CEFAZOLIN- cefazolin sodium injection, powder, for solution
General Injectables & Vaccines, Inc
----------
Cefazolin for Injection USP 1 gram
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use CEFAZOLIN FOR INJECTION, USP safely and effectively. See full prescribing information for CEFAZOLIN FOR INJECTION, USP.
CEFAZOLIN FOR INJECTION, USP, for intravenous use
Initial U.S. Approval: 1973
To reduce the development of drug-resistant bacteria and maintain the effectiveness of cefazolin for injection and other antibacterial drugs, cefazolin for injection should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria.
INDICATIONS AND USAGE
Cefazolin for Injection, USP is a cephalosporin antibacterial indicated in the treatment of the following infections caused by susceptible isolates of the designated microorganisms:
- Respiratory tract infections. (1.1)
- Urinary tract infections. (1.2)
- Skin and skin structure infections. (1.3)
- Billiary tract infections. (1.4)
- Bone and joint infections. (1.5)
- Genital infections. (1.6)
- Septicemia. (1.7)
- Endocarditis. (1.8)
- Perioperative prophylaxis. (1.9)
DOSAGE AND ADMINISTRATION
For intravenous or intramuscular use. (2)
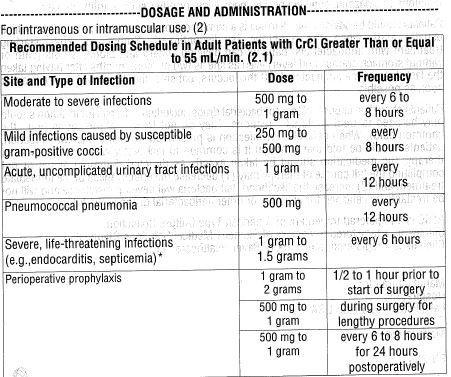
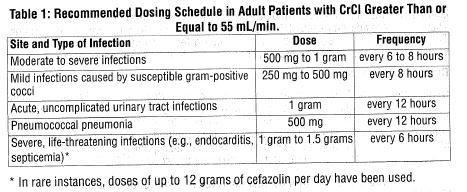
*In rare instances, doses of up to 12 grams of cefazolin per day have been used.
DOSAGE FORMS AND STRENGTHS
- 1 g per vial (3)
CONTRAINDICATIONS
- Hypersensitivity to cefazolin or other cephalosporin class antibacterial drugs, penicillins, or other beta-lactams. (4.1)
WARNINGS AND PRECAUTIONS
- Hypersensitivity Reactions: Cross-hypersensitivity may occur in up to 10% of patients with a history of penicillin allergy. If an allergic reaction occurs, discontinue the drug. (5.1)
- Use in Patients with Renal Impairment: Dose adjustment required for patients with CrCl less than 55 mL/min. (5.2)
- Clostridium difficile-associated Diarrhea: May range from mild diarrhea to fatal colitis. Evaluate if diarrhea occurs. (5.3)
ADVERSE REACTIONS
- Most common Adverse Reactions: Gastrointestinal (nausea, vomiting, diarrhea), and allergic reactions (anaphylaxis, urticaria, skin rash). (6)
To report SUSPECTED ADVERSE REACTIONS, contact Hospira, Inc. at 1-800-441-4100 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
Probenecid: May decrease renal tubular secreation of cephalosporins when used concurrently, resulting in increased and more prolonged cephalosproin blood concentrations. (7.1)
USE IN SPECIFIC POPULATIONS
- Pediatric Use: Safety and effectiveness for use in premature infants and neonates have not been established. See Dosage and Administration (2.4) for recommended dosage in pediatric patients older than 1 month. (8.4)
- Renal Impairment: Lower daily dosage of cefazolin for injection is required in patients with impaired renal function (creatinine clearance less than 55 mL/min). (8.6)
See 17 for PATIENT COUNSELING INFORMATION
Revised: 3/2015
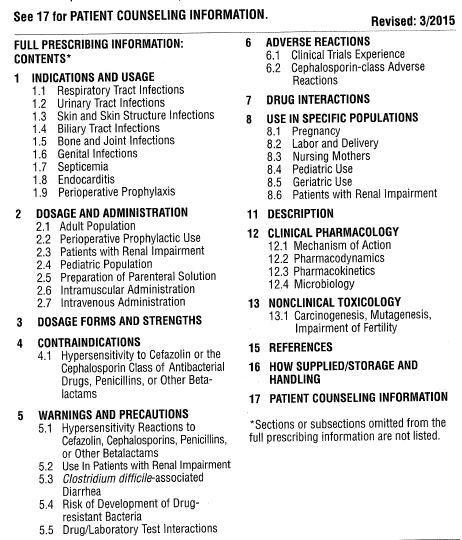
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
To reduce the development of drug-resistant bacteria and maintain the effectivness of Cefazolin for Injection, USP and other antibacterial drugs. Cefazolin for Injection, USP should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.
