Label: MANNITOL injection, solution


- NDC Code(s): 63323-024-01, 63323-024-25
- Packager: Fresenius Kabi USA, LLC
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: Abbreviated New Drug Application
Drug Label Information
Updated March 16, 2023
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
- SPL UNCLASSIFIED SECTION
-
DESCRIPTION
Mannitol is a 6-carbon sugar alcohol and has the following structure:
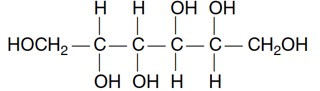
C6H14O6 182.17
Mannitol occurs naturally in fruits and vegetables, and is metabolically inert in humans.
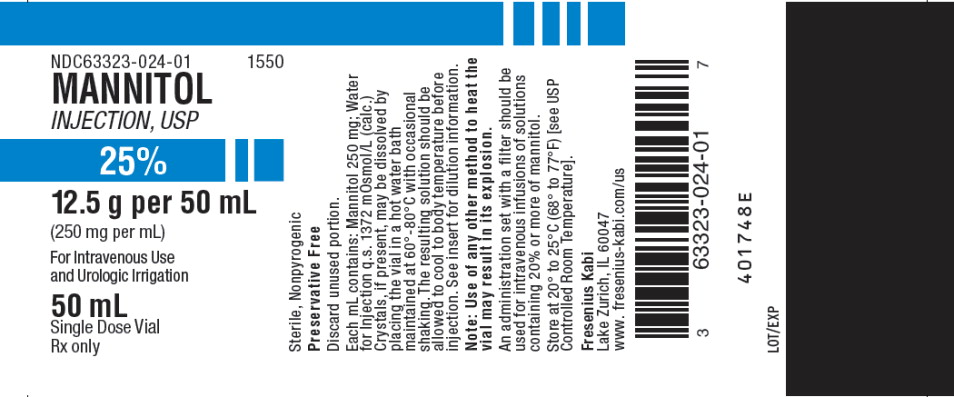
Mannitol Injection, USP, 25%, an osmotic diuretic, is a sterile, nonpyrogenic solution of mannitol in Water for Injection. It is a supersaturated solution at room temperature.
Each mL contains: Mannitol 250 mg; Water for Injection q.s. The osmolar concentration is 1372 mOsmol/L (calc.). It contains no antimicrobial agents. The pH of a 5% solution is between 4.5 and 7.0.
-
CLINICAL PHARMACOLOGY
Mannitol is an osmotic diuretic. After intravenous injection it is confined to the extracellular space, metabolized only slightly and excreted rapidly by the kidneys. Approximately 80% of a 100 g dose appears in the urine in three hours. Mannitol is freely filtered by the glomeruli with less than 10% tubular reabsorption. It is not secreted by tubular cells. It induces diuresis by elevating the osmolarity of the glomerular filtrate and thereby hinders tubular reabsorption of water. Urinary output of water and excretion of sodium and chloride are enhanced. Mannitol is poorly absorbed from the gastrointestinal tract.
Mannitol injection is free of electrolytes and is used in urology as a nonhemolytic irrigant. The amount of mannitol absorbed intravascularly during transurethral prostatic surgery is variable and depends primarily on the extent of the surgery. Such mannitol is excreted by the kidneys and produces osmotic diuresis.
-
INDICATIONS AND USAGE
For Intravenous Injection
Mannitol Injection, USP is indicated for the following therapeutic uses:
• The promotion of diuresis, in the prevention and/or treatment of the oliguric phase of acute renal failure before irreversible renal failure becomes established.
• The reduction of intracranial pressure and treatment of cerebral edema by reducing brain mass.
• The reduction of elevated intraocular pressure when it cannot be lowered by other means.
• The promotion of urinary excretion of toxic substances.
-
CONTRAINDICATIONS
• Well established anuria due to severe renal disease.
• Severe pulmonary congestion or frank pulmonary edema.
• Active intracranial bleeding except during craniotomy.
• Severe dehydration.
• Progressive renal damage or dysfunction after institution of mannitol therapy, including increasing oliguria and azotemia.
• Progressive heart failure or pulmonary congestion after mannitol therapy is started.
