Label: EPINEPHRINE injection







- NDC Code(s): 54288-119-10, 54288-119-25, 54288-120-01, 54288-152-01
- Packager: BPI Labs, LLC
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: New Drug Application
Drug Label Information
Updated March 21, 2024
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use EPINEPHRINE INJECTION USP safely and effectively. See full prescribing information for EPINEPHRINE INJECTION USP.
EPINEPHRINE INJECTION, USP for intravenous, intramuscular and subcutaneous use only
Initial U.S. Approval: 1939INDICATIONS AND USAGE
Epinephrine is a non-selective alpha and beta adrenergic agonist indicated: (1)
- To increase mean arterial blood pressure in adult patients with hypotension associated with septic shock (1.1)
- For emergency treatment of allergic reactions (Type 1), including anaphylaxis (1.2)
DOSAGE AND ADMINISTRATION
-
Hypotension associated with septic shock (2.2):
- Dilute epinephrine in dextrose solution prior to infusion.
- Infuse epinephrine into a large vein.
- Titrate 0.05 mcg/kg/min to 2 mcg/kg/min to achieve desired blood pressure.
- Wean gradually.
-
Anaphylaxis (2.3):
- Administer intramuscularly or subcutaneously into anterolateral thigh every 5-10 minutes as needed
- Adults and children over 30 kg (66 lb): 0.3-0.5 mg (0.3-0.5 mL)
- Children under 30 kg (66 lb): 0.01 mg/kg (0.01 mL/kg)
DOSAGE FORMS AND STRENGTHS
CONTRAINDICATIONS
None (4)
WARNINGS AND PRECAUTIONS
- Monitor patient for acute severe hypertension. (5.1)
- Avoid extravasation into tissues, which can cause local necrosis. (5.2)
- Do not inject into buttocks, digits, hands, or feet. (5.3)
- Potential for pulmonary edema, which may be fatal. (5.4)
- May constrict renal blood vessels and decrease urine formation. (5.5)
- May induce potentially serious cardiac arrhythmias or aggravate angina pectoris, particularly in patients with underlying heart disease. (5.6)
- Presence of sulfite in this product should not deter use. (5.9)
ADVERSE REACTIONS
Most common adverse reactions to systemically administered epinephrine are headache; anxiety; apprehensiveness; restlessness; tremor; weakness; dizziness; sweating; palpitations; pallor; peripheral coldness; nausea/vomiting; and/or respiratory difficulties. Arrhythmias, including fatal ventricular fibrillation, rapid rises in blood pressure producing cerebral hemorrhage, and angina have occurred. (6.1, 6.2) (6)
To report SUSPECTED ADVERSE REACTIONS, contact BPI Labs, LLC at (727) 471-0850 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch . (6)
DRUG INTERACTIONS
- Drugs that counter the pressor effects of epinephrine include alpha blockers, vasodilators such as nitrates, diuretics, antihypertensives, and ergot alkaloids. (7)
- Drugs that potentiate the effects of epinephrine include sympathomimetics, beta blockers, tricyclic antidepressants, MAO inhibitors, COMT inhibitors, clonidine, doxapram, oxytocin, levothyroxine sodium, and certain antihistamines. (7)
- Drugs that increase the arrhythmogenic potential of epinephrine include beta blockers, cyclopropane and halogenated hydrocarbon anesthetics, quinidine, antihistamines, exogenous thyroid hormones, diuretics, and cardiac glycosides. Observe for development of cardiac arrhythmias. (7)
- Potassium-depleting drugs, including corticosteroids, diuretics, and theophylline, potentiate the hypokalemic effects of epinephrine. (7)
USE IN SPECIFIC POPULATIONS
- Pregnancy: May cause fetal harm. (8.1)
- Elderly patients and pregnant women may be at greater risk of developing adverse reactions when epinephrine is administered parenterally. (8.1, 8.5)
Revised: 3/2024
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
1.1 Hypotension associated with Septic Shock
1.2 Anaphylaxis
2 DOSAGE AND ADMINISTRATION
2.1 General Considerations
2.2 Hypotension associated with Septic Shock
2.3 Anaphylaxis
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Hypertension
5.2 Extravasation and Tissue Necrosis with Intravenous Infusion
5.3 Incorrect Locations of Injection for Anaphylaxis
5.4 Pulmonary Edema
5.5 Renal Impairment
5.6 Cardiac Arrhythmias and Ischemia
5.7 Serious Infections at the Injection Site
5.8 Other Disease Interactions
5.9 Allergic Reactions Associated with Sulfite
6 ADVERSE REACTIONS
6.1 Adverse Reactions associated with Epinephrine Infusion (for Hypotension associated with Septic Shock)
6.2 Adverse Reactions associated with Intramuscular or Subcutaneous Use (for Anaphylaxis)
7 DRUG INTERACTIONS
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
14.1 Hypotension associated with Septic Shock
16 HOW SUPPLIED/STORAGE AND HANDLING
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
1.1 Hypotension associated with Septic Shock
Epinephrine Injection, USP 1 mg/mL is indicated to increase mean arterial blood pressure in adult patients with hypotension associated with septic shock.