Cefazolin for Injection, USP is indicated for the treatment of the following infections when caused by susceptible bacteria.
1.1 Respiratory Tract Infections
Respiratory tract infections due to Streptococcus pneumoniae, Staphylococcus aureus and Streptococcus pyogenes.
Injectable benzatine penicillin is considered the drug of choice in treatment and prevention of streptococcal infections, including prophylaxis of rheumatic fever.
Cefazolin is effective in the eradication of streptococci from the nasopharynx; however, data establishing the efficacy of cefazolin in the subsequent prevention of rheumatic fever are not available.
1.2 Urinary Tract Infections
Urinary tract infections due to Escherichia coli, and Proteus mirabilis.
1.3 Skin and Skin Structure Infections
Skin and skin structure infections due to S. aureus, S. pyogenes, and Streptococcus agalactiae.
1.4 Biliary Tract Infections
Biliary tract infections due to E. coli, various isolates of streptococci, P. mirabilis,and S. aureus.
1.5 Bone and Joint Infections
Bone and joing infections due to S. aureus.
1.6 Genital Infections
Genital infections due to E. coli, and P. mirabilis.
1.7 Septicemia
Septicemia due to S. pneumoniae, S. aureus, P. mirabilis, and E. coli.
1.8 Endocarditis
Endocarditis due to S. aureus and S. pyogenes.
1.9 Perioperative Prophylaxis
The prophylactic administration of cefazolin preoperatively, intraoperatively, and postoperatively may reduce the incidence of certain postoperative infections in patients undergoing surgical procedures which are classified as contaminated or potentially contaminated (e.g., vaginal hysterectomy, and cholecystectomy in high-risk patients such as those older than 70 years, with acute cholecystitis,obstructive jaundice, or common duct bile stones).
DOSAGE AND ADMINISTRATION
2.1 Adult Population
The recommended adult dosages are outlined in Table 1. Cefazolin for injection should be administered intravenously (IV) or intramuscularly (IM).
2.2 Perioperative Prophylactic Use
To prevent postoperative infection in contaminated or potentially contaminated surgery, recommended doses are:
- 1 to 2 gram IV administered 1/2 hour to 1 hour prior to the start of surgery.
- For lengthy operative procedures (e.g., 2 hours or more), 500 mg to 1 gram IV during surgery (administration modified depending on the duration of the operative procedure).
- 500 mg to 1 gram IV every 6 to 8 hours for 24 hours postoperatively.
It is important that (i) the preoperative dose be given to just prior (1/2 hour to 1 hour) to the start of surgery so that adequate antibacterial concentrations are present in the serum and tissues at the time of initial surgical incision; and (ii) cefazolin be administered, if necessary, at appropriate intervals during surgery to provide sufficient concentrations of the antibacterial drug at the anticipated moments of greatest exposure to infective organisms.
The prophylactic administration of cefazolin should usually be discontinued within a 24-hour period after the surgical procedure. In surgery where the occurrence of infection may be particularly devastating (e.g.,open-heart surgery and prosthetic arthroplasty), the prophylactic administration of cefazolinmay be continued for 3 to 5 days following the completion of surgery.
