October 12, 2022
Important Prescribing Information
Temporary Importation of Fludarabine Phosphate Injection USP from Canada to Address Drug Shortage
Dear Healthcare Professional:
Due to the current critical shortage of Fludarabine Phosphate Injection USP products in the United States (U.S.) market, Accord Healthcare Inc., USA (Accord) is coordinating with the U.S. Food and Drug Administration (FDA) to temporarily import unapproved Fludarabine Phosphate Injection USP [50 mg/2 mL (25 mg/mL)] into the U.S. market. The Fludarabine Phosphate Injection USP from Accord Healthcare Inc., is marketed in Canada
Effective immediately, and during this temporary period of shortage, Accord will offer the following presentation of Fludarabine Phosphate Injection USP from Canada to the U.S. market:
|
Product Name & Description |
Strength/ Presentation |
Dosage Form |
Package size |
NDC |
|
Fludarabine Phosphate Injection, USP |
50 mg/2 mL (25 mg/mL) |
Injectable |
2 mL, Single Dose, Clear Glass Vial with Orange Flip-Off Seal |
16729-131-30 |
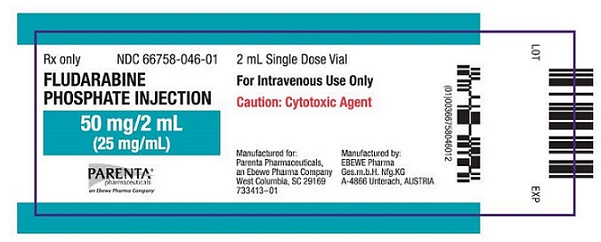
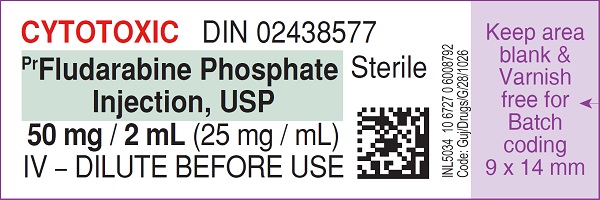
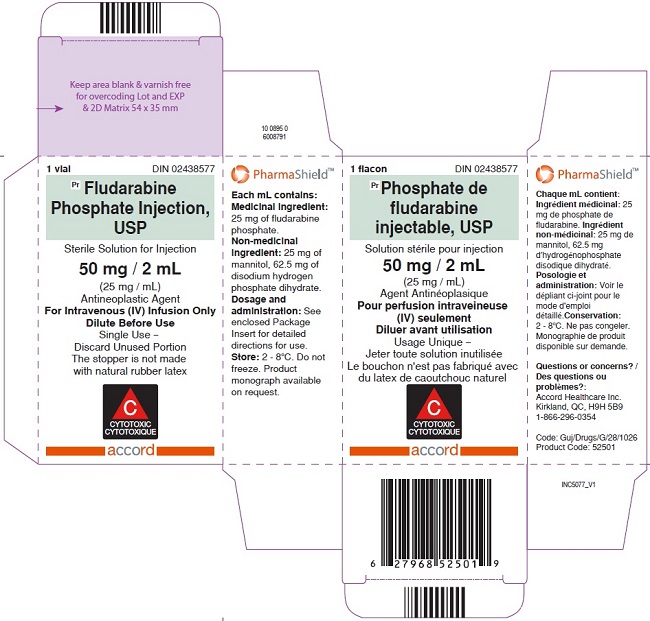
The vial and carton labels will display the text used and approved for marketing the products in Canada with both English and French translations. It is important to note that there are differences in the format and content of the labeling as mentioned below between the US approved product and Accords Fludarabine Phosphate Injection USP. Specifically, the preparation and stability of this product differs from the U.S. version. Please see the product comparison table at the end of this letter.
Table 1. Key differences in Fludarabine Phosphate Injection USP
- Vial container label
- Vial carton label
- Ingredients
- Compatibility and storage
- How supplied
- Indication
- Recommended dose
- Contraindications
- Drug Interactions
- Overdosage
- Boxed Warning
- Warnings and Precautions
- Adverse Reactions
- Use in Specific Populations
The barcode on the imported product label may not register accurately on the U.S. scanning systems. Institutions should manually input the imported product information into their systems and confirm that the barcode, if scanned, provides correct information. Alternative procedures should be followed to assure that the correct drug product is being used and administered to individual patients.
In addition, the packaging of the imported product does not include serialization information. Accords Fludarabine Phosphate Injection USP does not meet the Drug Supply Chain Security Act (DSCSA) requirements for the Interoperable Exchange of Information for Tracing of Human, Finished Prescription Drugs.
Fludarabine Phosphate Injection USP is available only by prescription in the U.S. Please refer to the package insert for the FDA-approved Fludarabine Phosphate Injection USP drug product for full prescribing information
To report adverse events associated with the use of this product, Healthcare providers should report to Accord Healthcare Inc at 1-866-941-7875.
To report quality problems, or if you have any questions about the information contained in this letter or the use of Accords Fludarabine Phosphate Injection USP, please contact Accord Healthcare Inc at 1-866-941-7875 or at accord_usa@accord-healthcare.com.
Adverse events or quality problems experienced with the use of this product may also be reported to the FDAs MedWatch Adverse Event Reporting Program either online, by regular mail, or by fax:
- Complete and submit the report Online: www.fda.gov/medwatch/report.htm
- Regular mail or Fax: Download form www.fda.gov/MedWatch/getforms.htm or call 1-800-332-1088 to request a reporting form, then complete and return to the address on the pre-addressed form or submit by fax to 1-800-FDA-0178 (1-800-332-0178).
To place an order, please contact Accord at csaccord@intaspharma.com.
We remain at your disposal to answer any questions you may have about our product; and provide more information if needed.
