Label: MINOLIRA EXTENDED RELEASE- minocycline hydrochloride tablet


-
Contains inactivated NDC Code(s)
NDC Code(s): 71403-101-05, 71403-101-30, 71403-102-05, 71403-102-30 - Packager: EPI Health, Inc
- Category: HUMAN PRESCRIPTION DRUG LABEL
- DEA Schedule: None
- Marketing Status: New Drug Application
Drug Label Information
Updated November 2, 2022
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use MINOLIRA™ safely and effectively. See full prescribing information for MINOLIRA.
MINOLIRA™ (minocycline hydrochloride) extended-release tablets, for oral use
Initial U.S. Approval: 1971INDICATIONS AND USAGE
MINOLIRA is a tetracycline-class drug indicated to treat only inflammatory lesions of non-nodular moderate to severe acne vulgaris in patients 12 years of age and older. (1)
Limitations of Use
This formulation of minocycline has not been evaluated in the treatment of infections. To reduce the development of drug-resistant bacteria as well as to maintain the effectiveness of other antibacterial drugs, MINOLIRA should be used only as indicated [see Warnings and Precautions (5.13)].
DOSAGE AND ADMINISTRATION
Recommended dosage: Approximately 1 mg/kg once daily for 12 weeks. (2)
DOSAGE FORMS AND STRENGTHS
Extended- release tablets: 105 mg and 135 mg of minocycline, functionally scored (3)
CONTRAINDICATIONS
This drug is contraindicated in persons who have shown hypersensitivity to any of the tetracyclines. (4)
WARNINGS AND PRECAUTIONS
- The use of MINOLIRA during the second and third trimesters of pregnancy, infancy and childhood up to the age of 8 years may cause permanent discoloration of the teeth (yellow-gray-brown) and reversible inhibition of bone growth. (5.1, 5.2, 5.3, 8.1, 8.4)
- If pseudomembranous colitis occurs, discontinue MINOLIRA. (5.4)
- If liver injury is suspected, discontinue MINOLIRA. (5.5)
- If renal impairment exists, MINOLIRA doses may need to be adjusted to avoid excessive systemic accumulations of the drug and possible liver toxicity. (5.6)
- Minocycline may cause central nervous system side effects including lightheadedness, dizziness, or vertigo. (5.7)
- Minocycline may cause intracranial hypertension in adults and adolescents. Discontinue MINOLIRA if symptoms occur. (5.8)
- Minocycline has been associated with autoimmune syndromes; discontinue MINOLIRA immediately if symptoms occur. (5.9)
- Minocycline has been associated with anaphylaxis, serious skin reactions, erythema multiforme, and DRESS syndrome. Discontinue MINOLIRA immediately if symptoms occur. (5.11)
ADVERSE REACTIONS
The most commonly observed adverse reactions (incidence ≥5%) are headache, fatigue, dizziness, and pruritus. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact EPI Health, LLC at 1-800-499-4468 or www.epihealth.com or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 6/2018
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Teratogenic Effects
5.2 Tooth Discoloration
5.3 Inhibition of Bone Growth
5.4 Pseudomembranous Colitis
5.5 Hepatotoxicity
5.6 Metabolic Effects
5.7 Central Nervous System Effects
5.8 Intracranial Hypertension
5.9 Autoimmune Syndromes
5.10 Photosensitivity
5.11 Serious Skin/Hypersensitivity Reaction
5.12 Tissue Hyperpigmentation
5.13 Development of Drug-Resistant Bacteria
5.14 Superinfection
5.15 Laboratory Monitoring
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
7.1 Anticoagulants
7.2 Penicillin
7.3 Antacids and Iron Preparations
7.4 Low Dose Oral Contraceptives
7.5 Drug/Laboratory Test Interactions
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
MINOLIRA is indicated to treat the inflammatory lesions of non-nodular moderate to severe acne vulgaris in patients 12 years of age and older.
Limitations of Use
This formulation of minocycline has not been evaluated in the treatment of infections.
To reduce the development of drug-resistant bacteria as well as to maintain the effectiveness of other antibacterial drugs, MINOLIRA should be used only as indicated [see Warnings and Precautions (5.13)].
-
2 DOSAGE AND ADMINISTRATION
The recommended dosage of MINOLIRA is approximately 1 mg/kg once daily for 12 weeks. Higher doses have not shown to be of additional benefit in the treatment of inflammatory lesions of acne, and may be associated with more acute vestibular side effects. The 105 mg and 135 mg tablets may be split on the score line for dosing of patient weight ranges of 45-59 kg and 60-89 kg, respectively (see Table 1).
Table 1: Dosing Table for MINOLIRA Patient's Weight
(kg)Daily Dose Tablet Strength and Size to Administer Actual Dose
(mg/kg)45 – 59 52.5 half of the 105 mg tablet 1.16 –0.88 60 – 89 67.5 half of the 135 mg tablet 1.13 – 0.76 90 – 125 105 one 105 mg tablet 1.17 – 0.84 126 – 136 135 one 135 mg tablet 1.07 – 0.99 MINOLIRA may be taken with or without food [see Clinical Pharmacology (12.3)]. Ingestion of food along with MINOLIRA may help reduce the risk of esophageal irritation and ulceration. MINOLIRA tablets should not be chewed or crushed.
In patients with renal impairment, the total dosage should be decreased by either reducing the recommended individual doses and/or by extending the time intervals between doses [see Warnings and Precautions (5.6)].
-
3 DOSAGE FORMS AND STRENGTHS
MINOLIRA extended-release tablets are white to off-white, functionally scored, rectangular tablets with brown or gold color speckles and a single score line on both surfaces. MINOLIRA are available in the following two strengths.
- 105 mg extended-release tablets: ‘M1’debossed on one surface, where ‘M’ and ‘1’ are on either side of the score line. Each tablet contains 105 mg minocycline, equivalent to 113.4 mg of minocycline hydrochloride.
