FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
Oxcarbazepine tablets are indicated for use as monotherapy or adjunctive therapy in the treatment of partial-onset seizures in adults and as monotherapy in the treatment of partial-onset seizures in pediatric patients aged 4 years and above and as adjunctive therapy in pediatric patients aged 2 years and above with partial-onset seizures.
2 DOSAGE AND ADMINISTRATION
2.1 Adjunctive Therapy for Adults
Initiate oxcarbazepine tablets with a dose of 600 mg/day, given twice-a-day. If clinically indicated, the dose may be increased by a maximum of 600 mg/day at approximately weekly intervals; the maximum recommended daily dose is 1200 mg/day. Daily doses above 1200 mg/day show somewhat greater effectiveness in controlled trials, but most patients were not able to tolerate the 2400 mg/day dose, primarily because of CNS effects.
Dosage adjustment is recommended with concomitant use of strong CYP3A4 enzyme inducers or UGT inducers, which include certain antiepileptic drugs (AEDs) [see Drug Interactions (7.1, 7.2)].
2.2 Conversion to Monotherapy for Adults
Patients receiving concomitant AEDs may be converted to monotherapy by initiating treatment with oxcarbazepine tablets at 600 mg/day (given in a twice-a-day regimen) while simultaneously initiating the reduction of the dose of the concomitant AEDs. The concomitant AEDs should be completely withdrawn over 3 to 6 weeks, while the maximum dose of oxcarbazepine tablets should be reached in about 2 to 4 weeks. Oxcarbazepine tablets may be increased as clinically indicated by a maximum increment of 600 mg/day at approximately weekly intervals to achieve the maximum recommended daily dose of 2400 mg/day. A daily dose of 1200 mg/day has been shown in one study to be effective in patients in whom monotherapy has been initiated with oxcarbazepine tablets. Patients should be observed closely during this transition phase.
2.3 Initiation of Monotherapy for Adults
Patients not currently being treated with AEDs may have monotherapy initiated with oxcarbazepine tablets. In these patients, initiate oxcarbazepine tablets at a dose of 600 mg/day (given a twice-a-day); the dose should be increased by 300 mg/day every third day to a dose of 1200 mg/day. Controlled trials in these patients examined the effectiveness of a 1200 mg/day dose; a dose of 2400 mg/day has been shown to be effective in patients converted from other AEDs to oxcarbazepine tablets monotherapy (see above).
2.4 Adjunctive Therapy for Pediatric Patients (Aged 2 to 16 Years)
In pediatric patients aged 4 to 16 years, initiate oxcarbazepine tablets at a daily dose of 8 to 10 mg/kg generally not to exceed 600 mg/day, given twice-a-day. The target maintenance dose of oxcarbazepine tablets should be achieved over 2 weeks, and is dependent upon patient weight, according to the following chart:
- 20 to 29 kg – 900 mg/day
- 29.1 to 39 kg – 1200 mg/day
- >39 kg – 1800 mg/day
In the clinical trial, in which the intention was to reach these target doses, the median daily dose was 31 mg/kg with a range of 6 to 51 mg/kg.
In pediatric patients aged 2 to <4 years, initiate oxcarbazepine tablets at a daily dose of 8 to 10 mg/kg generally not to exceed 600 mg/day, given twice-a-day. For patients less than 20 kg, a starting dose of 16 to 20 mg/kg may be considered [see Clinical Pharmacology (12.3)]. The maximum maintenance dose of oxcarbazepine tablets should be achieved over 2 to 4 weeks and should not exceed 60 mg/kg/day in a twice-a-day regimen.
In the clinical trial in pediatric patients (2 to 4 years of age) in which the intention was to reach the target dose of 60 mg/kg/day, 50% of patients reached a final dose of at least 55 mg/kg/day.
Under adjunctive therapy (with and without enzyme-inducing AEDs), when normalized by body weight, apparent clearance (L/hr/kg) decreased when age increased such that children 2 to <4 years of age may require up to twice the oxcarbazepine dose per body weight compared to adults; and children 4 to ≤12 years of age may require a 50% higher oxcarbazepine dose per body weight compared to adults.
Dosage adjustment is recommended with concomitant use of strong CYP3A4 enzyme inducers or UGT inducers, which include certain antiepileptic drugs (AEDs) [see Drug Interactions (7.1, 7.2)].
2.5 Conversion to Monotherapy for Pediatric Patients (Aged 4 to 16 Years)
Patients receiving concomitant antiepileptic drugs may be converted to monotherapy by initiating treatment with oxcarbazepine tablets at approximately 8 to 10 mg/kg/day given twice-a-day, while simultaneously initiating the reduction of the dose of the concomitant antiepileptic drugs. The concomitant antiepileptic drugs can be completely withdrawn over 3 to 6 weeks while oxcarbazepine tablets may be increased as clinically indicated by a maximum increment of 10 mg/kg/day at approximately weekly intervals to achieve the recommended daily dose. Patients should be observed closely during this transition phase.
The recommended total daily dose of oxcarbazepine tablets is shown in Table 1.
2.6 Initiation of Monotherapy for Pediatric Patients (Aged 4 to 16 Years)
Patients not currently being treated with antiepileptic drugs may have monotherapy initiated with oxcarbazepine tablets. In these patients, initiate oxcarbazepine tablets at a dose of 8 to 10 mg/kg/day given twice-a-day. The dose should be increased by 5 mg/kg/day every third day to the recommended daily dose shown in the table below.
|
From
|
To
|
|
|
Weight in kg
|
Dose (mg/day)
|
Dose (mg/day)
|
|
20 |
600 |
900 |
|
25 |
900 |
1200 |
|
30 |
900 |
1200 |
|
35 |
900 |
1500 |
|
40 |
900 |
1500 |
|
45 |
1200 |
1500 |
|
50 |
1200 |
1800 |
|
55 |
1200 |
1800 |
|
60 |
1200 |
2100 |
|
65 |
1200 |
2100 |
|
70 |
1500 |
2100 |
2.7 Dosage Modification for Patients with Renal Impairment
In patients with impaired renal function (creatinine clearance <30 mL/min) initiate oxcarbazepine tablets at one-half the usual starting dose (300 mg/day, given twice-a-day) and increase slowly to achieve the desired clinical response [see Clinical Pharmacology (12.3)].
2.8 Administration Information
Oxcarbazepine tablets can be taken with or without food [see Clinical Pharmacology (12.3)].
Oxcarbazepine oral suspension and oxcarbazepine film-coated tablets may be interchanged at equal doses.
3 DOSAGE FORMS AND STRENGTHS
- •
- 150 mg Film-Coated Tablets: Yellow, film-coated oval, biconvex tablets with a deep break line on both sides and "G" engraved on one side of the deep break line on one side of the tablet and "13" and "7" engraved on either side of the deep break line on the other side of the tablet.
- •
- 300 mg Film-Coated Tablets: Yellow, film-coated oval, biconvex tablets with a deep break line on both sides and "G" and "4" engraved on either side of the deep break line on one side of the tablet.
- •
- 600 mg Film-Coated Tablets: Yellow, film-coated oval, biconvex tablets with a deep break line on both sides and "G" engraved on one side of the deep break line on one side of the tablet and "13" and "9" engraved on either side of the deep break line on the other side of the tablet.
4 CONTRAINDICATIONS
Oxcarbazepine tablets are contraindicated in patients with a known hypersensitivity to oxcarbazepine or to any of its components, or to eslicarbazepine acetate [see Warnings and Precautions (5.2, 5.3)].
5 WARNINGS AND PRECAUTIONS
5.1 Hyponatremia
Clinically significant hyponatremia (sodium <125 mmol/L) can develop during oxcarbazepine use. In the 14 controlled epilepsy studies 2.5% of oxcarbazepine-treated patients (38/1,524) had a sodium of less than 125 mmol/L at some point during treatment, compared to no such patients assigned placebo or active control (carbamazepine and phenobarbital for adjunctive and monotherapy substitution studies, and phenytoin and valproate for the monotherapy initiation studies). Clinically significant hyponatremia generally occurred during the first 3 months of treatment with oxcarbazepine, although there were patients who first developed a serum sodium <125 mmol/L more than 1 year after initiation of therapy. Most patients who developed hyponatremia were asymptomatic but patients in the clinical trials were frequently monitored and some had their oxcarbazepine dose reduced, discontinued, or had their fluid intake restricted for hyponatremia. Whether or not these maneuvers prevented the occurrence of more severe events is unknown. Cases of symptomatic hyponatremia and syndrome of inappropriate antidiuretic hormone secretion (SIADH) have been reported during postmarketing use. In clinical trials, patients whose treatment with oxcarbazepine was discontinued due to hyponatremia generally experienced normalization of serum sodium within a few days without additional treatment.
Measurement of serum sodium levels should be considered for patients during maintenance treatment with oxcarbazepine, particularly if the patient is receiving other medications known to decrease serum sodium levels (e.g., drugs associated with inappropriate ADH secretion) or if symptoms possibly indicating hyponatremia develop (e.g., nausea, malaise, headache, lethargy, confusion, obtundation, or increase in seizure frequency or severity).
5.2 Anaphylactic Reactions and Angioedema
Rare cases of anaphylaxis and angioedema involving the larynx, glottis, lips and eyelids have been reported in patients after taking the first or subsequent doses of oxcarbazepine. Angioedema associated with laryngeal edema can be fatal. If a patient develops any of these reactions after treatment with oxcarbazepine, the drug should be discontinued and an alternative treatment started. These patients should not be rechallenged with the drug [see Warnings and Precautions (5.3)].
5.3 Cross Hypersensitivity Reaction to Carbamazepine
Approximately 25% to 30% of patients who have had hypersensitivity reactions to carbamazepine will experience hypersensitivity reactions with oxcarbazepine. For this reason patients should be specifically questioned about any prior experience with carbamazepine, and patients with a history of hypersensitivity reactions to carbamazepine should ordinarily be treated with oxcarbazepine only if the potential benefit justifies the potential risk. If signs or symptoms of hypersensitivity develop, oxcarbazepine should be discontinued immediately [see Warnings and Precautions (5.2, 5.8)].