Sincerely,
Sabita Nair, RAC, ASQ-CPGP
Vice President-Regulatory Affairs
Accord Healthcare, Inc.
|
US FDA Approved Product |
Imported Product |
|||||||||||
|
Vial container label |
|
|
||||||||||
|
Vial carton label |
|
|
||||||||||
|
Product name |
Fludarabine Phosphate Injection 50 mg/2 mL |
PrFludarabine Phosphate Injection, USP 50 mg/2 mL |
||||||||||
|
Route of administration |
For Intravenous use only |
For Intravenous use only |
||||||||||
|
Specific information |
Cytotoxic agent |
Cytotoxic |
||||||||||
|
Ingredients |
Each mL contains 25 mg of the active ingredient fludarabine phosphate, 1.78 mg disodium phosphate dihydrate, water for injection and sodium hydroxide to adjust pH to 7.5. The pH range for the final product is 7.3 to 7.7. Fludarabine Phosphate Injection is a sterile solution intended for intravenous administration. |
Each mL contains 25 mg of the active ingredient fludarabine phosphate, 25 mg mannitol, 62.5 mg of disodium hydrogen phosphate dehydrate and water for injection. The pH range of the final solution is 6.0-7.1. FLUDARABINE PHOSPHATE INJECTION, USP is supplied as a colourless to slightly brown yellow, sterile solution for intravenous administration. |
||||||||||
|
Compatibility and storage |
Fludarabine Phosphate Injection contains no antimicrobial preservative and should be used within 8 hours of opening. Care must be taken to assure sterility of infusion solutions. Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. |
The product must be further diluted for intravenous infusion administration in PVC bags to a concentration of 1 mg/mL in 5% Dextrose Injection USP, or in 0.9% Sodium Chloride Injection USP. Use within 24 hours when kept at room temperature and 72 hours when refrigerated. FLUDARABINE PHOSPHATE INJECTION, USP contains no antimicrobial preservative and thus care must be taken to ensure the sterility of prepared solutions. |
||||||||||
|
Incompatibilities |
Fludarabine Phosphate Injection should not be mixed with other drugs. |
The formulation for intravenous use must not be mixed with other drugs. |
||||||||||
|
Storage condition |
Store in a refrigerator between 2° and 8°C (36° to 46°F). |
Store FLUDARABINE PHOSPHATE INJECTION, USP under refrigeration between 2°C and 8°C. Do not freeze. Discard unused portion. |
||||||||||
|
How supplied |
Fludarabine Phosphate Injection is supplied as a sterile solution containing 25 mg of fludarabine phosphate in a single use vial. NDC 66758-046-01 one carton containing 1 vial of Fludarabine Phosphate Injection. |
FLUDARABINE PHOSPHATE INJECTION, USP is supplied in a 2 mL, single dose, clear glass vial with orange flip-off seal, packaged individually. |
||||||||||
|
Indication |
Fludarabine Phosphate Injection is indicated for the treatment of adult patients with B-cell chronic lymphocytic leukemia (CLL) who have not responded to or whose disease has progressed during treatment with at least one standard alkylating agent containing regimen. The safety and effectiveness of Fludarabine Phosphate Injection in previously untreated or nonrefractory patients with CLL have not been established. |
FLUDARABINE PHOSPHATE INJECTION, USP is indicated for:
|
||||||||||
|
Recommended dose |
The recommended adult dose of Fludarabine Phosphate Injection is 25 mg/m 2 administered intravenously over a period of approximately 30 minutes daily for five consecutive days. Each 5-day course of treatment should commence every 28 days. Dosage may be decreased or delayed based on evidence of hematologic or nonhematologic toxicity. Physicians should consider delaying or discontinuing the drug if neurotoxicity occurs. A number of clinical settings may predispose to increased toxicity from Fludarabine Phosphate Injection. These include advanced age, renal impairment, and bone marrow impairment. Such patients should be monitored closely for excessive toxicity and the dose modified accordingly. The optimal duration of treatment has not been clearly established. It is recommended that three additional cycles of Fludarabine Phosphate Injection be administered following the achievement of a maximal response and then the drug should be discontinued. |
The usual starting dose of FLUDARABINE PHOSPHATE INJECTION, USP (fludarabine phosphate) is 25 mg/m 2 administered intravenously over a period of approximately 30 minutes, daily for five days every 28 days. Dosage may be decreased based on evidence of hematologic or nonhematologic toxicity. Note that in patients with decreased renal function (creatinine clearance between 30 and 70 mL/min) the dose should be reduced by up to 50%. FLUDARABINE PHOSPHATE INJECTION, USP (fludarabine phosphate) treatment is contraindicated, if creatinine clearance is < 30 mL/min. (See WARNINGS AND PRECAUTIONS). The duration of treatment depends on the treatment success and the tolerability of the drug. FLUDARABINE PHOSPHATE INJECTION, USP should be administered until the achievement of a maximal response (complete or partial remission, usually 6 cycles) and then the drug should be discontinued. |
||||||||||
|
Contraindications |
None |
|
||||||||||
|
Drug Interactions |
Pentostatin: The use of Fludarabine Phosphate Injection in combination with pentostatin is not recommended due to the risk of fatal pulmonary toxicity. [see Warnings and Precautions (5.5)] |
Serious Drug Interactions: In a clinical investigation using fludarabine phosphate in combination with pentostatin (deoxycoformycin) for the treatment of refractory CLL, there was an unacceptably high incidence of fatal pulmonary toxicity. Therefore, the use of FLUDARABINE PHOSPHATE INJECTION, USP in combination with pentostatin is contraindicated. |
||||||||||
|
|
||||||||||||
|
For management of a suspected drug overdose, contact your regional Poison Control Centre. |
||||||||||||
|
Overdosage |
High doses of fludarabine phosphate [see Warnings and Precautions (5)] have been associated with an irreversible central nervous system toxicity characterized by delayed blindness, coma and death. High doses are also associated with severe thrombocytopenia and neutropenia due to bone marrow suppression. There is no known specific antidote for fludarabine phosphate overdosage. Treatment consists of drug discontinuation and supportive therapy. |
Higher than recommended doses of fludarabine phosphate have been associated with leukoencephalopathy, acute toxic leukoencephalopathy, or posterior reversible encephalopathy syndrome (PRES)/ reversible posterior leukoencephalopathy syndrome (RPLS). Symptoms, which may be delayed and irreversible, may include headache, nausea and vomiting, seizures, visual disturbances such as vision loss, altered sensorium, focal neurological deficits, coma, and death. Additional effects may include optic neuritis, and papillitis, confusion, somnolence, agitation, paraparesis/ quadriparesis, muscle spasticity and incontinence. High doses are also associated with bone marrow suppression manifested by thrombocytopenia and neutropenia. There is no known specific antidote for fludarabine phosphate overdosage. Treatment consists of drug discontinuation and supportive therapy. |