- 135 mg extended-release tablets: ‘M3’ is debossed on one surface, where ‘M’ and ‘3’ are on either side of the score line. Each tablet contains 135 mg minocycline, equivalent to 145.8 mg of minocycline hydrochloride.
-
4 CONTRAINDICATIONS
MINOLIRA is contraindicated in patients who have shown hypersensitivity to any of the tetracyclines [see Serious Skin/Hypersensitivity Reactions (5.11)].
-
5 WARNINGS AND PRECAUTIONS
5.1 Teratogenic Effects
Avoid MINOLIRA use during pregnancy.
MINOLIRA, like other tetracycline-class drugs, can cause fetal harm when administered to a pregnant woman. MINOLIRA, like other tetracycline-class drugs, may cause permanent discoloration of the teeth and inhibit bone growth when administered during pregnancy. Based on animal data, tetracyclines cross the placenta, are found in fetal tissues, and can cause skeletal malformation and retardation of skeletal development on the developing fetus. Evidence of embryotoxicity has been noted in animals treated early in pregnancy. If MINOLIRA is used during pregnancy, advise the patient of the potential risk to the fetus and discontinue treatment [see Use in Specific Populations (8.1)].
5.2 Tooth Discoloration
The use of tetracycline class drugs during tooth development (second and third trimesters of pregnancy, infancy, and childhood up to the age of 8 years) may cause permanent discoloration of the teeth (yellow-gray-brown). This adverse reaction is more common during long-term use of the tetracycline but has been observed following repeated short-term courses. Enamel hypoplasia has also been reported. Use of tetracycline drugs is not recommended during tooth development.
The safety and effectiveness of MINOLIRA have not been established in pediatric patients less than 12 years of age.
5.3 Inhibition of Bone Growth
All tetracyclines form a stable calcium complex in any bone-forming tissue. A decrease in fibula growth rate has been observed in premature human infants given oral tetracycline in doses of 25 mg/kg every 6 hours. This reaction was shown to be reversible when the drug was discontinued. The safety and effectiveness of MINOLIRA have not been established in patients less than 12 years of age [see Use in Specific Populations (8.1, 8.4)].
Results of animal studies indicate that tetracyclines cross the placenta, are found in fetal tissues, and can cause retardation of skeletal development on the developing fetus. Evidence of embryotoxicity has been noted in animals treated early in pregnancy [see Use in Specific Populations (8.1)].
5.4 Pseudomembranous Colitis
Clostridium difficile associated diarrhea (CDAD) has been reported with nearly all antibacterial agents, including minocycline, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile.
C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin producing strains of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibiotic use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents.
If CDAD is suspected or confirmed, antibiotic use not directed against C. difficile may need to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibiotic treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated.
5.5 Hepatotoxicity
Post-marketing cases of serious liver injury, including irreversible drug-induced hepatitis and fulminant hepatic failure (sometimes fatal) have been reported with minocycline use in the treatment of acne.
5.6 Metabolic Effects
The anti-anabolic action of the tetracyclines may cause an increase in BUN. While this is not a problem in those with normal renal function, in patients with significantly impaired function, higher serum levels of tetracycline-class drugs may lead to azotemia, hyperphosphatemia, and acidosis. If renal impairment exists, even usual oral or parenteral doses may lead to excessive systemic accumulations of the drug and possible liver toxicity. Under such conditions, lower than usual total doses are indicated, and if therapy is prolonged, serum level determinations of the drug may be advisable.
5.7 Central Nervous System Effects
Central nervous system side effects including light-headedness, dizziness or vertigo have been reported with minocycline therapy. Patients who experience these symptoms should be cautioned about driving vehicles or using hazardous machinery while on minocycline therapy. These symptoms may disappear during therapy and usually rapidly disappear when the drug is discontinued.
5.8 Intracranial Hypertension
Intracranial hypertension has been associated with the use of tetracycline-class drugs including MINOLIRA. Clinical manifestations of intracranial hypertension include headache, blurred vision, diplopia and vision loss; papilledema can be found on fundoscopy. Women of childbearing age who are overweight or have a history of IH are at a greater risk for developing intracranial hypertension. Concomitant use of isotretinoin and tetracycline should be avoided because isotretinoin, a systemic retinoid, is also known to cause intracranial hypertension.
Although intracranial hypertension typically resolves after discontinuation of treatment, the possibility for permanent visual loss exists. If visual disturbance occurs during treatment, prompt ophthalmologic evaluation is warranted. Because intracranial pressure can remain elevated for weeks after drug cessation, patients should be monitored until they stabilize.
5.9 Autoimmune Syndromes
Tetracyclines have been associated with the development of autoimmune syndromes. The long- term use of minocycline in the treatment of acne has been associated with drug-induced lupus- like syndrome, autoimmune hepatitis and vasculitis. Sporadic cases of serum sickness have presented shortly after minocycline use. Symptoms may be manifested by fever, rash, arthralgia, and malaise. In symptomatic patients, immediately discontinue the use of all tetracycline-class drugs, including MINOLIRA.
5.10 Photosensitivity
Photosensitivity manifested by an exaggerated sunburn reaction has been observed in some individuals taking tetracyclines; this reaction has been reported less frequently with minocycline. Patients should minimize or avoid exposure to natural or artificial sunlight (tanning beds or UVA/B treatment) while using minocycline. If patients need to be outdoors while using MINOLIRA, they should wear loose-fitting clothes that protect skin from sun exposure and discuss other sun protection measures with their physician.
