HYDROMORPHONE HYDROCHLORIDE- hydromorphone hydrochloride injection, solution
Hospira, Inc.
Disclaimer: This drug has not been found by FDA to be safe and effective, and this labeling has not been approved by FDA. For further information about unapproved drugs, click here.
----------
Hydromorphone Hydrochloride Injection
|
|
|
| URGENT: Important Drug Information
|
|
| Subject: | Temporary Importation of Hydromorphone Hydrochloride Injection, USP 2 mg/mL ampules from Canada to Address U.S. Drug Shortage |

August 2018
Dear Health Care Provider,
Due to the current critical shortage of Hydromorphone Hydrochloride Injection, USP CII in the United States (U.S.) market, Hospira, Inc., a Pfizer company (Hospira), is coordinating with the U.S. Food and Drug Administration (FDA) to increase the availability of the drug.
Hospira has initiated temporary importation of Hydromorphone Hydrochloride Injection, USP 2 mg/mL ampules into the U.S. market. This product is marketed in Canada, and is manufactured in Canada by Sandoz Canada Inc. (Sandoz). At this time, no other entity except Hospira is authorized by the FDA to import or distribute Sandoz Hydromorphone Hydrochloride Injection, USP 2 mg/mL ampules in the United States.
The Sandoz Canada site is an FDA-registered facility and is in compliance with current good manufacturing practice requirements. The facility is subject to inspections by FDA, and is currently supplying other sterile injectable products to the U.S. market. FDA has not approved Sandoz's Hydromorphone Hydrochloride Injection, USP 2 mg/mL ampules in the United States.
Effective immediately, and during this temporary period, Hospira will offer the following presentation of Hydromorphone Hydrochloride Injection, USP:
| Product | Strength | Packaging | NDC Number | Marketing Authorization # |
|---|---|---|---|---|
| Hydromorphone Hydrochloride Injection, USP | 2 mg/mL | 1 mL amber Ampule | 00409-3459-07 | Drug Identification Number (DIN) 02145901 (Canada) |
It is important to note the following:
- The Sandoz ampule does not have the CII controlled substance symbol on the ampule label, only on the outer carton. Please ensure your staff and any provider in your institution who may be involved in the handling, preparation and administration of this product are aware that this product is a controlled substance and follows proper procedures when handling this controlled substance.
- It is recommended that you and/or your institution develop a diversion prevention strategy for handling, using and storing this product
- The barcode may not register accurately on the U.S. scanning systems. Institutions should manually input the product into their systems and confirm that barcode systems do not provide incorrect information when the product is scanned. Alternative procedures should be followed to assure that the correct drug product is being used and administered to individual patients.
- Follow standard aseptic technique and withdraw contents of the Sandoz hydromorphone ampules with a 5 micron needle filter. After withdrawing the contents of the ampule, change the needle before injection.
There are some key substantive differences in the format and content of the labeling between the FDA-approved Hydromorphone Hydrochloride for Injection, USP and the imported Sandoz Canada product. The product comparison tables attached highlight the differences between Hospira's Hydromorphone Hydrochloride for Injection, USP and Sandoz Canada's non-US approved Hydromorphone Hydrochloride for Injection, USP.
Hydromorphone hydrochloride is available only by prescription in the U.S.
This letter and the attachments are not intended as a complete description of the benefits and risks related to the use of Hydromorphone Hydrochloride for Injection, USP. Please refer to the package insert for the FDA approved Hydromorphone Hydrochloride for Injection, USP for full prescribing information, available from: https://www.pfizerinjectables.com/products/Hydromorphone_Hydrochloride.
Contact Information
Please contact Hospira, Inc., (Pfizer) customer Service at 1-844-646-4398 (Mon.–Fri. 8am–7pm ET) or your Hospira (Pfizer) representative for any questions you may have regarding this notification.
Adverse Events and Product Quality Complaints
To report adverse reactions or quality issues, contact Hospira (Pfizer) at 1-800-438-1985.
Adverse reactions or quality problems experienced with the use of this product may be reported to the FDA's MedWatch Adverse Event Reporting Program either online, by regular mail, or by fax:
- Complete and submit the report Online: www.fda.gov/medwatch/report.htm
- Regular mail or Fax: download form www.fda.gov/MedWatch/getforms.htm or call 1-800-332-1088 to request a reporting form, then complete and return to the address on the pre-addressed form, or submit by fax to 1-800-FDA-0178 (1-800-332-0178)
Sincerely,
Eddie G M Power PhD MBA
Vice President, US Medical Affairs, Chief Medical Office
Pfizer Essential Health
Product Ampul and Carton Comparison Table
| US FDA APPROVED PRODUCT | IMPORTED PRODUCT |
|---|---|
HYDROMORPHONE HYDROCHLORIDE INJECTION, USP, CII – Hospira, Inc. Ampul Label (Clear Ampul) | HYDROmorphone Hydrochloride Injection USP – Sandoz Canada Inc. Ampule Label (Amber Ampule)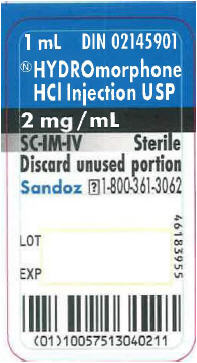 |
HYDROMORPHONE HYDROCHLORIDE INJECTION, USP, CII – Hospira, Inc. Carton Label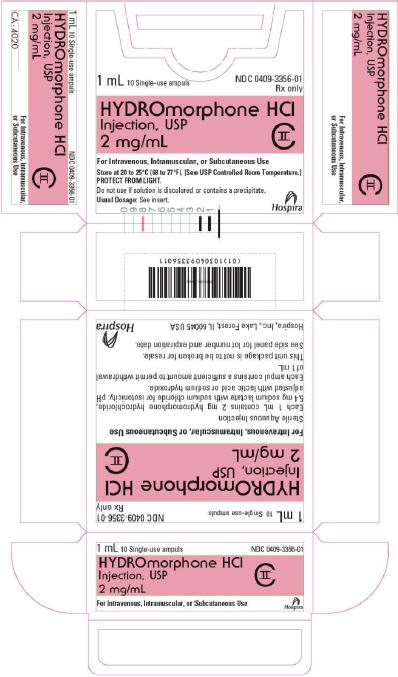 | HYDROmorphone Hydrochloride Injection USP* – Sandoz Canada Inc. Carton Label (5 ampule × 1 mL)a
 *'Chlorhydrate d'HYDROmorphone' is French for Hydromorphone Hydrochloride a Product may be packaged in either a 5 ampule × 1 mL carton or 10 ampule × 1 mL carton. Product is equivalent, the only difference is in packaging |
HYDROMORPHONE HYDROCHLORIDE INJECTION, USP, CII – Hospira, Inc. Carton Label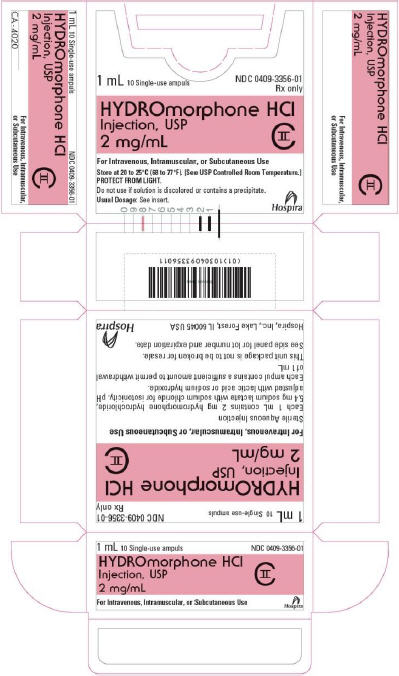 | HYDROmorphone Hydrochloride Injection USP* – Sandoz Canada Inc. Carton Label (10 ampule × 1 mL)a
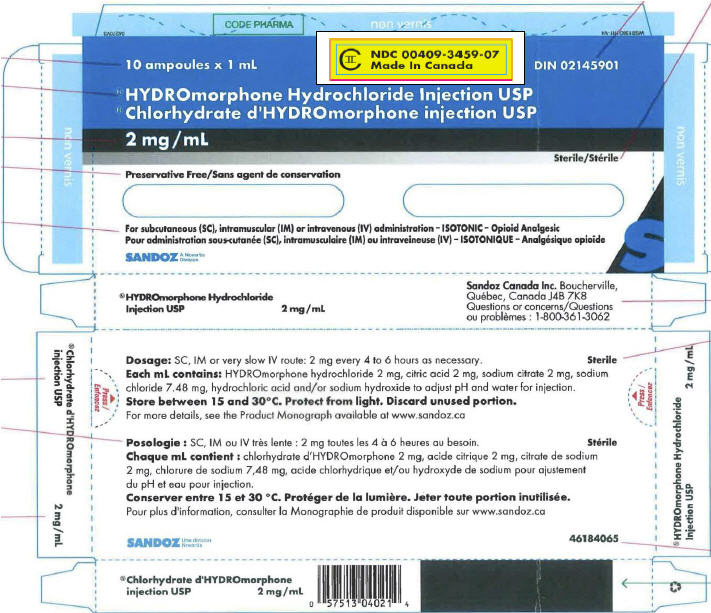 *'Chlorhydrate d'HYDROmorphone' is French for Hydromorphone Hydrochloride a Product may be packaged in either a 5 ampule × 1 mL carton or 10 ampule × 1 mL carton. Product is equivalent, the only difference is in packaging |
Product Prescribing Information Comparison Table
| US FDA APPROVED PRODUCT | IMPORTED PRODUCT | |||||||
|---|---|---|---|---|---|---|---|---|
|
HYDROMORPHONE HYDROCHLORIDE INJECTION, USP, CII – Hospira, Inc. |
HYDROmorphone Hydrochloride Injection USP – Sandoz Canada Inc. |
|||||||
|
BOXED WARNING |
||||||||
|
WARNING: ADDICTION, ABUSE, AND MISUSE; LIFE-THREATENING RESPIRATORY DEPRESSION; NEONATAL OPIOID WITHDRAWAL SYNDROME; and RISK FROM CONCOMITANT USE WITH BENZODIAZEPINES OR OTHER CNS DEPRESSANTS |
SERIOUS WARNINGS AND PRECAUTIONS
Limitations of Use
|
|||||||
|
Addiction, Abuse, and Misuse Hydromorphone Hydrochloride Injection exposes patients and other users to the risks of opioid addiction, abuse, and misuse, which can lead to overdose and death. Assess each patient's risk prior to prescribing Hydromorphone Hydrochloride Injection, and monitor all patients regularly for the development of these behaviors and conditions [See Warnings and Precautions (5.1)]. |
Addiction, Abuse, and Misuse
|
|||||||
|
Accidental Exposure
|
||||||||
|
Life-Threatening Respiratory Depression Serious, life-threatening, or fatal respiratory depression may occur with use of Hydromorphone Hydrochloride Injection. Monitor for respiratory depression, especially during initiation of Hydromorphone Hydrochloride Injection or following a dose increase [See Warnings and Precautions (5.2)]. |
Life-threatening Respiratory Depression
|
|||||||
|
Neonatal Opioid Withdrawal Syndrome Prolonged use of Hydromorphone Hydrochloride Injection during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized and treated, and requires management according to protocols developed by neonatology experts. If opioid use is required for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available [See Warnings and Precautions (5.3)]. |
Neonatal Opioid Withdrawal Syndrome
|
|||||||
|
Interaction with Alcohol The co-ingestion of alcohol with HYDROmorphone Hydrochloride Injection USP should be avoided as it may result in dangerous additive effects, causing serious injury or death (see WARNINGS AND PRECAUTIONS and DRUG INTERACTIONS). |
||||||||
|
Risks From Concomitant Use With Benzodiazepines Or Other CNS Depressants Concomitant use of opioids with benzodiazepines or other central nervous system (CNS) depressants, including alcohol, may result in profound sedation, respiratory depression, coma, and death [see Warnings and Precautions (5.4), Drug Interactions (7)].
|
Risks From Concomitant Use With Benzodiazepines Or Other CNS Depressants
|
|||||||
|
Indications and Usage |
||||||||
|
INDICATIONS AND USAGE |
INDICATIONS AND CLINICAL USE |
|||||||
|
Hydromorphone Hydrochloride Injection is indicated for the management of pain severe enough to require an opioid analgesic and for which alternative treatments are inadequate. Limitations of Use Because of the risks of addiction, abuse, and misuse with opioids, even at recommended doses [see Warnings and Precautions (5.1)], reserve Hydromorphone Hydrochloride Injection for use in patients for whom alternative treatment options [e.g., non-opioid analgesics or opioid combination products]: |