||||||||||
|
Boxed Warning |
SEVERE BONE MARROW SUPPRESSION, CNS TOXICITY, HEMOLYTIC ANEMIA, AND PULMONARY TOXICITY Fludarabine Phosphate Injection should be administered under the supervision of a qualified physician experienced in the use of antineoplastic therapy. Fludarabine phosphate injection can severely suppress bone marrow function. When used at high doses in dose-ranging studies in patients with acute leukemia, fludarabine phosphate injection was associated with severe neurologic effects, including blindness, coma, and death. This severe central nervous system toxicity occurred in 36% of patients treated with doses approximately four times greater (96 mg/m 2/day for 5 to 7 days) than the recommended dose. Similar severe central nervous system toxicity, including coma, seizures, agitation and confusion, has been reported in patients treated at doses in the range of the dose recommended for chronic lymphocytic leukemia. [see Warnings and Precautions (5.2)] Instances of life-threatening and sometimes fatal autoimmune phenomena such as hemolytic anemia, autoimmune thrombocytopenia / thrombocytopenic purpura (ITP), Evans syndrome, and acquired hemophilia have been reported to occur after one or more cycles of treatment with fludarabine phosphate injection. Patients undergoing treatment with Fludarabine Phosphate Injection should be evaluated and closely monitored for hemolysis. [see Warnings and Precautions (5.3)] In a clinical investigation using fludarabine phosphate in combination with pentostatin (deoxycoformycin) for the treatment of refractory chronic lymphocytic leukemia (CLL), there was an unacceptably high incidence of fatal pulmonary toxicity. Therefore, the use of Fludarabine Phosphate Injection in combination with pentostatin is not recommended [see Warnings and Precautions (5.5)] |
Serious Warnings and Precautions FLUDARABINE PHOSPHATE INJECTION, USP should be administered under the supervision of, or prescribed by, a qualified physician experienced in the use of antineoplastic therapy. Fludarabine phosphate is associated with:
In a clinical investigation using fludarabine phosphate in combination with pentostatin (deoxycoformycin) for the treatment of refractory CLL, there was an unacceptably high incidence of fatal pulmonary toxicity. Therefore, the use of FLUDARABINE PHOSPHATE INJECTION, USP in combination with pentostatin is contraindicated. |
||||||||||
|
Warnings and Precautions |
5 WARNINGS AND PRECAUTIONS 5.1 Dose Dependent Neurologic Toxicities There are clear dose dependent toxic effects seen with fludarabine phosphate. Dose levels approximately 4 times greater (96 mg/m 2/day for 5 to 7 days) than that recommended for CLL (25 mg/m 2/day for 5 days) were associated with a syndrome characterized by delayed blindness, coma and death. Symptoms appeared from 21 to 60 days following the last dose. Thirteen of 36 patients (36%) who received fludarabine phosphate at high doses (96 mg/m 2/day for 5 to 7 days) developed this severe neurotoxicity. Similar severe central nervous system toxicity, including coma, seizures, agitation and confusion, has been reported in patients treated at doses in the range of the dose recommended for chronic lymphocytic leukemia. In postmarketing experience neurotoxicity has been reported to occur either earlier or later than in clinical trials (range 7 to 225 days). The effect of chronic administration of fludarabine phosphate on the central nervous system is unknown; however, patients have received the recommended dose for up to 15 courses of therapy. Fludarabine phosphate may reduce the ability to drive or use mechanical equipment, since fatigue, weakness, visual disturbances, confusion, agitation and seizures have been observed. 5.2 Bone Marrow Suppression Severe bone marrow suppression, notably anemia, thrombocytopenia and neutropenia, has been reported in patients treated with fludarabine phosphate. In a Phase I study in adult solid tumor patients, the median time to nadir counts was 13 days (range, 3 to 25 days) for granulocytes and 16 days (range, 2 to 32 days) for platelets. Most patients had hematologic impairment at baseline either as a result of disease or as a result of prior myelosuppressive therapy. Cumulative myelosuppression may be seen. While chemotherapy-induced myelosuppression is often reversible, administration of Fludarabine Phosphate Injection requires careful hematologic monitoring. Several instances of trilineage bone marrow hypoplasia or aplasia resulting in pancytopenia, sometimes resulting in death, have been reported in adult patients. The duration of clinically significant cytopenia in the reported cases has ranged from approximately 2 months to approximately 1 year. These episodes have occurred both in previously treated or untreated patients. 5.3 Autoimmune Reactions Instances of life-threatening and sometimes fatal autoimmune phenomena such as hemolytic anemia, autoimmune thrombocytopenia/thrombocytopenic purpura (ITP), Evans syndrome, and acquired hemophilia have been reported to occur after one or more cycles of treatment with fludarabine phosphate in patients with or without a previous history of autoimmune hemolytic anemia or a positive Coombs' test and who may or may not be in remission from their disease. Steroids may or may not be effective in controlling these hemolytic episodes. The majority of patients rechallenged with fludarabine phosphate developed a recurrence in the hemolytic process. The mechanism(s) which predispose patients to the development of this complication has not been identified. Patients undergoing treatment with Fludarabine Phosphate Injection should be evaluated and closely monitored for hemolysis. Discontinuation of therapy with Fludarabine Phosphate Injection is recommended in case of hemolysis. 5.4 Transfusion Associated Graft-Versus-Host Disease Transfusion-associated graft-versus-host disease has been observed after transfusion of non-irradiated blood in fludarabine phosphate treated patients. Fatal outcome as a consequence of this disease has been reported. Therefore, to minimize the risk of transfusion-associated graft-versus-host disease, patients who require blood transfusion and who are undergoing, or who have received, treatment with Fludarabine Phosphate Injection should receive irradiated blood only. 5.5 Pulmonary Toxicity In a clinical investigation using fludarabine phosphate in combination with pentostatin (deoxycoformycin) for the treatment of refractory chronic lymphocytic leukemia (CLL) in adults, there was an unacceptably high incidence of fatal pulmonary toxicity. Therefore, the use of Fludarabine Phosphate Injection in combination with pentostatin is not recommended. 5.6 Pregnancy Pregnancy Category D Based on its mechanism of action, fludarabine phosphate can cause fetal harm when administered to a pregnant woman. There are no adequate and well-controlled studies of fludarabine phosphate injection in pregnant women, Fludarabine phosphate was embryolethal and teratogenic in rats and rabbits. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to the fetus. Women of childbearing potential should be advised to avoid becoming pregnant. [see Use in Specific Populations (8.1)] 5.7 Male Fertility and Reproductive Outcomes Males with female sexual partners of childbearing potential should use contraception during and after cessation of fludarabine phosphate therapy. Fludarabine phosphate may damage testicular tissue and spermatozoa. Possible sperm DNA damage raises concerns about loss of fertility and genetic abnormalities in fetuses. The duration of this effect is uncertain. [see Nonclinical Toxicology (13.1)] 5.8 Tumor Lysis Tumor lysis syndrome has been associated with fludarabine phosphate treatment. This syndrome has been reported in CLL patients with large tumor burdens. Since fludarabine phosphate can induce a response as early as the first week of treatment, precautions should be taken in those patients at risk of developing this complication. 5.9 Renal Impairment Fludarabine Phosphate Injection must be administered cautiously in patients with renal impairment. The total body clearance of 2-fluoro-ara-A has been shown to be directly correlated with creatinine clearance. Patients with creatinine clearance 30 to 79 mL/min should have their fludarabine phosphate dose reduced and be monitored closely for excessive toxicity. Fludarabine phosphate should not be administered to patients with creatinine clearance less than 30 mL/min. [see Dosage and Administration (2.2) and Use in Specific Populations (8.6)] In patients aged 65 years or older, creatinine clearance should be measured before start of treatment. 5.10 Vaccination During and after treatment with Fludarabine Phosphate Injection, vaccination with live vaccines should be avoided. |
General FLUDARABINE PHOSPHATE INJECTION, USP is a potent antineoplastic agent with potentially significant toxic side effects. Patients undergoing therapy should be closely observed for signs of hematologic and nonhematologic toxicity. Periodic assessment of peripheral blood counts is recommended to detect the development of neutropenia, thrombocytopenia, anemia and leukopenia. Vaccination with live vaccines should be avoided during and after treatment with FLUDARABINE PHOSPHATE INJECTION, USP. Carcinogenesis and Mutagenesis Disease progression and transformation (eg, Richters Syndrome) have been commonly reported in CLL patients (see WARNINGS AND PRECAUTIONS - Skin). Endocrine and Metabolism Tumor lysis syndrome associated with fludarabine phosphate treatment has been reported in CLL patients with large tumor burdens. Since FLUDARABINE PHOSPHATE INJECTION, USP can induce a response as early as the first week of treatment, precautions should be taken in those patients at risk of developing this complication. Gastrointestinal In clinical trials with oral fludarabine phosphate, nausea/vomiting and/or diarrhea were reported in approximately 38% of patients. In most cases, the severity was mild to moderate (WHO toxicity grading). Only a small percentage of patients, approximately 1 % with nausea/vomiting and 5% with diarrhea, required therapy. Patients with prolonged, clinically relevant, nausea/vomiting and diarrhea should be closely monitored to avoid dehydration. Hematologic In patients with an impaired state of health, FLUDARABINE PHOSPHATE INJECTION, USP should be given with caution and after careful risk/benefit consideration. This applies especially to patients with severe impairment of bone marrow function (thrombocytopenia, anemia, and/or granulocytopenia), immunodeficiency or with a history of opportunistic infection. Prophylactic treatment should be considered in patients at increased risk of developing opportunistic infections (see ADVERSE REACTIONS). Severe bone marrow suppression, notably thrombocytopenia, anemia, leukopenia and neutropenia, may occur with administration of FLUDARABINE PHOSPHATE INJECTION, USP and requires careful hematologic monitoring. In a Phase I study in solid tumor patients, the median time to nadir counts was 13 days (range, 3- 25 days) for granulocytes and 16 days (range, 2-32 days) for platelets. Most patients had hematologic impairment at baseline either as a result of disease or as a result of prior myelosuppressive therapy. Cumulative myelosuppression may be seen. While chemotherapy-induced myelosuppression is often reversible, administration of FLUDARABINE PHOSPHATE INJECTION, USP requires careful hematologic monitoring. Several instances of trilineage bone marrow hypoplasia or aplasia resulting in pancytopenia, sometimes resulting in death, have been reported in adult patients. The duration of clinically significant cytopenia in the cases reported has ranged from approximately 2 months to approximately 1 year. These episodes have occurred in both previously treated and untreated patients. Instances of life-threatening and sometimes fatal autoimmune phenomena (e.g. autoimmune hemolytic anemia, autoimmune thrombocytopenia, thrombocytopenic purpura, pemphigus, acquired hemophilia and Evans' syndrome) have been reported to occur during or after treatment with fludarabine phosphate in patients with or without a previous history of autoimmune processes or a positive Coombs' test and who may or may not be in remission from their disease. Steroids may or may not be effective in controlling these hemolytic episodes. One study was performed with 31 patients with hemolytic anemia related to the administration of fludarabine phosphate. Since the majority (90%) of these patients rechallenged with fludarabine phosphate developed a recurrence in the hemolytic process, rechallenge with FLUDARABINE PHOSPHATE INJECTION, USP should be avoided. The mechanisms which predispose patients to the development of this complication have not been identified. Patients undergoing treatment with FLUDARABINE PHOSPHATE INJECTION, USP should be evaluated and closely monitored for signs of autoimmune hemolytic anemia (a decline in hemoglobin linked with hemolysis and a positive Coombs' test). Discontinuation of therapy with FLUDARABINE PHOSPHATE INJECTION, USP is recommended in the event of hemolysis. The transfusion of irradiated blood and the administration of corticosteroids are the most common treatment measures for autoimmune hemolytic anemia. Hepatic/Biliary/Pancreatic No data are available concerning the use of fludarabine phosphate in patients with hepatic impairment. In this group of patients, FLUDARABINE PHOSPHATE INJECTION, USP should be used with caution and administered if the perceived benefit outweighs any potential risk. Immune Transfusion-associated graft-versus-host disease (reaction by the transfused immunocompetent lymphocytes to the host) has been observed after transfusion of nonirradiated blood in patients treated with fludarabine phosphate. Fatal outcome as a consequence of this disease has been reported with a high frequency. Therefore, to minimize the risk of transfusion-associated graft-versus-host disease, patients who require blood transfusion and who are undergoing or who have received treatment with FLUDARABINE PHOSPHATE INJECTION, USP should receive irradiated blood only. Neurologic Administration of fludarabine phosphate can be associated with leukoencephalopathy (LE), acute toxic leukoencephalopathy (ATL), or posterior reversible encephalopathy syndrome (PRES)/ reversible posterior leukoencephalopathy syndrome (RPLS). LE, ATL or PRES/RPLS may occur:
When high doses of fludarabine phosphate were administered in dose-ranging studies in acute leukemia patients, a syndrome with delayed onset, characterized by blindness, coma, and death was identified. Symptoms appeared from 21 to 60 days post dosing (however, in post marketing experience, cases of neurotoxicity have been reported to occur both earlier and later than seen in clinical trials). Demyelination, especially of the occipital cortex of the brain was noted. The majority of these cases occurred in patients treated intravenously with doses approximately four times greater (96 mg/m 2/day for 5-7 days) than the recommended dose. Thirteen of 36 patients (36.1%) who received fludarabine phosphate at high doses ( 96 mg/m 2/day for 5 to 7 days per course) developed severe neurotoxicity, while only one of 443 patients (0.2%) who received the drug at low doses ( 40 mg/m2/day for 5 days per course) developed the toxicity. In patients treated at doses in the range of the dose recommended for CLL, Lg-NHL, severe central nervous system toxicity occurred rarely (coma, seizures and agitation) or uncommonly (confusion). LE, ATL or PRES/RPLS symptoms may include headache, nausea and vomiting, seizures, visual disturbances such as vision loss, altered sensorium, and focal neurological deficits. Additional effects may include optic neuritis, and papillitis, confusion, somnolence, agitation, paraparesis/quadriparesis, muscle spasticity, incontinence, and coma. The onset of the neurologic symptoms can be delayed and may occur after discontinuation of fludarabine. Late-occurring encephalopathy has been reported up to 4.8 years following fludarabine. LE/ ATL/ PRES/RPLS may be irreversible, life-threatening, or fatal. The effect of chronic administration of fludarabine phosphate on the central nervous system is unknown. In some studies, however, patients tolerated the recommended dose, for relatively long treatment periods (up to 26 courses of therapy). Periodic neurological assessments are recommended. Whenever LE, ATL or PRES/RPLS is suspected, FLUDARABINE PHOSPHATE INJECTION, USP treatment should be stopped. Patients should be monitored and should undergo brain imaging, preferably utilizing MRI. If the diagnosis is confirmed, FLUDARABINE PHOSPHATE INJECTION, USP therapy should be permanently discontinued. Renal The total body clearance of the principal plasma metabolite 2F-ara-A shows a correlation with creatinine clearance, indicating the importance of the renal excretion pathway for the elimination of the compound. Patients with reduced renal function demonstrated an increased total body exposure (AUC of 2F-ara-A). Limited clinical data are available in patients with impairment of renal function (creatinine clearance below 70 mL/min). Therefore, if renal impairment is clinically suspected, or in patients over the age of 70 years, creatinine clearance should be measured. If creatinine clearance is between 30 and 70 mL/min, the dose should be reduced by up to 50% and close hematological monitoring should be used to assess toxicity. FLUDARABINE PHOSPHATE INJECTION, USP treatment is contraindicated, if creatinine clearance is < 30 mL/min. (See DOSAGE AND ADMINISTRATION). Sexual Function/Reproduction Preclinical toxicology studies in mice, rats and dogs have demonstrated dose-related adverse effects on the male reproductive system. Observations consisted of a decrease in mean testicular weights in dogs and degeneration and necrosis of spermatogenic epithelium of the testes in mice, rats and dogs. The possible adverse effects on fertility in males and females in humans have not been adequately evaluated. Therefore, it is recommended that men and women of child-bearing potential take contraceptive measures during FLUDARABINE PHOSPHATE INJECTION, USP therapy, and for at least 6 months after the cessation of FLUDARABINE PHOSPHATE INJECTION, USP therapy. Skin The worsening or flare-up of pre-existing skin cancer lesions, as well as new onset of skin cancer, has been reported to occur in patients during or after intravenous (i.v.) fludarabine phosphate therapy. Special Populations
Pregnant Women:
FLUDARABINE PHOSPHATE INJECTION, USP should not be used during pregnancy unless clearly necessary (e.g., life-threatening situation, no alternative safer treatment available without compromising the therapeutic benefit, treatment cannot be avoided). It has the potential to cause fetal harm. Prescribers may only consider it to be used if the potential benefits justify the potential risks to the fetus. Women of childbearing potential must be apprised of the potential hazard to the fetus. Women should avoid becoming pregnant while on FLUDARABINE PHOSPHATE INJECTION, USP therapy. Women of childbearing potential or fertile males must take effective contraceptive measures during and at least for 6 months after cessation of therapy. Nursing Women: Breast-feeding should not be initiated during FLUDARABINE PHOSPHATE INJECTION, USP treatment. Nursing women should discontinue breastfeeding. It is not known whether this drug is excreted in human milk. There is evidence from preclinical data that after intravenous administration to rats that fludarabine phosphate and/or metabolites transfer from maternal blood to milk. Pediatrics: The safety and effectiveness of fludarabine phosphate in children have not been established. Geriatrics (> 75 years of age): Since there are limited data for the use of fludarabine phosphate in elderly persons (> 75 years), caution should be exercised with the administration of FLUDARABINE PHOSPHATE INJECTION, USP in these patients. The total body clearance of the principal plasma metabolite 2F-ara-A shows a correlation with creatinine clearance, indicating the importance of the renal excretion pathway for the elimination of the compound. Patients with reduced kidney function demonstrated an increased total body exposure (AUC of 2F-ara-A). Limited clinical data are available in patients with impairment of renal function (creatinine clearance below 70 mL/min). Since renal impairment is frequently present in patients over the age of 70 years, creatinine clearance should be measured. If creatinine clearance is between 30 and 70 mL/min, the dose should be reduced by up to 50%, and close hematologic monitoring should be used to assess toxicity. FLUDARABINE PHOSPHATE INJECTION, USP treatment is contraindicated if creatinine clearance is < 30 mL/min. (See DOSAGE AND ADMINISTRATION). Monitoring and Laboratory Tests During treatment, the patient's hematologic (particularly neutrophils and platelets) and serum chemistry profiles should be monitored regularly. Effects on Ability to Drive or Operate Machines FLUDARABINE PHOSPHATE INJECTION, USP may reduce the ability to drive or use machines, since fatigue, weakness, visual disturbances, confusion, agitation and seizures have been observed. |