5.11 Serious Skin/Hypersensitivity Reaction
Cases of anaphylaxis, serious skin reactions (e.g. Stevens Johnson syndrome), erythema multiforme, and drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome have been reported postmarketing with minocycline use in patients with acne. DRESS syndrome consists of cutaneous reaction (such as rash or exfoliative dermatitis), eosinophilia, and one or more of the following visceral complications such as: hepatitis, pneumonitis, nephritis, myocarditis, and pericarditis. Fever and lymphadenopathy may be present. In some cases, death has been reported. If this syndrome is recognized, discontinue MINOLIRA immediately.
5.12 Tissue Hyperpigmentation
Tetracyclines are known to cause hyperpigmentation. Tetracycline therapy may induce hyperpigmentation in many organs, including nails, bone, skin, eyes, thyroid, visceral tissue, oral cavity (teeth, mucosa, alveolar bone), sclerae and heart valves. Skin and oral pigmentation has been reported to occur independently of time or amount of drug administration, whereas other tissue pigmentation has been reported to occur upon prolonged administration. Skin pigmentation includes diffuse pigmentation as well as pigmentation over sites of scars or injury.
5.13 Development of Drug-Resistant Bacteria
MINOLIRA has not been evaluated in the treatment of infections.
Bacterial resistance to the tetracyclines may develop in patients using MINOLIRA. Because of the potential for drug-resistant bacteria to develop during the use of MINOLIRA, it should be used only as indicated.
-
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug, and may not reflect the rates observed in practice.
The following table summarizes selected adverse reactions reported in clinical trials at a rate of ≥1% for minocycline hydrochloride extended release tablets.
Table 2: Selected Treatment-Emergent Adverse Reactions in at least 1% of Clinical Trial Adverse Reactions Minocycline Hydrochloride Extended-Release Tablets
(1 mg/kg)
N = 674
(%)Placebo
N = 364
(%)At least one treatment emergency event 379 (56) 197 (54) Headache 152(23) 83(23) Fatigue 62 (9) 24 (7) Dizziness 59 (9) 17 (5) Pruritus 31 (5) 16 (4) Malaise 26 (4) 9 (3) Mood alteration 17 (3) 9 (3) Somnolence 13 (2) 3 (1) Urticaria 10 (2) 1 (0) Tinnitus 10 (2) 5 (1) Arthralgia 9 (1) 2 (0) Vertigo 8 (1) 3 (1) Dry Mouth 7 (1) 5 (1) Myalgia 7 (1) 4 (1) 6.2 Postmarketing Experience
Adverse reactions that have been reported with minocycline hydrochloride use in a variety of indications include:
Skin and hypersensitivity reactions: fixed drug eruptions, balanitis, erythema multiforme, Stevens-Johnson syndrome, anaphylactoid purpura, photosensitivity, pigmentation of skin and mucous membranes, hypersensitivity reactions, angioneurotic edema, anaphylaxis, DRESS syndrome [see Warnings and Precautions (5.11)].
Autoimmune conditions: polyarthralgia, pericarditis, exacerbation of systemic lupus, pulmonary infiltrates with eosinophilia, transient lupus-like syndrome.
Central nervous system: pseudotumor cerebri, bulging fontanels in infants, decreased hearing.
Endocrine: brown-black microscopic thyroid discoloration, abnormal thyroid function.
Oncology: thyroid cancer.
Oral: glossitis, dysphagia, tooth discoloration.
Gastrointestinal: enterocolitis, pancreatitis, hepatitis, liver failure.
Genitourinary: Preliminary studies suggest that use of minocycline may have deleterious effects on human spermatogenesis [see Nonclinical Toxicoloty (13.1)].
Renal: reversible acute renal failure.
Hematology: hemolytic anemia, thrombocytopenia, eosinophilia.
-
7 DRUG INTERACTIONS
7.1 Anticoagulants
Because tetracyclines have been shown to depress plasma prothrombin activity, patients who are on anticoagulant therapy may require downward adjustment of their anticoagulant dosage.
7.2 Penicillin
Because bacteriostatic drugs may interfere with the bactericidal action of penicillin, to avoid giving tetracycline-class drugs in conjunction with penicillin.
7.3 Antacids and Iron Preparations
Absorption of tetracyclines is impaired by antacids containing aluminum, calcium or magnesium and iron-containing preparations.
7.4 Low Dose Oral Contraceptives
In a multi-center study to evaluate the effect of minocycline extended release tablets on low dose oral contraceptives, hormone levels over one menstrual cycle with and without minocycline extended release tablets 1 mg/kg once-daily were measured. Based on the results of this trial, minocycline-related changes in estradiol, progestinic hormone, FSH and LH plasma levels, of breakthrough bleeding, or of contraceptive failure, cannot be ruled out. To avoid contraceptive failure during treatment with minocycline, advise patients of reproductive potential to use a second form of contraception in addition to low-dose oral contraceptives.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
MINOLIRA, like tetracycline class drugs, may cause permanent discoloration of teeth and reversible inhibition of bone growth when administered during pregnancy [see Warnings and Precautions (5.1) and Use in Specific Populations (8.4)]. Post-marketing cases of minocycline use in pregnant women report congenital anomalies such as limb reductions. The limited data are not sufficient to inform a drug-associated risk for birth defects or miscarriage. In animal reproduction studies, minocycline induced skeletal malformations in fetuses when orally administered to pregnant rats and rabbits during the period of organogenesis at systemic exposure of approximately 3 times and 2 times, respectively, the systemic exposure to minocycline observed in patients administered MINOLIRA (see Data). If a patient becomes pregnant while taking this drug, advise the patient of the risk to the fetus and discontinue treatment.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
Data
Human Data
The use of tetracycline during tooth development (second and third trimesters of pregnancy) may cause permanent discoloration of deciduous teeth. This adverse reaction is more common during long-term use of the drug but has been observed following repeated short-term courses.
Animal Data
Results of animal studies indicate that tetracyclines cross the placenta, are found in fetal tissues, and can cause retardation of skeletal development of the developing fetus. [see Warnings and Precautions (5.1)].
