Label: CLADRIBINE- cladribine injection


- NDC Code(s): 63323-140-10
- Packager: Fresenius Kabi USA, LLC
- Category: HUMAN PRESCRIPTION DRUG LABEL
Drug Label Information
Updated December 31, 2019
If you are a healthcare professional or from the pharmaceutical industry please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
- SPL UNCLASSIFIED SECTION
-
BOXED WARNING
(What is this?)
WARNING:
Cladribine injection should be administered under the supervision of a qualified physician experienced in the use of antineoplastic therapy. Suppression of bone marrow function should be anticipated. This is usually reversible and appears to be dose dependent. Serious neurological toxicity (including irreversible paraparesis and quadraparesis) has been reported in patients who received cladribine injection by continuous infusion at high doses (four to nine times the recommended dose for Hairy Cell Leukemia). Neurologic toxicity appears to demonstrate a dose relationship; however, severe neurological toxicity has been reported rarely following treatment with standard cladribine dosing regimens.
Acute nephrotoxicity has been observed with high doses of cladribine injection (four to nine times the recommended dose for Hairy Cell Leukemia), especially when given concomitantly with other nephrotoxic agents/therapies.
-
DESCRIPTION:
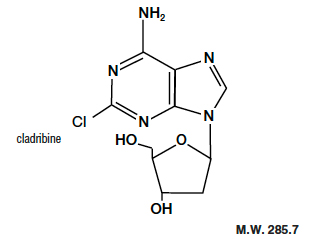
Cladribine Injection, USP (also commonly known as 2-chloro-2’-deoxy-ß-D-adenosine) is a synthetic antineoplastic agent for continuous intravenous infusion. It is a clear, colorless, sterile, preservative-free, isotonic solution. Cladribine injection, USP is available in single-dose vials containing 10 mg (1 mg/mL) of cladribine, a chlorinated purine nucleoside analog. Each milliliter of cladribine injection, USP contains 1 mg of the active ingredient and 9 mg (0.15 mEq) of sodium chloride as an inactive ingredient. The solution has a pH range of 5.5 to 8.0. Phosphoric acid and/or dibasic sodium phosphate may have been added to adjust the pH to 6.3 ± 0.3.
The chemical name for cladribine is 2-chloro-6-amino-9-(2-deoxy-ß-D-erythropento-furanosyl) purine and the structure is represented below:
-
CLINICAL PHARMACOLOGY:
Cellular Resistance and Sensitivity
The selective toxicity of 2-chloro-2’-deoxy-ß-D-adenosine towards certain normal and malignant lymphocyte and monocyte populations is based on the relative activities of deoxycytidine kinase and deoxynucleotidase. Cladribine passively crosses the cell membrane. In cells with a high ratio of deoxycytidine kinase to deoxynucleotidase, it is phosphorylated by deoxycytidine kinase to 2-chloro-2’-deoxy-ß-D-adenosine monophosphate (2-CdAMP). Since 2-chloro-2’-deoxy-ß-D-adenosine is resistant to deamination by adenosine deaminase and there is little deoxynucleotide deaminase in lymphocytes and monocytes, 2-CdAMP accumulates intracellularly and is subsequently converted into the active triphosphate deoxynucleotide,2-chloro-2’-deoxy-ß-D-adenosine triphosphate (2-CdATP). It is postulated that cells with high deoxycytidine kinase and low deoxynucleotidase activities will be selectively killed by 2-chloro-2’-deoxy-ß-D-adenosine as toxic deoxynucleotides accumulate intracellularly.
Cells containing high concentrations of deoxynucleotides are unable to properly repair single-strand DNA breaks. The broken ends of DNA activate the enzyme poly (ADP-ribose) polymerase resulting in NAD and ATP depletion and disruption of cellular metabolism. There is evidence, also, that 2-CdATP is incorporated into the DNA of dividing cells, resulting in impairment of DNA synthesis. Thus, 2-chloro-2’-deoxy-ß-D-adenosine can be distinguished from other chemotherapeutic agents affecting purine metabolism in that it is cytotoxic to both actively dividing and quiescent lymphocytes and monocytes, inhibiting both DNA synthesis and repair.
Pharmacokinetics
In a clinical investigation, 17 patients with Hairy Cell Leukemia (HCL) and normal renal function were treated for seven days with the recommended treatment regimen of cladribine injection (0.09 mg/kg/day) by continuous intravenous infusion. The mean steady-state serum concentration was estimated to be 5.7 ng/mL with an estimated systemic clearance of 663.5 mL/h/kg when cladribine injection was given by continuous infusion over seven days. In Hairy Cell Leukemia patients, there does not appear to be a relationship between serum concentrations and ultimate clinical outcome.