1.2 Anaphylaxis
Emergency treatment of allergic reactions (Type I), including anaphylaxis, which may result from allergic reactions to insect stings, biting insects, foods, drugs, sera, diagnostic testing substances and other allergens, as well as idiopathic anaphylaxis or exercise-induced anaphylaxis. The signs and symptoms associated with anaphylaxis include flushing, apprehension, syncope, tachycardia, thready or unobtainable pulse associated with hypotension, convulsions, vomiting, diarrhea and abdominal cramps, involuntary voiding, airway swelling, laryngospasm, bronchospasm, pruritus, urticaria or angioedema, swelling of the eyelids, lips, and tongue.
-
2 DOSAGE AND ADMINISTRATION
2.1 General Considerations
Inspect visually for particulate matter and discoloration prior to administration, whenever solution and container permit. Do not use if the solution is colored or cloudy, or if it contains particulate matter. Discard any unused portion.
2.2 Hypotension associated with Septic Shock
Dilute epinephrine in 5 percent dextrose solution or 5 percent dextrose and sodium chloride solution. These dextrose containing fluids provide protection against significant loss of potency by oxidation. Administration in saline solution alone is not recommended. Whole blood or plasma, if indicated to increase blood volume, should be administered separately.
Add 1 mL (1 mg) of epinephrine from its vial to 1,000 mL of a 5 percent dextrose containing solution. Each mL of this dilution contains 1 mcg of epinephrine.
Correct blood volume depletion as fully as possible before any vasopressor is administered. When, as an emergency measure, intraaortic pressures must be maintained to prevent cerebral or coronary artery ischemia, epinephrine can be administered before and concurrently with blood volume replacement.
Whenever possible, give infusions of epinephrine into a large vein. Avoid using a catheter tie-in technique, because the obstruction to blood flow around the tubing may cause stasis and increased local concentration of the drug. Occlusive vascular diseases (for example, atherosclerosis, arteriosclerosis, diabetic endarteritis, Buerger’s disease) are more likely to occur in the lower than in the upper extremity; therefore, avoid the veins of the leg in elderly patients or in those suffering from such disorders. There is potential for gangrene in a lower extremity when infusions of catecholamine are given in an ankle vein.
To provide hemodynamic support in septic shock associated hypotension in adult patients, the suggested dosing infusion rate of intravenously administered epinephrine is 0.05 mcg/kg/min to 2 mcg/kg/min, and is titrated to achieve a desired mean arterial pressure (MAP). The dosage may be adjusted periodically, such as every 10 to 15 minutes, in increments of 0.05 mcg/kg/min to 0.2 mcg/kg/min, to achieve the desired blood pressure goal.
Continuous epinephrine infusion is generally required over several hours or days until the patient’s hemodynamic status improves. The duration of perfusion or total cumulative dose cannot be predicted.
After hemodynamic stabilization, wean incrementally over time, such as by decreasing doses of epinephrine every 30 minutes over a 12- to 24-hour period.
2.3 Anaphylaxis
Inject epinephrine intramuscularly or subcutaneously into the anterolateral aspect of the thigh, through clothing if necessary. When administering to a child, to minimize the risk of injection related injury, hold the leg firmly in place and limit movement prior to and during an injection. The injection may be repeated every 5 to 10 minutes as necessary. For intramuscular administration, use a needle long enough (at least 1/2 inch to 5/8 inch) to ensure the injection is administered into the muscle. Monitor the patient clinically for the severity of the allergic reaction and potential cardiac effects of the drug, with repeat doses titrated to effect. Do not administer repeated injections at the same site, as the resulting vasoconstriction may cause tissue necrosis.
Adults and Children 30 kg (66 lbs) or more: 0.3 to 0.5 mg (0.3 mL to 0.5 mL) of undiluted epinephrine administered intramuscularly or subcutaneously in the anterolateral aspect of the thigh, up to a maximum of 0.5 mg (0.5 mL) per injection, repeated every 5 to 10 minutes as necessary. Monitor clinically for reaction severity and cardiac effects.
Children less than 30 kg (66 lbs): 0.01 mg/kg (0.01 mL/kg) of undiluted epinephrine administered intramuscularly or subcutaneously in the anterolateral aspect of the thigh repeated every 5 to 10 minutes as necessary. Monitor clinically for reaction severity and cardiac effects.