Minocycline induced skeletal malformations (bent limb bones) in fetuses when administered to pregnant rats and rabbits during the period of organogenesis at doses of 30 mg/kg/day and 100 mg/kg/day, respectively, (resulting in approximately 3 times and 2 times, respectively, the systemic exposure to minocycline observed in patients administered MINOLIRA). Reduced mean fetal body weight was observed when minocycline was administered to pregnant rats during the period of organogenesis at a dose of 10 mg/kg/day (which resulted in approximately the same level of systemic exposure to minocycline as that observed in patients administered MINOLIRA).
Minocycline was assessed for effects on peri- and post-natal development of rats in a study that involved oral administration to pregnant rats during the period of organogenesis through lactation , at doses of 5, 10, or 50 mg/kg/day. In this study, body weight gain was significantly reduced in pregnant females that received 50 mg/kg/day (resulting in approximately 2.5 times the systemic exposure to minocycline observed in patients administered MINOLIRA). No effects of treatment on the duration of the gestation period or the number of live pups born per litter were observed. Gross external anomalies observed in F1 pups (offspring of animals that received minocycline) included reduced body size, improperly rotated forelimbs, and reduced size of extremites. No effects were observed on the physical development, behavior, learning ability, or reproduction of F1 pups, and there was no effect on gross appearance of F2 pups (offspring of F1 animals).
8.2 Lactation
Risk Summary
Tetracycline-class drugs including minocycline are present in breast milk. It is not known whether minocycline has an effect on the breastfed infant or on milk production. Because of the potential for serious adverse effects on bone and tooth development in breastfed infants from the tetracycline-class drugs, advise a woman that breastfeeding is not recommended with MINOLIRA therapy [see Warnings and Precautions (5.1)].
8.3 Females and Males of Reproductive Potential
Contraception
MINOLIRA may reduce the effectiveness of low-dose oral contraceptives. Patients of reproductive potential should not rely on low-dose oral contraceptives as an effective contraceptive method, and should use an additional method of contraception during treatment with MINOLIRA [see Drug Interactions (7.4)].
Infertility
Avoid using MINOLIRA in males who are attempting to conceive a child. Limited human studies suggest that minocycline may have a deleterious effect on spermatogenesis. In a fertility study in rats, minocycline adversely affected spermatogenesis when orally administered to male rats at doses resulting in approximately 15 to 40 times the level of systemic exposure to minocycline observed in patients administered MINOLIRA [see Nonclinical Toxicology (13.1)].
8.4 Pediatric Use
The safety and effectiveness of MINOLIRA have been established in pediatric patients 12 years of age and older for the treatment of inflammatory lesions of non-nodular moderate to severe acne vulgaris [see Pharmacokinetics (12.3) and Clinical Studies (14)]. Tooth discoloration and inhibition of bone growth have been observed in pediatric patients [see Warnings and Precautions (5.2, 5.3)]. The safety and effectiveness of MINOLIRA have not been established in pediatric patients less than 12 years of age.
8.5 Geriatric Use
Clinical studies of MINOLIRA did not include sufficient numbers of subjects aged 65 years and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients.
In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and concomitant disease or other drug therapy.
- 10 OVERDOSAGE
-
11 DESCRIPTION
Minocycline hydrochloride, a semi synthetic derivative of tetracycline, is [4S (4α,4aα,5aα,12aα)]-4,7-Bis(dimethylamino)-1,4,4a,5,5a,6,11,12a-octahydro-3,10,12,12a tetrahydroxy-1,11-dioxo-2-naphthacenecarboxamide mono hydrochloride. The structural formula is representated below:
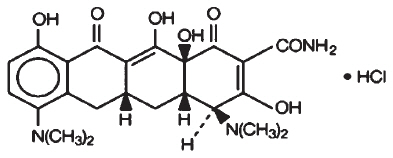
C23H27N3O7∙HCl M. W. 493.95
MINOLIRA (minocycline hydrochloride) extended-release tablets for oral administration contain 105 mg or 135 mg of minocycline, equivalent to 113.4 mg or 145.8 mg of minocycline hydrochloride, respectively. MINOLIRA extended-release tablets, 105 mg and 135 mg, contain 25% of minocycline as immediate release beads and 75% of minocycline as extended release beads.
In addition, 105 mg and 135 mg tablets contain the following inactive ingredients: ethyl cellulose NF, hypromellose USP, isopropyl alcohol USP, microcrystalline cellulose NF, polytheylene glycol 400 NF, purified water USP, silicified microcrystalline cellulose NF, sodium stearyl fumarate NF, talc USP, triethyl citrate NF.
Both 105 mg and 135 mg tablets also contain Opadry clear which contains hydroxyl propyl cellulose NF and hypromellose USP.
-
12 CLINICAL PHARMACOLOGY
12.3 Pharmacokinetics
The pharmacokinetics of minocycline following oral administration of a single dose of MINOLIRA (135 mg) was investigated in 77 healthy male and female adult subjects under fasting conditions. The pharmacokinetic parameters of minocycline under fasting conditions are presented in Table 3.
Table 3 : Pharmacokinetic Parameters of Minocycline Following Administration of a Single Dose of MINOLIRA (135 mg) under Fasting Conditions (N = 77) Cmax (ng/mL) Tmax (hr)* AUC0-t (ng∙hr/mL) T1/2 (hr) - *
- Median (Min-Max)
Mean ± SD 700 ± 261 2.0 (1.0 – 4.5) 10874 ± 3717 15.6 ± 2.46 In a separate trial, a single dose of MINOLIRA (135 mg) was administered orally with a high-fat, high-calorie meal that included dairy products to 36 healthy male and female adult subjects. The estimated calorie content of the meal was 848 Kcal, consisting of 145 Kcal from protein, 250 Kcal from carbohydrates, and 453 Kcal from fat. The pharmacokinetic parameters of minocycline under fed conditions are presented in Table 4.