In another study, eight patients with hematologic malignancies received a two (2) hour infusion of cladribine injection (0.12 mg/kg). The mean end-of-infusion plasma cladribine injection concentration was 48 ± 19 ng/mL. For five of these patients, the disappearance of cladribine injection could be described by either a biphasic or triphasic decline. For these patients with normal renal function, the mean terminal half-life was 5.4 hours. Mean values for clearance and steady-state volume of distribution were 978 ± 422 mL/h/kg and 4.5 ± 2.8 L/kg, respectively.
Cladribine plasma concentration after intravenous administration declines multi-exponentially with an average half-life of 6.7 +/- 2.5 hours. In general, the apparent volume of distribution of cladribine is approximately 9 L/kg, indicating an extensive distribution in body tissues.
Cladribine penetrates into cerebrospinal fluid. One report indicates that concentrations are approximately 25% of those in plasma.
Cladribine injection is bound approximately 20% to plasma proteins.
Except for some understanding of the mechanism of cellular toxicity, no other information is available on the metabolism of cladribine injection in humans. An average of 18% of the administered dose has been reported to be excreted in urine of patients with solid tumors during a five-day continuous intravenous infusion of 3.5 to 8.1 mg/m 2/day of cladribine injection. The effect of renal and hepatic impairment on the elimination of cladribine has not been investigated in humans.
-
CLINICAL STUDIES:
Two single-center open label studies of cladribine injection have been conducted in patients with Hairy Cell Leukemia with evidence of active disease requiring therapy. In the study conducted at the Scripps Clinic and Research Foundation (Study A), 89 patients were treated with a single course of cladribine injection given by continuous intravenous infusion for seven days at a dose of 0.09 mg/kg/day. In the study conducted at the M.D. Anderson Cancer Center (Study B), 35 patients were treated with a seven-day continuous intravenous infusion of cladribine injection at a comparable dose of 3.6 mg/m 2/day. A complete response (CR) required clearing of the peripheral blood and bone marrow of hairy cells and recovery of the hemoglobin to 12 g/dL, platelet count to 100 x 10 9/L, and absolute neutrophil count to 1,500 x 10 6/L. A good partial response (GPR) required the same hematologic parameters as a complete response, and that fewer than 5% hairy cells remain in the bone marrow. A partial response (PR) required that hairy cells in the bone marrow be decreased by at least 50% from baseline and the same response for hematologic parameters as for complete response. A pathologic relapse was defined as an increase in bone marrow hairy cells to 25% of pretreatment levels. A clinical relapse was defined as the recurrence of cytopenias, specifically, decreases in hemoglobin ≥ 2 g/dL, ANC ≥ 25% or platelet counts ≥ 50,000. Patients who met the criteria for a complete response but subsequently were found to have evidence of bone marrow hairy cells (< 25% of pretreatment levels) were reclassified as partial responses and were not considered to be complete responses with relapse.
Among patients evaluable for efficacy (N=106), using the hematologic and bone marrow response criteria described above, the complete response rates in patients treated with cladribine injection were 65% and 68% for Study A and Study B, respectively, yielding a combined complete response rate of 66%. Overall response rates (i.e., Complete plus Good Partial plus Partial Responses) were 89% and 86% in Study A and Study B, respectively, for a combined overall response rate of 88% in evaluable patients treated with cladribine injection.
Using an intent-to-treat analysis (N=123) and further requiring no evidence of splenomegaly as a criterion for CR (i.e., no palpable spleen on physical examination and ≤ 13 cm on CT scan), the complete response rates for Study A and Study B were 54% and 53%, respectively, giving a combined CR rate of 54%. The overall response rates (CR + GPR + PR) were 90% and 85%, for Studies A and B, respectively, yielding a combined overall response rate of 89%.
RESPONSE RATES TO CLADRIBINE INJECTION TREATMENT IN PATIENTS WITH HAIRY CELL LEUKEMIA
CR
Overall
Evaluable Patients
N=106
66%
88%
Intent-to-treat Population
N=123
54%
89%
In these studies, 60% of the patients had not received prior chemotherapy for Hairy Cell Leukemia or had undergone splenectomy as the only prior treatment and were receiving cladribine injection as a first-line treatment. The remaining 40% of the patients received cladribine injection as a second-line treatment, having been treated previously with other agents, including α-interferon and/or deoxycoformycin. The overall response rate for patients without prior chemotherapy was 92%, compared with 84% for previously treated patients. Cladribine injection is active in previously treated patients; however, retrospective analysis suggests that the overall response rate is decreased in patients previously treated with splenectomy or deoxycoformycin and in patients refractory to α-interferon.
