Label: zingo- lidocaine hydrochloride powder for intradermal use
-
Contains inactivated NDC Code(s)
NDC Code(s): 28000-105-12 - Packager: Anesiva, Inc.
- Category: HUMAN PRESCRIPTION DRUG LABEL WITH HIGHLIGHTS
- DEA Schedule: None
Drug Label Information
Updated June 25, 2008
If you are a consumer or patient please visit this version.
- Download DRUG LABEL INFO: PDF XML
- Official Label (Printer Friendly)
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
Zingo™ (lidocaine hydrochloride monohydrate powder intradermal injection system)
INDICATIONS AND USAGE
DOSAGE AND ADMINISTRATION
DOSAGE FORMS AND STRENGTHS
CONTRAINDICATIONS
Zingo™ is contraindicated in patients with a known history of sensitivity to local anesthetics of the amide type. (4)
WARNINGS AND PRECAUTIONS
ADVERSE REACTIONS
The most common adverse reactions (>5%) are skin reactions at the site of administration: erythema, petechiae, edema. (6.1)
Revised: April 2008See 17 for PATIENT COUNSELING INFORMATION.
Revised: 6/2008
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Instructions for Use
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Labor and Delivery
8.3 Nursing Mothers
8.4 Pediatric Use
8.5 Geriatric Use
9 DRUG ABUSE AND DEPENDENCE
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- *
- Sections or subsections omitted from the full prescribing information are not listed.
- N/A - Section Title Not Found In Database
- 1 INDICATIONS AND USAGE
-
2
DOSAGE AND ADMINISTRATION
Apply one Zingo™ (0.5 mg lidocaine hydrochloride monohydrate) to the site planned for venipuncture or intravenous cannulation, one to three minutes prior to needle insertion.
Perform the procedure within 10 minutes after Zingo™ administration.
Use Zingo™ only on intact skin.
Application of one additional Zingo™ at a new location is acceptable after a failed attempt at venous access. Multiple administrations of Zingo™ at the same location are not recommended.
When Zingo™ is used concomitantly with other products containing local anesthetic agents, the amount absorbed from all sources should be considered, as local anesthetics are thought to have at least additive toxicities.
2.1 Instructions for Use
Prepare the Treatment Site and Device: Examine the treatment site to ensure that the skin is intact. Clean the site, according to standard practice.
Visually inspect the pouch. Do not use if the pouch has been torn, or damaged or if the device has been dropped.
Tear open the pouch using the notch provided (Figure 1a). Remove Zingo™ from the pouch, being careful not to touch the purple outlet (open end) to avoid contamination (Figure 1b).
Figure 1a
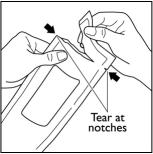
Figure 1b
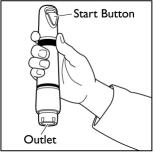
Position Zingo™: Grip Zingo™ and place on the application site, with one hand, as illustrated in Figure 2, or with both hands, as shown in Figure 3.
Figure 2

Figure 3

Ensure that the patient’s treatment site is supported to prevent movement. Seal the purple Zingo™ outlet against the patient’s skin. Hold the device perpendicular to the skin, making sure that your thumb can reach the green start button.
Avoid gaps between the skin and the Zingo™ outlet, like the one illustrated in Figure 4, as gaps will impede drug delivery.Figure 4

Release the Safety Interlock: Apply adequate downward pressure to release the safety interlock, while maintaining the seal between Zingo™ and the skin.
Zingo™ is ready for administration when the green start button has moved into the upward position, as illustrated in Figure 5a.
Figure 5a

Zingo™ cannot be actuated without releasing the internal safety interlock, as illustrated in Figure 5b.
Figure 5b
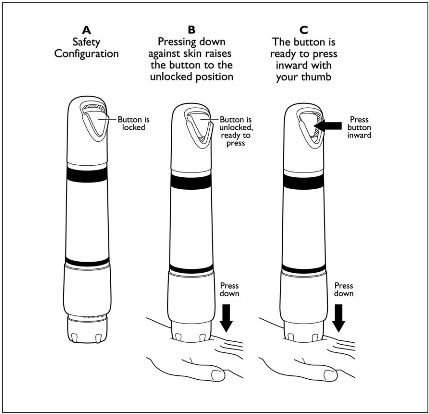
Administer Zingo™: While maintaining downward pressure, administer the dose by pressing the green start button, as illustrated in Figure 6. Do not move Zingo™ during administration. Actuation is accompanied by a “popping” sound, indicating that the dose has been discharged.