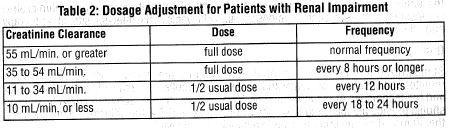
2.3 Patients with Renal Impairment
Cefazolin may be used in patients with renall impairment with the dosage adjustments outlined in Table 2. All reduced dosage recommendations apply after an initial loading dose appropriate to the severity of the infection.
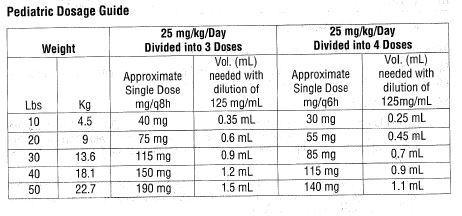
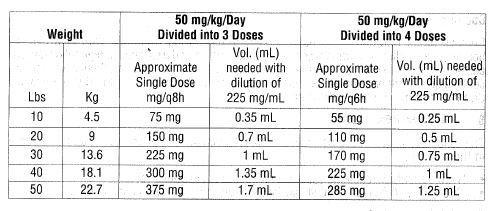
2.4 Pediatric Population
In pediatric patients, a total daily dosage of 25 to 50 mg per kg (approximately 10 to 20 mg per pound) of body weight, divided into 3 or 4 equal doses, is effective for most mild to moderately severe infections. Total daily dosage may be increased to 100 mg per kg (45 mg per pound) of body weight for severe infections. Since safety for use in premature infants and in neonates has not been established, the use of cefazolin for injection in these patients is not recommended.
In pediatric patients with mild to moderate renal impairment (creatinine clearance of 70 to 40 mL/min.), 60 percent of the normal daily dose given in equally divided doses every 12 hours should be sufficient. In patients with moderate impairment (creatinine clearance of 40 to 20 mL/min.), 25 percent of the normal daily dose given in equally divided doses every 12 hours should be adequate. Pediatric patients with sever renal impairment (creatinine clearance of 20 to 5 mL/min.) may be given 10 percent of the normal daily dose every 24 hours. All dosage recommendations apply after an initial loading dose.
2.5 Preparation of Parenteral Solution
Parental drug products should be SHAKEN WELL when reconstituted, and inspected visually for particulate matter prior to administration. If particulate matter is evident in reconstitued fluids, the drug solutions should be discarded.
When reconstituted or diluted according to the instructions below, cefazolin for injection is stable for 24 hours at room temperature or for 10 days if stored under refrigeration (5°C or 41°F). Reconstituted solutions may range in color from pale yellow to yellow without a change in potency.
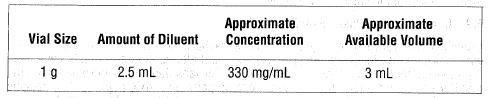
Single-Dose Vials
For IM injection, IV direct (bolus) injection or IV infustion reconstitute with Sterile Water for Injection according to the following table. SHAKE WELL.
2.6 Intramuscular Administration
Reconstitute vials with Sterile Water for Injection acording to the dilution table above. Shake well until dissolved. Cefazolin should be injected into a large muscle mass. Pain on injection is frequent with cefazolin.
2.7 Intravenous Administration
Direct (bolus) injection: Following reconstitution according to the above table, further dilute vials with approximately 5 mL Sterile Water for Injection. Inject the solution slowly over 3 to 5 minutes, directly or through tubing for patients receiving parenteral fluids (see list below).
Intermittent or continuous infusion: Dilute reconstituted cefazolin in 50 to 100 mL of one of the following solutions:
Sodium Chloride Injection, USP
5% or 10% Dextrose Injection, USP
5% Dextrose in Lactated Ringer's Injection, USP
5% Dextrose and 0.9% Sodium Chloride Injection, USP
5% Dextrose and 0.45% Sodium Chloride Injection, USP
5% Dextrose and 0.2% Sodium Chloride Injection, USP
Lactated Ringer's Injection, USP
Invert Sugar 5% or 10% in Sterile Water for Injection
Ringer's Injection, USP
5% Sodium Bicarbonate Injection, USP
Prior to administration parenteral drug products should be inspected visually for particulate matter and discoloration whenever solution and container permit.