OVERALL RESPONSE RATES (CR + GPR + PR) TO CLADRIBINE INJECTION TREATMENT IN PATIENTS WITH HAIRY CELL LEUKEMIA
OVERALL
RESPONSE
(N=123)
NR + RELAPSE
No Prior Chemotherapy
68/74
92%
6 + 4
14%
Any Prior Chemotherapy
41/49
84%
8 +3
22%
Previous Splenectomy
32/41*
78%
9 + 1
24%
Previous Interferon
40/48
83%
8 + 3
23%
Interferon Refractory
6/11*
55%
5 + 2
64%
Previous Deoxycoformycin
3/6*
50%
3 + 1
66%
NR = No Response
* P < 0.05
After a reversible decline, normalization of peripheral blood counts (Hemoglobin >12 g/dL, Platelets >100 x 10 9/L, Absolute Neutrophil Count (ANC) >1,500 x 10 6/L) was achieved by 92% of evaluable patients. The median time to normalization of peripheral counts was nine weeks from the start of treatment (Range: 2 to 72). The median time to normalization of Platelet Count was two weeks, the median time to normalization of ANC was five weeks and the median time to normalization of Hemoglobin was eight weeks. With normalization of Platelet Count and Hemoglobin, requirements for platelet and RBC transfusions were abolished after Months 1 and 2, respectively, in those patients with complete response. Platelet recovery may be delayed in a minority of patients with severe baseline thrombocytopenia. Corresponding to normalization of ANC, a trend toward a reduced incidence of infection was seen after the third month, when compared to the months immediately preceding cladribine injection therapy (see also WARNINGS, PRECAUTIONS and ADVERSE REACTIONS).
CLADRIBINE INJECTION TREATMENT IN PATIENTS WITH HAIRY CELL LEUKEMIA TIME TO NORMALIZATION OF PERIPHERAL BLOOD COUNTS
Parameter
Median Time to
Normalization
of Count*
Platelet Count
2 weeks
Absolute Neutrophil Count
5 weeks
Hemoglobin
8 weeks
ANC, Hemoglobin and
Platelet Count
9 weeks
*Day 1 = First day of infusion
For patients achieving a complete response, the median time to response (i.e., absence of hairy cells in bone marrow and peripheral blood together with normalization of peripheral blood parameters), measured from treatment start, was approximately four months. Since bone marrow aspiration and biopsy were frequently not performed at the time of peripheral blood normalization, the median time to complete response may actually be shorter than that which was recorded. At the time of data cut-off, the median duration of complete response was greater than eight months and ranged to 25+ months. Among 93 responding patients, seven had shown evidence of disease progression at the time of the data cut-off. In four of these patients, disease was limited to the bone marrow without peripheral blood abnormalities (pathologic progression), while in three patients there were also peripheral blood abnormalities (clinical progression). Seven patients who did not respond to a first course of cladribine injection received a second course of therapy. In the five patients who had adequate follow-up, additional courses did not appear to improve their overall response.
- INDICATIONS AND USAGE:
- CONTRAINDICATIONS:
-
WARNINGS:
Due to increased risk of infection in the setting of immunosuppression with chemotherapy including cladribine, it is recommended not to administer live attenuated vaccines to patients receiving cladribine injection.
Severe bone marrow suppression, including neutropenia, anemia and thrombocytopenia, has been commonly observed in patients treated with cladribine injection, especially at high doses. At initiation of treatment, most patients in the clinical studies had hematologic impairment as a manifestation of active Hairy Cell Leukemia. Following treatment with cladribine injection, further hematologic impairment occurred before recovery of peripheral blood counts began. During the first two weeks after treatment initiation, mean Platelet Count, ANC, and Hemoglobin concentration declined and subsequently increased with normalization of mean counts by Day 12, Week 5 and Week 8, respectively. The myelosuppressive effects of cladribine injection were most notable during the first month following treatment. Forty-four percent (44%) of patients received transfusions with RBCs and 14% received transfusions with platelets during Month 1. Careful hematologic monitoring, especially during the first four to eight weeks after treatment with cladribine injection, is recommended (see PRECAUTIONS).
Fever (T ≥ 100°F) was associated with the use of cladribine injection in approximately two-thirds of patients (131/196) in the first month of therapy. Virtually all of these patients were treated empirically with parenteral antibiotics. Overall, 47% (93/196) of all patients had fever in the setting of neutropenia (ANC ≤ 1,000), including 62 patients (32%) with severe neutropenia (i.e., ANC ≤ 500).
In a Phase I investigational study using cladribine injection in high doses (four to nine times the recommended dose for Hairy Cell Leukemia) as part of a bone marrow transplant conditioning regimen, which also included high dose cyclophosphamide and total body irradiation, acute nephrotoxicity and delayed onset neurotoxicity were observed. Thirty-one (31) poor-risk patients with drug-resistant acute leukemia in relapse (29 cases) or non-Hodgkins Lymphoma (two cases) received cladribine for 7 to 14 days prior to bone marrow transplantation. During infusion, eight patients experienced gastrointestinal symptoms. While the bone marrow was initially cleared of all hematopoietic elements, including tumor cells, leukemia eventually recurred in all treated patients. Within 7 to 13 days after starting treatment with cladribine, six patients (19%) developed manifestations of renal dysfunction (e.g., acidosis, anuria, elevated serum creatinine, etc.) and five required dialysis. Several of these patients were also being treated with other medications having known nephrotoxic potential. Renal dysfunction was reversible in two of these patients. In the four patients whose renal function had not recovered at the time of death, autopsies were performed; in two of these, evidence of tubular damage was noted. Eleven (11) patients (35%) experienced delayed onset neurologic toxicity. In the majority, this was characterized by progressive irreversible motor weakness (paraparesis/quadriparesis), of the upper and/or lower extremities, first noted 35 to 84 days after starting high dose therapy with cladribine. Non-invasive testing (electromyography and nerve conduction studies) was consistent with demyelinating disease. Severe neurologic toxicity has also been noted with high doses of another drug in this class.
