Tablets, USP
1.5 mg/0.03 mg
This product (like all oral contraceptives) is intended to prevent pregnancy. It does not protect against HIV infection (AIDS) and other sexually transmitted diseases.
3 pouches, each contains one blister pack of 21 tablets
Each blue tablet contains norethindrone acetate 1.5 mg and ethinyl estradiol 0.03 mg.
Each blister pack contains 21 blue tablets.
DOSAGE: One tablet daily as prescribed. See prescribing information.
IMPORTANT: The “Patient Instructions” which are packaged inside each pouch provides important instructions to the patient. Please supply these instructions and the carrier sleeve to the patient when dispensing.
Store at 20° to 25°C (68° to 77°F). [See USP Controlled Room Temperature.]
Keep this and all medications out of the reach of children.
Manufactured for:
Mylan Pharmaceuticals Inc.
Morgantown, WV 26505 U.S.A.
Made in India
Code No.: GUJ-DRUGS/G/28/1297
Mylan.com
FC:7274:3C:R4