HYDROmorphone Hydrochloride Injection USP (HYDROmorphone hydrochloride) is indicated for the relief of moderate to severe pain. HYDROmorphone Hydrochloride Injection USP should only be used in patients for whom alternative treatment options are ineffective or not tolerated (e.g., non-opioid analgesics). |
|||||||
| ||||||||
|
Dosage and Administration |
||||||||
|
HYDROmorphone Hydrochloride Injection USP should only be used in patients for whom alternative treatment options are ineffective or not tolerated (e.g., non-opioid analgesics).
Dosing Considerations
Dose Titration: Dose titration is the key to success with opioid analgesic therapy. Proper optimization of doses scaled to the relief of the individual's pain should aim at the regular administration of the lowest dose which will achieve the overall treatment goal of satisfactory pain relief with acceptable side effects. |
||||||||
|
||||||||
|
Use of Hydromorphone Hydrochloride Injection as the First Opioid Analgesic Subcutaneous or Intramuscular Administration The usual starting dose is 1 mg to 2 mg every 2 to 3 hours as necessary for pain. Depending on the clinical situation, the initial starting dose may be lowered in patients who are opioid naïve. Intravenous Administration The initial starting dose is 0.2 mg to 1 mg every 2 to 3 hours as necessary for pain control. Intravenous administration should be given slowly, over at least 2 to 3 minutes, depending on the dose. Titrate the dose to achieve acceptable pain management and tolerable adverse events. The initial dose should be educed in the elderly or debilitated and may be lowered to 0.2 mg. Conversion from Other Opioids to Hydromorphone Hydrochloride Injection There is inter-patient variability in the potency of opioid drugs and opioid formulations. Therefore, a conservative approach is advised when determining the total daily dosage of Hydromorphone Hydrochloride Injection. It is safer to underestimate a patient's 24-hour Hydromorphone Hydrochloride Injection dosage than to overestimate the 24-hour Hydromorphone Hydrochloride Injection dosage and manage an adverse reaction due to overdose. If the decision is made to convert to Hydromorphone Hydrochloride Injection from another opioid analgesic using publicly available data, convert the current total daily amount(s) of opioid(s) received to an equivalent total daily dose of Hydromorphone Hydrochloride Injection and reduce by one-half due to the possibility of incomplete cross tolerance. Divide the new total amount by the number of doses permitted based on dosing interval (e.g., 8 doses for every-three-hour dosing). Titrate the dose according to the patient's response. |
||||||||
|
|
Patients with Hepatic Impairment: One-fourth to one-half the usual HYDROmorphone Hydrochloride Injection USP injection starting dose depending on the extent of impairment . |
|||||||
|
Start patients with hepatic impairment on one-fourth to one-half the usual dose of Hydromorphone Hydrochloride Injection depending on the extent of impairment [see Clinical Pharmacology, Pharmacokinetics and Metabolism (12.3)]. |
||||||||
|
|
Patients with Renal Impairment: One-fourth to one-half the usual HYDROmorphone Hydrochloride Injection USP injection starting dose depending on the degree of impairment. |
|||||||
|
Start patients with renal impairment on one-fourth to one-half the usual starting dose of Hydromorphone Hydrochloride Injection depending on the degree of impairment [see Clinical Pharmacology, Pharmacokinetics (12.3)]. |
||||||||
|
| ||||||||
|
Individually titrate Hydromorphone Hydrochloride Injection to a dose that provides adequate analgesia and minimizes adverse reactions. Continually reevaluate patients receiving Hydromorphone Hydrochloride Injection to assess the maintenance of pain control and the relative incidence of adverse reactions, as well as monitoring for the development of addiction, abuse, or misuse [see Warnings and Precautions (5.1)]. Frequent communication is important among the prescriber, other members of the healthcare team, the patient, and the caregiver/family during periods of changing analgesic requirements, including initial titration. If the level of pain increases after dosage stabilization, attempt to identify the source of increased pain before increasing the Hydromorphone Hydrochloride Injection dosage. If unacceptable opioid-related adverse reactions are observed, consider reducing the dosage. Adjust the dosage to obtain an appropriate balance between management of pain and opioid-related adverse reactions. | ||||||||
|
Adjustment or Reduction of Dosage: Following successful relief of moderate to severe pain, periodic attempts to reduce the opioid dose should be made. Smaller doses or complete discontinuation may become feasible due to a change in the patient's condition or mental state. If treatment discontinuation is required, the dose of opioid may be decreased as follows: one- half of the previous daily dose given q6h for the first two days, followed thereafter by a 25% reduction every two days. |
||||||||
|
When a patient who has been taking Hydromorphone Hydrochloride Injection regularly and may be physically dependent no longer requires therapy with Hydromorphone Hydrochloride Injection, taper the dose gradually, by 25% to 50% every 2 to 4 days, while monitoring carefully for signs and symptoms of withdrawal. If the patient develops these signs or symptoms, raise the dose to the previous level and taper more slowly, either by increasing the interval between decreases, decreasing the amount of change in dose, or both. Do not abruptly discontinue Hydromorphone Hydrochloride Injection in a physically-dependent patient [see Warnings and Precautions (5.11), Drug Abuse and Dependence (9.3)]. |
||||||||
|
Dosage Forms and Strengths |
||||||||
|
DOSAGE FORMS, COMPOSITION AND PACKAGING
Dosage Forms and Composition |
||||||||
|
DOSAGE FORMS AND STRENGTHS Hydromorphone Hydrochloride Injection is available as: |
||||||||
|
1 mg/mL, 2 mg/mL, and 4 mg/mL 1 mg/mL, 2 mg/mL, and 4 mg/mL 0.5 mg/0.5 mL, 1 mg/mL, and 2 mg/mL 2 mg/mL |
|||||||
|
The drug product is a clear, colorless to nearly colorless aqueous sterile solution. Each 1 mL of sterile solution contains 1 mg, 2 mg or 4 mg hydromorphone hydrochloride. |
||||||||
| Contraindications | ||||||||
|
Hydromorphone Hydrochloride Injection is contraindicated in patients with:
|
|
|||||||
|
Hydromorphone Hydrochloride Injection contains hydromorphone, a Schedule II controlled substance. As an opioid, Hydromorphone Hydrochloride Injection exposes users to the risks of addiction, abuse, and misuse [see Drug Abuse and Dependence (9)]. Although the risk of addiction in any individual is unknown, it can occur in patients appropriately prescribed Hydromorphone Hydrochloride Injection. Addiction can occur at recommended dosages and if the drug is misused or abused. Assess each patient's risk for opioid addiction, abuse, or misuse prior to prescribing Hydromorphone Hydrochloride Injection, and monitor all patients receiving Hydromorphone Hydrochloride Injection for the development of these behaviors and conditions. Risks are increased in patients with a personal or family history of substance abuse (including drug or alcohol abuse or addiction) or mental illness (e.g., major depression). The potential for these risks should not, however, prevent the proper management of pain in any given patient. Patients at increased risk may be prescribed opioids such as Hydromorphone Hydrochloride Injection, but use in such patients necessitates intensive counseling about the risks and proper use of Hydromorphone Hydrochloride Injection along with intensive monitoring for signs of addiction, abuse, and misuse. Opioids are sought by drug abusers and people with addiction disorders and are subject to criminal diversion. Consider these risks when prescribing or dispensing Hydromorphone Hydrochloride Injection. Strategies to reduce these risks include prescribing the drug in the smallest appropriate quantity. Contact local state professional licensing board or state controlled substances authority for information on how to prevent and detect abuse or diversion of this product. | ||||||||
|
|
Respiratory Depression: |
|||||||
|
Serious, life-threatening, or fatal respiratory depression has been reported with the use of opioids, even when used as recommended. Respiratory depression, if not immediately recognized and treated, may lead to respiratory arrest and death. Management of respiratory depression may include close observation, supportive measures, and use of opioid antagonists, depending on the patient's clinical status [see Overdosage (10)]. Carbon dioxide (CO2) retention from opioid-induced respiratory depression can exacerbate the sedating effects of opioids. While serious, life-threatening, or fatal respiratory depression can occur at any time during the use of Hydromorphone Hydrochloride Injection, the risk is greatest during the initiation of therapy or following a dosage increase. Monitor patients closely for respiratory depression, especially within the first 24–72 hours of initiating therapy with and following dosage increases of Hydromorphone Hydrochloride Injection. To reduce the risk of respiratory depression, proper dosing and titration of Hydromorphone Hydrochloride Injection are essential [see Dosage and Administration (2.1)]. Overestimating the Hydromorphone Hydrochloride Injection dosage when converting patients from another opioid product can result in a fatal overdose with the first dose. |
