FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
1.1 Indication
Fluocinonide cream USP, 0.1% is indicated for the relief of the inflammatory and pruritic manifestations of corticosteroid responsive dermatoses in patients 12 years of age or older [see Use in Specific Populations (8.4)].
1.2 Limitation of Use
Treatment beyond 2 consecutive weeks is not recommended and the total dosage should not exceed 60 g per week because the safety of fluocinonide cream for longer than 2 weeks has not been established and because of the potential for the drug to suppress the hypothalamic-pituitary-adrenal (HPA) axis. Therapy should be discontinued when control of the disease is achieved. If no improvement is seen within 2 weeks, reassessment of the diagnosis may be necessary. Do not use more than half of the 120 g tube per week.
Fluocinonide cream should not be used in the treatment of rosacea or perioral dermatitis, and should not be used on the face, groin, or axillae.
2 DOSAGE AND ADMINISTRATION
For topical use only. Fluocinonide cream is not for ophthalmic, oral, or intravaginal use.
For psoriasis, apply a thin layer of fluocinonide cream once or twice daily to the affected skin areas as directed by a physician. Twice daily application for the treatment of psoriasis has been shown to be more effective in achieving treatment success during 2 weeks of treatment.
For atopic dermatitis, apply a thin layer of fluocinonide cream once daily to the affected skin areas as directed by a physician. Once daily application for the treatment of atopic dermatitis has been shown to be as effective as twice daily treatment in achieving treatment success during 2 weeks of treatment [see Clinical Studies (14)].
For corticosteroid responsive dermatoses, other than psoriasis or atopic dermatitis, apply a thin layer of fluocinonide cream once or twice daily to the affected areas as directed by a physician.
5 WARNINGS AND PRECAUTIONS
5.1 Effect on Endocrine System
Systemic absorption of topical corticosteroids, including fluocinonide cream, can produce reversible hypothalamic-pituitary-adrenal (HPA) axis suppression with the potential for clinical glucocorticosteroid insufficiency. This may occur during treatment or upon withdrawal of the topical corticosteroid. In addition, the use of fluocinonide cream for longer than 2 weeks may suppress the immune system [see Nonclinical Toxicology (13.1)].
HPA axis suppression has been observed with fluocinonide cream, 0.1% applied once or twice daily in 2 out of 18 adult patients with plaque-type psoriasis, 1 out of 31 adult patients with atopic dermatitis and 4 out of 123 pediatric patients with atopic dermatitis [see Use in Specific Population (8.4) and Clinical Pharmacology (12.2)].
Because of the potential for systemic absorption, use of topical corticosteroids, including fluocinonide cream, may require that patients be periodically evaluated for HPA axis suppression. Factors that predispose a patient using a topical corticosteroid to HPA axis suppression include the use of more potent steroids, use over large surface areas, use over prolonged periods, use under occlusion, use on an altered skin barrier, and use in patients with liver failure.
An ACTH stimulation test may be helpful in evaluating patients for HPA axis suppression. If HPA axis suppression is documented, an attempt should be made to gradually withdraw the drug, to reduce the frequency of application, or to substitute a less potent steroid. Manifestations of adrenal insufficiency may require supplemental systemic corticosteroids. Recovery of HPA axis function is generally prompt and complete upon discontinuation of topical corticosteroids.
Cushing's syndrome, hyperglycemia, and unmasking of latent diabetes mellitus can also result from systemic absorption of topical corticosteroids.
Use of more than one corticosteroid-containing product at the same time may increase the total systemic absorption of topical corticosteroids.
Studies conducted in pediatric patients demonstrated reversible HPA axis suppression after use of fluocinonide cream. Pediatric patients may be more susceptible than adults to systemic toxicity from equivalent doses of fluocinonide cream due to their larger skin surface-to-body-mass ratios [See Use in Specific Populations (8.4)].
5.2 Local Adverse Reactions with Topical Corticosteroids
Local adverse reactions may be more likely to occur with occlusive use, prolonged use or use of higher potency corticosteroids. Reactions may include atrophy, striae, telangiectasis, burning, itching, irritation, dryness, folliculitis, acneiform eruptions, hypopigmentation, perioral dermatitis, allergic contact dermatitis, secondary infection, and miliaria. Some local adverse reactions may be irreversible.
5.3 Concomitant Skin Infections
If concomitant skin infections are present or develop, an appropriate antifungal or antibacterial agent should be used. If a favorable response does not occur promptly, use of fluocinonide cream should be discontinued until the infection has been adequately controlled.