5.4 Serious Dermatological Reactions
Serious dermatological reactions, including Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN), have been reported in both children and adults in association with oxcarbazepine use. Such serious skin reactions may be life threatening, and some patients have required hospitalization with very rare reports of fatal outcome. The median time of onset for reported cases was 19 days after treatment initiation. Recurrence of the serious skin reactions following rechallenge with oxcarbazepine has also been reported.
The reporting rate of TEN and SJS associated with oxcarbazepine use, which is generally accepted to be an underestimate due to underreporting, exceeds the background incidence rate estimates by a factor of 3- to 10-fold. Estimates of the background incidence rate for these serious skin reactions in the general population range between 0.5 to 6 cases per million-person years. Therefore, if a patient develops a skin reaction while taking oxcarbazepine, consideration should be given to discontinuing oxcarbazepine use and prescribing another antiepileptic medication.
Association with HLA-B*1502
Patients carrying the HLA-B*1502 allele may be at increased risk for SJS/TEN with oxcarbazepine treatment. Human Leukocyte Antigen (HLA) allele B*1502 increases the risk for developing SJS/TEN in patients treated with carbamazepine. The chemical structure of oxcarbazepine is similar to that of carbamazepine. Available clinical evidence, and data from nonclinical studies showing a direct interaction between oxcarbazepine and HLA-B*1502 protein, suggest that the HLA-B*1502 allele may also increase the risk for SJS/TEN with oxcarbazepine.
The frequency of HLA-B*1502 allele ranges from 2 to 12% in Han Chinese populations, is about 8% in Thai populations, and above 15% in the Philippines and in some Malaysian populations. Allele frequencies up to about 2% and 6% have been reported in Korea and India, respectively. The frequency of the HLA-B*1502 allele is negligible in people from European descent, several African populations, indigenous peoples of the Americas, Hispanic populations, and in Japanese (<1%).
Testing for the presence of the HLA-B*1502 allele should be considered in patients with ancestry in genetically at-risk populations, prior to initiating treatment with oxcarbazepine. The use of oxcarbazepine should be avoided in patients positive for HLA-B*1502 unless the benefits clearly outweigh the risks. Consideration should also be given to avoid the use of other drugs associated with SJS/TEN in HLA-B*1502 positive patients, when alternative therapies are otherwise equally acceptable. Screening is not generally recommended in patients from populations in which the prevalence of HLAB* 1502 is low, or in current oxcarbazepine users, as the risk of SJS/TEN is largely confined to the first few months of therapy, regardless of HLA B*1502 status.
The use of HLA-B*1502 genotyping has important limitations and must never substitute for appropriate clinical vigilance and patient management. The role of other possible factors in the development of, and morbidity from, SJS/TEN, such as antiepileptic drug (AED) dose, compliance, concomitant medications, comorbidities, and the level of dermatologic monitoring have not been well characterized.
5.5 Suicidal Behavior and Ideation
Antiepileptic drugs (AEDs), including oxcarbazepine, increase the risk of suicidal thoughts or behavior in patients taking these drugs for any indication. Patients treated with any AED for any indication should be monitored for the emergence or worsening of depression, suicidal thoughts or behavior, and/or any unusual changes in mood or behavior.
Pooled analyses of 199 placebo-controlled clinical trials (mono- and adjunctive therapy) of 11 different AEDs showed that patients randomized to one of the AEDs had approximately twice the risk (adjusted Relative Risk 1.8, 95% CI:1.2, 2.7) of suicidal thinking or behavior compared to patients randomized to placebo. In these trials, which had a median treatment duration of 12 weeks, the estimated incidence rate of suicidal behavior or ideation among 27,863 AED-treated patients was 0.43%, compared to 0.24% among 16,029 placebo-treated patients, representing an increase of approximately one case of suicidal thinking or behavior for every 530 patients treated. There were 4 suicides in drug-treated patients in the trials and none in placebo-treated patients, but the number is too small to allow any conclusion about drug effect on suicide.
The increased risk of suicidal thoughts or behavior with AEDs was observed as early as one week after starting drug treatment with AEDs and persisted for the duration of treatment assessed. Because most trials included in the analysis did not extend beyond 24 weeks, the risk of suicidal thoughts or behavior beyond 24 weeks could not be assessed.
The risk of suicidal thoughts or behavior was generally consistent among drugs in the data analyzed. The finding of increased risk with AEDs of varying mechanisms of action and across a range of indications suggests that the risk applies to all AEDs used for any indication. The risk did not vary substantially by age (5 to 100 years) in the clinical trials analyzed. Table 2 shows absolute and relative risk by indication for all evaluated AEDs.
|
Indication
|
Placebo Patients
|
Drug Patients with
|
Relative Risk: Incidenceof Events in Drug
|
Risk Difference:
|
|
Epilepsy |
1 |
3.4 |
3.5 |
2.4 |
|
Psychiatric |
5.7 |
8.5 |
1.5 |
2.9 |
|
Other |
1 |
1.8 |
1.9 |
0.9 |
|
Total |
2.4 |
4.3 |
1.8 |
1.9 |
The relative risk for suicidal thoughts or behavior was higher in clinical trials for epilepsy than in clinical trials for psychiatric or other conditions, but the absolute risk differences were similar for the epilepsy and psychiatric indications.
Anyone considering prescribing oxcarbazepine or any other AED must balance the risk of suicidal thoughts or behavior with the risk of untreated illness. Epilepsy and many other illnesses for which AEDs are prescribed are themselves associated with morbidity and mortality and an increased risk of suicidal thoughts and behavior. Should suicidal thoughts and behavior emerge during treatment, the prescriber needs to consider whether the emergence of these symptoms in any given patient may be related to the illness being treated.
Patients, their caregivers, and families should be informed that AEDs increase the risk of suicidal thoughts and behavior and should be advised of the need to be alert for the emergence or worsening of the signs and symptoms of depression, any unusual changes in mood or behavior, or the emergence of suicidal thoughts, behavior, or thoughts about self-harm. Behaviors of concern should be reported immediately to healthcare providers.
5.6 Withdrawal of AEDs
As with most antiepileptic drugs, oxcarbazepine should generally be withdrawn gradually because of the risk of increased seizure frequency and status epilepticus [see Dosage and Administration (2.4) and Clinical Studies (14)]. But if withdrawal is needed because of a serious adverse event, rapid discontinuation can be considered.
5.7 Cognitive/Neuropsychiatric Adverse Reactions
Use of oxcarbazepine has been associated with central nervous system-related adverse reactions. The most significant of these can be classified into 3 general categories: 1) cognitive symptoms including psychomotor slowing, difficulty with concentration, and speech or language problems, 2) somnolence or fatigue, and 3) coordination abnormalities, including ataxia and gait disturbances.
Patients should be monitored for these signs and symptoms and advised not to drive or operate machinery until they have gained sufficient experience on oxcarbazepine to gauge whether it adversely affects their ability to drive or operate machinery.
Adult Patients
In one large, fixed-dose study, oxcarbazepine was added to existing AED therapy (up to three concomitant AEDs). By protocol, the dosage of the concomitant AEDs could not be reduced as oxcarbazepine was added, reduction in oxcarbazepine dosage was not allowed if intolerance developed, and patients were discontinued if unable to tolerate their highest target maintenance doses. In this trial, 65% of patients were discontinued because they could not tolerate the 2400 mg/day dose of oxcarbazepine on top of existing AEDs. The adverse events seen in this study were primarily CNS related and the risk for discontinuation was dose related.
In this trial, 7.1% of oxcarbazepine-treated patients and 4% of placebo-treated patients experienced a cognitive adverse reaction. The risk of discontinuation for these events was about 6.5 times greater on oxcarbazepine than on placebo. In addition, 26% of oxcarbazepine-treated patients and 12% of placebo-treated patients experienced somnolence. The risk of discontinuation for somnolence was about 10 times greater on oxcarbazepine than on placebo. Finally, 28.7% of oxcarbazepine-treated patients and 6.4% of placebo-treated patients experienced ataxia or gait disturbances. The risk for discontinuation for these events was about 7 times greater on oxcarbazepine than on placebo.
In a single placebo-controlled monotherapy trial evaluating 2400 mg/day of oxcarbazepine, no patients in either treatment group discontinued double-blind treatment because of cognitive adverse events, somnolence, ataxia, or gait disturbance.
In the 2 dose-controlled conversion to monotherapy trials comparing 2400 mg/day and 300 mg/day oxcarbazepine, 1.1% of patients in the 2400 mg/day group discontinued double-blind treatment because of somnolence or cognitive adverse reactions compared to 0% in the 300 mg/day group. In these trials, no patients discontinued because of ataxia or gait disturbances in either treatment group.
Pediatric Patients
A study was conducted in pediatric patients (3 to 17 years old) with inadequately controlled partial-onset seizures in which oxcarbazepine was added to existing AED therapy (up to 2 concomitant AEDs). By protocol, the dosage of concomitant AEDs could not be reduced as oxcarbazepine was added. Oxcarbazepine was titrated to reach a target dose ranging from 30 mg/kg to 46 mg/kg (based on a patient's body weight with fixed doses for predefined weight ranges).
Cognitive adverse events occurred in 5.8% of oxcarbazepine-treated patients (the single most common event being concentration impairment, 4 of 138 patients) and in 3.1% of patients treated with placebo. In addition, 34.8% of oxcarbazepine-treated patients and 14% of placebo-treated patients experienced somnolence. (No patient discontinued due to a cognitive adverse reaction or somnolence.). Finally, 23.2% of oxcarbazepine-treated patients and 7% of placebo-treated patients experienced ataxia or gait disturbances. Two (1.4%) oxcarbazepine-treated patients and 1 (0.8%) placebo-treated patient discontinued due to ataxia or gait disturbances.
5.8 Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS)/Multi-Organ Hypersensitivity
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS), also known as multi-organ hypersensitivity, has occurred with oxcarbazepine. Some of these events have been fatal or life-threatening. DRESS typically, although not exclusively, presents with fever, rash, lymphadenopathy and/or facial swelling, in association with other organ system involvement, such as hepatitis, nephritis, hematologic abnormalities, myocarditis, or myositis sometimes resembling an acute viral infection. Eosinophilia is often present. This disorder is variable in its expression, and other organ systems not noted here may be involved. It is important to note that early manifestations of hypersensitivity (e.g., fever, lymphadenopathy) may be present even though rash is not evident. If such signs or symptoms are present, the patient should be evaluated immediately. Oxcarbazepine should be discontinued if an alternative etiology for the signs or symptoms cannot be established.