||||||||
|
|
Neonatal Opioid Withdrawal Syndrome (NOWS)
|
|||||||
|
Prolonged use of Hydromorphone Hydrochloride Injection during pregnancy can result in withdrawal in the neonate. Neonatal opioid withdrawal syndrome, unlike opioid withdrawal syndrome in adults, may be life-threatening if not recognized and treated, and requires management according to protocols developed by neonatology experts. Observe newborns for signs of neonatal opioid withdrawal syndrome and manage accordingly. Advise pregnant women using opioids for a prolonged period of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available [see Use in Specific Populations (8.1), Patient Counseling Information (17)]. |
||||||||
|
|
||||||||
|
Risks from Concomitant Use with Benzodiazepines or Other CNS Depressants |
Interactions with CNS Depressants (including benzodiazepines and alcohol): HYDROmorphone should be used with caution and in a reduced dosage during concomitant administration of other opioid analgesics, general anesthetics, phenothiazines and other tranquilizers, sedative-hypnotics, tricyclic antidepressants, antipsychotics, antihistamines, benzodiazepines, centrally-active anti-emetics and other CNS depressants. Respiratory depression, hypotension and profound sedation, coma or death may result. |
|||||||
|
Profound sedation, respiratory depression, coma, and death may result from the concomitant use of Hydromorphone Hydrochloride Injection with benzodiazepines or other CNS depressants (e.g., non-benzodiazepine sedatives/hypnotics, anxiolytics, tranquilizers, muscle relaxants, general anesthetics, antipsychotics, other opioids, alcohol). Because of these risks, reserve concomitant prescribing of these drugs for use in patients for whom alternative treatment options are inadequate. Observational studies have demonstrated that concomitant use of opioid analgesics and benzodiazepines increases the risk of drug-related mortality compared to use of opioid analgesics alone. Because of similar pharmacological properties, it is reasonable to expect similar risk with the concomitant use of other CNS depressant drugs with opioid analgesics [see Drug Interactions (7)]. If the decision is made to prescribe a benzodiazepine or other CNS depressant concomitantly with an opioid analgesic, prescribe the lowest effective dosages and minimum durations of concomitant use. In patients already receiving an opioid analgesic, prescribe a lower initial dose of the benzodiazepine or other CNS depressant than indicated in the absence of an opioid, and titrate based on clinical response. If an opioid analgesic is initiated in a patient already taking a benzodiazepine or other CNS depressant, prescribe a lower initial dose of the opioid analgesic, and titrate based on clinical response. Follow patients closely for signs and symptoms of respiratory depression and sedation. Advise both patients and caregivers about the risks of respiratory depression and sedation when Hydromorphone Hydrochloride Injection is used with benzodiazepines or other CNS depressants (including alcohol and illicit drugs). Advise patients not to drive or operate heavy machinery until the effects of concomitant use of the benzodiazepine or other CNS depressant have been determined. Screen patients for risk of substance use disorders, including opioid abuse and misuse, and warn them of the risk for overdose and death associated with the use of additional CNS depressants including alcohol and illicit drugs [see Drug Interactions (7) and Patient Counseling Information (17)]. |
||||||||
|
Life-Threatening Respiratory Depression in Patients with Chronic Pulmonary Disease or in Elderly, Cachectic, or Debilitated Patients |
Use in Patients with Chronic Pulmonary Disease: Monitor patients with significant chronic obstructive pulmonary disease or cor pulmonale, and patients having a substantially decreased respiratory reserve, hypoxia, hypercapnia, or preexisting respiratory depression for respiratory depression, particularly when initiating therapy and titrating with HYDROmorphone Hydrochloride Injection USP, as in these patients, even usual therapeutic doses of HYDROmorphone Hydrochloride Injection USP may decrease respiratory drive to the point of apnea. In these patients, use of alternative non-opioid analgesics should be considered, if possible. The use of HYDROmorphone Hydrochloride Injection USP is contraindicated in Patients with acute or severe bronchial asthma, chronic obstructive airway, or status asthmaticus (see CONTRAINDICATIONS). |
|||||||
|
The use of Hydromorphone Hydrochloride Injection in patients with acute or severe bronchial asthma in an unmonitored setting or in the absence of resuscitative equipment is contraindicated. Patients with Chronic Pulmonary Disease: Hydromorphone Hydrochloride Injection-treated patients with significant chronic obstructive pulmonary disease or cor pulmonale, and those with a substantially decreased respiratory reserve, hypoxia, hypercapnia, or pre-existing respiratory depression are at increased risk of decreased respiratory drive including apnea, even at recommended dosages of hydromorphone hydrochloride [see Warnings and Precautions (5.2)]. Elderly, Cachectic, or Debilitated Patients: Life-threatening respiratory depression is more likely to occur in elderly, cachectic, or debilitated patients because they may have altered pharmacokinetics or altered clearance compared to younger, healthier patients [see Warnings and Precautions (5.2)]. Monitor such patients closely, particularly when initiating and titrating Hydromorphone Hydrochloride Injection and when Hydromorphone Hydrochloride Injection is given concomitantly with other drugs that depress respiration [see Warnings and Precautions (5.2)]. Alternatively, consider the use of non-opioid analgesics in these patients. |
||||||||
|
|
||||||||
|
Cases of adrenal insufficiency have been reported with opioid use, more often following greater than one month of use. Presentation of adrenal insufficiency may include non-specific symptoms and signs including nausea, vomiting, anorexia, fatigue, weakness, dizziness, and low blood pressure. If adrenal insufficiency is suspected, confirm the diagnosis with diagnostic testing as soon as possible. If adrenal insufficiency is diagnosed, treat with physiologic replacement doses of corticosteroids. Wean the patient off of the opioid to allow adrenal function to recover and continue corticosteroid treatment until adrenal function recovers. Other opioids may be tried as some cases reported use of a different opioid without recurrence of adrenal insufficiency. The information available does not identify any particular opioids as being more likely to be associated with adrenal insufficiency. |
||||||||
|
|
||||||||
|
Hydromorphone Hydrochloride Injection may cause severe hypotension including orthostatic hypotension and syncope in ambulatory patients. There is increased risk in patients whose ability to maintain blood pressure has already been compromised by a reduced blood volume or concurrent administration of certain CNS depressant drugs (e.g. phenothiazines or general anesthetics) [see Drug Interactions (7)]. Monitor these patients for signs of hypotension after initiating or titrating the dosage of Hydromorphone Hydrochloride Injection. In patients with circulatory shock, Hydromorphone Hydrochloride Injection may cause vasodilation that can further reduce cardiac output and blood pressure. Avoid the use of Hydromorphone Hydrochloride Injection in patients with circulatory shock. |
||||||||
|
Risks of Use in Patients with Increased Intracranial Pressure, Brain Tumors, Head Injury, or Impaired Consciousness |
Head Injury: The respiratory depressant effects of HYDROmorphone, and the capacity to elevate cerebrospinal fluid pressure, may be greatly increased in the presence of an already elevated intracranial pressure produced by trauma. Also, HYDROmorphone may produce confusion, miosis, vomiting and other side effects which obscure the clinical course of patients with head injury. In such patients, HYDROmorphone must be used with extreme caution and only if it is judged essential (see CONTRAINDICATIONS). |
|||||||
|
In patients who may be susceptible to the intracranial effects of CO2 retention (e.g., those with evidence of increased intracranial pressure or brain tumors), Hydromorphone Hydrochloride Injection may reduce respiratory drive, and the resultant CO2 retention can further increase intracranial pressure. Monitor such patients for signs of sedation and respiratory depression, particularly when initiating therapy with Hydromorphone Hydrochloride Injection. Opioids may also obscure the clinical course in a patient with a head injury. Avoid the use of Hydromorphone Hydrochloride Injection in patients with impaired consciousness or coma. |
||||||||
|
|
Gastrointestinal Tract and Other Smooth Muscle:
|
|||||||
|
