ALBENDAZOLE- albendazole tablet, film coated
Lineage Therapeutics Inc
----------
Albendazole Tablets
Rx only
DESCRIPTION
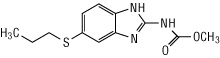
Albendazole is an orally administered broad-spectrum anthelmintic. Chemically, it is methyl 5-(propylthio)-2-benzimidazolecarbamate. Its molecular formula is C12H15N3O2S. Its molecular weight is 265.34. It has the following chemical structure:
Albendazole is a white to off-white powder. It is soluble in dimethylsulfoxide, strong acids, and strong bases. It is slightly soluble in methanol, chloroform, ethyl acetate, and acetonitrile. Albendazole is practically insoluble in water. Each white to off-white, film-coated tablet contains 200 mg of albendazole.
Inactive ingredients consist of: carnauba wax, hypromellose, lactose monohydrate, magnesium stearate, microcrystalline cellulose, povidone, sodium lauryl sulfate, sodium saccharin, sodium starch glycolate, and starch.
CLINICAL PHARMACOLOGY
Pharmacokinetics:
Absorption and Metabolism: Albendazole is poorly absorbed from the gastrointestinal tract due to its low aqueous solubility. Albendazole concentrations are negligible or undetectable in plasma as it is rapidly converted to the sulfoxide metabolite prior to reaching the systemic circulation. The systemic anthelmintic activity has been attributed to the primary metabolite, albendazole sulfoxide. Oral bioavailability appears to be enhanced when albendazole is coadministered with a fatty meal (estimated fat content 40 g) as evidenced by higher (up to 5-fold on average) plasma concentrations of albendazole sulfoxide as compared to the fasted state.
Maximal plasma concentrations of albendazole sulfoxide are typically achieved 2 to 5 hours after dosing and are on average 1.31 mcg/mL (range 0.46 to 1.58 mcg/mL) following oral doses of albendazole (400 mg) in 6 hydatid disease patients, when administered with a fatty meal. Plasma concentrations of albendazole sulfoxide increase in a dose-proportional manner over the therapeutic dose range following ingestion of a fatty meal (fat content 43.1 g). The mean apparent terminal elimination half-life of albendazole sulfoxide typically ranges from 8 to 12 hours in 25 normal subjects, as well as in 14 hydatid and 8 neurocysticercosis patients.
Following 4 weeks of treatment with albendazole (200 mg three times daily), 12 patients’ plasma concentrations of albendazole sulfoxide were approximately 20% lower than those observed during the first half of the treatment period, suggesting that albendazole may induce its own metabolism.
Distribution: Albendazole sulfoxide is 70% bound to plasma protein and is widely distributed throughout the body; it has been detected in urine, bile, liver, cyst wall, cyst fluid, and cerebral spinal fluid (CSF). Concentrations in plasma were 3- to 10-fold and 2- to 4-fold higher than those simultaneously determined in cyst fluid and CSF, respectively. Limited in vitro and clinical data suggest that albendazole sulfoxide may be eliminated from cysts at a slower rate than observed in plasma.
Metabolism and Excretion: Albendazole is rapidly converted in the liver to the primary metabolite, albendazole sulfoxide, which is further metabolized to albendazole sulfone and other primary oxidative metabolites that have been identified in human urine. Following oral administration, albendazole has not been detected in human urine. Urinary excretion of albendazole sulfoxide is a minor elimination pathway with less than 1% of the dose recovered in the urine. Biliary elimination presumably accounts for a portion of the elimination as evidenced by biliary concentrations of albendazole sulfoxide similar to those achieved in plasma.
Special Populations:
Patients with Impaired Renal Function: The pharmacokinetics of albendazole in patients with impaired renal function have not been studied. However, since renal elimination of albendazole and its primary metabolite, albendazole sulfoxide, is negligible, it is unlikely that clearance of these compounds would be altered in these patients.
Biliary Effects: In patients with evidence of extrahepatic obstruction (n = 5), the systemic availability of albendazole sulfoxide was increased, as indicated by a 2-fold increase in maximum serum concentration and a 7-fold increase in area under the curve. The rate of absorption/conversion and elimination of albendazole sulfoxide appeared to be prolonged with mean Tmax and serum elimination half-life values of 10 hours and 31.7 hours, respectively. Plasma concentrations of parent albendazole were measurable in only 1 of 5 patients.
Microbiology:
The principal mode of action for albendazole is by its inhibitory effect on tubulin polymerization which results in the loss of cytoplasmic microtubules.
In the specified treatment indications albendazole appears to be active against the larval forms of the following organisms:
Echinococcus granulosus
Taenia solium
INDICATIONS AND USAGE
Albendazole is indicated for the treatment of the following infections:
Neurocysticercosis: Albendazole is indicated for the treatment of parenchymal neurocysticercosis due to active lesions caused by larval forms of the pork tapeworm, Taenia solium.