5.9 Hematologic Events
Rare reports of pancytopenia, agranulocytosis, and leukopenia have been seen in patients treated with oxcarbazepine during postmarketing experience. Discontinuation of the drug should be considered if any evidence of these hematologic events develops.
5.10 Seizure Control During Pregnancy
Due to physiological changes during pregnancy, plasma levels of the active metabolite of oxcarbazepine, the 10-monohydroxy derivative (MHD), may gradually decrease throughout pregnancy. It is recommended that patients be monitored carefully during pregnancy. Close monitoring should continue through the postpartum period because MHD levels may return after delivery.
5.11 Risk of Seizure Aggravation
Exacerbation of or new onset primary generalized seizures has been reported with oxcarbazepine. The risk of aggravation of primary generalized seizures is seen especially in children but may also occur in adults. In case of seizure aggravation, oxcarbazepine should be discontinued.
6 ADVERSE REACTIONS
The following serious adverse reactions are described below and elsewhere in the labeling:
- •
- Hyponatremia [see Warnings and Precautions (5.1)]
- •
- Anaphylactic Reactions and Angioedema [see Warnings and Precautions (5.2)]
- •
- Cross Hypersensitivity Reaction to Carbamazepine [see Warnings and Precautions (5.3)]
- •
- Serious Dermatological Reactions [see Warnings and Precautions (5.4)]
- •
- Suicidal Behavior and Ideation [see Warnings and Precautions (5.5)]
- •
- Cognitive/Neuropsychiatric Adverse Reactions [see Warnings and Precautions (5.7)]
- •
- Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS)/Multi-Organ Hypersensitivity [see Warnings and Precautions (5.8)]
- •
- Hematologic Events [see Warnings and Precautions (5.9)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Most Common Adverse Reactions in All Clinical Studies
Adjunctive Therapy/Monotherapy in Adults Previously Treated with Other AEDs
The most common (≥10% more than placebo for adjunctive or low dose for monotherapy) adverse reactions with oxcarbazepine: dizziness, somnolence, diplopia, fatigue, nausea, vomiting, ataxia, abnormal vision, headache, nystagmus tremor, and abnormal gait.
Approximately 23% of these 1,537 adult patients discontinued treatment because of an adverse reaction. The adverse reactions most commonly associated with discontinuation were: dizziness (6.4%), diplopia (5.9%), ataxia (5.2%), vomiting (5.1%), nausea (4.9%), somnolence (3.8%), headache (2.9%), fatigue (2.1%), abnormal vision (2.1%), tremor (1.8%), abnormal gait (1.7%), rash (1.4%), hyponatremia (1%).
Monotherapy in Adults Not Previously Treated with Other AEDs
The most common (≥5%) adverse reactions with oxcarbazepine in these patients were similar to those in previously treated patients.
Approximately 9% of these 295 adult patients discontinued treatment because of an adverse reaction. The adverse reactions most commonly associated with discontinuation were: dizziness (1.7%), nausea (1.7%), rash (1.7%), headache (1.4%).
Adjunctive Therapy/Monotherapy in Pediatric Patients 4 Years Old and Above Previously Treated with Other AEDs
The most common (≥5%) adverse reactions with oxcarbazepine in these patients were similar to those seen in adults.
Approximately 11% of these 456 pediatric patients discontinued treatment because of an adverse reaction. The adverse reactions most commonly associated with discontinuation were: somnolence (2.4%), vomiting (2%), ataxia (1.8%), diplopia (1.3%), dizziness (1.3%), fatigue (1.1%), nystagmus (1.1%).
Monotherapy in Pediatric Patients 4 Years Old and Above Not Previously Treated with Other AEDs
The most common (≥5%) adverse reactions with oxcarbazepine in these patients were similar to those in adults.
Approximately 9.2% of 152 pediatric patients discontinued treatment because of an adverse reaction. The adverse reactions most commonly associated (≥1%) with discontinuation were rash (5.3%) and maculopapular rash (1.3%).
Adjunctive Therapy/Monotherapy in Pediatric Patients 1 Month to <4 Years Old Previously Treated or Not Previously Treated with Other AEDs:
The most common (≥5%) adverse reactions with oxcarbazepine in these patients were similar to those seen in older children and adults except for infections and infestations which were more frequently seen in these younger children.
Approximately 11% of these 241 pediatric patients discontinued treatment because of an adverse reaction. The adverse reactions most commonly associated with discontinuation were: convulsions (3.7%), status epilepticus (1.2%), and ataxia (1.2%).
Controlled Clinical Studies of Adjunctive Therapy/Monotherapy in Adults Previously Treated with Other AEDs
Table 3 lists adverse reactions that occurred in at least 2% of adult patients with epilepsy, treated with oxcarbazepine or placebo as adjunctive treatment and were numerically more common in the patients treated with any dose of oxcarbazepine.
Table 4 lists adverse reactions in patients converted from other AEDs to either high-dose oxcarbazepine (2400 mg/day) or low-dose (300 mg/day) oxcarbazepine. Note that in some of these monotherapy studies patients who dropped out during a preliminary tolerability phase are not included in the tables.
|
Oxcarbazepine Dosage (mg/day) |
||||
|
Body System/
|
Oxcarbazepine 600
|
Oxcarbazepine
|
Oxcarbazepine
|
Placebo
|
|
Body as a Whole | ||||
|
15 |
12 |
15 |
7 |
|
6 |
3 |
6 |
5 |
|
2 |
1 |
2 |
1 |
|
1 |
2 |
2 |
1 |
|
0 |
1 |
2 |
0 |
|
Cardiovascular System | ||||
|
0 |
1 |
2 |
0 |
|
Digestive System | ||||
|
15 |
25 |
29 |
10 |
|
13 |
25 |
36 |
5 |
|
10 |
13 |
11 |
5 |
|
5 |
6 |
7 |
6 |
|
5 |
5 |
6 |
2 |
|
2 |
2 |
6 |
4 |
|
2 |
1 |
2 |
1 |
|
Metabolic and Nutritional Disorders | ||||
|
3 |
1 |
2 |
1 |
|
Musculoskeletal System | ||||
|
1 |
2 |
2 |
0 |
|
0 |
2 |
2 |
1 |
|
Nervous System | ||||
|
32 |
28 |
26 |
23 |
|
26 |
32 |
49 |
13 |
|
20 |
28 |
36 |
12 |
|
9 |
17 |
31 |
5 |
|
7 |
20 |
26 |
5 |
|
5 |
10 |
17 |
1 |
|
4 |
2 |
3 |
1 |
|
3 |
8 |
16 |
5 |
|
2 |
4 |
2 |
1 |
|
1 |
1 |
2 |
1 |
|
1 |
3 |
2 |
1 |
|
0 |
0 |
2 |
0 |
|
1 |
1 |
3 |
0 |
|
1 |
1 |
2 |
1 |
|
1 |
0 |
2 |
1 |
|
1 |
2 |
3 |
0 |
|
0 |
2 |
4 |
0 |
|
Respiratory System | ||||
|
2 |
4 |
5 |
4 |
|
Skin and Appendages | ||||
|
1 |
2 |
2 |
0 |
|
Special Senses | ||||
|
14 |
30 |
40 |
5 |
|
6 |
12 |
15 |
2 |
|
6 |
14 |
13 |
4 |
|
0 |
0 |
2 |
0 |
|
Body System/
|
Oxcarbazepine
|
Oxcarbazepine
|
|
Body as a Whole | ||
|
21 |
5 |
|
3 |
0 |
|
2 |
0 |
|
2 |
1 |
|
2 |
0 |
|
Digestive System | ||
|
22 |
7 |
|
15 |
5 |
|
7 |
5 |
|
6 |
1 |
|
5 |
3 |
|
5 |
3 |
|
3 |
0 |
|
2 |
0 |
|
2 |
1 |
|
Hemic and Lymphatic System | ||
|
2 |
0 |
|
Infections and Infestations | ||
|
7 |
5 |
|
2 |
0 |
|
Metabolic and Nutritional Disorders | ||
|
5 |
0 |
|
2 |
0 |
|
Nervous System | ||
|
31 |
15 |
|
28 |
8 |
|
19 |
5 |
|
7 |
5 |
|
7 |
1 |
|
7 |
0 |
|
7 |
0 |
|
6 |
3 |
|
6 |
3 |
|
5 |
1 |
|
5 |
2 |
|
3 |
2 |
|
3 |
1 |
|
2 |
1 |
|
2 |
0 |
|
2 |
0 |
|
Respiratory System | ||
|
10 |
5 |
|
5 |
0 |
|
3 |
0 |
|
3 |
0 |
|
Skin and Appendages | ||
|
2 |
1 |
|
2 |
0 |
|
Special Senses | ||
|
14 |
2 |
|
12 |
1 |
|
5 |
0 |
|
3 |
0 |
|
2 |
1 |
|
2 |
0 |
|
Urogenital and Reproductive System | ||
|
5 |
1 |
|
2 |
1 |
|
2 |
0 |
Controlled Clinical Study of Monotherapy in Adults Not Previously Treated with Other AEDs
Table 5 lists adverse reactions in a controlled clinical study of monotherapy in adults not previously treated with other AEDs that occurred in at least 2% of adult patients with epilepsy treated with oxcarbazepine or placebo and were numerically more common in the patients treated with oxcarbazepine.
|
Body System/
|
Oxcarbazepine
|
Placebo
|
|
Body as a Whole | ||
|
4 |
0 |
|
Digestive System | ||
|
16 |
12 |
|
7 |
2 |
|
7 |
6 |
|
5 |
0 |
|
5 |
4 |
|
Musculoskeletal System | ||
|
4 |
2 |
|
Nervous System | ||
|
22 |
6 |
|
13 |
10 |
|
5 |
0 |
|
5 |
2 |
|
4 |
2 |
|
4 |
2 |
|
4 |
0 |
|
Respiratory System | ||
|
7 |
0 |
|
4 |
0 |
|
4 |
0 |
|
4 |
2 |
|
Skin and Appendages | ||
|
4 |
2 |
|
Special Senses | ||
|
4 |
0 |
Controlled Clinical Studies of Adjunctive Therapy/Monotherapy in Pediatric Patients Previously Treated with Other AEDs
Table 6 lists adverse reactions that occurred in at least 2% of pediatric patients with epilepsy treated with oxcarbazepine or placebo as adjunctive treatment and were numerically more common in the patients treated with oxcarbazepine.