-
3 DOSAGE FORMS AND STRENGTHS
Injection solution: 1 mL single-dose clear glass vial containing 1 mg/mL epinephrine as a sterile, nonpyrogenic, clear and colorless solution.
Injection solution: 10 mL multiple dose amber glass vial containing 10 mg/10 mL (1 mg/mL) epinephrine as a sterile, nonpyrogenic, clear and colorless solution.
Injection solution: 30 mL multiple dose amber glass vial containing 30 mg/30 mL (1 mg/mL) epinephrine as a sterile, nonpyrogenic, clear and colorless solution.
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Hypertension
When Epinephrine Injection is administered intravenously, titrate the infusion while monitoring vital signs. Invasive arterial blood pressure monitoring and central venous pressure monitoring are recommended. Because of varying response to epinephrine, dangerously high blood pressure may occur [see Drug Interactions (7)].
5.2 Extravasation and Tissue Necrosis with Intravenous Infusion
When Epinephrine Injection is administered intravenously, the infusion site should be checked frequently for free flow. Avoid extravasation of epinephrine into the tissues, to prevent local necrosis. Blanching along the course of the infused vein, sometimes without obvious extravasation, may be attributed to vasa vasorum constriction with increased permeability of the vein wall, permitting some leakage. This also may progress on rare occasions to superficial slough. Hence, if blanching occurs, consider changing the infusion site at intervals to allow the effects of local vasoconstriction to subside.
Antidote for Extravasation Ischemia: To prevent sloughing and necrosis in areas in which extravasation has taken place, infiltrate the area with 10 mL to 15 mL of saline solution containing from 5 mg to 10 mg of phentolamine, an adrenergic blocking agent. Use a syringe with a fine hypodermic needle, with the solution being infiltrated liberally throughout the area, which is easily identified by its cold, hard, and pallid appearance. Sympathetic blockade with phentolamine causes immediate and conspicuous local hyperemic changes if the area is infiltrated within 12 hours.
5.3 Incorrect Locations of Injection for Anaphylaxis
When Epinephrine Injection is used for the treatment of anaphylaxis, the most appropriate location for administration is into the anterolateral aspect of the thigh (vastus lateralis muscle) because of its location, size, and available blood flow. Injection into (or near) smaller muscles, such as in the deltoid, is not recommended due to possible differences in absorption associated with this use.
Do not administer repeated injections of epinephrine at the same site, as the resulting vasoconstriction may cause tissue necrosis.
Do not inject into buttock. Injection into the buttock may not provide effective treatment of anaphylaxis and has been associated with the development of Clostridial infections (gas gangrene). Cleansing with alcohol does not kill bacterial spores, and therefore, does not lower this risk.
Do not inject into digits, hands, or feet. Epinephrine is a strong vasoconstrictor. Accidental injection into the digits, hands or feet may result in loss of blood flow to the affected area and has been associated with tissue necrosis.
5.4 Pulmonary Edema
When Epinephrine Injection is administered intravenously, there is risk of pulmonary edema because of the peripheral constriction and cardiac stimulation produced. Treatment of pulmonary edema consists of a rapidly acting alpha-adrenergic blocking drug (such as phentolamine mesylate) and respiratory support.
5.5 Renal Impairment
Intravenously administered epinephrine initially may produce constriction of renal blood vessels and decrease urine formation.
5.6 Cardiac Arrhythmias and Ischemia
Epinephrine may induce cardiac arrhythmias and angina pectoris in patients, especially patients suffering from coronary artery disease, organic heart disease, cerebrovascular disease, hypertension, or patients who are receiving drugs that sensitize the myocardium [see Adverse Reactions (6) and Drug Interactions (7)]. Treatment of arrhythmias consists of administration of a beta-adrenergic blocking drug (such as propranolol).
5.7 Serious Infections at the Injection Site
Rare cases of serious skin and soft tissue infections, including necrotizing fasciitis and myonecrosis caused by Clostridia (gas gangrene), have been reported at the injection site following epinephrine injection for anaphylaxis. Clostridium spores can be present on the skin and introduced into the deep tissue with subcutaneous or intramuscular injection. While cleansing with alcohol may reduce presence of bacteria on the skin, alcohol cleansing does not kill Clostridium spores. To decrease the risk of Clostridium infection, do not inject Epinephrine Injection into the buttock [see Warnings and Precautions (5.3)]. Advise patients to seek medical care if they develop signs or symptoms of infection, such as persistent redness, warmth, swelling, or tenderness, at the epinephrine injection site.