Hydromorphone Hydrochloride Injection is contraindicated in patients with known or suspected gastrointestinal obstruction, including paralytic ileus. The hydromorphone in Hydromorphone Hydrochloride Injection may cause spasm of the sphincter of Oddi. Opioids may cause increases in serum amylase. Monitor patients with biliary tract disease, including acute pancreatitis, for worsening symptoms. |
||||||||
|
Increased Risk of Seizures in Patients with Seizure Disorders |
||||||||
|
The hydromorphone in Hydromorphone Hydrochloride Injection may increase the frequency of seizures in patients with seizure disorders, and may increase the risk of seizures occurring in other clinical settings associated with seizures. Monitor patients with a history of seizure disorders for worsened seizure control during Hydromorphone Hydrochloride Injection therapy. |
||||||||
|
|
||||||||
|
Avoid the use of mixed agonist/antagonist (e.g, pentazocine, nalbuphine, and butorphanol) or partial agonist (e.g., buprenorphine) analgesics in patients who are receiving a full opioid agonist analgesic, including Hydromorphone Hydrochloride Injection. In these patients, mixed agonist/antagonist and partial agonist analgesics may reduce the analgesic effect and/or precipitate withdrawal symptoms [see Drug Interactions (7)]. When discontinuing Hydromorphone Hydrochloride Injection, in a physically-dependent patient, gradually taper the dosage [see Dosage and Administration (2.6)]. Do not abruptly discontinue Hydromorphone Hydrochloride Injection in these patients [see Drug Abuse and Dependence (9.3)]. |
||||||||
|
|
Psychomotor Impairment
|
|||||||
|
Hydromorphone Hydrochloride Injection may impair the mental or physical abilities needed to perform potentially hazardous activities such as driving a car or operating machinery. Warn patients not to drive or operate dangerous machinery unless they are tolerant to the effects of Hydromorphone Hydrochloride Injection and know how they will react to the medication. |
||||||||
|
Respiratory |
||||||||
|
Increased Risk of Hypotension and Respiratory Depression with Rapid Intravenous Administration |
Respiratory Depression: While serious, life-threatening, or fatal respiratory depression can occur at any time during the use of HYDROmorphone Hydrochloride Injection USP, the risk is greatest during the initiation of therapy or following a dose increase. Patients should be closely monitored for respiratory depression when initiating therapy with HYDROmorphone Hydrochloride Injection USP and following dose increases. |
|||||||
|
Hydromorphone Hydrochloride Injection may be given intravenously, but the injection should be given very slowly. Rapid intravenous injection of opioid analgesics increases the possibility of side effects such as hypotension and respiratory depression [see Dosage and Administration (2.1)]. |
||||||||
|
Adverse Drug Reaction Overview
The most frequently observed adverse effects are constipation, light-headedness, dizziness, sedation, nausea, vomiting, and sweating. Pain at injection site, local tissue irritation and induration following subcutaneous injection, particularly when repeated in the same area, have occurred. |
||||||||
|
The following serious adverse reactions are described, or described in greater detail, in other sections:
The following adverse reactions associated with the use of hydromorphone were identified in clinical studies or postmarketing reports. Because some of these reactions were reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. The most common adverse effects are light-headedness, dizziness, sedation, nausea, vomiting, sweating, flushing, dysphoria, euphoria, dry mouth, and pruritus. These effects seem to be more prominent in ambulatory patients and in those not experiencing severe pain. Less Frequently Observed Adverse Reactions |
||||||||
|
Cardiac disorders: tachycardia, bradycardia, palpitations |
Cardiovascular: Bradycardia, chills, faintness, flushing of the face, hypertension, hypotension, palpitation, syncope, and tachycardia have been reported. |
|||||||
|
Eye disorders: vision blurred, diplopia, miosis, visual impairment | ||||||||
|
Gastrointestinal disorders: constipation, ileus, diarrhea, abdominal pain |
Gastrointestinal: Abdominal pain, anorexia, biliary colic, biliary tract spasm, cramps, diarrhea, dry mouth, hepatic enzymes increased, ileus and taste alterations have been reported. |
|||||||
|
General disorders and administration site conditions: weakness, feeling abnormal, chills, injection site urticaria Hepatobiliary disorders: biliary colic Metabolism and nutrition disorders: decreased appetite Musculoskeletal and connective tissue disorders: muscle rigidity Nervous system disorders: headache, tremor, paraesthesia, nystagmus, increased intracranial pressure, syncope, taste alteration, involuntary muscle contractions, presyncope Psychiatric disorders: agitation, mood altered, nervousness, anxiety, depression, hallucination, disorientation, insomnia, abnormal dreams Renal and urinary disorders: urinary retention, urinary hesitation, antidiuretic effects Respiratory, thoracic and mediastinal disorders: bronchospasm, laryngospasm Skin and subcutaneous tissue disorders: injection site pain, urticaria, rash, hyperhidrosis Vascular disorders: flushing, hypotension, hypertension Serotonin syndrome: Cases of serotonin syndrome, a potentially life-threatening condition, have been reported during concomitant use of opioids with serotonergic drugs. Adrenal insufficiency: Cases of adrenal insufficiency have been reported with opioid use, more often following greater than one month of use. Anaphylaxis: Anaphylaxis has been reported with ingredients contained in Hydromorphone Hydrochloride Injection. Androgen deficiency: Cases of androgen deficiency have occurred with chronic use of opioids. |
Sedation: Sedation is a common side effect of opioid analgesics, especially in opioid naïve individuals. Sedation may also occur partly because patients often recuperate from prolonged fatigue after the relief of persistent pain. Most patients develop tolerance to the sedative effects of opioids within three to five days and, if the sedation is not severe, will not require any treatment except reassurance. If excessive sedation persists beyond a few days, the dose of the opioid should be reduced and alternate causes investigated. Some of these are: concurrent CNS depressant medication, hepatic or renal dysfunction, brain metastases, hypercalcemia and respiratory failure. If it is necessary to reduce the dose, it can be carefully increased again after three or four days if it is obvious that the pain is not being well controlled. Dizziness and unsteadiness may be caused by postural hypotension particularly in elderly or debilitated patients and may be alleviated if the patient lies down. Nausea and Vomiting: Nausea is a common side effect on initiation of therapy with opioid analgesics and is thought to occur by activation of the chemoreceptor trigger zone, stimulation of the vestibular apparatus and through delayed gastric emptying. The prevalence of nausea declines following continued treatment with opioid analgesics. When instituting prolonged therapy with an opioid for chronic pain, the routine prescription of an antiemetic should be considered. In the cancer patient, investigation of nausea should include such causes as constipation, bowel obstruction, uremia, hypercalcemia, hepatomegaly, tumor invasion of celiac plexus and concurrent use of drugs with emetogenic properties. Persistent nausea which does not respond to dosage reduction may be caused by opioid-induced gastric stasis and may be accompanied by other symptoms including anorexia, early satiety, vomiting and abdominal fullness. These symptoms respond to chronic treatment with gastrointestinal prokinetic agents. Constipation: Practically all patients become constipated while taking opioids on a persistent basis. In some patients, particularly the elderly or bedridden, fecal impaction may result. It is essential to caution the patients in this regard and to institute an appropriate regimen of bowel management at the start of prolonged opioid analgesic therapy. Stool softeners, stimulant laxatives and other appropriate measures should be used as required. As fecal impaction may present as overflow diarrhea, the presence of constipation should be excluded in patients on opioid therapy prior to initiating treatment for diarrhea. The following adverse effects occur less frequently with opioid analgesics and include those reported in HYDROmorphone Hydrochloride Injection USP clinical trials, whether related or not to HYDROmorphone. Dermatologic: Diaphoresis, other skin rashes, pruritus, urticaria and wheal and flare over the vein with intravenous injection have been reported with opioid analgesics. General and CNS: Agitation, anxiety, apprehension, asthenic conditions, blurred vision, confusion, convulsions, depression, diplopia, disorientation, drug dependence, drug tolerance, drug withdrawal syndrome, dyskinesia, dysphoria, euphoria, hallucinations, headache, hyperalgesia, increased intracranial pressure, insomnia, miosis, muscle rigidity, muscle tremor, nightmares, nystagmus, other alterations of mood (nervousness, floating feelings, dreams), paresthesia, peripheral edema, somnolence, tremor, uncoordinated muscle movements, visual disturbances and weakness may occur.