|
Body System/
|
Oxcarbazepine
|
Placebo
|
|
Body as a Whole | ||
|
13 |
9 |
|
2 |
0 |
|
2 |
1 |
|
Digestive System | ||
|
33 |
14 |
|
19 |
5 |
|
4 |
1 |
|
2 |
0 |
|
Nervous System | ||
|
31 |
19 |
|
31 |
13 |
|
28 |
8 |
|
13 |
4 |
|
9 |
1 |
|
8 |
4 |
|
8 |
3 |
|
6 |
4 |
|
3 |
1 |
|
2 |
1 |
|
2 |
1 |
|
2 |
1 |
|
Respiratory System | ||
|
10 |
9 |
|
2 |
1 |
|
Skin and Appendages | ||
|
4 |
2 |
|
3 |
0 |
|
Special Senses | ||
|
17 |
1 |
|
13 |
1 |
|
2 |
0 |
Other Events Observed in Association with the Administration of Oxcarbazepine
In the paragraphs that follow, the adverse reactions, other than those in the preceding tables or text, that occurred in a total of 565 children and 1,574 adults exposed to oxcarbazepine and that are reasonably likely to be related to drug use are presented. Events common in the population, events reflecting chronic illness and events likely to reflect concomitant illness are omitted particularly if minor. They are listed in order of decreasing frequency. Because the reports cite events observed in open label and uncontrolled trials, the role of oxcarbazepine in their causation cannot be reliably determined.
Body as a Whole: fever, malaise, pain chest precordial, rigors, weight decrease.
Cardiovascular System: bradycardia, cardiac failure, cerebral hemorrhage, hypertension, hypotension postural, palpitation, syncope, tachycardia.
Digestive System: appetite increased, blood in stool, cholelithiasis, colitis, duodenal ulcer, dysphagia, enteritis, eructation, esophagitis, flatulence, gastric ulcer, gingival bleeding, gum hyperplasia, hematemesis, hemorrhage rectum, hemorrhoids, hiccup, mouth dry, pain biliary, pain right hypochondrium, retching, sialoadenitis, stomatitis, stomatitis ulcerative.
Hematologic and Lymphatic System: thrombocytopenia.
Laboratory Abnormality: gamma-GT increased, hyperglycemia, hypocalcemia, hypoglycemia, hypokalemia, liver enzymes elevated, serum transaminase increased.
Musculoskeletal System: hypertonia muscle.
Nervous System: aggressive reaction, amnesia, anguish, anxiety, apathy, aphasia, aura, convulsions aggravated, delirium, delusion, depressed level of consciousness, dysphonia, dystonia, emotional lability, euphoria, extrapyramidal disorder, feeling drunk, hemiplegia, hyperkinesia, hyperreflexia, hypoesthesia, hypokinesia, hyporeflexia, hypotonia, hysteria, libido decreased, libido increased, manic reaction, migraine, muscle contractions involuntary, nervousness, neuralgia, oculogyric crisis, panic disorder, paralysis, paroniria, personality disorder, psychosis, ptosis, stupor, tetany.
Respiratory System: asthma, dyspnea, epistaxis, laryngismus, pleurisy.
Skin and Appendages: acne, alopecia, angioedema, bruising, dermatitis contact, eczema, facial rash, flushing, folliculitis, heat rash, hot flushes, photosensitivity reaction, pruritus genital, psoriasis, purpura, rash erythematous, rash maculopapular, vitiligo, urticaria.
Special Senses: accommodation abnormal, cataract, conjunctival hemorrhage, edema eye, hemianopia, mydriasis, otitis externa, photophobia, scotoma, taste perversion, tinnitus, xerophthalmia.
Surgical and Medical Procedures: procedure dental oral, procedure female reproductive, procedure musculoskeletal, procedure skin.
Urogenital and Reproductive System: dysuria, hematuria, intermenstrual bleeding, leukorrhea, menorrhagia, micturition frequency, pain renal, pain urinary tract, polyuria, priapism, renal calculus.
Other: Systemic lupus erythematosus.
Laboratory Tests
Serum sodium levels below 125 mmol/L have been observed in patients treated with oxcarbazepine [see Warnings and Precautions(5.1)]. Experience from clinical trials indicates that serum sodium levels return toward normal when the oxcarbazepine dosage is reduced or discontinued, or when the patient was treated conservatively (e.g., fluid restriction).
Laboratory data from clinical trials suggest that oxcarbazepine use was associated with decreases in T4, without changes in T3 or TSH.
6.2 Postmarketing Experience
The following adverse reactions have been identified during postapproval use of oxcarbazepine. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Body as a Whole: multi-organ hypersensitivity disorders characterized by features such as rash, fever, lymphadenopathy, abnormal liver function tests, eosinophilia and arthralgia [see Warnings and Precautions (5.8)]
Cardiovascular System: atrioventricular block
Immune System Disorders: anaphylaxis [see Warnings and Precautions (5.2)]
Digestive System: pancreatitis and/or lipase and/or amylase increase
Hematologic and Lymphatic Systems: aplastic anemia [see Warnings and Precautions (5.9)]
Metabolism and Nutrition Disorders: hypothyroidism and syndrome of inappropriate antidiuretic hormone secretion (SIADH)
Skin and Subcutaneous Tissue Disorders: erythema multiforme, Stevens-Johnson syndrome, toxic epidermal necrolysis [see Warnings and Precautions (5.4)], Acute Generalized Exanthematous Pustulosis (AGEP)
Musculoskeletal, connective tissue and bone disorders: There have been reports of decreased bone mineral density, osteoporosis and fractures in patients on long-term therapy with oxcarbazepine.
Injury, Poisoning, and Procedural Complications: fall
Nervous System Disorders: dysarthria
7 DRUG INTERACTIONS
7.1 Effect of Oxcarbazepine on Other Drugs
Phenytoin levels have been shown to increase with concomitant use of oxcarbazepine at doses greater than 1200 mg/day [see Clinical Pharmacology (12.3)]. Therefore, it is recommended that the plasma levels of phenytoin be monitored during the period of oxcarbazepine titration and dosage modification. A decrease in the dose of phenytoin may be required.
7.2 Effect of Other Drugs on Oxcarbazepine
Strong inducers of cytochrome P450 enzymes and/or inducers of UGT (e.g., rifampin, carbamazepine, phenytoin and phenobarbital) have been shown to decrease the plasma/serum levels of MHD, the active metabolite of oxcarbazepine (25% to 49%) [see Clinical Pharmacology (12.3)]. If oxcarbazepine and strong CYP3A4 inducers or UGT inducers are administered concurrently, it is recommended that the plasma levels of MHD be monitored during the period of oxcarbazepine titration. Dose adjustment of oxcarbazepine may be required after initiation, dosage modification, or discontinuation of such inducers.
7.3 Hormonal Contraceptives
Concurrent use of oxcarbazepine with hormonal contraceptives may render these contraceptives less effective [see Use in Specific Populations (8.3) and Clinical Pharmacology (12.3)]. Studies with other oral or implant contraceptives have not been conducted.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to AEDs, such as oxcarbazepine, during pregnancy. Encourage women who are taking oxcarbazepine during pregnancy to enroll in the North American Antiepileptic Drug (NAAED) Pregnancy Registry by calling 1-888-233-2334 or visiting http://www.aedpregnancyregistry.org/.
Risk Summary
There are no adequate data on the developmental risks associated with the use of oxcarbazepine in pregnant women; however, oxcarbazepine is closely related structurally to carbamazepine, which is considered to be teratogenic in humans. Data on a limited number of pregnancies from pregnancy registries suggest that oxcarbazepine monotherapy use is associated with congenital malformations (e.g., craniofacial defects such as oral clefts, and cardiac malformations such as ventricular septal defects). Increased incidences of fetal structural abnormalities and other manifestations of developmental toxicity (embryolethality, growth retardation) were observed in the offspring of animals treated with either oxcarbazepine or its active 10-hydroxy metabolite (MHD) during pregnancy at doses similar to the maximum recommended human dose (MRHD).
In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively. The background risk of major birth defects and miscarriage for the indicated population is unknown.
Clinical Considerations
An increase in seizure frequency may occur during pregnancy because of altered levels of the active metabolite of oxcarbazepine. Monitor patients carefully during pregnancy and through the postpartum period [see Warnings and Precautions (5.10)].
Data
Human Data
Data from published registries have reported craniofacial defects such as oral clefts and cardiac malformations such as ventricular septal defects in children with prenatal oxcarbazepine exposure.
Animal Data
When pregnant rats were given oxcarbazepine (0, 30, 300, or 1000 mg/kg/day) orally throughout the period of organogenesis, increased incidences of fetal malformations (craniofacial, cardiovascular, and skeletal) and variations were observed at the intermediate and high doses (approximately 1.2 and 4 times, respectively, the MRHD on a mg/m2 basis). Increased embryofetal death and decreased fetal body weights were seen at the high dose. Doses ≥300 mg/kg/day were also maternally toxic (decreased body weight gain, clinical signs), but there is no evidence to suggest that teratogenicity was secondary to the maternal effects.
In a study in which pregnant rabbits were orally administered MHD (0, 20, 100, or 200 mg/kg/day) during organogenesis, embryofetal mortality was increased at the highest dose (1.5 times the MRHD on a mg/m2 basis). This dose produced only minimal maternal toxicity.
In a study in which female rats were dosed orally with oxcarbazepine (0, 25, 50, or 150 mg/kg/day) during the latter part of gestation and throughout the lactation period, a persistent reduction in body weights and altered behavior (decreased activity) were observed in offspring exposed to the highest dose (less than the MRHD on a mg/m2 basis). Oral administration of MHD (0, 25, 75, or 250 mg/kg/day) to rats during gestation and lactation resulted in a persistent reduction in offspring weights at the highest dose (equivalent to the MRHD on a mg/m2 basis).