5.8 Other Disease Interactions
Epinephrine should be administered with caution to patients with hyperthyroidism, Parkinson’s disease, diabetes mellitus, pheochromocytoma, elderly individuals, and pregnant women. Patients with Parkinson’s disease may experience psychomotor agitation or notice a temporary worsening of symptoms. Diabetic patients may experience transient increases in blood sugar. Despite these concerns, the presence of these conditions is not a contraindication to epinephrine administration in an acute, life-threatening situation.
5.9 Allergic Reactions Associated with Sulfite
Epinephrine is the preferred treatment for serious allergic or other emergency situations even though this product contains sodium metabisulfite, a sulfite that may in other products cause allergic-type reactions including anaphylactic symptoms or life-threatening or less severe asthmatic episodes in certain susceptible persons. The alternatives to using epinephrine in a life-threatening situation may not be satisfactory. The presence of sulfite(s) in this product should not deter administration of the drug for treatment of serious allergic or other emergency situations.
-
6 ADVERSE REACTIONS
6.1 Adverse Reactions associated with Epinephrine Infusion (for Hypotension associated with Septic Shock)
The following adverse reactions associated with the infusion of epinephrine were identified in the literature. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to estimate their frequency reliably or to establish a causal relationship to drug exposure.
Cardiovascular disorders: tachycardia, supraventricular tachycardia, ventricular arrhythmias, myocardial ischemia, myocardial infarction, limb ischemia, pulmonary edema
Gastrointestinal disorders: Nausea, vomiting
General disorders and administrative site conditions: Chest pain, extravasation,
Metabolic: hypoglycemia, hyperglycemia, insulin resistance, hypokalemia, lactic acidosis
Nervous system disorders: Headache, nervousness, paresthesia, tremor, stroke, central nervous system bleeding
Psychiatric disorders: Excitability
Renal disorders: Renal insufficiency
Respiratory: Pulmonary edema, rales
Skin and subcutaneous tissue disorders: Diaphoresis, pallor, piloerection, skin blanching, skin necrosis with extravasation
6.2 Adverse Reactions associated with Intramuscular or Subcutaneous Use (for Anaphylaxis)
Common adverse reactions to systemically administered epinephrine include anxiety, apprehensiveness, restlessness, tremor, weakness, dizziness, sweating, palpitations, pallor, nausea and vomiting, headache, and respiratory difficulties. These symptoms occur in some persons receiving therapeutic doses of epinephrine, but are more likely to occur in patients with heart disease, hypertension, or hyperthyroidism [see Warnings and Precautions (5.8)].
Due to the lack of randomized, controlled clinical trials of epinephrine for the treatment of anaphylaxis, the true incidence of adverse reactions associated with the systemic use of epinephrine is difficult to determine. Adverse reactions reported in observational trials, case reports, and studies are listed below by body system:
Cardiovascular [see Warnings and Precautions (5.6)]: angina, arrhythmias, hypertension, pallor, palpitations, tachyarrhythmia, tachycardia, vasoconstriction, and ventricular ectopy. Angina may occur in patients with coronary artery disease. Arrhythmias, including fatal ventricular fibrillation, have occurred, particularly in patients with underlying organic heart disease or patients receiving drugs that sensitize the heart to arrhythmias. Rapid rises in blood pressure associated with epinephrine use have produced cerebral hemorrhage, particularly in elderly patients with cardiovascular disease.
Respiratory: respiratory difficulties.
Neurological: dizziness, disorientation, excitability, headache, impaired memory, lightheadedness, nervousness, panic, psychomotor agitation, sleepiness, tingling, tremor, and weakness.
Psychiatric: anxiety, apprehensiveness, restlessness.
Gastrointestinal: nausea, vomiting.
Skin: sweating.
Other: Patients with Parkinson’s disease may experience psychomotor agitation or a temporary worsening of symptoms [see Warnings and Precautions (5.8)]. Diabetic patients may experience transient increases in blood sugar [see Warnings and Precautions (5.8)].
Accidental injection into the digits, hands or feet may result in loss of blood flow to the affected area [ see Warnings and Precautions (5.3)]. Adverse events experienced as a result of an injection into these areas include increased heart rate, local reactions including injection site pallor, coldness, hypoesthesia, and tissue loss, or injury at the injection site resulting in bruising, bleeding, discoloration, erythema, and skeletal injury.
Injection into the buttock has resulted in cases of gas gangrene [see Warnings and Precautions (5.3)].
Rare cases of serious skin and soft tissue infections, including necrotizing fasciitis and myonecrosis caused by Clostridia (gas gangrene), have been reported following epinephrine injection in the thigh [see Warnings and Precautions (5.7)].