CONTRAINDICATIONS
4.1 hypersensitivity to Cefazolin or the Cephalosporin Class of Antibacterial Drugs, Penicillins, or Other Beta-lactams
Cefazolin for injection is contraindicated in patients who have a history of immediate hypersensitivity reactions (e.g., anaphylaxis, serious skin reactions) to cefazolin or the cephalosporin class of antibacterial drugs, penicillins, or other beta-lactams [see Warnings and Precautions (5.1)].
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity Reactions to Cefazolin, Cephalosporins, Penicillins, or Other Beta-lactams
Serious and occasionally fatal hypersensitivity (anaphylactic) reactions have been reported in patients receiving beta-lactam antibacterial drugs. Before therapy with cefazolin for injection is instituted, careful inquiry should be made to determine whether the patient has had previous immediate hypersensitivity reactions to cefazolin, cephalosporins, penicillins, or carbapenems. Exercise caution if this product is to be given to penicillin-sensitive patients because cross-hypersensitivity amove beat-lactam antibacterial drugs has been clearly documented and may occur in up to 10% of patients with a history of penicillin allergy. If an allergic reaction to cefazolin for injection occurs, discontinue the drug.
5.2 Use in Patients with Renal Impairment
As with other beta-lactam antibacterial drugs, seizures may occur if inappropriately high doses are administered to patients with impaired renal function (creatinine clearance less than 55 mL/min.) [see Dosage and Administration 2.3)].
5.3 Clostridium difficile-associated Diarrhea
Clostridium difficile-associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including cefazolin, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile.
C. difficile produces toxins A and B, which contribute to the development of CDAD. Hypertoxin-producing isolates of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhead following antibacterial drug use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents.
If CDAD is suspected or confirmed, ongoing antibacterial drugs use not direct against C. difficile may need to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibacterial drug treatment of C. difficile, and surgical evaluation should be instituted as clincially indicated.
5.4 Drug/Laboratory Test Interactions
Urinary Glucose
The administration of cefazolin may result in a false-positive reaction with glucose in the urine when using CLINITEST® tablets. It is recommended that glucose tests based on enzymatic glucose oxidase reactions (e.g., CLINISTIX®) be used.
Coombs' Test
Positive direct Coombs' tests have been reported during treatment with cefazolin. In hematologic studies or in transfusion cross-matching procedures when antiglobulin tests are performed on the minor side or in Coombs' testing of newborns whos mothers have received cephalosporin antibacterial drugs before parturition, it should be recognized that a positive Coombs' test may be due to the drug.
ADVERSE REACTIONS
The following serious adverse reactions to cefazolin are described below and elsewhere in the labeling:
- Hypersensitivity reactions [see Warnings and Precautions (5.1)]
- Clostridium difficile-associated diarrhea [see Warnings and Precautions (5.3)]
6.1 Clinical Trials Experience
The following adverse reactions were reported from clinical trials:
Gastrointestinal: Diarrhea, oral candidiasis (oral thrush), mouth ulcers, vomiting, nausea, stomach cramps, epigastric pain, heartburn, flatus, anorexia and pseudomembranous colitis. Onset of pseudomembranous colitis symptoms may occur during or after antibacterial treatment [see Warnings and Precautions (5.3)].
Allergic: Anaphylaxis, eosinophilia, urticaria, itching, drug fever, skin rash, Stevens-Johnson syndrome.
Hematologic: Neuropenia, leukopenia, thrombocytopenia, thrombocythemia.
Hepatic: Transient rise in SGOT, SGPT, and alkaline phosphatase levels have been observed. As with other cephalosporins, reports of hepatitis have been received.
Local Reactions: Instances of phlebitis have been reported at site of injection. Some induration has occurred.
Other Reactions: Pruritus (including genital, vulvar andanal pruritus, genital moniliasis, and vaginitis). Dizziness, fainting, lightheadedness, confusion, weakness, tiredness, hypotension, somnolence and headache.