Figure 6

Remove Zingo™: Remove Zingo from the application site and dispose.
Begin Procedure: Start the venipuncture or intravenous cannulation procedure 1–3 minutes after Zingo™ administration. - 3 DOSAGE FORMS AND STRENGTHS
- 4 CONTRAINDICATIONS
-
5
WARNINGS AND PRECAUTIONS
Do not use around the eyes.
Do not use Zingo™ on body orifices, mucous membranes, or on areas with a compromised skin barrier. Only use Zingo™ on skin locations where an adequate seal can be maintained.
Patients with severe hepatic disease or pseudocholinesterase deficiency, because of their inability to metabolize local anesthetics normally, are at a greater risk of developing toxic plasma concentrations of lidocaine.
Patients with bleeding tendencies or platelet disorders could have a higher risk of superficial dermal bleeding.
-
6
ADVERSE REACTIONS
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
The safety of Zingo™ was evaluated in five randomized, double-blind, parallel-arm, sham-placebo controlled trials in which 1761 patients, ages 3 to 18, received either Zingo™ or a sham placebo device. A total of 906 received active treatment, while 855 received placebo.
Application Site Reaction
The application site was specifically assessed for four categories of skin site reaction (erythema, edema, pruritus, and petechiae). Erythema occurred in 53% of Zingo-treated patients, and in 27% of placebo-treated patients. Petechiae occurred in 44% of Zingo-treated patients, and in 5% of placebo-treated patients. Edema occurred in 8% of Zingo-treated patients, and in 3% of placebo-treated patients. Pruritus occurred in 1% of patients in both treatment groups.
Adverse Reactions
Amongst the 906 pediatric patients receiving active treatment and 855 pediatric patients receiving sham placebo treatment, the percentage of pediatric patients with any adverse reactions was approximately 9% in each treatment group.
Most adverse reactions were application-site related (i.e., bruising, burning, pain, contusion, hemorrhage), occurring in 4% of pediatric patients in each treatment group.
The most common systemic adverse reactions were nausea (2%) and vomiting (1%).
-
8
USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Zingo™ was not formally evaluated for effects on reproduction. Significant systemic exposure to lidocaine is not expected under recommended conditions of use of Zingo™ as lidocaine levels were below the limit of detection in human studies. Lidocaine has been previously tested for reproductive toxicity in animal studies, however. The following ratios are based on the assumption that the applied dose is completely absorbed through the skin.
Teratogenic Effects
Pregnancy Category B. Lidocaine was not teratogenic in rats given subcutaneous doses up to 60 mg/kg [360 mg/m2 or 1200-fold the single dermal administration (SDA) of 0.5 mg lidocaine in a 60 kg individual (0.3 mg/m2)] or in rabbits up to 15 mg/kg (180 mg/m2 or 600-fold the SDA). There are, however, no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, Zingo™ should be used during pregnancy only if clearly needed.
Nonteratogenic Effects
Lidocaine, containing 1:100,000 epinephrine, at a dose of 6 mg/kg (36 mg/m2 or 120-fold the SDA) injected into the masseter muscle of the jaw or into the gum of the lower jaw of Long-Evans hooded pregnant rats on gestation day 11 led to developmental delays in neonatal behavior among offspring. Developmental delays were observed for negative geotaxis, static righting reflex, visual discrimination response, sensitivity and response to thermal and electrical shock stimuli, and water maze acquisition. The developmental delays of the neonatal animals were transient with responses becoming comparable to untreated animals later in life. The clinical relevance of the animal data is uncertain. No adequate and well–controlled studies have been conducted in pregnant women. Because animal studies are not always predictive of human response, Zingo™ should be used during pregnancy only if the potential benefit justifies risk to the fetus.
8.2 Labor and Delivery
Lidocaine is not contraindicated in labor and delivery. In humans, the use of lidocaine for labor conduction analgesia has not been associated with an increased incidence of adverse fetal effects either during delivery or during the neonatal period. Should Zingo™ be used concomitantly with other products containing lidocaine, total doses contributed by all formulations must be considered.
8.3 Nursing Mothers
Lidocaine is excreted into human milk; therefore, caution should be exercised when Zingo™ is administered to a nursing mother. Because no plasma concentrations of lidocaine are detected after topical administration of Zingo™ in recommended doses, the small amount of lidocaine that would be ingested orally by a suckling infant is unlikely to cause adverse effects.