-
7 DRUG INTERACTIONS
Drugs antagonizing pressor effects of epinephrine
- α-blockers, such as phentolamine
- Vasodilators, such as nitrates
- Diuretics
- Antihypertensives
- Ergot alkaloids
Drugs potentiating pressor effects of epinephrine
- Sympathomimetics
- β-blockers, such as propranolol
- Tricyclic anti-depressants
- Monoamine oxidase (MAO) inhibitors
- Catechol-O-methyl transferase (COMT) inhibitors, such as entacapone
- Clonidine
- Doxapram
- Oxytocin
Drugs potentiating arrhythmogenic effects of epinephrine
Patients who are concomitantly receiving any of the following drugs should be observed carefully for the development of cardiac arrhythmias [see Warnings and Precautions (5.6) and Adverse Reactions (6)].
- β-blockers, such as propranolol
- Cyclopropane or halogenated hydrocarbon anesthetics, such as halothane
- Antihistamines
- Thyroid hormones
- Diuretics
- Cardiac glycosides, such as digitalis glycosides
- Quinidine
Drugs potentiating hypokalemic effects of epinephrine
- Potassium depleting diuretics
- Corticosteroids
- Theophylline
Epinephrine should not be used to counteract circulatory collapse or hypotension caused by phenothiazines, as a reversal of the pressor effects of epinephrine may result in further lowering of blood pressure.
Epinephrine may antagonize the neuronal blockade produced by guanethidine resulting in decreased antihypertensive effect and requiring increased dosage of the latter.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Prolonged experience with epinephrine use in pregnant women over several decades, based on published literature, does not identify a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. However, there are risks to the mother and fetus associated with epinephrine use during labor or delivery (see Clinical Considerations). In animal reproduction studies, epinephrine administered by the subcutaneous route to pregnant rabbits, mice, and hamsters, during the period of organogenesis, resulted in adverse developmental effects (including gastroschisis, embryonic lethality, and delayed skeletal ossification) at doses approximately 2 times the maximum recommended daily intramuscular, subcutaneous, or intravenous dose (see Data).
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the United States general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively.
Clinical Considerations
Disease-associated maternal and/or embryo/fetal risk
During pregnancy, anaphylaxis can be catastrophic and can lead to hypoxic-ischemic encephalopathy and permanent central nervous system damage or death in the mother and, more commonly, in the fetus or neonate. The prevalence of anaphylaxis occurring during pregnancy is reported to be approximately 3 cases per 100,000 deliveries.
Management of anaphylaxis during pregnancy is similar to management in the general population. Epinephrine is the first line-medication of choice for treatment of anaphylaxis; it should be used in the same manner in pregnant and non-pregnant patients. In conjunction with the administration of epinephrine, the patient should seek immediate medical or hospital care.
Hypotension associated with septic shock is a medical emergency in pregnancy which can be fatal if left untreated. Delaying treatment in pregnant women with hypotension associated with septic shock may increase the risk of maternal and fetal morbidity and mortality. Life-sustaining therapy for the pregnant woman should not be withheld due to potential concerns regarding the effects of epinephrine on the fetus.
Labor or Delivery
Epinephrine usually inhibits spontaneous or oxytocin-induced contractions of the pregnant human uterus and may delay the second stage of labor. Avoid epinephrine during the second stage of labor. In dosage sufficient to reduce uterine contractions, the drug may cause a prolonged period of uterine atony with hemorrhage. Avoid epinephrine in obstetrics when maternal blood pressure exceeds 130/80 mmHg.
Although epinephrine may improve maternal hypotension associated with septic shock and anaphylaxis, it may result in uterine vasoconstriction, decreased uterine blood flow, and fetal anoxia.
Data
Animal Data
In an embryofetal development study with pregnant rabbits dosed during the period of organogenesis (on days 3 to 5, 6 to 7, or 7 to 9 of gestation), epinephrine caused teratogenic effects (including gastroschisis) at doses approximately 15 times the maximum recommended intramuscular, subcutaneous, or intravenous dose (on a mg/m2 basis at a maternal subcutaneous dose of 1.2 mg/kg/day for 2 to 3 days). Animals treated on days 6 to 7 had decreased number of implantations.
In an embryofetal development study, pregnant mice were administered epinephrine (0.1 to 10 mg/kg/day) on Gestation Days 6 to 15. Teratogenic effects, embryonic lethality, and delays in skeletal ossification were observed at approximately 3 times the maximum recommended intramuscular, subcutaneous, or intravenous dose (on a mg/m2 basis at maternal subcutaneous dose of 1 mg/kg/day for 10 days). These effects were not seen in mice at approximately 2 times the maximum recommended daily intramuscular or subcutaneous dose (on a mg/m2 basis at a subcutaneous maternal dose of 0.5 mg/kg/day for 10 days).