Lesions considered responsive to albendazole therapy appear as nonenhancing cysts with no surrounding edema on contrast-enhanced computerized tomography. Clinical studies in patients with lesions of this type demonstrate a 74% to 88% reduction in number of cysts; 40% to 70% of albendazole-treated patients showed resolution of all active cysts.
Hydatid Disease: Albendazole is indicated for the treatment of cystic hydatid disease of the liver, lung, and peritoneum, caused by the larval form of the dog tapeworm, Echinococcus granulosus.
This indication is based on combined clinical studies which demonstrated non-infectious cyst contents in approximately 80 to 90% of patients given albendazole for 3 cycles of therapy of 28 days each (see DOSAGE AND ADMINISTRATION). Clinical cure (disappearance of cysts) was seen in approximately 30% of these patients, and improvement (reduction in cyst diameter of ≥25%) was seen in an additional 40%.
NOTE: When medically feasible, surgery is considered the treatment of choice for hydatid disease. When administering albendazole in the pre- or post-surgical setting, optimal killing of cyst contents is achieved when 3 courses of therapy have been given.
NOTE: The efficacy of albendazole in the therapy of alveolar hydatid disease caused by Echinococcus multilocularis has not been clearly demonstrated in clinical studies.
CONTRAINDICATIONS
Albendazole is contraindicated in patients with known hypersensitivity to the benzimidazole class of compounds or any components of albendazole.
WARNINGS
Rare fatalities associated with the use of albendazole have been reported due to granulocytopenia or pancytopenia (see PRECAUTIONS). Albendazole has been shown to cause bone marrow suppression, aplastic anemia, and agranulocytosis in patients with and without underlying hepatic dysfunction. Blood counts should be monitored at the beginning of each 28-day cycle of therapy, and every 2 weeks while on therapy with albendazole in all patients. Patients with liver disease, including hepatic echinococcosis, appear to be more at risk for bone marrow suppression leading to pancytopenia, aplastic anemia, agranulocytosis, and leukopenia attributable to albendazole and warrant closer monitoring of blood counts. Albendazole should be discontinued in all patients if clinically significant decreases in blood cell counts occur.
Albendazole should not be used in pregnant women except in clinical circumstances where no alternative management is appropriate. Patients should not become pregnant for at least 1 month following cessation of albendazole therapy. If a patient becomes pregnant while taking this drug, albendazole should be discontinued immediately. If pregnancy occurs while taking this drug, the patient should be apprised of the potential hazard to the fetus.
PRECAUTIONS
General: Patients being treated for neurocysticercosis should receive appropriate steroid and anticonvulsant therapy as required. Oral or intravenous corticosteroids should be considered to prevent cerebral hypertensive episodes during the first week of anticysticeral therapy.
Pre-existing neurocysticercosis may also be uncovered in patients treated with albendazole for other conditions. Patients may experience neurological symptoms (e.g. seizures, increased intracranial pressure and focal signs) as a result of an inflammatory reaction caused by death of the parasite within the brain. Symptoms may occur soon after treatment; appropriate steroid and anticonvulsant therapy should be started immediately.
Cysticercosis may, in rare cases, involve the retina. Before initiating therapy for neurocysticercosis, the patient should be examined for the presence of retinal lesions. If such lesions are visualized, the need for anticysticeral therapy should be weighed against the possibility of retinal damage caused by albendazole-induced changes to the retinal lesion.
Information for Patients: Patients should be advised that:
- Some people, particularly young children, may experience difficulties swallowing the tablets whole. In young children, the tablets should be crushed or chewed and swallowed with a drink of water.
- Albendazole may cause fetal harm, therefore, women of childbearing age should begin treatment after a negative pregnancy test.
- Women of childbearing age should be cautioned against becoming pregnant while on albendazole or within 1 month of completing treatment.
- During albendazole therapy, because of the possibility of harm to the liver or bone marrow, routine (every 2 weeks) monitoring of blood counts and liver function tests should take place.
- Albendazole should be taken with food.
Laboratory Tests:
White Blood Cell Count: Albendazole has been shown to cause occasional (less than 1% of treated patients) reversible reductions in total white blood cell count. Rarely, more significant reductions may be encountered including granulocytopenia, agranulocytosis, or pancytopenia. Blood counts should be performed at the start of each 28-day treatment cycle and every 2 weeks during each 28-day cycle in all patients. Patients with liver disease, including hepatic echinococcosis, appear to be more at risk of bone marrow suppression and warrant closer monitoring of blood counts (see WARNINGS). Albendazole should be discontinued in all patients if clinically significant decreases in blood cell counts occur.