- 9 DRUG ABUSE AND DEPENDENCE
-
10
OVERDOSAGE
In adults following a single administration of Zingo™ the plasma levels of lidocaine were below the limit of detection (5 ng/mL). Signs of central nervous system (CNS) toxicity may start at plasma concentrations of lidocaine as low as 1000 ng/mL, and the risk of seizures generally increases with increasing plasma levels. Very high levels of lidocaine can cause respiratory arrest, coma, decreases in cardiac output, total peripheral resistance, and mean arterial pressure, ventricular arrhythmias, and cardiac arrest. The toxicity of coadministered local anesthetics is thought to be at least additive. In the absence of massive topical overdose or oral ingestion, other etiologies for the clinical effects or overdosage from other sources of lidocaine or other local anesthetics should be considered. The management of overdosage includes close monitoring, supportive care, and symptomatic treatment. Dialysis is of negligible value in the treatment of acute overdosage of lidocaine.
-
11
DESCRIPTION
Zingo™ (lidocaine hydrochloride monohydrate) powder intradermal injection system contains 0.5 mg of sterile lidocaine hydrochloride monohydrate.
The chemical name is 2-diethylamino-2',6'-acetoxylidide, monohydrochloride, monohydrate. The molecular formula is C14H22N2O · HCl · H2O with a molecular weight of 288.8 Da. Lidocaine hydrochloride monohydrate, a local anesthetic of the amide class, has the following structural formula:
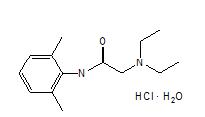
Lidocaine hydrochloride monohydrate is freely soluble in water, soluble in alcohol and chloroform, insoluble in ether, and melts at around 74–79°C.
Zingo™ is a ready-to-use, sterile, single-use, disposable, needle-free delivery system. Zingo™ consists of the following components: a drug reservoir cassette filled with 0.5 mg lidocaine hydrochloride monohydrate as a powder with a nominal particle size of 40 µm, a pressurized helium gas cylinder, and a safety interlock. The safety interlock prevents inadvertent actuation of the device. Once Zingo™ is pressed against the skin, the interlock is released, allowing the button to be depressed to actuate the device. A sound similar to that of a popping balloon is emitted at the time Zingo™ is actuated.
-
12
CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Zingo™ delivers lidocaine hydrochloride monohydrate into the dermis. Lidocaine is an amide-type local anesthetic agent that blocks sodium ion channels required for the initiation and conduction of neuronal impulses, resulting in local anesthesia.
12.2 Pharmacodynamics
Zingo™ provides local dermal analgesia within 1–3 minutes of application. Analgesia diminishes within 10 minutes of treatment.
12.3 Pharmacokinetics
Absorption
A single dose of Zingo™ in adults did not produce detectable plasma concentrations of lidocaine (limit of quantitation 5 ng/mL) in any subject tested (n = 38).
Application of Zingo™ to broken or inflamed skin, or multiple Zingo™ applications, could result in systemic plasma levels of lidocaine that could produce systemic toxicity.
Distribution
When lidocaine is administered intravenously to healthy volunteers, the steady-state volume of distribution is approximately 0.8 to 1.3 L/kg. At much higher plasma concentrations (1 to 4 mcg/mL of free base) than those found following application of Zingo™, the plasma protein binding of lidocaine is concentration dependent. Lidocaine crosses the placental and blood brain barriers, presumably by passive diffusion. CNS toxicity may typically be observed around 5000 ng/mL of lidocaine; however a small number of patients reportedly may show signs of toxicity at approximately 1000 ng/mL.
Metabolism
It is not known if lidocaine is metabolized in the skin. Lidocaine is metabolized rapidly by the liver to a number of metabolites including monoethylglycinexylidide (MEGX) and glycinexylidide (GX), both of which have pharmacologic activity similar to, but less potent than that of lidocaine. The major metabolic pathway of lidocaine, sequential N-deethylation to monoethylglycinexylidide (MEGX) and glycinexylidide (GX), is primarily mediated by CYP1A2 with a minor role of CYP3A4. The metabolite, 2,6-xylidine, has unknown pharmacologic activity. Following intravenous administration of lidocaine, MEGX and GX concentrations in serum range from 11% to 36% and from 5% to 11% of lidocaine concentrations, respectively. Serum concentrations of MEGX are about one-third the serum lidocaine concentrations.
Elimination
The half-life of lidocaine elimination from the plasma following intravenous administration is approximately 1.8 hours. Lidocaine and its metabolites are excreted by the kidneys. More than 98% of an absorbed dose of lidocaine can be recovered in the urine as metabolites or parent drug. Less than 10% of lidocaine is excreted unchanged in adults, and approximately 20% is excreted unchanged in neonates. The systemic clearance is approximately 8–10 mL/min/kg. During intravenous studies, the elimination half-life of lidocaine was statistically significantly longer in elderly patients (2.5 hours) than in younger patients (1.5 hours).