Table 4 : Pharmacokinetic Parameters of Minocycline Following Administration of a Single Dose of MINOLIRA (135 mg) under Fed Conditions (N = 36) Cmax (ng/mL) Tmax (hr)* AUC0-t (ng∙hr/mL) T1/2 (hr) - *
- Median (Min-Max)
Mean ± SD 707 ± 190 3.5 (1.5 – 6.0) 12000 ± 2967 17.1 ± 3.03 Minocycline is lipid soluble and distributes into the skin and sebum.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
In a carcinogenicity study in which minocycline hydrochloride was orally administered to male and female rats once daily for up to 104 weeks at dosages up to 200 mg/kg/day, minocycline hydrochloride was associated in both genders with follicular cell tumors of the thyroid gland, including increased incidences of adenomas, carcinomas, and the combined incidence of adenomas and carcinomas in males, and adenomas and the combined incidence of adenomas and carcinomas in females. In a carcinogenicity study in which minocycline hydrochloride was orally administered to male and female mice once daily for up to 104 weeks at dosages up to 150 mg/kg/day, exposure to minocycline hydrochloride did not result in a significantly increased incidence of neoplasms in either males or females.
Minocycline was not mutagenic in vitro in a bacterial reverse mutation assay (Ames test) or CHO/HGPRT mammalian cell assay in the presence or absence of metabolic activation. Minocycline was not clastogenic in vitro using human peripheral blood lymphocytes or in vivo in a mouse micronucleus test.
Male and female reproductive performance in rats was unaffected by oral doses of minocycline of up to 300 mg/kg/day (which resulted in up to approximately 40 times the level of systemic exposure to minocycline observed in patients administered MINOLIRA). However, oral administration of 100 or 300 mg/kg/day of minocycline to male rats (resulting in approximately 15 to 40 times the level of systemic exposure to minocycline observed in patients administered MINOLIRA) adversely affected spermatogenesis. Effects observed at 300 mg/kg/day included a reduced number of sperm cells per gram of epididymis, an apparent reduction in the percentage of sperm that were motile, and (at 100 and 300 mg/kg/day) increased numbers of morphologically abnormal sperm cells. Morphological abnormalities observed in sperm samples included absent heads, misshapen heads, and abnormal flagella.
-
14 CLINICAL STUDIES
The safety and efficacy of minocycline hydrochloride extended-release tablets in the treatment of inflammatory lesions of non-nodular moderate to severe acne vulgaris was assessed in two 12-week, multi-center, randomized, double-blind, placebo-controlled, trials in subjects ≥12 years. The mean age of subjects was 20 years and subjects were from the following racial groups: White (73%), Hispanic (13%), Black (11%), Asian/Pacific Islander (2%), and Other (2%).
In two efficacy and safety trials, a total of 924 subjects with non-nodular moderate to severe acne vulgaris received minocycline hydrochloride extended-release tablets (approximately 1 mg/kg) or placebo for a total of 12 weeks.
The two primary efficacy endpoints were:
1) Mean percent change in inflammatory lesion counts from Baseline to 12 weeks.
2) Percentage of subjects with an Evaluator's Global Severity Assessment (EGSA) of clear or almost clear at 12 weeks.
Efficacy results are presented in Table 5.
Table 5: Efficacy Results at Week 12 Trial 1 Trial 2 Minocycline Hydrochloride Extended Release Tablets
(1 mg/kg)
N=300Placebo
N=151Minocycline Hydrochloride Extended Release Tablets
(1 mg/kg)
N=315Placebo
N=158- *
- Evaluator's Global Severity Assessment
Mean Percent
Improvement in Inflammatory Lesions43.1% 31.7% 45.8% Number of subjects clear or almost clear on EGSA* 52
(17.3%)12
(7.9%)50
(15.9%)15
(9.5%)Minocycline hydrochloride did not demonstrate any effect on non-inflammatory lesions (benefit or worsening).
-
16 HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
MINOLIRA is supplied as functionally scored extended-release tablets containing minocycline hydrochloride equivalent to 105 mg and 135 mg of minocycline.
The 105 mg extended-release tablets are white to off-white, rectangular, with brown or gold color speckles. The tablets have a single score line on both surfaces and are debossed with ‘M1’ on one surface. On the face with debossing, ‘M’ and ‘1’ are on either side of the score line. Each tablet contains 26.25 mg of minocycline as immediate release beads and 78.75 mg of minocycline as extended release beads. The 105 mg tablets are supplied as follows:
NDC 71403-101-30 Bottle of 30 The 135 mg extended-release tablets are white to off-white, rectangular with brown or gold color speckles. The tablets have a single score line on both surfaces and are debossed with ‘M3’ on one surface. On the face with debossing, ‘M’ and ‘3’ are on either side of the score line. Each tablet contains 33.75 mg of minocycline as immediate release beads and 101.25 of minocycline as extended release beads. The 135 mg tablets are supplied as follows:
NDC 71403-102-30 Bottle of 30 -
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information and Instruction for Use).
Advise patients of the following:
Teratogenic effects
- Advise patients to avoid use of MINOLIRA during pregnancy.
- Advise patients that MINOLIRA use during pregnancy may cause inhibition of fetal bone growth.
- Advise patients that MINOLIRA use during pregnancy may cause discoloration of deciduous teeth.
- Advise patients to discontinue MINOLIRA during pregnancy.
Tooth Discoloration
- Advise caregivers of pediatric patients that MINOLIRA use may cause permanent discoloration of deciduous and permanent teeth.
Contraception
- Advise patients of reproductive potential that MINOLIRA may reduce the effectiveness of low-dose oral contraceptives. Advise patients of reproductive potential not rely on low-dose oral contraceptives as an effective contraceptive method and to use an additional method of contraception during treatment with MINOLIRA.