Genitourinary: Antidiuretic effects, hesitancy and urinary retention have been reported.
Post-Marketing Experience
|
|||||||
|
Drug Interactions |
||||||||
|
|
Overview
|
|||||||
|
Benzodiazepines and other Central Nervous System (CNS) Depressants | ||||||||
|
Clinical Impact: |
Due to additive pharmacologic effect, the concomitant use of CNS depressants, including alcohol, can increase the risk of hypotension, respiratory depression, profound sedation, coma, and death. | |||||||
|
Intervention: |
Reserve concomitant prescribing of these drugs for use in patients for whom alternative treatment options are inadequate. Limit dosages and durations to the minimum required. Follow patients closely for signs of respiratory depression and sedation [see Warnings and Precautions (5.4)]. | |||||||
|
Examples: |
Benzodiazepines and other sedatives/hypnotics, anxiolytics, tranquilizers, muscle relaxants, general anesthetics, antipsychotics, other opioids, alcohol. | |||||||
|
Serotonergic Drugs | ||||||||
|
Clinical Impact: |
The concomitant use of opioids with other drugs that affect the serotonergic neurotransmitter system has resulted in serotonin syndrome. |
Serotonergic Agents: Coadministration of HYDROmorphone with a serotonergic agent, such as a Selective Serotonin Re-uptake Inhibitor or a Serotonin Norepinephrine Re-uptake Inhibitor, may increase the risk of serotonin syndrome, a potentially life-threatening condition (see WARNINGS AND PRECAUTIONS, Neurologic). |
||||||
|
Intervention: |
If concomitant use is warranted, carefully observe the patient, particularly during treatment initiation and dose adjustment. Discontinue Hydromorphone Hydrochloride Injection if serotonin syndrome is suspected. | |||||||
|
Examples: |
Selective serotonin reuptake inhibitors (SSRIs), serotonin and norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), triptans, 5-HT3 receptor antagonists, drugs that effect the serotonin neurotransmitter system (e.g., mirtazapine, trazodone, tramadol), monoamine oxidase (MAO) inhibitors (those intended to treat psychiatric disorders and also others, such as linezolid and intravenous methylene blue). | |||||||
|
Monoamine Oxidase Inhibitors (MAOIs) | ||||||||
|
Clinical Impact: |
MAOI interactions with opioids may manifest as serotonin syndrome or opioid toxicity (e.g., respiratory depression, coma) [see Warnings and Precautions (5.4)]. If urgent use of an opioid is necessary, use test doses and frequent titration of small doses to treat pain while closely monitoring blood pressure and signs and symptoms of CNS and respiratory depression. | |||||||
|
Intervention: |
The use of Hydromorphone Hydrochloride Injection is not recommended for patients taking MAOIs or within 14 days of stopping such treatment. | |||||||
|
Examples: |
phenelzine, tranylcypromine, linezolid | |||||||
|
Mixed Agonist/Antagonist and Partial Agonist Opioid Analgesics |
Drug-Drug Interactions Administration with Mixed Activity Agonist/Antagonist Opioids: Mixed agonist/antagonist opioid analgesics (i.e., pentazocine, nalbuphine, butorphanol, and buprenorphine) should be administered with caution to a patient who has received or is receiving a course of therapy with a pure opioid agonist analgesic such as HYDROmorphone. In this situation, mixed agonist/antagonist analgesics may reduce the analgesic effect of HYDROmorphone and/or may precipitate withdrawal symptoms in these patients. MAO Inhibitors: MAO Inhibitors intensify the effects of opioid drugs which can cause anxiety, confusion and decreased respiration. HYDROmorphone Hydrochloride Injection USP is contraindicated in patients receiving MAO inhibitors or who have used them within the previous 14 days (see CONTRAINDICATIONS).
Drug-Herb Interactions
Drug-Laboratory Interactions
Drug-Lifestyle Interactions
|
|||||||
|
Clinical Impact: | May reduce the analgesic effect of Hydromorphone Hydrochloride Injection and/or precipitate withdrawal symptoms. | |||||||
|
Intervention: |
Avoid concomitant use. | |||||||
|
Examples: |
butorphanol, nalbuphine, pentazocine, buprenorphine, | |||||||
|
Muscle Relaxants | ||||||||
|
Clinical Impact: |
Hydromorphone may enhance the neuromuscular blocking action of skeletal muscle relaxants and produce an increased degree of respiratory depression. | |||||||
|
Intervention: |
Monitor patients for signs of respiratory depression that may be greater than otherwise expected and decrease the dosage of Hydromorphone Hydrochloride Injection and/or the muscle relaxant as necessary. | |||||||
|
Diuretics | ||||||||
|
Clinical Impact: |
Opioids can reduce the efficacy of diuretics by inducing the release of antidiuretic hormone. | |||||||
|
Intervention: |
Monitor patients for signs of diminished diuresis and/or effects on blood pressure and increase the dosage of the diuretic as needed. | |||||||
|
Anticholinergic Drugs | ||||||||
|
Clinical Impact: |
The concomitant use of anticholinergic drugs may increase risk of urinary retention and/or severe constipation, which may lead to paralytic ileus. | |||||||
|
Intervention: |
Monitor patients for signs of urinary retention or reduced gastric motility when Hydromorphone Hydrochloride Injection is used concomitantly with anticholinergic drugs. | |||||||
|
Special Populations |
||||||||
|
Risk Summary Prolonged use of opioid analgesics during pregnancy may cause neonatal opioid withdrawal syndrome [see Warnings and Precautions (5.3)]. There are no available data with Hydromorphone Hydrochloride Injection in pregnant women to inform a drug-associated risk for major birth defects and miscarriage. In published animal reproduction studies, neural tube defects were noted following subcutaneous injection of hydromorphone to pregnant hamsters at doses 6.4 times the HDD and soft tissue and skeletal abnormalities were noted following subcutaneous continuous infusion of 3 times the HDD to pregnant mice. No malformations were noted at 4 or 40.5 times the HDD in pregnant rats or rabbits, respectively [see Data]. Based on animal data, advise pregnant women of the potential risk to a fetus. The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2–4% and 15–20%, respectively. Clinical Considerations Fetal/Neonatal Adverse Reactions Prolonged use of opioid analgesics during pregnancy for medical or nonmedical purposes can result in physical dependence in the neonate and neonatal opioid withdrawal syndrome shortly after birth. Neonatal opioid withdrawal syndrome presents as irritability, hyperactivity and abnormal sleep pattern, high pitched cry, tremor, vomiting, diarrhea, and failure to gain weight. The onset, duration, and severity of neonatal opioid withdrawal syndrome vary based on the specific opioid used, duration of use, timing and amount of last maternal use, and rate of elimination of the drug by the newborn. Observe newborns for symptoms of neonatal opioid withdrawal syndrome and manage accordingly [see Warnings and Precautions (5.3)]. |
Pregnant Women:
|
|||||||
|
Labor or Delivery | ||||||||
|
Opioids cross the placenta and may produce respiratory depression and psycho-physiologic effects in neonates. An opioid antagonist, such as naloxone, must be available for reversal of opioid-induced respiratory depression in the neonate. Hydromorphone Hydrochloride Injection is not recommended for use in pregnant women during or immediately prior to labor, when other analgesic techniques are more appropriate. Opioid analgesics, including Hydromorphone Hydrochloride Injection, can prolong labor through actions which temporarily reduce the strength, duration, and frequency of uterine contractions. However, this effect is not consistent and may be offset by an increased rate of cervical dilation, which tends to shorten labor. Monitor neonates exposed to opioid analgesics during labor for signs of excess sedation and respiratory depression. Animal Data No effects on teratogenicity or embryotoxicity were observed in pregnant rats given oral doses up to 7 mg/kg/day which is 3-fold higher than the human dose of 24 mg Hydromorphone Hydrochloride Injection (4 mg every 4 hours), on a body surface area basis. In a published study, neural tube defects (exencephaly and cranioschisis) were noted following subcutaneous administration of hydromorphone hydrochloride (19 to 258 mg/kg) on Gestation Day 8 to pregnant hamsters (6.4 to 87.2 times the HDD of 24 mg/day based on body surface area). The findings cannot be clearly attributed to maternal toxicity. No neural tube defects were noted at 14 mg/kg (4.7 times the human daily dose of 24 mg/day). In a published study, CF-1 mice were treated subcutaneously with continuous infusion of 7.5, 15, or 30 mg/kg/day hydromorphone hydrochloride (1.5, 3, or 6.1 times the human daily dose of 24 mg based on body surface area) via implanted osmotic pumps during organogenesis (Gestation Days 7 to 10). Soft tissue malformations (cryptorchidism, cleft palate, malformed ventricles and retina), and skeletal variations (split supraoccipital, checkerboard and split sternebrae, delayed ossification of the paws and ectopic ossification sites) were observed at doses 3 times the human dose of 24 mg/day based on body surface area. The findings cannot be clearly attributed to maternal toxicity. Risk Summary Low levels of opioid analgesics have been detected in human milk. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for Hydromorphone Hydrochloride Injection and any potential adverse effects on the breastfed infant from Hydromorphone Hydrochloride Injection or from the underlying maternal condition. Clinical Considerations Monitor infants exposed to Hydromorphone Hydrochloride Injection through breast milk for excess sedation and respiratory depression. Withdrawal symptoms can occur in breastfed infants when maternal administration of hydromorphoneis stopped, or when breast-feeding is stopped. Females and Males of Reproductive Potential Infertility Chronic use of opioids may cause reduced fertility in females and males of reproductive potential. It is not known whether these effects on fertility are reversible [see Adverse Reactions (6), Clinical Pharmacology (12.2)]. |