Axonal peripheral polyneuropathy was observed in a dose escalation study at the highest dose levels (approximately four times the recommended dose for Hairy Cell Leukemia) in patients not receiving cyclophosphamide or total body irradiation. Severe neurological toxicity has been reported rarely following treatment with standard cladribine dosing regimens.
In patients with Hairy Cell Leukemia treated with the recommended treatment regimen (0.09 mg/kg/day for seven consecutive days), there have been no reports of nephrologic toxicities.
Serious (e.g. respiratory infection, pneumonia and viral skin infections), including fatal infections (e.g., sepsis) were reported (see ADVERSE REACTIONS).
Of the 196 Hairy Cell Leukemia patients entered in the two trials, there were eight deaths following treatment. Of these, six were of infectious etiology, including three pneumonias, and two occurred in the first month following cladribine therapy. Of the eight deaths, six occurred in previously treated patients who were refractory to α-interferon.
Benzyl alcohol is a constituent of the recommended diluent for the seven-day infusion solution. Benzyl alcohol has been reported to be associated with a fatal “Gasping Syndrome” in premature infants (see DOSAGE AND ADMINISTRATION).
Pregnancy Category D
Cladribine can cause fetal harm when administered to a pregnant woman. Although there is no evidence of teratogenicity in humans due to cladribine, other drugs which inhibit DNA synthesis have been reported to be teratogenic in humans. Cladribine is teratogenic in animals. Advise females of reproductive potential to use highly effective contraception during treatment with cladribine. If cladribine is used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to the fetus.
Cladribine is teratogenic in mice and rabbits and consequently has the potential to cause fetal harm when administered to a pregnant woman. A significant increase in fetal variations was observed in mice receiving 1.5 mg/kg/day (4.5 mg/m 2) and increased resorptions, reduced litter size and increased fetal malformations were observed when mice received 3 mg/kg/day (9 mg/m 2). Fetal death and malformations were observed in rabbits that received 3 mg/kg/day (33 mg/m 2). No fetal effects were seen in mice at 0.5 mg/kg/day (1.5 mg/m 2) or in rabbits at 1 mg/kg/day (11 mg/m 2).
-
PRECAUTIONS:
General
Cladribine injection is a potent antineoplastic agent with potentially significant toxic side effects. It should be administered only under the supervision of a physician experienced with the use of cancer chemotherapeutic agents. Patients undergoing therapy should be closely observed for signs of hematologic and non-hematologic toxicity. Periodic assessment of peripheral blood counts, particularly during the first four to eight weeks posttreatment, is recommended to detect the development of anemia, neutropenia and thrombocytopenia and for early detection of any potential sequelae (e.g., infection or bleeding). As with other potent chemotherapeutic agents, monitoring of renal and hepatic function is also recommended, especially in patients with underlying kidney or liver dysfunction (see WARNINGS and ADVERSE REACTIONS).
Fever was a frequently observed side effect during the first month on study. Since the majority of fevers occurred in neutropenic patients, patients should be closely monitored during the first month of treatment and empiric antibiotics should be initiated as clinically indicated. Although 69% of patients developed fevers, less than 1/3 of febrile events were associated with documented infection. Given the known myelosuppressive effects of cladribine, practitioners should carefully evaluate the risks and benefits of administering this drug to patients with active infections (see WARNINGS and ADVERSE REACTIONS).
There are inadequate data on dosing of patients with renal or hepatic insufficiency. Development of acute renal insufficiency in some patients receiving high doses of cladribine has been described. Until more information is available, caution is advised when administering the drug to patients with known or suspected renal or hepatic insufficiency (see WARNINGS).
Rare cases of tumor lysis syndrome have been reported in patients treated with cladribine with other hematologic malignancies having a high tumor burden.
Cladribine injection must be diluted in designated intravenous solutions prior to administration (see DOSAGE AND ADMINISTRATION).
Laboratory Tests
During and following treatment, the patient’s hematologic profile should be monitored regularly to determine the degree of hematopoietic suppression. In the clinical studies, following reversible declines in all cell counts, the mean Platelet Count reached 100 x 10 9/L by Day 12, the mean Absolute Neutrophil Count reached 1,500 x 10 6/L by Week 5 and the mean Hemoglobin reached 12 g/dL by Week 8. After peripheral counts have normalized, bone marrow aspiration and biopsy should be performed to confirm response to treatment with cladribine. Febrile events should be investigated with appropriate laboratory and radiologic studies. Periodic assessment of renal function and hepatic function should be performed as clinically indicated.