6.2 Cephalosporin-class Adverse Reactions
In addition to the adverse reactions listed above that have been observed in patients treated with cefazolin, the follwoing adverse reactions and altered laboratory tests have been reported for cephalosporin-class antibacterials: Stevens-Johnson syndrome, erythema multiforme, toxic epidermal necrolysis, renal impairment, toxic nephropathy, aplastic anemia, hemolytic anemia, hemorrhage, hepatic impairment including cholestasis, and pancytopenia.
DRUG INTERACTIONS
Probenecid may decrease renal tubular secretion of cephalosporins when used concurrently, resulting in increased and more prolonged cephalosporin blood levels.
USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Category B
Reproduction studies have been performed in rats, mice and rabbits at doses of 2000, 4000 and 240 kg/kg/day or 1 to 3 times the maximum recommended human dose on a body surface area basis. There was no evidence of impaired fertility or harm to the fetus due to cefazolin.
8.2 Labor and Delivery
When cefazolin has been administered prior to caesarean section, drug concentrations in cord blood habe been approximately one quarter to one third of maternal drug levels. The drug appears to have no adverse effect on the fetus.
8.3 Nursing Mothers
Cefazolin is present in very low concentrations in the milk of nursing mothers. Caution should be exercised when cefazolin for injection is administered to a nursing woman.
8.4 Pediatric Use
Safety and effectiveness for use in premature infants and neonates have not been established. See Dosage and Administration (2.4) for recommended dosage in pediatric patients older than 1 month.
8.5 Geriatric Use
Of the 920 subjects who received cefazolin in clinical studies, 313 (34%) were 65 years and over, while 138 (15%) were 75 years and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
The drug is known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function [see Dosage and Administration (2.3) and Warnings and Precautions (5.2)].
8.6 Patients with Renal Impairment
When cefazolin for injection is administered to patients with low urinary output because of impaired renal function (creatinine clearance less than 55 mL/min.), lower daily dosage is required [see Dosage and Administration (2.3) and Warnings and Precautions (5.2)].
DESCRIPTION
Cefazolin for Injection, USP is a semi-synthetic cephalosporin for parenteral administration. It is the sodium salt of (6R, 7R)-3[[(5-methyl-1,3,4-thiadiazol-2-yl)thio]methyl]-8-oxo-7-[2(1H-tetrazol-1-yl)acetamido]-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylic acid.
Structural Formula:
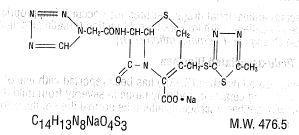
Cefazolin for Injection, USP is a sterile white to off-white crystalline powder.
Each vial contains 48 mg (2 mEq) of sodium/1 gram of cefazolin sodium.
CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Cefazolin is an antibacterial drug [see Microbiology (12.4)].
12.2 Pharmacodynamics
The pharmacokinetic/pharmacodynamic relationship for cefazolin has not been evaluated in patients.
12.3 Pharmocokinetics
After intramuscular administration of cefazolin to normal volunteers, the mean serum concentrations were 37 mcg/mL at 1 hour and 3 mcg/mL at 8 hours following a 1 gram dose.
Studies have shown that following intravenous adminstration of cefazolin to normal volunteers, mean serum concentrations peaked at approximately 185 mcg/mL and were approximately 4 mcg/mL at 8 hours of a 1 gram dose.
The serum half-life for cefazolin is approximately 1.8 hours following IV administration and approximately 2 hours following IM administration.
In a study (using normal volunteers) of constant intravenous infusion with dosages of 3.5 mg/kg for 1 hour (approximately 250 mg) and 1.5 mg/kg the next 2 hours (approximately 100 mg), cefazolin produced a steady serum concentration at the third hour of approximately 28 mcg/mL.
Studies in patients hospitalized with infections indicate that cefazolin for injection produces mean peak serum concentrations approximately equivalent to those seen in normal volunteers.