5.4 Allergic Contact Dermatitis
If irritation develops, fluocinonide cream should be discontinued and appropriate therapy instituted. Allergic contact dermatitis with corticosteroids is usually diagnosed by observing failure to heal rather than noting a clinical exacerbation as with most topical products not containing corticosteroids.
Such an observation should be corroborated with appropriate diagnostic patch testing.
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
Because clinical studies are conducted under widely varying conditions, adverse reaction rates observed in the clinical studies of a drug cannot be directly compared to rates in the clinical studies of another drug and may not reflect the rates observed in practice.
In clinical trials, a total of 443 adult subjects with atopic dermatitis or plaque-type psoriasis were treated once daily or twice daily with fluocinonide cream for 2 weeks. The most commonly observed adverse reactions in these clinical trials were as follows:
| Adverse
Reaction | Fluocinonide Cream,
once daily (n=216) | Fluocinonide Cream,
twice daily (n=227) | Vehicle Cream,
once or twice daily (n=211) |
| Headache | 8 (3.7%) | 9 (4.0%) | 6 (2.8%) |
| Application Site Burning | 5 (2.3%) | 4 (1.8%) | 14 (6.6%) |
| Nasopharyngitis | 2 (0.9%) | 3 (1.3%) | 3 (1.4%) |
| Nasal Congestion | 3 (1.4%) | 1 (0.4%) | 0 |
Safety in patients 12 to 17 years of age was similar to that observed in adults.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post approval use of fluocinonide cream:
Administration Site Conditions: discoloration, erythema, irritation, pruritus, swelling, pain and condition aggravated.
Immune System Disorders: hypersensitivity.
Nervous System Disorders: headache and dizziness.
Skin and Subcutaneous Tissue Disorders: acne, dry skin, rash, skin exfoliation and skin tightness.
Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Category C
There are no adequate and well-controlled studies in pregnant women. Therefore, fluocinonide cream should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Corticosteroids have been shown to be teratogenic in laboratory animals when administered systemically at relatively low dosage levels. Some corticosteroids have been shown to be teratogenic after dermal application in laboratory animals.
8.3 Nursing Mothers
Systemically administered corticosteroids appear in human milk and could suppress growth, interfere with endogenous corticosteroid production, or cause other untoward effects. It is not known whether topical administration of corticosteroids could result in sufficient systemic absorption to produce detectable quantities in breast milk. Nevertheless, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
8.4 Pediatric Use
Safety and efficacy of fluocinonide cream in pediatric patients younger than 12 years of age have not been established; therefore use in pediatric patients younger than 12 years of age is not recommended.
HPA axis suppression was studied in 4 sequential cohorts of pediatric patients with atopic dermatitis covering at least 20% of the body surface area, treated once daily or twice daily with fluocinonide cream. The first cohort of 31 patients (mean 36.3% BSA) 12 to < 18 years old; the second cohort included 31 patients (mean 39.0% BSA) 6 to < 12 years old; the third cohort included 30 patients (mean 34.6% BSA) 2 to < 6 years old; the fourth cohort included 31 patients (mean 40.0% BSA) 3 months to < 2 years old. Fluocinonide cream caused HPA-axis suppression in 1 patient in the twice daily group in Cohort 1, 2 patients in the twice daily group in Cohort 2, and 1 patient in the twice daily group in Cohort 3. Follow-up testing 14 days after treatment discontinuation, available for all 4 suppressed patients, demonstrated a normally responsive HPA axis. Signs of skin atrophy were present at baseline and severity was not determined making it difficult to assess local skin safety. Therefore, the safety of fluocinonide cream in patients younger than 12 years of age has not been demonstrated [see Warnings and Precautions (5.2)].
HPA axis suppression has not been evaluated in patients with psoriasis who are less than 18 years of age.
Because of a higher ratio of skin surface area to body mass, pediatric patients are at a greater risk than adults of HPA-axis suppression and Cushing's syndrome when they are treated with topical corticosteroids. They are therefore also at greater risk of adrenal insufficiency during or after withdrawal of treatment. Adverse effects including striae have been reported with inappropriate use of topical corticosteroids in infants and children.
HPA-axis suppression, Cushing's syndrome, linear growth retardation, delayed weight gain, and intracranial hypertension have been reported in children receiving topical corticosteroids. Manifestations of adrenal suppression in children include low plasma cortisol levels and absence of response to cosyntropin (ACTH1-24) stimulation. Manifestations of intracranial hypertension include bulging fontanelles, headaches, and bilateral papilledema.
10 OVERDOSAGE
Topically applied fluocinonide cream can be absorbed in sufficient amounts to produce systemic effects [see Warnings and Precautions (5.1)].
