INFED- iron dextran injection, solution
General Injectables & Vaccines, Inc
----------
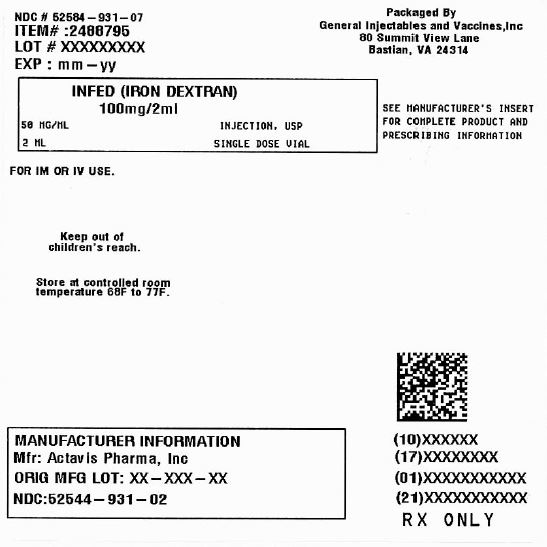
Infed (Iron Dextran) 20 mg/mL Injection, USP 2 mL Single Dose Vial
Boxed Warning
WARNING: RISK FOR ANAPHYLACTIC-TYPE REACTIONS
Anaphylactic-type reactions, including fatalities, have followed the parenteral administration of iron dextran injection.
- Have resuscitation equipment and personnel trained in the detection and treatment of anaphylactic-type reactions readily available during INFeD administration.
- Administer a test INFeD dose prior to the first therapeutic dose. If no signs or symptoms of anaphylactic-type reactions follow the test dose, administer the full therapeutic INFeD dose.
- During all INFeD administrations, observe for signs or symptoms of anaphylactic-type reactions. Fatal reactions have followed the test dose of iron dextran injection. Fatal reactions have also occurred in situations where the test dose was tolerated.
- Use INFeD only in patients in whom clinical and laboratory investigations have established an iron deficient state not amenable to oral iron therapy.
- Patients with a history of drug allergy or multiple drug allergies may be at increased risk of anaphylactic-type reactions to INFeD.
Description
INFeD (Iron Dextran Injection USP) is a dark brown, slightly viscous sterile liquid complex of ferric hydroxide and dextran for intravenous or intramuscular use.
Each mL contains the equivalent of 50 mg of elemental iron (as an iron dextran complex), approximately 0.9% sodium chloride, in water for injection. Sodium hydroxide and/or hydrochloric acid may have been used to adjust pH. The pH of the solution is between 5.2 and 6.5.
Therapeutic Class: Hematinic
Clinical Pharmacology
General: After intramuscular injection, iron dextran is absorbed from the injection site into the capillaries and the lymphatic system. Circulating iron dextran is removed from the plasma by cells of the reticuloendothelial system, which split the complex into its components of iron and dextran. The iron is immediately bound to the available protein moieties to form hemosiderin or ferritin, the physiological forms of iron, or to a lesser extent to transferrin. This iron which is subject to physiological control replenishes hemoglobin and depleted iron stores.
Dextran, a polyglucose, is either metabolized or excreted. Negligible amounts of iron are lost via the urinary or alimentary pathways after administration of iron dextran.
The major portion of intramuscular injections of iron dextran is absorbed within 72 hours; most of the remaining iron is absorbed over the ensuing 3 to 4 weeks.
Various studies involving intravenously administered 59Fe iron dextran to iron deficient subjects, some of whom had coexisting diseases, have yielded half-life values ranging from 5 hours to more than 20 hours. The 5-hour value was determined for 59Fe iron dextran from a study that used laboratory methods to separate the circulating 59Fe iron dextran from the transferrin-bound 59Fe. The 20-hour value reflects a half-life determined by measuring total 59Fe, both circulating and bound. It should be understood that these half-life values do not represent clearance of iron from the body. Iron is not easily eliminated from the body and accumulation of iron can be toxic.
In vitro studies have shown that removal of iron dextran by dialysis is negligible.1,2 Six different dialyzer membranes were investigated (polysulfone, cuprophane, cellulose acetate, cellulose triacetate, polymethylmethacrylate and polyacrylonitrile), including those considered high efficiency and high flux.
Indications and Usage
Intravenous or intramuscular injections of INFeD are indicated for treatment of patients with documented iron deficiency in whom oral administration is unsatisfactory or impossible.