Liver Function: In clinical trials, treatment with albendazole has been associated with mild to moderate elevations of hepatic enzymes in approximately 16% of patients. These elevations have generally returned to normal upon discontinuation of therapy. There have also been case reports of acute liver failure of uncertain causality and hepatitis (see ADVERSE REACTIONS).
Liver function tests (transaminases) should be performed before the start of each treatment cycle and at least every 2 weeks during treatment. If hepatic enzymes exceed twice the upper limit of normal, consideration should be given to discontinuing albendazole therapy based on individual patient circumstances. Restarting albendazole treatment in patients whose hepatic enzymes have normalized off treatment is an individual decision that should take into account the risk/benefit of further albendazole usage. Laboratory tests should be performed frequently if albendazole treatment is restarted.
Patients with abnormal liver function test results are at increased risk for hepatotoxicity and bone marrow suppression (see WARNINGS). Therapy should be discontinued if liver enzymes are significantly increased or if clinically significant decreases in blood cell counts occur.
Theophylline: Although single doses of albendazole have been shown not to inhibit theophylline metabolism (see Drug Interactions), albendazole does induce cytochrome P450 1A in human hepatoma cells. Therefore, it is recommended that plasma concentrations of theophylline be monitored during and after treatment with albendazole.
Drug Interactions:
Dexamethasone: Steady-state trough concentrations of albendazole sulfoxide were about 56% higher when 8 mg dexamethasone was coadministered with each dose of albendazole (15 mg/kg/day) in 8 neurocysticercosis patients.
Praziquantel: In the fed state, praziquantel (40 mg/kg) increased mean maximum plasma concentration and area under the curve of albendazole sulfoxide by about 50% in healthy subjects (n = 10) compared with a separate group of subjects (n = 6) given albendazole alone. Mean Tmax and mean plasma elimination half-life of albendazole sulfoxide were unchanged. The pharmacokinetics of praziquantel were unchanged following coadministration with albendazole (400 mg).
Cimetidine: Albendazole sulfoxide concentrations in bile and cystic fluid were increased (about 2-fold) in hydatid cyst patients treated with cimetidine (10 mg/kg/day) (n = 7) compared with albendazole (20 mg/kg/day) alone (n = 12). Albendazole sulfoxide plasma concentrations were unchanged 4 hours after dosing.
Carcinogenesis, Mutagenesis, Impairment of Fertility:
Long-term carcinogenicity studies were conducted in mice and rats. In the mouse study, albendazole was administered in the diet at doses of 25, 100, and 400 mg/kg/day (0.1, 0.5, and 2 times the recommended human dose based on body surface area in mg/m2, respectively) for 108 weeks. In the rat study, albendazole was administered in the diet at doses of 3.5, 7, and 20 mg/kg/day (0.04, 0.08, and 0.21 times the recommended human dose based on body surface area in mg/m2, respectively) for 117 weeks. There was no evidence of increased incidence of tumors in the treated mice and rats when compared to the control group.
In genotoxicity tests, albendazole was found negative in an Ames Salmonella/Microsome Plate mutation assay with and without metabolic activation or with and without pre-incubation, cell-mediated Chinese Hamster Ovary chromosomal aberration test and in vivo mouse micronucleus test. In the in vitro BALB/3T3 cells transformation assay, albendazole produced weak activity in the presence of metabolic activation while no activity was found in the absence of metabolic activation.
Albendazole did not adversely affect male or female fertility in the rat at an oral dose of 30 mg/kg/day (0.32 times the recommended human dose based on body surface area in mg/m2).
Pregnancy:
Teratogenic Effects: Pregnancy Category C.
Albendazole has been shown to be teratogenic (to cause embryotoxicity and skeletal malformations) in pregnant rats and rabbits. The teratogenic response in the rat was shown at oral doses of 10 and 30 mg/kg/day (0.10 times and 0.32 times the recommended human dose based on body surface area in mg/m2, respectively) during gestation days 6 to 15 and in pregnant rabbits at oral doses of 30 mg/kg/day (0.60 times the recommended human dose based on body surface area in mg/m2) administered during gestation days 7 to 19. In the rabbit study, maternal toxicity (33% mortality) was noted at 30 mg/kg/day. In mice, no teratogenic effects were observed at oral doses up to 30 mg/kg/day (0.16 times the recommended human dose based on body surface area in mg/m2), administered during gestation days 6 to 15.
There are no adequate and well-controlled studies of albendazole administration in pregnant women. Albendazole should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus (see WARNINGS).
Nursing Mothers: Albendazole is excreted in animal milk. It is not known whether it is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when albendazole is administered to a nursing woman.