-
13
NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Long-term studies in animals have not been performed to evaluate the carcinogenic potential of lidocaine.
Mutagenesis
No mutagenic potential of lidocaine was demonstrated in the in vitro Ames Bacterial Reverse Mutation Assay, the in vitro chromosome aberration assay using Chinese hamster ovary cells, and the in vivo mouse micronucleus assay.
Impairment of Fertility
Zingo™ was not formally evaluated for effects on fertility. Significant systemic exposure to lidocaine is not expected under recommended conditions of use of Zingo™, as lidocaine levels were below the limit of detection in human studies. Lidocaine has been previously tested in animal studies for effects on fertility, however. The following ratios are based on the assumption that the applied dose is completely absorbed through the skin.
Lidocaine did not affect fertility in female rats when given via continuous subcutaneous infusion via osmotic minipumps up to doses of 250 mg/kg/day [1500 mg/m2 or 5000-fold higher than the SDA of 0.5 mg lidocaine in a 60 kg individual (0.3 mg/m2)]. Although lidocaine treatment of male rats increased the copulatory interval and led to a dose-related decreased homogenization resistant sperm head count, daily sperm production, and spermatogenic efficiency, the treatment did not affect overall fertility in male rats when given subcutaneous doses up to 60 mg/kg (360 mg/m2 or 1200-fold the SDA).
-
14
CLINICAL STUDIES
Efficacy in Pediatric Patients
The efficacy of Zingo™ in patients 3–18 years of age was evaluated in 2 randomized, double-blind, parallel-arm, sham-placebo controlled trials in which pediatric patients received either Zingo™ or a sham placebo device.
The overall patient population consisted of healthy pediatric patients as well as those with acute and chronic medical conditions (i.e., diabetes, asthma, seizure disorder, juvenile rheumatoid arthritis and renal or hepatic transplantation) ages 3–18 years. All patients required peripheral venipuncture or intravenous cannulation as part of their clinical care.
Two efficacy trials (Studies 1 and 2) were conducted during which patients were treated with Zingo™ or a placebo device at the back of hand or antecubital fossa, between one and three minutes prior to venipuncture or peripheral venous cannulation. Measurements of pain were made immediately following the venous procedure. Efficacy was measured using a modified version of the Wong-Baker FACES pain rating scale [a categorical 6-point scale containing 6 faces ranging from 0 (“no hurt”) to 5 (“hurts worst”)].
In both studies, treatment with active drug resulted in less pain, from venipuncture or peripheral IV cannulation, compared with placebo (See Table 1).
Table 1: Modified FACES Scale Score (ITT Population), Studies 1 and 2 Study 1 Study 2 Active
(N = 292)Placebo
(N = 287)Active
(N = 269)Placebo
(N = 266)Adjusted Mean
LSM11.77 2.10 1.38 1.77 Difference in LSMs (SE2) -0.33 (0.13) -0.39 (0.13) 95% Confidence Limits -0.58, -0.08 -0.65, -0.13
1least squares mean
2standard error -
16
HOW SUPPLIED/STORAGE AND HANDLING
NDC 28000-105-12 Zingo™ (lidocaine hydrochloride monohydrate) powder intradermal injection system contains 0.5 mg of sterile lidocaine hydrochloride monohydrate. Zingo™ is a single-use device packaged in an individual foil/clear pouch placed inside a bubble-wrap sleeve. Twelve sleeves are placed in labeled cartons.
Cartons are stored at controlled room temperature (15–30°C, 59–86°F).
-
17
PATIENT COUNSELING INFORMATION
Patients should be made aware that a sound similar to that of a popping balloon is emitted at the time Zingo™ is actuated.
Patients should be informed that skin reactions including erythema, petechiae and edema may occur.
Manufactured by:
Anesiva, Inc.
South San Francisco, CA 94080
Distributed by:
Sagent Pharmaceuticals, Inc.
Schaumburg, IL 60195 -
INGREDIENTS AND APPEARANCE
ZINGO
lidocaine hydrochloride powderProduct Information Product Type Item Code (Source) NDC:28000-105 Route of Administration INTRADERMAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength lidocaine hydrochloride (UNII: V13007Z41A) (lidocaine - UNII:98PI200987) 0.5 mg Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC:28000-105-12 12 in 1 CARTON 1 1 in 1 POUCH Labeler - Anesiva, Inc.