Tissue Hyperpigmentation
- Inform patients that MINOLIRA may cause discoloration of skin, scars, teeth or gums.
Pseudomembranous Colitis
- Advise patients that pseudomembranous colitis can occur with minocycline therapy, including MINOLIRA. Advise patients to seek medical attention if they develop watery or bloody stools.
Hepatotoxicity
- Inform patients about the possibility of hepatotoxicity. Advise patients to seek medical advice if they experience symptoms or signs of hepatotoxicity, including loss of appetite, tiredness, diarrhea, jaundice, increased bleeding tendencies, confusion, and sleepiness.
Central Nervous System Effects
- Inform patients that central nervous system adverse reactions including dizziness or vertigo have been reported with minocycline therapy. Caution patients about driving vehicles or using hazardous machinery if they experience such symptoms while on MINOLIRA.
Intracranial Hypertension
- Inform patients that intracranial hypertension can occur with minocycline therapy. Advise patients to seek medical attention if they develop unusual headache, visual symptoms, such as blurred vision, diplopia, and vision loss.
- Inform patients that autoimmune syndromes, including drug-induced lupus-like syndrome, autoimmune hepatitis, vasculitis and serum sickness have been observed with tetracycline-class drugs, including minocycline. Symptoms may be manifested by arthralgia, fever, rash and malaise.
- Advise patients who experience such symptoms to stop the drug immediately and seek medical help.
Photosensitivity
- Inform patients that photosensitivity manifested by an exaggerated sunburn reaction has been observed in some individuals taking tetracyclines, including minocycline.
- Advise patients to minimize or avoid exposure to natural or artificial UV light (tanning beds or UVA/B treatment) while using MINOLIRA.
- Discuss other sun protection measures, if patients need to be outdoors while using MINOLIRA.
- Advise patients to discontinue treatment at the first evidence of sunburn.
Important Administration Instructions
- Inform patients to take MINOLIRA as directed. Missing doses or not completing the full course of therapy may decrease the effectiveness of the current treatment course and increase the likelihood that bacteria will develop resistance and will not be treatable by other antibacterial drugs in the future.
- Advise patient not to chew or crush the tablet.
- Advise patients to split MINOLIRA tablet across the score line, if required depending on patient's body weight.
-
SPL UNCLASSIFIED SECTION
Manufactured by:
Dr. Reddy's Laboratories Limited
FTO-SEZ-Process-Unit-01
Survey No: 57 to 59, 60, 52 & 72
Sector No: 9 to14 & 17 to 20, Devunipalavalasa Village
Ranasthalam Mandal
Srikakulam District
Andhra Pradesh, IndiaManufactured for:
EPI Health, LLC
134 Columbus St.
Charleston, SC 29403, USAMIN-PI-0618
150073673 -
PATIENT INFORMATION MINOLIRA (min-oh-li'-rah) (minocycline hydrochloride) extended-release tablets
WHAT IS MINOLIRA?
MINOLIRA is prescription medicine used to treat only pimples and red bumps (non-nodular inflammatory lesions) that happen with moderate to severe acne vulgaris in people 12 years and older.
MINOLIRA should not be used for the treatment of infections.
It is not known if MINOLIRA is safe and effective in children under the age of 12 years.
Who should not take MINOLIRA?
- Do not take MINOLIRA if you are allergic to medicines in the tetracycline class. Ask your healthcare provider or pharmacist for a list of these medicines if you are not sure.
Before you take MINOLIRA, tell your healthcare provider about all of your medical conditions, including if you:
- have kidney problems
- have liver problems
- have diarrhea or watery stools
- have vision problems.
- are pregnant or plan to become pregnant. MINOLIRA may harm your unborn baby. Taking MINOLIRA while you are pregnant may cause serious side effects on the growth of bone and teeth of your baby. Stop taking MINOLIRA and call your healthcare provider right away if you become pregnant during treatment with MINOLIRA.
- are breastfeeding or plan to breastfeed. MINOLIRA can pass into your breast milk and may harm your baby. You should not breastfeed during treatment with MINOLIRA.
Tell your healthcare provider about all the other medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. MINOLIRA and other medicines may affect each other causing serious side effects.
Especially tell your healthcare provider if you take:
- birth control pills. MINOLIRA may reduce the effectiveness of certain birth control pills. You could become pregnant. You should use a second form of birth control during treatment with MINOLIRA. Talk to your healthcare provider about what types of birth control you can use to prevent pregnancy during treatment with MINOLIRA.
- a medicine taken by mouth that contains isotretinoin.
How should I take MINOLIRA?
See the detailed "Instructions for Use" that comes with MINOLIRA for information about breaking your MINOLIRA extended-release tablets.
- Take MINOLIRA exactly as your healthcare provider tells you.
- Your healthcare provider will tell you how much MINOLIRA to take and if you will need to break your MINOLIRA extended-release tablets based on your weight. MINOLIRA comes in 2 strengths:
- 105 mg extended-release tablets
- 135 mg extended-release tablets
-
Do not miss your dose of MINOLIRA. Missing doses or not taking all doses of MINOLIRA may:
- make the treatment not work as well
- increase the chance that the bacteria will become resistant to MINOLIRA
- Take MINOLIRA with or without food. Taking MINOLIRA with food may lower your risk of getting irritation or ulcers in your esophagus. Your esophagus is the tube that connects your mouth to your stomach.
- Do not crush or chew MINOLIRA tablets.
- If you take too much MINOLIRA, call your healthcare provider right away or go to the nearest hospital emergency room.
What should I avoid during treatment with MINOLIRA?
- Avoid sunlight or artificial sunlight, such as sunlamps or tanning beds. You could get severe sunburn. Use sunscreen and wear loose-fitting clothes that cover your skin while out in sunlight. Stop taking MINOLIRA if you get sunburn.