Pediatric Use: Experience in children under the age of 6 years is limited. In hydatid disease, infection in infants and young children is uncommon, but no problems have been encountered in those who have been treated. In neurocysticercosis, infection is more frequently encountered. In 5 published studies involving pediatric patients as young as 1 year, no significant problems were encountered, and the efficacy appeared similar to the adult population.
ADVERSE REACTIONS
The adverse event profile of albendazole differs between hydatid disease and neurocysticercosis. Adverse events occurring with a frequency of ≥1% in either disease are described in the table below.
These symptoms were usually mild and resolved without treatment. Treatment discontinuations were predominantly due to leukopenia (0.7%) or hepatic abnormalities (3.8% in hydatid disease). The following incidence reflects events that were reported by investigators to be at least possibly or probably related to albendazole.
| Adverse Event | Hydatid Disease | Neurocysticercosis |
| Abnormal Liver Function Tests | 15.6 | <1.0 |
| Abdominal Pain | 6.0 | 0 |
| Nausea/Vomiting | 3.7 | 6.2 |
| Headache | 1.3 | 11.0 |
| Dizziness/Vertigo | 1.2 | <1.0 |
| Raised Intracranial Pressure | 0 | 1.5 |
| Meningeal Signs | 0 | 1.0 |
| Reversible Alopecia | 1.6 | <1.0 |
| Fever | 1.0 | 0 |
The following adverse events were observed at an incidence of <1%:
Blood and Lymphatic System Disorders: Leukopenia. There have been rare reports of granulocytopenia, pancytopenia, agranulocytosis, or thrombocytopenia (see WARNINGS). Patients with liver disease, including hepatic echinococcosis, appear to be more at risk of bone marrow suppression (see WARNINGS and PRECAUTIONS).
Postmarketing Adverse Reactions: In addition to adverse events reported from clinical trials, the following events have been identified during world-wide post-approval use of albendazole. Because they are reported voluntarily from a population of unknown size, estimates of frequency cannot be made. These events have been chosen for inclusion due to a combination of their seriousness, frequency of reporting, or potential causal connection to albendazole.
OVERDOSAGE
Significant toxicity and mortality were shown in male and female mice at doses exceeding 5,000 mg/kg; in rats, at estimated doses between 1,300 and 2,400 mg/kg; in hamsters, at doses exceeding 10,000 mg/kg; and in rabbits, at estimated doses between 500 and 1,250 mg/kg. In the animals, symptoms were demonstrated in a dose-response relationship and included diarrhea, vomiting, tachycardia, and respiratory distress.
One overdosage has been reported with albendazole in a patient who took at least 16 grams over 12 hours. No untoward effects were reported. In case of overdosage, symptomatic therapy and general supportive measures are recommended.
DOSAGE AND ADMINISTRATION
Dosing of albendazole will vary, depending upon which of the following parasitic infections is being treated. In young children, the tablets should be crushed or chewed and swallowed with a drink of water.
| Indication | Patient Weight | Dose | Duration |
| Hydatid Disease | 60 kg or greater | 400 mg twice daily, with meals | 28-day cycle followed by a 14-day albendazole-free interval, for a total of 3 cycles |
| less than 60 kg | 15 mg/kg/day given in divided doses twice daily with meals (maximum total daily dose 800 mg) |
||
| NOTE: When administering albendazole in the pre- or post-surgical setting, optimal killing of cyst contents is achieved when 3 courses of therapy have been given. |
|||
| Neurocysticercosis | 60 kg or greater | 400 mg twice daily, with meals | 8 to 30 days |
| less than 60 kg | 15 mg/kg/day given in divided doses twice daily with meals (maximum total daily dose 800 mg) |
||
Patients being treated for neurocysticercosis should receive appropriate steroid and anticonvulsant therapy as required. Oral or intravenous corticosteroids should be considered to prevent cerebral hypertensive episodes during the first week of treatment.
HOW SUPPLIED
Albendazole is supplied as 200 mg, white to off white, circular, biconvex, bevel-edged, film coated TILTAB tablet embossed "ap" and "550". They are supplied as follows:
Bottles of 2 NDC 54505-055-22
Bottles of 28 NDC 54505-055-28
Store at 20° to 25°C (68° to 77°F) [See USP Controlled Room Temperature].
TILTAB is a registered trademarks of GlaxoSmithKline, used with permission.
Manufactured by:
GlaxoSmithKline
Mississauga, Ontario
L5N 6L4 Canada
Distributed by:
Lineage Therapeutics Inc.
Horsham, PA 19044
LB# 610-02 Rev. December, 2017
70012585
| ALBENDAZOLE
albendazole tablet, film coated |
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
| Labeler - Lineage Therapeutics Inc (078677620) |