8.2 Lactation
Risk Summary
Oxcarbazepine and its active metabolite (MHD) are present in human milk after Oxcarbazepine administration. The effects of oxcarbazepine and its active metabolite (MHD) on the breastfed infant or on milk production are unknown. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for Oxcarbazepine and any potential adverse effects on the breastfed infant from Oxcarbazepine or from the underlying maternal condition.
8.3 Females and Males of Reproductive Potential
Contraception
Use of Oxcarbazepine with hormonal contraceptives containing ethinylestradiol or levonorgestrel is associated with decreased plasma concentrations of these hormones and may result in a failure of the therapeutic effect of the oral contraceptive drug. Advise women of reproductive potential taking Oxcarbazepine who are using a contraceptive containing ethinylestradiol or levonorgestrel to use additional or alternative non-hormonal birth control [see Drug interactions (7.3) and Clinical Pharmacology (12.3)].
8.4 Pediatric Use
Oxcarbazepine is indicated for use as adjunctive therapy for partial-onset seizures in patients aged 2 to 16 years.
The safety and effectiveness for use as adjunctive therapy for partial-onset seizures in pediatric patients below the age of 2 have not been established.
Oxcarbazepine is also indicated as monotherapy for partial-onset seizures in patients aged 4 to 16 years.
The safety and effectiveness for use as monotherapy for partial-onset seizures in pediatric patients below the age of 4 have not been established.
Oxcarbazepine has been given to 898 patients between the ages of 1 month to 17 years in controlled clinical trials (332 treated as monotherapy) and about 677 patients between the ages of 1 month to 17 years in other trials [see Warnings and Precautions (5.11), Adverse Reactions (6.1), Clinical Pharmacology (12.3), and Clinical Studies (14)].
8.5 Geriatric Use
There were 52 patients over age 65 in controlled clinical trials and 565 patients over the age of 65 in other trials. Following administration of single (300 mg) and multiple (600 mg/day) doses of oxcarbazepine in elderly volunteers (60 to 82 years of age), the maximum plasma concentrations and AUC values of MHD were 30% to 60% higher than in younger volunteers (18 to 32 years of age). Comparisons of creatinine clearance in young and elderly volunteers indicate that the difference was due to age-related reductions in creatinine clearance. Close monitoring of sodium levels is required in elderly patients at risk for hyponatremia [see Warnings and Precautions (5.1)].
8.6 Renal Impairment
Dose adjustment is recommended for renally impaired patients (CLcr <30 mL/min) [see Dosage and Administration (2.7) and Clinical Pharmacology (12.3)].
10 OVERDOSAGE
10.1 Human Overdose Experience
Isolated cases of overdose with oxcarbazepine have been reported. The maximum dose taken was approximately 48,000 mg. All patients recovered with symptomatic treatment. Nausea, vomiting, somnolence, aggression, agitation, hypotension, and tremor each occurred in more than one patient. Coma, confusional state, convulsion, dyscoordination, depressed level of consciousness, diplopia, dizziness, dyskinesia, dyspnea, QT prolongation, headache, miosis, nystagmus, overdose, decreased urine output, blurred vision also occurred.
11 DESCRIPTION
Oxcarbazepine Tablets USP are an antiepileptic drug available as 150 mg, 300 mg, and 600 mg film-coated tablets for oral administration. Oxcarbazepine, USP is 10,11-Dihydro-10-oxo-5H-dibenz[b,f]azepine-5-carboxamide, and its structural formula is:
Oxcarbazepine, USP is a light orange to creamish white or off-white powder. It is soluble in acetic acid, sparingly soluble in chloroform, practically insoluble in water. Its molecular weight is 252.27 g/mol.
Oxcarbazepine film-coated tablets contain the following inactive ingredients: colloidal silicon dioxide, crospovidone, ferric oxide (yellow), hypromellose, magnesium stearate, meglumine, microcrystalline cellulose, polyethylene glycol, and titanium dioxide.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
The pharmacological activity of oxcarbazepine is primarily exerted through the 10-monohydroxy metabolite (MHD) of oxcarbazepine [see Clinical Pharmacology (12.3)]. The precise mechanism by which oxcarbazepine and MHD exert their anti-seizure effect is unknown; however, in vitro electrophysiological studies indicate that they produce blockade of voltage-sensitive sodium channels, resulting in stabilization of hyperexcited neural membranes, inhibition of repetitive neuronal firing, and diminution of propagation of synaptic impulses. These actions are thought to be important in the prevention of seizure spread in the intact brain. In addition, increased potassium conductance and modulation of high-voltage activated calcium channels may contribute to the anticonvulsant effects of the drug. No significant interactions of oxcarbazepine or MHD with brain neurotransmitter or modulator receptor sites have been demonstrated.
12.2 Pharmacodynamics
Oxcarbazepine and its active metabolite (MHD) exhibit anticonvulsant properties in animal seizure models. They protected rodents against electrically induced tonic extension seizures and, to a lesser degree, chemically induced clonic seizures, and abolished or reduced the frequency of chronically recurring focal seizures in Rhesus monkeys with aluminum implants. No development of tolerance (i.e., attenuation of anticonvulsive activity) was observed in the maximal electroshock test when mice and rats were treated daily for 5 days and 4 weeks, respectively, with oxcarbazepine or MHD.
12.3 Pharmacokinetics
Following oral administration of oxcarbazepine tablets, oxcarbazepine is completely absorbed and extensively metabolized to its pharmacologically active 10-monohydroxy metabolite (MHD). In a mass balance study in people, only 2% of total radioactivity in plasma was due to unchanged oxcarbazepine, with approximately 70% present as MHD, and the remainder attributable to minor metabolites.
The half-life of the parent is about 2 hours, while the half-life of MHD is about 9 hours, so that MHD is responsible for most antiepileptic activity.
Absorption
After single-dose administration of oxcarbazepine tablets to healthy male volunteers under fasted conditions, the median tmax was 4.5 (range 3 to 13) hours.
Steady-state plasma concentrations of MHD are reached within 2 to 3 days in patients when oxcarbazepine is given twice a day. At steady state the pharmacokinetics of MHD are linear and show dose proportionality over the dose range of 300 to 2400 mg/day.
Food has no effect on the rate and extent of absorption of oxcarbazepine from oxcarbazepine tablets. Therefore, oxcarbazepine tablets can be taken with or without food.
Distribution
The apparent volume of distribution of MHD is 49 L.
Approximately 40% of MHD is bound to serum proteins, predominantly to albumin. Binding is independent of the serum concentration within the therapeutically relevant range. Oxcarbazepine and MHD do not bind to alpha-1-acid glycoprotein.
Metabolism and Excretion
Oxcarbazepine is rapidly reduced by cytosolic enzymes in the liver to its 10-monohydroxy metabolite, MHD, which is primarily responsible for the pharmacological effect of oxcarbazepine. MHD is metabolized further by conjugation with glucuronic acid. Minor amounts (4% of the dose) are oxidized to the pharmacologically inactive 10,11-dihydroxy metabolite (DHD).
Oxcarbazepine is cleared from the body mostly in the form of metabolites which are predominantly excreted by the kidneys. More than 95% of the dose appears in the urine, with less than 1% as unchanged oxcarbazepine. Fecal excretion accounts for less than 4% of the administered dose. Approximately 80% of the dose is excreted in the urine either as glucuronides of MHD (49%) or as unchanged MHD (27%); the inactive DHD accounts for approximately 3% and conjugates of MHD and oxcarbazepine account for 13% of the dose.
The half-life of the parent is about 2 hours, while the half-life of MHD is about 9 hours.
Specific Populations
Geriatrics
Following administration of single (300 mg) and multiple (600 mg/day) doses of oxcarbazepine to elderly volunteers (60 to 82 years of age), the maximum plasma concentrations and AUC values of MHD were 30% to 60% higher than in younger volunteers (18 to 32 years of age). Comparisons of creatinine clearance in young and elderly volunteers indicate that the difference was due to age-related reductions in creatinine clearance.
Pediatrics
Weight-adjusted MHD clearance decreases as age and weight increases, approaching that of adults. The mean weight-adjusted clearance in children 2 years to <4 years of age is approximately 80% higher on average than that of adults. Therefore, MHD exposure in these children is expected to be about one-half that of adults when treated with a similar weight-adjusted dose. The mean weight-adjusted clearance in children 4 to 12 years of age is approximately 40% higher on average than that of adults. Therefore, MHD exposure in these children is expected to be about three-quarters that of adults when treated with a similar weight-adjusted dose. As weight increases, for patients 13 years of age and above, the weight-adjusted MHD clearance is expected to reach that of adults.
Gender
No gender-related pharmacokinetic differences have been observed in children, adults, or the elderly.
Race
No specific studies have been conducted to assess what effect, if any, race may have on the disposition of oxcarbazepine.
Renal Impairment
There is a linear correlation between creatinine clearance and the renal clearance of MHD. When oxcarbazepine is administered as a single 300 mg dose in renally-impaired patients (creatinine clearance <30 mL/min), the elimination half-life of MHD is prolonged to 19 hours, with a 2-fold increase in AUC [see Dosage and Administration (2.7) and Use in Specific Populations (8.6)].
Hepatic Impairment
The pharmacokinetics and metabolism of oxcarbazepine and MHD were evaluated in healthy volunteers and hepatically-impaired subjects after a single 900-mg oral dose. Mild-to-moderate hepatic impairment did not affect the pharmacokinetics of oxcarbazepine and MHD [see Dosage and Administration (2.8)].
Pregnancy
Due to physiological changes during pregnancy, MHD plasma levels may gradually decrease throughout pregnancy [see Use in Specific Populations (8.1)]
Drug Interactions:
- •
- In Vitro
Oxcarbazepine can inhibit CYP2C19 and induce CYP3A4/5 with potentially important effects on plasma concentrations of other drugs. In addition, several AEDs that are cytochrome P450 inducers can decrease plasma concentrations of oxcarbazepine and MHD. No autoinduction has been observed with oxcarbazepine.