In an embryofetal development study with pregnant hamsters dosed during the period of organogenesis from gestation days 7 to 10, epinephrine produced reductions in litter size and delayed skeletal ossification at doses approximately 2 times the maximum recommended intramuscular, subcutaneous, or intravenous dose (on a mg/m2 basis at a maternal subcutaneous dose of 0.5 mg/kg/day).
8.2 Lactation
Risk Summary
There is no information regarding the presence of epinephrine in human milk or the effects of epinephrine on the breastfed infant or on milk production. However, due to its poor oral bioavailability and short half-life, epinephrine exposure is expected to be very low in the breastfed infant.
Epinephrine is the first-line medication of choice for treatment of anaphylaxis; it should be used in the same manner for anaphylaxis in breastfeeding and non-breastfeeding patients.
8.4 Pediatric Use
Safety and effectiveness of epinephrine in pediatric patients with septic shock have not been established.
Clinical use data support weight-based dosing for treatment of anaphylaxis in pediatric patients, and other reported clinical experience with the use of epinephrine suggests that the adverse reactions seen in children are similar in nature and extent to those both expected and reported in adults.
8.5 Geriatric Use
Clinical studies of epinephrine for the treatment of hypotension associated with septic shock did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
Clinical studies for the treatment of anaphylaxis have not been performed in subjects aged 65 and over to determine whether they respond differently from younger subjects. However, other reported clinical experience with use of epinephrine for the treatment of anaphylaxis has identified that geriatric patients may be particularly sensitive to the effects of epinephrine. Therefore, for the treatment of anaphylaxis, consider starting with a lower dose to take into account potential concomitant disease or other drug therapy.
-
10 OVERDOSAGE
Overdosage of epinephrine may produce extremely elevated arterial pressure, which may result in cerebrovascular hemorrhage, particularly in elderly patients. Overdosage may also result in pulmonary edema because of peripheral vascular constriction together with cardiac stimulation. Epinephrine overdosage may also cause transient bradycardia followed by tachycardia and these may be accompanied by potentially fatal cardiac arrhythmias. Premature ventricular contractions may appear within one minute after injection and may be followed by multifocal ventricular tachycardia (prefibrillation rhythm). Subsidence of the ventricular effects may be followed by atrial tachycardia and occasionally by atrioventricular block. Myocardial ischemia and infarction, cardiomyopathy, extreme pallor and coldness of the skin, metabolic acidosis due to elevated blood lactic acid levels, and renal insufficiency and failure have also been reported.
Epinephrine is rapidly inactivated in the body and treatment following overdose is primarily supportive. Treatment of pulmonary edema consists of a rapidly acting alpha-adrenergic blocking drug (such as phentolamine mesylate) and respiratory support. Treatment of arrhythmias consists of administration of a beta-adrenergic blocking drug (such as propranolol). If necessary, pressor effects may be counteracted by rapidly acting vasodilators (such as nitrites) or alpha-adrenergic blocking drugs. If prolonged hypotension follows such measures, it may be necessary to administer another pressor drug.
-
11 DESCRIPTION
Epinephrine Injection, USP is a clear, colorless, sterile solution containing 1 mg/mL epinephrine.
1 mL Single-dose Vial:
1 mL single-dose clear glass vial containing 1 mg/mL epinephrine as a sterile, nonpyrogenic, clear and colorless solution. Each mL of Epinephrine Injection, USP solution contains 1 mg epinephrine, 8.60 mg sodium chloride, 0.75 mg sodium metabisulfite, hydrochloric acid for pH adjustment and water for injection. The pH range is 2.2-5.0.
10 mL Multiple dose Vial:
10 mL multiple dose amber glass vial containing 10 mg/10 mL (1 mg/mL) epinephrine as a sterile, nonpyrogenic, clear and colorless solution. Each 1 mL of Epinephrine Injection, USP solution contains 1 mg epinephrine, 5.0 mg chlorobutanol as preservative, 7.5 mg sodium chloride, 0.5 mg sodium metabisulfite, hydrochloric acid for pH adjustment and water for injection. The pH range is 2.2-5.0.30 mL Multiple dose Vial:
30 mL multiple dose amber glass vial containing 30 mg/30 mL epinephrine as a sterile, nonpyrogenic, clear and colorless solution. Each 1 mL of Epinephrine Injection, USP solution contains 1 mg epinephrine, 5.0 mg chlorobutanol as preservative, 7.5 mg sodium chloride, 0.5 mg sodium metabisulfite, hydrochloric acid for pH adjustment and water for injection. The pH range is 2.2-5.0.Epinephrine is a sympathomimetic catecholamine. The chemical name of epinephrine is: 1,2- Benzenediol, 4-[(1R)-1-hydroxy-2-(methylamino)ethyl]-, or (-)-3,4-Dihydroxy-α-[2- (methylamino)ethyl]benzyl alcohol. The chemical structure of epinephrine is:
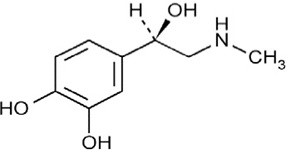
The molecular weight of epinephrine is 183.2.