Warnings
Risk for Anaphylactic-type Reactions: Anaphylactic-type reactions, including fatalities have followed the parenteral administration of iron dextran. Always have resuscitation equipment and personnel trained in the detection and treatment of anaphylactic-type reactions readily available during INFeD administration. Prior to the first therapeutic dose, administer a test INFeD dose of 0.5 mL. (See DOSAGE AND ADMINISTRATION.) Although reactions are usually evident within a few minutes, observe patients for at least one hour before administering the therapeutic dose. During all INFeD administrations, observe patients for signs or symptoms of anaphylactic-type reactions. Fatal reactions have followed the test dose of iron dextran and have also occurred in situations where the test dose was tolerated. Use INFeD only in patients in whom clinical and laboratory investigations have established an iron deficient state not amenable to oral iron therapy.
The factors that affect the risk for anaphylactic-type reactions to iron dextran products are not fully known but limited clinical data suggest the risk may be increased among patients with a history of drug allergy or multiple drug allergies. Additionally, concomitant use of angiotensin-converting enzyme inhibitor drugs may increase the risk for reactions to an iron dextran product. The extent of risk for anaphylactic-type reactions following exposure to any specific iron dextran product is unknown and may vary among the products.
Iron dextran products differ in chemical characteristics and may differ in clinical effects. Iron dextran products are not clinically interchangeable.
Delayed Reactions: Large intravenous doses, such as used with total dose infusions (TDI), have been associated with an increased incidence of adverse effects. The adverse effects frequently are delayed (1-2 days) reactions typified by one or more of the following symptoms: arthralgia, backache, chills, dizziness, moderate to high fever, headache, malaise, myalgia, nausea, and vomiting. The onset is usually 24-48 hours after administration and symptoms generally subside within 3-4 days. The etiology of these reactions is not known. The potential for a delayed reaction must be considered when estimating the risk/benefit of treatment.
The maximum daily dose should not exceed 2 mL undiluted iron dextran.
Risk in Patients with Underlying Conditions: INFeD should be used with extreme care in patients with serious impairment of liver function. It should not be used during the acute phase of infectious kidney disease.
Adverse reactions experienced following administration of INFeD may exacerbate cardiovascular complications in patients with pre-existing cardiovascular disease.
Carcinogenesis: A risk of carcinogenesis may attend the intramuscular injection of iron-carbohydrate complexes. Such complexes have been found under experimental conditions to produce sarcoma when large doses or small doses injected repeatedly at the same site were given to rats, mice, and rabbits, and possibly in hamsters.
The long latent period between the injection of a potential carcinogen and the appearance of a tumor makes it impossible to measure accurately the risk in man. There have, however, been several reports in the literature describing tumors at the injection site in humans who had previously received intramuscular injections of iron-carbohydrate complexes.
Precautions
General: Unwarranted therapy with parenteral iron will cause excess storage of iron with the consequent possibility of exogenous hemosiderosis. Such iron overload is particularly apt to occur in patients with hemoglobinopathies and other refractory anemias that might be erroneously diagnosed as iron deficiency anemias.
INFeD should be used with caution in individuals with histories of significant allergies and/or asthma.
Anaphylaxis and other hypersensitivity reactions have been reported after uneventful test doses as well as therapeutic doses of iron dextran injection. Therefore, administer a test dose prior to the first therapeutic dose of INFeD. (See BOXED WARNING and DOSAGE AND ADMINISTRATION: ADMINISTRATION.)
Epinephrine should be immediately available in the event of acute hypersensitivity reactions. (Usual adult dose: 0.5 mL of a 1:1000 solution, by subcutaneous or intramuscular injection.) Note: Patients using beta-blocking agents may not respond adequately to epinephrine. Isoproterenol or similar beta-agonist agents may be required in these patients.
Patients with rheumatoid arthritis may have an acute exacerbation of joint pain and swelling following the administration of INFeD.
Reports in the literature from countries outside the United States (in particular, New Zealand) have suggested that the use of intramuscular iron dextran in neonates has been associated with an increased incidence of gram-negative sepsis, primarily due to E. Coli.
Information For Patients: Patients should be advised of the potential adverse reactions associated with the use of INFeD.
Drug/Laboratory Test Interactions: Large doses of iron dextran (5 mL or more) have been reported to give a brown color to serum from a blood sample drawn 4 hours after administration.
The drug may cause falsely elevated values of serum bilirubin and falsely decreased values of serum calcium.