11 DESCRIPTION
Fluocinonide cream USP, 0.1% contains fluocinonide, a synthetic corticosteroid for topical dermatologic use. The corticosteroids constitute a class of primarily synthetic steroids used topically as anti-inflammatory and antipruritic agents. Fluocinonide has the chemical name 6 alpha, 9 alpha- difluoro-11 beta, 21-dihydroxy-16 alpha, 17 alpha- isopropylidenedioxypregna-1, 4-diene-3, 20-dione 21-acetate. Its chemical formula is C26H32F2O7 and it has a molecular weight of 494.58.
It has the following chemical structure:
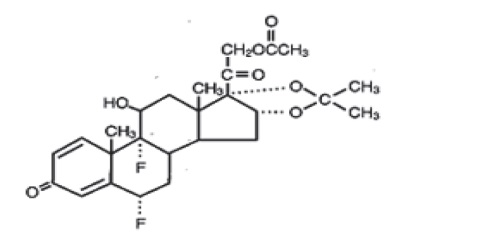
Fluocinonide, USP is white or almost white microcrystalline powder. It is practically insoluble in water, very slightly soluble in ether, slightly soluble in ethanol, methanol and dioxane, sparingly soluble in acetone and chloroform.
Each gram of fluocinonide cream, USP contains 1 mg micronized fluocinonide in a cream base of anhydrous citric acid, carbomer homopolymer type C, diethylene glycol monoethyl ether, diisopropanolamine, glyceryl monostearate, glyceryl stearate/PEG-100 stearate, propylene glycol and purified water.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Corticosteroids play a role in cellular signaling, immune function, inflammation, and protein regulation; however, the precise mechanism of action of fluocinonide cream in corticosteroid responsive dermatoses is unknown.
12.2 Pharmacodynamics
Vasoconstrictor studies performed with fluocinonide cream in healthy subjects indicate that it is in the super-high range of potency as compared with other topical corticosteroids; however, similar blanching scores do not necessarily imply therapeutic equivalence.
Application of fluocinonide cream twice daily for 14 days in 18 adult subjects with plaque-type psoriasis (10 to 50% BSA, mean 19.6% BSA) and 31 adult subjects (17 treated once daily; 14 treated twice daily) with atopic dermatitis (2 o 10% BSA, mean 5% BSA) showed demonstrable HPA-axis suppression in 2 subjects with psoriasis (with 12% and 25% BSA) and 1 subject with atopic dermatitis (treated once daily, 4% BSA) where the criterion for HPA-axis suppression is a serum cortisol level of less than or equal to 18 micrograms per deciliter 30 minutes after stimulation with cosyntropin (ACTH1-24) [see Warnings and Precautions (5.1)].
HPA-axis suppression following application of fluocinonide cream, 0.1% (once or twice daily) was also evaluated in 123 pediatric patients from 3 months to < 18 years of age with atopic dermatitis (mean BSA range 34.6 % to 40.0 %). HPA-axis suppression was observed in 4 patients in the twice daily groups. Follow-up testing 14 days after treatment discontinuation demonstrated a normally responsive HPA axis in all 4 suppressed patients [see Warnings and Precautions (5.1) and Use in Specific populations (8.4)].
12.3 Pharmacokinetics
The extent of percutaneous absorption of topical corticosteroids is determined by many factors including the vehicle and the integrity of the epidermal barrier. Topical corticosteroids can be absorbed from normal intact skin. Inflammation and/or other disease processes in the skin may increase percutaneous absorption.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term animal studies have not been performed to evaluate the carcinogenic potential of fluocinonide cream because of severe immunosuppression induced in a 13-week dermal rat study. The effects of fluocinonide on fertility have not been evaluated.
Fluocinonide revealed no evidence of mutagenic or clastogenic potential based on the results of two in vitro genotoxicity tests (Ames test and chromosomal aberration assay using human lymphocytes). However, fluocinonide was positive for clastogenic potential when tested in the in vivo mouse micronucleus assay.
Topical (dermal) application of 0.0003%-0.03% fluocinonide cream to rats once daily for 13 weeks resulted in a toxicity profile generally associated with long term exposure to corticosteroids including decreased skin thickness, adrenal atrophy, and severe immunosuppression. A NOAEL could not be determined in this study. In addition, topical (dermal) application of 0.1% fluocinonide cream plus UVR exposure to hairless mice for 13 weeks and 150-900 mg/kg/day of 0.1% fluocinonide cream to minipigs (a model which more closely approximates human skin) for 13 weeks produced glucocorticoid-related suppression of the HPA axis, with some signs of immunosuppression noted in the dermal minipig study. Although the clinical relevance of the findings in animals to humans is not clear, sustained glucocorticoid-related immune suppression may increase the risk of infection and possibly the risk for carcinogenesis.