Labour, Delivery and Nursing Women:
|
|||||||
|
Pediatric Use The safety and effectiveness of Hydromorphone Hydrochloride Injection in pediatric patients has not been established. |
Pediatrics (< 18 years of age):
|
|||||||
|
Geriatric Use Elderly patients (aged 65 years or older) may have increased sensitivity to hydromorphone. In general, use caution when selecting a dosage for an elderly patient, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function and of concomitant disease or other drug therapy. Respiratory depression is the chief risk for elderly patients treated with opioids, and has occurred after large initial doses were administered to patients who were not opioid-tolerant or when opioids were co-administered with other agents that depress respiration. Titrate the dosage of Hydromorphone Hydrochloride Injection slowly in geriatric patients and monitor closely for signs of central nervous system and respiratory depression [see Warnings and Precautions (5.5)]. Hydromorphone is known to be substantially excreted by the kidney, and the risk of adverse reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function. |
Geriatrics (> 65 years of age):
|
|||||||
|
The pharmacokinetics of hydromorphone are affected by hepatic impairment. Due to increased exposure of hydromorphone, patients with moderate hepatic impairment should be started at one fourth to one half the recommended starting dose depending on the degree of hepatic dysfunction and closely monitored during dose titration. The pharmacokinetics of hydromorphone in patients with severe hepatic impairment has not been studied. A further increase in Cmax and AUC of hydromorphone in this group is expected and should be taken into consideration when selecting a starting dose [see Clinical Pharmacology (12.3)]. |
Patients with Hepatic Impairment: Mean exposure to HYDROmorphone (Cmax and AUC∞) is increased 4-fold in patients with moderate (Child-Pugh Group B) hepatic impairment compared with subjects with normal hepatic function. The pharmacokinetics of HYDROmorphone in patients with severe hepatic impairment has not been studied. A further increase in Cmax and AUC of HYDROmorphone in this group is expected and should be taken into consideration when selecting a starting dose. |
|||||||
|
The pharmacokinetics of hydromorphone are affected by renal impairment. In addition, in patients with severe renal impairment, hydromorphone appeared to be more slowly eliminated with a longer terminal elimination half-life. Start patients with renal impairment on one-fourth to one-half the usual starting dose depending on the degree of impairment. Patients with renal impairment should be closely monitored during dose titration. [see Clinical Pharmacology (12.3)] |
Patients with Renal Impairment: Mean exposure to HYDROmorphone (Cmax and AUC 0–∝ ) is increased by 2-fold in patients with moderate (CLcr =40 – 60 mL/min) renal impairment and increased by 4-fold in patients with severe (CLcr < 30 mL/min) renal impairment compared with normal subjects (CLcr > 80 mL/min). In addition, in patients with severe renal impairment, HYDROmorphone appeared to be more slowly eliminated with a longer terminal elimination half-life (40 hr) compared to patients with normal renal function (15 hr). Patients with renal impairment should be closely monitored during dose titration. Special Populations
Special Risk Groups: HYDROmorphone should be administered with caution to patients with a history of alcohol and drug abuse and in a reduced dosage to debilitated patients, and in patients with severely impaired pulmonary function, Addison's disease, hypothyroidism, myxedema, toxic psychosis, prostatic hypertrophy or urethral stricture. |
|||||||
|
Hydromorphone Hydrochloride Injection contains hydromorphone, a Schedule II controlled substance. Hydromorphone Hydrochloride Injection contains hydromorphone, a substance with a high potential for abuse similar to other opioids including fentanyl, hydrocodone, methadone, morphine, oxycodone, oxymorphone, and tapentadol. Hydromorphone Hydrochloride Injection can be abused and is subject to misuse, addiction, and criminal diversion [see Warnings and Precautions (5.1)]. All patients treated with opioids require careful monitoring for signs of abuse and addiction, because use of opioid analgesic products carries the risk of addiction even under appropriate medical use. Prescription drug abuse is the intentional non-therapeutic use of a prescription drug, even once, for its rewarding psychological or physiological effects. Drug addiction is a cluster of behavioral, cognitive, and physiological phenomena that develop after repeated substance use and includes: a strong desire to take the drug, difficulties in controlling its use, persisting in its use despite harmful consequences, a higher priority given to drug use than to other activities and obligations, increased tolerance, and sometimes a physical withdrawal. "Drug-seeking" behavior is very common in persons with substance use disorders. Drug-seeking tactics include emergency calls or visits near the end of office hours, refusal to undergo appropriate examination, testing, or referral, repeated "loss" of prescriptions, tampering with prescriptions and reluctance to provide prior medical records or contact information for other treating health care provider(s). "Doctor shopping" (visiting multiple prescribers to obtain additional prescriptions) is common among drug abusers and people suffering from untreated addiction. Preoccupation with achieving adequate pain relief can be appropriate behavior in a patient with poor pain control. Abuse and addiction are separate and distinct from physical dependence and tolerance. Health care providers should be aware that addiction may not be accompanied by concurrent tolerance and symptoms of physical dependence in all addicts. In addition, abuse of opioids can occur in the absence of true addiction. Hydromorphone Hydrochloride Injection, like other opioids, can be diverted for non-medical use into illicit channels of distribution. Careful record-keeping of prescribing information, including quantity, frequency, and renewal requests, as required by state and federal law, is strongly advised. Proper assessment of the patient, proper prescribing practices, periodic re-evaluation of therapy, and proper dispensing and storage are appropriate measures that help to limit abuse of opioid drugs. Risks Specific to Abuse of Hydromorphone Hydrochloride Injection Abuse of Hydromorphone Hydrochloride Injection poses a risk of overdose and death. The risk is increased with concurrent use of Hydromorphone Hydrochloride Injection with alcohol and other central nervous system depressants. Parenteral drug abuse is commonly associated with transmission of infectious diseases such as hepatitis and HIV. | ||||||||
|
Both tolerance and physical dependence can develop during chronic opioid therapy. Tolerance is the need for increasing doses of opioids to maintain a defined effect such as analgesia (in the absence of disease progression or other external factors). Tolerance may occur to both the desired and undesired effects of drugs, and may develop at different rates for different effects. Physical dependence results in withdrawal symptoms after abrupt discontinuation or a significant dosage reduction of a drug. Withdrawal also may be precipitated through the administration of drugs with opioid antagonist activity (e.g., naloxone, nalmefene), mixed agonist/antagonist analgesics (e.g., pentazocine, butorphanol, nalbuphine), or partial agonists (e.g., buprenorphine). Physical dependence may not occur to a clinically significant degree until after several days to weeks of continued opioid usage. Hydromorphone Hydrochloride Injection should not be abruptly discontinued in a physically-dependent patient [see Dosage and Administration (2.6)]. If Hydromorphone Hydrochloride Injection is abruptly discontinued in a physically-dependent patient, a withdrawal syndrome may occur. Some or all of the following can characterize this syndrome: restlessness, lacrimation, rhinorrhea, yawning, perspiration, chills, myalgia, and mydriasis. Other signs and symptoms also may develop, including: irritability, anxiety, backache, joint pain, weakness, abdominal cramps, insomnia, nausea, anorexia, vomiting, diarrhea, or increased blood pressure, respiratory rate, or heart rate. Infants born to mothers physically dependent on opioids will also be physically dependent and may exhibit respiratory difficulties and withdrawal signs [see Use in Specific Populations (8.1)]. |
Dependence/Tolerance
Physical dependence and tolerance reflect the neuroadaptation of the opioid receptors to chronic exposure to an opioid, and are separate and distinct from abuse and addiction. Tolerance, as well as physical dependence, may develop upon repeated administration of opioids, and are not by themselves evidence of an addictive disorder or abuse. |
|||||||
|
OVERDOSAGE |
||||||||
|
Clinical Presentation Acute overdose with Hydromorphone Hydrochloride Injection can be manifested by respiratory depression, somnolence progressing to stupor or coma, skeletal muscle flaccidity, cold and clammy skin, constricted pupils, and, in some cases, pulmonary edema, bradycardia, hypotension, partial or complete airway obstruction, atypical snoring, and death. Marked mydriasis rather than miosis may be seen with hypoxia in overdose situations [see Clinical Pharmacology (12.2)]. |
For management of a suspected drug overdose, contact your Regional Poison Control Centre.