- You should not drive or operate dangerous machinery until you know how MINOLIRA affects you. MINOLIRA may cause you to feel dizzy or lightheaded, or have a spinning feeling (vertigo).
What are possible side effects of MINOLIRA?
MINOLIRA may cause serious side effects, including:
- Harm to an unborn baby. See "What should I tell my healthcare provider before taking MINOLIRA?"
- Permanent teeth discoloration. MINOLIRA may permanently turn a baby or child's teeth yellow-gray-brown during tooth development. You should not use MINOLIRA during tooth development. Tooth development happens in the second and third trimesters of pregnancy, and from birth to 8 years of age.
- Slow bone growth. MINOLIRA may slow bone growth in infants and children. Slow bone growth is reversible after stopping treatment with MINOLIRA.
- Diarrhea. Diarrhea can happen with most antibiotics, including MINOLIRA. This diarrhea may be caused by an infection (Clostridium difficile) in your intestines. Call your healthcare provider right away if you get watery or bloody stools.
-
Liver problems. MINOLIRA can cause liver problems that may lead to death. Stop taking MINOLIRA and call your healthcare provider right away if you get any of the following signs or symptoms of liver problems:
- loss of appetite
- tiredness
- diarrhea
- yellowing of your skin or the whites of your eyes
- bleeding more easily than normal
- confusion
- sleepiness
- Increased pressure around the brain (intracranial hypertension). This condition may lead to vision changes and permanent vision loss. You may be more likely to get intracranial hypertension if you are a female of childbearing potential and are overweight or have a history of intracranial hypertension. Stop taking MINOLIRA and tell your healthcare provider right away if you have blurred vision, double vision, vision loss, or headaches.
- Immune system reactions including a lupus-like syndrome, hepatitis, and inflammation of blood or lymph vessels (vasculitis). Call your healthcare provider right away if you get a fever, rash, joint pain, or body weakness.
-
Serious skin or allergic reactions that may affect parts of your body such as your liver, lungs, kidneys and heart. Sometimes these can lead to death. Stop taking MINOLIRA and go to the nearest hospital emergency room right away if you have any of the following signs or symptoms:
- skin rash, hives, sores in your mouth, or your skin blisters and peels
- swelling of your face, eyes, lips, tongue, or throat
- trouble swallowing or breathing
- blood in your urine
- fever, yellowing of the skin or the whites of your eyes, dark colored urine
- pain on the right side of the stomach area (abdominal pain)
- chest pain or abnormal heartbeats
- swelling in your legs, ankles, and feet
- darkening of your nails, skin, eyes, scars, teeth, and gums
- Discoloration (hyperpigmentation). MINOLIRA can cause darkening of your skin, scars, teeth, gums, nails, and whites of your eyes.
The most common side effects of MINOLIRA include:
- headache
- tiredness
- dizziness
- itching
MINOLIRA may cause fertility problems in males. This may affect your ability to father a child. Talk to your healthcare provider if you have concerns about fertility.
Your healthcare provider may tell you to decrease your dose or completely stop taking MINOLIRA if you develop certain serious side effects during treatment with MINOLIRA.
Your healthcare provider may do blood tests to check you for side effects during treatment with MINOLIRA.
These are not all the side effects of MINOLIRA. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. You may also report side effects to EPI Health, LLC at 1-800-499-4468.
How should I store MINOLIRA?
- Store MINOLIRA at room temperature between 68°F to 77°F (20°C to 25°C).
- Keep MINOLIRA in the container that it comes in and keep the container tightly closed.
- Keep MINOLIRA away from light and moisture.
Keep MINOLIRA and all medicines out of the reach of children. General information about the safe and effective use of MINOLIRA.
Medicines are sometimes prescribed for purposes other than those listed in the Patient Information leaflet. Do not use MINOLIRA for a condition for which it was not prescribed. Do not give MINOLIRA to other people, even if they have the same symptoms you have. It may harm them. You can ask your healthcare provider or pharmacist for information about MINOLIRA that is written for health professionals.
What are the ingredients in MINOLIRA?
Active ingredient: minocycline hydrochloride.
Inactive ingredients: ethyl cellulose, hypromellose, isopropyl alcohol, microcrystalline cellulose, polyethylene glycol 400, purified water, silicified microcrystalline cellulose, sodium stearyl fumarate, talc, triethyl citrate
Both 105 mg and 135 mg tablets also contain Opadry clear which contains hydroxyl propyl cellulose and hypromellose.
Manufactured for:
EPI Health, LLC
134 Columbus St.
Charleston, SC 29403, USAManufactured by:
Dr. Reddy's Laboratories Limited
FTO-SEZ, Process Unit-01,
Devunipalavalasa Village, Srikakulam (District),
Andhra Pradesh, India.
Pin-:532409MINOLIRA is a registered trademark of EPI Health, LLC
Item No. MIN-PI-0618/150073673
Issued: 06/2018
-
INSTRUCTIONS FOR USE MINOLIRA (min-oh-li'-rah) (minocycline hydrochloride) extended-release tablets
Read this Instructions for Use before you start using MINOLIRA and each time you get a refill. There may be new information. This information does not take the place of talking to your healthcare provider about your medical condition or treatment.
Note:
- Your healthcare provider will tell you how much of MINOLIRA to take and if you will need to break MINOLIRA extended-release tablets based on your weight.
- MINOLIRA comes in 2 strengths:
- 105 mg extended-release tablets
- 135 mg extended-release tablets
The 105 mg MINOLIRA tablets:
- are marked with an "M" and "1" on one side and is separated by a scored line
- can be taken whole or may be broken at the scored line to provide two equal halves of 52.5 mg each
How to break your MINOLIRA tablets?
- Hold the tablet between your thumbs and index fingers close to the scored line.
- Apply enough pressure to break the tablet at the scored line.
-
Do not break the MINOLIRA tablet in any other way.