Drug Interactions
There are no known drug interactions with cladribine injection. Caution should be exercised if cladribine injection is administered before, after, or in conjunction with other drugs known to cause immunosuppression or myelosuppression (see WARNINGS).
Carcinogenesis
No animal carcinogenicity studies have been conducted with cladribine. However, its carcinogenic potential cannot be excluded based on demonstrated genotoxicity of cladribine.
Mutagenesis
As expected for compounds in this class, the actions of cladribine yield DNA damage. In mammalian cells in culture, cladribine caused the accumulation of DNA strand breaks. Cladribine was also incorporated into DNA of human lymphoblastic leukemia cells. Cladribine was not mutagenic in vitro (Ames and Chinese hamster ovary cell gene mutation tests) and did not induce unscheduled DNA synthesis in primary rat hepatocyte cultures. However, cladribine was clastogenic both in vitro (chromosome aberrations in Chinese hamster ovary cells) and in vivo (mouse bone marrow micronucleus test).
Impairment of Fertility
The effect on human fertility is unknown. When administered intravenously to Cynomolgus monkeys, cladribine has been shown to cause suppression of rapidly generating cells, including testicular cells.
Nursing Mothers
It is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from cladribine, a decision should be made whether to discontinue nursing or discontinue the drug, taking into account the importance of the drug for the mother.
Pediatric Use
Safety and effectiveness in pediatric patients have not been established. In a Phase I study involving patients 1 to 21 years old with relapsed acute leukemia, cladribine injection was given by continuous intravenous infusion in doses ranging from 3 to 10.7 mg/m 2/day for five days (one-half to twice the dose recommended in Hairy Cell Leukemia). In this study, the dose-limiting toxicity was severe myelosuppression with profound neutropenia and thrombocytopenia. At the highest dose (10.7 mg/m 2/day), three of seven patients developed irreversible myelosuppression and fatal systemic bacterial or fungal infections. No unique toxicities were noted in this study (1) (see WARNINGS and ADVERSE REACTIONS).
Geriatric Use
Clinical studies of cladribine did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy in elderly patients.
-
ADVERSE REACTIONS:
Clinical Trials Experience
Adverse drug reactions reported by ≥ 1% of cladribine-treated patients with HCL noted in the HCL clinical dataset (studies K90-091 and L91-048, n=576) are shown in the table below.
Adverse Drug Reactions in ≥ 1% of Patients Treated with Cladribine in HCL Clinical Trials
System Organ Class
Preferred Term
Cladribine (n=576) %
Blood and Lymphatic System Disorder (see also sections WARNINGS and PRECAUTIONS)
Anemia
1
Febrile neutropenia
8
Psychiatric Disorders
Anxiety
1
Insomnia
3
Nervous System Disorders
Dizziness
6
Headache
14
Cardiac Disorders
Tachycardia
2
Respiratory, Thoracic and Mediastinal Disorders
Breath sounds abnormal
4
Cough
7
Dyspnea*
5
Rales
1
Gastrointestinal Disorders
Abdominal pain**
4
Constipation
4
Diarrhea
7
Flatulence
1
Nausea
22
Vomiting
9
Skin and Subcutaneous Tissue Disorders
Ecchymosis
2
Hyperhidrosis
3
Petechiae
2
Pruritus
2
Rash***
16
Musculoskeletal, Connective Tissue, and Bone Disorders
Arthralgia
3
Myalgia
6
Pain****
6
General Disorders and Administration Site Conditions (see also sections WARNINGS and PRECAUTIONS)
Administration site reaction*****
11
Asthenia
6
Chills
2
Decreased appetite
8
Fatigue
31
Malaise
5
Muscular weakness
1
Edema peripheral
2
Pyrexia
33
Injury, Poisoning and Procedural Complications
Contusion
1
* Dyspnea includes dyspnea, dyspnea exertional, and wheezing
** Abdominal pain includes abdominal discomfort, abdominal pain, and abdominal pain (lower and upper)
*** Rash includes erythema, rash, and rash (macular, macula-papular, papular, pruritic, pustular and erythematous)
**** Pain includes pain, back pain, chest pain, arthritis pain, bone pain, and pain in extremity
*****Administration site reaction includes administration site reaction, catheter site (cellulitis, erythema, hemorrhage, and pain), and infusion site reaction (erythema, edema, and pain)
The following safety data are based on 196 patients with Hairy Cell Leukemia: the original cohort of 124 patients plus an additional 72 patients enrolled at the same two centers after the original enrollment cutoff. In Month 1 of the Hairy Cell Leukemia clinical trials, severe neutropenia was noted in 70% of patients, fever in 69%, and infection was documented in 28%. Most non-hematologic adverse experiences were mild to moderate in severity.