Epinephrine solution deteriorates rapidly on exposure to air or light, turning pink from oxidation to adrenochrome and brown from the formation of melanin.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Epinephrine acts on both alpha (α)- and beta (β)-adrenergic receptors. The mechanism of the rise in blood pressure is 3-fold: a direct myocardial stimulation that increases the strength of ventricular contraction (positive inotropic action), an increased heart rate (positive chronotropic action), and peripheral vasoconstriction.
12.2 Pharmacodynamics
Intravenous use for hypotension associated with septic shock
Following intravenous administration of epinephrine, increases in systolic blood pressure and heart rate are observed. Decreases in systemic vascular resistance and diastolic blood pressure are observed at low doses of epinephrine because of β2-mediated vasodilation, but are overtaken by α1-mediated peripheral vasoconstriction at higher doses leading to increase in diastolic blood pressure. The onset of blood pressure increase following an intravenous dose of epinephrine is < 5 minutes and the time to offset blood pressure response occurs within 20 min. Most vascular beds are constricted including renal, splanchnic, mucosal and skin.
Intramuscular and subcutaneous use for anaphylaxis
Through its action on alpha-adrenergic receptors, epinephrine lessens the vasodilation and increased vascular permeability that occurs during anaphylaxis, which can lead to loss of intravascular fluid volume and hypotension.
Through its action on beta-adrenergic receptors, epinephrine causes bronchial smooth muscle relaxation and helps alleviate bronchospasm, wheezing and dyspnea that may occur during anaphylaxis.
Epinephrine also alleviates pruritus, urticaria, and angioedema and may relieve gastrointestinal and genitourinary symptoms associated with anaphylaxis because of its relaxer effects on the smooth muscle of the stomach, intestine, uterus and urinary bladder.
Epinephrine increases glycogenolysis, reduces glucose up take by tissues, and inhibits insulin release in the pancreas, resulting in hyperglycemia and increased blood lactic acid [see Warnings and Precautions (5.8)].
12.3 Pharmacokinetics
When administered parenterally, epinephrine has a rapid onset and short duration of action.
Following intravenous injection, epinephrine is rapidly cleared from the plasma with an effective half-life of < 5 min. A pharmacokinetic steady state following continuous intravenous infusion is achieved within 10 to 15 min. In patients with septic shock, epinephrine displays dose-proportional pharmacokinetics in the infusion dose range of 0.03 mcg/kg/min to 1.7 mcg/kg/min.
Epinephrine is extensively metabolized with only a small amount excreted unchanged.
Epinephrine is rapidly degraded to vanillylmandelic acid, an inactive metabolite, by monoamine oxidase and catechol-O-methyltransferase that are abundantly expressed in the liver, kidneys and other extraneuronal tissues. The tissues with the highest contribution to removal of circulating exogenous epinephrine are the liver (32%), kidneys (25%), skeletal muscle (20%), and mesenteric organs (12%).
Special Populations
Elderly
In a pharmacokinetic study of 45-minute epinephrine infusions given to healthy men aged 20 to 25 years and healthy men aged 60 to 65 years, the mean plasma metabolic clearance rate of epinephrine at steady state was greater among the older men (144.8 versus 78 mL/kg/min for a 14.3 ng/kg/min infusion).
Body Weight
Body weight has been found to influence epinephrine pharmacokinetics. Higher body weight was associated with a higher plasma epinephrine clearance and a lower concentration plateau.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term studies to evaluate the carcinogenic potential of epinephrine have not been conducted.
Epinephrine and other catecholamines have been shown to have mutagenic potential in vitro. Epinephrine was positive in the Salmonella bacterial reverse mutation assay, positive in the mouse lymphoma assay, and negative in the in vivo micronucleus assay. Epinephrine is an oxidative mutagen based on the E. coli WP2 Mutoxitest bacterial reverse mutation assay. This should not prevent the use of epinephrine under the conditions noted under the Indications and Usage.
The potential for epinephrine to impair reproductive performance has not been evaluated, but epinephrine has been shown to decrease implantation in female rabbits dosed subcutaneously with 1.2 mg/kg/day (15-fold the highest human intramuscular or subcutaneous daily dose) during gestation days 3 to 9.
13.2 Animal Toxicology and/or Pharmacology
Epinephrine was associated with metabolic effects, decreased mesentery, coronary and renal conductance in a sheep model of septic shock. Data from hemolysis study have shown that epinephrine at 1:1000 dilution is non-hemolytic. Epinephrine infusion significantly increased the MAP (69 vs. 86 mmHg) and cardiac output (6.4 vs. 7.1 L/min) and decreased renal blood flow (330 vs. 247 mL/min).