Symptoms
|
|||||||
|
Treatment of Overdose In case of overdose, priorities are the reestablishment of a patent and protected airway and institution of assisted or controlled ventilation, if needed. Employ other supportive measures (including oxygen and vasopressors) in the management of circulatory shock and pulmonary edema as indicated. Cardiac arrest or arrhythmias will require advanced life-support techniques. The opioid antagonists, naloxone or nalmefene, are specific antidotes to respiratory depression resulting from opioid overdose. For clinically significant respiratory or circulatory depression secondary to hydromorphone overdose, administer an opioid antagonist. Opioid antagonists should not be administered in the absence of clinically significant respiratory or circulatory depression secondary to hydromorphone overdose. Because the duration of opioid reversal is expected to be less than the duration of action of hydromorphone in Hydromorphone Hydrochloride Injection, carefully monitor the patient until spontaneous respiration is reliably reestablished. If the response to an opioid antagonist is suboptimal or only brief in nature, administer additional antagonist as directed by the product's prescribing information. In an individual physically dependent on opioids, administration of the recommended usual dosage of the antagonist will precipitate an acute withdrawal syndrome. The severity of the withdrawal symptoms experienced will depend on the degree of physical dependence and the dose of the antagonist administered. If a decision is made to treat serious respiratory depression in the physically dependent patient, administration of the antagonist should be initiated with care and by titration with smaller than usual doses of the antagonist. |
Treatment In the treatment of overdosage, primary attention should be given to the re-establishment of adequate respiratory exchange through provision of a patent airway and institution of assisted or controlled ventilation. It should be borne in mind that for individuals who are physically dependent on opioids and are receiving large doses of these drugs, the administration of the usual dose of opioid antagonist will precipitate an acute withdrawal syndrome. The severity will depend on the degree of physical dependence and the dose of the antagonist administered. Use of an opioid antagonist in such persons should be avoided. If necessary to treat serious respiratory depression in the physically dependent patient, the antagonist should be administered with extreme care and by titration, commencing with 10 to 20% of the usual recommended initial dose. |
|||||||
|
Description |
||||||||
|
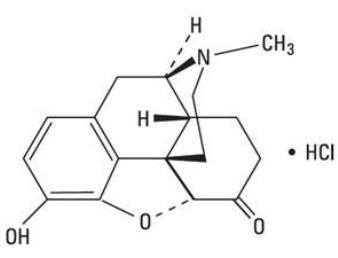
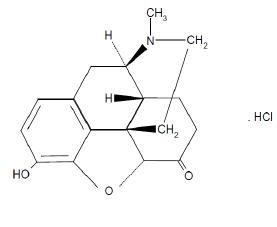
Hydromorphone Hydrochloride Injection is an opioid agonist, available as an aqueous sterile solution. Each 1 mL of sterile solution contains 1 mg, 2 mg, or 4 mg hydromorphone hydrochloride for use in intravenous, intramuscular and subcutaneous administration. Each 1 mL also contains 5.4 mg sodium lactate and sodium chloride for isotonicity. The chemical name of hydromorphone hydrochloride is 4,5α- epoxy-3-hydroxy-17-methylmorphinan-6-one hydrochloride. The molecular weight is 321.8 and it has the following chemical structure.
Hydromorphone hydrochloride is a white or almost white crystalline powder that is freely soluble in water, very slightly soluble in ethanol (96%), and practically insoluble in methylene chloride. The solution pH is adjusted with lactic acid or sodium hydroxide to between pH 3.5 and 5.5. |
Drug Substance
Chemical Name: (1) Morphinan-6-one,4,5-epoxy-3-hydroxy-17-methyl-, hydrochloride, (5α)-(2) 4,5α-Epoxy-3-hydroxy-17-methylmorphinan-6-one hydrochloride
Physicochemical
pH: A 1% aqueous solution of HYDROmorphone hydrochloride has a pH of 5.3. |
|||||||
|
Clinical Pharmacology |
||||||||
|
ACTION AND CLINICAL PHARMACOLOGY |
||||||||
|
Hydromorphone is a full opioid agonist and is relatively selective for the mμ-opioid receptor, although it can bind to other opioid receptors at higher doses. The principal therapeutic action of hydromorphone is analgesia. Like all full opioid agonists, there is no ceiling effect for analgesia with morphine. Clinically, dosage is titrated to provide adequate analgesia and may be limited by adverse reactions, including respiratory and CNS depression. The precise mechanism of the analgesic action is unknown. However, specific CNS opioid receptors for endogenous compounds with opioid-like activity have been identified throughout the brain and spinal cord and are thought to play a role in the analgesic effects of this drug. |
Mechanism of Action
|
|||||||
|
Effects on the Central Nervous System Hydromorphone produces respiratory depression by direct action on brain stem respiratory centers. The respiratory depression involves a reduction in the responsiveness of the brain stem respiratory centers to both increases in carbon dioxide tension and electrical stimulation. Hydromorphone causes miosis, even in total darkness. Pinpoint pupils are a sign of opioid overdose but are not pathognomonic (e.g., pontine lesions of hemorrhagic or ischemic origins may produce similar findings). Marked mydriasis rather than miosis may be seen due to hypoxia in overdose situations. |
Pharmacodynamics
Central Nervous System:
|
|||||||
|
Effects on the Gastrointestinal Tract and Other Smooth Muscle Hydromorphone causes a reduction in motility associated with an increase in smooth muscle tone in the antrum of the stomach and duodenum. Digestion of food in the small intestine is delayed and propulsive contractions are decreased. Propulsive peristaltic waves in the colon are decreased, while tone may be increased to the point of spasm resulting in constipation. Other opioid-induced effects may include a reduction in biliary and pancreatic secretions, spasm of sphincter of Oddi, and transient elevations in serum amylase. |
Gastrointestinal Tract and Other Smooth Muscle:
|
|||||||
|
Effects on the Cardiovascular System Hydromorphone produces peripheral vasodilation which may result in orthostatic hypotension or syncope. Manifestations of histamine release and/or peripheral vasodilation may include pruritus, flushing, red eyes and sweating and/or orthostatic hypotension. |
Cardiovascular System:
Cardiovascular
Rapid intravenous injection of opioid analgesics increases the possibility of hypotension and respiratory depression and should be avoided (see DOSAGE AND ADMINISTRATION). |
|||||||
|
Effects on the Endocrine System Opioids inhibit the secretion of adrenocorticotropic hormone (ACTH), cortisol, and luteinizing hormone (LH) in humans [see Adverse Reactions (6)]. They also stimulate prolactin, growth hormone (GH) secretion, and pancreatic secretion of insulin and glucagon [see Adverse Reactions (6)]. Chronic use of opioids may influence the hypothalamic-pituitary-gonadal axis, leading to androgen deficiency that may manifest as low libido, impotence, erectile dysfunction, amenorrhea, or infertility. The causal role of opioids in the clinical syndrome of hypogonadism is unknown because the various medical, physical, lifestyle, and psychological stressors that may influence gonadal hormone levels have not been adequately controlled for in studies conducted to date [see Adverse Reactions (6)]. |
Endocrine System:
Endocrine
|
|||||||
|
Effects on the Immune System Opioids have been shown to have a variety of effects on components of the immune system in in vitro and animal models. The clinical significance of these findings is unknown. Overall, the effects of opioids appear to be modestly immunosuppressive. Concentration–Efficacy Relationships The minimum effective analgesic concentration will vary widely among patients, especially among patients who have been previously treated with potent agonist opioids. The minimum effective analgesic concentration of hydromorphone for any individual patient may increase over time due to an increase in pain, the development of a new pain syndrome and/or the development of analgesic tolerance [see Dosage and Administration (2.1)]. Concentration–Adverse Reaction Relationships There is a relationship between increasing hydromorphone plasma concentration and increasing frequency of dose-related opioid adverse reactions such as nausea, vomiting, CNS effects, and respiratory depression. In opioid-tolerant patients, the situation may be altered by the development of tolerance to opioid-related adverse reactions [see Dosage and Administration (2.1, 2.2)]. |
Immune System:
|
|||||||
|