- 105 mg treatment (take whole tablet)

top view of whole tablet side view of whole tablet side view of whole tablet with thumbs and index fingers -
- 52.5 mg treatment (take one-half of the tablet)



side view of breaking a whole tablet with thumbs and index fingers top view of a split tablet side view of one-half tablet with a thumb and an index finger The 135 mg MINOLIRA tablets:
- are marked with an "M" and "3" on one side and is separated by a scored line
- can be taken whole or may be broken at the scored line to provide two equal halves of 67.5 mg each
How to break your MINOLIRA tablets?
- Hold the tablet between your thumbs and index fingers close to the scored line.
- Apply enough pressure to break the tablet at the scored line.
-
Do not break the MINOLIRA tablet in any other way.
- 135 mg treatment (take whole tablet)



top view of whole tablet side view of whole tablet side view of whole tablet with thumbs and index fingers -
- 67.5 mg treatment (take one-half of the tablet)



side view of breaking a whole tablet with thumbs and index fingers top view of a split tablet side view of one-half tablet with a thumb and an index finger How should I store MINOLIRA?
- Store MINOLIRA at room temperature between 68°F to 77°F (20°C to 25°C).
- Keep MINOLIRA in the container that it comes in and keep the container tightly closed.
- Keep MINOLIRA away from light and moisture.
Keep MINOLIRA and all medicines out of the reach of children.
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Manufactured for:
EPI Health, LLC
134 Columbus St.
Charleston, SC 29403, USAManufactured by:
Dr. Reddy's Laboratories Limited
FTO-SEZ, Process Unit-01,
Devunipalavalasa Village, Srikakulam (District),
Andhra Pradesh, India.
Pin-:532409MINOLIRA is a registered trademark of EPI Health, LLC
Item No. MIN-PI-0618/150073673
Issued: 06/2018
-
PRINCIPAL DISPLAY PANEL - 135 mg Tablet Bottle Label
NDC 71403-102-30
Rx Onlyminolira™
(minocycline hydrochloride)
extended-release tablets135 mg*
*Each tablet contains 135 mg of minocycline
(33.75 mg as immediate release beads and
101.25 mg as extended release beads), equivalent
to 145.8 mg of minocycline hydrochloride.30 Tablets
EPIHEALTH
Advancing Dermatology
-
PRINCIPAL DISPLAY PANEL - 105 mg Tablet Bottle Label
NDC 71403-101-30
Rx Onlyminolira™
(minocycline hydrochloride)
extended-release tablets105 mg*
*Each tablet contains 105 mg of minocycline
(26.25 mg as immediate release beads and 78.75
mg as extended release beads), equivalent to
113.4 mg of minocycline hydrochloride.30 Tablets
EPIHEALTH
Advancing Dermatology
-
INGREDIENTS AND APPEARANCE
MINOLIRA EXTENDED RELEASE
minocycline hydrochloride tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:71403-102 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Minocycline Hydrochloride (UNII: 0020414E5U) (MINOCYCLINE - UNII:FYY3R43WGO) MINOCYCLINE 135 mg Inactive Ingredients Ingredient Name Strength Isopropyl Alcohol (UNII: ND2M416302) Sodium Stearyl Fumarate (UNII: 7CV7WJK4UI) Talc (UNII: 7SEV7J4R1U) MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) Hypromellose 2910 (5 Mpa.S) (UNII: R75537T0T4) Polyethylene Glycol 400 (UNII: B697894SGQ) Ethylcellulose (10 Mpa.S) (UNII: 3DYK7UYZ62) Hypromellose 2910 (15 Mpa.S) (UNII: 36SFW2JZ0W) Triethyl Citrate (UNII: 8Z96QXD6UM) HYDROXYPROPYL CELLULOSE (1600000 WAMW) (UNII: RFW2ET671P) Water (UNII: 059QF0KO0R) Product Characteristics Color WHITE Score 2 pieces Shape RECTANGLE Size 20mm Flavor Imprint Code M3 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:71403-102-30 1 in 1 CARTON 03/15/2019 1 30 in 1 BOTTLE; Type 0: Not a Combination Product 2 NDC:71403-102-05 1 in 1 CARTON 03/15/2019 2 5 in 1 BOTTLE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA209269 03/15/2019 MINOLIRA EXTENDED RELEASE
minocycline hydrochloride tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:71403-101 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Minocycline Hydrochloride (UNII: 0020414E5U) (MINOCYCLINE - UNII:FYY3R43WGO) MINOCYCLINE 105 mg Inactive Ingredients Ingredient Name Strength Isopropyl Alcohol (UNII: ND2M416302) Sodium Stearyl Fumarate (UNII: 7CV7WJK4UI) Talc (UNII: 7SEV7J4R1U) MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) Hypromellose 2910 (5 Mpa.S) (UNII: R75537T0T4) Polyethylene Glycol 400 (UNII: B697894SGQ) Ethylcellulose (10 Mpa.S) (UNII: 3DYK7UYZ62) Hypromellose 2910 (15 Mpa.S) (UNII: 36SFW2JZ0W) Triethyl Citrate (UNII: 8Z96QXD6UM) HYDROXYPROPYL CELLULOSE (1600000 WAMW) (UNII: RFW2ET671P) Water (UNII: 059QF0KO0R) Product Characteristics Color WHITE Score 2 pieces Shape RECTANGLE Size 19mm Flavor Imprint Code M1 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:71403-101-30 1 in 1 CARTON 03/15/2019 1 30 in 1 BOTTLE; Type 0: Not a Combination Product 2 NDC:71403-101-05 1 in 1 CARTON 03/15/2019 2 5 in 1 BOTTLE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA209269 03/15/2019 Labeler - EPI Health, Inc (080638894) Establishment Name Address ID/FEI Business Operations EPI Health, Inc. 080638894 MANUFACTURE(71403-102, 71403-101)