-
WARNINGS
In severe impairment of renal function a test dose should be given (see DOSAGE AND ADMINISTRATION). A second test dose may be given if there is an inadequate response. No more than two test doses should be attempted.
Excessive loss of water and electrolytes may lead to serious imbalances. Serum sodium and potassium should be carefully monitored during mannitol therapy.
The diuresis after rapid infusion of mannitol may increase preexisting hemoconcentration. With continued use of mannitol a loss of water in excess of electrolytes can cause hypernatremia.
Shift of sodium-free intracellular fluid into the extracellular compartment after mannitol infusion may lower serum sodium concentration and aggravate preexisting hyponatremia.
Closely monitor the urine output and discontinue mannitol infusion promptly if output is low. Inadequate urine output results in accumulation of mannitol, expansion of extracellular fluid volume and could result in water intoxication or congestive heart failure. Renal function must be closely monitored during mannitol infusion.
Mannitol solution must be used with caution in patients with significant cardiopulmonary or renal dysfunction.
Irrigating solutions used in transurethral prostatectomy have been shown to enter the systemic circulation in relatively large volumes, exert a systemic effect and may significantly alter cardiopulmonary and renal dynamics.
-
PRECAUTIONS
General
Crystals, if present in mannitol injection, 25%, may be dissolved by placing the vial in a hot water bath maintained at 60° to 80°C with occasional shaking. The resulting solution should be allowed to cool to body temperature before injection.
An administration set with a filter should be used for intravenous infusions of solutions containing 20% or more of mannitol.
NOTE: Use of any other method to heat the vial may result in its explosion.
The cardiovascular status should be carefully evaluated before mannitol is administered by rapid intravenous injection or before and during transurethral resection since expansion of extracellular fluid may lead to fulminating congestive heart failure.
By sustaining diuresis, mannitol may obscure and intensify inadequate hydration or hypovolemia.
Unless it is essential, electrolyte-free mannitol solutions should not be combined with blood. When it is essential to give the combination, at least 20 mEq of sodium chloride should be added to each liter of mannitol solution to avoid pseudoagglutination. The contents of opened containers should be used promptly and unused contents should be discarded.
A white flocculant mannitol precipitate may result from contact with PVC surfaces which act as nuclei for rapid rate crystallization of small crystals. This condition has also been reported to occur when mannitol has come in contact with other plastic and rough glass surfaces. Attempting to resolubilize the white flocculant precipitate with the aid of heat is not useful because crystallization may recur in a short period of time.
Carcinogenesis, Mutagenesis, Impairment of Fertility
In an early study of 1, 5 or 10% mannitol, given for 94 weeks in the diet of Wistar rats, a low incidence of benign thymomas occurred in females which was apparently treatment related. A subsequent life-time study at similar dose levels in Spraque-Dawley, Fischer and Wistar rats revealed no carcinogenic effect in the thymus.
Mannitol had no mutagenic activity in a series of in vitro and in vivo test systems.
Adequate studies measuring the effects of mannitol on fertility have not been done.
Pregnancy
Pregnancy Category B–Teratogenic studies in the mouse, rat and rabbit at oral doses up to 1600 mg/kg did not reveal harm to the fetus or adverse effects on reproduction due to mannitol. There are, however, no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.
-
ADVERSE REACTIONS
Reactions are infrequent and may include:
To report SUSPECTED ADVERSE REACTIONS, contact Fresenius Kabi USA, LLC at 1-800-551-7176 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Metabolic: fluid and electrolyte imbalance, acidosis, dehydration.
Gastrointestinal: dryness of mouth, nausea, vomiting, diarrhea.
Genitourinary: osmotic nephrosis, urinary retention.
Central Nervous System: headache, convulsions, dizziness.
Special Senses: Blurred vision, rhinitis.
Cardiovascular: pulmonary edema, edema, hypotension, hypertension, tachycardia, angina-like chest pains.
Dermatologic: skin necrosis, thrombophlebitis.
Hypersensitivity: urticaria.
Miscellaneous: thirst, arm pain, chills, fever.
-
DOSAGE AND ADMINISTRATION
For Intravenous Injection
General Recommendations–Give mannitol injection only intravenously. The total dosage, concentration and rate of administration should be governed by the nature and severity of the condition being treated, fluid requirement and urinary output. Usual adult dosage ranges from 50 to 200 g in 24 hours but in most instances an adequate response will be achieved at a dosage of approximately 100 g in 24 hours. The rate is usually adjusted to maintain an adequate urine flow (at least 30 to 50 mL/hr).