Serum iron determinations (especially by colorimetric assays) may not be meaningful for 3 weeks following the administration of iron dextran.
Serum ferritin peaks approximately 7 to 9 days after an intravenous dose of INFeD and slowly returns to baseline after about 3 weeks.
Examination of the bone marrow for iron stores may not be meaningful for prolonged periods following iron dextran therapy because residual iron dextran may remain in the reticuloendothelial cells.
Bone scans involving 99m Tc-diphosphonate have been reported to show a dense, crescentic area of activity in the buttocks, following the contour of the iliac crest, 1 to 6 days after intramuscular injections of iron dextran.
Bone scans with 99m Tc-labeled bone seeking agents, in the presence of high serum ferritin levels or following iron dextran infusions, have been reported to show reduction of bony uptake, marked renal activity, and excessive blood pool and soft tissue accumulation.
Carcinogenesis, Mutagenesis, Impairment Of Fertility: See WARNINGS.
Pregnancy: Pregnancy Category C: Iron dextran has been shown to be teratogenic and embryocidal in mice, rats, rabbits, dogs, and monkeys when given in doses of about 3 times the maximum human dose.
No consistent adverse fetal effects were observed in mice, rats, rabbits, dogs and monkeys at doses of 50 mg iron/kg or less. Fetal and maternal toxicity has been reported in monkeys at a total intravenous dose of 90 mg iron/kg over a 14 day period. Similar effects were observed in mice and rats on administration of a single dose of 125 mg iron/kg. Fetal abnormalities in rats and dogs were observed at doses of 250 mg iron/kg and higher. The animals used in these tests were not iron deficient. There are no adequate and well-controlled studies in pregnant women. INFeD should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Placental Transfer: Various animal studies and studies in pregnant humans have demonstrated inconclusive results with respect to the placental transfer of iron dextran as iron dextran. It appears that some iron does reach the fetus, but the form in which it crosses the placenta is not clear.
Nursing Mothers: Caution should be exercised when INFeD is administered to a nursing woman. Traces of unmetabolized iron dextran are excreted in human milk.
Pediatric Use: Not recommended for use in infants under 4 months of age. (See DOSAGE AND ADMINISTRATION.)
Adverse Reactions
Severe/Fatal: Anaphylactic reactions have been reported with the use of iron dextran injection; on occasions these reactions have been fatal. Such reactions, which occur most often within the first several minutes of administration, have been generally characterized by sudden onset of respiratory difficulty and/or cardiovascular collapse. Because fatal anaphylactic reactions have been reported after administration of iron dextran injection, the drug should be given only when resuscitation techniques and treatment of anaphylactic and anaphylactoid shock are readily available. (See BOXED WARNING and PRECAUTIONS: GENERAL, pertaining to immediate availability of epinephrine.)
Cardiovascular: Chest pain, chest tightness, shock, cardiac arrest, hypotension, hypertension, tachycardia, bradycardia, flushing, arrhythmias. (Flushing and hypotension may occur from too rapid injections by the intravenous route.)
Dermatologic: Urticaria, pruritus, purpura, rash, cyanosis.
Gastrointestinal: Abdominal pain, nausea, vomiting, diarrhea.
Hematologic/lymphatic: Leucocytosis, lymphadenopathy.
Musculoskeletal/soft tissue: Arthralgia, arthritis (may represent reactivation in patients with quiescent rheumatoid arthritis - See PRECAUTIONS: GENERAL), myalgia; backache; sterile abscess, atrophy/fibrosis (intramuscular injection site); brown skin and/or underlying tissue discoloration (staining), soreness or pain at or near intramuscular injection sites; cellulitis; swelling; inflammation; local phlebitis at or near intravenous injection site.
Neurologic: Convulsions, seizures, syncope, headache, weakness, unresponsiveness, paresthesia, febrile episodes, chills, dizziness, disorientation, numbness, unconsciousness.
Respiratory: Respiratory arrest, dyspnea, bronchospasm, wheezing.
Urologic: Hematuria.
Delayed reactions: Arthralgia, backache, chills, dizziness, fever, headache, malaise, myalgia, nausea, vomiting. (See WARNINGS)
Miscellaneous: Febrile episodes, sweating, shivering, chills, malaise, altered taste.