Myelosuppression was frequently observed during the first month after starting treatment. Neutropenia (ANC < 500 x 10 6/L) was noted in 70% of patients, compared with 26% in whom it was present initially. Severe anemia (Hemoglobin < 8.5 g/dL) developed in 37% of patients, compared with 10% initially and thrombocytopenia (Platelets < 20 x 10 9/L) developed in 12% of patients, compared to 4% in whom it was noted initially.
During the first month, 54 of 196 patients (28%) exhibited documented evidence of infection. Serious infections (e.g., septicemia, pneumonia) were reported in 6% of all patients; the remainder were mild or moderate. Several deaths were attributable to infection and/or complications related to the underlying disease. During the second month, the overall rate of documented infection was 6%; these infections were mild to moderate and no severe systemic infections were seen. After the third month, the monthly incidence of infection was either less than or equal to that of the months immediately preceding cladribine therapy.
During the first month, 11% of patients experienced severe fever (i.e., ≥ 104°F). Documented infections were noted in fewer than one-third of febrile episodes. Of the 196 patients studied, 19 were noted to have a documented infection in the month prior to treatment. In the month following treatment, there were 54 episodes of documented infection: 23 (42%) were bacterial, 11 (20%) were viral and 11 (20%) were fungal. Seven (7) of 8 documented episodes of herpes zoster occurred during the month following treatment. Fourteen (14) of 16 episodes of documented fungal infections occurred in the first two months following treatment. Virtually all of these patients were treated empirically with antibiotics (see WARNINGS and PRECAUTIONS).
Analysis of lymphocyte subsets indicates that treatment with cladribine is associated with prolonged depression of the CD4 counts. Prior to treatment, the mean CD4 count was 766/ μL. The mean CD4 count nadir, which occurred four to six months following treatment, was 272/ μL. Fifteen (15) months after treatment, mean CD4 counts remained below 500/ μL. CD8 counts behaved similarly, though increasing counts were observed after nine months. The clinical significance of the prolonged CD4 lymphopenia is unclear.
Another event of unknown clinical significance includes the observation of prolonged bone marrow hypocellularity. Bone marrow cellularity of < 35% was noted after four months in 42 of 124 patients (34%) treated in the two pivotal trials. This hypocellularity was noted as late as Day 1,010. It is not known whether the hypocellularity is the result of disease related marrow fibrosis or if it is the result of cladribine toxicity. There was no apparent clinical effect on the peripheral blood counts.
The vast majority of rashes were mild. Most episodes of nausea were mild, not accompanied by vomiting, and did not require treatment with antiemetics. In patients requiring antiemetics, nausea was easily controlled, most frequently with chlorpromazine.
When used in other clinical settings the following ADRs were reported: bacteremia, cellulitis, localized infection, pneumonia, anemia, thrombocytopenia (with bleeding or petechiae), phlebitis, purpura, crepitations, localized edema and edema.
For a description of adverse reactions associated with use of high doses in non-Hairy Cell Leukemia patients, see WARNINGS.
Postmarketing Experience
The following additional adverse reactions have been reported since the drug became commercially available. These adverse reactions have been reported primarily in patients who received multiple courses of cladribine injection:
Infections and infestations: Septic shock. Opportunistic infections have occurred in the acute phase of treatment.
Blood and lymphatic system disorders: Bone marrow suppression with prolonged pancytopenia, including some reports of aplastic anemia; hemolytic anemia (including autoimmune hemolytic anemia), which was reported in patients with lymphoid malignancies, occurring within the first few weeks following treatment. Rare cases of myelodysplastic syndrome have been reported.
Immune system disorders: Hypersensitivity.
Metabolism and nutrition disorders: Tumor lysis syndrome.
Psychiatric disorders: Confusion (including disorientation).
Hepatobiliary disorders: Reversible, generally mild increases in bilirubin (uncommon) and transaminases.
Nervous System disorders: Depressed level of consciousness, neurological toxicity (including peripheral sensory neuropathy, motor neuropathy (paralysis), polyneuropathy, paraparesis); however, severe neurotoxicity has been reported rarely following treatment with standard cladribine dosing regimens.
Eye disorders: Conjunctivitis.
Respiratory, thoracic and mediastinal disorders: Pulmonary interstitial infiltrates (including lung infiltration, interstitial lung disease, pneumonitis and pulmonary fibrosis); in most cases, an infectious etiology was identified.
Skin and tissue disorders: Urticaria, hypereosinophilia; Stevens-Johnson. In isolated cases toxic epidermal necrolysis has been reported in patients who were receiving or had recently been treated with other medications (e.g., allopurinol or antibiotics) known to cause these syndromes.
Renal and urinary disorders: Renal failure (including renal failure acute, renal impairment).