Distribution At therapeutic plasma levels, hydromorphone is approximately 8–19% bound to plasma proteins. After an intravenous bolus dose, the steady state of volume of distribution [mean (%cv)] is 302.9 (32%) liters. Elimination The systemic clearance is approximately 1.96 (20%) liters/minute. The terminal elimination half-life of hydromorphone after an intravenous dose is about 2.3 hours. Metabolism Hydromorphone is extensively metabolized via glucuronidation in the liver, with greater than 95% of the dose metabolized to hydromorphone-3-glucuronide along with minor amounts of 6-hydroxy reduction metabolites. Excretion Only a small amount of the hydromorphone dose is excreted unchanged in the urine. Most of the dose is excreted as hydromorphone-3-glucuronide along with minor amounts of 6-hydroxy reduction metabolites. |
Pharmacokinetics
|
|||||||
|
Specific Populations Hepatic Impairment After oral administration of hydromorphone at a single 4 mg dose (2 mg hydromorphone immediate-release tablets), mean exposure to hydromorphone (Cmax and AUC∞) is increased 4 fold in patients with moderate (Child-Pugh Group B) hepatic impairment compared with subjects with normal hepatic function. Patients with moderate hepatic impairment should be started at one fourth to one half the recommended starting dose and closely monitored during dose titration. The pharmacokinetics of hydromorphone in patients with severe hepatic impairment has not been studied. A further increase in Cmax and AUC of hydromorphone in this group is expected and should be taken into consideration when selecting a starting dose [see Use in Specific Populations (8.6)]. Renal Impairment The pharmacokinetics of hydromorphone following an oral administration of hydromorphone at a single 4 mg dose (2 mg hydromorphone immediate-release tablets) are affected by renal impairment. Mean exposure to hydromorphone (Cmax and AUC0–∞) is increased by 2 fold in patients with moderate (CLcr = 40 – 60 mL/min) renal impairment and increased by 4 fold in patients with severe (CLcr < 30 mL/min) renal impairment compared with normal subjects (CLcr > 80 mL/min). In addition, in patients with severe renal impairment, hydromorphone appeared to be more slowly eliminated with a longer terminal elimination half-life (40 hr) compared to patients with normal renal function (15 hr). Start patients with renal impairment on one-fourth to one-half the usual starting dose depending on the degree of impairment. Patients with renal impairment should be closely monitored during dose titration [see Use in Specific Populations (8.7)]. Age: Geriatric Population In the geriatric population, age has no effect on the pharmacokinetics of hydromorphone. Sex Sex has little effect on the pharmacokinetics of hydromorphone. Females appear to have a higher Cmax (25%) than males with comparable AUC0–24 values. The difference observed in Cmax may not be clinically relevant. |
Special Population and Conditions Pediatrics: Individuals under 18 years of age should not take HYDROmorphone Hydrochloride Injection USP. |
|||||||
|
Nonclinical Toxicology |
||||||||
|
Carcinogenesis, Mutagenesis, Impairment of Fertility Carcinogenesis Long-term studies in animals to evaluate the carcinogenic potential of hydromorphone have not been conducted. Mutagenesis Hydromorphone was not mutagenic in the in vitro bacterial reverse mutation assay (Ames assay). Hydromorphone was not clastogenic in either the in vitro human lymphocyte chromosome aberration assay or the in vivo mouse micronucleus assay. Impairment of Fertility No effects on fertility, reproductive performance, or reproductive organ morphology were observed in male or female rats given oral doses up to 7 mg/kg/day which is 2.8 times the human dose of 24 mg hydromorphone hydrochloride injection (4 mg every 4 hours), on a body surface area basis. | ||||||||
|
How Supplied/Storage and Handling |
||||||||
|
Safety and Handling Instructions Access to drugs with a potential for abuse such as Hydromorphone Hydrochloride Injection presents an occupational hazard for addiction in the health care industry. Routine procedures for handling controlled substances developed to protect the public may not be adequate to protect health care workers. Implementation of more effective accounting procedures and measures to restrict access to drugs of this class (appropriate to the practice setting) may minimize the risk of self-administration by health care providers. Carpuject™ Single-use cartridges with Luer Lock are packaged in a Slim-Pak™ tamper detection package. Note that a needle is not included. |
STORAGE AND STABILITY
SPECIAL HANDLING INSTRUCTIONS
|
|||||||
|
PROTECT FROM LIGHT Keep covered in carton until time of use. Store at 20° to 25°C (68° to 77°F); excursions permitted to 15° to 30°C (59° to 86°F) [See USP Controlled Room Temperature]. |
Sterile Solution for Injection: Store HYDROmorphone Hydrochloride Injection USP sterile solution for injection at 15° to 30°C. Protect from light. Discard unused portion. |
|||||||
|
Serotonin Syndrome Inform patients that opioids could cause a rare but potentially life-threatening condition resulting from concomitant administration of serotonergic drugs. Warn patients of the symptoms of serotonin syndrome and to seek medical attention right away if symptoms develop. Instruct patients to inform their physicians if they are taking, or plan to take serotonergic medications. [see Drug Interactions 7]. |
Serotonin Syndrome: HYDROmorphone Hydrochloride Injection USP could cause a rare but potentially life-threatening condition resulting from concomitant administration of serotonergic drugs (e.g. anti-depressants, migraine medications). Treatment with the serotonergic drug should be discontinued if such events (characterized by clusters of symptoms such as hyperthermia, rigidity, myoclonus, autonomic instability with possible rapid fluctuations of vital signs, mental status changes including confusion, irritability, extreme agitation progressing to delirium and coma) occur and supportive symptomatic treatment should be initiated. HYDROmorphone Hydrochloride Injection USP should not be used in combination with MAO inhibitors or serotonin-precursors (such as L-tryptophan, oxitriptan) and should be used with caution in combination with other serotonergic drugs (triptans, certain tricyclic antidepressants, lithium, tramadol, St. John's Wort) due to the risk of serotonergic syndrome (see DRUG INTERACTIONS). |
|||||||
|
Constipation Advise patients of the potential for severe constipation, including management instructions and when to seek medical attention [see Adverse Reactions (6)]. |
Gastrointestinal Tract and Other Smooth Muscle:
Patient Counselling Information
|
|||||||
|
Revision Date |
||||||||
|
December 2016 |
April 10, 2017 |
|||||||
|
Barcode |
||||||||
|
A unit of use barcode is on individual units. |
Barcode use by HYDROmorphone Hydrochloride Injection USP (HYDROmorphone hydrochloride) 2 mg/mL Sterile Solution for Injection may not register accurately in the United States scanning systems. Alternate procedures should be followed to assure that the correct drug product is being used and administered to individual patients. |
|||||||
|
Additional information |
||||||||
|
Instructions for Use of the Syringe Systems Instructions for using the Carpuject™ Syringe are available with the reusable Carpuject™ Holder, List 2049-02. Carpuject™ Single-use cartridges are to be used ONLY with Carpuject™ Holders, List 2049-02. |
Route of Administration |
Dosage Form / Strength |
Non-medicinal Ingredients |
|||||
|
Intramuscular, Intravenous, Subcutaneous |
Sterile Solution for Injection / 2 mg/mL |
Citric acid, hydrochloric acid, sodium citrate, sodium chloride, sodium hydroxide, water for injection |
||||||
|
General
If necessary, HYDROmorphone may be given intravenously but the injection should be given very slowly. Rapid intravenous injection of narcotic analgesic agents, including HYDROmorphone, increases the possibility of adverse effects, such as hypotension and respiratory depression.
Use in Drug and Alcohol Addiction
Peri-Operative Considerations
Sexual Function / Reproduction
|
||||||||
PRINCIPAL DISPLAY PANEL - 1 mL Ampule Label
1 mL
DIN 02145901
ⓃHYDROmorphone
HCl Injection USP
2 mg / mL
SC-IM-IV
Sterile
Discard unused portion
Sandoz ? 1-800-361-3062
LOT
EXP
46183955
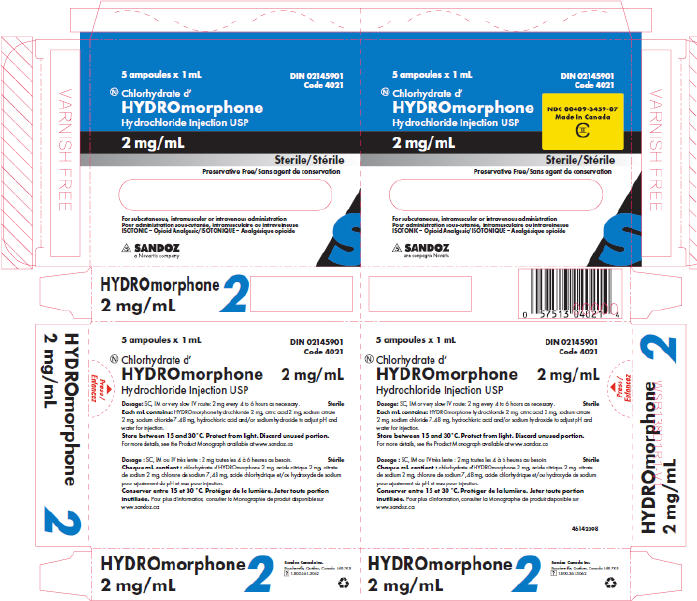
PRINCIPAL DISPLAY PANEL - 5 Ampule Carton
5 ampoules x 1 mL
NDC 00409-3459-07
Made In Canada
CII
DIN 02145901
Code 4021
Ⓝ Chlorhydrate d'
HYDROmorphone
Hydrochloride Injection USP
2 mg/mL
Sterile
Preservative Free
For subcutaneous, intramuscular or intravenous administration
ISOTONIC – Opioid Analgesic
SANDOZ
a Novartis company
PRINCIPAL DISPLAY PANEL - 10 Ampule Carton
10 ampoules x 1 mL
DIN 02145901
Ⓝ HYDROmorphone Hydrochloride Injection USP
NDC 00409-3459-07
Made In Canada
CII
2 mg / mL
Sterile
Preservative Free
For subcutaneous (SC), intramuscular (IM) or intravenous (IV) administration – ISOTONIC – Opioid Analgesic
SANDOZ
A Novartis
Division
| HYDROMORPHONE HYDROCHLORIDE
hydromorphone hydrochloride injection, solution |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - Hospira, Inc. (141588017) |