- 14 CLINICAL STUDIES
-
16 HOW SUPPLIED/STORAGE AND HANDLING
Epinephrine Injection supplied as a clear colorless solution available as follows:
1 mL Single-dose Vial:
Each carton contains 10 single-dose vials containing 1 mL of a 1 mg/mL epinephrine injection, USP solution in a clear glass vial.
NDC 54288-119-10 Box of 10 × 1 mL Single-Dose Vials
Each carton contains 25 single-dose vials containing 1 mL of a 1 mg/mL epinephrine injection, USP solution in a clear glass vial.
NDC 54288-119-25 Box of 25 × 1 mL Single-Dose Vials
10 mL Multiple dose Vial:
Each carton contains 1 multiple dose vial containing 10 mg/10 mL (1 mg/mL) epinephrine injection, USP solution in an amber glass vial.
NDC 54288-120-01 10 mL Multiple Dose Vial
Multiple Dose Vial and contents must be discarded 30 days after initial use.
30 mL Multiple dose Vial:
Each carton contains 1 multiple dose vial containing 30 mg/30 mL (1 mg/mL) epinephrine injection, USP solution in an amber glass vial.NDC 54288-152-01 30 mL Multiple Dose Vial
Multiple Dose Vial and contents must be discarded 30 days after initial use.
Epinephrine is light sensitive. Protect from light until ready to use.
Do not refrigerate. Protect from freezing.
Vial and contents must be discarded 30 days after initial use.
Store at room temperature, between 20°C to 25°C (68°F to 77°F). (See USP Controlled Room Temperature.) Protect from alkalis and oxidizing agents.
-
17 PATIENT COUNSELING INFORMATION
Advise patients or their caregivers about common adverse reactions associated with the use of epinephrine, including an increase in heart rate, the sensation of a more forceful heartbeat, palpitations, sweating, nausea and vomiting, difficulty breathing, pallor, dizziness, weakness or shakiness, headache, apprehension, nervousness, or anxiety. These symptoms and signs usually subside rapidly, especially with rest, quiet and recumbent positioning.
Warn patients with a good response to initial treatment about the possibility of recurrence of anaphylaxis symptoms and instruct patients to obtain medical attention if symptoms return.
Advise patients with diabetes that they may develop increased blood glucose levels following epinephrine administration.
Rare cases of serious skin and soft tissue infections, including necrotizing fasciitis and myonecrosis caused by Clostridia (gas gangrene), have been reported at the injection site following epinephrine injection for anaphylaxis. Advise patients to seek medical care if they develop signs or symptoms of infection, such as persistent redness, warmth, swelling, or tenderness, at the epinephrine injection site [see Warnings and Precautions (5.7)].
- SPL UNCLASSIFIED SECTION
- PACKAGE LABEL PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
EPINEPHRINE
epinephrine injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:54288-120 Route of Administration INTRAVENOUS, INTRAMUSCULAR, SUBCUTANEOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength EPINEPHRINE (UNII: YKH834O4BH) (EPINEPHRINE - UNII:YKH834O4BH) EPINEPHRINE 1 mg in 1 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:54288-120-01 1 in 1 CARTON 03/16/2022 1 10 mL in 1 VIAL; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA205029 03/16/2022 EPINEPHRINE
epinephrine injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:54288-119 Route of Administration INTRAVENOUS, INTRAMUSCULAR, SUBCUTANEOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength EPINEPHRINE (UNII: YKH834O4BH) (EPINEPHRINE - UNII:YKH834O4BH) EPINEPHRINE 1 mg in 1 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:54288-119-10 10 in 1 CARTON 03/07/2024 1 1 mL in 1 VIAL; Type 0: Not a Combination Product 2 NDC:54288-119-25 25 in 1 CARTON 03/07/2024 2 1 mL in 1 VIAL; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA205029 03/07/2024 EPINEPHRINE
epinephrine injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:54288-152 Route of Administration INTRAVENOUS, INTRAMUSCULAR, SUBCUTANEOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength EPINEPHRINE (UNII: YKH834O4BH) (EPINEPHRINE - UNII:YKH834O4BH) EPINEPHRINE 30 mg in 30 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:54288-152-01 1 in 1 CARTON 03/21/2024 1 30 mL in 1 VIAL; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA205029 03/21/2024 Labeler - BPI Labs, LLC (078627620) Establishment Name Address ID/FEI Business Operations BPI Labs, LLC 078627620 manufacture(54288-119, 54288-120, 54288-152) , analysis(54288-119, 54288-120, 54288-152)