Overdosage
Overdosage with iron dextran is unlikely to be associated with any acute manifestations. Dosages of iron dextran in excess of the requirements for restoration of hemoglobin and replenishment of iron stores may lead to hemosiderosis. Periodic monitoring of serum ferritin levels may be helpful in recognizing a deleterious progressive accumulation of iron resulting from impaired uptake of iron from the reticuloendothelial system in concurrent medical conditions such as chronic renal failure, Hodgkins disease, and rheumatoid arthritis. The LD50 of iron dextran is not less than 500 mg/kg in the mouse.
Dosage and Administration
Oral iron should be discontinued prior to administration of INFeD.
Dosage:
I. Iron Deficiency Anemia: Periodic hematologic determination (hemoglobin and hematocrit) is a simple and accurate technique for monitoring hematological response, and should be used as a guide in therapy. It should be recognized that iron storage may lag behind the appearance of normal blood morphology. Serum iron, total iron binding capacity (TIBC) and percent saturation of transferrin are other important tests for detecting and monitoring the iron deficient state.
After administration of iron dextran complex, evidence of a therapeutic response can be seen in a few days as an increase in the reticulocyte count.
Although serum ferritin is usually a good guide to body iron stores, the correlation of body iron stores and serum ferritin may not be valid in patients on chronic renal dialysis who are also receiving iron dextran complex.
Although there are significant variations in body build and weight distribution among males and females, the accompanying table and formula represent a convenient means for estimating the total iron required. This total iron requirement reflects the amount of iron needed to restore hemoglobin concentration to normal or near normal levels plus an additional allowance to provide adequate replenishment of iron stores in most individuals with moderately or severely reduced levels of hemoglobin. It should be remembered that iron deficiency anemia will not appear until essentially all iron stores have been depleted. Therapy, thus, should aim at not only replenishment of hemoglobin iron but iron stores as well.
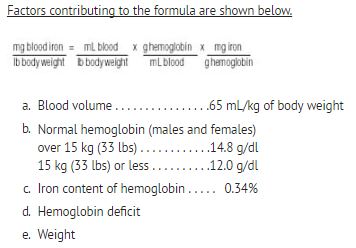
Based on the above factors, individuals with normal hemoglobin levels will have approximately 33 mg of blood iron per kilogram of body weight (15 mg/lb).
Note: The table and accompanying formula are applicable for dosage determinations only in patients with iron deficiency anemia; they are not to be used for dosage determinations in patients requiring iron replacement for blood loss.
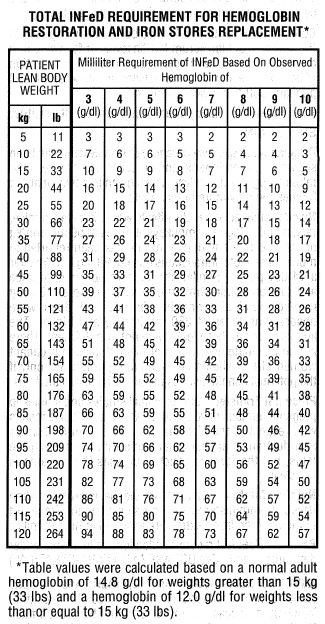
The total amount of INFeD in mL required to treat the anemia and replenish iron stores may be approximated as follows:
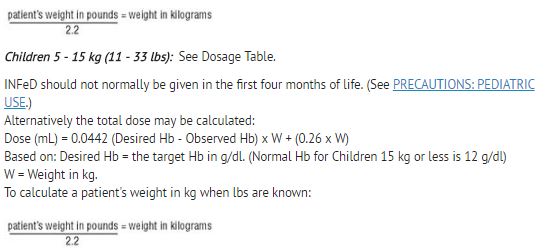
Adults and Children over 15 kg (33 lbs): See Dosage Table. Alternatively the total dose may be calculated:
Dose (mL) = 0.0442 (Desired Hb - Observed Hb) x LBW + (0.26 x LBW)
Based on: Desired Hb = the target Hb in g/dl.
Observed Hb = the patient’s current hemoglobin in g/dl.
LBW = Lean body weight in kg. A patient’s lean body weight (or actual body weight if less than lean body weight) should be utilized when determining dosage.
For males: LBW = 50 kg + 2.3 kg for each inch of patient’s height over 5 feet
For females: LBW = 45.5 kg + 2.3 kg for each inch of patient’s height over 5 feet
To calculate a patient's weight in kg when lbs are known:
II. Iron Replacement for Blood Loss: Some individuals sustain blood losses on an intermittent or repetitive basis. Such blood losses may occur periodically in patients with hemorrhagic diatheses (familial telangiectasia; hemophilia; gastrointestinal bleeding) and on a repetitive basis from procedures such as renal hemodialysis.