||||||||||
|
Adverse Reactions |
6 ADVERSE REACTIONS Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. Very common adverse reactions include myelosuppression (neutropenia, thrombocytopenia and anemia), fever and chills, fatigue, weakness, infection, pneumonia, cough, nausea, vomiting and diarrhea. Other commonly reported events include malaise, mucositis, and anorexia. Serious opportunistic infections have occurred in CLL patients treated with fludarabine phosphate. The most frequently reported adverse reactions and those reactions which are more clearly related to the drug are arranged below according to body system. 6.1 Hematopoietic Systems Hematologic events (neutropenia, thrombocytopenia, and/or anemia) were reported in the majority of CLL patients treated with fludarabine phosphate. During fludarabine phosphate treatment of 133 patients with CLL, the absolute neutrophil count decreased to less than 500/mm3 in 59% of patients, hemoglobin decreased from pretreatment values by at least 2 grams percent in 60%, and platelet count decreased from pretreatment values by at least 50% in 55%. Myelosuppression may be severe, cumulative, and may affect multiple cell lines. Bone marrow fibrosis occurred in one CLL patient treated with fludarabine phosphate. Several instances of trilineage bone marrow hypoplasia or aplasia resulting in pancytopenia, sometimes resulting in death, have been reported in post-marketing surveillance. The duration of clinically significant cytopenia in the reported cases has ranged from approximately 2 months to approximately 1 year. These episodes have occurred both in previously treated or untreated patients. Life-threatening and sometimes fatal autoimmune phenomena such as hemolytic anemias, autoimmune thrombocytopenia/thrombocytopenic purpura (ITP), Evans syndrome, and acquired hemophilia have been reported to occur in patients receiving fludarabine phosphate [see Warnings and Precautions (5.3)]. The majority of patients rechallenged with fludarabine phosphate developed a recurrence in the hemolytic process. In post-marketing experience, cases of myelodysplastic syndrome and acute myeloid leukemia, mainly associated with prior, concomitant or subsequent treatment with alkylating agents, topoisomerase inhibitors, or irradiation have been reported. 6.2 Infections Serious and sometimes fatal infections, including opportunistic infections and reactivations of latent viral infections such as VZV (herpes zoster), Epstein-Barr virus and JC virus (progressive multifocal leukoencephalopathy) have been reported in patients treated with fludarabine phosphate. Rare cases of Epstein-Barr (EBV) associated lymphoproliferative disorders have been reported in patients treated with fludarabine phosphate. In post-marketing experience, cases of progressive multifocal leukoencephalopathy have been reported. Most cases had a fatal outcome. Many of these cases were confounded by prior and/or concurrent chemotherapy. The time to onset ranged from a few weeks to approximately one year after initiating treatment. Of the 133 adult CLL patients in the two trials, there were 29 fatalities during study, approximately 50% of which were due to infection. 6.3 Metabolic Tumor lysis syndrome has been reported in CLL patients treated with fludarabine phosphate. This complication may include hyperuricemia, hyperphosphatemia, hypocalcemia, metabolic acidosis, hyperkalemia, hematuria, urate crystalluria, and renal failure. The onset of this syndrome may be heralded by flank pain and hematuria. 6.4 Nervous System Objective weakness, agitation, confusion, seizures, visual disturbances, optic neuritis, optic neuropathy, blindness and coma have occurred in CLL patients treated with fludarabine phosphate at the recommended dose. Peripheral neuropathy has been observed in patients treated with fludarabine phosphate and one case of wrist-drop was reported. There have been additional reports of cerebral hemorrhage though the frequency is not known [see Warnings and Precautions (5)]. 6.5 Pulmonary System Pneumonia, a frequent manifestation of infection in CLL patients, occurred in 16%, and 22% of those treated with fludarabine phosphate in the MDAH and SWOG studies, respectively. Pulmonary hypersensitivity reactions to fludarabine phosphate characterized by dyspnea, cough and interstitial pulmonary infiltrate have been observed. In post-marketing experience, cases of severe pulmonary toxicity have been observed with fludarabine phosphate use which resulted in ARDS, respiratory distress, pulmonary hemorrhage, pulmonary fibrosis, pneumonitis and respiratory failure. After an infectious origin has been excluded, some patients experienced symptom improvement with corticosteroids. 6.6 Gastrointestinal System Gastrointestinal disturbances such as nausea, vomiting, anorexia, diarrhea, stomatitis, and hemorrhage have been reported in patients treated with fludarabine phosphate. Elevations of pancreatic enzyme levels have also been reported. 6.7 Cardiovascular Edema has been frequently reported. One patient developed a pericardial effusion possibly related to treatment with fludarabine phosphate. There have been reports of heart failure and arrhythmia. No other severe cardiovascular events were considered to be drug related. 6.8 Genitourinary System Hemorrhagic cystitis has been reported in patients treated with fludarabine phosphate. 6.9 Skin Skin toxicity, consisting primarily of skin rashes, has been reported in patients treated with fludarabine phosphate. Erythema multiforme, Steven-Johnson syndrome, toxic epidermal necrolysis and pemphigus have been reported, with fatal outcomes in some cases. 6.10 Neoplasms Worsening or flare-up of preexisting skin cancer lesions, as well as new onset of skin cancer, has been reported in patients during or after treatment with fludarabine phosphate. 6.11 Hepatobiliary Disorders Elevations of hepatic enzyme levels have been reported. 6.12 Adverse Reactions from Clinical Trials Data in Table 1 are derived from the 133 patients with CLL who received fludarabine phosphate in the MDAH and SWOG studies. |
Adverse Drug Reaction Overview The most common adverse events occurring with fludarabine phosphate use include myelosuppression (anemia, leukopenia, neutropenia and thrombocytopenia), leading to decreased resistance to infection, including pneumonia, cough, fever, fatigue, weakness, nausea, vomiting and diarrhea. Other commonly reported events include chills, edema, malaise, peripheral neuropathy, visual disturbance, anorexia, mucositis, stomatitis and skin rash. Serious opportunistic infections have occurred in patients treated with fludarabine phosphate. Fatalities as a consequence of serious adverse events have been reported. The table below reports adverse events by MedDRA system organ classes (MedDRA SOCs). The frequencies are based on clinical trial data regardless of the causal relationship with fludarabine phosphate. |