Oxcarbazepine was evaluated in human liver microsomes to determine its capacity to inhibit the major cytochrome P450 enzymes responsible for the metabolism of other drugs. Results demonstrate that oxcarbazepine and its pharmacologically active 10-monohydroxy metabolite (MHD) have little or no capacity to function as inhibitors for most of the human cytochrome P450 enzymes evaluated (CYP1A2, CYP2A6, CYP2C9, CYP2D6, CYP2E1, CYP4A9 and CYP4A11) with the exception of CYP2C19 and CYP3A4/5. Although inhibition of CYP3A4/5 by oxcarbazepine and MHD did occur at high concentrations, it is not likely to be of clinical significance. The inhibition of CYP2C19 by oxcarbazepine and MHD can cause increased plasma concentrations of drugs that are substrates of CYP2C19, which is clinically relevant.
In vitro, the UDP-glucuronyl transferase level was increased, indicating induction of this enzyme. Increases of 22% with MHD and 47% with oxcarbazepine were observed. As MHD, the predominant plasma substrate, is only a weak inducer of UDP-glucuronyl transferase, it is unlikely to have an effect on drugs that are mainly eliminated by conjugation through UDP-glucuronyl transferase (e.g., valproic acid, lamotrigine).
In addition, oxcarbazepine and MHD induce a subgroup of the cytochrome P450 3A family (CYP3A4 and CYP3A5) responsible for the metabolism of dihydropyridine calcium antagonists, oral contraceptives and cyclosporine resulting in a lower plasma concentration of these drugs.
As binding of MHD to plasma proteins is low (40%), clinically significant interactions with other drugs through competition for protein binding sites are unlikely.
- •
- In Vivo
Other Antiepileptic Drugs
Potential interactions between oxcarbazepine and other AEDs were assessed in clinical studies. The effect of these interactions on mean AUCs and Cmin are summarized in Table 7 [see Drug Interactions (7.1, 7.2)].
Table 7: Summary of AED Interactions with Oxcarbazepine
|
AED Coadministered |
Dose of AED (mg/day) |
Oxcarbazepine Dose (mg/day) |
Influence of Oxcarbazepine on AED Concentration (Mean Change, 90% Confidence Interval) |
Influence of AED on MHD Concentration (Mean Change, 90% Confidence Interval) |
|
Carbamazepine |
400 to 2000 |
900 |
nc1 |
40% decrease [CI: 17% decrease, 57% decrease] |
|
Phenobarbital |
100 to 150 |
600 to 1800 |
14% increase [CI: 2% increase, 24% increase] |
25% decrease [CI: 12% decrease, 51% decrease] |
|
Phenytoin |
250 to 500 |
600 to 1800 >1200 to 2400 |
nc1,2 up to 40% increase3 [CI: 12% increase, 60% increase] |
30% decrease [CI: 3% decrease, 48% decrease] |
|
Valproic acid |
400 to 2800 |
600 to 1800 |
nc1 |
18% decrease [CI: 13% decrease, 40% decrease] |
|
Lamotrigine |
200 |
1200 |
nc1 |
nc1 |
1nc denotes a mean change of less than 10%
2Pediatrics
3Mean increase in adults at high oxcarbazepine doses
Hormonal Contraceptives
Coadministration of oxcarbazepine with an oral contraceptive has been shown to influence the plasma concentrations of the two hormonal components, ethinylestradiol (EE) and levonorgestrel (LNG) [see Drug Interactions (7.3)]. The mean AUC values of EE were decreased by 48% [90% CI: 22 to 65] in one study and 52% [90% CI: 38 to 52] in another study. The mean AUC values of LNG were decreased by 32% [90% CI: 20 to 45] in one study and 52% [90% CI: 42 to 52] in another study.
Other Drug Interactions
Calcium Antagonists: After repeated coadministration of oxcarbazepine, the AUC of felodipine was lowered by 28% [90% CI: 20 to 33]. Verapamil produced a decrease of 20% [90% CI: 18 to 27] of the plasma levels of MHD.
Cimetidine, erythromycin and dextropropoxyphene had no effect on the pharmacokinetics of MHD. Results with warfarin show no evidence of interaction with either single or repeated doses of oxcarbazepine.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
In 2-year carcinogenicity studies, oxcarbazepine was administered in the diet at doses of up to 100 mg/kg/day to mice and by gavage at doses of up to 250 mg/kg/day to rats, and the pharmacologically active 10-hydroxy metabolite (MHD) was administered orally at doses of up to 600 mg/kg/day to rats. In mice, a dose-related increase in the incidence of hepatocellular adenomas was observed at oxcarbazepine doses ≥70 mg/kg/day which is less than the maximum recommended human dose (MRHD) on a mg/m2 basis. In rats, the incidence of hepatocellular carcinomas was increased in females treated with oxcarbazepine at doses ≥25 mg/kg/day (less than the MRHD on a mg/m2 basis), and incidences of hepatocellular adenomas and/or carcinomas were increased in males and females treated with MHD at doses of 600 mg/kg/day (2.4 times the MRHD on a mg/m2 basis) and ≥250 mg/kg/day (equivalent to the MRHD on a mg/m2 basis), respectively. There was an increase in the incidence of benign testicular interstitial cell tumors in rats at 250 mg oxcarbazepine/kg/day and at ≥250 mg MHD/kg/day, and an increase in the incidence of granular cell tumors in the cervix and vagina in rats at 600 mg MHD/kg/day.
Mutagenesis
Oxcarbazepine increased mutation frequencies in the in vitro Ames test in the absence of metabolic activation. Both oxcarbazepine and MHD produced increases in chromosomal aberrations and polyploidy in the Chinese hamster ovary assay in vitro in the absence of metabolic activation. MHD was negative in the Ames test, and no mutagenic or clastogenic activity was found with either oxcarbazepine or MHD in V79 Chinese hamster cells in vitro. Oxcarbazepine and MHD were both negative for clastogenic or aneugenic effects (micronucleus formation) in an in vivo rat bone marrow assay.
Impairment of Fertility
In a study in which male and female rats were administered oxcarbazepine (0, 25, 75 and 150 mg/kg/day) orally prior to and during mating and continuing in females during gestation, no adverse effects on fertility or reproductive performance were observed. The highest dose tested is less than the MRHD on a mg/m2 basis. In a fertility study in which rats were administered MHD (0, 50, 150, or 450 mg/kg/day) orally prior to and during mating and early gestation, estrous cyclicity was disrupted and numbers of corpora lutea, implantations, and live embryos were reduced in females receiving the highest dose (approximately 2 times the MRHD on a mg/m2 basis).
14 CLINICAL STUDIES
The effectiveness of oxcarbazepine as adjunctive and monotherapy for partial-onset seizures in adults, and as adjunctive therapy in children aged 2 to 16 years was established in seven multicenter, randomized, controlled trials.
The effectiveness of oxcarbazepine as monotherapy for partial-onset seizures in children aged 4 to 16 years was determined from data obtained in the studies described, as well as by pharmacokinetic/pharmacodynamics considerations.
14.1 Oxcarbazepine Monotherapy Trials
Four randomized, controlled, double-blind, multicenter trials, conducted in a predominately adult population, demonstrated the efficacy of oxcarbazepine as monotherapy. Two trials compared oxcarbazepine to placebo and 2 trials used a randomized withdrawal design to compare a high dose (2400 mg) with a low dose (300 mg) of oxcarbazepine, after substituting oxcarbazepine 2400 mg/day for 1 or more antiepileptic drugs (AEDs). All doses were administered on a twice-a-day schedule. A fifth randomized, controlled, rater-blind, multicenter study, conducted in a pediatric population, failed to demonstrate a statistically significant difference between low and high dose oxcarbazepine treatment groups.
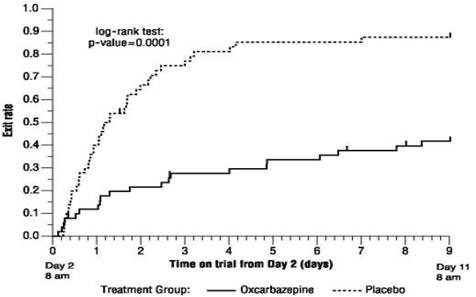
One placebo-controlled trial was conducted in 102 patients (11 to 62 years of age) with refractory partial-onset seizures who had completed an inpatient evaluation for epilepsy surgery. Patients had been withdrawn from all AEDs and were required to have 2 to 10 partial-onset seizures within 48 hours prior to randomization. Patients were randomized to receive either placebo or oxcarbazepine given as 1500 mg/day on Day 1 and 2400 mg/day thereafter for an additional 9 days, or until 1 of the following 3 exit criteria occurred: 1) the occurrence of a fourth partial-onset seizure, excluding Day 1, 2) 2 new-onset secondarily generalized seizures, where such seizures were not seen in the 1-year period prior to randomization, or 3) occurrence of serial seizures or status epilepticus. The primary measure of effectiveness was a between-group comparison of the time to meet exit criteria. There was a statistically significant difference in favor of oxcarbazepine (see Figure 1), p=0.0001.
Figure 1: Kaplan-Meier Estimates of Exit Rate by Treatment Group
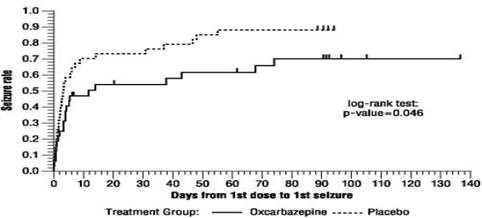
The second placebo-controlled trial was conducted in 67 untreated patients (8 to 69 years of age) with newly-diagnosed and recent-onset partial seizures. Patients were randomized to placebo or oxcarbazepine, initiated at 300 mg twice a day and titrated to 1200 mg/day (given as 600 mg twice a day) in 6 days, followed by maintenance treatment for 84 days. The primary measure of effectiveness was a between-group comparison of the time to first seizure. The difference between the 2 treatments was statistically significant in favor of oxcarbazepine (see Figure 2), p=0.046.