Bile concentrations in patients without obstructive biliary disease can reach or exceed serum concentrations by up to five times; however, in patietns with obstructive biliary disease, bile concentrations of cefazolin are considerably lower than serum concentrations (<1 mcg/mL).
In synovial fluid, the cefazolin concentration becomes comparable to that reached in serum at about 4 hours after drug administration.
Studies of cord blood show prompt transfer of cefazolin across the placenta. Cefazolin is present in very low concentrations in the milk of nursing mothers.
Cefazolin is excreted unchanged in the urine. In the first 6 hours approximately 60% of the drug is excreted in the urine and this increases to 70% to 80% within 24 hours. Cefazolin achieves peak urine concentrations of approximately 2,400 mcg/mL and 4,000 mcg/mL respectively following 500 mg and 1 gram intramuscular doses.
In patients undergoing peritoneal dialysis (2 L/hr.), cefazolin produced mean serum concentrations of approximately 10 and 30 mcg/mL after 24 hours instillation of a dialyzing solution containing 50 mg/L and 150 mg/L, respectively. Mean peak levels were 29 mcg/mL (range 13 to 44 mcg/mL) with 50 mg/L (3 patients), and 72 mcg/mL (range 26 to 142 mcg/mL) with 150 mg/L (6 patients). Intraperitoneal administration of cefazolin is usually well tolerated.
12.4 Microbiology
Mechanism of Action
Cefazolin is a bactericidal agent that acts by inhibition of bacterial cell wall synthesis.
Mechanism of Resistance
Predominant mechanisms of bacterial resistance to cephalosporins include the presence of extended-spectrum beta-lactamases and enzymatic hydrolysis.
Lists of Microorganisms
Cefazolin has been shown to be active against most isolates of the following microorganisms, both in vitroand in clinical infections as described in the Indications and Usage (1) section.
- Gram-Positive Bacteria
Staphylococcus aureus
Staphylococcus epidermidis
Streptococcus pyogenes, Streptococcus agalactiae
Streptococcus pneumoniae
Methicillin-resistant staphylococci are uniformly resistant to cefazolin.
- Gram-Negative Bacteria
Escherichia coli
Proteus mirabilis
Most isolates of indole positive Proteus (Proteus vulgaris), Enterobacter spp., Morganella morganii, Providencia rettgeri, Serratia spp., and Pseudomonas spp. are resistant to cefazolin.
Susceptibility Test Methods
When available, the clinical microbiology laboratory should provide the results of in vitro susceptibility test results for antimicrobial drug products used in resident hospitals to the physician as periodic reports that describe the susceptibility profile of nosocomial and community-acquired pathogens. These reports should aid the physician in selecting an antibacterial drug product for treatment.
Dilution Techniques
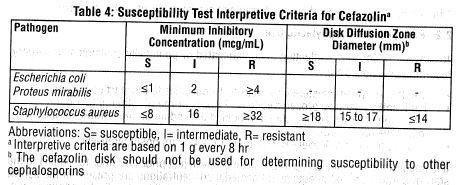
Quantitative methods are used to determine minimum inhibitory concentrations (MICs). These MICs provide estimates of the susceptibility of bacteria to antimicrobial compounds. The MICs should be determined using a standard test1,2 (broth and/or agar). The MIC values obtained should be interpreted according to criteria as provided in Table 4.
Diffusion Techniques
Quantitative methods that require measurement of zone diameters provide reproducible estimates of the susceptibility of bacteria to antimicrobial compounds. The zone size provides an estimate of the susceptibility of bacteria to antimicrobial compounds. The zone size should be interpreted using a standard test method 2,3. This procedure uses paper disks impregnated with 30 mcg cefazolin to test the susceptibility of microorganisms to cefazolin. The disk diffusion interpretive criteria are provided in Table 4.
NOTE:
S. pyogenes and S. agalactiae that have a penicillin MIC of ≤0.12 mcg/mL, or disk diffusion zone diameters of ≥24 mm with a 10 mcg penicillin disk, may be interpreted as susceptible to cefazolin. Non-meningitis isolates of S. pneumoniae that have a penicillin MIC of ≤0.06 mcg/mL, may be interpreted as susceptible to cefazolin.