Topical doses of 0% (fluocinonide cream vehicle), 0.0001%, 0.005% and 0.001% fluocinonide cream were evaluated in a 52 week dermal photo- carcinogenicity study (40 weeks of treatment followed by 12 weeks of observation) conducted in hairless albino mice with concurrent exposure to low level ultraviolet radiation. Topical treatment with increasing concentrations of fluocinonide cream did not have an adverse effect in this study. The results of this study suggest that topical treatment with fluocinonide cream would not enhance photo-carcinogenesis.
14 CLINICAL STUDIES
Two adequate and well-controlled efficacy and safety studies of fluocinonide cream have been completed, one in adult subjects with plaque-type psoriasis (Table 2), and one in adult subjects with atopic dermatitis (Table 3). In each of these studies, subjects with between 2% and 10% body surface area involvement at baseline treated all affected areas either once daily or twice daily with fluocinonide cream for 14 consecutive days. The primary measure of efficacy was the proportion of subjects whose condition was cleared or almost cleared at the end of treatment. The results of these studies are presented in the tables below as percent and number of patients achieving treatment success at Week 2.
|
*Cleared or almost cleared |
||||
|
| Fluocinonide Cream, once daily
(n=107) | Vehicle, once daily
(n=54) | Fluocinonide Cream, twice daily
(n=107) | Vehicle, twice daily
(n=55) |
| Subjects cleared | 0 (0) | 0 (0) | 6 (6%) | 0 (0) |
| Subjects achieving treatment success* | 19 (18%) | 4 (7%) | 33 (31%) | 3 (5%) |
|
*Cleared or almost cleared |
||||
|
| Fluocinonide Cream, once daily
(n=109) | Vehicle, once daily
(n=50) | Fluocinonide Cream, twice daily
(n=102) | Vehicle, twice daily
(n=52) |
| Subjects cleared | 11 (10%) | 0 (0) | 17 (17%) | 0 (0) |
| Subjects achieving treatment success* | 64 (59%) | 6 (12%) | 58 (57%) | 10 (19%) |
No efficacy studies have been conducted to compare fluocinonide cream, 0.1% with any other topical corticosteroid product, including fluocinonide cream 0.05%.
16 HOW SUPPLIED/STORAGE AND HANDLING
Fluocinonide Cream USP, 0.1% is white to off white cream, free from lumps and foreign matter with no phase separation. Filled in aluminum tube fitted with white color cap and supplied as follows:
NDC 72578-087-06 in tube of 30 g
NDC 72578-087-02 in tube of 60 g
NDC 72578-087-07 in tube of 120 g
Store at controlled room temperature: 15o to 30oC (59o to 86oF). Keep the tube tightly closed.
17 PATIENT COUNSELING INFORMATION
[See FDA-approved patient labeling (Patient Information)]
Patients using fluocinonide cream should receive the following information and instructions. This information is intended to aid in the safe and effective use of this medication. It is not a disclosure of all possible adverse or unintended effects:
- Fluocinonide cream is to be used as directed by the physician. It is for external use only. Avoid contact with the eyes. It should not be used on the face, groin, and underarms.
- Fluocinonide cream should not be used for any disorder other than that for which it was prescribed.
- The treated skin area should not be bandaged or otherwise covered or wrapped, so as to be occlusive unless directed by the physician.
- Patients should report to their physician any signs of local adverse reactions.
- Other corticosteroid-containing products should not be used with fluocinonide cream without first talking to the physician.
- As with other corticosteroids, therapy should be discontinued when control is achieved. If no improvement is seen in 2 weeks, the patient should be instructed to contact a physician. The safety of the use of fluocinonide cream for longer than 2 weeks has not been established.
- Patients should be informed to not use more than 60 g per week of fluocinonide cream. Do not use more than half of the 120 g tube per week.
- Patients should inform their physicians that they are using fluocinonide cream if surgery is contemplated.
- Patients should wash their hands after applying medication.
Zydus Lifesciences Ltd.
Changodar, Ahmedabad, India.
Distributed by:
Viona Pharmaceuticals Inc.
Cranford, NJ 07016
Rev.: 08/22
Fluocinonide
(floo" oh sin' oh nide)
Cream USP, 0.1%
| Important: For skin use only. Do not get fluocinonide cream in your eyes, mouth, or vagina. Not for use on the face, groin, or underarms. |
|
Read the Patient Information that comes with fluocinonide cream before you start using it and each time you get a refill. There may be new information. This leaflet does not take the place of talking to your doctor about your condition or treatment.
What is fluocinonide cream?