Test Dose–In marked oliguria or inadequate renal function a test dose of mannitol should be given. The test dose may be approximately 0.2 g/kg (about 50 mL of a 25% solution) infused in three to five minutes to produce an adequate urine flow (at least 30 to 50 mL/hr). If urine flow does not increase within two or three hours a second test dose may be given. If there is an inadequate response the patient should be reevaluated.
Prevention of Acute Renal Failure (Oliguria)–When used during surgery, immediately postoperatively or following trauma, 50 to100 g of mannitol as a 5 to 25% solution maybe given. The concentration and amount will depend upon the fluid requirements of the patient. Following suspected or actual hemolytic transfusion reactions 20 g of mannitol may be given intravenously over a five minute period to provoke diuresis. If diuresis does not occur the 20 g dose may be repeated. If there is an adequate urine flow (30 to 50 mL/hr) then intravenous fluids containing not more than 50 to 75 mEq of sodium per liter should be given in sufficient volume to match the desired urine flow (100 mL/hr) until fluids can be taken orally.
Treatment of Oliguria–The usual dose for treatment of oliguria is 50 to 100 g as a 15 to 25% solution.
Reduction of Intracranial Pressure, Cerebral Edema or Intraocular Pressure–A 25% solution of mannitol is recommended since its effectiveness depends on establishing intravascular hyperosmolarity. When used before or after surgery, a total dose of 1.5 to 2 g/kg can be given over a period of 30 to 60 minutes. Careful evaluation must be made of the circulatory and renal reserve prior to and during use of mannitol at this relatively high dose and rapid infusion rate. Careful attention must be paid to fluid and electrolyte balance, body weight, and total input and output before and after infusion of mannitol. Evidence of reduced cerebral spinal fluid pressure may be observed within 15 minutes after starting infusion.
Maximal reduction of intraocular pressure occurs 30 to 60 minutes after injection.
Urinary Excretion of Toxic Substances–Mannitol in 5 to 25% solutions is used as an infusion as long as indicated if the level of urinary output remains high. The concentration will depend upon the fluid requirement and urinary output. Intravenous water and electrolytes must be given to replace the loss of these substances in the urine, sweat and expired air. If benefits are not observed after 200 g of mannitol are given, discontinue it.
For Urologic Irrigation
A 2.5% solution is used. The use of 2.5% mannitol solution minimizes the hemolytic effect of water alone, the entrance of hemolyzed blood into the circulation, and the resulting hemoglobinemia which is considered a major factor in producing serious renal complications.
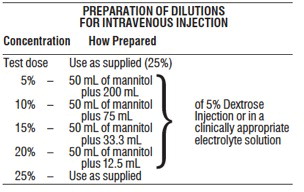
PREPARATION OF DILUTIONS
FOR UROLOGIC IRRIGATIONConcentration How Prepared 2.5% Add contents of two 50 mL vials (25% mannitol) to 900 mL Sterile Water for Injection. -
HOW SUPPLIED:
Mannitol Injection, USP, 25%
Product
CodeUnit of Sale Strength Each 1550 NDC 63323-024-25
Unit of 25250 mg per mL NDC 63323-024-01
50 mL Single Dose
Flip-off Top VialUse only if solution is clear and seal intact and undamaged.
Store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature].
Preservative Free. Discard unused portion.
- SPL UNCLASSIFIED SECTION
- PRINCIPAL DISPLAY PANEL
- PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
MANNITOL
mannitol injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:63323-024 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength MANNITOL (UNII: 3OWL53L36A) (MANNITOL - UNII:3OWL53L36A) MANNITOL 250 mg in 1 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:63323-024-25 25 in 1 TRAY 03/19/2000 1 NDC:63323-024-01 50 mL in 1 VIAL, SINGLE-DOSE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA080677 03/19/2000 Labeler - Fresenius Kabi USA, LLC (608775388) Establishment Name Address ID/FEI Business Operations Fresenius Kabi USA, LLC 840771732 manufacture(63323-024) , analysis(63323-024)