-
OVERDOSAGE:
High doses of cladribine have been associated with: irreversible neurologic toxicity (paraparesis/quadriparesis), acute nephrotoxicity, and severe bone marrow suppression resulting in neutropenia, anemia and thrombocytopenia (see WARNINGS). There is no known specific antidote to overdosage. Treatment of overdosage consists of discontinuation of cladribine, careful observation, and appropriate supportive measures. It is not known whether the drug can be removed from the circulation by dialysis or hemofiltration.
-
DOSAGE AND ADMINISTRATION:
Usual Dosage
The recommended dose and schedule of cladribine injection for active Hairy Cell Leukemia is as a single course given by continuous infusion for seven consecutive days at a dose of 0.09 mg/kg/day. Deviations from this dosage regimen are not advised. If the patient does not respond to the initial course of cladribine injection for Hairy Cell Leukemia, it is unlikely that they will benefit from additional courses. Physicians should consider delaying or discontinuing the drug if neurotoxicity or renal toxicity occurs (see WARNINGS).
Specific risk factors predisposing to increased toxicity from cladribine injection have not been defined. In view of the known toxicities of agents of this class, it would be prudent to proceed carefully in patients with known or suspected renal insufficiency or severe bone marrow impairment of any etiology. Patients should be monitored closely for hematologic and non-hematologic toxicity (see WARNINGS and PRECAUTIONS).
Preparation and Administration of Intravenous Solutions
Cladribine injection must be diluted with the designated diluent prior to administration. Since the drug product does not contain any antimicrobial preservative or bacteriostatic agent, aseptic technique and proper environmental precautions must be observed in preparation of cladribine injection solutions.
To prepare a single daily dose
Cladribine injection should be passed through a sterile 0.22 μm disposable hydrophilic syringe filter prior to introduction into the infusion bag, prior to each daily infusion. Add the calculated dose (0.09 mg/kg or 0.09 mL/kg) of cladribine injection through the sterile filter to an infusion bag containing 500 mL of 0.9% Sodium Chloride Injection, USP. Infuse continuously over 24 hours. Repeat daily for a total of seven consecutive days. The use of 5% dextrose as a diluent is not recommended because of increased degradation of cladribine. Admixtures of cladribine injection are chemically and physically stable for at least 24 hours at room temperature under normal room fluorescent light in Baxter Viaflex ® PVC infusion containers. Since limited compatibility data are available, adherence to the recommended diluents and infusion systems is advised.
Dose of
Cladribine Injection
Recommended
Diluent
Quantity of
Diluent
24-hour
infusion
method
1 (day) x 0.09 mg/kg
0.9% Sodium
Chloride
Injection, USP
500 mL
To prepare a 7-day infusion
The seven-day infusion solution should only be prepared with Bacteriostatic 0.9% Sodium Chloride Injection, USP (0.9% benzyl alcohol preserved). In order to minimize the risk of microbial contamination, both cladribine injection and the diluent should be passed through a sterile 0.22 μm disposable hydrophilic syringe filter as each solution is being introduced into the infusion reservoir. First add the calculated dose of cladribine injection (7 days x 0.09 mg/kg or mL/kg) to the infusion reservoir through the sterile filter.
Then add a calculated amount of Bacteriostatic 0.9% Sodium Chloride Injection, USP (0.9% benzyl alcohol preserved) also through the filter to bring the total volume of the solution to 100 mL. After completing solution preparation, clamp off the line, disconnect and discard the filter. Aseptically aspirate air bubbles from the reservoir as necessary using the syringe and a dry second sterile filter or a sterile vent filter assembly. Reclamp the line and discard the syringe and filter assembly. Infuse continuously over seven days. Solutions prepared with Bacteriostatic Sodium Chloride Injection for individuals weighing more than 85 kg may have reduced preservative effectiveness due to greater dilution of the benzyl alcohol preservative. Admixtures for the seven-day infusion have demonstrated acceptable chemical and physical stability for at least seven days in the SIMS Deltec MEDICATION CASSETTE™ Reservoir.
Dose of Cladribine Injection
Recommended Diluent
Quantity of Diluent
7-day infusion method (use sterile 0.22 μm filter when preparing infusion solution
7 (days) x 0.09 mg/kg
Bacteriostatic 0.9% Sodium Chloride Injection, USP (0.9% benzyl alcohol)
q.s. to 100 mL
Since limited compatibility data are available, adherence to the recommended diluents and infusion systems is advised. Solutions containing cladribine injection should not be mixed with other intravenous drugs or additives or infused simultaneously via a common intravenous line, since compatibility testing has not been performed. Preparations containing benzyl alcohol should not be used in neonates (see WARNINGS).
Care must be taken to assure the sterility of prepared solutions. Once diluted, solutions of cladribine injection should be administered promptly or stored in the refrigerator (2° to 8°C) for no more than eight hours prior to start of administration. Vials of cladribine injection are for single-use only. Any unused portion should be discarded in an appropriate manner (see Handling and Disposal).