||||||||||
|
|
Table 2 Fludarabine phosphate Clinical Trial Adverse Events (by MedDRA SOC) |
|||||||||||
| Adverse Reactions | MDAH (N=101) | SWOG (N=32) | System Organ Class MedDRA | Very Common 1/10 | Common 1/100 to <1/10 | Uncommon 1/1000 to < 1/100 | Rare 1/10,000 to < 1/1000 | |||||
| ANY ADVERSE REACTION | 88% | 91% | Infections and infestations | Infections / opportunistic infections (like latent viral reactivation, e.g., Herpes zoster virus, Epstein-Barr virus, Progressive multifocal leucoencephalopathy), pneumonia | Lymphoproliferative disorder (EBV-associated) | |||||||
| BODY AS A WHOLE | 72 | 84 | Neoplasms benign, malignant and unspecified (including cysts and polyps) | Myelodysplastic syndrome and acute myeloid leukaemia (mainly associated with prior, concomitant, or subsequent treatment with alkylating agents, topoisomerase inhibitors or irradiation) | ||||||||
| FEVER | 60 | 69 | Blood and lymphatic system disorders | Neutropenia, anemia, thrombocytopenia | Myelosuppression | |||||||
| CHILLS | 11 | 19 | Immune system disorders | Autoimmune disorder (including autoimmune hemolytic anemia, thrombocytopenic purpura, pemphigus, Evans syndrome, acquired hemophilia) | ||||||||
| FATIGUE | 10 | 38 | Metabolism and nutrition disorders | Anorexia | Tumor lysis syndrome (including renal failure, hyperkalemia, metabolic acidosis, hematuria, urate crystalluria, hyperuricemia, hyperphosphatemia, hypocalcemia) | |||||||
| INFECTION | 33 | 44 | Nervous system disorders | Neuropathy peripheral | Confusion | Agitation, seizures, coma | ||||||
| PAIN | 20 | 22 | Eye disorders | Visual disturbance | Optic neuritis, optic neuropathy, blindness | |||||||
| PAIN | 20 | 22 | Cardiac disorders | Heart failure, arrhythmia | ||||||||
| MALAISE | 8 | 6 | Respiratory, thoracic and mediastinal disorders | Cough | Pulmonary toxicity (including dyspnea, pulmonary fibrosis, pneumonitis) | |||||||
| DIAPHORESIS | 1 | 13 | Gastrointestinal disorders | Nausea, vomiting, diarrhea | Stomatitis | Gastrointestinal hemorrhage, pancreatic enzymes abnormal | ||||||
| ALOPECIA | 0 | 3 | Hepatobiliary disorders | Hepatic enzyme abnormal | ||||||||
| ANAPHYLAXIS | 1 | 0 | Skin and subcutaneous tissue disorders | Rash | Skin cancer, Stevens-Johnson syndrome, necrolysis epidermal toxic (Lyell type) | |||||||
| HEMORRHAGE | 1 | 0 | Renal and urinary disorder | Urinary tract hemorrhage (including hemorrhagic cystitis) | ||||||||
| HYPERGLYCEMIA | 1 | 6 | General disorders and administration site conditions | Fever, fatigue, weakness | Chills, malaise, edema, mucositis | |||||||
| DEHYDRATION | 1 | 0 | ||||||||||
| NEUROLOGICAL | 21 | 69 | ||||||||||
| WEAKNESS | 9 | 65 | ||||||||||
| PARESTHESIA | 4 | 12 | ||||||||||
| HEADACHE | 3 | 0 | ||||||||||
| VISUAL DISTURBANCE | 3 | 15 | ||||||||||
| HEARING LOSS | 2 | 6 | ||||||||||
| SLEEP DISORDER | 1 | 3 | ||||||||||
| DEPRESSION | 1 | 0 | ||||||||||
| CEREBELLAR SYNDROME | 1 | 0 | ||||||||||
| IMPAIRED MENTATION | 1 | 0 | ||||||||||
| PULMONARY | 35 | 69 | ||||||||||
| COUGH | 10 | 44 | ||||||||||
| PNEUMONIA | 16 | 22 | ||||||||||
| DYSPNEA | 9 | 22 | ||||||||||
| SINUSITIS | 5 | 0 | ||||||||||
| PHARYNGITIS | 0 | 9 | ||||||||||
| UPPER RESPIRATORY INFECTION | 2 | 16 | ||||||||||
| ALLERGIC PNEUMONITIS | 0 | 6 | ||||||||||
| EPISTAXIS | 1 | 0 | ||||||||||
| HEMOPTYSIS | 1 | 6 | ||||||||||
| BRONCHITIS | 1 | 0 | ||||||||||
| HYPOXIA | 1 | 0 | ||||||||||
| GASTROINTESTINAL | 46 | 63 | ||||||||||
| NAUSEA/VOMITING | 36 | 31 | ||||||||||
| DIARRHEA | 15 | 13 | ||||||||||
| ANOREXIA | 7 | 34 | ||||||||||
| STOMATITIS | 9 | 0 | ||||||||||
| GI BLEEDING | 3 | 13 | ||||||||||
| ESOPHAGITIS | 3 | 0 | ||||||||||
| MUCOSITIS | 2 | 0 | ||||||||||
| LIVER FAILURE | 1 | 0 | ||||||||||
| ABNORMAL LIVER FUNCTION TEST | 1 | 3 | ||||||||||
| CONSTIPATION | 1 | 3 | ||||||||||
| DYSPHAGIA | 1 | 0 | ||||||||||
| CUTANEOUS | 17 | 18 | ||||||||||
| RASH | 15 | 15 | ||||||||||
| PRURITUS | 1 | 3 | ||||||||||
| SEBORRHEA | 1 | 0 | ||||||||||
| GENITOURINARY | 12 | 22 | ||||||||||
| DYSURIA | 4 | 3 | ||||||||||
| URINARY INFECTION | 2 | 15 | ||||||||||
| HEMATURIA | 2 | 3 | ||||||||||
| RENAL FAILURE | 1 | 0 | ||||||||||
| ABNORMAL RENAL FUNCTION TEST | 1 | 0 | ||||||||||
| PROTEINURIA | 1 | 0 | ||||||||||
| HESITANCY | 0 | 3 | ||||||||||
| CARDIOVASCULAR | 12 | 38 | ||||||||||
| EDEMA | 8 | 3 | ||||||||||
| ANGINA | 0 | 6 | ||||||||||
| CONGESTIVE HEART FAILURE | 0 | 3 | ||||||||||
| ARRHYTHMIA | 0 | 3 | ||||||||||
| SUPRAVENTRICULAR TACHYCARDIA | 0 | 3 | ||||||||||
| MYOCARDIAL INFARCTION | 0 | 3 | ||||||||||
| DEEP VENOUS THROMBOSIS | 1 | 3 | ||||||||||
| PHLEBITIS | 1 | 3 | ||||||||||
| TRANSIENT ISCHEMIC ATTACK | 1 | 0 | ||||||||||
| ANEURYSM | 1 | 0 | ||||||||||
| CEREBROVASCULAR ACCIDENT | 0 | 3 | ||||||||||
| MUSCULOSKELETAL | 7 | 16 | ||||||||||
| MYALGIA | 4 | 16 | ||||||||||
| OSTEOPOROSIS | 2 | 0 | ||||||||||
| ARTHRALGIA | 1 | 0 | ||||||||||
| TUMOR LYSIS SYNDROME | 1 | 0 | ||||||||||
|
|
Post-Market Adverse Reaction The following adverse reactions are based on post-marketing data regardless of the causal relationship with fludarabine phosphate. Blood and lymphatic disorders: pancytopenia, myelosuppression, neutropenia, thrombocytopenia, anemia, cytopenia, tri-lineage bone marrow aplasia Cardiac disorders: edema, heart failure, arrhythmia Eye disorders: blindness, optic neuritis, optic neuropathy, eye hemorrhage including retinalGastrointestinal disorders: anorexia General disorders and administrative conditions: chills Genitourinary disorders (initial PI)/Metabolism and nutritional disorders: hematuria (context of TLS), hypocalcemia (context of TLS), hyperphosphatemia (context of TLS), hyperuricemia, renal failure (context of TLS), urate crystalluria (context of TLS), metabolic acidosis (context of TLS), hyperkalemia (context of TLS) Hepatobiliary disorders: hepatic enzymes abnormal, pancreatic enzymes abnormal Immune system disorders: transfusion-related GVHD, thrombocytopenic purpura, Evans syndrome, pemphigus, autoimmune hemolytic anemia, acquired hemophilia Infections and infestations: opportunistic infections, herpes zoster virus, Epstein-Barr virus, latent viral reactivation, progressive multifocal leucoencephalopathy, human polyomavirus JC virus (context of PML), disease transformation CLL Neoplasms, benign, malignant and unspecified: acute myeloid leukemia, Richters syndrome, myelodysplastic syndrome, disease progressive CLL, lympho-proliferative disorder (EBV-associated) Nervous system disorders: seizures, agitation, confusion, coma; leukoencephalopathy, acute toxic leukoencephalopathy, posterior reversible encephalopathy syndrome/ reversible posterior leukoencephalopathy syndrome (see WARNINGS AND PRECAUTIONS, Neurologic). Respiratory, thoracic and mediastinal disorders: pulmonary toxicity, pneumonitis, pulmonary fibrosis, dyspnea Skin and subcutaneous tissue disorders: toxic epidermal necrolysis, rash, worsening of pre-existing skin cancer lesions, skin cancer, Stevens-Johnson syndrome Vascular disorders: hemorrhage, pulmonary hemorrhage, gastrointestinal hemorrhage, urinary tract hemorrhage including hemorrhagic cystitis, cerebral hemorrhage |