Iron therapy in these patients should be directed toward replacement of the equivalent amount of iron represented in the blood loss. The table and formula described under I. Iron Deficiency Anemia are not applicable for simple iron replacement values.
Quantitative estimates of the individual’s periodic blood loss and hematocrit during the bleeding episode provide a convenient method for the calculation of the required iron dose.
The formula shown below is based on the approximation that 1 mL of normocytic, normochromic red cells contains 1 mg of elemental iron:
Replacement iron (in mg) = Blood loss (in mL) x hematocrit
Example: Blood loss of 500 mL with 20% hematocrit
Replacement Iron = 500 x 0.20 = 100 mg
INFeD dose = 100 mg = 2 mL
50
Administration:
The total amount of INFeD required for the treatment of iron deficiency anemia or iron replacement for blood loss is determined from the table or appropriate formula. (See DOSAGE).
I. Intravenous Injection - PRIOR TO THE FIRST INTRAVENOUS INFeD THERAPEUTIC DOSE, ADMINISTER AN INTRAVENOUS TEST DOSE OF 0.5 ML. ADMINISTER THE TEST DOSE AT A GRADUAL RATE OVER AT LEAST 30 SECONDS. Although anaphylactic reactions known to occur following INFeD administration are usually evident within a few minutes, or sooner, it is recommended that a period of an hour or longer elapse before the remainder of the initial therapeutic dose is given.
Individual doses of 2 mL or less may be given on a daily basis until the calculated total amount required has been reached. INFeD is given undiluted at a slow gradual rate not to exceed 50 mg (1 mL) per minute.
2. Intramuscular Injection - PRIOR TO THE FIRST INTRAMUSCULAR INFeD THERAPEUTIC DOSE, ADMINISTER AN INTRAMUSCULAR TEST DOSE OF 0.5 ML. (See BOXED WARNING and PRECAUTIONS.) The test dose should be administered in the buttock using the same technique as described in the last paragraph of this section. Although anaphylactic reactions known to occur following INFeD administration are usually evident within a few minutes or sooner, it is recommended that at least an hour or longer elapse before the remainder of the initial therapeutic dose is given.
If no adverse reactions are observed, INFeD can be given according to the following schedule until the calculated total amount required has been reached. Each day’s dose should ordinarily not exceed 0.5 mL (25 mg of iron) for infants under 5 kg (11 lbs); 1.0 mL (50 mg of iron) for children under 10 kg (22 lbs); and 2.0 mL (100 mg of iron) for other patients.
INFeD should be injected only into the muscle mass of the upper outer quadrant of the buttock - never into the arm or other exposed areas - and should be injected deeply, with a 2-inch or 3-inch 19 or 20 gauge needle. If the patient is standing, he/she should be bearing his/her weight on the leg opposite the injection site, or if in bed, he/she should be in the lateral position with injection site uppermost. To avoid injection or leakage into the subcutaneous tissue, a Z-track technique (displacement of the skin laterally prior to injection) is recommended.
NOTE: Do not mix INFeD with other medications or add to parenteral nutrition solutions for intravenous infusion.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever the solution and container permit.
How Supplied
INFeD (Iron Dextran Injection USP) containing 50 mg of elemental iron per mL, is available in 2 mL single dose amber vials (for intramuscular or intravenous use) in cartons of 10 (NDC 52544-931-02).
Store at 20 -25°C (68 -77°F) [See USP Controlled Room Temperature].
Rx Only
References
-
Hatton RC, Portales IT, Finlay A, Ross EA. Removal of Iron Dextran by Hemodialysis: An In Vitro Study. Am J Kid Dis. 1995; 26(2):327-330.
-
Manuel MA, Stewart WK, St. Clair Neill GD, Hutchinson F. Loss of Iron-Dextran through Cuprophane Membrane of a Disposable Coil Dialyser. Nephron. 1972;9:94-98.
For all medical inquiries contact:
ACTAVIS
Medical Communications
Parsippany, NJ 07054
1-800-272-5525
Distributed By:
Actavis Pharma, Inc.
Parsippany, NJ 07054 USA
Manufactured By:
Patheon Italia S.p.A.
Ferentino, Italy 03013
Content Updated: January 2014
255769
| INFED
iron dextran injection, solution |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - General Injectables & Vaccines, Inc (108250663) |