Fluocinonide cream is a prescription corticosteroid medicine used on the skin (topical) to treat adults and children 12 years and older with certain skin conditions that cause red, flaky, and itchy skin.
- You should not use fluocinonide cream for longer than 2 weeks in a row.
- You should not use more than 60 grams of fluocinonide cream or more than half of the 120 gram tube in 1 week.
- Fluocinonide cream should not be used:
- if you have skin swelling or redness on the nose of face (rosacea)
- for a scaly or bumpy rash around your mouth (perioral dermatitis)
- on your face, underarms, or groin area
It is not known if fluocinonide cream is safe and effective in children under 12 years of age.
What should I tell my doctor before using fluocinonide cream?
Before using fluocinonide cream, tell your doctor if you:
- have had irritation or other skin reaction to a steroid medicine in the past
- adrenal gland problems
- plan to have surgery
- are pregnant or plan to become pregnant. It is not known if fluocinonide cream will harm your unborn baby. Talk to your doctor if you are pregnant or plan to become pregnant.
- are breast-feeding or plan to breastfeed. It is not known if fluocinonide cream passes into your breast milk. Talk to your doctor about the best way to feed your baby if you use fluocinonide cream.
Tell your doctor about all the medicine you take including prescriptions and non-prescriptions medicines, vitamins, and herbal supplements. Especially tell your doctor if you take a corticosteroid medicine by mouth or use other products on your skin that contain corticosteroids. Ask your doctor or pharmacist if you are not sure.
Know the medicines you take. Keep a list of your medicines with you to show your doctor and pharmacist when you get a new medicine.
How should I use fluocinonide cream?
- See"Whatisfluocinonidecream?"
- Use fluocinonide cream exactly as your doctor tells you.
- This medicine is for use on the skin only. Do not use fluocinonide cream in your eyes, mouth or vagina.
- Wash your hands after you use fluocinonide cream.
- Do not use fluocinonide cream for longer than 2weeks in a row.
- Talk to your doctor if your skin does not get better after 2 weeks of treatment with fluocinonide cream.
- Do not bandage or cover the skin treated with fluocinonide cream unless your doctor tells you to.
What are the possible side effects with fluocinonide cream?
Fluocinonide cream may cause side effects, including:
- Symptomsofadisorderwheretheadrenalglanddoesnotmakeenoughofcertainhormones(adrenalinsufficiency)duringtreatmentorafterstoppingtreatment. Your doctor may do blood tests to check you for adrenal insufficiency while you are using fluocinonide cream. Tell your doctor if you have any of these symptoms of adrenal insufficiency:
- tiredness that worsens and does not go away
- nausea or vomiting
- dizziness or fainting
- muscle weakness
- irritability and depression
- loss of appetite
- weight loss
- Cushing'ssyndrome , whenthebodyisexposedtotoomuchofthehormonecortisol. Your doctor may do tests to check for this. Symptoms can include:
- weight gain, especially around your upper back and midsection
- slow healing of cuts, insect bites and infections
- tiredness and muscle weakness
- depression, anxiety and irritability
- roundness of your face (moon face)
- new or worsening high blood pressure
The most common side effect of fluocinonide cream is burning of your skin treated with fluocinonide cream.
Talk to your doctor about any side effect that bothers you or that does not go away.
These are not all the side effects with fluocinonide cream. Ask your doctor or pharmacist for more information.
Call your doctor for medical advice about side effects. You may report side effects to Viona Pharmaceuticals Inc. at 1-888-304-5011 or FDA at 1-800-FDA-1088.
How should I store fluocinonide cream?
- Store fluocinonide cream at room temperature, between 59°F to 86°F (15°C to 30°C).
- Keep the tube tightly closed.
Keep fluocinonide cream and all medicines out of the reach of children.
General information about fluocinonide cream
Medicines are sometimes prescribed for purposes other than those listed in the Patient Information leaflet. Do not use fluocinonide cream for a condition for which it was not prescribed. Do not give fluocinonide cream to other people, even if they have the same symptoms you have. It may harm them.
This Patient Information leaflet summarizes the most important information about fluocinonide cream. If you would like more information, talk with your doctor. You can also ask your pharmacist or doctor for information about fluocinonide cream that is written for healthcare professionals.
What are the ingredients in fluocinonide cream?
Active ingredient: fluocinonide, USP
Inactive ingredients: anhydrous citric acid, carbomer homopolymer type C, diethylene glycol monoethyl ether, diisopropanolamine, glyceryl monostearate, glyceryl stearate/PEG-100 stearate, propylene glycol and purified water.
This Patient Information has been approved by the U.S. Food and Drug Administration.