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. A precipitate may occur during the exposure of cladribine injection to low temperatures; it may be resolubilized by allowing the solution to warm naturally to room temperature and by shaking vigorously. DO NOT HEAT OR MICROWAVE.
Chemical Stability of Vials
When stored in refrigerated conditions between 2° to 8°C (36° to 46°F) and protected from light, unopened vials of cladribine injection are stable until the expiration date indicated on the package. Freezing does not adversely affect the solution. If freezing occurs, thaw naturally to room temperature. DO NOT heat or microwave. Once thawed, the vial of cladribine injection is stable until expiry if refrigerated. DO NOT refreeze. Once diluted, solutions containing cladribine injection should be administered promptly or stored in the refrigerator (2° to 8°C) for no more than 8 hours prior to administration.
Handling and Disposal
The potential hazards associated with cytotoxic agents are well established and proper precautions should be taken when handling, preparing, and administering cladribine injection. The use of disposable gloves and protective garments is recommended. If cladribine injection contacts the skin or mucous membranes, wash the involved surface immediately with copious amounts of water. Several guidelines on this subject have been published. (2-8) There is no general agreement that all of the procedures recommended in the guidelines are necessary or appropriate. Refer to your Institution’s guidelines and all applicable state/local regulations for disposal of cytotoxic waste.
-
HOW SUPPLIED:
Product
No.
NDC
No.
104010
63323-140-10
Cladribine Injection, USP is available as 10 mg per 10 mL (1 mg per mL), single-dose vial, packaged individually.
Store refrigerated 2° to 8°C (36° to 46°F). Protect from light (keep in outer carton until time of use).
The container closure is not made with natural rubber latex.
-
REFERENCES:
- Santana VM, Mirro J, Harwood FC, et al: A phase I clinical trial of 2-Chloro-deoxyadenosine in pediatric patients with acute leukemia. J. Clin. Onc., 9: 416(1991).
- Recommendations for the Safe Handling of Parenteral Antineoplastic Drugs. NIH Publication No. 83-2621. For sale by the Superintendent of Documents, U.S. Government Printing Office, Washington D.C. 20402.
- AMA Council Report. Guidelines for Handling Parenteral Antineoplastics, JAMA, March 15 (1985).
- National Study Commission on Cytotoxic Exposure-Recommendations for Handling Cytotoxic Agents. Available from Louis P. Jeffrey, Sc.D., Chairman, National Study Commission on Cytotoxic Exposure, Massachusetts College of Pharmacy and Allied Health Sciences, 179 Longwood Avenue, Boston, Massachusetts 02115.
- Clinical Oncological Society of Australia: Guidelines and Recommendations for Safe Handling of Antineoplastic Agents, Med. J. Australia 1:425 (1983).
- Jones RB, et al. Safe Handling of Chemotherapeutic Agents: A Report from the Mount Sinai Medical Center. Ca—A Cancer Journal for Clinicians, Sept/Oct. 258-263 (1983).
- American Society of Hospital Pharmacists Technical Assistance Bulletin on Handling Cytotoxic Drugs in Hospitals. Am. J. Hosp. Pharm., 42:131 (1985).
- OSHA Work-Practice Guidelines for Personnel Dealing with Cytotoxic (antineoplastic) Drugs. Am. J. Hosp. Pharm., 43:1193 (1986).
The brand names mentioned in this document are the trademarks of their respective owners.
- SPL UNCLASSIFIED SECTION
-
PRINCIPAL DISPLAY PANEL
PACKAGE LABEL - PRINCIPAL DISPLAY - Cladribine 10 mL Single Dose Vial Label
Cladribine Injection, USP
10 mg per 10 mL (1 mg per mL )
For intravenous infusion.
10 mL Single Dose Vial
Rx only
PACKAGE LABEL - PRINCIPAL DISPLAY - Cladribine 10 mL Single Dose Vial Carton Panel
Cladribine Injection, USP
10 mg per 10 mL (1 mg per mL )
For intravenous infusion.
-
INGREDIENTS AND APPEARANCE
CLADRIBINE
cladribine injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:63323-140 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength CLADRIBINE (UNII: 47M74X9YT5) (CLADRIBINE - UNII:47M74X9YT5) CLADRIBINE 1 mg in 1 mL Inactive Ingredients Ingredient Name Strength SODIUM CHLORIDE (UNII: 451W47IQ8X) 9 mg in 1 mL PHOSPHORIC ACID (UNII: E4GA8884NN) SODIUM PHOSPHATE, DIBASIC (UNII: GR686LBA74) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:63323-140-10 1 in 1 CARTON 12/01/2004 1 10 mL in 1 VIAL, SINGLE-DOSE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA076571 12/01/2004 Labeler - Fresenius Kabi USA, LLC (608775388) Establishment Name Address ID/FEI Business Operations Fresenius Kabi USA, LLC 023648251 manufacture(63323-140)