Figure 2: Kaplan-Meier Estimates of First Seizure Event Rate by Treatment Group
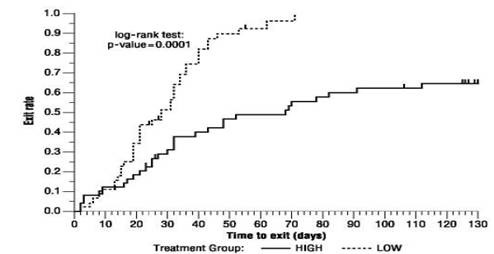
A third trial substituted oxcarbazepine monotherapy at 2400 mg/day for carbamazepine in 143 patients (12 to 65 years of age) whose partial-onset seizures were inadequately controlled on carbamazepine (CBZ) monotherapy at a stable dose of 800 to 1600 mg/day, and maintained this oxcarbazepine dose for 56 days (baseline phase). Patients who were able to tolerate titration of oxcarbazepine to 2400 mg/day during simultaneous carbamazepine withdrawal were randomly assigned to either 300 mg/day of oxcarbazepine or 2400 mg/day oxcarbazepine. Patients were observed for 126 days or until 1 of the following 4 exit criteria occurred: 1) a doubling of the 28-day seizure frequency compared to baseline, 2) a 2-fold increase in the highest consecutive 2-day seizure frequency during baseline, 3) a single generalized seizure if none had occurred during baseline, or 4) a prolonged generalized seizure. The primary measure of effectiveness was a between-group comparison of the time to meet exit criteria. The difference between the curves was statistically significant in favor of the oxcarbazepine 2400 mg/day group (see Figure 3), p=0.0001.
Figure 3: Kaplan-Meier Estimates of Exit Rate by Treatment Group
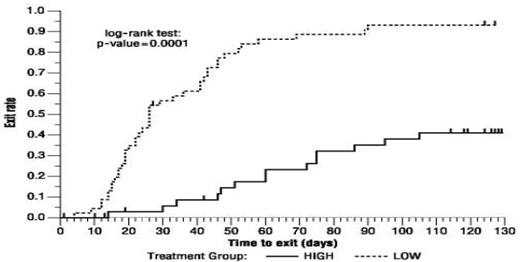
Another monotherapy substitution trial was conducted in 87 patients (11 to 66 years of age) whose seizures were inadequately controlled on 1 or 2 AEDs. Patients were randomized to either oxcarbazepine 2400 mg/day or 300 mg/day and their standard AED regimen(s) were eliminated over the first 6 weeks of double-blind therapy. Double-blind treatment continued for another 84 days (total double-blind treatment of 126 days) or until 1 of the 4 exit criteria described for the previous study occurred. The primary measure of effectiveness was a between-group comparison of the percentage of patients meeting exit criteria. The results were statistically significant in favor of the oxcarbazepine 2400 mg/day group (14/34; 41.2%) compared to the oxcarbazepine 300 mg/day group (42/45; 93.3%) (p<0.0001). The time to meeting one of the exit criteria was also statistically significant in favor of the oxcarbazepine 2400 mg/day group (see Figure 4), p=0.0001.
Figure 4: Kaplan-Meier Estimates of Exit Rate by Treatment Group
A monotherapy trial was conducted in 92 pediatric patients (1 month to 16 years of age) with inadequately-controlled or new-onset partial seizures. Patients were hospitalized and randomized to either oxcarbazepine 10 mg/kg/day or were titrated up to 40 to 60 mg/kg/day within 3 days while withdrawing the previous AED on the second day of oxcarbazepine. Seizures were recorded through continuous video-EEG monitoring from Day 3 to Day 5. Patients either completed the 5-day treatment or met 1 of the 2 exit criteria: 1) three study-specific seizures (i.e., electrographic partial-onset seizures with a behavioral correlate), 2) a prolonged study-specific seizure. The primary measure of effectiveness was a between-group comparison of the time to meet exit criteria in which the difference between the curves was not statistically significant (p=0.904). The majority of patients from both dose groups completed the 5-day study without exiting.
Although this study failed to demonstrate an effect of oxcarbazepine as monotherapy in pediatric patients, several design elements, including the short treatment and assessment period, the absence of a true placebo, and the likely persistence of plasma levels of previously administered AEDs during the treatment period, make the results uninterpretable. For this reason, the results do not undermine the conclusion, based on pharmacokinetic/pharmacodynamic considerations, that oxcarbazepine is effective as monotherapy in pediatric patients 4 years old and older.
14.2 Oxcarbazepine Adjunctive Therapy Trials
The effectiveness of oxcarbazepine as an adjunctive therapy for partial-onset seizures was established in 2 multicenter, randomized, double-blind, placebo-controlled trials, one in 692 patients (15 to 66 years of age) and one in 264 pediatric patients (3 to 17 years of age), and in one multicenter, rater-blind, randomized, age-stratified, parallel-group study comparing 2 doses of oxcarbazepine in 128 pediatric patients (1 month to <4 years of age).
Patients in the 2 placebo-controlled trials were on 1 to 3 concomitant AEDs. In both of the trials, patients were stabilized on optimum dosages of their concomitant AEDs during an 8-week baseline phase. Patients who experienced at least 8 (minimum of 1 to 4 per month) partial-onset seizures during the baseline phase were randomly assigned to placebo or to a specific dose of oxcarbazepine in addition to their other AEDs.
In these studies, the dose was increased over a 2-week period until either the assigned dose was reached, or intolerance prevented increases. Patients then entered a 14- (pediatrics) or 24-week (adults) maintenance period.
In the adult trial, patients received fixed doses of 600, 1200 or 2400 mg/day. In the pediatric trial, patients received maintenance doses in the range of 30 to 46 mg/kg/day, depending on baseline weight. The primary measure of effectiveness in both trials was a between-group comparison of the percentage change in partial-onset seizure frequency in the double-blind treatment phase relative to baseline phase. This comparison was statistically significant in favor of oxcarbazepine at all doses tested in both trials (p=0.0001 for all doses for both trials). The number of patients randomized to each dose, the median baseline seizure rate, and the median percentage seizure rate reduction for each trial are shown in Table 8. It is important to note that in the high-dose group in the study in adults, over 65% of patients discontinued treatment because of adverse events; only 46 (27%) of the patients in this group completed the 28-week study [see Adverse Reactions (6)], an outcome not seen in the monotherapy studies.
| 1 p=0.0001; * = number of seizures per 28 days. | ||||
|
Trial |
Treatment Group | |||
|
N |
Baseline
|
Median
|
||
|
1 (pediatrics) |
Oxcarbazepine |
136 |
12.5 |
34.81 |
|
Placebo |
128 |
13.1 |
9.4 |
|
|
2 (adults) |
Oxcarbazepine 2400 mg/day |
174 |
10 |
49.91 |
|
Oxcarbazepine 1200 mg/day |
177 |
9.8 |
40.21 |
|
|
Oxcarbazepine 600 mg/day |
168 |
9.6 |
26.41 |
|
|
Placebo |
173 |
8.6 |
7.6 |
|
Subset analyses of the antiepileptic efficacy of oxcarbazepine with regard to gender in these trials revealed no important differences in response between men and women. Because there were very few patients over the age of 65 years in controlled trials, the effect of the drug in the elderly has not been adequately assessed.
The third adjunctive therapy trial enrolled 128 pediatric patients (1 month to <4 years of age) with inadequately-controlled partial-onset seizures on 1 to 2 concomitant AEDs. Patients who experienced at least 2 study-specific seizures (i.e., electrographic partial-onset seizures with a behavioral correlate) during the 72-hour baseline period were randomly assigned to either oxcarbazepine 10 mg/kg/day or were titrated up to 60 mg/kg/day within 26 days. Patients were maintained on their randomized target dose for 9 days and seizures were recorded through continuous video-EEG monitoring during the last 72 hours of the maintenance period. The primary measure of effectiveness in this trial was a between-group comparison of the change in seizure frequency per 24 hours compared to the seizure frequency at baseline. For the entire group of patients enrolled, this comparison was statistically significant in favor of oxcarbazepine 60 mg/kg/day. In this study, there was no evidence that oxcarbazepine was effective in patients below the age of 2 years (N=75).
16 HOW SUPPLIED/STORAGE AND HANDLING
150 mg Film-Coated Tablets: yellow, film-coated oval, biconvex tablets with a deep break line on both sides and "G" engraved on one side of the deep break line on one side of the tablet and "13" and "7" engraved on either side of the deep break line on the other side of the tablet.
Bottle of 100.........NDC 68462-137-01
Bottle of 500.........NDC 68462-137-05
300 mg Film-Coated Tablets: yellow, film-coated oval, biconvex tablets with a deep break line on both sides and "G" and "4" engraved on either side of the deep break line on one side of the tablet.
Bottle of 100.........NDC 68462-138-01
Bottle of 500.........NDC 68462-138-05
600 mg Film-Coated Tablets: yellow, film-coated oval, biconvex tablets with a deep break line on both sides and "G" engraved on one side of the deep break line on one side of the tablet and "13" and "9" engraved on either side of the deep break line on the other side of the tablet.
Bottle of 100.........NDC 68462-139-01
Bottle of 500.........NDC 68462-139-05
Store at 20°C to 25°C (68°F to 77°F); excursions permitted to 15°C to 30°C (59°F to 86°F) [see USP Controlled Room Temperature]. Dispense in tight container (USP).
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Administration Information
Counsel patients that oxcarbazepine may be taken with or without food.
Hyponatremia
Advise patients that oxcarbazepine may reduce the serum sodium concentrations especially if they are taking other medications that can lower sodium. Instruct patients to report symptoms of low sodium like nausea, tiredness, lack of energy, confusion, and more frequent or more severe seizures [see Warnings and Precautions (5.1)].
Anaphylactic Reactions and Angioedema
Anaphylactic reactions and angioedema may occur during treatment with oxcarbazepine. Advise patients to report immediately signs and symptoms suggesting angioedema (swelling of the face, eyes, lips, tongue or difficulty in swallowing or breathing) and to stop taking the drug until they have consulted with their physician [see Warnings and Precautions (5.2)].