A report of Susceptible indicates that the antimicrobial is likely to inhibit growth of the pathogen if the antimicrobial compund reaches the concentrations at the infection site necessare to inhibit growth of the pathogen. A report of Intermediate indicates that the result should be considered equivocal, and, if the microorganism is not fully susceptible to alternative, clinically feasible drugs, the test should be repeated. This category implies possible clinical applicability in body sites where the drug product is physiologically concentrated or in situations where a high dosage of the drug product can be used. This category also provides a buffer zone also prevents small uncontrolled technical factors from causing major descrepancies in interpretation. A report of Resistand indicates that the antimicrobial is not likely to inhibit growth of the pathogen if the antimicrobial compund reaches the concentrations usually achievable at the infection site; other therapy should be selected.
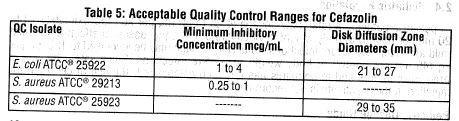
Quality Control
Standardized susceptibility test procedures require the use of laboratory controls to monitor and ensure the accuracy and precision of supplies and reagents used in the assay, and the techniques of the individual performing the test 1,2,3. Standard cefazolin powder should provide the following MIC values noted in Table 5. For the diffusion technique using the 30 mcg disk, the criteria in Table 5 should be achieved.
NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Mutagenicity studies and long-term studies in animals to determine the carcinogenic potential of cefazolin for injection have not been performed.
REFERENCES
- Clinical Laboratory Standards Institute (CLSI). Methods for Dilution Antimi crobial Susceptibility Tests for Bacteria the Grow Aerobically; Approved Standard-Ninth Edition. CLSI Document M07-A9. CLSI, 940 West Valley Road, Suite 2500, Wayne, PA, 2012.
- Clinical Laboratory Standards Institute (CLSI) Performance Standards for Antimicrobial Susceptibility Testing; Twentieth Informational Supplement. CLSI document M100-S20. CLSI, Wayne, PA, 2010.
- Clinical Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Disk Susceptibility Tests; Approved Standard-Eleventh Edition. CLSI Document M02-A11. CLSI, Wayne, PA, 2012.
HOW SUPPLIED/STORAGE AND HANDLING
Cefazolin for Injection, USP is supplied as a sterile, white to off-white crystalline powder. Each vial contains cefazolin sodium equivalent to 1 gram of cefazolin.

As with other cephalosporins, cefazolin tends to darken depending on storage conditions; within the stated recommendations, however, product potency is not adversely affected.
Before reconstitution protect from light and store at 20° to 25°C (68° to 77°F) [See USP Controlled Room Temperature].
PATIENT COUNSELING INFORMATION
Patient should be advised that allergic reactions, including serious allergic reactions could occur and that serious reactions require immediate treatment and discontinuation of cefazolin. Patients should resport to their health care provider any previous allergic reactions to cefazolin, cephalosporins, penicillins, or other similar antibacterials.
Patients should be advised that diarrhea is a common problem caused by antibiotics, which usually ends when the antibiotic is discontinued. Sometimes after starting treatment with anitbacterials, patients can develop watery and bloody stools (with or without stomach cramps and fever) even as late as two or more months after having taken the last dose of the antibacterials. If this occurs, patients should contact a physician as soon as possible.
Patients should be counseled that antibacterial drugs, including cefazolin for injection should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). When cefazolin for injection is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by cefazolin for injection or other antibacterial drugs in the future.
ATCC is a registered trademark of American Type Culture Collection.
Clinitest is a registered trademark of Siemens Medical Solutions Diagnostics.
Clinistix is a registered trademark of Bayer Healthcare LLC.
Manufactured for:
Hospira, Inc.
Lake Forest, IL 60045 USA
Made in India
EN-3547
948026315
| CEFAZOLIN
cefazolin sodium injection, powder, for solution |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - General Injectables & Vaccines, Inc (108250663) |