|||||||||||
|
Use in Specific Populations |
8.1 Pregnancy [See Warnings and Precautions (5.6)]. Based on its mechanism of action, fludarabine phosphate can cause fetal harm when administered to a pregnant woman. There are no adequate and well-controlled studies of Fludarabine Phosphate Injection in pregnant women. In rats, repeated intravenous doses of fludarabine phosphate at 2.4 times and 7.2 times the recommended human IV dose (25 mg/m 2) administered during organogenesis caused an increase in resorptions, skeletal and visceral malformations (cleft palate, exencephaly, and fetal vertebrae deformities) and decreased fetal body weights. Maternal toxicity was not apparent at 2.4 times the human IV dose, and was limited to slight body weight decreases at 7.2 times the human IV dose. In rabbits, repeated intravenous doses of fludarabine phosphate at 3.8 times the human IV dose administered during organogenesis increased embryo and fetal lethality as indicated by increased resorptions and a decrease in live fetuses. A significant increase in malformations including cleft palate, hydrocephaly, adactyly, brachydactyly, fusions of the digits, diaphragmatic hernia, heart/great vessel defects, and vertebrae/rib anomalies were seen in all dose levels ( 0.5 times the human IV dose). If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to the fetus. Women of childbearing potential should be advised to avoid becoming pregnant. 8.3 Nursing Mothers It is not known whether fludarabine phosphate is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions including tumorigenicity in nursing infants, a decision should be made to discontinue nursing or discontinue the drug, taking into account the importance of the drug for the mother. 8.4 Pediatric Use Data submitted to the FDA was insufficient to establish efficacy in any childhood malignancy. Fludarabine phosphate was evaluated in 62 pediatric patients (median age 10, range 1 to 21) with refractory acute leukemia (45 patients) or solid tumors (17 patients). Limited pharmacokinetic data for fludarabine phosphate are available in children (ages 1 to 21 years). When fludarabine phosphate was administered as a loading dose over 10 minutes immediately followed by a 5-day continuous infusion, steady-state conditions were reached early. The fludarabine phosphate regimen tested for pediatric lymphocytic leukemia (ALL) patients was a loading bolus of 10.5 mg/m 2/day followed by a continuous infusion of 30.5 mg/m 2/day for 5 days. In 12 pediatric patients with solid tumors, dose-limiting myelosuppression was observed with a loading dose of 8 mg/m 2/day followed by a continuous infusion of 23.5 mg/m 2/day for 5 days. The maximum tolerated dose was a loading dose of 7 mg/m 2/day followed by a continuous infusion of 20 mg/m 2/day for 5 days. Treatment toxicity included bone marrow suppression. Platelet counts appeared to be more sensitive to the effects of fludarabine phosphate than hemoglobin and white blood cell counts. Other adverse events included fever, chills, asthenia, rash, nausea, vomiting, diarrhea, and infection. There were no reported occurrences of peripheral neuropathy or pulmonary hypersensitivity reaction. 8.6 Patients with Renal Impairment The total body clearance of the principal metabolite 2-fluoro-ara-A correlated with the creatinine clearance, indicating the importance of the renal excretion pathway for the elimination of the drug. Renal clearance represents approximately 40% of the total body clearance. Patients with creatinine clearance 30 to 79 mL/min should have their fludarabine phosphate dose reduced and be monitored closely for excessive toxicity. Due to insufficient data, fludarabine phosphate should not be administered to patients with creatinine clearance less than 30 mL/min [see Dosage and Administration (2.2), Warnings and Precautions (5.9)]. |
Pregnant Women: There are very limited data of fludarabine phosphate use in pregnant women in the first trimester: one newborn has been described with absent bilateral radii and normal thumbs, thrombocytopenia, fossa ovalis aneurysm and a small patent ductus arteriosus. Early pregnancy loss has been reported in fludarabine phosphate monotherapy as well as in combination therapy. Premature delivery has been reported. FLUDARABINE PHOSPHATE INJECTION, USP should not be used during pregnancy unless clearly necessary (e.g., life-threatening situation, no alternative safer treatment available without compromising the therapeutic benefit, treatment cannot be avoided). It has the potential to cause fetal harm. Prescribers may only consider it to be used if the potential benefits justify the potential risks to the fetus. Women of childbearing potential must be apprised of the potential hazard to the fetus. Women should avoid becoming pregnant while on FLUDARABINE PHOSPHATE INJECTION, USP therapy. Women of childbearing potential or fertile males must take effective contraceptive measures during and at least for 6 months after cessation of therapy. Nursing Women: Breast-feeding should not be initiated during FLUDARABINE PHOSPHATE INJECTION, USP treatment. Nursing women should discontinue breastfeeding. It is not known whether this drug is excreted in human milk. There is evidence from preclinical data that after intravenous administration to rats that fludarabine phosphate and/or metabolites transfer from maternal blood to milk. Pediatrics: The safety and effectiveness of fludarabine phosphate in children have not been established. Geriatrics (>75 years of age): Since there are limited data for the use of fludarabine phosphate in elderly persons (> 75 years), caution should be exercised with the administration of FLUDARABINE PHOSPHATE INJECTION, USP in these patients. The total body clearance of the principal plasma metabolite 2F-ara-A shows a correlation with creatinine clearance, indicating the importance of the renal excretion pathway for the elimination of the compound. Patients with reduced kidney function demonstrated an increased total body exposure (AUC of 2F-ara-A). Limited clinical data are available in patients with impairment of renal function (creatinine clearance below 70 mL/min). Since renal impairment is frequently present in patients over the age of 70 years, creatinine clearance should be measured. If creatinine clearance is between 30 and 70 mL/min, the dose should be reduced by up to 50%, and close hematologic monitoring should be used to assess toxicity. FLUDARABINE PHOSPHATE INJECTION, USP treatment is contraindicated if creatinine clearance is <30 mL/min. (See DOSAGE AND ADMINISTRATION). |
||||||||||

HOW SUPPLIED
|
Product Name & Description |
Strength/ Presentation |
Dosage Form |
Package size |
NDC |
|
Fludarabine Phosphate Injection, USP |
50 mg/2 mL (25 mg/mL) |
Injectable |
2 mL, Single Dose, Clear Glass Vial with Orange Flip-Off Seal |
16729-131-30 |