Cross Hypersensitivity Reaction to Carbamazepine
Inform patients who have exhibited hypersensitivity reactions to carbamazepine that approximately 25% to 30% of these patients may experience hypersensitivity reactions with oxcarbazepine. Patients should be advised that if they experience a hypersensitivity reaction while taking oxcarbazepine they should consult with their physician immediately [see Warnings and Precautions (5.3)].
Serious Dermatological Reactions
Advise patients that serious skin reactions have been reported in association with oxcarbazepine. In the event a skin reaction should occur while taking oxcarbazepine, patients should consult with their physician immediately [see Warnings and Precautions (5.4)].
Suicidal Behavior and Ideation
Patients, their caregivers, and families should be counseled that AEDs, including oxcarbazepine, may increase the risk of suicidal thoughts and behavior and should be advised of the need to be alert for the emergence or worsening of symptoms of depression, any unusual changes in mood or behavior, or the emergence of suicidal thoughts, behavior, or thoughts about self-harm. Behaviors of concern should be reported immediately to healthcare providers [see Warnings and Precautions (5.5)].
Driving and Operating Machinery
Advise patients that oxcarbazepine may cause adverse reactions such as dizziness, somnolence, ataxia, visual disturbances, and depressed level of consciousness. Accordingly, advise patients not to drive or operate machinery until they have gained sufficient experience on oxcarbazepine to gauge whether it adversely affects their ability to drive or operate machinery [see Warnings and Precautions (5.7) and Adverse Reactions (6)].
Multi-Organ Hypersensitivity
Instruct patients that a fever associated with other organ system involvement (e.g., rash, lymphadenopathy, hepatic dysfunction) may be drug-related and should be reported to their healthcare provider immediately [see Warnings and Precautions (5.8)].
Hematologic Events
Advise patients that there have been rare reports of blood disorders reported in patients treated with oxcarbazepine. Instruct patients to immediately consult with their physician if they experience symptoms suggestive of blood disorders [see Warnings and Precautions (5.9)].
Drug Interactions
Caution female patients of reproductive potential that the concurrent use of oxcarbazepine with hormonal contraceptives may render this method of contraception less effective [seeDrug Interactions (7.2) and Use in Specific Populations (8.1)]. Additional non-hormonal forms of contraception are recommended when using oxcarbazepine.
Caution should be exercised if alcohol is taken in combination with oxcarbazepine, due to a possible additive sedative effect.
Pregnancy Registry
Encourage patients to enroll in the North American Antiepileptic Drug (NAAED) Pregnancy Registry if they become pregnant. This registry is collecting information about the safety of antiepileptic drugs during pregnancy [see Use in Specific Populations (8.1)].
MEDICATION GUIDE
Oxcarbazepine Tablets
(ox kar baz' e peen),
for oral use
What is the most important information I should know about oxcarbazepine tablets?
Do not stop taking oxcarbazepine tablets without first talking to your healthcare provider. Stopping oxcarbazepine tablets suddenly can cause serious problems.
Oxcarbazepine tablets can cause serious side effects, including:
1. Oxcarbazepine tablets may cause the level of sodium in your blood to be low. Symptoms of low blood sodium include:
|
|
Similar symptoms that are not related to low sodium may occur from taking oxcarbazepine tablets. You should tell your healthcare provider if you have any of these side effects and if they bother you or they do not go away.
Some other medicines can also cause low sodium in your blood. Be sure to tell your healthcare provider about all the other medicines that you are taking.
Your healthcare provider may do blood tests to check your sodium levels during your treatment with oxcarbazepine tablets.
2. Oxcarbazepine tablets may also cause allergic reactions or serious problems which may affect organs and other parts of your body like the liver or blood cells. You may or may not have a rash with these types of reactions.
- Call your healthcare provider right away if you have any of the following:
|
|
Many people who are allergic to carbamazepine are also allergic to oxcarbazepine tablets. Tell your healthcare provider if you are allergic to carbamazepine.
3. Like other antiepileptic drugs, oxcarbazepine tablets may cause suicidal thoughts or actions in a very small number of people, about 1 in 500.
Call a healthcare provider right away if you have any of these symptoms, especially if they are new, worse, or worry you:
|
|
How can I watch for early symptoms of suicidal thoughts and actions?
- •
- Pay attention to any changes, especially sudden changes, in mood, behaviors, thoughts, or feelings.
- •
- Keep all follow-up visits with your healthcare provider as scheduled.
Call your healthcare provider between visits as needed, especially if you are worried about symptoms.
Do not stop taking oxcarbazepine tablets without first talking to a healthcare provider.
- •
- Stopping oxcarbazepine tablets suddenly can cause serious problems.
- •
- Stopping a seizure medicine suddenly in a patient who has epilepsy may cause seizures that will not stop (status epilepticus).
Suicidal thoughts or actions may be caused by things other than medicines. If you have suicidal thoughts or actions, your healthcare provider may check for other causes.
What are oxcarbazepine tablets?
Oxcarbazepine tablets are a prescription medicine used:
- •
- alone or with other medicines to treat partial-onset seizures in adults
- •
- alone to treat partial-onset seizures in children 4 years and older
- •
- with other medicines to treat partial-onset seizures in children 2 years and older
It is not known if oxcarbazepine tablets are safe and effective for use alone to treat partial-onset seizures in children less than 4 years of age or for use with other medicines to treat partial-onset seizures in children less than 2 years of age.
Do not take oxcarbazepine tablets if you are allergic to oxcarbazepine tablets or any of the other ingredients in oxcarbazepine tablets, or to eslicarbazepine acetate. See the end of this Medication Guide for a complete list of ingredients in oxcarbazepine tablets.
Many people who are allergic to carbamazepine are also allergic to oxcarbazepine tablets. Tell your healthcare provider if you are allergic to carbamazepine.
Before taking oxcarbazepine tablets, tell your healthcare provider about all your medical conditions, including if you:
- •
- have or have had suicidal thoughts or actions, depression or mood problems
- •
- have liver problems
- •
- have kidney problems
- •
- are allergic to carbamazepine. Many people who are allergic to carbamazepine are also allergic to oxcarbazepine tablets.
- •
- use birth control medicine. Oxcarbazepine tablets may cause your birth control medicine to be less effective. Talk to your healthcare provider about the best birth control method to use.
- •
- are pregnant or plan to become pregnant. Oxcarbazepine tablets may harm your unborn baby. Tell your healthcare provider right away if you become pregnant while taking oxcarbazepine tablets. You and your healthcare provider will decide if you should take oxcarbazepine tablets while you are pregnant.
If you become pregnant while taking oxcarbazepine tablets, talk to your healthcare provider about registering with the North American Antiepileptic Drug (NAAED) Pregnancy Registry. The purpose of this registry is to collect information about the safety of antiepileptic medicine during pregnancy. You can enroll in this registry by calling 1-888-233-2334.
- •
- are breastfeeding or plan to breastfeed oxcarbazepine passes into breast milk. Talk with your healthcare provider about the best way to feed your baby if you take oxcarbazepine.
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. Taking oxcarbazepine tablets with certain other medicines may cause side effects or affect how well they work. Do not start or stop other medicines without talking to your healthcare provider.
Know the medicines you take. Keep a list of them to show your healthcare provider and pharmacist when you get a new medicine.
How should I take oxcarbazepine tablets?
- •
- Do not stop taking oxcarbazepine tablets without talking to your healthcare provider. Stopping oxcarbazepine tablets suddenly can cause serious problems, including seizures that will not stop (status epilepticus).
- •
- Take oxcarbazepine tablets exactly as prescribed. Your healthcare provider may change your dose. Your healthcare provider will tell you how much oxcarbazepine tablets to take.
- •
- Take oxcarbazepine tablets 2 times a day.
- •
- Take oxcarbazepine tablets with or without food.
- •
- If you take too much oxcarbazepine tablets, call your healthcare provider right away.
What should I avoid while taking oxcarbazepine tablets?
- •
- Do not drive or operate machinery until you know how oxcarbazepine tablets affects you. Oxcarbazepine tablets may slow your thinking and motor skills.
- •
- Do not drink alcohol or take other drugs that make you sleepy or dizzy while taking oxcarbazepine tablets until you talk to your healthcare provider. Oxcarbazepine tablets taken with alcohol or drugs that cause sleepiness or dizziness may make your sleepiness or dizziness worse.
What are the possible side effects of oxcarbazepine tablets?
See "What is the most important information I should know about oxcarbazepine tablets?"
Oxcarbazepine tablets may cause other serious side effects including:
- •
- trouble concentrating
- •
- problems with your speech and language
- •
- feeling confused
- •
- feeling sleepy and tired
- •
- trouble with walking and coordination
- •
- seizures that can happen more often or become worse, especially in children
Get medical help right away if you have any of the symptoms listed above or listed in "What is the most important information I should know about oxcarbazepine tablets?"
The most common side effects of oxcarbazepine tablets include:
|
|
These are not all the possible side effects of oxcarbazepine tablets. Tell your healthcare provider if you have any side effect that bothers you or that does not go away.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store oxcarbazepine tablets?
- •
- Store oxcarbazepine film-coated tablets at 20°C to 25°C (68°F to 77°F); excursions permitted to 15°C to 30°C (59°F to 86°F).
- •
- Keep oxcarbazepine film-coated tablets dry.
Keep oxcarbazepine tablets and all medicines out of the reach of children.
General Information about the safe and effective use of oxcarbazepine tablets.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use oxcarbazepine tablets for a condition for which it was not prescribed. Do not give oxcarbazepine tablets to other people, even if they have the same symptoms that you have. It may harm them.
You can ask your pharmacist or healthcare provider for information about oxcarbazepine tablets that is written for health professionals.
What are the ingredients in oxcarbazepine tablets?
Active ingredient:s oxcarbazepine
Inactive ingredients: colloidal silicon dioxide, crospovidone, ferric oxide (yellow), hypromellose, magnesium stearate, meglumine, microcrystalline cellulose, polyethylene glycol, and titanium dioxide.
Medication Guide available at
www.glenmarkpharma-us.com/medguides
Manufactured by:
Glenmark Pharmaceuticals Limited
India
Manufactured for:

Glenmark Pharmaceuticals Inc., USA
Mahwah, NJ 07430
Questions? 1 (888)721-7115
August 2019
This Medication Guide has been approved by the U.S. Food and Drug Administration